Update on Medications and Drug Interactions for the Pediatric Dentist Pamela J. Sims, Pharm.D., Ph. D. Professor Department of Pharmaceutical, Social and Administrative Sciences McWhorter School of Pharmacy Samford University and Adjunct Professor Department of Pediatric Dentistry University of Alabama School of Dentistry

Challenges of Treating Children Taking Psychotropic Drugs
Dec 05, 2014
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Update on Medications and Drug Interactions for the Pediatric Dentist
Pamela J. Sims, Pharm.D., Ph. D.Professor
Department of Pharmaceutical, Social and Administrative SciencesMcWhorter School of Pharmacy
Samford Universityand
Adjunct ProfessorDepartment of Pediatric Dentistry
University of Alabama School of Dentistry
Topics
Pharmacokinetic differences between children and adults
Preventing infection Managing behavior Interactions with local anesthesia Treating pain Treating nausea
Pediatric Pharmacokinetic Changes Absorption
– increased pH– Variable motility– Frequent presence of food and/or milk– Affects rate and extent
Distribution
Body composition– Primarily lean body mass– Increased V of water soluble drugs
• increased LD on mg/kg basis
– Decreased V of fat soluble drugs• decreased LD on mg/kg basis
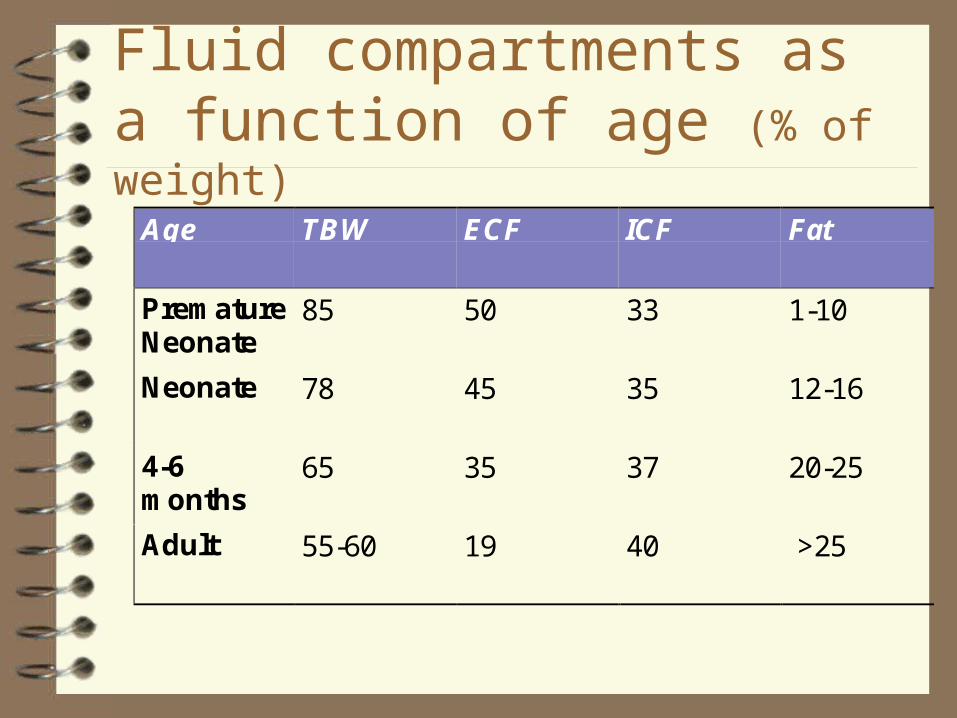
Fluid compartments as a function of age (% of weight)
Age TBW ECF ICF Fat
PrematureNeonate
85 50 33 1-10
Neonate 78 45 35 12-16
4-6months
65 35 37 20-25
Adult 55-60 19 40 >25
Distribution
Altered Protein Binding– Decreased plasma protein concentrations– Lower binding capacity– Decreased affinity

Comparative protein binding of certain drugs
Drug % PB in newborn % PB in adult
Acetaminophen 37 48
Diazepam 84 99
Morphine 46 66
Phenobarbital 32 51
Phenytoin 80 90
Theophylline 36 56
Metabolism
Phase I– Alternative pathways
– Develops slowly• concentration same,
activity reduced
– Affected by diet and drugs
• Inhibitors
• Inducers
Phase II– Glucuronidation
slowest to develop• 3-4 years of age
Excretion
Glomerular Filtration– Neonate
• RBF 5-6% of CO
• 30% of adult
Tubular Secretion and Reabsorption– decreased RBF
– Small, undeveloped tubules
Creatinine not as helpful a predictor of renal function as in adults– still one way of
monitoring nephrotoxic drugs
Preventing Infection
Prophylaxis against endocarditis Prophylaxis for joint replacement patients Prophylaxis for solid organ transplant patients Prophylaxis for immunocompromised patients
– Rheumatoid arthritis
– Type I diabetes
– Lupus
– Oncology patients
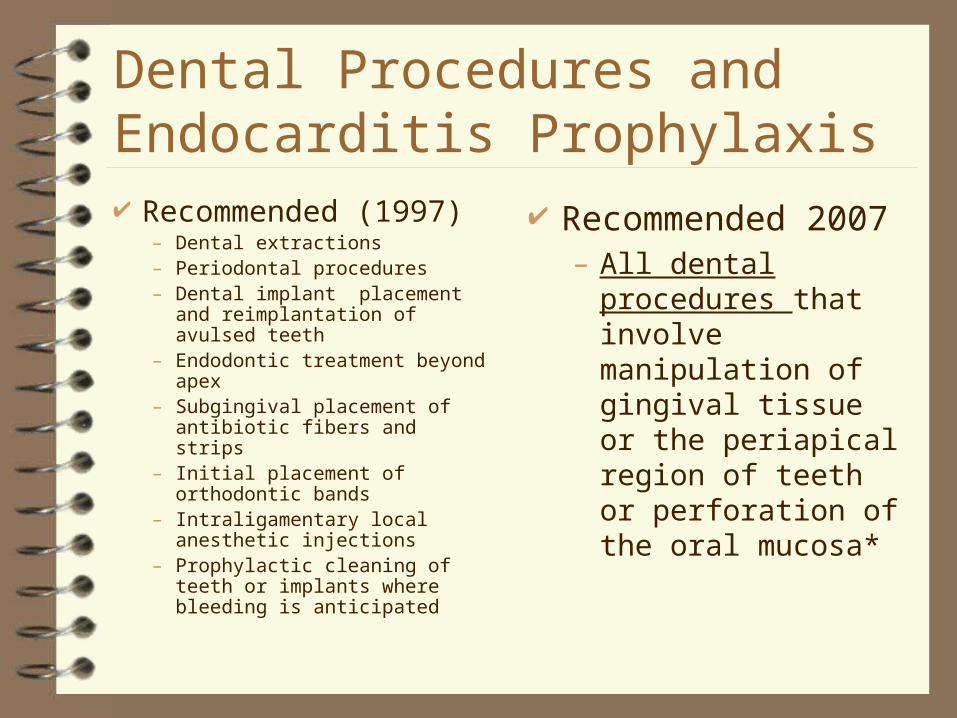
Dental Procedures and Endocarditis Prophylaxis Recommended (1997)
– Dental extractions – Periodontal procedures– Dental implant placement and
reimplantation of avulsed teeth– Endodontic treatment beyond apex– Subgingival placement of
antibiotic fibers and strips– Initial placement of orthodontic
bands– Intraligamentary local anesthetic
injections– Prophylactic cleaning of teeth or
implants where bleeding is anticipated
Recommended 2007– All dental procedures
that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa*

