Chapter 1: Introduction

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chapter 1: Introduction

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 1
1.1 Biofilms
John Donne (1572–1631) famously wrote ‘‘No man is an island, entire of itself ’’;
words that summarise an absolute truth of humanity- it is impossible to thrive and
flourish in isolation. An idea that we, as humans, still do not completely understand
has been accepted and incorporated since times immemorial into the lives of the most
seemingly primitive creatures - Microorganisms.
For most of the history of microbiology, microorganisms have primarily been
characterized as planktonic, freely suspended cells and described on the basis of their
growth characteristics in nutritionally rich culture media (Donlan, 2002). The extent
to which microbial growth and development occurred on surfaces, as complex
communities had not been clearly fathomed (Hall-Stoodley et al., 2004). It was in the
1970s that scientists began to appreciate that in most natural environments, majority
of bacterial biomass exist in the form of surface-associated microbial communities
(Costerton et al., 1999). Such a population of surface-associated well organised, co-
operating communities of microorganisms then came to be referred to as a ‘Biofilm’,
a term coined by Bill Costerton in 1978 (Kolter, 2010; Kokare et al., 2009; Chandki et
al., 2011). The widespread recognition that biofilms possessed the ability to impact a
plethora of varied environments from water pipes to catheters and stents of patients
led to a curiosity about molecular mechanisms underlying the formation and
maintenance of these communities (Costerton et al., 1999). This interest triggered the
development of various imaging techniques and experimental models that have now
elucidated that biofilms are not simply passive assemblages of cells that are stuck to
surfaces, but are structurally and dynamically complex biological systems (Hall-
Stoodley et al., 2004). In 2002, Donlan and Costerton offered the most salient
description of a biofilm by describing it as “a microbially derived sessile community
characterized by cells that are irreversibly attached to a substratum or interface or to
each other, are embedded in a matrix of extracellular polymeric substances that they
have produced, and exhibit an altered phenotype with respect to growth rate and gene
transcription” (Donlan and Costerton, 2002). The biofilm mode of existence has
developed as a survival strategy where in the cooperative communal nature of a
microbial community provides advantages to the participating microorganisms. These
advantages include broader habitat range for growth, an enhanced resistance to

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 2
antimicrobial agents and host defence and an enhanced virulence (Donlan and
Costerton, 2002).
1.2 Mouth as a microbial habitat
It has been estimated that the human body is made up of 1014 cells of which only 10%
are mammalian while the rest are the microorganisms that make up the resident
microflora of the host (Marsh, 2000a; Avila et al., 2009). The composition of this
microflora varies at distinct habitats like urogentital tract, human gut, skin, etc but is
relatively consistent over time at each individual site among individuals (Marsh,
2000a). The oral cavity is one such site of the body whose distinct resident microflora
has been of great interest due to its vast diversity (Bowden and Hamilton, 1998). The
following unique features of the mouth make it a unique microbial habitat:
1. Within the oral cavity, mucosal surfaces like lips, cheek and palate are subject to
continuous shedding of cells or desquamation which impedes accumulation of
biofilms. In contrast, teeth provide hard non-shedding surfaces that allow
accumulation of higher quantities of biomass. Such differences in the type of
subtratum and the environmental factors they are exposed to, leads to local variations
in microbial composition of biofilms at different locations within the oral cavity
(Marsh, 2000a; Liljemark and Bloomquist, 1996).
2. The constant flushing of saliva within the mouth has a substantial effect on the oral
microflora. Saliva has a pH range (6.75-7.25) that encourages the growth of many
microorganisms. Components of saliva influence the development of biofilms by the
following mechanisms: (Marsh, 2000a; Scannapieco, 1994)
a. Aggregating microbes to facilitate their clearance from the mouth
b. Adsorbing to teeth surface to form an acquired pellicle to which
microorganisms can attach
c. Serving as a primary source of nutrients
d. Mediating microbial inhibition or killing
3. In addition to saliva, the gingival crevicular fluid (GCF), a plasma derived fluid
that flows through the junctional epithelium, provides microbes in the gingival crevice

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 3
with nutrients and carries host immune components that play an important role in
regulating the microflora therein (Marsh, 2000a).
The oral cavity is not a homogenous environment. It is characterised by differences
among sites in key ecological factors like adhesion ligands, pH, nutrients, redox
potential, oxygen and temperature. To persist in the oral cavity, bacteria must be able
to tolerate rapid and substantial environmental fluctuations (Lemos et al., 2005).
Different sites of the mouth like lips, palate, cheek, tongue and the different teeth
surfaces provide distinct habitats, thereby resulting in the development of distinct site-
specific microbial communities. The properties of the habitat influence the type and
number of species colonising it. Factors affecting the growth of microorganisms in the
healthy oral cavity are enlisted in Table 1.1.
Table 1.1: Key environmental factors affecting the growth of microorganisms in
the healthy oral cavity (Marsh, 2000b)
Factor Range Comment Temperature 35–36°C
Oxygen 0–21%
Oxygen is abundant at mucosal surfaces Gradients exist in dental plaque enabling obligate anaerobes to grow.
Redox potential
(Eh)
+ 200 to < - 200 mV
Gradients exist within plaque; lowest value recorded in gingival crevice.
pH 6.75-7.25 Plaque pH falls during dietary sugar metabolism Sub-gingival plaque pH rises during inflammation.
Nutrients
Endogenous
Exogenous
Peptides, proteins and glycoproteins in saliva and gingival crevicular fluid. Dietary sugars facilitate selection of acidogenic and acid-tolerating species in plaque causing a reduction in plaque pH and demineralisation of enamel.

