Chapter 11

Chapter 11. Oldest non-food crop cultivated by man/woman Originated in central Asia Cultivated & dispersed before written history 2700 BC - first.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chapter 11
Oldest non-food crop cultivated by man/woman Originated in central Asia Cultivated & dispersed before written history 2700 BC - first written record in China
◦ Used for medicinal properties

Major cannabis spread about 200 BC with Scythians◦ warlike Middle Eastern tribe, gave us word “cannabis”◦ used in cleansing ceremony after funerals◦ threw hemp seeds on heated rocks inside tents & inhaled
vapors

Hebrews also used cannabis(Old Testament in Exodus)◦ God told Moses to make holy oil containing cannabis
Most infamous use by Muslim sect founded by Hasan-Sabbah (Hashishin)◦ secret assassination◦ gave us words hashish & assassin

France in mid 1800s with "Club des Hachichins"◦ writer Gautier offered reward to anyone who invented
a new pleasure – was given hashish by a doctor Victor Hugo, Alexander Dumas
◦ consumed large quantities of hash-like material◦ wrote accounts of their experiences

In U.S., primarily for rope (George Washington) Introduced by Mexican laborers in early 1900s (group targeted by
1st laws) 1920s & 1930s - major attention - drug of violent crime & danger to
society◦ Commissioner of Narcotics, Harry Anslinger -crusade against
marijuana
1937 Marijuana Tax Act made possession of marijuana without having
paid special tax illegalEarly 1940s NYC Mayor Fiorello La Guardia
◦ set up commission of experts to determine consequences of marijuana use
◦ Final report - marijuana fairly minor intoxicant with few side effects even when used excessively
◦ Report ridiculed by Anslinger

Marijuana comeback: late 1950s to early 1960s Now most broadly used illicit substance in U.S.
◦ 35-40% of Americans having tried ◦ Numerous states have compassionate use laws

Leaves, stems and flowering buds of cannabis sativa
Most of the THC is in the buds
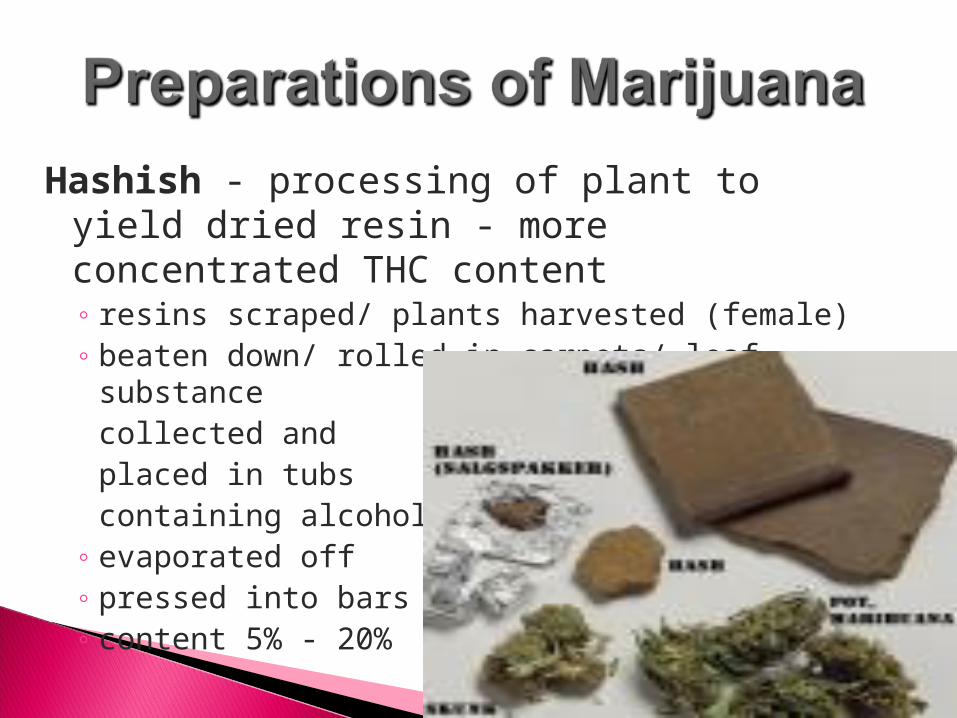
Hashish - processing of plant to yield dried resin - more concentrated THC content◦ resins scraped/ plants harvested (female)◦ beaten down/ rolled in carpets/ leaf substance
collected andplaced in tubscontaining alcohol
◦ evaporated off ◦ pressed into bars ◦ content 5% - 20%