Dental Procedures and Endocarditis Prophylaxis Not Recommended (1997)
– Restorative dentistry– Nonintraligamentary local anesthetic
inj.– Post placement and buildup intracanal
endodontic tx.– Placement of rubber dams– Postoperative suture removal– Placement of removable prosthodontic
or orthodontic appliances– Taking of oral impressions– Fluoride treatments– Taking of oral radiographs– Orthodontic appliance adjustment– Shedding of primary teeth
*Not Recommended 2007– Routine anesthetic injections
through noninfected tissue– Taking dental radiographs– Placement of removable
prosthodontic or orthodontic appliances
– Adjustment of orthodontic appliances
– Placement of orthodontic brackets
– Shedding of deciduous teeth– Bleeding from trauma to the
lips or oral mucosa
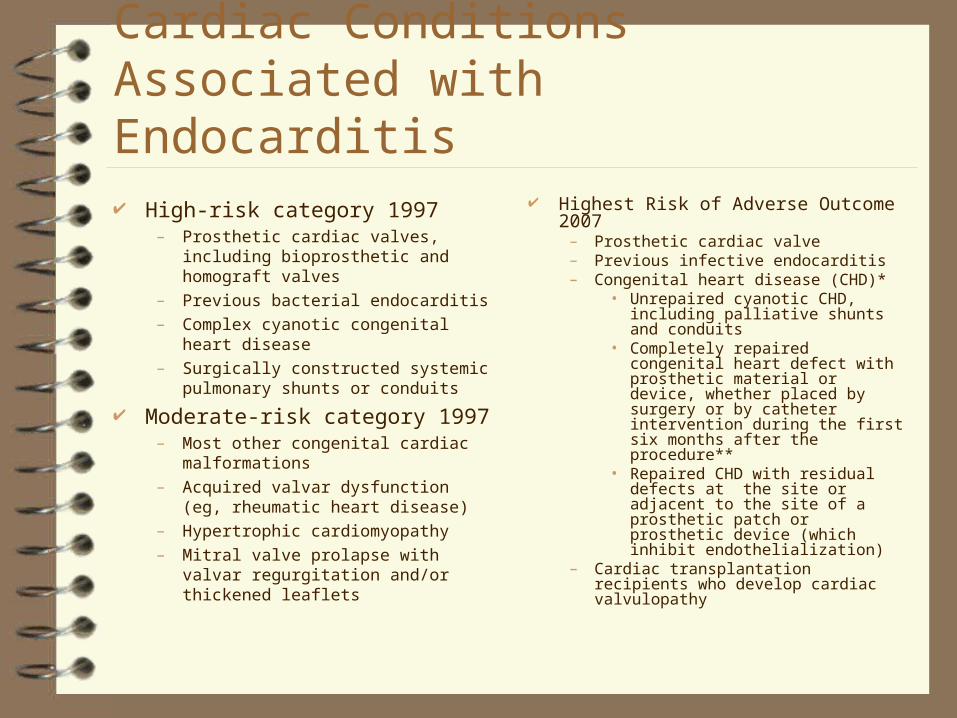
Cardiac Conditions Associated with Endocarditis High-risk category 1997
– Prosthetic cardiac valves, including bioprosthetic and homograft valves
– Previous bacterial endocarditis
– Complex cyanotic congenital heart disease
– Surgically constructed systemic pulmonary shunts or conduits
Moderate-risk category 1997– Most other congenital cardiac
malformations
– Acquired valvar dysfunction (eg, rheumatic heart disease)
– Hypertrophic cardiomyopathy
– Mitral valve prolapse with valvar regurgitation and/or thickened leaflets
Highest Risk of Adverse Outcome 2007– Prosthetic cardiac valve– Previous infective endocarditis– Congenital heart disease (CHD)*
• Unrepaired cyanotic CHD, including palliative shunts and conduits
• Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention during the first six months after the procedure**
• Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization)
– Cardiac transplantation recipients who develop cardiac valvulopathy