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 4
Once the early colonisers form their niche, they may modify the surrounding
environment, making it suitable for other species to colonize. Thus, a bidirectional
relation exists between the habitat and the microbial community (Takashi, 2005).
1.3 Oral Microflora
The oral microbial community is diverse. Oral microbes are predominantly bacteria
but fungi, viruses, mycoplasmas and even protozoa (Marsh, 2000a) and archaea
(Kulik et al., 2001) can also be found. Previous studies utilizing culture-dependent
and culture independent molecular techniques have estimated the diversity within the
oral cavity to consist of over 700 species or phylotypes, however, not all of these have
been identified (Kulik et al., 2001; Aas et al., 2005; Kreth et al., 2009). Numerous
factors impede the identification of this vast number of species. The most challenging
hurdles are as follows:
• Many of the species are non-culturable with available laboratory technologies.
• Genomic similarities do not allow for organismal determination based on short
read lengths.
In spite of these limitations, efforts are under way to identify and characterize the
microorganisms with the largest representation within the communities of healthy
mouths (Jenkinson and Lamont, 2005;Avila et al; 2009). The different bacterial
genera commonly found in the oral cavity have been enlisted in Table 1.2.

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 5
Table 1.2: Bacterial genera found in the oral cavity (Marsh and Martin, 1999)
Gram positive Gram negative
Cocci
Abiotrophia
Enterococcus
Peptostreptococcus
Streptococcus
Staphylococcus
Stomatococcus
Moraxella
Neisseria
Veillonella
Rods
Actinomyces
Bifidobacterium
Corynebacterium
Eubacterium
Lactobacillus
Propionibacterium
Pseudoramibacter
Rothia
Actinobacillus Haemophilus
Bacteroids Campylobacter
Leptotrichia Cantonella
Prophyromonas Capnocytophaga
Prevotella Cantipedia
Selenomonas Desulphovibro
Simonsiella Desulphobacter
Eikenella Fusobacterium
Treponema Wolinella
Some of these bacteria tend to predominate in certain distinct microbial habitats
within the oral cavity as summarized in Table 1.3

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 6
Table 1.3: Distinct microbial habitats within a healthy mouth (Marsh, 2000a)
Habitat Predominant
microbial groups Comments
Lips, palate,
cheek
Streptococcus spp.
Neisseria,
Veillonella
Desquamation restricts biomass
Surfaces have distinct cell types
Candida act as opportunistic pathogens
Staphylococcus may be present
Tongue
Streptococcus spp.
Actinomyces
Veillonella
Obligate anaerobes
Simonsiella
Highly papillated surface-reservoir for
anaerobes
Teeth
Streptococcus spp.
Actinomyces
Veillonella,
Eubacterium
Obligate anaerobes
Spirochaetes
Haemophili
Non-shedding surfaces that promote biofilm
formation
Distinct surfaces for colonisation (fissures,
approximal, gingival crevice) which support a
characteristic flora due to their intrinsic
biological properties.
Teeth harbour the most diverse oral microbial
communities
In spite of being well equipped with an array of host defences provided by both the
innate and adaptive arms of the immune system, all mucosal and dental surfaces of the
mouth are naturally colonised by a diverse collection of micro-organisms. There is
evidence to suggest that the resident bacteria have developed mechanisms to evade
host defences to ensure longer survival in the oral cavity (Macotte and Lavoie, 1998).
Studies show that there exists an active communication between some of the resident
bacteria and mucosal cells that down regulates potentially damaging pro-
inflammatory host responses to the normal oral microflora, while the host retains the
ability to respond to genuine microbial insults (Cosseau et al., 2008; Marsh, 2012).

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 7
The oral resident flora has developed mechanisms that permit a beneficial relationship
with the host which include:
• ‘Colonisation resistance’: Resident oral bacteria prevent the establishment of
exogenous microorganisms within the mouth. The natural oral microflora is
better adapted at attachment to oral surfaces and more efficient at metabolising
the available nutrients for growth. They can also produce inhibitory factors
and create hostile environments that restrict colonisation by potential
microbial invaders (Marsh, 1992; Lemos et al., 2005; Marsh and Percival,
2006).
• Contributions to gastrointestinal and cardiovascular health: Recent
findings suggest that the resident oral bacteria contribute to the maintenance of
healthy gastrointestinal and cardiovascular systems via the metabolism of
dietary nitrate. Approximately 25% of ingested nitrate is secreted in saliva
where some oral resident bacteria reduce nitrate to nitrite. Nitrite can affect a
number of key physiological processes including the regulation of blood flow,
blood pressure, gastric integrity and tissue protection against ischemic injury
(Lundberg, 2009; Marsh 2012).
Therefore, it is imperative, antimicrobial agents used to treat oral health issues are
used judiciously with respect to doses and duration of treatments, to ensure that
beneficial resident microflora of the mouth are not indiscriminately killed.
1.4 Dental plaque
The diverse oral microflora were initially thought to be free living but were later
understood to be thriving in the form of one of the most complex surface associated
microbial communities of the human body - Dental plaque. In 1683, The Dutch
naturalist Anton van Leeuwenhoek (1632-1723) was the first to open the world’s eyes
to the world of microorganisms by examining samples of his own dental plaque using
his homemade microscope (Kuramitsu et al., 2007; Huang et al., 2011). Clinically,
dental plaque is the soft, tenacious deposit that forms on tooth surfaces and which is
not readily removed by rinsing with water (Bowen, 1972). Microbiologically, Marsh

