1636 CHAPTER 125 Electrolyte Disorders Camiron L. Pfennig and Corey M. Slovis Electrolyte abnormalities are common in emergency medicine and can vary greatly in importance, severity, and symptoms. Asymptomatic electrolyte abnormalities can usually be gradually corrected, but those that cause alterations in consciousness or life- threatening dysrhythmias require immediate therapy to avoid permanent sequelae or death. In some cases, therapy for life- threatening electrolyte disorders may even need to be initiated before laboratory results become available. HYPERKALEMIA Principles of Disease Hyperkalemia, defined as serum potassium level greater than 5.0 mEq/L, is the most dangerous acute electrolyte abnormality, potentially leading to life-threatening arrhythmias and death. Although hyperkalemia may have vague and varied symptoms, it is usually totally asymptomatic, with cardiac arrest as its first “symptom.” 1 Thus the diagnosis of hyperkalemia depends on paying specific attention to risk factors for impaired potassium excretion, such as dehydration and renal failure, along with an awareness of medications that cause potassium retention. Evalua- tion of the electrocardiogram (ECG) of patients at risk for this electrolyte disturbance is critical. Hyperkalemia can be rapidly progressive, and lifesaving interventions must be instituted at the earliest suspicion of toxicity. Upwards of 98% of potassium in the body is contained intracel- lularly, whereas less than 2% remains circulating in the blood. Serum potassium concentration is normally between 3.5 and 5.0 mEq/L and is tightly regulated by the kidney. In the healthy state, at least 90% of potassium excretion occurs through the kidney; in the renally impaired state, the gastrointestinal tract may account for roughly 25% of excretion. Hyperkalemia usually develops from impaired renal excretion or increased release from cells; however, in advanced chronic kidney disease or end-stage renal disease, dietary intake of potassium may be a significant factor in its development. 2 Hyperkalemia causes cardiotoxicity by increasing the resting membrane potential of the cardiac myocyte, causing “membrane excitability” and conversely sluggish depolarization as well as decreasing the duration of repolarization. At very high levels, potassium causes the depolarization threshold to rise, leading to overall depressed cardiac function. Nearly any cardiac arrhythmia can be seen with hyperkalemia, including heart blocks, bradydys- rhythmias, pseudoinfarction ST segment elevation, and the classic “sine wave” pattern. As hyperkalemia advances, the end result is cardiac arrest, usually from disintegration into ventricular fibrillation, pulseless electrical activity, or asystole. A serum potas- sium level of 10.0 mEq/L is usually fatal, but decompensation and death can occur at any level above 7 to 8 mEq/L. The most common cause of hyperkalemia is spurious elevation due to hemolysis during or after the blood draw. Thus an ECG should be used to assess for true hyperkalemia while another sample is analyzed. Most causes of true hyperkalemia are due to release from cells or renal insufficiency. Renal failure is the most common cause of confirmed hyperkalemia and is often com- pounded by medications that further impair renal potassium handling. Box 125-1 organizes the most common causes of hyper- kalemia. The presence of one of these conditions may be the lone historical clue in hyperkalemia. 3 Clinical Features Hyperkalemia remains a difficult clinical diagnosis to make on clinical grounds alone. It is not uncommon for a patient with mild to moderate hyperkalemia to be identified during routine blood sampling for an unrelated condition. Patients with moderate to severe hyperkalemia may have gastrointestinal effects such as nausea, vomiting, and diarrhea often in association with their underlying disease. Neuromuscular findings, including muscle cramps, generalized weakness, paresthesias, tetany, and focal or global paralysis, may be seen in patients with severe hyperkalemia. The signs and symptoms of progressive muscle weakness, pares- thesias, dyspnea, and depressed deep tendon reflexes are neither sensitive nor specific, nor do they appear reliably with a particular serum potassium level. 3 Patients with severe hypokalemia may present with hemodynamic instability and cardiac arrhythmias requiring immediate intervention. Diagnostic Strategies The ECG is helpful in making the diagnosis of hyperkalemia and can be used in unstable patients to initiate treatment (Figs. 125-1 to 125-3). Classic electrocardiographic changes—the peaked T wave, flattened p wave with prolonged PR interval or a totally absent P wave, wide QRS, and sine wave pattern, portending imminent cardiac arrest—have been well described as appearing sequentially with rising serum potassium levels. 4,5 Peaked T waves usually appear as serum potassium levels exceed 5.5 to 6.5 mEq/L; P wave disappearance and PR prolongation are common with levels above 6.5 to 7.5 mEq/L; and QRS prolongation is seen with potassium levels above 7.0 to 8.0 mEq/L. Although these changes may occur in only half the patients, recognition of these patterns

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1636
CHAPTER 125
Electrolyte DisordersCamiron L. Pfennig and Corey M. Slovis
Electrolyte abnormalities are common in emergency medicine and can vary greatly in importance, severity, and symptoms. Asymptomatic electrolyte abnormalities can usually be gradually corrected, but those that cause alterations in consciousness or life-threatening dysrhythmias require immediate therapy to avoid permanent sequelae or death. In some cases, therapy for life-threatening electrolyte disorders may even need to be initiated before laboratory results become available.
HYPERKALEMIA
Principles of Disease
Hyperkalemia, defined as serum potassium level greater than 5.0 mEq/L, is the most dangerous acute electrolyte abnormality, potentially leading to life-threatening arrhythmias and death. Although hyperkalemia may have vague and varied symptoms, it is usually totally asymptomatic, with cardiac arrest as its first “symptom.”1 Thus the diagnosis of hyperkalemia depends on paying specific attention to risk factors for impaired potassium excretion, such as dehydration and renal failure, along with an awareness of medications that cause potassium retention. Evalua-tion of the electrocardiogram (ECG) of patients at risk for this electrolyte disturbance is critical. Hyperkalemia can be rapidly progressive, and lifesaving interventions must be instituted at the earliest suspicion of toxicity.
Upwards of 98% of potassium in the body is contained intracel-lularly, whereas less than 2% remains circulating in the blood. Serum potassium concentration is normally between 3.5 and 5.0 mEq/L and is tightly regulated by the kidney. In the healthy state, at least 90% of potassium excretion occurs through the kidney; in the renally impaired state, the gastrointestinal tract may account for roughly 25% of excretion. Hyperkalemia usually develops from impaired renal excretion or increased release from cells; however, in advanced chronic kidney disease or end-stage renal disease, dietary intake of potassium may be a significant factor in its development.2
Hyperkalemia causes cardiotoxicity by increasing the resting membrane potential of the cardiac myocyte, causing “membrane excitability” and conversely sluggish depolarization as well as decreasing the duration of repolarization. At very high levels, potassium causes the depolarization threshold to rise, leading to overall depressed cardiac function. Nearly any cardiac arrhythmia can be seen with hyperkalemia, including heart blocks, bradydys-rhythmias, pseudoinfarction ST segment elevation, and the classic “sine wave” pattern. As hyperkalemia advances, the end
result is cardiac arrest, usually from disintegration into ventricular fibrillation, pulseless electrical activity, or asystole. A serum potas-sium level of 10.0 mEq/L is usually fatal, but decompensation and death can occur at any level above 7 to 8 mEq/L.
The most common cause of hyperkalemia is spurious elevation due to hemolysis during or after the blood draw. Thus an ECG should be used to assess for true hyperkalemia while another sample is analyzed. Most causes of true hyperkalemia are due to release from cells or renal insufficiency. Renal failure is the most common cause of confirmed hyperkalemia and is often com-pounded by medications that further impair renal potassium handling. Box 125-1 organizes the most common causes of hyper-kalemia. The presence of one of these conditions may be the lone historical clue in hyperkalemia.3
Clinical Features
Hyperkalemia remains a difficult clinical diagnosis to make on clinical grounds alone. It is not uncommon for a patient with mild to moderate hyperkalemia to be identified during routine blood sampling for an unrelated condition. Patients with moderate to severe hyperkalemia may have gastrointestinal effects such as nausea, vomiting, and diarrhea often in association with their underlying disease. Neuromuscular findings, including muscle cramps, generalized weakness, paresthesias, tetany, and focal or global paralysis, may be seen in patients with severe hyperkalemia. The signs and symptoms of progressive muscle weakness, pares-thesias, dyspnea, and depressed deep tendon reflexes are neither sensitive nor specific, nor do they appear reliably with a particular serum potassium level.3 Patients with severe hypokalemia may present with hemodynamic instability and cardiac arrhythmias requiring immediate intervention.
Diagnostic Strategies
The ECG is helpful in making the diagnosis of hyperkalemia and can be used in unstable patients to initiate treatment (Figs. 125-1 to 125-3). Classic electrocardiographic changes—the peaked T wave, flattened p wave with prolonged PR interval or a totally absent P wave, wide QRS, and sine wave pattern, portending imminent cardiac arrest—have been well described as appearing sequentially with rising serum potassium levels.4,5 Peaked T waves usually appear as serum potassium levels exceed 5.5 to 6.5 mEq/L; P wave disappearance and PR prolongation are common with levels above 6.5 to 7.5 mEq/L; and QRS prolongation is seen with potassium levels above 7.0 to 8.0 mEq/L. Although these changes may occur in only half the patients, recognition of these patterns

Chapter 125 / Electrolyte Disorders 1637
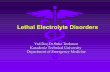
Figure 125-1. Hyperkalemia with QRS widening merging into T wave, absent P wave.
I
II
III
IV
aVF
aVL
aVR V1
V2
V3
V4
V5
V6
BOX 125-1
Spurious elevation Hemolysis due to drawing or storing of the laboratory sample or post–blood sampling leak from markedly elevated white blood cells, red blood cells, or platelets
Renal failure Acute or chronicAcidosis Diabetic ketoacidosis, Addison’s disease,
adrenal insufficiency, type 4 renal tubular acidosis
Cell death Rhabdomyolysis, tumor lysis syndrome, massive hemolysis or transfusion, crush injury, burn
Drugs Beta-blockers, acute digitalis overdose, succinylcholine, angiotensin-converting enzyme inhibitors, angiotension receptor blockers, nonsteroidal anti-inflammatory drugs, spironolactone, amiloride, potassium supplementation
Five Most Common Causes of Hyperkalemia
Figure 125-2. Hyperkalemia in the same patient as in Figure 125-1 after potassium-lowering therapy has begun. Tall peaked T waves, decreased P wave.
I
II
III
VI
V5
150 Hz 25.0 mm/s 10.0 mm/mV 4 by 2.5s + 3 rhythm lds 12SLTMv237oMAC5K 008B
I
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
hyperkalemia should not be the sole reason to treat a stable patient not likely to have an elevated potassium concentration until serum levels have returned.3
Management
Patients with suspected or known hyperkalemia require intrave-nous access and continuous cardiac monitoring. The treatment of hyperkalemia is based on the clinical scenario combined with the 12-lead ECG and the laboratory potassium value. The treatment strategy consists of three main steps: stabilization of the cardiac membrane, shifting of potassium into the cells, and then removal of potassium from the body. In patients who do not require urgent treatment, lowering of total body potassium may be the only step necessary. A variety of treatment options are considered for the acute management of hyperkalemia, including calcium, insulin, beta2-adrenergic agonists, sodium bicarbonate, resins, and dialysis (Table 125-1).
Intravenous calcium is used to stabilize the cardiac membrane by restoring the electrical gradient. Calcium increases the depo-larization threshold and the calcium gradient across the cardiac membrane, quieting myocyte excitability and increasing cardiac conduction speed, thus narrowing the QRS. Calcium does not decrease serum potassium levels, and its effect is rapid but tran-sient. The dose is one ampule, or 10 mL of 10% calcium chloride
when they are present is vital to rapid diagnosis and initiation of lifesaving treatment.6 A serum potassium level above 5.0 mEq/L is diagnostic of hyperkalemia, but the value itself does not always predict electrocardiographic changes or the degree of car-diotoxicity. Subtle electrocardiographic changes consistent with