Cardiac Conditions for which Endocarditis Prophylaxis Not Recommended
Negligible-risk category (no greater risk than the general population) (1997)
– Isolated secundum atrial septal defect
– Surgical repair of atrial septal defect, ventricular septal defect, or patent ductus arteriosus (without residua beyond 6 mo)
– Previous coronary artery bypass graft surgery
– Mitral valve prolapse without valvar regurgitation
– Physiologic, functional., or innocent heart murmurs
– Previous Kawasaki disease without valvar dysfunction
– Previous rheumatic fever without valvar dysfunction
– Cardiac pacemakers and implanted defibrillators
2007– *Except for the conditions
listed, antibiotic prophylaxis is not longer recommended for any other form of CHD
– **Prophylaxis is recommended because endothelialization of prosthetic material occurs within 6 months after the procedure
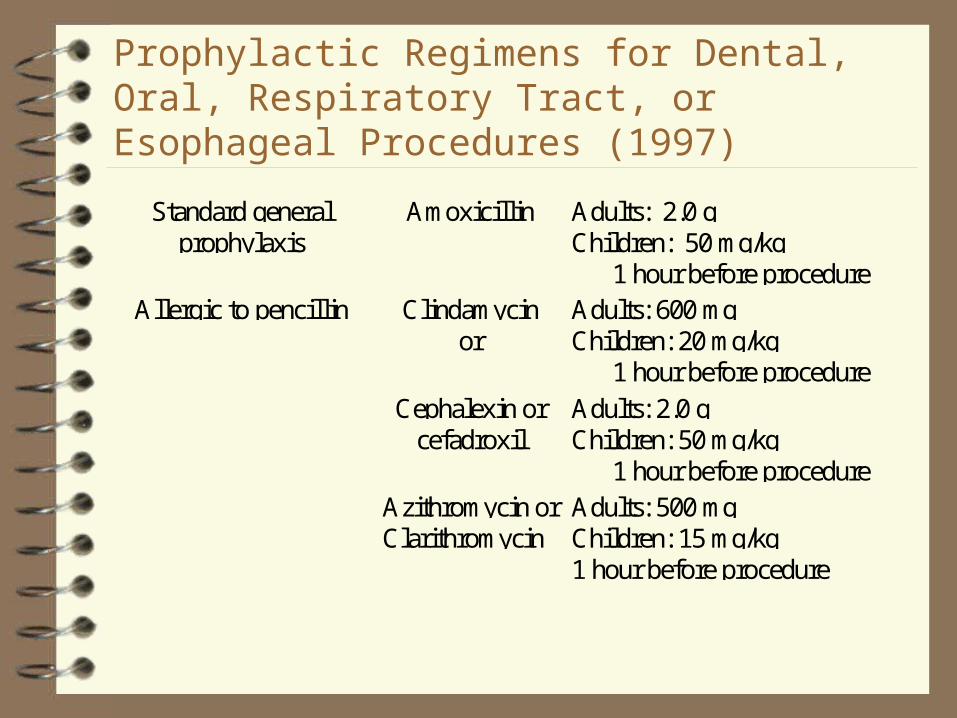
Prophylactic Regimens for Dental, Oral, Respiratory Tract, or Esophageal Procedures (1997)
Standard generalprophylaxis
Amoxicillin Adults: 2.0 gChildren: 50 mg/kg
1 hour before procedureAllergic to pencillin Clindamycin
orAdults: 600 mgChildren: 20 mg/kg
1 hour before procedure
Cephalexin orcefadroxil
Adults: 2.0 gChildren: 50 mg/kg
1 hour before procedureAzithromycin orClarithromycin
Adults: 500 mgChildren: 15 mg/kg1 hour before procedure
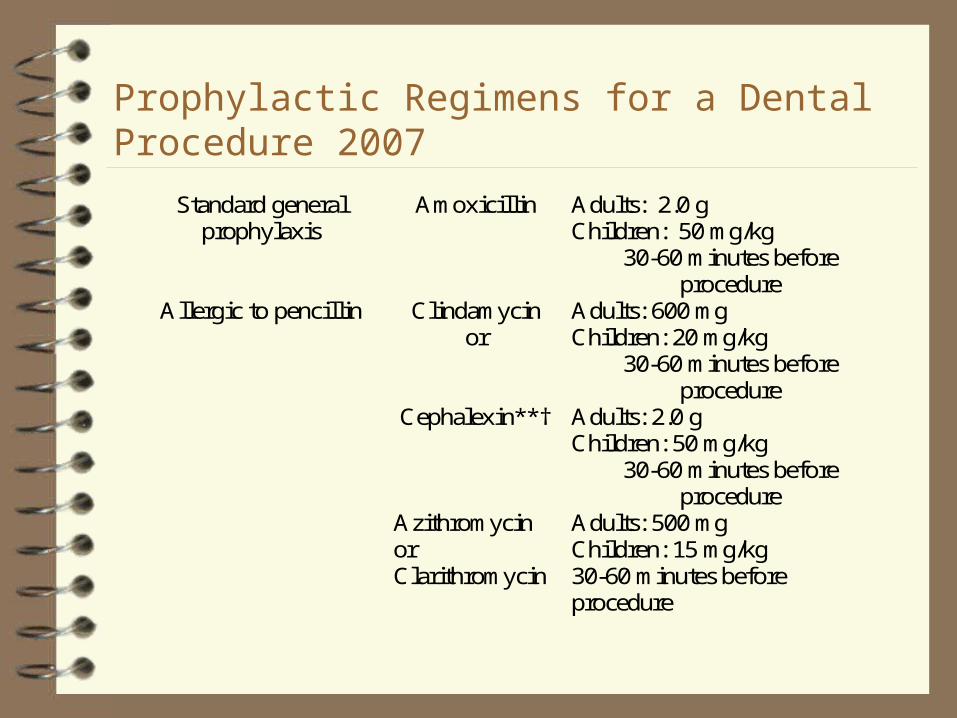
Prophylactic Regimens for a Dental Procedure 2007
Standard general prophylaxis
Amoxicillin Adults: 2.0 g Children: 50 mg/kg
30-60 minutes before procedure
Allergic to pencillin Clindamycin or
Adults: 600 mg Children: 20 mg/kg
30-60 minutes before procedure
Cephalexin**† Adults: 2.0 g Children: 50 mg/kg
30-60 minutes before procedure
Azithromycin or Clarithromycin
Adults: 500 mg Children: 15 mg/kg 30-60 minutes before procedure

Amino-penicillinsBroader Spectrum
Ampicillin Amoxicillin
– 125, 200, 250, 400 mg chewable tablets
– 250, 500 mg capsules– 500, 875 mg filmcoated
tablet– 125mg/5cc, 200 mg/5cc ,
250 mg/5cc, 400 mg /5cc suspension
– 50 mg/ml drop Bacampicillin
(Spectrobid)
Gram + and some Gram - coverage
More stable in GI tract Amoxicillin
– May be taken with food, milk or juice
– Food may delay peak concentrations
Cephalosporins
**or other first or second generation oral cephalosporin in equivalent adult or pediatric dosage.
†Cephalosporins should not be used in an individual with a history of anaphylaxis, angioedema, or urticaria with penicillins or ampicillin
First Generation CephalosporinsGood Gram+, Moderate Gram -
Parenteral: Cephalothin, Cefazolin, Cephapirin, Cephradine
Oral: Cephalexin (Keflex, Keftab), Cephradine (Anspor, Velosef, Eskacef), Cefadroxil (Duricef, Ultracef)
Similar spectrum to ampicillin and amoxicillin
Not affected by food More slowly absorbed in
children Higher bone penetration
than penicillins
Oral First Generation Cephalosporins Cephalexin
Monohydrate (Keflex)– 250, 500 mg capsule
– 250,500 mg tablet
– 125mg/5cc, 250 mg/5cc oral susp
Cephalexin HCl Monohydrate (Keftab)– 250, 500 mg tablet
Cephradine (Anspor, Velosef, Eskacef)– 250, 500 mg capsule
– 250 mg/5cc oral susp
Cefadroxil (Duricef)– 500 mg capsule
– 1 g tablet
– 250 mg/5cc, 500 mg/5cc oral susp
Second Generation CephalosporinsIncreased activity against Gram-
Parenteral: Cefamandole, Cefmetazole, Cefonicid, Cefotetan, Cefoxitin, Cefuroxime
Oral: Cefaclor(Ceclor, Ceclor CD), Cefprozil(Cefzil), Cefuroxime Axetil(Ceftin), Loracarbef(Lorabid)
Oral Second Generation Cephalosporins Cefaclor (Ceclor)
– 250, 500 mg capsules– 125/5, 187/5, 250/5
and 375/5 susp and chewables
– 20-40 mg/kg/day Cefaclor (Ceclor CD)
– 375, 500 mg extended release tablets
– 375-500 mg q 12 h
Cefprozil (Cefzil)– 250,500 mg tablets
– 125,250/5cc susp
– 250-500 mg q 12 h
– Children: 7.5 - 10 mg/kg q 12 h
Cefuroxime axetil (Ceftin)– 125, 250, 500 mg tablets
– 125/5cc susp
– 125-500 mg bid
– Children: 125-250 mg bid