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 8
(2004) has saliently defined plaque as “the diverse community of microorganisms
found on the tooth surface as a biofilm, embedded in an extracellular matrix of
polymers of host and microbial origin”.
From a microbial physiology aspect, oral microbial communities are classical
examples of biofilms. Just as initially proposed by Costerton et al., (1995) the
behaviours displayed by oral microbial organisms grown in liquid culture are very
different from those of the same organisms grown on a solid surface or within a
community such as dental plaque (Davey and O’Toole, 2000; Islam et al., 2007).
Dental plaque is characterised by unique properties enlisted in Table 1.4
Table 1.4: Properties of dental biofilms (Marsh, 2004; Garcia-Godoy and Hicks,
2008)
Property Mechanism of Action
Open architecture Presence of channels and voids
Protection from host
defences Extracellular polymers form a functional matrix
Enhanced resistance to
antimicrobial agents
Increased resistance to antibiotic agents and
chlorhexidine
Neutralization of inhibitors Beta-lactamase production by bacteria to protect
sensitive neighbouring bacteria
Gene transfer Drug-resistant genes and increased ability to take
up DNA
Novel gene expression Synthesis of novel proteins
Coordinated gene responses Production of cell-cell signalling molecules
(competence-stimulating peptide, autoinducer-2)
Spatial and Environmental
Heterogeneity
pH and oxygen concentration gradients and co-
adhesion
Broad Habitat Range Obligate anaerobes in an aerobic environment
Pathogenic Synergism Enhanced virulence and resistance to stress
Efficient Metabolism Catabolism of complex macromolecules by
bacterial community working in concert

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 9
As a result of these properties, dental plaque possesses a highly resilient nature. In the
presence of good dental hygiene practices, it is destroyed on a daily basis yet quickly
and repeatedly re-establishes itself (Palmer et al., 2006). Of all oral microbial
ecosystems, dental plaque has been the major focus of oral microbiological research
probably because of its characteristic features as a complex polymicrobial biofilm and
its association with dental caries and periodontal diseases.
1.4.1 Microbial composition of dental plaque
Based on its location and its relationship with the gingival margin, plaque can be
broadly classified into two categories:
• Supragingival plaque: Plaque situated superior to the gingival margin
• Subgingival plaque: Plaque situated inferior to the gingival margin. It may or
may not be attached to the epithelium or tooth surface (Reddy, 2008).

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 10
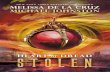
Figure 1.1: Diagrammatic representation depicting the classification of plaque on
the basis of their location and relationship with gingival margin (Marsh and
Martin, 1999)

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 11
Microbial constituents vary among the two types of plaque due to differences in their
biological properties. The comparisons between supragingival plaque and
subginigival plaque have been summarized in Table 1.5
Table 1.5: Comparison between supragingival plaque and subgingival plaque
(Takahashi, 2005; Aas et al., 2005; Kuramitsu et al., 2007; Reddy, 2008)
Supragingival Plaque Subgingival Plaque
Surface for microbial
adhesion Saliva-coated tooth
GCF-coated tooth
GCF-coated epithelium
Matrix 50% Matrix Little or no matrix
Flora Mostly Gram positive Mostly Gram negative
Motile bacteria Few Common
Anaerobic/ Aerobic Aerobic unless thick Highly anaerobic
Nutrition Saliva
Carbohydrates
GCF
Desquamated epithelium
pH Neutral/ Acidic Neutral
Oxygen concentration High/ Low Low
Metabolic property
of
microbial ecosystem
Saccharolytic Asaccharolytic/ Proteolytic
Dominant bacterial
species
Streptococcus sanguinis
Streptococcus mutans
Streptococcus mitis
Streptococcus salivarius
Lactobacillus
Aggregatibacter
actinomycetemcomitans
Tannerella forsythia
Campylobacter spp.
Capnocytophoga spp.
Eikenella corrodens
Fusobacterium nucleatum
Porphyromonas gingivalis
Prevotella intermedia
Treponema denticola

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 12
In the cases of both, supragingival and subgingival plaque, the microbial communities
on teeth and gingival tissues can accumulate high concentrations of bacterial
metabolites. These include fatty acid end products, ammonia, hydrogen peroxide,
oxidants and carbon dioxide within their local environments, which further influence
the bacterial species within the microbial community, as well as the host (Kuramitsu
et al., 2007).
1.4.2 Formation of dental plaque
Formation of dental plaque is a dynamic process involving continuous attachment,
growth, detachment and reattachment of oral microorganisms, but can be divided into
several stages. As delineated by Marsh (2000a), these stages are:
a) Acquired enamel (or dental) pellicle formation: Within minutes of tooth
eruption or professional cleaning of tooth, molecules of salivary and microbial
origin selectively adsorb to the tooth surface. Li et al. (2004a) have identified
different molecules of the acquired pellicle which include albumin, amylase,
carbonic anhydrase II, secretory Immunoglobulin A (sIgA), Immunoglobulin
G (IgG), Immunoglobulin M (IgM), lactoferrin, lysozyme, proline-rich
proteins (PRP), statherin, histatin 1 and mucous glycoprotein. Some of these
like PRP, amylase, mucins and statherin function as receptors for bacterial
adhesins (Scannapeico et al., 1994). Glucosyltransferases can also be found in
the active form in the enamel pellicle where they catalyze the synthesis of
glucan that serves as a ligand for glucan binding proteins on Streptococci.
b) Passive transport of microorganisms to the pellicle: The primary colonizers
of the biofilm attach to the receptors of the pellicle. They are mostly Gram
positive cocci and rods and filaments and a small number of gram-negative
cocci (Li et al., 2004b; Sbordone and Bortolaia 2003).
c) Reversible bacterial adhesion: This results from long-range (10-20 nm)
physico-chemical interactions between the bacterial surface and the pellicle-
coated tooth. The interplay of repulsive electrostatic forces (both surfaces are
negatively charged) and Van der Waals attraction result in a weak net
attraction. This can be augmented by cation bridging and hydrophobic

