Changing health behaviors to improve health outcomes after angioplasty: a randomized trial of net present value versus future value risk communication M. E. Charlson 1 *, J. C. Peterson 1 , C. Boutin-Foster 1 , W. M. Briggs 2 , G. G. Ogedegbe 3 , C. E. McCulloch 4 , J. Hollenberg 1 , C. Wong 5 and J. P. Allegrante 1,6 Abstract Patients who have undergone angioplasty expe- rience difficulty modifying at-risk behaviors for subsequent cardiac events. The purpose of this study was to test whether an innovative ap- proach to framing of risk, based on ‘net present value’ economic theory, would be more effective in behavioral intervention than the standard ‘fu- ture value approach’ in reducing cardiovascular morbidity and mortality following angioplasty. At baseline, all patients completed a health as- sessment, recieved an individualized risk profile and selected risk factors for modification. The intervention randomized patients into two vary- ing methods for illustrating positive effects of behavior change. For the experimental group, each selected risk factor was assigned a numeric biologic age (the net present value) that approx- imated the relative potential to improve current health status and quality of life when modifying that risk factor. In the control group, risk reduc- tion was framed as the value of preventing future health problems. Ninety-four percent of patients completed 2-year follow-up. There was no differ- ence between the rates of death, stroke, myocar- dial infarction, Class II–IV angina or severe ischemia (on non-invasive testing) between the net present value group and the future value group. Our results show that a net present risk communication intervention did not result in significant differences in health outcomes. Introduction Patients who have undergone percutaneous trans- luminal coronary angioplasty (PTCA) must make behavioral changes, such as stopping smoking, in- creasing physical activity, decreasing cholesterol and reducing weight, in order to reduce the risk of subsequent cardiac events. Cessation of smoking, for example, has been shown to result in a lower recurrence rate, with less angina, fewer limitations of physical activity and increased survival [1–5]. Other lifestyle changes, such as taking lipid-lowering medicine, have been shown to reduce the recur- rence of the disease. At least two studies have shown that intensive lipid-lowering therapy can re- sult in regression of disease [6, 7]. Despite the risk of recurrence, most patients with coronary heart disease who have undergone PTCA do not make major changes in behaviors [8]. Because patients find it difficult to adopt and maintain behavioral changes after angioplasty [9, 10], we sought to investigate a novel approach 1 Center for Complementary and Integrative Medicine, Weill Cornell Medical College, New York, NY 10065, USA, 2 Department of Mathematics, Central Michigan University, Mount Pleasant, 48859, 3 Department of Medicine, College of Physicians and Surgeons, Columbia University, New York, NY 10032, USA, 4 Department of Epidemiology and Biostatistics, School of Medicine, University of California, San Francisco, CA 94143, USA, 5 Department of Medicine, Weill Cornell Medical College New York, New York, NY 10021, USA and 6 Department of Health and Behavior Studies, Teachers College and Department of Sociomedical Sciences, Mailman School of Public Health, Columbia University, New York, NY 10027, USA *Correspondence to: M. E. Charlson. E-mail: [email protected] Ó The Author 2007. Published by Oxford University Press. All rights reserved. For permissions, please email: [email protected] doi:10.1093/her/cym068 HEALTH EDUCATION RESEARCH Vol.23 no.5 2008 Pages 826–839 Advance Access publication 19 November 2007 by guest on February 18, 2016 http://her.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Changing health behaviors to improve health outcomesafter angioplasty: a randomized trial of net present value
versus future value risk communication
M. E. Charlson1*, J. C. Peterson1, C. Boutin-Foster1, W. M. Briggs2,G. G. Ogedegbe3, C. E. McCulloch4, J. Hollenberg1, C. Wong5 and
J. P. Allegrante1,6
Abstract
Patients who have undergone angioplasty expe-rience difficulty modifying at-risk behaviors forsubsequent cardiac events. The purpose of thisstudy was to test whether an innovative ap-proach to framing of risk, based on ‘net presentvalue’ economic theory, would be more effectivein behavioral intervention than the standard ‘fu-ture value approach’ in reducing cardiovascularmorbidity and mortality following angioplasty.At baseline, all patients completed a health as-sessment, recieved an individualized risk profileand selected risk factors for modification. Theintervention randomized patients into two vary-ing methods for illustrating positive effects ofbehavior change. For the experimental group,each selected risk factor was assigned a numericbiologic age (the net present value) that approx-imated the relative potential to improve currenthealth status and quality of life when modifying
that risk factor. In the control group, risk reduc-tion was framed as the value of preventing futurehealth problems. Ninety-four percent of patientscompleted 2-year follow-up. There was no differ-ence between the rates of death, stroke, myocar-dial infarction, Class II–IV angina or severeischemia (on non-invasive testing) between thenet present value group and the future valuegroup. Our results show that a net present riskcommunication intervention did not result insignificant differences in health outcomes.
Introduction
Patients who have undergone percutaneous trans-
luminal coronary angioplasty (PTCA) must make
behavioral changes, such as stopping smoking, in-
creasing physical activity, decreasing cholesterol
and reducing weight, in order to reduce the risk of
subsequent cardiac events. Cessation of smoking,
for example, has been shown to result in a lower
recurrence rate, with less angina, fewer limitations
of physical activity and increased survival [1–5].
Other lifestyle changes, such as taking lipid-lowering
medicine, have been shown to reduce the recur-
rence of the disease. At least two studies have
shown that intensive lipid-lowering therapy can re-
sult in regression of disease [6, 7].
Despite the risk of recurrence, most patients
with coronary heart disease who have undergone
PTCA do not make major changes in behaviors
[8]. Because patients find it difficult to adopt and
maintain behavioral changes after angioplasty
[9, 10], we sought to investigate a novel approach
1Center for Complementary and IntegrativeMedicine,Weill
Cornell Medical College, New York, NY 10065, USA,2Department of Mathematics, Central Michigan University,
Mount Pleasant, 48859, 3Department of Medicine, College of
Physicians and Surgeons, Columbia University, New York,
NY 10032, USA, 4Department of Epidemiology and
Biostatistics, School of Medicine, University of California,
San Francisco, CA 94143, USA, 5Department of Medicine,
Weill Cornell Medical College New York, New York, NY
10021, USA and 6Department of Health and Behavior
Studies, Teachers College and Department of Sociomedical
Sciences, Mailman School of Public Health, Columbia
University, New York, NY 10027, USA
*Correspondence to: M. E. Charlson.