Hash Oil - boil with solvent, solvent then strained out
THC concentration as high as 60% - 70% Becoming more popular - ease of smuggling

Cannabis L.
Stems Seeds Vegetable matter
PaperPlasticsFuelsTextilesAnimal BeddingMulch
Bird seedFlour and cerealsBody care productsNon diary milk/cheeseNut butterSalad dressingSports Bars/Protein PowderMargarinePaints/ VarnishesDetergents
Industrial hempIncense

-9-THC
-8-THC
Cannabidiol
Active Metabolites

Cannabidiol - slows metabolism of THC increase duration
converted to THC when burned may have neuroprotective, anticonvulsant and
anti-psychotic effects
◦
Administration◦ Inhalation – Smoke◦ Oral – Tincture,
Eating, Tea Marinol
◦ Oral-mucosal Sativex
Absorption◦ Smoking – rapid and
complete◦ Oral – Half that of
smoking Distribution
◦ Everywhere as it is highly lipophilic Flies across BBB

• Binds to proteins and fats
• Slow metabolism in liver
• Metabolites for a week – three weeks• Primary metabolic product is more potent
(11-OH- 9-THC)(11-OH- 9-THC) • Delay between peak plasma levels and “high”
Mostly unknown until the late 1980s ◦ 1988 – Isolated the receptors◦ 1992 – Discovered the first neurotransmitter for
that receptor
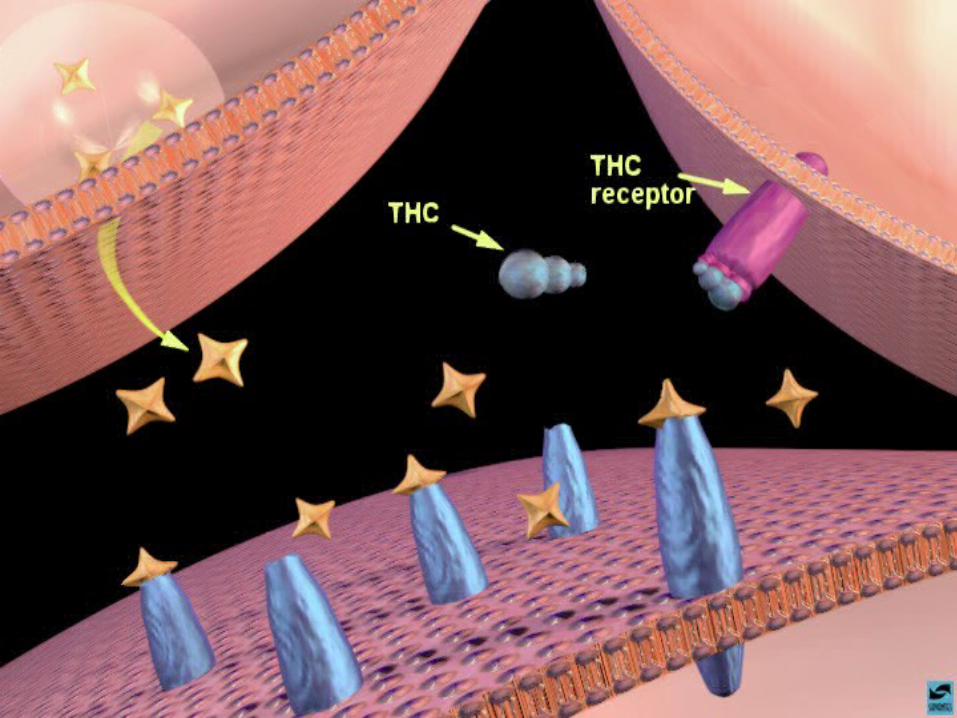
THC binds to cannabinoid receptors◦ It’s and Agonist
Anandamide & 2-AG are the NTs for cannabinoid receptors◦ Works as a retrograde NT
It modulates the activity of many neurotransmitters This is way it has such broad effects

CB-1 ReceptorCB-1 Receptor CB-2 ReceptorCB-2 Receptor
Mostly in periphery
Found primarily in immune system
Found on heart – protects from inflammation?
oLocated in CNS and PNS



Red = abundant CB1 receptor expression Black = moderately abundant CB1 receptor expression
◦ Disinhibition ◦ Relaxation
◦ Drowsiness
◦ Exhilaration, euphoria
◦ Sensory - perceptual changes Overestimate time passage
◦STM impairment
◦ Balance impaired
◦ Decreased muscle strength
◦ Small tremor
◦ Poor on complex tasks (e.g., driving)