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 13
interactions or further weakened by hydration forces (Jenkinson and Lamont,
1997). As soon as the pioneer bacteria attach to the pellicle, they begin to
excrete extracellular polysaccharides (EPS), which helps the bacteria stay
bound together and attach to the pellicle (Huang et al., 2011).
d) Irreversible bacterial adhesion: The reversible adhesion, discussed above, is
followed by a much stronger, irreversible attachment. Short-range (<1 nm)
stronger, specific stereochemical interactions involving bacterial surface
components (adhesins) and cognate receptors on the pellicle begin to occur.
Lectin-like adhesion, which involves binding of carbohydrate (glycosidic)
receptors by bacterial polypeptide adhesins are a commonly observed
interaction (Jenkinson and Lamont, 1997).
e) Late colonization: This stage is characterised by two crucial physical
interactions - co-aggregation and co-adhesion. Co-aggregation is the cell-cell
recognition between genetically distinct bacteria in a planktonic suspension,
whereas co-adhesion refers to the recognition between a planktonic cell and a
surface-attached cell (Foster and Kolenbrander, 2004). These interactions
involve adhesin-receptor interactions between approaching bacteria and
already attached early colonizers, increasing the diversity of the biofilm. The
cohesion process results in characteristic morphological structures such as
corncobs and test-tube brushes (Seniviratne et al., 2011) and may facilitate
metabolic interactions.
f) Multiplication of the attached microorganisms and confluent growth: The
bacterial cells continue to divide until a three-dimensional mixed-culture
biofilm forms that is spatially and functionally organized. Metabolism of
microorganisms modifies the local environment and creates gradients in key
parameters (oxygen, redox potential, pH, nutrients, and metabolic end
products) creating micro-environments that enable coexistence and growth of
diverse bacteria with conflicting needs (Marsh and Bradshaw, 1997).
Synthesis of extracellular polysaccharides also takes place, resulting in the
formation of intercellular matrix. The spatial arrangement of the cells and

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 14
intercellular matrix will determine the architecture of the biofilm (Marsh,
2004).
g) Active detachment of bacteria: The detachment of bacteria from biofilms is
essential to allow colonization of new habitats. Detachment may occur in
multiple ways: detachment as single cells in a continuous predictable fashion
(erosion), sporadic detachment of large groups of cells (sloughing) or as an
intermediate process whereby large pieces of biofilm consisting of about 104
cells are shed from the biofilm in a predictable manner (Thomas and Naikishi,
2006). Bacteria within the biofilm can produce enzymes that break specific
adhesins, enabling cells to detach into saliva and probably colonize elsewhere
(Marsh, 2004).

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 15
Figure 1.2: Diagrammatic representation depicting pattern of biofilm
development in dental plaque (Rickard et al., 2003)

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 16
1.4.3 Structure of dental plaque
In order to gain a better understanding, conventional techniques like light and electron
microscopy have been used to visualise biofilms. However, biofilm specimen
preparation (dehydration, fixation, and staining) may result in artifacts, shrinkage and
distortion. With the advent of confocal laser scanning microscopy (CLSM), it has
become possible to observe living biofilms while they grow and metabolize and is
aided with information from modern staining methods. In addition to fluorescent
staining methods, it is possible to use dyes that bind selectively to either dead or live
bacteria allowing the investigator to understand the distribution of viable and non
viable cells within the biofilm (ten Cate, 2006). The current concept of biofilm
structure is based on the pioneering studies done by the Bozeman Montana Center for
Biofilm Engineering (Costerton et al., 1995). They showed the biofilm as a thin basal
layer on the substratum, in contact and occasionally penetrating the acquired pellicle,
and with columnar, mushroom-shaped multi-bacterial extensions into the lumen of the
solution, separated by regions (“channels”) seemingly empty or filled with
extracellular polysaccharide (EPS).
1.4.4 Interactions between resident flora within dental plaque
Microorganisms within the dental biofilm are spatially arranged in close proximity to
each other, which facilitates interactions among them. These interactions are crucial to
maintenance of stability of the biofilm. The interactions include: (Kuramitsu et al.,
2007)
• Competition between bacteria for nutrients
• Synergistic interactions which may stimulate the growth or survival of one or
more residents
• Production of an antagonist by one resident which inhibits the growth of
another
• Neutralization of a virulence factor produced by one organism by another
resident
• Interference in the growth-dependent signalling mechanisms of one organism
by another

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 17
In addition to these interactions, bacteria additionally communicate with each other
through a phenomenon called Quorum sensing. Quorum sensing is a process of
chemical communication among bacteria, which is defined as a gene regulation in
response to cell density, which influences various functions, like virulence, acid
tolerance and biofilm formation (Hojo et al., 2009). Quorum sensing signalling serves
intra-species communication and is often highly specific. The quorum-sensing
systems found in oral bacteria include signal molecules called autoinducers like AI-2
and streptococcal competence stimulating peptide (CSP) (Olsen, 2006). The luxS gene
expressing AI-2 is conserved among many species of bacteria, including
Streptococcus mutans, Streptococcus gordonii, Streptococcus oralis, Porphyromonas
gingivalis, Aggregatibacter actinomycetemcomitans and other oral microorganisms
(Huang et al., 2011). AI-2 produced is detected by a large number of diverse bacteria,
hence it is called a “universal language” used for cross-species communication
(Yung-Hua and Xiaolin, 2012). The competence stimulating peptide (CSP) is known
to induce alarmones- intracellular signal molecules that are produced due to harsh
environmental factors. These alarmones can convey sophisticated messages in a
population including the induction of altruistic cellular suicide under stressful
conditions (Huang et al., 2011). These quorum sensing systems are indispensible in
mature biofilms characterised by high cell density and the presence of a varied array
of species. Efforts are under way to develop therapies that interference with these
quorum sensing mechanisms to deal with oral biofilm related ailments and diseases
(Olsen, 2006). 1.4.5 Microbial homeostasis
Once resident plaque microflora develop at a healthy site within the mouth, its species
composition is characterized by a degree of stability or balance among the component
species, in spite of regular minor environmental stresses caused due to dietary
components, oral hygiene, host defences, diurnal changes in saliva flow, etc. (Marsh,
2006). This stability, termed as “Microbial homeostasis”, develops not due to
indifference among the component species but rather results from a dynamic balance
of microbial interactions, including synergism and antagonism as well as subtle cell-
cell signalling (Marsh, 1992). Mature dental plaque biofilm acts as a community or a
unit rather than as a sum of the properties of individual bacterial members
(Seneviratne et al., 2011). In a state of Microbial homeostasis, dental plaque does not