E-mail: [email protected]
� The Author 2007. Published by Oxford University Press. All rights reserved.For permissions, please email: [email protected]
doi:10.1093/her/cym068
HEALTH EDUCATION RESEARCH Vol.23 no.5 2008
Pages 826–839
Advance Access publication 19 November 2007
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

to communicating risk in an effort to motivate
patients to make changes in health behavior. The
current approach to communicating risk informa-
tion largely helps patients to understand how mak-
ing behavioral changes will reduce ‘future risk’.
Our intervention approach was designed to ap-
proach the communication of risk by framing the
value of behavior modification in terms of the ‘net
present value’ (what patients can gain now) of the
change. Thus, our approach was designed to pro-
vide patients and their physicians with a personally
relevant means by which they could prioritize life-
style changes in terms of a tangible value associated
with the change in relative risk associated with
a change in behavior. This approach and its poten-
tial application to understanding risk communica-
tion in health behavior change have theoretical
origins in net present value economic theory [11].
In economic theory, the concept of net present
value involves taking the future value of a good or
investment and relating it to what it is worth in
present dollar terms by discounting based on
expectations of interest rate, inflation and demand.
For the study, this theoretical perspective was ap-
plied in communicating the benefit of changing
health behavior in terms of reduced risk. To do
so, the health effects of a potentially beneficial be-
havioral change were portrayed in present value or
present value health terms that have been calculated
within a short (3-year) time frame and for which the
change in mortality can be clearly and understand-
ably related to the change in risk at any given age.
Thus, as Allegrante and Roizen [11] have pointed
out: ‘. if smoking a pack {of cigarettes} a day
increases the risk for the average 50-year-old Cau-
casian male to that of the average 58-year-old
{counterpart}, net-present value of smoking today
is 8 years of aging (or, in effect, a loss of 8 years)’.
We have outlined in detail the theoretical frame-
work and intervention methods underlying our ap-
proach to communicating future health risks in the
PTCA patient population in a previously published
paper [12].
This paper reports a randomized trial whose ob-
jective was to evaluate the efficacy of a behavioral
intervention that communicated risk based on a net
present value approach versus a standard ‘future
value’ approach in reducing cardiovascular morbid-
ity and mortality following angioplasty or stenting.
In addition, we examined the impact of the inter-
vention on stages of change operationalized from
the Transtheoretical Model of Stages of Change
[13, 14] and behavior-specific self-efficacy [15, 16].
Methods
Patient eligibility criteria, screening andrecruitment
This study protocol (#0302005991) was approved
by the Institutional Review Board of Weill-
Cornell Medical College on 6 July 1998 and has
been reapproved every year since. The study was
conducted from 1999 to 2003. All patients under-
going coronary artery catheterization who had at
least single-vessel stenosis and revascularization
with PTCA or coronary artery stenting were eligible
for enrollment if they were (i) not enrolled in an-
other trial designed to modify behavior, (ii) verbally
fluent in English and (iii) able to provide informed
consent within 1 week after the procedure. We
identified and screened for potential eligibility a to-
tal of 2022 patients through a systematic, daily re-
view of the cardiac catheterization schedule at the
New York-Presbyterian Hospital—Weill-Cornell
Medical College during an 18-month period.
Patients were enrolled during hospitalization fol-
lowing PTCA or coronary artery stenting.
Various factors contributed to the ineligibility of
screened patients (Fig. 1). In total, 38% of patients
who were screened met eligibility requirements. In
total 53% of eligible patients were enrolled. A total
of 660 patients provided written informed consent
and were randomized.
Baseline demographic and clinical history
Patient demographic status was documented for
age, sex, marital status, ethnicity, occupation, edu-
cation and employment. The mean age of all
patients was 62 years, and 27% were female.
Twenty-one percent were African-American or La-
tino. Sixty-two percent were married. Forty-three
Changing health behaviors after angioplasty
827
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

Fig. 1. CONSORT model: flow of patients through the study.
M. E. Charlson et al.
828
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

percent were college graduates, and 16% had not
completed high school. Forty-three percent were
working full time and 36% were retired.
The duration and history of patients’ symptoms
and treatments were noted, as well as history of
myocardial infarction, unstable angina, congestive
heart failure, previous catheterization or coronary
artery bypass grafting. Prior to angioplasty, 58%
of patients had unstable angina and 25% had a his-
tory of myocardial infarction. The mean ejection
fraction 50%. At baseline, 17% had undergone
prior bypass surgery, while 36% had prior angio-
plasty/stenting. Overall, 57% had hypertension,
26% diabetes and 14% obesity.
The Charlson comorbidity scale [17] was used to
evaluate the burden of comorbid disease. Baseline
medications were also recorded, especially the use of
aspirin, nitrates, beta adrenergic blockers, calcium
channel blockers, digitalis, diuretics, angiotensin-
converting enzyme inhibitors, other anti-hypertensive
agents, insulin or oral hypoglycemic agents, sedative/
hypnotics, anti-depressants and steroids. Height and
weight were recorded, and body mass index was cal-
culated. Total cholesterol, high density lipoprotein
(HDL) and low density lipoprotein (LDL) levels were
also recorded. Pertinent data from the angioplasty in-
cluded the number of vessels treated, the number and
type of stents, the ejection fraction and complications
of the procedure, if any. Procedures were performed
on an average of two vessels.
Patients completed a health assessment that eval-
uated 13 cardiac risk factors, including physical
activity, smoking, diet and medications. The dietary
questionnaire was based on the semi-quantitative
food frequency questionnaire, a reproducible and
valid measure of intake of many nutrients, which
has been used longitudinally to assess the dietary
habits of older adults and patients with chronic and
cardiac disease [18–21]. The physical activity ques-
tionnaire comprised a modification of the Minne-
sota leisure time activity questionnaire [22]. The
risk assessment provided all patients with their
own individualized risk factor profile in which
the behavior was highlighted for change, if an
individual patient’s status was outside normal or
recommended ranges. The possible areas for car-
diovascular risk behavior change can be broadly
cast in five major domains:
Physical activity: increase physical activity, in-
crease aerobic exercise or increase strength training.
Smoking: stop smoking (or continue not to
smoke).