Drug-related Concerns of Penicillin and Cephalosporin Antibiotics
Allergy– Cross-sensitivity between penicillins and cephalosporins. If a
person is truly allergic to penicillin, 10-25% patients will be allergic to cephalosporins. If a person is allergic to cephalosporins, the patient will generally be allergic to penicillins.
Increased bleeding in patients taking warfarin (Coumadin)– Antibiotics can decrease local flora responsible for
synthesis of Vitamin K (Vitamin K is the antagonist to warfarin and warfarin exerts its anticoagulant effects by inhibition of Vitamin K dependent clotting factors)

Drug-related Concerns of Penicillin Antibiotics Decreased efficacy of oral contraceptives
– Today’s low dose BCP’s require endogenous GI flora to conjugate hormone to allow absorption. If bacteria are absent, hormone which prevent egg implantation will be absent. Patients utilizing oral contraceptive agents should use another form of BC during the entire “cycle” in which antibiotics were administered.
Macrolides Azithromycin (Zithromax)
– 250 mg, Z-pak (250 mg), 500, Tri-pak (500 mg) 600 mg tablet
– 100 mg/5cc, 200 mg/5cc susp
– 1 g susp
Clarithromycin (Biaxin)– 250, 500 mg tablet
– 125 mg/5cc, 250 mg/5cc susp
– 500 mg XL
Erythromycin
– Base (E-mycin, Ery-Tab, Ilotycin, PCE)
– Estolate (Ilosone)
– Ethylsuccinate (EES)
– Stearate (Erythrocin) Troleandomycin (Tao)
– 250 mg capsules
Drug-related Concerns of Macrolides Active Metabolite
– Clarithromycin
GI upset– Erythromycin
Hepatic Enzyme Inhibition– Erythromycin– Clarithromycin
Drug-related Concerns of Macrolides Hepatic Enzyme
Inhibition– Increases blood levels– Increases risk of toxicity– Decreases clearance
Cisapride (Propulcid) Phenytoin (Dilantin) Carbamazepine (Tegretol) Cyclosporine Warfarin (Coumadin) Corticosteroids Theophylline Benzodiazepines Digoxin

Lincosamides Lincomycin
(Lincocin)– 500 mg capsules
Clindamycin (Cleocin)– (HCl) 75, 150, 300 mg
capsules
– (Palmitate) 75mg/5cc solution
ADR– Pseudomembranous
Colitis (Clostridium difficile)
Patients at increased risk of hematogenous total joint infection
Immunocompromised/Immunosuppressed
– Inflammatory arthropathies, rheumatoid arthritis, systemic lupus
– disease, drug or radiation-induced
Insulin dependent diabetics
First 2 years post-replacement
Previous joint infections
Malnourishment Hemophilia
Higher Incidence of Bacteremic Dental Procedures Dental Extractions Periodontal
procedures Dental implant
placement and reimplantation of avulsed teeth
Endodontic beyond the apex
Initial orthodontic bands/not brackets
Intraligamentary local anesthetic injections
Prophylactic cleaning of teeth or implants where bleeding is anticipated
Suggested Prophylaxis Regimens Patients not allergic to
penicillin:– Cephalexin,
Cephradine or Amoxicillin
• 2 gm orally 1 hour prior to procedure
Patients allergic to penicillin:– Clindamycin 600 mg
orally 1 hour prior to the dental procedure.

Fen-Phen, Pondimin or Redux PatientsFenfluramine or dexfenfluramine w or w/o phentermine
If a patient needs to undergo a dental procedure for which the AHA recommends prophylaxis against endocarditis, patient needs an echo.
If no echo must prophylax
If valvar disease discovered, must prophylax

Oral Infections
Acute endodontic abscess– Augmentin– Clindamycin
Acute periodontal infections – Augmentin
Gingival abscess– Amoxicillin
ANUG– Metronidazole
Localized juvenile periodontitis– Doxycycline and scale and
root planing– Augmentin
• Can add metronidazole– Ciprofloxacin
Abscessed teeth to be extracted– Augmentin– Clindamycin– Ceftin
Chlorhexidine mouthwash

Antibiotics
Augmentin– Amoxicillin/clavulanic acid
– 20 – 40 mg/kg/day amoxicillin in divided doses q 8 h
– 20 – 45 mg/kg/day amoxicillin in divided doses q 12 h
– Use lowest doses of clavulanic acid
• GI ADE
For oral susp– For bid: 200/28.5, 400/57,
600/42.9
– 125/31.5, 250/62.5
Chewable– For bid: 200/28.5, 400/57
– 125/31.25, 250/62.5
Tablet– 250/125, 500/125
– For bid: 875/125

Tetracyclines Demeclocycline
(Declomycin)– 150 mg capsule– 150, 300 mg tablet
Doxycycline (Vibramycin)– 50,100 mg capsule,
tablet– 25 mg/5cc oral susp– 50 mg/5cc syrup
Minocycline (Minocin)– 50, 100 mg tablet,
capsule– 50 mg/5cc susp
Oxytetracycline– 250 mg capsule
Tetracycline– 100, 250, 500 mg capsule– 125 mg/5cc susp– 250, 500 mg tablet

Drug-related Concerns of Tetracyclines Bacteriostatic Photosensitivity Chelation with any di or trivalent cation
– antacids– mineral supplements (Ca, Fe, Mg)– Dairy products– Sucralfate (Carafate)– Stains teeth