Psychotomimetic ◦ Pseudo hallucinations
◦ Synesthesias
◦ Paranoia
◦ Agitation
◦ Disorganized thoughts
◦ Confusion
Impaired executive function◦ Increased
impulsivity
◦ Impaired judgment, slower RT
◦ Pronounced motor deficits

Physiological effects Increase in pulse rate & slight drop in BP Produces dry mouth & occasional dizziness Reddening of eyes (dilation of vessels in cornea) No permanent adverse cardiovascular
◦ People with heart disease should abstain Increased risk for heart attack four an hour after smoking
Appetite increased◦ Hypothalamus◦ “Hedonic Hotspot” – specific area of NAC when stimulated by
cannabinoids there is an increase in the reward value of natural rewards.
THC suppresses immune system, but not enough to increase risk of infection it appears.
Lowers testosterone levels & sperm count as well as estrogen
Crosses placental barrier◦ Lower birth weight◦ Some evidence suggests a relation between
mother smoking while pregnant and childhood cancer
Most severe side effects ◦ Respiratory - can lead to asthma & bronchitis◦ Anxiety/panic in some users

Almost impossible to OD◦ 1-1.8 kg w/5% taken orally in a female◦ THC not toxic in this sense
Pot smoke contains more tar than cigarette smoke◦ Does one smoke the same?◦ Cancer and respiratory possibilities
Data on cancer is very mixed – recent studies show no relationship
THC found to kill cultured hippocampal cells, but so far not in other cells high in CB receptor density◦ Effect reversed with NSAIDS◦ Possible mechanism for memory loss

Tolerance develops with heavy long-term use Reverse tolerance in consistent users Cross tolerance with sedatives - alcohol Dependence – mild (like SSRIs)
◦ Mild withdrawal symptoms in humans, with irritability, depression, sleep disturbances, nausea, diarrhea, sweating, tremors, reduced food intake, and salivation 50% of heavy users may experience it 30 mg THC / 4 hrs / 10-20 days (unusual levels of intake) Begin within 48 hours after cessation and lasts 2 – 10
days
Amotivational Syndrome◦ Most research has not found this to be true◦ Is it a HOST effect?
It may be psychopathology independent of use Gateway Drug
◦ Most well-designed studies suggest this is false. “Common liability model” is a better explanation
◦ Alcohol and cigarettes are stronger gateway drugs if one accepts the data
Many states have compassionate use laws◦ California, Washington, Oregon, Nevada, Alaska,
Vermont, Maine, Colorado, New Mexico, Montana, Rhode Island, Maryland
Physicians “recommend” marijuana and patient buy it at buyers clubs.◦ Would lose license if prescribed
2003 Gallup Pole – 75% for medical use, 66% against legalization
2005 study of physicians'’ attitudes◦ 36 % were in favor of legal prescription◦ 26% were neutral

1998 IOM report concluded that there is scientific evidence for the medical use of marijuana◦ Analgesic – Next slide◦ Anti-emetic◦ Anti-spastic◦ Appetite Stimulant◦ Glaucoma◦ Tumor suppression (lung cancer)◦ Siezures? – THC & Cannibidiol protect against
neurotoxicity Cannabinoid Antagonists?
- Ramonabant

Likely mediated through CNS/PNS mechanism as well as non-NS systems◦ RVM – Part of brainstem
THC increases activity of pain suppressing neurons and decreases activity of pain enhancing neurons
Inhibits glutamate release Increases dynorphin release
◦ CB receptors located on peripheral sensory nerves Reduce pain signaling from the site of “damage”
◦ Inhibits prostaglandin synthesis

Studies show smoking is superior to oral administration of either synthetic or natural THC
Significant problems w/smoking however Tar and toxins Respiratory problems Cancer? – Want to
make sure it’s not an issue
Vaporizers ◦ Heat pot to 180-200
degrees ◦ Releases active drugs,
but does not produce toxins
Sativex – THC spray◦ Delivered as a mist◦ Used in Western
Europe and Canada◦ Studies are positve

The Empirical View…….◦ There is a medical use for THC◦ Medical use does not require legalization◦ You can be anti-drug and pro-medicalization◦ Saying there is no medical value is a
statement based in either politics or ignorance/stupidity
◦ There are ways to get the gains of smoked THC without smoking
◦ Like many other medicines, there are risks and the a potential for abuse

Related Documents