Diet/weight: reduce weight, reduce red meat,
reduce dietary intake of saturated fat and choles-
terol, increase fiber-rich food, increase flavonoid-
rich food, increase folic acid intake.
Blood pressure, diabetes: control/reduce blood
pressure, control diabetes.
Medications: take beta blockers/reduce heart rate.
All patients received feedback about their status
on the selected list of 13 cardiovascular risk factors.
Recommendations for behaviors to target for
change were based on pre-specified cutoffs [12].
Patients were then asked to choose two to three risk
factors to target for lifestyle change. Although more
risk factors could have been chosen, we decided
that only two to three risk factors could be feasibly
managed by patients. Both the patient and cardiol-
ogist received a copy of the risk profile and behavior
change choices. All patients were then asked to
consult with their cardiologist prior to implementing
any new health behavior change activity.
Stage of change is a measure of readiness for
initiating changes in each risk factor and included
five possible stages: pre-contemplation, contempla-
tion, preparation, action and maintenance. The
stage of change model has been utilized in assessing
behavior change with various health-related behav-
iors, including diet [23], weight [24], exercise [25]
and changing more than one behavior at a time [26].
Researchers have evaluated rates of the stages of
change and how they differently impact behavior
change likelihood [27].
Experimental and control intervention
The intervention theory and methods utilized in this
study have been described in extensive detail in an
earlier report [12]. Patients were randomized to one
Changing health behaviors after angioplasty
829
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

of two groups, which determined the specific type
of feedback that they would receive: the experimen-
tal net present value (n = 329) or the control stan-
dard future value intervention (n = 331). The study
biostatistician prepared a randomization schedule
from random numbers prior to the enrollment of
the first patient. The assignments were placed in
sealed opaque numbered envelopes prior to the on-
set of the study. Randomization was stratified for
diabetes, gender and minority status in order to
achieve balancing of those factors. None of the de-
mographic or clinical characteristics differed statis-
tically between the two groups (Table I). Once
adjusting for multiple comparisons among each of
the characteristics, there was no significant differ-
ence for any of the patient characteristics at baseline.
Patient education about each risk factor in an in-
dividualized profile was framed using either a future
risk approach or a net present value approach,
where each factor is weighted according to its rel-
ative risk. To help patients in both groups get
started, we provided them with behavior change
‘tip sheets’ for each of the risks they selected to
change, as well as referrals for behavior change
programs and other community resources. The tip
sheets provided practical advice about how to
change behavior. For example, the physical activity
tip sheet suggested parking a car at the far end
of a parking lot in order to walk further to one’s
destination.
In both groups, stages of behavioral change [13]
and behavior-specific self-efficacy [15, 16] for each
of the behaviors of interest—increasing physical ac-
tivity, stopping smoking, increasing or decreasing
certain dietary elements, losing weight, controlling
blood pressure and taking medications—were also
assessed. The stage of change construct was
assessed by a single-item rating of five stages (1 =
pre-contemplation, 2 = contemplation, 3 = prepara-
tion, 4 = action and 5 = maintenance). We assessed
stage of change for all patients at baseline and again
at 12- and 24-month follow-ups for each of the cho-
sen risk factor behaviors. To measure the discrete
stage of change, we asked the individual whether
they were seriously considering changing a risk fac-
tor behavior of interest within the next 6 months.
Similarly, behavior-specific self-efficacy was
assessed with a single-item confidence rating on
a scale of 1–10 (1 = not at all confident, 10 = very
confident) for each chosen behavioral risk factors,
at baseline and at 12- and 24-month follow-ups. For
example, to measure self-efficacy with regard to
overall physical activity, we asked: ‘How confident
are you that you will be able to start doing more
regular physical activity (starting with 10 min a day
for at least 3 days a week; and gradually working up
Table I. Selected demographic and clinical characteristics of
patients in the net present value and future value groups at
baseline (by percent, unless otherwise indicated)
Characteristic Net present
value
Future
value
Demographics
Age (mean age in years 6s.d.) 62.7 6 11.6 62.8 6 1.5
Female 27 27
African-American 12 12
Latino 8 10
Married 61 64
High school graduate 43 39
College graduate 39 46
Employed full time 43 44
Clinical
Prior myocardial infarction 24 43
Prior angioplasty 35 38
Congestive heart failure 6 5
Hypertension 56 58
Depression (mean CES-D
score 6s.d.)
11.2 6 11 11.6 6 11
Average Body Mass Index in
kg/m2
28.0 6 5.3 28.0 6 5.3
Ejection fraction 51 51
Charlson comorbidity score
0 34 34
1–2 39 41
>3 27 25
Peripheral Vascular Disease 18 20
Diabetes 26 27
Cancer 12 14
Stroke 8 5
Medications
Calcium channel blockers 9 9
Beta blockers 54 46
Nitrates 26 22
Diuretics 11 12
Aspirin 76 76
Number of vessels treated 2.3 6 2.0 2.2 6 1.9
Left main disease 6 4
M. E. Charlson et al.
830
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

to longer periods for 4–5 days a week) within the
next month?’
Net present value approach (experimentalgroup)
The experimental group received feedback about
their cardiovascular risk factors framed in a com-
mon metric—‘biologic age’. Biologic age was cal-
culated with a research version of the RealAge�software, which was modified for use in this study.
RealAge combines a person’s historical data and
habits to provide a posterior state of knowledge
risk. In the modified version, at the outset an indi-
vidual’s biologic age is the same as his or her chro-
nologic or calendar age. Patients were told their
estimated biologic age (calculated using data from
the baseline health risk assessment). The data for
each risk factor were communicated in terms of the
amount of ‘biologic age reduction’ one could
achieve within 3 months and within 2 years, if each
risk factor was changed. From this individual pro-
file, patients were asked to choose two to three of
these risk behaviors to begin changing ‘now’ be-
cause doing so ‘will decrease your biologic age’.
For each risk factor, they were given a set of action
steps, i.e. individualized guidelines for each risk
factor that emphasized the present value of making
a behavioral change.
Future value or standard approach(control group)
The control group received feedback about their
cardiovascular risk factors in terms of deviation
from normative values. From their individual pro-
files, patients were asked to choose two to three of
these risk factors to begin changing now because
doing so ‘will increase your lifespan’. For each risk
factor, they were given a set of action steps, i.e.
individualized guidelines for each risk factor that
emphasized the future value of behavioral change.