Quinolones Ciprofloxacin (Cipro)
– 100, 250, 500, 750 mg tablet– 5, 10 g/100 mg susp– 20-30 mg/kg/day in two divided
doses Cinoxacin (Cinobac)
– 250, 500 mg capsules Enoxacin (Penetrex)
– 200, 400 mg tablet Gatifloxacin
– 20, 400 mg tablets Grepafloxacin (Raxar)
– 200 mg tablet Levafloxacin (Levaquin)
– 250, 500 mg tablet
Lomefloxacin (Maxaquin)– 400 mg tablet
Moxifloxacin– 400 mg tablets
Norfloxacin (Noroxin)– 400 mg tablet
Ofloxacin (Floxin)– 200, 300, 400 mg tablet
Sparfloxacin (Zagam)– 200 mg tablet
Trovafloxacin (Trovan)– 100, 200 mg tablets
Drug-related Concerns of Quinolones Primarily Gram - spectrum Resistance develops quickly All contraindicated in pregnant and nursing
women All cause photosensitivity
Metronidazole Enters cells which contain
nitroreductase, where its nitro group is reduced
Unstable intermediate compounds bind to DNA and inhibit synthesis causing cell death
Active against anaerobes and protozoa
Flagyl– Active against anaerobes and
protozoa
– 250, 500 mg tablet
– 750 mg extended release tablet
– 375 mg capsule
– Bacterial vaginosis• 500 mg bid for 7 days
• 2 g
– Giardiasis• 250 mg tid for 7 day
Drug-related Concerns of Metronidazole Increased
Metronidazole levels– Cimetidine
Disulfiram-like reaction– Ethanol
Acute psychosis or confusional state– Disulfiram
Hepatic Enzyme Inhibition– Anticoagulants
– Hydantoins
Decreased renal excretion– Lithium

Behavior Management
Antihistamines Anxiolytic Antihistamines Anxiolytic Benzodiazepines Sedative/Hypnotic Benzodiazepines Anesthetic Benzodiazepines

ADA Old Definitions Conscious Sedation
– A controlled, pharmacologically induced, minimally depressed level of consciousness that retains the patient’s ability to maintain a patent airway independently and continuously and respond appropriately to physical stimulation and/or verbal command.
– Drugs, dosages and techniques used should carry a margin of safety which is unlikely to render the child non-interactive and non-arousable.
Deep Sedation– A controlled, pharmacologically-induced state of depressed consciousness from
which the patient is not easily aroused which may be accompanied by a partial loss of protective reflexes, including the ability to maintain a patent airway independently and/or respond purposefully to physical stimulation or verbal commands.
General Anesthesia– A controlled, state of unconsciousness, accompanied by a partial or complete loss
of protective reflexes, including ability to independently maintain an airway or respond purposefully to physical stimulation or verbal command.

ADA New Definitions Minimal Sedation
– (Previously associated with anxiolysis and conscious sedation)– A minimally depressed level of consciousness that retains the patient’s
ability to independently and continuously maintain an airway and respond appropriately to physical stimulation or verbal command and that is produced by a pharmacological or non-pharmacological method or a combination thereof. Although cognitive function and coordination may be modestly impaired, ventilatory and cardiovascular functions are unaffected.
• Note: In accord with this particular definition, the drug(s) and/or techniques used should carry a margin of safety wide enough to render unintended loss of consciousness unlikely. Further, patients whose only response is reflex withdrawal from repeated painful stimuli would not be considered to be in a state of minimal sedation.
• When the intent is minimal sedation for adults, the appropriate dosing of enteral drugs is not more than the maximum recommended dose of a single drug that can be prescribed for unmonitored home use.

ADA New Definitions
Moderate sedation– A drug-induced depression of consciousness during which patients
respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Cardiovascular function is usually maintained.
• Note: In accord with this particular definition, the drugs and/or techniques used should carry a margin of safety wide enough to render unintended loss of consciousness unlikely. Repeated dosing of an agent before the effects of previous dosing can be fully appreciated may result in a greater alteration of the state of consciousness than is the intent of the dentist. Further, a patient whose only response is reflex withdrawal from a painful stimulus is not considered to be in a state of moderate sedation.
ADA New Definitions Deep sedation
– A drug-induced depression of consciousness during which patients cannot be easily aroused but respond purposefully following repeated or painful stimulation. The ability to independently maintain ventilatory function may be impaired. Patients may require assistance in maintaining a patent airway, and spontaneous ventilation may be inadequate. Cardiovascular function is usually maintained.
General anesthesia– A drug-induced loss of consciousness during which patients are not
arousable, even by painful stimulation. The ability to independently maintain ventilatory function is often impaired. Patients often require assistance in maintaining a patent airway, and positive pressure ventilation may be required because of depressed spontaneous ventilation or drug-induced depression of neuromuscular function. Cardiovascular function may be impaired.

ADA New Definitions Note: Because sedation and general anesthesia are a continuum, it is not
always possible to predict how and individual patient will respond. Hence, practitioners intending to produce a given level of sedation would be able to diagnose and manage the physiologic consequences (rescue) for patients whose level of sedation becomes deeper than initially intended.
For all levels of sedation, the practitioner must have the training, skills and equipment to identify and manage such an occurrence until either assistance arrive (emergency medical service) or the patient returns to the intended level of sedation without airway or cardiovascular complications.
All areas in which local anesthesia and sedation are being used must be properly equipped with suction, physiologic monitoring equipment, a positive pressure oxygen delivery system suitable for the patient being treated and emergency drugs. Protocols for the management of emergencies must be developed and training programs held at frequent intervals.

Levels of Sedation
Level 1 Level 2 Level 3 Level 4 Mild Sedation (Anxiolysis)
Interactive Non-Interactive Arousable with Mild/Moderate Stimulus
Non-Interactive Non-Arousable except with Intense Stimulus
Totally Awake Responds to verbal commands Eyes open or temporarily closed
Mimics Sleep Responds to physical stimuli May require airway re-adjustment
Depressed vitals in Sleep-like state Airway requires constant monitoring
ASA Physical Status Scale Class I Normal Healthy individual Class II Mild systemic disease
– (eg, controlled diabetes or hypertension) Class III Severe systemic disease that is not
incapacitating
– (eg, COPD, mental retardation, hemophilia) Class IV Incapacitating disease that is a constant
threat to life– (eg, unstable angina or renal failure)
Class V Moribund patient not expected to survive 24 hours
Class E Emergency
Considerations for the Pediatric Patient Patient’s age Level of cognitive and coping skills ASA Class
– I or II candidate for level 1,2, 3 or 4– III or IV should be treated in a hospital setting
Antihistamines Diphenhydramine
(Benadryl)– Dosage forms
• Capsules 25, 50 mg
• Elixir 12.5 mg/tsp
– Dose• 5 mg/kg/day
• <5 yo 12.5-25 mg
• >5 yo 25-50 mg
Advantages– drowsiness
– dry mouth
– low respiratory depression
– no dependence
Disadvantages– paradoxical excitement
Anxiolytic Antihistamines
Hydroxyzine– Atarax (HCl)
• tablets 10,25,50,100 mg
• syrup 2 mg/ml (10mg/tsp)
– Vistaril (Pamoate)• capsules 25,50,100 mg
• susp 5 mg/ml (25mg/tsp)
• Inj 25 mg/ml as HCl
Anxiety– 50 - 100 mg qid
– Children: 12.5 - 25 mg qid
Sedation– 50 - 100 mg
– Children: 0.6 mg/kg
Pre-operative adjunct– 50 - 100 mg
– Children: 1.1 mg/kg
Hydroxyzine
Advantages– Sedative– Dry mouth– H1 antagonist in GI tract– No dependence– Antagonizes vasopressor
effects of epinephrine– No respiratory depression
• May protect from respiratory depression of meperidine
– No effect on QT interval
Disadvantages– No IV dosage form