1638 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
solution. Some authors prefer calcium gluconate rather than calcium chloride on the basis of the reduced risk of tissue necrosis should it extravasate at the injection site.4,5 More than 10 mL of calcium gluconate will often be required as it contains only one third the calcium contained in calcium chloride. Calcium gluconate is also preferred in pediatric cases as well as in more chronic, less emergent hyperkalemic patients when a slow infusion is desired.
Potassium can be shifted intracellularly with beta2-agonists, insulin, saline, and potentially sodium bicarbonate. Insulin is the most reliable agent to move potassium into cells, but beta2-adrenergic receptor agonists also provide benefit in some patients. Insulin, given intravenously in combination with glucose to
Figure 125-3. The same patient as in Figures 125-1 and 125-2 after dialysis. The electrocardiogram is now normal.
I
II
II
VI
V5
III
aVR V1 V4
aVL V2 V5
aVF V3 V6
150 Hz 25.0 mm/s 10.0 mm/mV 4 by 2.5s + 3 rhythm lds 12SLTMv237oMAC5K 008B
TREATMENT MEDICATION FEATURES
Stabilize cardiac membrane
Calcium chloride (10 mL, maximum 20 mL) or calcium gluconate (10-30 mL), IV push
For wide QRS, restores the electrical gradient; does not decrease serum potassium
Shift potassium into cells
Insulin, 10 units, IV push, combined with 100 mL of 50% dextrose, IV pushHigh-dose nebulized albuterol by face mask (15-25 mg by continuous inhalation)Bicarbonate 50-100 mLNormal saline 100-250 mL
If severely acidoticIn conjunction with nephrologist if dialysis dependent
Remove potassium from the body
HemodialysisNormal saline and furosemideIon exchange resin
Emergently in cardiac arrest, urgently in renal failure; may delay if renal function is normalIn patients with rhabdomyolysis or tumor lysis syndrome with intact urine outputNot effective acutely
Table 125-1 Treatment of Hyperkalemiaprevent hypoglycemia, also shifts potassium into cells by stimula-tion of the Na+,K+-ATPase pump. The onset of action is less than 15 minutes, and the effect is maximal between 30 and 60 minutes, with a maximal drop of 0.6 mEq/L on average.
Nebulized albuterol by face mask is effective in shifting potas-sium into cells by stimulation of the Na+,K+-ATPase pump.6 Nebu-lized albuterol begins to take measurable effect after 15 minutes and lowers the serum potassium level by 0.5 to 1 mEq/L, depend-ing on the dose.7 The effective dose is at least four times higher than that typically used for bronchodilation.8 Mild tachycardia is the main side effect but is generally well tolerated. The combina-tion of nebulized albuterol and insulin with glucose appears to be additive, lowering serum potassium by a mean of 1.2 mEq/L.9
Saline infusions also stimulate the Na+,K+-ATPase pump, and only a few hundred milliliters is required for beneficial effects. Saline infusions are given judiciously in anuric patients and usually in consultation with the nephrologist. Sodium bicarbonate is effective only in hyperkalemic patients who are acidotic and has no benefit when it is used for hyperkalemia in nonacidotic patients.10 Sodium bicarbonate buffers hydrogen ions extracellu-larly while shifting potassium intracellularly but should be reserved for patients with confirmed acidosis. Although intravenous mag-nesium also can drive potassium intracellularly, it should never be used in hyperkalemia as most patients with elevated potassium levels are also at risk for concomitant hypermagnesemia.
Potassium can best be removed from the body acutely by hemo-dialysis. Hemodialysis effectively and reliably decreases serum potassium levels by at least 1 mEq/L in the first hour and another 1 mEq/L during the next 2 hours.7,11 It is the only reliable method of potassium removal that has been experimentally studied and should be instituted early in the treatment of life-threatening hyperkalemia in patients with renal failure. In patients with intact renal function, medical management alone is usually sufficient, even in extreme cases, and hemodialysis may not be necessary unless multiple medical modalities fail. There are no randomized trials addressing the use of diuretics such as furosemide in the emergent management of hyperkalemia, but in cases such as rhab-domyolysis or tumor lysis syndrome, it may be appropriate to use a normal saline infusion supplemented by furosemide to enhance diuresis and potassium excretion in the urine.
Cation exchange resins, such as sodium polystyrene sulfonate (Kayexalate), have not been shown to decrease the serum

Chapter 125 / Electrolyte Disorders 1639
or osmotic diuretics to cause hypokalemia, but both the thiazide and loop diuretics block chloride-associated sodium and increase delivery of sodium to the collecting tubules. Hypokalemia is a common adverse effect of treatment with diuretics and may cause fatal arrhythmias and increase the risk of digitalis toxicity.23 In addition to diuretics, other drugs and disorders can cause signifi-cant renal potassium losses, including hyperaldosteronism, steroid excess, metabolic acidosis, DKA, renal tubular acidosis, and alcohol consumption. Penicillin and its synthetic derivatives, when they are given in large doses, promote renal potassium excretion by increasing sodium delivery to the distal nephron.
Individuals with secondary hyperaldosteronism, whether it is due to congestive heart failure (CHF), hepatic insufficiency, or nephrotic syndrome, may also exhibit hypokalemia. Patients with renal tubular acidosis can become hypokalemic because a defect in the distal tubule leads to increased potassium excretion.
Administration of insulin may cause a reduction in serum potassium because of insulin’s ability to stimulate the Na+,K+-ATPase pump and move potassium intracellularly; hypokalemia can be a dangerous complication with intentional overdoses of insulin and during treatment of DKA. Although most patients with DKA present with high-normal or mildly elevated serum potassium levels, patients are usually 2 to 3 mEq/kg body weight deficient in total body potassium.24 Failure to appreciate this total body deficit—and to not begin potassium infusion once significant hyperkalemia has been ruled out and intact renal function confirmed—may lead to otherwise unexplained arrhyth-mias or cardiac arrest in patients hours after their initial therapy has begun.
Hypokalemia can also occur from gastrointestinal and dermal losses. In diarrheal states, large quantities of potassium can be lost as the volume of stool increases and secondary hyperaldosteron-ism can occur. Although hypokalemia is often seen after pro-tracted vomiting or nasogastric suctions, only 5 to 10 mEq/L of potassium is lost in gastric fluid. The hypokalemia is secondary to the resultant metabolic alkalosis, chloride losses, and hyperaldo-steronism. Large doses of laxatives and repeated enemas cause excessive potassium loss in the stool and can cause hypokalemia. On occasion, excessive sweating can lead to hypokalemia from losses of potassium through the skin. In addition, patients with extensive burns can also suffer from hypokalemia because of sig-nificant losses from the skin.
Dietary potassium deficiency should be considered in the severely malnourished patient and the chronic alcoholic.25 When poor potassium intake is combined with increased nonrenal losses, severe hypokalemia can result. Hypokalemia can also result from an acute shift of potassium from the extracellular compart-ment into cells. This is most commonly seen in patients with metabolic alkalosis, in patients with hyperventilation, and in those patients taking medications such as beta-agonists or deconges-tants. Beta receptor stimulation can lead to hypokalemia, espe-cially in patients using repetitive and high doses of beta-agonists for chronic obstructive pulmonary disease or asthma. Albuterol-induced hypokalemia can occur even at normal therapeutic doses.26 A standard dose of nebulized albuterol reduces serum potassium by 0.2 to 0.4 mEq/L, and a second dose taken within 1 hour has the potential to reduce it by almost 1 mEq/L. Patients with starvation or near-starvation may suffer from hypokalemia when they are fed because insulin secretion and increased cellular uptake can cause an acute intracellular migration of potassium.
Clinical Features
Hypokalemia is usually asymptomatic but can be manifested with nonspecific complaints, including palpitations, skeletal muscle weakness, easy fatigability, depression, and muscle pain.
potassium level within the first 4 hours of treatment and should not be used in the acute management of hyperkalemia.12
Hyperkalemia is seen in diabetic ketoacidosis (DKA), although most hyperkalemic patients with DKA are actually total body defi-cient of potassium. In this insulin-deficient and acidotic state, serum potassium levels rise because of cellular shifts. Simply treat-ing the patient’s underlying DKA will also treat the hyperkalemia. In fact, the mainstay of treatment of DKA—fluids and insulin—closely mirrors the treatment of hyperkalemia itself.13
As hyperkalemia progresses, the end result will be cardiopulmo-nary arrest due to ventricular fibrillation, pulseless electrical activ-ity, or asystole. In a known or suspected hyperkalemic arrest, an approach beginning with standard advanced cardiac life support combined with the use of multiple potassium-lowering medica-tions is rational.14,15 Epinephrine has been shown to lower potas-sium by 0.25 mEq/L.16,17 Calcium chloride is given immediately by intravenous push, followed by insulin and glucose. Bicarbonate should be given by bolus dose if the patient is believed to be aci-dotic. Emergent hemodialysis is recommended if it is readily avail-able. Hemodialysis through central venous access can be used during ongoing cardiopulmonary resuscitation to acutely lower the serum potassium level and may result in return of spontane-ous circulation with intact neurologic status despite prolonged resuscitative efforts and failure of conventional medications and defibrillation.18
HYPOKALEMIA
Principles of Disease
Hypokalemia is the most common electrolyte abnormality encountered in clinical practice. When it is defined as a value of less than 3.5 mEq/L, hypokalemia is found in more than 20% of hospitalized patients and in 10 to 40% of patients treated with thiazide diuretics in the outpatient setting.19 Although hypokale-mia is usually asymptomatic, severe cardiac dysrhythmias and rhabdomyolysis can occur secondary to potassium’s effect on the heart and muscle.20 The five most common causes of hypokalemia are renal losses, increased nonrenal losses, decreased potassium intake, intracellular shift, and endocrine etiologies (Box 125-2). Hypokalemia is often seen in association with hypomagnesemia, and patients with low serum potassium levels should be assumed to be hypomagnesemic also.20-22
Increased excretion of potassium, especially coupled with poor intake, is the most common cause of hypokalemia, and patients receiving diuretics represent the single most common patient group encountered in clinical practice. Hypokalemia from thia-zide diuretics occurs through increases in distal sodium delivery in the nephron and by activation of the renin-angiotensin- aldosterone system. Thiazide diuretics are more likely than loop
BOX 125-2
Renal losses Diuretic use, drugs, steroid use, metabolic acidosis, hyperaldosteronism, renal tubular acidosis, diabetic ketoacidosis, alcohol consumption
Increased nonrenal losses
Sweating, diarrhea, vomiting, laxative use
Decreased intake Ethanol, malnutritionIntracellular shift Hyperventilation, metabolic alkalosis, drugsEndocrine Cushing’s disease, Bartter’s syndrome,
insulin therapy
Five Most Common Causes of Hypokalemia

1640 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
that it may also cause a prolonged QT interval. Once the QT interval becomes longer than 500 milliseconds, the risk of malig-nant ventricular arrhythmias and torsades de pointes increases dramatically.28 Hypokalemia is also notorious for causing nonspe-cific ST and T wave changes. In addition, prolonged potassium depletion of even modest proportion can provoke or exacerbate kidney injury or hypertension. A severe degree of hypokalemia with paralysis is a potentially life-threatening medical emergency; measurement of relative urinary potassium excretion and an assessment of the acid-base status might help narrow the differ-ential diagnosis in the emergency setting.
Management
Potassium is an intracellular cation, so a low serum potassium level almost always reflects a significant total potassium deficit. When treating hypokalemia, one should remember that each 0.3 mEq potassium drop below normal correlates with an approx-imately 100 mEq total body deficit.29 Patients who have mild or moderate hypokalemia are usually asymptomatic or present with minor symptoms. These patients may only need oral potassium replacement therapy if they do not have nausea or vomiting as the cause of their hypokalemia. Oral replacement is available in liquid, powder, and tablet form. Potassium chloride is the most com-monly used supplementation, and 40 to 60 mEq orally every 2 to 4 hours is typically well tolerated. If the cause of hypokalemia is not clear or the hypokalemia is severe and associated with profound weakness, obtain a spot urine potassium level before starting therapy to assess whether the patient’s kidneys are inap-propriately wasting potassium from a renal or endocrine cause.
Although short periods of mild potassium depletion are typically well tolerated in healthy individuals, severe potassium depletion can result in serious cardiovascular instability, neurologic dys-function, glucose intolerance, gastrointestinal symptoms, and renal failure as well as affect the acid-base balance in the body.27 The likelihood of symptoms appears to correlate with the rapidity of the decrease in serum potassium. In patients without underly-ing heart disease, abnormalities in cardiac conduction are extremely unusual, even when the serum potassium concentration is below 3.0 mEq/L. Paresthesias, depressed deep tendon reflexes, fasciculations, muscle weakness, and confusion can occur when the serum potassium level is less than 2.5 mEq/L. However, in patients with cardiac ischemia or heart failure, even mild to mod-erate hypokalemia increases the likelihood of cardiac arrhythmias secondary to potassium’s effect on the action potential. The data linking hypokalemia with arrhythmias and cardiac arrest in acute myocardial infarction are fairly strong, but the direct myo-cardial stimulatory effects of increased circulating epinephrine is a possible confounder.20 Hypokalemia is an independent risk factor contributing to reduced survival of cardiac patients and increased incidence of arrhythmic death. On the basis of available evidence, it appears best to attempt to maintain a serum potas-sium concentration above 4.5 mEq/L in patients having an acute myocardial infarction. Hypokalemic patients can demonstrate first- and second-degree heart block, atrial fibrillation, ventricular fibrillation, and asystole. Hypokalemia can also promote meta-bolic acidosis.
Hypokalemic periodic paralysis is a rare disorder characterized by potentially fatal episodes of muscle weakness through the involvement of the respiratory muscles. Life-threatening cardiac arrhythmias are managed by restoration of serum potassium levels into the normal range.28
Diagnostic Strategies
Hypokalemia is rarely suspected on the basis of clinical presenta-tion, and the diagnosis is typically made by measurement of the serum potassium concentration during routine laboratory study. If there is any suspicion for hypokalemia or a patient presents with generalized weakness, palpitations, or arrhythmias, an ECG should be obtained. Just as a tall-peaked T wave is characteristic of hyperkalemia, a flattened T wave can be seen in hypokalemia. U waves, which are small deflections after the T wave, may also be seen (Figs. 125-4 and 125-5). The real danger of hypokalemia is
Figure 125-4. Hypokalemic electrocardiographic changes, including flattened T wave, prolonged QT interval, nonspecific ST changes, and prominent U wave (arrow).
I aVR V1 V4
II aVL V2 V5
III
VI
aVF V3 V6
Figure 125-5. Electrocardiographic changes in hypokalemia.
Prolonged Q-T interval
STdepression
Flat T waveU wave
Hypokalemia