Follow-up
For 2 years, both groups of patients were contacted
and interviewed by telephone at 3-month intervals.
The telephone contact provided motivational sup-
port to patients in both groups, using a specific
script that was based loosely on the principles of
motivational interviewing developed by Emmons
and Rollnick [28], to assist patients in adopting
and maintaining behavioral changes. In addition,
each call included an updated assessment of interval
clinical events and changes in cardiovascular risk
profile, as well as an opportunity for the individual
patient to change or add new risk factors.
The follow-up was designed to capture all rele-
vant interval events, including behavioral change
and new outcomes or cardiac procedures or related
hospitalizations. In total, 88% of patients had their
clinical status assessed at 3–6 months, 76% at 9–12
months, 63% at 15–18 months and 93% at 24
months. In total, 86% of patients had detailed risk
factor profiles updated at 3–6 months, 71% at 9–12
months, 53% at 15–18 months and 47% at 21–24
months. There was no difference in follow-up rates
between the net present value and future value
groups. Seventy-six percent of the patients com-
pleted four or more follow-up assessments.
Primary outcomes
Patients completed their final evaluation for major
post-operative clinical outcomes at ;24 months
(68 weeks). The primary outcome was freedom
from death, myocardial infarction, stroke, Class
II–IV angina or severe asymptomatic ischemia at
24 months. The time course of freedom from death,
myocardial infarction, stroke, Class II–IV angina or
severe asymptomatic ischemia was also docu-
mented, with the primary end point being the time
to first event. Revascularization was not included as
an end point because indications vary widely.
End point review was conducted by a cardiolo-
gist who was blinded to randomization group and
included:
Mortality: all deaths from any cause.
Myocardial infarction: new persistent Q waves of
>0.03 msec and >1 mV in depth were required
in two contiguous leads on a standard 12-lead
electrocardiogram in the absence of a new con-
duction abnormality or a marked change in the
QRS axis.
Changing health behaviors after angioplasty
831
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

Angina: the absence of angina was defined as
freedom from Class II–V anginal symptoms.
Severe ischemia on non-invasive testing: non-
invasive testing was not routinely performed on
patients enrolled in this trial. Whether or not
patients had non-invasive testing was decided
entirely by the patient’s own physician. This
end point was designed to capture those pa-
tients who were without anginal symptoms,
but who were found on non-invasive testing to
have sufficiently severe ischemia to warrant
revascularization.
Stroke: this was defined as the occurrence of
a new major focal neurologic deficit, which per-
sisted >24 hours.
Power and data analysis
We have estimated the occurrence of the principal
outcome defined above (mortality, myocardial in-
farction, stroke, Class II–IV angina or severe is-
chemia) is 30%. (Total event rates after
angioplasty range from 30—to 45%, and the event
rates after stents are somewhat lower; 30% is taken
as the event rate in the control arm.) Hence, the
expected outcome rate in the control arm, Pc, is
taken to be 0.30. A drop in the incidence of any of
the adverse outcomes to a level of 0.20 would con-
stitute a clinically important difference between the
two management strategies. Therefore, d (where d =
Pc � Pe) is taken to be 0.10. Based on the above
values of Pc, d and a two-sided alpha of 0.05, with
a b error of 0.2 for 80% power, the sample size is
estimated to be a total of 590 patients or 295 in each
group.
Sample size was based on 80% power for the
occurrence of any one of the following out-
comes: death, myocardial infarction, stroke, Class
II–IV angina or severe ischemia on non-invasive
testing. The level for testing the significance of
the principal outcome was set at P = 0.05. All
data were entered into an integrated series of data-
bases and then transported to SAS for windows
v.8.02 (Cary, SC) for statistical analyses. After 24
months of follow-up, we analyzed the data for main
effects between groups, efficacy and safety accord-
ing to the intention-to-treat principle.
Results
Risk factors at baseline
Overall, there were no statistically significant dif-
ferences between randomization groups in the spe-
cific risk factors chosen for change, as described
below. Patients had an average of six risk factors
recommended for behavioral change at baseline.
Patients in both groups were asked to identify risk
factors they wished to select for change, and, on
average, they chose three risk factors for change.
Table II shows the percentage of patients at baseline
for whom a risk factor was recommended for
change and the percentage of patients who chose
a risk factor for change, if recommended. Increas-
ing physical activity was recommended for change
in 85% of patients and reducing cholesterol was
recommended in 86%; quitting smoking was rec-
ommended in the 25% of patients who were cur-
rent smokers. The most common risk factors
chosen at baseline for change were overall physi-
cal activity (66%), smoking (62%) and weight loss
(59%).
Table II shows the proportion of patients whose
stage of change was preparation as well as ratings of
perceived self-efficacy. Most patients who chose to
change a behavior were at the preparation stage for
change. Patients had high self-efficacy or confi-
dence in their ability to modify health behaviors
immediately after angioplasty, with average self-
efficacy scores of between 7 and 9. For either stage
of change or self-efficacy, there were no statistically
significant differences between randomization
groups.
At baseline, patient biologic ages were calcu-
lated, with biologic age being an identical mean
of 68 years in both groups. On average, the biologic
age of patients participating in the study was ;6
years older than their actual chronologic age. Only
patients in the net present value group were given
feedback in terms of biologic age.