Benzodiazepines
Controlled substance– potential for abuse and
dependence
Anterograde amnesia Muscle relaxant Potentiated by enzyme
inhibitors
Reversal agent available– Flumazenil
(Romazicon)
Good margin of safety– Respiratory depression
– Reduce dose with opiates

Anxiolytic Benzodiazepines
Speed of Onset Elimination Half-life
Active Metabolites
Alprazolam (Xanax)
Intermediate 6.3-26.9 No
Chlordiazepoxide (Librium)
Intermediate 5-30 Yes
Clorazepate (Tranxene)
Fast 40-50 Yes
Diazepam (Valium)
Very Fast 20-80 Yes
Halazepam (Paxipam)
Slow 14 Yes
Lorazepam (Ativan)
Intermediate 10-20 No
Oxazepam (Serax)
Slow 5-20 No
Prazepam (Centrax)
nd 50-100 Yes
Anxiolytic Benzodiazepines Lorazepam
– Ativan• tablets 0.5,1,2 mg
– Lorazepam Intensol• conc. oral sol. 2 mg/ml,
30 ml dropper
– Adults:• 2-4 mg
• 0.5 - 1 mg tid
• increase dose as needed
– Pediatric dose:• 0.05 mg/kg
• Doses > 0.09 mg/kg produce inc. ataxia w/o inc. sedation
• Safety of oral lorazepam in children < 12 yo not established
Anxiolytic Benzodiazepines
Lorazepam– Ativan– Intermediate onset
– No active metabolites
– Short acting
• 10-20 hour half-life
– sublingual absorption more rapid than oral
Anxiolytic Benzodiazepines Diazepam
– Valium– 2,5,10 mg tablets
– 5 mg/5ml solution
– 5 mg/ml Intensol sol
– 5 mg/ml inj
– Adult:• 5-10 mg
– Pediatric:• 0.2-0.3 mg/kg 90
minutes prior to procedure
Anxiolytic Benzodiazepines
Diazepam– History of use in children
– Rapid onset
– Active metabolites• desmethyldiazepam
• temazepam
• oxazepam
– Long Acting• 20-80 hr half-life
Anesthetic Benzodiazepines Midazolam
– Versed
– 1 mg/ml inj
– 5 mg/ml inj
– 2 mg/ml syrup• peds 2-16 yo only
Adult– IM 0.07-0.08 mg/kg up to 1 hr
before procedure
– IV dilute 1mg/ml with NaCl or D5W and administer slowly
Pediatric:– IM 0.1-0.15 mg/kg, 30-60 min prior
– IV
• <5 yo:0.05-0.1 mg/kg
• 5-12 yo 0.025-0.05 mg/kg
• >12 yo 1-5 mg, titrate slowly over 10-20 min
– Oral
• 0.2-0.4 mg/kg, 30-45 min prior
– Rectal
• 0.3 mg/kg
– Nasal
• 0.2-0.3 mg/kg

Drug-related Effects of Benzodiazepines Additive effects with other CNS
depressants Amnesia Paradoxical reactions Flumazenil (Romazicon)
Benzodiazepine Antagonist– 0.01 mg/kg (max 0.2 mg) over 15 seconds, may
repeat after 45 seconds
Drug Interactions of Benzodiazepines Effect increased by other CNS depressants Effect increased by enzyme inhibitors
– Cimetidine (Tagamet), Macrolides (Erythromycin, Biaxin), Oral contraceptives, Disulfiram (Antabuse), Isoniazid
Effect decreased by enzyme inducers
– Rifampin, Smoking, Phenytoin Effect antagonized by CNS stimulants
– Theophylline
Sedative/Hypnotic
Chloral Hydrate (Noctec)
– 250, 500 mg capsules
– 250, 500 mg/5cc syrup
– Adults• Sedative 250 mg tid• Hypnotic 500-1000 mg 15-30 minutes before procedure
– Pediatric• Sedative 25 mg/kg/day up to 500 mg single dose• Hypnotic 50 mg/kg/day up to 1 g single dose
• Doses of 75 mg/kg uses for dental sedation with NO
Chloral Hydrate Good margin of safety Low respiratory
depression No anxiolytic
properties Agitation before
sedation and after
Controlled substance– abuse and dependence
No reversal agent