Chapter 125 / Electrolyte Disorders 1641
Patients in whom severe hypokalemia is suspected should be immediately placed on a cardiac monitor and intravenous access secured.
Treatment of hypokalemia is essential in multiple populations of patients. Hypokalemia is arrhythmogenic, especially in the set-tings of acute myocardial infarction, high catecholamine states, and hypertrophied or dilated ventricles. Hypokalemia is an impor-tant independent risk factor for morbidity and mortality in patients with heart failure. Correction of serum potassium levels to between 4.0 and 5.0 mEq/L is important in these patients.30
If intravenous infusion is necessary, potassium chloride at a rate of 10 to 20 mEq/hr is considered safe. Potassium may burn patients with small veins, so small amounts of lidocaine can be added to the intravenous solution. In the rare instance in which intravenous repletion is planned at more than 20 mEq/hr, closely monitor the patient with continuous cardiac monitoring and establish central line access.
Hypokalemia is associated with hypomagnesemia, and the severity of the hypokalemia correlates with a similar degree of hypomagnesemia.31 Magnesium replacement should usually accompany potassium repletion. Unless the patient receives at least 0.5 g/hr of magnesium sulfate along with potassium replace-ment, potassium will not move intracellularly and the patient will lose potassium through excretion.22 Correction of large potassium deficits may require several days, and oral and intravenous replace-ment can occur simultaneously.
HYPERNATREMIA
Principles of Disease
Hypernatremia is defined as a serum sodium concentration above 145 mEq/ L and is usually associated with a poor prognosis. It is uncommon in previously normal patients, and in adults it is almost exclusively due to a total body water deficit.32 Most hyper-natremic patients have either an impaired sense of thirst or no access to water. Thus elders, infants, patients in coma or with mental impairment, and those who are intubated and paralyzed are at highest risk for this disorder.33,34 Hypernatremia can be divided into three physiologic pairings (Box 125-3). Diabetes insipidus, a condition that results in insufficient production of or lack of response to antidiuretic hormone, can lead to life-threatening hypernatremia35 (Box 125-4).
Clinical Features
Hypernatremia is a disease seen predominantly in elders, but it can also be seen in patients who depend on others to provide them with water, including infants, intubated patients, and persons with mental debilitation.36,37 In addition, patients will also have multi-factorial causes leading to severe hypernatremia.38 Patients may complain of polyuria or polydipsia or have obvious causes of extrarenal fluid losses; others may have no complaints at all.
Hypernatremia should be considered in any patient presenting with altered mental status, especially individuals with severe mental retardation, cerebral palsy, and head injury, as well as in bed-ridden patients who have no access to water.
Diagnostic Strategies
In addition to routine serum chemistries, serum osmolarity and urine sodium concentration and osmolality should be obtained. The degree of hypernatremia almost always equals the total body water deficit in adults. The patient’s total body water (TBW) deficit can be estimated by the formula
TBW deficit TBW serum Na= × −+( / )140 1
BOX 125-4
CentralIdiopathicFamilial diseaseCancerHypoxic encephalopathyInfiltrative disordersPostsupraventricular tachycardiaAnorexia nervosa
NephrogenicChronic renal insufficiencyPolycystic kidney diseaseLithium toxicity93
HypercalcemiaHypokalemiaTubulointerstitial diseaseHereditarySickle cell disease
More Common Causes of Diabetes Insipidus
BOX 125-3
Hypernatremia with dehydration and low total body sodium
HeatstrokeIncreased insensible losses: burns, sweating
Gastrointestinal loss: diarrhea, protracted vomiting, continuous gastrointestinal suction
Osmotic diuresis: glucose, mannitol, enteral feeding
Hypernatremia with low total body water and normal total body sodium
Diabetes insipidusNeurogenicElderly with “reset” osmostatHypothalamic dysfunctionSuprasellar or infrasellar tumorsRenal diseaseDrugs (amphotericin, phenytoin, lithium, aminoglycosides, methoxyflurane)
Sickle cell diseaseHypernatremia with increased total body sodium
Salt tablet ingestionSalt water ingestion92
Saline infusionsSaline enemasIntravenous sodium bicarbonatePoorly diluted interval feedingsPrimary hyperaldosteronismHemodialysisCushing’s syndromeConn’s syndrome
Three Types of Hypernatremia
A patient’s total body water is usually calculated by multiplying the patient’s body weight in kilograms times 0.6. However, because of percentage body fat differences based on the age and sex of the patient, it is more accurate to use the correction factors listed in Table 125-2.
Management
The treatment of hypernatremia has three interdependent goals: first, to quickly correct underlying shock, hypoperfusion, or sig-nificant hypovolemia with normal saline; second, to treat the underlying cause of hypernatremia, such as fever, vomiting, or diabetes insipidus; and third, to carefully lower the serum sodium level, usually by replacement of the body’s total water deficit.39 Until hypoperfusion and hypovolemia are corrected, homeostatic

1642 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
mechanisms for sodium balance will promote sodium resorption to maintain intravascular volume, even at the expense of the serum sodium concentration.
The rate of correction in hypernatremia is extremely important to minimize morbidity and mortality. In adult patients who have had hypernatremia during a short time as a result of sodium loading, “rapid correction” at 1 to 2 mEq/hr lowering of serum sodium appears relatively safe.39,40 However, most adult patients have hypernatremia during days to weeks. In this group of patients, serum sodium concentration should be slowly corrected at no more than 0.5 mEq/hr or 10 to 12 mEq/day.
Normal saline can typically be started for volume replacement until the patient is hemodynamically stable and then changed to half-normal saline at 100 mL/hr once vital signs have normalized. The treatment of central diabetes insipidus with desmopressin (DDAVP) is an effective means of improving polyuria and hyper-natremia; initial doses in the acute setting range from 1 to 2 µg.33
HYPONATREMIA
Principles of Disease
Hyponatremia, defined as serum sodium concentration of less than 135 mEq/L, is the second most common electrolyte abnor-mality encountered in clinical practice.37 It is important to recog-nize hyponatremia because of its potential morbidity and also because it can be a marker of underlying disease. The most common causes of severe hyponatremia in adults are therapy with thiazides, the postoperative state including transurethral prosta-tectomy, the syndrome of inappropriate secretion of antidiuretic hormone (SIADH), polydipsia in psychiatric patients, and unin-tentional water intoxication. Gastrointestinal fluid loss, ingestion of overly dilute formula, accidental ingestion of excessive water, and receipt of multiple tap-water enemas are the main causes of severe hyponatremia in infants and children. Most patients pre-senting to the emergency department (ED) with hyponatremia are asymptomatic and do not require emergent therapy. If symptoms are present, they are typically based on the degree of hyponatremia and how acutely the hyponatremia developed. Symptoms range from headache, nausea, and vomiting to confusion, seizures, and coma. There are two groups of hyponatremic patients that will require treatment with either normal saline or hypertonic saline: (1) severe but asymptomatic hyponatremia with a sodium level of 110 mEq/L or less and (2) acute symptomatic hyponatremia with a sodium level below 120 mEq/L.
Central nervous system (CNS) damage due to hyponatremia may be caused by cerebral edema and increased intracranial pres-sure, by osmotic fluid shifts during overly aggressive treatment, or by both. When they are subjected to a hyponatremic environment, neurons become depleted of sodium and potassium in an attempt to limit their own osmolarity to prevent intracellular fluid shifts that would lead to cerebral edema. If fluid therapy raises extracel-lular sodium levels too quickly, fluids shift out of neurons and diffuse demyelination may occur, leading to flaccid paralysis and often death due to a syndrome most commonly referred to as
POPULATION TOTAL BODY WATER
Children and adult men Body weight (kg) × 0.6
Adult women Body weight (kg) × 0.5
Elderly men Body weight (kg) × 0.5
Elderly women Body weight (kg) × 0.45
Table 125-2 Calculation of Body Water
central pontine myelinolysis, although it is more accurately labeled the osmotic demyelinating syndrome.41
Although hyponatremia has many causes, they fall into four general categories: pseudohyponatremia, hyponatremia with dehydration and decreased extracellular volume, hyponatremia with increased extracellular volume, and euvolemic hyponatremia with increased total body water (Box 125-5).
Pseudohyponatremia
Pseudohyponatremia is a falsely low sodium reading caused by the presence of other osmolar particles in the serum. The phenome-non of pseudohyponatremia is explained by the increased percent-age of large molecular particles relative to sodium. These large molecules do not contribute to plasma osmolality, resulting in a state in which the relative sodium concentration is decreased but the overall osmolality remains unchanged. Severe hypertriglyceri-demia and hyperproteinemia are two common causes of this con-dition.42 Blood draw or laboratory error should also be considered a possible cause of a patient’s hyponatremia, especially if the blood sample was drawn near an infusion site using 5% dextrose in water (D5W) or 5% dextrose in half-normal saline or when a very abnor-mal sodium level is reported in an otherwise healthy patient.
Hyperglycemia is sometimes considered a cause of pseudo-hyponatremia; however, it actually causes a dilutional hyponatre-mia by pulling water into the vascular space by osmosis. Two
BOX 125-5
Pseudohyponatremia HyperlipidemiaHyperproteinemia (multiple myeloma, macroglobulinemia)
Dilutional Hyperglycemia*
Hypovolemic hyponatremia: decreased total body water and sodium, with a relatively greater decrease in sodium
Body fluid losses: sweating, vomiting, diarrhea, gastrointestinal suction
Third spacing: bowel obstruction, burns, pancreatitis, rhabdomyolysis
Renal causes: diuretics, mineralocorticoid deficiency, osmotic diuresis, renal tubular acidosis, salt-wasting nephropathies
Hypervolemic hyponatremia: increased total body sodium with a relatively greater increase in total body water
Heart failureChronic renal failureHepatic failure or cirrhosis
Euvolemic hyponatremia: increased total body water with nearly normal total body sodium
SIADHDrugs causing SIADH (diuretics, barbiturates, carbamazepine, chlorpropamide, clofibrate, opioids, tolbutamide, vincristine)
Psychogenic polydipsiaBeer potomaniaHypothyroidismAdrenal insufficiencyMDMA (ecstasy)Accidental or intentional water intoxication
Causes of Hyponatremia
*Hyperglycemia is referred by some as pseudohyponatremia, but hyperglycemia is actually a dilutional hyponatremia.SIADH, syndrome of inappropriate secretion of antidiuretic hormone.