M. E. Charlson et al.
832
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from
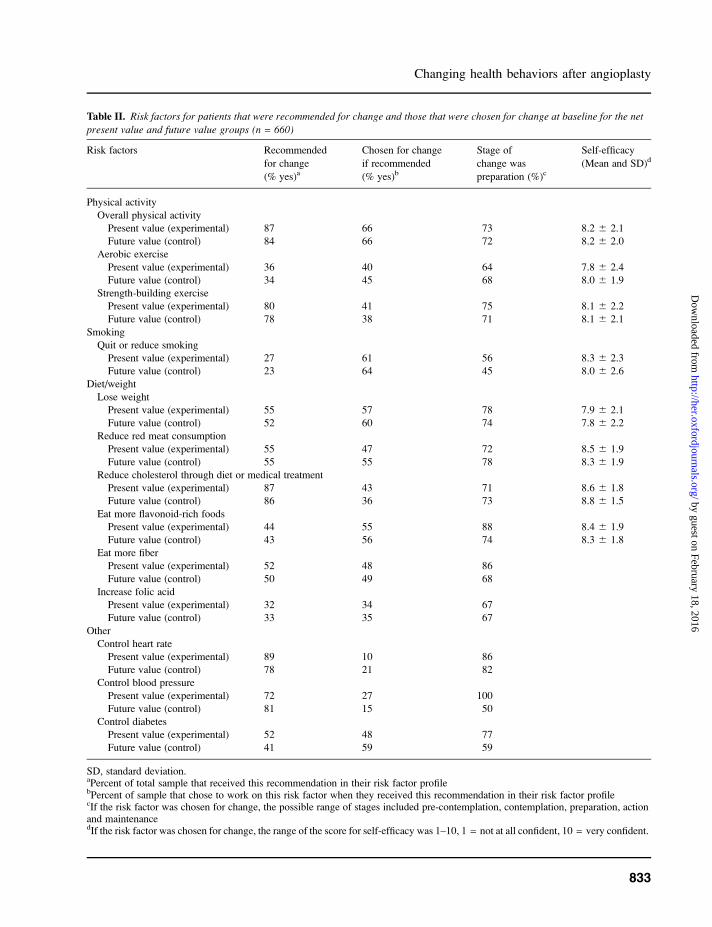
Table II. Risk factors for patients that were recommended for change and those that were chosen for change at baseline for the net
present value and future value groups (n = 660)
Risk factors Recommended
for change
(% yes)a
Chosen for change
if recommended
(% yes)b
Stage of
change was
preparation (%)c
Self-efficacy
(Mean and SD)d
Physical activity
Overall physical activity
Present value (experimental) 87 66 73 8.2 6 2.1
Future value (control) 84 66 72 8.2 6 2.0
Aerobic exercise
Present value (experimental) 36 40 64 7.8 6 2.4
Future value (control) 34 45 68 8.0 6 1.9
Strength-building exercise
Present value (experimental) 80 41 75 8.1 6 2.2
Future value (control) 78 38 71 8.1 6 2.1
Smoking
Quit or reduce smoking
Present value (experimental) 27 61 56 8.3 6 2.3
Future value (control) 23 64 45 8.0 6 2.6
Diet/weight
Lose weight
Present value (experimental) 55 57 78 7.9 6 2.1
Future value (control) 52 60 74 7.8 6 2.2
Reduce red meat consumption
Present value (experimental) 55 47 72 8.5 6 1.9
Future value (control) 55 55 78 8.3 6 1.9
Reduce cholesterol through diet or medical treatment
Present value (experimental) 87 43 71 8.6 6 1.8
Future value (control) 86 36 73 8.8 6 1.5
Eat more flavonoid-rich foods
Present value (experimental) 44 55 88 8.4 6 1.9
Future value (control) 43 56 74 8.3 6 1.8
Eat more fiber
Present value (experimental) 52 48 86
Future value (control) 50 49 68
Increase folic acid
Present value (experimental) 32 34 67
Future value (control) 33 35 67
Other
Control heart rate
Present value (experimental) 89 10 86
Future value (control) 78 21 82
Control blood pressure
Present value (experimental) 72 27 100
Future value (control) 81 15 50
Control diabetes
Present value (experimental) 52 48 77
Future value (control) 41 59 59
SD, standard deviation.aPercent of total sample that received this recommendation in their risk factor profilebPercent of sample that chose to work on this risk factor when they received this recommendation in their risk factor profilecIf the risk factor was chosen for change, the possible range of stages included pre-contemplation, contemplation, preparation, actionand maintenancedIf the risk factor was chosen for change, the range of the score for self-efficacy was 1–10, 1 = not at all confident, 10 = very confident.
Changing health behaviors after angioplasty
833
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

Overall patterns of behavior change
At baseline, patients chose an average of 2.8 risk
factors for change. This increased to a total of 5.1
over the course of the 2-year follow-up interval.
Table III shows the percentage of risk factors cho-
sen for change at any follow-up compared with
those chosen at baseline for both groups. Also
shown is the percent of patients who achieved ac-
tion or maintenance on any behavior at any time
point compared with action or maintenance at the
last assessment for the behavior. Over the period of
follow-up, patients in the net present value group
reached action on 1.5 risk factors, identical to the
rates of action in the future value group. On aver-
age, patients in both groups were able to maintain
action at the last assessment on 1.1 risk factors,
most often physical activity, weight reduction or
lowering cholesterol. Overall, 37% of patients
made no health behavior changes, 34% changed
one health behavior and 29% changed two or more
health behaviors.
Main trial outcomes
In total, we obtained major trial outcomes at the 2-
year follow-up on 622 of the 660 patients (94%)
enrolled in the study (Fig. 1). Of the 622 patients
who completed a 2-year follow-up, 6 patients had
died before the end of the study. Thirty-eight
patients were lost to follow-up at 24 months, though
six of these patients had outcomes prior to loss to
follow-up.
At the 2-year follow-up, there was no difference
in the principal outcome of the trial or in the com-
bined rates of death, stroke, myocardial infarction,
Class II–IV angina and severe ischemia on non-in-
vasive testing by randomization group. The differ-
ence in outcome rate between the two groups was
not statistically significant, assessed with a test for
difference in proportions P = 0.23; with a 95%
confidence interval for the difference of the net
present value percentage minus the future value
percentage of �13 to 2.9%. Using logistic regres-
sion to control for baseline and demographic vari-
ables such as sex, age, comorbidity score and
clinical status (ejection fraction, etc.) did not
change the results: there was no difference between
the net present value and future value groups. This
was not unexpected as the two groups were so
closely matched (Table I). Table IV shows that
the rates of each outcome were similar in both
groups, and the overall rate of combined outcomes
was 39.1% in the net present value group and
34.2% in the future value group.
When we analyzed all patients regardless of ran-
domization group, the greater the number of health
behaviors successfully changed, the less likely it
was that an adverse event would occur for an in-
dividual patient.
Discussion
Cardiac rehabilitation following coronary revascu-
larization seeks to assist patients who have under-
gone PTCA with necessary lifestyle changes.