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 18
have the ability to cause harm but in fact promotes good oral health, since they share a
beneficial relationship with the host as previously described.
1.4.6 Perturbations to dental plaque
Plaque preferentially accumulates at stagnant or retentive sites unless it is removed by
diligent oral hygiene. As the plaque mass increases, the buffering and antimicrobial
properties of saliva are less able to penetrate plaque and protect the enamel and
gingival tissues. Insufficient oral hygiene, aging processes, genetic factors, changes in
dietary intake as well as changes in immunity of host can encourage the plaque
microbiota into a diseases associated state. There is a shift in the balance of the
predominant bacteria in plaque away from those associated with health and microbial
homeostasis breaks down (Garcia-Godoy and Hicks, 2008).
Current hypotheses to explain the role of plaque bacteria in the etiology of
diseases
The fact that periodontitis and dental caries, the most prevalent diseases in humans,
are dental plaque-mediated diseases is very well established (Sbordone and Bortolaia,
2003). However, despite 120 years of active research, there has been on-going
controversy as to which bacteria within the biofilm are involved in causation of these
diseases. Two hypotheses have been proposed in this respect:
• Specific plaque hypothesis
The "Specific Plaque Hypothesis" proposed by Loesche (1976) stated that, out of the
diverse collection of organisms comprising the resident plaque microflora, only a few
species are actively involved in disease. It therefore entails that treatment involving an
antimicrobial component should be aimed at diagnosis and then elimination of
causative organisms (Marsh, 2006).
• Non-Specific Plaque Hypothesis
This hypothesis proposed by Theilade (1986) purports that caries are an outcome of
the overall activity of the multiple species present within the heterogeneous plaque
microflora and not a specific organism. In keeping with this hypothesis, the flora
would need to be suppressed either continuously or periodically using agents that

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 19
ensure maximum lethality of flora. This could lead to over usage of broad-spectrum
agents or the combination of agents (Loesche, 1999; Marsh, 2006).
As an alternative to the two main schools of thought mentioned above, a hypothesis
has been proposed that reconciles the key elements of the two earlier hypotheses.
• Ecological Plaque Hypothesis
A direct relationship exists between the environment and the balance and behaviour of
resident plaque microflora. A shift in the homeostatic balance of the resident
microflora due to a change in local environmental conditions can lead to the selection
or enrichment of previously minor components of the oral biofilm thereby causing
diseases. This concept led to the proposal of a modified hypothesis by Marsh (1991,
1994) called the "Ecological Plaque Hypothesis". Common factors that disrupt
homeostasis include frequent exposure to nutrients like fermentable carbohydrates,
consistently low pH within the oral cavity and low availability of oxygen.
Manipulation of physiological factors that drive changes in the oral environment
could lead to some degree of control over the composition of the plaque community,
and lead to the identification of new physiological strategies to maintain the beneficial
properties of the biofilm (Marsh and Bradshaw, 1997).
1.5 Plaque mediated diseases
Much attention has been focused on the identification of bacteria which cause oral
diseases. It is of equal importance that bacteria associated with health also be
identified so that a microbiological goal for therapy can be established (Aas et al,
2005; Filoche et al., 2010). However, it is difficult to define a normal flora given the
prevalence and complexity of these diseases, although recent research has indicated
that there is a distinctive bacterial flora in a healthy oral cavity which is different from
that of diseased oral cavities (Filoche et al., 2010). Figure 1.3 depicts transitions in the
composition of predominant plaque microflora in health and disease.

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 20
Figure 1.3: Transitions in the composition of predominant plaque microflora in
health and disease (Marsh, 1992)
Figure 1.4: Accumulation of dental plaque beyond levels compatible with oral
health (Walsh, 2006)

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 21
1.5.1 Plaque mediated dental caries
Dental caries is a transmissible bacterial disease process caused by acids from
bacterial metabolism diffusing into enamel and dentine and dissolving the mineral
(Featherstone, 2008). Dental caries was once thought to be a simple disease with the
mutans streptococci group being attributed as the sole etiological agent. Caries
research was dominated by treatments targeted at these species (Loeche et al., 1975;
Minahi and Loesche, 1977; Nishikawara et al., 2006; Filoche et al., 2010). The group
Mutans streptococci includes Streptococcus mutans and Streptococcus sobrinus. Their
key virulence factors include synthesis of water insoluble glucans from sucrose,
adherence, acidogenicity and aciduricity (Nishikawara et al., 2006). However, it has
now been established that the presence of high numbers of mutans streptococci alone
is insufficient for the development of caries (Seneviratne et al., 2011). The direct
cause of dental caries is cariogenic plaque which develops when normally low
populations of acidogenic and aciduric bacterial species, previously in balance with
the oral environment, increase following high frequency carbohydrate exposure
(Loesche, 1986; Filoche et al., 2010). Cariogenic plaques (CP) harbour high levels of
S. mutans, S. mitis, Bifidobacterium spp, low levels of Streptococcus sanguinis and
moderate to high levels of Actinomyces species. Levels of lactobacilli steadily
increase as the lesion progresses (Minahi and Loesche, 1977; Seneviratne et al., 2011;
Filoche et al., 2010). The metabolism of fermentable carbohydrates by these
microbiota result in the acidification of plaque (pH<5). The acid induced
demineralization of the enamel and dentin cause cavitation in the teeth.