Chapter 125 / Electrolyte Disorders 1643
SIADH, the most common of which are thiazide diuretics, narcot-ics, lithium, oral hypoglycemics, barbiturates, and antineoplastics. The mainstay of treatment of most patients with SIADH and other causes of euvolemic hyponatremia is free water restriction.
Diagnostic Strategies
A spot urinary sodium or urinary chloride level is useful to deter-mine if hyponatremia of undetermined origin is renal in etiology. Patients with hypovolemic hyponatremia due to nonrenal causes typically have a low urinary sodium or chloride level (<20 mEq/L) as they try to retain solute. Patients with hypovolemic hyponatre-mia due to renal causes will have elevated urine sodium and chlo-ride levels above 20 mEq/L as their kidneys cannot retain sodium or chloride. Patients with euvolemic hyponatremia typically have a urinary sodium concentration greater than 20 mEq/L secondary to volume expansion caused by water retention. Patients with hypervolemic hyponatremia secondary to CHF or cirrhosis have urine sodium levels of less than 20 mEq/L because of renal hypo-perfusion, whereas those with renal causes of hypervolemic hypo-natremia or with SIADH have sodium levels in excess of 20 mEq/L as their kidneys are not able to retain sodium. In interpreting serum sodium levels, consider the possibility of sampling error if the reported value does not seem consistent with the patient’s presentation and confirm that a diuretic such as furosemide has not been recently administered, which will increase urinary sodium losses. It is also important to consider adrenal insuffi-ciency when a dehydrated patient has both hyponatremia and hyperkalemia.
Clinical Features
The signs and symptoms of hyponatremia increase as sodium levels decline and also correlate with the rapidity with which hyponatremia develops. Nonspecific signs of hyponatremia include anorexia, nausea, vomiting, and generalized weakness. Acutely hyponatremic patients whose sodium level drops below 120 mEq/L during 24 to 48 hours may present with severe neuro-logic findings, including confusion, seizures, cerebral edema, coma, and brainstem herniation. Determination of the hydration status of the patient may help establish the etiology of the hypo-natremia and help direct subsequent treatment. The diagnosis of hypovolemic hyponatremia is more likely in the patient with diminished skin turgor, increased capillary refill, dry mucous membranes, and orthostasis. On the contrary, the patient with jugular venous distention, peripheral edema, or pulmonary
different formulas based on the degree of a patient’s hyperglyce-mia are currently used to correct serum sodium levels. One com-monly used formula advocates the addition of 1.6 mEq/L to the measured sodium for every 100 mg/dL of glucose above 100. Another formula recommends use of 2.4 mEq as the correction factor because glucose values above 400 mg/dL may lower sodium values by 4 mEq/L per each 100 mg/dL of glucose rise.40
Hypovolemic Hyponatremia
Hypovolemic hyponatremia, or hyponatremia in association with dehydration, occurs when there is decreased extracellular volume combined with an even greater loss of sodium. Hyponatremia secondary to body fluid losses must be differentiated from that due to renal losses. Hyponatremia with dehydration due to body fluid losses includes sweating, vomiting, diarrhea, and gastrointes-tinal suction. Hypovolemic hyponatremia is also seen with “third spacing” in bowel obstruction, burns, and intra-abdominal sepsis. Hypovolemic hyponatremia due to renal causes includes diuretic use, mineralocorticoid deficiency, renal tubular acidosis, and salt-wasting nephropathy. Hypovolemic hyponatremia can be further exacerbated when fluid losses are replaced with hypotonic saline.
Hypervolemic Hyponatremia
Hypervolemic hyponatremia, or hyponatremia with increased extracellular volume, occurs when sodium and water are retained but water retention exceeds sodium retention. Most of these patients present with edema. Hyponatremia with increased total body sodium occurs in patients with heart failure, chronic renal failure, and hepatic failure. The fluid retention in these states is secondary to renal hypoperfusion, resulting in increased aldoste-rone secretion and a decrease in free water excretion.
Euvolemic Hyponatremia
The final category of hyponatremia is one in which patients are euvolemic but have increased total body water. Causes of this type of hyponatremia include SIADH, psychogenic polydipsia,43 beer potomania, hypothyroidism, diuretic use in patients with mild CHF, and accidental or intentional water intoxication. These patients do not present with edema because most of the increased body water is intracellular and not intravascular. Hyponatremia without edema has also been described in patients after the use of the recreational drug N-methyl-3,4-methylenedioxyamphetamine (MDMA or ecstasy). MDMA-induced hyponatremia is multifac-torial and is related to increased free water intake to avoid dehy-dration and rhabdomyolysis, along with the tendency to be very active while using the drug, leading to sweating and antidiuretic hormone secretion.41 In addition, there are extensive case reports of significant hyponatremia in endurance athletes.44
SIADH is an important cause of hyponatremia that occurs when normal antidiuretic hormone secretion is lost and antidi-uretic hormone is secreted independently of the body’s need to conserve water. The process results from excess antidiuretic hormone production that causes total body water to increase, diluting the body’s sodium and causing the serum sodium to decrease. Patients with SIADH have inappropriately concentrated urine despite a low serum osmolality and normal circulating blood volume. Patients with SIADH have excess total body water but no signs of edema, ascites, or heart failure because most of the increased body water is intracellular, not intravascular. The three most common causes of SIADH are pulmonary lung masses and infections, CNS disorders, and drugs (Box 125-6). Lung cancers (especially small cell cancer), pneumonia, and tuberculosis can lead to SIADH. CNS infections, masses, and psychosis can also cause SIADH. A large number of medications are associated with
BOX 125-6
Lung massesCancer (especially small cell)PneumoniaTuberculosisAbscess
Central nervous system disordersInfection (meningitis, brain abscess)Mass (subdural, postoperative, cerebrovascular accident)Psychosis (with psychogenic polydipsia)
DrugsThiazide diureticsNarcoticsOral hypoglycemic agentsBarbituratesAntineoplastics
Three Most Common Causes of SIADH
SIADH, syndrome of inappropriate secretion of antidiuretic hormone.

1644 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
during 10 minutes. If a second bolus is required, an additional 100 mL of the 3% solution (513 mEq/L of sodium) may be administered during the next 50 minutes. Increased neurologic stability is highly likely once a symptomatic hyponatremic patient’s serum sodium concentration has been raised by about 4 to 6 mEq acutely by the hypertonic saline. To minimize the likelihood of central pontine myelinolysis, it is essential that symptomatic patients with severe hyponatremia not have serum sodium levels rise by any more than a total of 10 to 12 mEq within the first 24 hours.46,47 Potassium deficits should be replaced aggressively in the treatment of hyponatremic patients with a sodium disorder. If patients are retaining volume and diuresis is not adequate, furo-semide can be used; D5W is infused if the sodium level is rising too quickly.46 Patients may be able to make full neurologic recover-ies from central pontine myelinolysis with the reinduction of hyponatremia in these extreme cases.44 Demeclocycline in a dosage of 600 to 1200 mg daily is effective in patients with refractory hyponatremia.48
Hypovolemic Hyponatremia
Treatment of hypovolemic hyponatremia begins with rehydration. Hypotensive, dehydrated patients are volume resuscitated with normal saline. Once the patient is hemodynamically stable, the infusion rate is slowed. Typically, the normal saline is started at 500 to 1000 mL/hr until the blood pressure is stable and then slowed to 200 mL/hr with frequent sodium checks. If the sodium value is below 120 mEq/L, the sodium concentration should be allowed to rise only by an average of 0.5 mEq/hr or 10 to 12 mEq/day.47 It is essential to treat the underlying cause of hyponatremia.
Hypervolemic Hyponatremia
Normal saline and hypertonic saline can cause pulmonary edema in the hypervolemic hyponatremic patient. Restriction of fluid and sodium is the preferred treatment of patients with hypervol-emic hyponatremia, although loop diuretics can be used in severe cases. Hemodialysis is an alternative in patients with renal impair-ment and will be required in significantly hyponatremic renal failure patients with volume overload. Patients with CHF will usually benefit from diuretics that will increase water excretion and cause vasodilation to improve cardiac output.49 In those patients with liver failure, albumin is a consideration, along with diuretics and possibly paracentesis to improve the underlying pathologic process. Water restriction may make the largest impact on the long-term care of these patients.
Euvolemic Hyponatremia
The mainstay of treatment of euvolemic hyponatremia is free water restriction. As the hypo-osmolality in SIADH results from a relative abundance of water in the intracellular and extracellular volumes, maintained by a reduced ability to excrete water, the restriction of free oral water intake is the first recommendation. The use of water restriction is insufficient to treat acute severe hyponatremia and is not recommended as a sole intervention in severely symptomatic hyponatremia, in which a more rapid cor-rection rate is necessary. The only definitive treatment of SIADH is elimination of its underlying cause. Most cases of SIADH caused by malignant disease resolve with effective antineoplastic therapy, and most due to medication resolve promptly when the offending agent is discontinued.50
In patients with SIADH, normal saline may cause the serum sodium concentration to decrease even more as free water is retained and hypertonic urine is excreted. If a patient is symptom-atic because of a rapid decrease in serum sodium concentration,
congestion is much more likely to have hypervolemic hyponatre-mia. Patients with SIADH will have no edema and have normal skin turgor.
Management
Treatment of hyponatremia is guided by the patient’s clinical pre-sentation, severity of symptoms, estimated duration of illness, fluid status, and underlying cause of the sodium disturbance. Typically, sodium should be corrected during a time course of 48 to 72 hours. Central pontine myelinolysis can occur with too rapid correction of sodium.43 Most cases of central pontine myelinolysis occur in the alcoholic, malnourished, and elder population, although this devastating side effect can occur in healthy, young patients as well. Patients with central pontine myelinolysis have a flaccid paralysis, dysarthria, dysphagia, and hypotension. If a patient have these symptoms during therapy, stop all sodium-containing fluids and administer D5W immediately to lower sodium values temporarily.44 Most patients presenting to the ED with hyponatremia are stable and require no emergent therapy. However, patients who have serum sodium levels of significantly less than 120 mEq/L and those who have acute alterations in mental status, seizures, or new focal findings due to hyponatremia need immediate intervention. Table 125-3 presents the sodium concentration of various infusates, and the following equation is helpful to estimate the effect of 1 liter of any infusate on serum sodium:
Change in serum Na infusate Naserum Na total body wate
+ +
+=
− / rr +1
There is no consensus regarding the optimal treatment of symptomatic hyponatremia. However, there is agreement that cor-rection should occur at a sufficient pace and magnitude to reverse the manifestations of hypotonicity but not be so rapid and large as to pose a risk for development of osmotic demyelination. For relatively asymptomatic patients with sodium values of 115 to 135 mEq/ L, free water restriction is typically the single most important treatment.
In more severe cases when the sodium value is 120 mEq/L or less and the patient has alterations in mental status, has focal find-ings, or is seizing, hypertonic saline is indicated.45-47 Correction of hyponatremia by 4 to 6 mEq/L within 6 hours, with bolus infu-sions of 3% saline if necessary, is sufficient to manage the most severe manifestations of hyponatremia.45
The serum sodium level should be below 120 mEq/L when administration of hypertonic saline is being considered. It is rec-ommended that critically ill hyponatremic patients with seizures, focal findings, or coma receive 100 mL of 3% hypertonic saline
INFUSATEINFUSATE
SODIUM (mmol/L)EXTRACELLULAR FLUID
DISTRIBUTION (%)
3% Hypertonic saline 513 100
0.9% Normal saline solution
154 100
Lactated Ringer’s solution
130 97
Half-normal saline solution
77 73
0.2% Sodium chloride + 5% dextrose in water
34 55
5% Dextrose in water 0 45
Table 125-3 Characteristics of Infusates