Interactions with Local Anesthesia
Patients treated for ADD/ADHD
Patients treated for narcolepsy
Patients treated for obesity Patients treated for
depression Patients treated for
enuresis
Stimulants Antidepressants Antipsychotics Beta-Blockers Monoamine Oxidase
Inhibitors (MAOIs)
Dental Issues
Local anesthesia– Contents of a Local Anesthetic Cartridge
• Local Anesthetic– Esters
– Amides
• Vasoconstrictor
• Preservative– Sodium Metabisulfite
• Sodium Chloride and Sterile Water
Systemic side effects
Local anesthetic– CNS excitation
• seizures
• depression
– CV excitation• arrhythmias
Vasoconstrictor– Increase heart rate
– Increase blood pressure
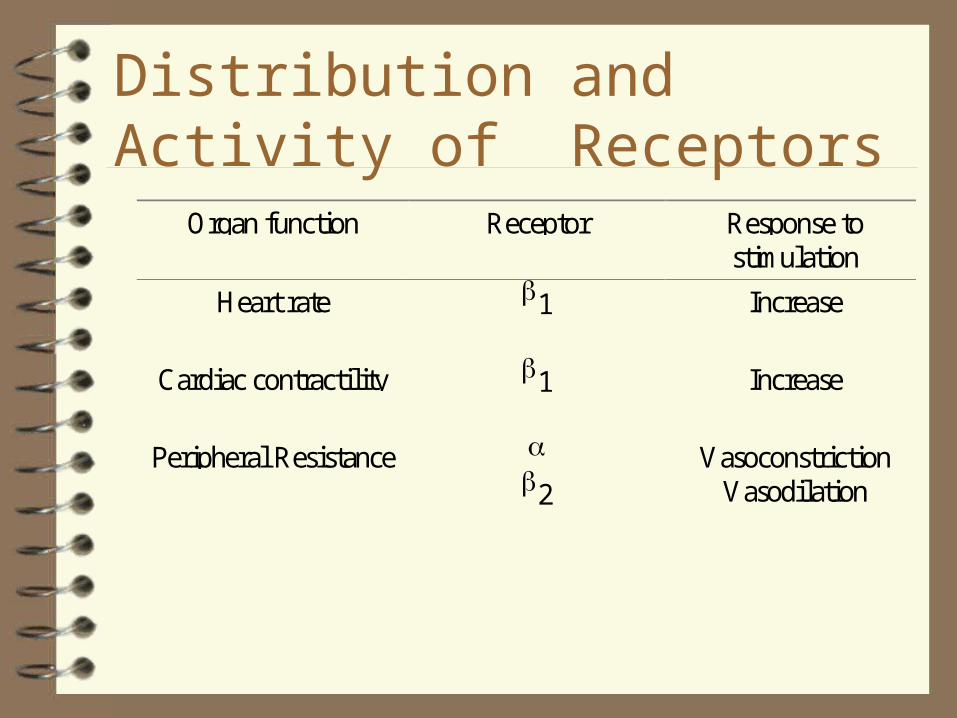
Distribution and Activity of Receptors
Organ function Receptor Response tostimulation
Heart rate 1 Increase
Cardiac contractility 1 Increase
Peripheral Resistance 2
VasoconstrictionVasodilation
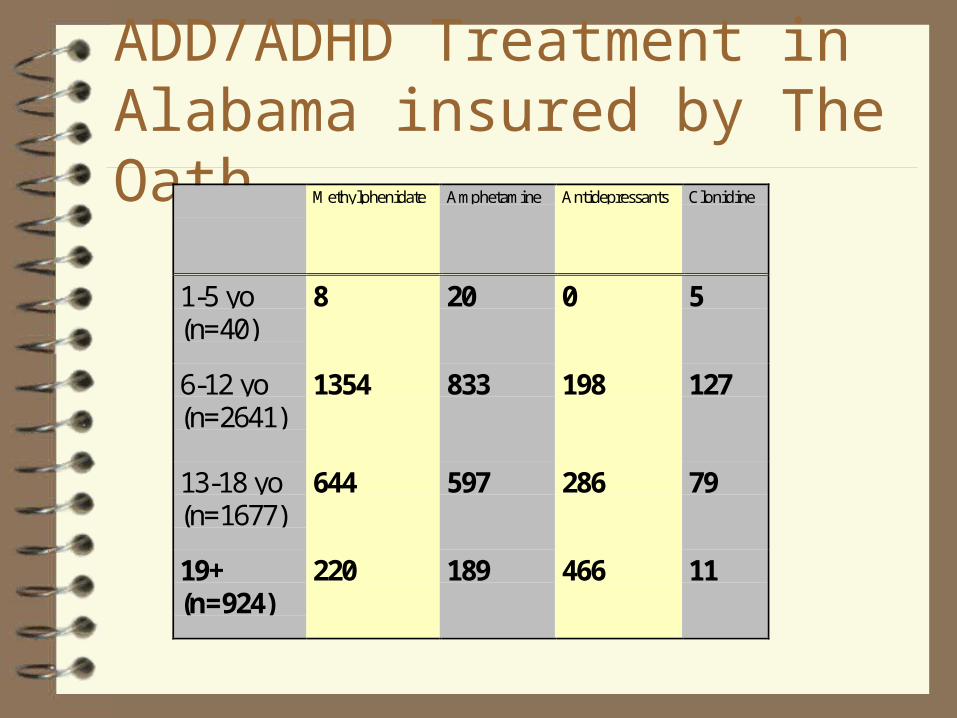
ADD/ADHD Treatment in Alabama insured by The Oath
Methylphenidate Amphetamine Antidepressants Clonidine
1-5 yo(n=40)
8 20 0 5
6-12 yo(n=2641)
1354 833 198 127
13-18 yo(n=1677)
644 597 286 79
19+(n=924)
220 189 466 11
Psychostimulants for ADD/ADHD and Narcolepsy Methylphenidate
– Standard methylphenidate
– Ritalin SR®
– Concerta®• Coated with immediate release • contains an osmotic pump
providing gradual release over 10 hours
• produces slightly ascending serum concentrations
• tablet remains intact and leaves GI tract as an empty shell
• take qd
Amphetamines– Dextroamphetamine
– Adderall®
– Dexedrine Spansules®
Pemoline (Cylert®)
Vasoconstrictor Interactions with CNS Stimulants
Additive CNS stimulation with other sympathomimetic agents
Decongestants Diet aids Psychostimulants
– Methylphenidate• Ritalin®• Concerta®
– Amphetamines• d-Amphetamine• Adderall®
Bronchodilators Albuterol® Theophylline
Antidepressants
ADD/ADHD– Atomoxetine (Strattera®)
Anxiety– Social Phobia– Panic Disorder– OCD
Depression Enuresis Sleep Disorders Premenstrual Dysphoric Disorder
Vasoconstrictor Interactions with Antidepressants Antidepressants
– Block reuptake of norepinephrine and/or serotonin
Interaction– Increased and prolonged
effects on receptors
Increased alpha and beta stimulation– increased heart rate
– increased cardiac contractility
– increased peripheral resistance
Interacting Antidepressants
Tricyclic Antidepressants Tertiary Amines
• Amitriptyline (Elavil)• Clomipramine (Anafranil)• Doxepin (Adapin, Sinequan)• Imipramine (Tofranil)• Trimipramine (Surmontil)
Secondary Amines• Amoxapine (Asendin)• Desipramine (Norpramin,
Pertofrane)• Maprotiline (Ludiomil)• Nortriptyline (Aventyl,
Pamelor)• Protriptyline (Vivactil)
Miscellaneous – Amoxapine (Asendin)– Venlaxafine (Effexor)– Mirtazapine (Remeron)
Selective norepinephrine reuptake inhibitors– Atomoxetine (Strattera)
Vasoconstrictor Interactionswith Antipsychotics and Antiemetics
blockade of alpha adrenergic receptors– orthostatic
hypertension
– reflex tachycardia
– potentiation of antihypertensives
predominance of beta adrenergic effects– increased heart rate
– increased cardiac contractility
– peripheral vasodilation