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 22
Figure 1.5: Use of ecological plaque hypothesis to explain the incidence and
prevention of caries. (Marsh and Bradshaw, 1997)
Figure 1.6: Severely damaged teeth due to carious lesions and cavitations.
(Szczawinska-Poplonyk et al., 2011)

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 23
1.5.2 Plaque mediated periodontal disease
Periodontal disease reflects a cellular inflammatory response of the gingival and
surrounding connective tissue to the bacterial accumulations on teeth (Filoche et al.,
2010; Kornman, 2008). These inflammatory responses are clinically classified as
gingivitis and periodontitis. Apart from the non-exfoliating surface of teeth being an
ideal substratum for plaque formation, they are also a link to the deep periodontal
space, offering microorganisms an easy route of entry into dentinal tubules and
enamel enamel fissures. These regions are easily colonized by microbes, but difficult
to reach for the host defence mechanisms (Sbordone and Bortolaia, 2003). The
accumulation of plaque around the gingival margin leads to inflammation or infection
of the gums called gingivitis. This inflammatory response leads to an increased flow
of GCF which, in addition to introducing components of the host response, also
provides a novel source of potential nutrients for the microflora (Marsh and Bradshaw,
1997). Additionally release of GCF leads to a reduction in the redox potential (Eh)
which is preferred by periodontopathic bacteria like Porphyromonas gingivalis
allowing them to overgrow other organisms in the dental plaque (Marsh and
Bradshaw, 1997; Seneviratne et al., 2011). When left untreated, the infection and
inflammation spread from the gingival to the ligaments and bone that support the
teeth leading to periodontitis. Loss of support causes the teeth to become loose and
eventually fall out. Periodontitis is the primary cause of tooth loss in adults (Savage,
2009). Periodontal disease is characterised by a significant increase in the prevalence
of obligate anaerobic Gram negative bacilli, especially proteolytic species (Marsh and
Bradshaw, 1997) like Porphyromonas gingivalis, Treponema denticola, Prevotella
intermedia, Aggregatibacter actinomycetecomintans and Fusobacterium nucleatum
(Marsh 1992, Filoche et al., 2010).

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 24
Figure 1.7: Use of ecological plaque hypothesis to explain the incidence and
prevention of periodontal diseases (Marsh and Bradshaw, 1997)
Figure 1.8: Accumulation of plaque around the gingival margin leading to
gingivitis and periodontitis (Preshaw et al., 2012)

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 25
1.5.3 Plaque and systemic health The periodontium responds to dental plaque by the process of inflammation. Plaque
releases a variety of biologically active products, such as bacterial lipopolysaccharides,
chemotactic peptides, protein toxins, and organic acids. These molecules stimulate the
host to produce a variety of responses, among them the production and release of
potent agents known as cytokines (Panagakos and Scannapieco, 2011). Considering
the chronic nature of these diseases and the exuberant local and systematic host
response to the microbial assault, it is reasonable to hypothesize that these infections
may influence systemic health and disease (Scannapieco, 1998; Panagakos and
Scannapieco, 2011). A number of epidemiological studies have suggested that an
infected oral cavity can act as the site of origin for dissemination of pathogenic
organisms to distant body sites, especially in immuno-compromised hosts or hosts
undergoing immunosuppressive treatments (Li et al, 2000). In 1891, Miller proposed
the theory of focal infection which stated that “foci” of sepsis were responsible for the
initiation and progression of a variety of inflammatory diseases. In spite of this theory
being largely unsubstantiated, there has been a renewed interest in investigating
relationships between systemic and oral health (Barnet, 2006).
With normal oral health and dental care, only small numbers of mostly facultative
bacterial species gain access to the bloodstream. In the absence of oral hygiene, the
numbers of bacteria colonizing the teeth, especially supragingivally, could increase 2-
to 10-fold (Li et al., 2000). Under normal circumstances, the host possesses barrier
systems that work together to inhibit and eliminate penetrating dental plaque bacteria.
However, as a result of advanced periodontitis, a thin, highly permeable, and
frequently ulcerated pocket epithelium is the only barrier between the bacterial
biofilms and the underlying connective tissues. The strands of the pocket epithelium
are easily broached, allowing large doses of bacterial toxins and other products access
to the tooth supporting connective tissues and blood vessels thereby introducing
bacteria into the bloodstream, leading to an increase in the prevalence and magnitude
of bacteremia (Li et al., 2000; Jin et al., 2003).
Once the bacteria and toxins gain access to the bloodstream, they may further lead to
cardiovascular diseases, infective endocarditis, bacterial pneumonia and diabetes