Recent American and European studies [29–34]
of cardiac rehabilitation that includes comprehen-
sive lifestyle modification have shown promise in
reducing and even reversing coronary artery dis-
ease. Early studies by Ornish et al. [29] and Haskell
et al. [30]demonstrated that a program of intensive
multifactor risk reduction reduced luminal narrow-
ing in coronary arteries of men and women with
coronary artery disease. In addition, those who
made changes in lifestyle and took lipid-lowering
medication over a 4-year period were found to have
decreased rates of hospitalization for cardiac-
related clinical events [30]. In a later study, Ornish
et al. [31] showed that an intensive lifestyle modi-
fication program of dietary fat restriction, stress
management, exercise, smoking cessation and
group psychosocial support over a 5-year period
could reduce coronary atherosclerosis without the
use of lipid-lowering drugs. Koertge et al. [32]
demonstrated that a multicomponent lifestyle
change program for diet, exercise, stress manage-
ment and social support can produce significant
improvements in diet, exercise and stress manage-
ment practices, which can be maintained over a
12-month period. In another study, Pasquali et al.[33] evaluated the impact of cardiac rehabilitation
M. E. Charlson et al.
834
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

Table III Behaviors chosen for change at baseline or at any time, and whether or not the patients achieved action or maintenance in
both the net present value and future value groups (n = 660)
Risk factors Chosen for
change at
baseline (%)
Behavior
chosen for
change at
any time (%)
Achieved action
or maintenance
of behavior at
any point (%)
Action or
maintenance of
behavior at last
assessment (%)
Physical activity
Overall physical activity
Present value (experimental) 56.8 83.6 38.6 21.3
Future value (control) 55.2 83.7 31.4 20.9
Aerobic exercise
Present value (experimental) 14.2 23.1 1.8 1.2
Future value (control) 15.1 26.0 3.0 2.4
Strength-building exercise
Present value (experimental) 32.9 65.1 7.3 4.3
Future value (control) 29.8 66.5 7.9 3.9
Smoking
Quit or reduce smoking
Present value (experimental) 16.3 20.7 12.8 11.6
Future value (control) 14.9 18.7 14.8 11.8
Diet/weight
Weight loss
Present value (experimental) 31.1 53.2 27.7 15.2
Future value (control) 31.3 54.7 29.9 20.9
Reduce red meat
Present value (experimental) 25.9 38 5.2 4.3
Future value (control) 30.3 43.8 6.3 4.5
Reduce cholesterol through diet or medical treatment
Present value (experimental) 36.8 61.4 25.8 17.3
Future value (control) 31.3 52.3 22.9 15.4
Eat more flavonoid-rich foods
Present value (experimental) 23.9 42 5.5 3.9
Future value (control) 24.3 47.4 6 3.6
Eat more fiber
Present value (experimental) 12.1 27.7 3.7 3.3
Future value (control) 13.4 29.3 4.5 3.9
Increase folic acid
Present value (experimental) 10.9 33.4 3.3 1.8
Future value (control) 11.9 32.3 3.0 2.7
Other
Control blood pressure
Present value (experimental) 16.0 32.5 17.6 10.6
Future value (control) 11.6 34.7 19.9 15.7
Control heart rate
Present value (experimental) 1.8 10.3 1.2 0.9
Future value (control) 4.9 14.5 2.4 0.9
Control diabetes
Present value (experimental) 3.9 8.5 5.2 4.6
Future value (control) 5.2 9.9 6.3 5.4
Changing health behaviors after angioplasty
835
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

on functional outcomes among patients who had
been revascularized and found significant improve-
ments in physical functioning and secondary pre-
ventive behaviors at 6 months, particularly among
men; similar findings have been reported in a 2003
study by the Norwegian Vestfold Heartcare Study
Group [34]. While such studies show the promise of
cardiac rehabilitation, most patients with coronary
heart disease do not easily make necessary lifestyle
changes following angioplasty, and maintaining
such changes in the long term still remains chal-
lenging. Recent surveys conducted by EUROAS-
PIRE I and II Group [35] show that lifestyle change
among people with coronary artery disease is a con-
cern. Moreover, McDonald et al. [36] have reported
that even when effective in the long term, behav-
ioral interventions designed to improve adherence
with medication often involve complex and inten-
sive combinations of information and various other
behavioral techniques.
The objective of this randomized trial was to
evaluate whether feedback of individualized risk
profiles framed as the opportunity to reduce one’s
biologic age was more effective after 2 years in
reducing mortality and major cardiovascular mor-
bidity among patients who had just undergone
PTCA or coronary artery stenting, as compared
with the standard risk reduction approach. The
novel theoretical concept underlying this behavior
change intervention was framing risk reduction as
the opportunity to reduce one’s present biologic age
(net present value approach) contrasted with the
standard motivation to reduce risk, which was
framed as one’s opportunity to reduce future risk
(future value approach).
In addition to the concept of communicating risk
using net present value (biologic age), our interven-
tion incorporated intervention concepts from well-
established models of behavior change, including
those of individualized feedback [37, 38], stages
of change [13, 14] and self-efficacy [15, 16]. We
also scheduled frequent telephone follow-up by
trained research interventionists who provided
a minimal level of motivational support to all
patients throughout the study. Our overall goal in
the experimental arm of the trial was to convey to
patients the immediate health impact of specific
behaviors on their biologic age as well as the im-
mediate impact of changing them. We hypothesized
that armed with the value of how much biologic age
reduction one could achieve by, for example, stop-
ping smoking (a difficult behavior, but one that
yields greater immediate reduction in biologic age
than, for example, taking folate), the pattern in the
choice of behaviors to change would be different in
the two groups. Although patients most often chose
physical activity, weight reduction or lowering cho-
lesterol as the behaviors of interest for change, there
was no difference in pattern of choice in the two
groups. Moreover, there was no difference in the
main trial outcomes at the end of the study. For
example, the confidence intervals calculated for
the difference in net present and future value
showed that this difference would probably not be
different by >13% and that net present value could
not be better than future value by >2.9%, which is
only a negligible improvement.
Why were no differences in pattern of choice for
health behavior change or health outcome observed
at the end of the trial? There are several plausible
reasons—both theoretical and methodological—
why the intervention failed to produce the hypoth-
esized changes. First, patients in both arms of
the trial received multiple telephone contacts
throughout a 2-year follow-up period during which
they were interviewed about their health and given
motivational support. As a consequence, the at-
tention to the control group may have diluted any
Table IV. Major trial outcomes by intervention groups
Outcomes Net
present
value (%)
Future
value
(%)
P values
Mortality 4.1 4.4 0.83 (chi square)
Myocardial
infarction
4.2 4.4 0.8774 (chi square)
Class II–IV
angina
33.0 28.2 0.1787 (chi square)
Severe ischemia 1.0 1.6 0.7249 (Fisher’s exact test)
Stroke 1.3 0.6 0.4475 (Fisher’s exact test)
Total 39.1 34.2 0.23 (chi square)
M. E. Charlson et al.
836
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

potential differential impact of the presentation of
biologic age in the experimental net present value
group.