Chapter 125 / Electrolyte Disorders 1645
include lethargy, altered mental status, seizures, and coma. Death due to hypercalcemia is usually related to complications caused by coma, dehydration, or electrolyte disturbances. Cardiac conduc-tion abnormalities may occur; bradydysrhythmias are the most common.53 Severe hypercalcemia has also been associated with sinus arrest, atrioventricular block, atrial fibrillation, and ven-tricular tachycardia.
Diagnostic Strategies
The diagnostic evaluation of a patient with suspected hypercalce-mia begins with obtaining of electrolyte and renal function tests and an ECG. Calcium is measured by determination of either a total serum calcium level or an ionized calcium level. Ionized calcium is the active form of the total calcium level. It is more accurate in the diagnosis and treatment of hypocalcemia, but it does need to be routinely evaluated in hypercalcemia.54 The serum total calcium level represents both bound and unbound calcium and thus should be corrected on the basis of the albumin concen-tration. The adjustment to serum albumin is accomplished by adding or subtracting 0.08 mg/dL to the measured total serum calcium for every 1.0 g/L of albumin below or above 4 g/L albumin, respectively.
A short QT interval can be seen in hypercalcemia and is con-sidered a classic finding. However, although the incidence and duration of QT shortening appear to be correlated with the degree of hypercalcemia, it is not a reliable finding and is not routinely seen in most patients (Fig. 125-6). ST segment elevation may be the least well documented but most consistent electrocardio-graphic finding, and hypercalcemia should be considered in the differential diagnosis of ST segment elevation caused by condi-tions other than myocardial infarction.55,56 In severe cases of hypercalcemia, sinus bradycardia, bundle branch block, and high-degree atrioventricular block may also been seen.
Management
Patients in hypercalcemic crisis are usually dehydrated, often obtunded, and also predisposed to arrhythmias as a result of con-comitant electrolyte disturbances; thus they require intravenous access with a normal saline infusion and close monitoring. Normal saline will inhibit proximal tubule reabsorption of calcium and also correct the patient’s volume depletion. Normal saline is infused “wide open” until blood pressure and perfusion are nor-malized. After the initial bolus, the saline infusion is adjusted to a rate of approximately 200 to 300 mL/hr, depending on the patient’s age and renal function. Patients with underlying cardiac or renal disease may require lower infusion rates that are carefully titrated. Although the administration of higher volumes of saline may further augment calcium excretion, it is much more likely to result in increased morbidity and mortality from volume overload, pul-monary edema, and myocardial ischemia. The routine use of furo-semide in the management of hypercalcemia is no longer recommended. Furosemide was once thought to block the distal reabsorption of calcium, thus complementing saline’s proximal tubule effects. However, no modern-day studies have shown furo-semide to have significant calcium reabsorption blocking effects. The use of furosemide is reserved to augment saline diuresis and to avoid volume overload during the treatment of hypercalce-mia.57 If it is given to patients who are not yet volume replete, this loop diuretic may worsen the hypercalcemia because of its volume depleting effects and also adversely affect the patient’s hemody-namics and renal status. Once calcium excretion by saline infusion has begun, other electrolyte values should be carefully monitored with attention to serum potassium levels.
Osteoclast-inhibiting therapies for severe hypercalcemia are generally considered in consultation with the patient’s primary
treatment with hypertonic saline is recommended. Demeclocy-cline and lithium are rarely used in the treatment of SIADH because of their many side effects and nephrotoxicity. Rapid cor-rection of hyponatremia may occur during hemodialysis. To mini-mize the risks of central pontine myelinolysis, hemodialysis is reserved for patients with documented renal failure and used in a very careful manner.50 Vaptans, which are oral agents that inhibit the effects of vasopressin, have been studied for treatment of patients with hyponatremia due to SIADH but need further evalu-ation before becoming standard of care.46,51
HYPERCALCEMIA
Principles of Disease
Hypercalcemia is usually defined as a serum calcium level above 10.5 mg/dL; normal levels are usually defined as between 9 and 10.5 mg/dL. Hypercalcemia is considered mild if the total serum calcium level is between 10.5 and 12 mg/dL; levels higher than 14 mg/dL can be life-threatening.
There are five major causes of hypercalcemia (Box 125-7). Primary hyperparathyroidism is the most common cause of hypercalcemia in outpatients, whereas malignant disease is the most common cause in hospitalized patients. Mild hypercalcemia, in an otherwise normal person, may be due to thiazide diuretics with minimal dehydration. Other less common causes of elevated calcium concentration are usually not considered until malignant disease and parathyroid disease are ruled out. Malignancy-associated hypercalcemia occurs in up to 10% of all patients with advanced cancer and generally conveys a poor prognosis. Other causes of hypercalcemia include granulomatous disease, such as sarcoidosis and tuberculosis; medications and pharmacologic agents; and a number of diverse conditions, such as rhabdomyoly-sis and prolonged immobilization.
Clinical Features
Unfortunately, the clinical presentation of hypercalcemia is often vague and nonspecific. Symptoms include nonfocal abdominal pain, constipation, fatigue, diffuse body aches, anorexia, nausea, and vomiting. Symptom severity depends on the degree of hyper-calcemia, the rapidity of onset, and the patient’s baseline neuro-logic and renal function.52 The diagnosis should be considered in a large number of differential diagnoses. In addition, some patients complain of polyuria or polydipsia. Neuropsychiatric disturbances include anxiety, depression, confusion, and hallucinations. The CNS manifestations that often predominate in more severe cases
BOX 125-7
Malignant disease Ectopic secretions of parathyroid hormone, multiple myeloma, cancer metastatic to bone
Most common: breast, lung, hematologic, kidney, prostate
Endocrine Hyperparathyroidism, multiple endocrine neoplasias, hyperthyroidism, pheochromocytoma, adrenal insufficiency
Granulomatous disease
Sarcoidosis, tuberculosis, histoplasmosis, berylliosis, coccidioidomycosis
Pharmacologic agents Vitamins A and D, thiazide diuretics, estrogens, milk-alkali syndrome
Miscellaneous Dehydration, prolonged immobilization, iatrogenic, rhabdomyolysis, familial, laboratory error
Five Most Common Causes of Hypercalcemia

1646 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
BOX 125-8
HypoalbuminemiaHypoparathyroidism: inherited, postsurgical, autoimmune,
infiltrativeVitamin D deficiency and vitamin D resistance: malabsorption
syndrome, liver disease, malnutrition, sepsis, anticonvulsants, lack of sunlight exposure
Chronic renal failureHyperphosphatemiaHypomagnesemiaRespiratory alkalosisSevere pancreatitisDrugs: bisphosphonates, phenytoin, phosphate, calcitoninTumor lysis syndromeRhabdomyolysis
Most Common Causes of Hypocalcemia
Figure 125-6. Short QT interval (arrow) in a patient with multiple myeloma and a calcium level of 14.2 mg/dL. (Courtesy Dr. Barton Campbell.)
I aVR V1 V4
II aVL V2 V5
III
II
aVF V3 V6
physician or oncologist. Drugs that inhibit osteoclast-mediated bone resorption include the bisphosphonates, mithramycin, calci-tonin, and glucocorticoids. Intravenous bisphosphonates are the most extensively studied and most efficacious agents for the treatment of malignancy-associated hypercalcemia.58 Their calcium-lowering effect is achieved predominantly by inhibition of osteoclast function and survival. Zoledronic acid is the bisphos-phonate of choice in hypercalcemia of malignancy.59 The infusion takes 15 minutes, and zoledronic acid may be more effective than other bisphosphonates at keeping the calcium level down over time. The use of intravenous bisphosphonates is restricted to the treatment of acute hypercalcemia associated with serum calcium concentrations above 15 mg/dL and rapid deterioration of CNS, cardiac, gastrointestinal, and renal function.
In the rare case in which a patient has a life-threatening hyper-calcemic arrhythmia or heart block, phosphates and hemodialysis are considered.60,61 In cases of hypercalcemic crisis resulting from primary hyperparathyroidism, urgent parathyroidectomy is potentially curative.
HYPOCALCEMIA
Principles of Disease
Calcium regulation is critical for normal cell function, neural transmission, membrane stability, bone structure, blood coagula-tion, and intracellular signaling. Total body calcium is controlled by a feedback system in which parathyroid hormone induces the bone and the kidneys to increase serum calcium levels. Vitamin D facilitates intestinal calcium absorption. Conversely, elevated calcium levels normally inhibit parathyroid hormone release.
There are multiple causes of hypocalcemia, of which hypoalbu-minemia is the most common (Box 125-8). Because calcium is bound to albumin and other serum proteins, hypoalbuminemia will cause a fall in the measured serum calcium by about 0.8 mg/dL for every 1 g/dL reduction in serum albumin. The active form of calcium is the ionized calcium, which is not affected by changes in albumin.
Hypoparathyroidism is a common cause of hypocalcemia and often develops because of surgery for head and neck cancers. It develops in 1 to 2% of patients after total thyroidectomy. Patients with vitamin D deficiency, including those with malabsorption syndromes, liver disease, malnutrition, and very little sunlight
exposure, are at high risk for development of hypocalcemia.62 Derangements in magnesium and phosphate can also lead to hypocalcemia. Hyperphosphatemic patients often have hypocal-cemia because of phosphate’s affinity to bind calcium, whereas hypomagnesemia causes end-organ resistance to parathyroid hormone and inhibits the hypocalcemic feedback loop. Patients with sepsis demonstrate hypocalcemia usually associated with hypoalbuminemia.
The most common causes of symptomatic hypocalcemia are massive blood transfusions, toxins, pancreatitis, tumor lysis syn-drome, and chronic malnutrition (Box 125-9). Patients receiving massive blood transfusions are at risk for development of hypo-calcemia because of citrate toxicity. Rapid blood transfusions and radiocontrast dyes containing citrate should be monitored closely in patients with hepatic failure, CHF, or other low-output states to avoid hypocalcemia.63
Hypocalcemia in acute pancreatitis is caused primarily by pre-cipitation of calcium soaps in the abdominal cavity, but glucagon-stimulated calcitonin release and decreased parathyroid hormone secretion may play a role. Toxic exposures to hydrofluoric acid and ethylene glycol can cause profound hypocalcemia secondary to their abilities to complex and chelate with calcium.
When patients are being treated for malignant neoplasms, they are at risk for development of tumor lysis syndrome and multiple

Chapter 125 / Electrolyte Disorders 1647
hypocalcemic patients who require calcium urgently. It is best given through a central line. Calcium gluconate contains 92 mg of elemental calcium. Although this is one-third the amount con-tained in calcium chloride, it is safer to administer and can be given peripherally.62 Most patients requiring intravenous calcium should be admitted to the hospital for monitoring and treatment of nausea, vomiting, hypertension, and bradycardia. Patients taking digoxin have increased cardiac sensitivity to fluctuations in serum calcium, so intravenous calcium administration is accom-panied by continuous electrocardiographic monitoring.65
HYPERMAGNESEMIA
Principles of Disease
Hypermagnesemia is a relatively rare electrolyte abnormality defined as a serum magnesium concentration above 2.2 mg/dL. Hypermagnesemia is most often seen in patients with renal insufficiency who cannot optimally regulate magnesium excre-tion, especially as their magnesium load increases. There have been reports of fatal and near-fatal cases involving hypermagne-semia in patients receiving magnesium with unrecognized renal failure.66 Hypermagnesemia can also be caused iatrogenically in patients receiving intravenous magnesium for medical treatment or in patients taking over-the-counter laxatives and antacids.67 Even though most patients at risk for hypermagnesemia have underlying renal impairment, hypermagnesemia has been reported in patients with normal renal function, especially in elders. Box 125-10 lists the most common causes of increased serum magne-sium levels.
Iatrogenic hypermagnesemia most commonly occurs from excessive intravenous infusions of magnesium in patients being treated for preeclampsia or eclampsia, cardiac arrhythmias, or asthma exacerbations. Magnesium administration during eclamp-sia can also cause fetal hypermagnesemia as magnesium crosses the placental barrier. Hypermagnesemia may also be seen in patients with chronic renal failure on hemodialysis if the dialysate solutions are not closely monitored for magnesium content.
In patients with normal renal function, large amounts of mag-nesium can be excreted daily in the stool and urine. However, in patients with impaired renal function, hypermagnesemia can be seen even with therapeutic doses of magnesium-containing prod-ucts. For example, a patient with renal insufficiency should not use magnesium citrate for treatment of constipation. An adult dose of 10 ounces of laxative syrup results in consumption of approximately 2.0 g of elemental magnesium per single dose. A healthy adult can excrete more than 6.0 g of magnesium daily, but renally impaired patients may not be able to tolerate a single dose of laxative syrup. Hypermagnesemia resulting from Epsom salt gargles and salt enemas has been reported.68,69
secondary electrolyte abnormalities. Hypocalcemia has been attributed to the precipitation of calcium phosphate salts. Finally, one should expect to encounter hypocalcemia in malnourished patients and chronic alcoholics who present to the ED, especially alcoholics with hyperventilation due to alcohol withdrawal.
Clinical Features
Although there are many clinical manifestations of hypocalcemia, neuromuscular and cardiovascular findings predominate. Severe, symptomatic hypocalcemia may result in cardiovascular collapse, hypotension, and dysrhythmias. Clinically evident hypocalcemia generally is manifested in milder forms and is usually the result of a chronic disease state. The patient may complain of muscle cramping, perioral or finger paresthesias, shortness of breath sec-ondary to bronchospasm, and tetanic contractions. More severe symptoms include hypotension, QT prolongation, angina, and CHF. Chronic hypocalcemia may be manifested with cataracts, poor dentition, dry skin, coarse hair, and pruritus. Chvostek’s sign may be present: when the examiner taps the facial nerve, facial or eye muscle twitching will be elicited. Trousseau’s sign may also be present: when the examiner inflates the blood pressure cuff to 20 mm Hg above the systolic blood pressure for 3 minutes, carpal spasms will be induced because of local ulnar and median nerve ischemia. Trousseau’s sign is relatively specific for hypocalcemia, whereas Chvostek’s test is less diagnostic.
Diagnostic Strategies
Most cases of hypocalcemia are discovered by clinical suspicion followed by appropriate laboratory testing. A serum calcium level less than 8.5 mg/dL or an ionized calcium level less than 2.0 mEq/L is considered diagnostic. Total serum calcium is approximately 50% free (ionized) and 50% bound, primarily to albumin; thus the serum level must be “corrected” when hypoalbuminemia exists. The ionized calcium level, which is not affected by the albumin level, is more accurate. It is best to perform the whole blood ionized calcium determination rapidly to avoid changes in chelation and pH.64 In select cases, a parathyroid hormone level may be sent to assist the admitting or consulting physician. Elec-trocardiography and cardiac monitoring are recommended in suspected hypocalcemia patients to evaluate the QT interval and to provide continuous monitoring for potential dysrhythmias.
Management
Most asymptomatic patients and those with mild symptoms can be treated with oral calcium supplementation, such as calcium carbonate. Intravenous calcium is administered, either as calcium chloride or calcium gluconate, to patients with moderate to severe symptoms; 100 to 300 mg of elemental calcium given during 5 to 30 minutes will raise the ionized calcium level 0.5 to 1.5 mEq. Calcium chloride contains 272 mg of elemental calcium but can be caustic to veins and thus should be given only to critically ill
BOX 125-9
Hyperventilation Anxiety, sympathomimeticsEthanol abuse, chronic malnutrition
Hypoalbuminemia
Massive blood transfusion More than 10 unitsToxins Hydrofluoric acid, ethylene glycolSevere pancreatitis
Five Most Common Symptomatic Causes of Hypocalcemia Seen in the Emergency Department
BOX 125-10
Iatrogenic Intravenous administration, dialysateOral administration Laxatives, antacids, vitamins, cathartics,
dialysate, parentalImpaired elimination: hypomotility
Bowel obstruction, chronic constipation
Impaired elimination: medications
Anticholinergics, narcotics, lithium therapy
Miscellaneous Hypothyroidism, tumor lysis syndrome, adrenal insufficiency, milk-alkali syndrome, near-drowning in Dead Sea94
Five Most Common Causes of Hypermagnesemia