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 26
mellitus. Periodontal disease is also linked to adverse pregnancy outcomes (Li et al.,
2000; Jin et al., 2003; Panagakos and Scannapieco, 2011). 1.6 Approaches to control of dental plaque
Considering the impact of dental plaque on oral and systemic health, there is a need to
devise therapies dedicated to its control. The various approaches towards the control
of dental plaque have been discussed below:
1.6.1 Mechanical control of dental plaque
Mechanical plaque control still remains the basic element for the prevention and
control of plaque build up (Vacaru et al., 2003). Toothbrushing is the most commonly
used measure for plaque control in daily oral self care (Creeth et al., 2009, Imai et al.,
2012). However, in spite of regular brushing, it is possible that plaque may still
remain as tooth brushes are unable to penetrate intact interdental areas. Power
toothbrushes can serve as an alternative to manual toothbrush by delivering more
enhanced plaque removal due to the mode of action, better compliance and/or, by
correcting poor brushing technique (Sharma et al., 2012). Use of tongue scrapers,
dental floss, interdental tooth brushes and tooth picks are recommended as adjuncts to
toothbrushing (manual or power) to achieve better results (Imai et al., 2012). A
professional tooth cleaning every 6-8 weeks aids in periodic removal of plaque from
all tooth surfaces using mechanically driven instruments. Regular dental visits are
recommended to keep oral health in check. These visits generally include plaque
evaluation, oral hygiene instructions, probing depth measurements, registration of
bleeding on probing, scaling (plaque removal) if required and tooth polishing
(Westfelt, 1996).
Limitations in mechanical control: (Asadoorian, 2006; Bansal et al., 2012; Creeth et
al., 2009; Teles and Teles, 2009; Imai et al., 2012)
• Results obtained from brushing are subject to a variety of factors like type of
brush, duration and technique of brushing, manual dexterity of the user, etc.
• Only 2-10% of the population perform interdental cleaning on daily basis
using floss or tooth picks.

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 27
• Epidemiological data have suggested that mechanical oral self care does not
achieve its theoretical potential for controlling bacterial plaque accumulation
and gingival disease.
1.6.2 Chemical control of dental plaque
Studies indicate that self performed mechanical plaque removal is inefficient and
leaves room for improvement. Efforts directed towards development of chemical
agents of plaque control have provided a plethora of agents that maybe used as an
adjunct to mechanical plaque control to reduce or prevent oral disease (Teles and
Teles, 2009; Asadoorian, 2006). Five categories of agents for approaches have been
considered: (Asadoorian, 2006; Mhaske et al., 2012)
• Antibiotics aimed at inhibition or killing of specific bacteria
• Broad spectrum antiseptics aimed at killing or preventing proliferation of all
plaque organisms
• Single or combinations of enzymes that could modify plaque structure or
activity
• Modifying agents that are non – enzymatic which act as dispersing or
denaturing agents that can alter structure or metabolic activity of plaque
• Agents that could affect bacterial attachment to pellicle surface
Table 1.6: Commonly used antibiotics in oral care and their mode of action
(Soares et al., 2012)
Antibiotic Mode of action
Penicillins Inhibition of peptidoglycan synthesis
Tetracylines Inhibition of amino acid and protein synthesis
Alterations in cytoplasmic membrane leading to leakage of cell
contents
Macrolides Inhibition of protein synthesis
Metronidazole Formation of redox intermediate intracellular metabolites that
target RNA, DNA and cellular proteins

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 28
Table 1.7: Commonly used antiseptics in oral care and their mode of action
(Marsh, 1992; Asadoorian, 2006; Ishiyama et al., 2012; Mhaske et al., 2012)
Active agents Examples Mode of action
Phenolic compounds Triclosan
Cell wall disruption
Induce leakage of cell
contents
Bacterial enzyme inhibition
Bis-biguanides Chlorhexidine
Cell wall disruption
Precipitation of cytoplasm
contents
Quaternary
ammonium compounds
Cetylpyridinium chloride
(CPC)
Domiphen bromide
(DB)
Benzethonium chloride
(BC)
Cell wall disruption
Alteration of cytoplasm
contents
Halogens Fluoride, Iodine
Bacterial enzyme inhibition
Interferes with acid
production of acidogenic
bacteria
Oxygenating agents Peroxides Cytotoxicity due to generation
of reactive oxygen species
Limitations in chemical control
• Chlorhexidine, often referred to as the “gold standard” for oral care is known
to cause side effects like staining of the tongue, teeth and restorations,
perturbation of taste and also supragingival calculus (Marsh, 1992; Bansal et
al, 2012).
• The dosage of a chemical agent is determined as per its laboratory evaluated
Minimum Inhibitory Concentration (MIC) or Minimum Bactericidal
Concentration (MBC). However within the oral cavity, a chemical agent may

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 29
remain at MIC levels for a very short duration due to loss of agent via
expectoration and constant swallowing (Marsh, 1992; Marsh 2012).
• Long term use of broad spectrum antimicrobials may lead to disruption of the
natural balance of the oral microflora, colonization by exogenous organisms
and development of microbial resistance (Marsh, 1992; Bansal et al., 2012).
1.6.3 Biological control of dental plaque
a) Probiotic therapy
Instead of using chemical agents that may disrupt the homeostasis of the resident
plaque flora, probiotic therapy is being explored as an alternative. Three main modes
of action have been proposed to contribute to the effects of probiotics: (Sugano et al.,
2012)
• Production of antimicrobial substances against pathogens
• Competitive exclusion mechanisms
• Modulation of host defence systems
Studies suggest that Lactobacillus salivarius T12711 and Streptococcus salivarius
K12 possess the potential to be used as non-cariogenic probiotics for maintaining a
healthy ecosystem for the oral microflora, thereby preventing the colonization of
periodontopathic bacteria (Burton et al., 2006; Islam et al., 2007; Sugano et al., 2012).
Additionally, a new class of pathogen-selective molecules, called specifically (or
selectively) targeted antimicrobial peptides (STAMPs) were developed to selectively
kill Streptococcus mutans within multi-species dental plaque. Competence stimulating
peptide (CSP) produced by S. mutans was selected as the STAMP targeting domain to
ensure the targeted delivery of the antimicrobial peptide. This ensured the elimination
of S. mutans without affecting closely related non cariogenic oral streptococci,
indicating the potential of these molecules to be developed into “probiotic” antibiotics
(Eckert et al., 2006).