Second, our use of an understandable and per-
sonally relevant metric—biologic age—was
intended to be consistent with a rational model of
risk communication. We believed that the value of
communicating risk in terms of biologic age was in
revealing to the patient the increment of reduction
in biologic age that could be gained by changing
each individual risk factor. However, we did not
assess our study participants’ belief in the concept
prior to the study, so it is possible that patients in
the intervention group simply did not believe in the
concept of biologic age reduction or that they could
successfully reduce their biologic age by changing
their health behaviors (the outcome expectancy).
Moreover, many people do not understand concepts
of probabilistic thinking, survival or the distinctions
between harmful events occurring within popula-
tions and those within individuals or absolute
versus relative risk [39, 40]. For example, when at-
tempting to communicate the potential reduction in
risk for coronary artery disease that can be attrib-
uted to taking lipid-lowering drugs, the difference
between reporting relative or absolute risk is
likely to influence the perception of risk by the
patient [41].
Third, consistent with the Transtheoretical Model
of Stages of Change, telling people that they can
reduce their biologic age by changing their behavior
constitutes an intervention largely aimed at raising
risk awareness and increasing positive outcome
expectancies. However, in the context of most theo-
ries of health behavior change, risk awareness and
outcome expectancies are typically specified as pre-
dictors of the non-action phases or behavioral inten-
tions. Thus, because of the ‘intention-behavior-gap’
that has been observed in previous research [42],
targeting such cognitive factors alone is not suffi-
cient for achieving behavior change.
Fourth, had we assessed potential mediating var-
iables such as risk awareness and outcome expec-
tancies, both of which theoretically might have
been influenced by our intervention, we may have
been able to gain additional insight into why our
intervention did not work and why [43]. For exam-
ple, it is possible that our intervention was not ef-
fective in influencing critical mediating variables or
that our intervention ‘did’ influence important medi-
ators that we did not assess, but, although doing so,
did not make any difference in the main outcomes.
Finally, our study was not only aimed at reducing
those behavioral risk factors that were potentially
modifiable but also showing an improvement in
clinical outcomes. Even though patients may rea-
sonably be expected to initiate behavior changes,
maintaining such changes over a 2-year period of
time is difficult without an intensive behavioral in-
tervention that was beyond our interventional at-
tempt to motivate patients through a novel risk
communication message. It is possible that we
might have observed the hypothesized difference
between the two groups had we designed the in-
tervention for a shorter time period. Moreover, the
dose-response rate of health behavior change and
clinical outcomes needs to be considered. Although
people might be able to increase their physical activ-
ity from 0 to 1 time a week, this might not be suffi-
cient to influence the clinical outcomes we studied.
While these results are disappointing, identifying
an effective means of motivating and supporting
behavioral changes in patients with coronary artery
disease who have undergone PTCA remains a chal-
lenge. Although the communication of risk to such
patients is of great interest, communicating risk
alone may not be sufficient to stimulate the neces-
sary behavior change in the face of treatment that
produces such dramatic results in the relief of
symptoms. Because patients undergoing PTCA
and stenting do get dramatic symptomatic relief
it is not surprising that patients—and the doctors
who perform such procedures—view the treatment
as a veritable magic bullet. In light of this, perhaps
the interventional cardiologist needs to reinforce
both the importance and urgency of behavioral
change rather than telling the patient that the prob-
lem ‘has been fixed’. To do otherwise may leave the
patient with a false sense of cure for the underlying
causes of a disease that invariably requires persis-
tence at changing behavior if the benefits of PTCA
are to be maintained over time.
Changing health behaviors after angioplasty
837
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

Funding
National Heart, Lung, and Blood Institute (R01
HL62161091).
Acknowledgements
A research version of the RealAge software was
made available to the investigators, without charge,
by RealAge. We thank Paula McKinley and Can-
dace Young for their contributions in the early
phases of the study and the anonymous reviewers
for their insightful comments and useful sugges-
tions for revision.
Conflict of interest statement
None declared.
References
1. Cavender JB, Rogers WJ, Fisher LD et al. Effects of smok-
ing on survival and morbidity in patients randomized to
medical or surgical therapy in the Coronary Artery Surgery
Study (CASS): 10-year follow-up. CASS Investigators.
J Am Coll Cardiol 1992; 20: 287–94.2. Galan KM, Deligonul U, Kern MJ et al. Increased frequency
of restenosis in patients continuing to smoke cigarettes after
percutaneous transluminal coronary angioplasty. Am J Car-
diol 1988; 61: 260–3.3. Myler RK, Shaw RE, Stertzer SH et al. Recurrence after
coronary angioplasty. Cathet Cardiovasc Diagn 1987; 13:
77–86.4. Ramanathan KB, Vander Zwaag R, Maddock V et al. In-
teractive effects of age and other risk factors on long-term
survival after coronary artery surgery. J Am Coll Cardiol
1990; 15: 1493–9.5. Reis GJ, Kuntz RE, Silverman DI et al. Effects of serum
lipid levels on restenosis after coronary angioplasty. Am J
Cardiol 1991; 68: 1431–5.6. Watts GF, Lewis B, Brunt JN et al. Effects on coronary
artery disease of lipid-lowering diet, or diet plus cholestyr-
amine, in the St Thomas’ Atherosclerosis Regression Study
(STARS). Lancet 1992; 339: 563–9.7. Brown G, Albers JJ, Fisher LD et al. Regression of coronary
artery disease as a result of intensive lipid-lowering therapy
in mean with high levels of apolipoprotein B. N Engl J Med
1990; 323: 1289–98.
8. McKenna KT, Mass F, McEniery PT. Coronary risk factorstatus after percutaneous transluminal coronary angioplasty.Heart Lung 1995; 24: 207–12.
9. Gaw BL. Motivation to change life-style following PTCA.Dimens Crit Care Nurs 1992; 11: 68–74.
10. Gulanick M, Bliley A, Perino B et al. Recovery patterns andlifestyle changes after coronary angioplasty: the patient’sperspective. Heart Lung 1998; 27: 253–62.