1648 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
with respiratory depression and cardiac instability. In treating life-threatening hypermagnesemia, initially administer 100 to 200 mg of intravenous calcium as either calcium chloride or calcium glu-conate (1-2 mL of 10% calcium chloride or 5 mL of 1% calcium gluconate during 2-5 minutes) and then titrate to effect.72 One can then consider a continuous infusion at 2 to 4 mg/kg/hr if it is needed while dialysis is being arranged.
HYPOMAGNESEMIA
Principles of Disease
Hypomagnesemia is a common electrolyte abnormality that often goes undetected. Normal serum magnesium levels range from 1.5 to 3.0 mEq/L. Symptoms of hypomagnesemia typically begin to be manifested at serum levels below 1.2 mEq/L, although symptoms are often not well correlated with the patient’s serum level. This is because most of the body’s magnesium is intracel-lular, and thus a single blood sample with a low serum magnesium level may not accurately reflect total body magnesium or the extent of true hypomagnesemia. Magnesium exists in three states: ionized magnesium, protein bound, and complexed to serum anions. Even though studies show the importance of measuring ionized calcium, most research shows that ionized magnesium can be inferred from total magnesium. Currently, the clinical role of measurement of ionized magnesium is unclear, and measurement of ionized magnesium is not standard practice in the ED; there may be a role for measurement of ionized magnesium in the intensive care setting.73
There are many causes of hypomagnesemia (Box 125-11). The following are the five most common ED presentations of hypomagnesemia.
Patients Maintained with Diuretics. Patients using either loop or thiazide diuretics are at increased risk for hypomagnesemia. Both types of diuretics can inhibit magnesium reabsorption. Con-versely, potassium-sparing diuretics are also magnesium sparing because they enhance magnesium reabsorption and decrease mag-nesium excretion. The degree of hypomagnesemia induced by the loop and thiazide diuretics is generally mild, partly because the associated volume contraction will tend to increase proximal sodium, water, and magnesium reabsorption.
Malnourished and Alcoholic Patients. Healthy patients consume enough magnesium in green vegetables, legumes, fruits, shellfish, fresh meat, and cocoa on a regular basis to maintain normal total body magnesium stores. However, hypomagnesemia is common in patients with chronic protein-calorie malnutrition because of an associated lack of essential minerals and vitamins including magnesium. This is especially true in chronic alcoholics, who may not eat foods rich in magnesium.74 Magnesium losses are further increased in chronic alcoholics because of alcohol’s diuretic effects. Hypomagnesemia may also be seen in patients with malabsorp-tion disorders (celiac sprue and short bowel syndrome) and in patients with increased magnesium excretion (chronic diarrhea or inflammatory bowel conditions).
Patients with Hypokalemia. Both potassium and magnesium are critical to help stabilize the membrane potential, to decrease cell
Decreased gastrointestinal elimination and increased gastroin-testinal absorption of magnesium due to intestinal hypomotility can also result in toxicity. Hypermagnesemia can be seen with bowel obstruction, colitis, gastric dilation, and use of medications that decrease motility, including narcotics and anticholinergics. Other less common causes of hypermagnesemia include rhabdo-myolysis, tumor lysis syndrome, adrenal insufficiency, hyperpara-thyroidism, and hypothyroidism.
Clinical Features
Patients with hypermagnesemia may present with flushing, nausea, vomiting, headache, and diminished deep tendon reflexes. Typi-cally, symptoms begin to be manifested around magnesium levels of 4 mg/dL (Table 125-4). Magnesium is a CNS and neuromus-cular depressant and can cause cardiac instability. Magnesium acts as a calcium channel blocker and also blocks potassium channels needed for repolarization. As magnesium levels rise, hypotension and electrocardiographic changes, including QRS widening and QT and PR prolongation, begin to occur. When serum magnesium levels rise above 7 mg/dL, patients can have signs and symptoms of hypotension, respiratory insufficiency, and heart block. Cardiac arrest and death have been reported in patients with serum mag-nesium levels above 10 mg/dL.70 Finally, hypermagnesemia causes suppression of parathyroid hormone secretion and can be associated with hypocalcemia.
Diagnostic Strategies
Measured plasma magnesium levels often do not reflect total magnesium content, making it difficult to consistently correlate symptoms to specific magnesium levels. Although there is some question of the role of measuring ionized magnesium in patients with hypomagnesemia, only total body magnesium needs to be followed in hypermagnesemic patients.71
Management
Management of hypermagnesemia is dictated by the neuromus-cular, cardiovascular, and CNS changes that occur. Most stable or asymptomatic hypermagnesemic patients can be treated with cessation of their magnesium therapy. As symptoms become more pronounced, intravenous isotonic fluids are administered to dilute the extracellular magnesium. Diuretics can be used to promote excretion of magnesium while more definitive treatment is arranged.
In patients with higher levels of serum magnesium or more severe symptoms, renal consultation should be initiated immedi-ately to arrange for dialysis. Intravenous calcium therapy to reverse magnesium toxicity should be reserved for patients with life-threatening symptoms while dialysis is being arranged. Calcium directly antagonizes the neuromuscular and cardiovascular effects of magnesium and is recommended in hypotensive patients
BOX 125-11
DietaryGastrointestinalRenalEndocrine or metabolicDrug induced
Most Common Causes of HypomagnesemiaEFFECT LEVEL (mg/dL)
Decreased deep tendon reflexes 4-5
Hypotension 5-7
Respiratory insufficiency 10
Heart block 10-15
Cardiac arrest 10-24
Table 125-4 Clinical Effects of Hypermagnesemia

Chapter 125 / Electrolyte Disorders 1649
with the total serum magnesium level. Because most of the total body magnesium is intracellular, the magnesium level alone does not guide therapy. However, the possibility of hypomagnesemia is considered in patients with malnourishment, significant or refrac-tory hypokalemia, and ventricular arrhythmias. Electrocardio-graphic findings in hypomagnesemia are nonspecific and may be caused by both the hypomagnesemia and concomitant hypokale-mia. Hypomagnesemia should be suspected whenever electrocar-diographic findings of hypokalemia are noted, including PR and QT interval prolongation, ST segment depression, flattening and widening of the T waves, loss of voltage, and U waves.
Management
The route of magnesium repletion varies with the severity of the clinical manifestations. Parenteral magnesium is recommended for life-threatening conditions. In patients with normal renal function, 1 to 2 g of magnesium sulfate is an appropriate loading dose. A stable patient with hypomagnesemia can be treated with a loading dose of 1 to 2 g of magnesium sulfate during 10 to 60 minutes, followed by a standard maintenance dose of 0.5 to 1 g/hr until symptoms have resolved or a therapeutic effect is obtained. However, patients in cardiac arrest should receive a bolus of 1 to 2 g magnesium sulfate by intravenous push.
Magnesium administration is strongly encouraged for patients receiving intravenous potassium repletion. A dose of 0.5 g/hr is safe in patients who are well hydrated and have normal renal func-tion. There are potential adverse effects to rapid aggressive mag-nesium replacement at more than 1 to 2 g/hr, including decreased deep tendon reflexes, respiratory depression, and heart block. Magnesium gluconate oral supplementation can be given if the patient is only mildly hypomagnesemic and asymptomatic. When preparing any patient for discharge, physicians can encourage life-style changes, including adequate magnesium intake that may benefit blood pressure control, promote weight loss, and improve chronic disease risk.
HYPERPHOSPHATEMIA
Principles of Disease
Hyperphosphatemia is defined as a serum level above 2.5 mg/dL, but it is usually clinically significant only when levels are greater than 5 mg/dL. Although it is rare in the general population, hyper-phosphatemia is extremely common in patients with renal insuf-ficiency or renal failure.80 Almost all patients with renal failure experience hyperphosphatemia at some time during the course of their disease. Hyperphosphatemia can occur because of four major pathways: decreased phosphate excretion, excessive phos-phate intake, increased renal tubular reabsorption, and shift of phosphate from intracellular to extracellular space. In addition, physicians must be aware of spurious elevations in phosphate (Box 125-12).
Decreased excretion of phosphate combined with excessive intake is the most common mechanism for the development of hyperphosphatemia. Excessive phosphate intake alone is an uncommon cause of hyperphosphatemia in patients with normal renal function. When patients have glomerular filtration rates below 30 mL/min, the kidneys do not allow excretion of the full amount of ingested phosphate to maintain homeostasis. Exoge-nous phosphate, including intravenous or oral phosphate admin-istration and phosphate enemas and laxatives can cause a large burden on the kidneys if they do not have normal baseline function.19
Hypoparathyroidism, vitamin D intoxication, and thyrotoxico-sis increase renal phosphate reabsorption and may cause elevated
excitability, and for function of the Na+,K+-ATPase pump. Approx-imately 50% of patients with hypokalemia also have concomitant magnesium deficiency. Increasing degrees of hypokalemia are cor-related with an increasing likelihood of a magnesium deficit.21 Hypokalemic patients who are refractory to potassium replace-ment are likely to also be hypomagnesemic.
Patients with Acute Coronary Artery Disease and Ventricular Arrhythmias. There appears to be a relationship between low serum magnesium levels and the subsequent development of coronary heart disease.75 Patients who have a myocardial infarc-tion are more likely than controls to be hypomagnesemic. At present, magnesium supplementation is recommended only for those acute coronary syndrome patients who have evidence of hypokalemia, prolonged QT, or known hypomagnesemia. Simi-larly, patients with acute myocardial infarction who have mild hypomagnesemia appear to have a twofold to threefold increase in the frequency of ventricular arrhythmias in the first 24 hours compared with those with normal magnesium levels.76 There is controversy about whether magnesium should be administered empirically after acute myocardial infarction.77 Dysrhythmia is the most common cardiovascular manifestation of hypomagnesemia. Magnesium affects the duration of phase 2 of the action potential, and hypomagnesemia can prolong the QT interval. Magnesium also has effects on phase 4, the resting membrane potential, when it serves to keep the cell more negative by stimulating the sodium-potassium pump. The exact mechanism underlying a possible association between hypomagnesemia and arrhythmias is at present unknown. Arrhythmias are likely to be due to concurrent hypokalemia, hypomagnesemia, or both, resulting in a prolonged QT interval and increases in spontaneous depolarization.
Patients Receiving Specific Medications. In addition to diuretics, many medications are associated with hypomagnesemia. Many nephrotoxic drugs, including aminoglycosides, amphotericin B, cisplatin, and pentamidine, can produce magnesium wasting. The mechanism responsible for hypomagnesemia associated with long-term proton pump inhibitor use is unknown; however, long-term use of proton pump inhibitors may be associated with changes in intestinal absorption of magnesium.78 Severe hypo-magnesemia can also be seen in patients preparing for colonos-copy with polyethylene glycol–based bowel preparations.
Clinical Features
Determination of the clinical consequences of isolated hypomag-nesemia is often difficult because patients with hypomagnesemia typically have hypokalemia, hypocalcemia, and hyponatremia. However, many signs and symptoms are reported to correlate with hypomagnesemia, including muscle cramping, diffuse weakness, palpitations, vertigo, ataxia, depression, and seizures. The clinical manifestations most likely seen in the ED typically involve the neuromuscular and cardiovascular systems. Patients may present with hyperactive deep tendon reflexes, muscle cramps, Trousseau’s and Chvostek’s signs, and dysarthria and dysphagia from esopha-geal dysmotility. Cardiac conduction abnormalities secondary to magnesium depletion, and often coexisting hypokalemia, can result in PR as well as QT interval prolongation. Dysrhythmias including atrial fibrillation, multifocal atrial tachycardia, prema-ture ventricular complexes, ventricular tachycardia, torsades de pointes, and ventricular fibrillation are the most common cardio-vascular manifestations of hypomagnesemia. Women with ade-quate intakes of magnesium are less likely to be affected by preeclampsia than are those with an inadequate intake.79
Diagnostic Strategies
Symptoms of hypomagnesemia begin to be manifested at serum levels below 1.2 mEq/L, but symptoms do not always correlate