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 30
b) Vaccines
Secretory IgA is the principal immune component of major and minor gland salivary
secretions and thus would be considered to be the primary mediator of adaptive
immunity in the salivary milieu apart from other immunoglobulins like IgG and IgM
which are derived from the gingival crevicular fluid. In addition to this, gingival
sulcus also contains various cellular components of the immune system like
lymphocytes, macrophages and neutrophils (Gambhir et al., 2012). The mode of
action of these antibodies is inhibition of the adherence and possibly metabolic
activities of pathogenic bacteria of the oral cavity (Islam et al., 2007). With a view of
developing vaccines, organisms crucial in the etiology of caries and periodontal
diseases are designated as targets. The virulence factors contributing to the
pathogenecity of these organisms are recognised as the key antigens for development
of vaccines. The research focus is mainly on the incorporation of these antigens into
mucosal immune systems and delivery with or without adjuvants to mucosal IgA-
inductive sites. P. gingivalis and S. mutans are being explored as targets for vaccine
development due to their roles in periodontal diseases and caries respectively (Islam
et al., 2007; Sugano et al., 2012).
c) Replacement therapy
Recombinant DNA technology had aided in the development of one of the most
promising new approaches to maintaining homeostasis within the oral cavity-
Replacement therapy. Genetic engineering is used to modify the wild type strain of a
pathogen into an “effector” strain such that it is deficient of its virulence factors but
posses excellent colonization potential. An effector strain should posses the following
properties: (Hillman et al., 2000)
• It must not cause disease itself or otherwise predispose the host to other
disease states by disrupting the ecosystem in which it resides.
• It must persistently colonize the host tissue at risk and thereby prevent
colonization or outgrowth of the pathogen to levels necessary for it to exert its
pathogenic potential.
• In situations where the pathogen is itself a member of the indigenous flora, an
effector strain should aggressively displace the resident pathogen
• It should possess a high degree of genetic stability.

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 31
When introduced into the oral cavity, the effector strain will colonize the niche,
thereby preventing colonization and outgrowth of wild-type strain (Islam et al., 2007).
Using this approach, a harmless strain is permanently implanted in the host’s oral
flora. Studies on S. mutans effector strains have shown promising results (Hillman et
al., 2007).
1.6.4 Herbal control of dental plaque
Considering the limitations of synthetic agents on plaque control, efforts are
underway to identify novel nature-based anti-plaque strategies. Medicinal plants have,
since time immemorial, provided mankind with an array of uses in amelioration of
diseases. Most developing countries still majorly rely on traditional medicine
(Palombo, 2009; Bansal et al., 2012). Multiple studies have reported the use of plants
in the form of crude extracts or as isolated phytochemicals in the treatment of oral
diseases.
Presence of phytochemicals like flavonoids, tannins, alkaloids and essential oils have
been reported to be responsible for the potential of plant extracts in improving oral
health (Ferrazzano et al., 2009; Palombo, 2009). Sanguinarine and essential oils like
thymol, menthol and eucalyptol are already making their presence felt as potent oral
care agents comparable to synthetic agents like Chlorhexidine (Marsh, 1992; Bansal
et al., 2012; Asadoorian, 2006).
Advantages of Herbal control:
• Herbal products have a larger public acceptance due its nature based approach
and minimal side effects.
• There is no dearth in availability of medicinal plants in India thereby ensuring
a sustainable supply of economic medicines.
1.7 Biofilm Models in Oral Care Research
Anti-plaque agents, synthetic or natural, are evaluated primarily in the laboratory
using conventional microbiological methods that allow the determination of MIC or
MBC values which are usually quoted as the primary indicator of their potential
efficacy (Marsh, 1992; Kinniment et al., 1996; Haraszthy et al., 2006). However,

Chapter 1: Introduction
School of Science, SVKM’s NMIMS (deemed-to-be) University Page 32
these agents may markedly vary in their efficacy when used in vivo. Reasons for this
discrepancy include: (Wilson, 1996; Sbordone and Bortolaia, 2003)
• Biofilms within the mouth are polymicrobial and more resistant.
• The effectiveness of antimicrobial agents decreases with increasing age of the
biofilm.
• Presence of extracellular polysaccharide matrix hinders penetration of the
agents.
• Growth of microbiota within the biofilm is very slow, leading to slow uptake
of the agent.
Due to these factors, many oral care agents fail clinically in spite of promising results
during laboratory evaluation. Therefore, it is now apparent that standardised tests
such as determination of MIC are no longer appropriate on their own to fully
characterise susceptibility of plaque to new therapeutics (Pratten and Ready, 2010).
Additionally, in vivo experimental studies on natural dental plaque is inconvenient
due to difficulties experienced during volunteer studies (Sissons, 1997). These
difficulties have given incentive to the development of range of biofilm models
(Sissons, 1997; Wimpenny, 1997; Pratten and Ready, 2010). These models may be
designed and set up to mimic various characteristics of the oral cavity thereby
allowing better understanding of the underlying mechanisms of biofilm formation and
the measure that need to be taken for its control (Pratten and Ready, 2010). Prediction
of in vivo plaque behaviour towards a therapeutic agent is made possible when
evaluated within an experimental biofilm model (Sissons, 1997).
Efforts have continually been directed towards the development of novel anti-plaque
agents. However, at present, the need for side effect free anti-plaque agents as well as
the resolution of issues regarding inadequacies in efficacy testing protocols are areas
that have become the prime focus of oral care research.
Related Documents