11. Allegrante JP, Roizen MF. Can net-present value economictheory be used to explain and change health-related behav-iors? Health Educ Res 1988; 13: i–iv.
12. Charlson ME, Allegrante JP, McKinley PS et al. Improvinghealth behaviors and outcomes after angioplasty: using eco-nomic theory to inform intervention. Health Educ Res 2002;17: 606–18.
13. Prochaska JO, DiClemente CC, Norcross JC. In search ofhow people change. Applications to addictive behaviors. AmPsychol 1992; 47: 1102–14.
14. Prochaska J, Redding C, Evers K. The transtheorecticalmodel and states of change. Health Behavior and HealthEducation. New York, NY: Jossey Bass, 1997
15. Bandura A. Social Learning Theory. Englewood Cliffs, NJ:Prentice-Hall, 1977
16. Strecher V, DeVellis B, Becker M et al. The role of self-efficacy in achieving health behavior change. Health Educ Q1986; 13: 73–91.
17. Charlson ME, Pompei P, Ales KL et al. A new methodof classifying prognostic comorbidity in longitudinal stud-ies: development and validation. J Chronic Dis 1987; 40:373–83.
18. Rimm EB, Giovannucci EL, Stampfer MJ et al. Reproduc-ibility and validity of an expended self-administered semi-quantitative food frequency questionnaire among malehealth professionals. Am J Epidemiol 1992; 135: 1114–26discussion 1127–36.
19. Liu S, Stampfer M, Hu F et al. Whole-grain consumptionand risk of coronary heart disease: results from the Nurses’Health Study. Am J Clin Nutr 1999; 70: 412–9.
20. Liu S, Lee I, Ajani U et al. Intake of vegetables rich incarotenoids and risk of coronary heart disease in men: thePhysicians’ Health Study. Int Epidemiol Assoc 2001; 30:130–5.
21. Sesso H, Liu S, Gaziano J et al. Dietary lycopene, tomato-based food products and cardiovascular disease in women.J Nutr 2003; 133: 2336–41.
22. Taylor HL, Jacobs DR, Schucker B et al. A questionnaire forthe assessment of leisure time physical activities. J ChronicDis 1997; 31: 741–55.
23. Ni Mhurchu C, Margetts B, Speller V. Applying the stages-of-change model to dietary change. Nutr Rev 1997; 55: 10–6.
24. Jeffery R, French S, Rothman A. Stage of change as a pre-dictor of success in weight control in adult women. HealthPsychol 1999; 18: 543–6.
25. Costakis C, Dunnagan T, Haynes G. The relationship be-tween the stages of exercise adoption and other healthbehaviors. Am J Health Promot 1999; 14: 22–30.
26. Boyle R, O’Connor P, Pronk N et al. Stages of change forphysical activity, diet, and smoking among HMO memberswith chronic conditions. Am J Health Promot 1998; 12:170–5.
M. E. Charlson et al.
838
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from

27. Nigg C, Burbank P, Padula C et al. Stages of change acrossten health risk behaviors for older adults. Gerontologist1999; 39: 473–82.
28. Emmons KM, Rollnick S. Motivational interviewing inhealth care setting. Opportunities and limitations. Am J PrevMed 2001; 20: 68–74.
29. Ornish D, Brown SE, Scherwitz LW et al. Can lifestylechanges reverse coronary heart disease? The Lifestyle HeartTrial. Lancet 1990; 336: 129–33.
30. Haskell WL, Alderman EL, Fair JM et al. Effects of in-tensive multiple risk factor reduction on coronary athero-sclerosis and clinical cardiac events in men and womenwith coronary artery disease. The Stanford CoronaryRisk Intervention Project (SCRIP). Circulation 1994; 89:975–90.
31. Ornish D, Scherwitz L, Billings J et al. Intensive lifestylechanges for reversal of coronary heart disease. J Am MedAssoc 1998; 280: 2001–7.
32. Koertge J, Weidner G, Elliott-Eller M et al. Improvement inmedical risk factors and quality of life in woman and menwith coronary artery disease in the Multicenter LifestyleDemonstration Project. Am J Cardiol 2003; 91: 1316–22.
33. Pasquali S, Alexander K, Coombs L et al. Effect of cardiacrehabilitation on functional outcomes after coronary revas-cularization. Am Heart J 2003; 145: 445–51.
34. Group VHS. Influence on lifestyle measures and five-yearcoronary risk by a comprehensive lifestyle intervention pro-gramme in patients with coronary heart disease. Eur J Car-diovasc Prev Rehabil 2003; 10: 429–37.
35. Group, E.I.a.I. European Action on Secondary Prevention
by Intervention to Reduce Events. Clinical reality of coro-
nary prevention guidelines: a comparison of EUROSPIREI
and II in nine countries. Lancet 2001; 357: 995–1001.36. McDonald HP, Garg AX, Haynes RB. Interventions to en-
hance patient adherence to medication prescriptions: scien-
tific review. J Am Med Assoc 2002; 288: 2868–79.37. Champion V, Foster J, Menon U. Tailoring interventions for
health behavior change in breast cancer screening. CancerPract 1997; 5: 283–8.
38. Prochaska J, DiClemente C, Velicer W et al. Standardized,
individualized, interactive, and personalized self-help pro-
grams for smoking cessation. Health Psychol 1993; 12:
399–405.39. Alasewski A, Horlick-Jones T. How can doctors communi-
cate information about risk more effectively? Br Med J2003; 327: 729–31.
40. Alasewski A. A person-centered approach to communicat-
ing risk. PLoS Med 2005; 2: e41.41. Skolbekken J. Communicating the risk reduction achieved
by cholesterol reducing drugs. Br Med J 1998; 316: 1956–8.42. Sheeran P. Intention-behavior Relations. A Conceptual and
Empirical Review. Chichester, England, 2002, 1–36.43. Michie S, Abraham C. Interventions to change health behav-
iors: evidence based or evidence-inspired? Psychol Health2004; 19: 29–49.
Received on April 21, 2006; accepted on September 4, 2007
Changing health behaviors after angioplasty
839
by guest on February 18, 2016http://her.oxfordjournals.org/
Dow
nloaded from
Related Documents