1650 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
HYPOPHOSPHATEMIA
Principles of Disease
Hypophosphatemia is defined as mild (2-2.5 mg/dL), moderate (1-2 mg/dL), or severe (<1 mg/dL). Mild to moderately severe hypophosphatemia is usually asymptomatic and like hypomagne-semia often goes unrecognized. Although most patients remain asymptomatic, severe hypophosphatemia may result in potentially life-threatening complications. Major clinical sequelae usually occur only in severe hypophosphatemia.
Symptoms of hypophosphatemia typically begin to be mani-fested at serum levels below 1.0 mg/dL. Acute hypophosphatemia is most commonly due to a rapid intracellular shift, but there are many other causes of clinical manifestations as well.86 Hyperven-tilation, glucose, insulin, volume, and resolving acidosis lead to hypophosphatemia by rapid intracellular shift. The many causes of hypophosphatemia include decreased phosphate intake or increased absorptive states, hyperventilatory states, hormonal and endocrine effects, medications, and disease states (Box 125-13). The ED patients most likely to have hypophosphatemia are those who are malnourished with alcohol withdrawal, acute hyperven-tilation, or sepsis and patients with DKA or alcohol ketoacidosis in whom reintroduction of insulin and glucose causes phosphate uptake into cells.87,88
Clinical Features
Mild to moderate hypophosphatemia is usually asymptomatic, but major clinical manifestations can occur with severe hypophos-phatemia. Hypophosphatemia can affect a variety of organ systems and cause a wide variety of symptoms because phosphate is an essential component to adenosine triphosphate (Box 125-14).
BOX 125-12
Decreased phosphate excretion
Acute and chronic renal failure
Increased renal tubular reabsorption
Hypoparathyroidism
ThyrotoxicosisExcess vitamin D administration
Excessive phosphate intake Phosphate enemas or laxativesIntravenous or oral phosphate administration
Shift of phosphate from intracellular to extracellular space
Diabetic ketoacidosis
Tumor lysisRhabdomyolysis
Spurious hyperphosphatemia ParaproteinemiaHyperbilirubinemiaHemolysisHyperlipidemia
Five Most Common Causes of Hyperphosphatemia
phosphate levels. Hyperphosphatemia may also occur when there is a large shift of phosphate from the intracellular to the extracel-lular space and the kidney’s ability to excrete phosphate is over-whelmed. This cause of hyperphosphatemia is seen in crush injuries and nontraumatic rhabdomyolysis, tumor lysis syndrome, and DKA.
Hyperphosphatemia can be a spurious finding in cases of hyperproteinemia, such as multiple myeloma, hyperlipidemia, hemolysis, or hyperbilirubinemia. Drawing of a blood sample from a line containing heparin is another cause of a falsely ele-vated phosphate level.81
Clinical Features
Patients with hyperphosphatemia may present with multiple com-plaints related to associated electrolyte abnormalities, particularly hypocalcemia. Hyperphosphatemia causes hypocalcemia by pre-cipitating calcium out of the blood and decreasing vitamin D production. It is this secondary hypocalcemia that can cause muscle cramping, tetany, and seizures. Chronic hyperphosphate-mia can also lead to metastatic calcifications in joints, tissues, and arteries.
Management
Dietary restriction alone may suffice for control of hyperphospha-temia in persons with mild renal insufficiency, but it is inadequate for control in those with overt renal failure. Because most patients presenting with severe hyperphosphatemia also have hypocalce-mia, treatment focuses on the correction of both electrolytes. In patients with normal renal function, phosphate excretion can be increased by saline infusion coupled with loop diuretics. Hyper-phosphatemia usually resolves in 6 to 12 hours in patients with normal renal function.82 In patients with hyperphosphatemia with renal failure, hemodialysis or peritoneal dialysis should be consid-ered early in the management. Currently, phosphate control is initiated only when hyperphosphatemia occurs, but a potentially beneficial and simple approach may be to intervene earlier in patients with chronic kidney disease.83 The optimal method for control of serum phosphate in patients undergoing dialysis is unknown and may involve combinations of dietary modification and enhancement of phosphate clearance through longer dialysis sessions.84,85
BOX 125-13
Decreased intake or increased absorptive states
Chronic alcoholismHome parenteral nutritionAIDSChemotherapyVomitingMalabsorption syndromesSecretory diarrheaVitamin D deficiency
Hyperventilatory states SepsisAlcohol withdrawalSalicylate poisoningNeuroleptic malignant syndromePanic attacksDiabetic ketoacidosisHepatic coma
Hormonal and endocrine effects
Insulin loadingGlucose loadingExogenous epinephrineHyperparathyroidism
Medications19,95 DiureticsChronic antacid ingestionSteroidsPhosphate bindersXanthine derivativesBeta2-agonists
Disease states TraumaSevere thermal burnsAcute renal failureGout
Five Most Common Causes of Hypophosphatemia in the Emergency Department

Chapter 125 / Electrolyte Disorders 1651
period.89 For routine replacement, give 0.5 mL/hr K2PO4; this may be increased to 1 mL/hr in severe symptomatic patients.87 Each milliliter of K2PO4 contains 3 mmol of phosphorus and 4.4 mEq of potassium. Typical replacement therapy provides approxi-mately 1 g of phosphorus per day. Monitoring of patients for the development of hypocalcemia, hyperkalemia, and hyperphospha-temia is required while intravenous phosphate is administered, especially in patients with renal insufficiency. Patients with DKA are initially hypophosphatemic. However, no studies have shown significant benefit to routine phosphate therapy in DKA.91 Risks of routine treatment with phosphate include hyperphosphatemia, renal failure, hypocalcemia, and hypomagnesemia. In patients with severe malnutrition or significant hypophosphatemia, replacement can be considered, but never administer more than 60 mmol/day without reason.
■ Asymptomatic electrolyte abnormalities can usually be corrected slowly, but those abnormalities that cause profound mental status changes or life-threatening arrhythmias require immediate correction to avoid cardiac arrest or seizures.
■ Intravenous calcium should be used only for hyperkalemic emergencies, defined as the following: widening QRS; sine wave; cardiac arrest believed to be due to hyperkalemia; or rapidly evolving electrocardiographic changes, from normal to development of tall peaked T waves and loss of the P wave. Acute, rapid rises in serum potassium concentration are rare but may be seen in tumor lysis syndrome, rhabdomyolysis, or massive hemolysis.
■ After the critical decision about administration of calcium has been made, a beta2-agonist, insulin and glucose, normal saline, and bicarbonate (if the patient is acidotic) can be given to shift potassium intracellularly.
■ In treatment of hypokalemia, it is critical that the physician also replace magnesium sulfate, in addition to potassium, or the patient will excrete most of the infused potassium in the urine.
■ Low serum potassium levels reflect a much greater total potassium deficit; correction of large deficits can require several days.
■ Hypertonic saline should be reserved for severely hyponatremic patients (typically in the 100-110 mEq range) who present with coma, seizures, or focal neurologic deficits. Central pontine myelinolysis can occur if serum sodium concentration is raised rapidly by more than 10 to 12 mEq/day.
KEY CONCEPTS
BOX 125-14
Central nervous system IrritabilityConfusionParesthesiasDepressionDysarthriaSeizureComa
Cardiovascular CardiomyopathyDepressed myocardial contractilityArrhythmias
Respiratory Acute respiratory failureDepressed myocardial contractility
Gastrointestinal Ileus, dysphagiaHematologic Depressed levels of
2,3-diphosphoglycerate and adenosine triphosphate
Leukocyte dysfunctionHemolysisPlatelet dysfunction
Renal Acute tubular necrosisMetabolic acidosisHypercalcemia
Endocrine Insulin resistanceHyperparathyroidism
Clinical Manifestations of Hypophosphatemia
Patients with hypophosphatemia may present with nonspecific complaints including joint pain, myalgias, irritability, and depres-sion. Severe hypophosphatemia can be manifested as seizures, arrhythmias, cardiomyopathy, insulin resistance, acute tubular necrosis, rhabdomyolysis, and acute respiratory failure.
Management
Therapy for hypophosphatemia is recommended as levels drop below 1.5 to 2.0 mg/dL, and therapy is essential as levels fall below 1.0 mg/dL. Because hypophosphatemia often is manifested with hypokalemia, phosphate repletion is considered in conjunction with potassium administration. Oral phosphorous, 250 to 500 mg twice daily, can be given to stable or asymptomatic patients. Intra-venous preparations are available as sodium phosphate (Na2PO4 and NaPO4) or potassium phosphate (K2PO4 and KPO4), and rate of infusion and choice of initial dosage should be based on severity of hypophosphatemia and presence of symptoms. If the serum phosphorus concentration is less than 1.5 mg/dL (0.48 mmol/L), 1.3 mmol/kg of elemental phosphorous (up to a maximum of 100 mmol) can be given in three or four divided doses in a 24-hour
The references for this chapter can be found online by accessing the accompanying Expert Consult website.

Chapter 125 / Electrolyte Disorders 1651.e1
References
1. Glasziou P: Practice corner: The first symptom of hyperkalemia is death. ACP J Club 2004; 140:A13.
2. Whang R, et al: Predictors of clinical hypomagnesemia. Hypokalemia, hypophosphatemia, hyponatremia, and hypocalcemia. Arch Intern Med 1984; 144:1794-1796.
3. Wrenn KD, Slovis CM, Slovis BS: The ability of physicians to predict hyperkalemia from the ECG. Ann Emerg Med 1991; 20:1229-1232.
4. Ahmed J, Weisberg LS: Hyperkalemia in dialysis patients. Semin Dial 2001; 14:348-356.
5. Semple P, Booth C: Calcium chloride; a reminder. Anaesthesia 1996; 51:93.
6. Singh BS, et al: Efficacy of albuterol inhalation in treatment of hyperkalemia in premature neonates. J Pediatr 2002; 141:16-20.
7. Allon M, Dunlay R, Copkney C: Nebulized albuterol for acute hyperkalemia in patients on hemodialysis. Ann Intern Med 1989; 110:426-429.
8. Nair S, et al: A randomized controlled trial to assess the optimal dose and effect of nebulized albuterol in acute exacerbations of COPD. Chest 2005; 128:48-54.
9. Allon M, Copkney C: Albuterol and insulin for treatment of hyperkalemia in hemodialysis patients. Kidney Int 1990; 38:869-872.
10. Allon M, Shanklin N: Effect of bicarbonate administration on plasma potassium in dialysis patients: Interactions with insulin and albuterol. Am J Kidney Dis 1996; 28:508-514.
11. Mahoney A, et al: Emergency interventions for hyperkalaemia. Cochrane Database Syst Rev 2005; 2:CD003235.
12. Gruy-Kapral C, et al: Effect of single dose resin-cathartic therapy on serum potassium concentration in patients with end-stage renal disease. J Am Soc Nephrol 1998; 9:1924-1930.
13. Kitabchi AE, et al: Hyperglycemic crises in adult patients with diabetes. Diabetes Care 2009; 32:1335-1343.
14. Alfonzo AV, et al: Potassium disorders—clinical spectrum and emergency management. Resuscitation 2006; 70:10-25.
15. Vanden Hoek TL, et al: Part 12: Cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010; 122(Suppl 3):S829-S861.
16. Blumberg A, et al: Effect of various therapeutic approaches on plasma potassium and major regulating factors in terminal renal failure. Am J Med 1988; 85:507-512.
17. Roffey P, et al: Implication of epinephrine-induced hypokalemia during cardiac arrest. Resuscitation 2003; 58:231.
18. Lin JL, et al: Outcomes of severe hyperkalemia in cardiopulmonary resuscitation with concomitant hemodialysis. Intensive Care Med 1994; 20:287-290.
19. Buckley MS, Leblanc JM, Cawley MJ: Electrolyte disturbances associated with commonly prescribed medications in the intensive care unit. Crit Care Med 2010; 38(Suppl):S253-S264.
20. Osadchii OE: Mechanisms of hypokalemia-induced ventricular arrhythmogenicity. Fundam Clin Pharmacol 2010; 24:547-559.
21. Huang CL, Kuo E: Mechanism of hypokalemia in magnesium deficiency. J Am Soc Nephrol 2007; 18:2649-2652.
22. Whang R, Whang DD, Ryan MP: Refractory potassium repletion. A consequence of magnesium deficiency. Arch Intern Med 1992; 152:40-45.
23. Hunt SA, et al: 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: Developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 2009; 119:e391-e479.
24. Umpierrez GE, et al: Treatment of diabetic ketoacidosis with subcutaneous insulin aspart. Diabetes Care 2004; 27:1873-1878.
25. Finsterer J, et al: Malnutrition-induced hypokalemic myopathy in chronic alcoholism. J Toxicol Clin Toxicol 1998; 36:369-373.
26. Udezue E, D’Souza L, Mahajan M: Hypokalemia after normal doses of nebulized albuterol (salbutamol). Am J Emerg Med 1995; 13:168-171.
27. Greenlee M, et al: Narrative review: Evolving concepts in potassium homeostasis and hypokalemia. Ann Intern Med 2009; 150:619-625.
28. Krahn LE, et al: Hypokalemia leading to torsades de pointes. Munchausen’s disorder or bulimia nervosa? Gen Hosp Psychiatry 1997; 19:370-377.
29. Gennari FJ: Hypokalemia. N Engl J Med 1998; 339:451-458.30. Coca SG, Perazella MA, Buller GK: The cardiovascular implications of
hypokalemia. Am J Kidney Dis 2005; 45:233-247.
31. Hamill-Ruth RJ, McGory R: Magnesium repletion and its effect on potassium homeostasis in critically ill adults: Results of a double-blind, randomized, controlled trial. Crit Care Med 1996; 24:38-45.
32. Huang WY, et al: Central pontine and extrapontine myelinolysis after rapid correction of hyponatremia by hemodialysis in a uremic patient. Ren Fail 2007; 29:635-638.
33. Adler SM, Verbalis JG: Disorders of body water homeostasis in critical illness. Endocrinol Metab Clin North Am 2006; 35:873-894, xi.
34. Jacobson J, Bohn D: Severe hypernatremic dehydration and hyperkalemia in an infant with gastroenteritis secondary to rotavirus. Ann Emerg Med 1993; 22:1630-1632.
35. Verbalis JG: Diabetes insipidus. Rev Endocr Metab Disord 2003; 4:177-185.
36. Palevsky PM, Bhagrath R, Greenberg A: Hypernatremia in hospitalized patients. Ann Intern Med 1996; 124:197-203.
37. Price TG, Kallenborn JC: Infant hypernatremia: A case report. J Emerg Med 2000; 19:153-157.
38. Holley AD, Green S, Davoren P: Extreme hypernatraemia: A case report and brief review. Crit Care Resusc 2007; 9:55-58.
39. Adrogue HJ, Madias NE: Hyponatremia. N Engl J Med 2000; 342:1581-1589.
40. Kaplan LJ, Kellum JA: Fluids, pH, ions and electrolytes. Curr Opin Crit Care 2010; 16:323-331.
41. Pirzada NA, Ali II: Central pontine myelinolysis. Mayo Clin Proc 2001; 76:559-562.
42. Turchin A, Seifter JL, Seely EW: Clinical problem-solving. Mind the gap. N Engl J Med 2003; 349:1465-1469.
43. Cheng JC, et al: Long-term neurologic outcome in psychogenic water drinkers with severe symptomatic hyponatremia: The effect of rapid correction. Am J Med 1990; 88:561-566.
44. Almond CS, et al: Hyponatremia among runners in the Boston Marathon. N Engl J Med 2005; 352:1550-1556.
45. Lien YHH, Shapiro JI: Hyponatremia: Clinical diagnosis and management. Am J Med 2007; 120:653-658.
46. Sterns RH, Hix JK, Silver S: Treatment of hyponatremia. Curr Opin Nephrol Hypertens 2010; 19:493-498.
47. Verbalis JG, et al: Hyponatremia treatment guidelines 2007: Expert panel recommendations. Am J Med 2007; 120(Suppl 1):S1-S21.
48. Janicic N, Verbalis JG: Evaluation and management of hypo-osmolality in hospitalized patients. Endocrinol Metab Clin North Am 2003; 32:459-481, vii.
49. Oren RM: Hyponatremia in congestive heart failure. Am J Cardiol 2005; 95:2B-7B.
50. Ellison DH, Berl T: Clinical practice. The syndrome of inappropriate antidiuresis. N Engl J Med 2007; 356:2064-2072.
51. Vaidya C, Ho W, Freda BJ: Management of hyponatremia: Providing treatment and avoiding harm. Cleve Clin J Med 2010; 77:715-726.
52. Stewart AF: Clinical practice. Hypercalcemia associated with cancer. N Engl J Med 2005; 352:373-379.
53. Ziegler R: Hypercalcemic crisis. J Am Soc Nephrol 2001; 12(Suppl 17):S3-S9.
54. Ariyan CE, Sosa JA: Assessment and management of patients with abnormal calcium. Crit Care Med 2004; 32(4 Suppl):S146-S154.
55. Nishi SP, Barbagelata NA, Atar S, Birnbaum Y, Tuero E: Hypercalcemia-induced ST-segment elevation mimicking acute myocardial infarction. J Electrocardiol 2006; 39:298-300.
56. Littmann L, Taylor L, Brearley WD: ST-segment elevation: A common finding in severe hypercalcemia. J Electrocardiol 2007; 40:60-62.
57. LeGrand SB, Leskuski D, Zama I: Narrative review: Furosemide for hypercalcemia: An unproven yet common practice. Ann Intern Med 2008; 149:259-263.
58. Drake MT, Clarke BL, Khosla S: Bisphosphonates: Mechanism of action and role in clinical practice. Mayo Clinic Proc 2008; 83:1032-1045.
59. Major P, et al: Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: A pooled analysis of two randomized, controlled clinical trials. J Clin Oncol 2001; 19:558-567.
60. Stewart AF: Clinical practice. Hypercalcemia associated with cancer. N Engl J Med 2005; 352:373-379.
61. Koo WS, et al: Calcium-free hemodialysis for the management of hypercalcemia. Nephron 1996; 72:424-428.
62. Cooper MS, Gittoes NJ: Diagnosis and management of hypocalcaemia. BMJ 2008; 336:1298-1302.
63. Aguilera M, Vaughan RS: Calcium and the anaesthetist. Anaesthesia 2000; 55:779-790.
64. Bosworth M, et al: Clinical inquiries: What is the best workup for hypocalcemia? J Fam Pract 2008; 57:677-679.
65. Levine M, Nikkanen H, Pallin DJ: The effects of intravenous calcium in patients with digoxin toxicity. J Emerg Med 2011; 40:41-46.

1651.e2 PART III ◆ Medicine and Surgery / Section Eleven • Metabolism and Endocrinology
66. Schelling JR: Fatal hypermagnesemia. Clin Nephrol 2000; 53:61-65.67. Qureshi T, Melonakos TK: Acute hypermagnesemia after laxative use.
Ann Emerg Med 1996; 28:552-555.68. Birrer RB, Shallash AJ, Totten V: Hypermagnesemia-induced fatality
following Epsom salt gargles. J Emerg Med 2002; 22:185-188.69. Tofil NM, et al: Fatal hypermagnesemia caused by an Epsom salt enema:
A case illustration. South Med J 2005; 98:253-256.70. Slovis CM, Meehan PM: Electrolyte abnormalities. In: Roppolo LP, ed.
Emergency Medicine Handbook: Critical Concepts for Clinical Practice. Philadelphia: Mosby/Elsevier; 2007:1166-1184.
71. Topf JM, Murray PT: Hypomagnesemia and hypermagnesemia. Rev Endocr Metab Disord 2003; 4:195-206.
72. Vanden Hoek TL, et al: Cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010; 122:S829-S861.
73. Soliman HM: Development of ionized hypomagnesemia is associated with higher mortality rates. Crit Care Med 2003; 31:1082-1087.
74. Poikolainen K, Alho H: Magnesium treatment in alcoholics: A randomized clinical trial. Subst Abuse Treat Prev Policy 2008; 3:1.
75. Liao F, Folsom AR, Brancati FL: Is low magnesium concentration a risk factor for coronary heart disease? The Atherosclerosis Risk in Communities (ARIC) Study. Am Heart J 1998; 136:480-490.
76. Agus ZS: Hypomagnesemia. J Am Soc Nephrol 1999; 10:1616-1622.77. ISIS-4: A randomized factorial trial assessing early captopril, oral
mononitrate, and intravenous magnesium sulfphate in 58,050 patients with suspected acute myocardial infarction. ISIS-4 Collaborative Group. Lancet 1995; 345:669.
78. Broeren MA, Geerdink EA, Vader HL, van den Wall Bake AW: Hypomagnesemia induced by several proton-pump inhibitors. Ann Intern Med 2009; 151:755-756.
79. Champagne CM: Magnesium in hypertension, cardiovascular disease, metabolic syndrome, and other conditions: A review. Nutr Clin Pract 2008; 23:142-151.
80. Kapoor M, Chan G: Fluid and electrolyte abnormalities. Crit Care Clin 2001; 17:503-529.
81. Ball CL, Tobler K, Ross BC, Connors MR, Lyon ME: Spurious hyperphosphatemia due to sample contamination with heparinized
saline from an indwelling catheter. Clin Chem Lab Med 2004; 42:107-108.
82. Slovis CM, Meehan PM: Electrolyte abnormalities. In: Roppolo LP, ed. Emergency Medicine Handbook: Critical Concepts for Clinical Practice. Philadelphia: Mosby/Elsevier; 2007:1166-1184.
83. Martin KJ, Gonzalez EA: Prevention and control of phosphate retention/hyperphosphatemia in CKD-MBD: What is normal, when to start, and how to treat? Clin J Am Soc Nephrol 2011; 6:440-446.
84. Tonelli M, Pannu N, Manns B: Oral phosphate binders in patients with kidney failure. N Engl J Med 2010; 362:1312-1324.
85. Culleton BF, et al: Effect of frequent nocturnal hemodialysis vs conventional hemodialysis on left ventricular mass and quality of life: A randomized controlled trial. JAMA 2007; 298:1291-1299.
86. Subramanian R, Khardori R: Severe hypophosphatemia. Pathophysiologic implications, clinical presentations, and treatment. Medicine (Baltimore) 2000; 79:1-8.
87. Miller DW, Slovis C: Hypophosphatemia in the emergency department therapeutics. Am J Emerg Med 2000; 18:457-461.
88. Shor R, et al: Severe hypophosphatemia in sepsis as a mortality predictor. Ann Clin Lab Sci 2006; 36:67-72.
89. Kraft MD, Btaiche IF, Sacks GS, Kudsk KA: Treatment of electrolyte disorders in adult patients in the intensive care unit. Am J Health Syst Pharm 2005; 62:1663.
90. Reference deleted in proofs.91. Chiasson JL, et al: Diagnosis and treatment of diabetic ketoacidosis and
the hyperglycemic hyperosmolar state. CMAJ 2003; 168:859-866.92. Casavant MJ, Fitch JA: Fatal hypernatremia from saltwater used as an
emetic. J Toxicol Clin Toxicol 2003; 41:861-863.93. Trepiccione F, Christensen BM: Lithium-induced nephrogenic diabetes
insipidus: New clinical and experimental findings. J Nephrol 2010; 23(Suppl 16):S43-S48.
94. Porath A, et al: Dead Sea water poisoning. Ann Emerg Med 1989; 18:187-191.
95. Liamis G, et al: Medication-induced hypophosphatemia: A review. QJM 2010; 103:449-459.
Related Documents