Interacting Antipsychotics and Antiemetics Phenothiazines
– Acetophenazine (Tindal)– Chlorpromazine (Thorazine)– Fluphenazine (Prolixin)– Mesoridazine (Serentil)– Perphenazine (Trilafon) – Prochlorperazine (Compazine) – Promazine (Sparine)– Promethazine (Phenergan)– Thioridazine (Mellaril)– Trifluoperazine (Stelazine)
Thiothixene (Navane) Haloperidol (Haldol) Clozapine (Clozaril) Loxapine (Loxitane) Molindone (Moban) Risperdal (Risperidone) Zyprexa (Olanzapine) Seroquel (Quetiapine)

Beta-adrenergic blockers
Hypertension Arrhythmias Mitral Valve Prolapse Migraine Performance anxiety
– Stage fright

Vasoconstrictor Interactions with Beta-adrenergic Antagonists
Blockade of beta 1 and beta 2 receptors
Causes unopposed alpha peripheral vasoconstriction
Initial hypertensive episode followed by bradycardia

Interacting Beta-adrenergic Antagonists
Selective beta 1 antagonists– Acebutolol (Sectral)
– Atenolol (Tenormin)
– Betaxolol (Kerlone)
– Bisoprolol (Zebeta)
– Metoprolol (Lopressor)
Non-selective beta antagonists– Carteolol (Cartrol)– Nadolol (Corgard)– Penbutolol (Levatol)– Pindolol (Visken)– Propranolol (Inderal)– Sotalol (Betapace)– Timolol (Blocadren)– Labetalol (Trandate,
Normodyne)

Monoamine Oxidase Inhibitors (MAOIs) Social Phobia Panic Disorder Depression
Monoamine Oxidase Inhibitors (MAOIs) Social Phobia Panic Disorder Depression Parkinsons
Antidepressants– Isocarboxazid (Marplan)– Phenelzine (Nardil)– Tranylcypromine (Parnate)– Selegiline (Emsam)
• Transdermal 6, 9, 12 mg/24h)
Antiparkinson– Selegiline
• Eldepryl 5 mg capsule• Carbex 5 mg tablet• Zelapar 1.25 mg orally
disintegrating tablet
Vasoconstrictors and MAOIs
MAOIs potentiate indirect or mixed-acting sympathomimetic substances– by inhibiting metabolism of
MAO B – severe headache,
hyperpyrexia, hypertension
Interaction with direct-acting agents is minimal– EMSAM inhibits
MAO A and therefore is contraindicated with epinephrine and levonordefrin

Sympathomimetic Agents
Direct acting-directly stimulates receptor– epinephrine
– norepinephrine
– levonordefrin
– isoproterenol
– dopamine
– methoxamine
– phenylephrine
Indirect-acting-releases norepi from nerve terminal– tyramine
– amphetamine
– methamphetamine
Mixed-acting-both direct and indirect actions– ephedrine
Treating Pain
Mild to moderate– Acetaminophen– Aspirin– NSAIDs
Moderate– Acetaminophen/Codeine
Moderate to severe– Acetaminophen/Hydrocodone– Acetaminophen/Oxycodone– Meperidine
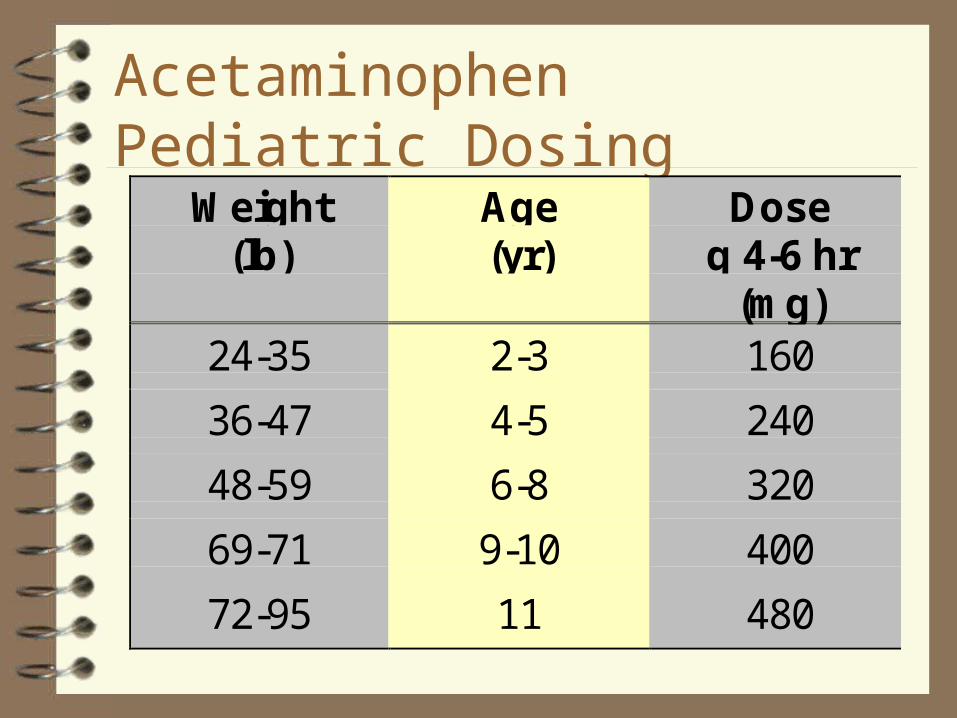
Acetaminophen Pediatric Dosing
Weight(lb)
Age(yr)
Doseq 4-6 hr
(mg)24-35 2-3 160
36-47 4-5 240
48-59 6-8 320
69-71 9-10 400
72-95 11 480
Acetaminophen
Not NSAID– not anti-inflammatory
– no cross-hypersensitivity
Pregnancy– generally safe
Lactation– generally safe
Central action on prostaglandins– no renal effects
• safest in pregnancy
• safest in renally compromised
– no GI effects
– no platelet effects• safest with
anticoagulants
AcetaminophenAdverse effects Hepatotoxicity
– overdose• 10-15 g
• children less susceptible
• chronic alcoholics more susceptible– not a contraindication
– Chronic toxicity• Adults 3 g per day

Aspirin Dosages in Children
Age(yrs)
Wt(lbs)
Dosage(mg q 4 h)
No. of 81 mgtabs q 4 h
No. of 325 mgtabsq 4 h
2-3 24-35 162 2 ½
4-5 36-47 243 3
6-8 48-59 324 4 1
9-10 60-71 405 5
11 72-95 486 6 1 1/2
12-14 >95 648 8 2

Ibuprofen Pediatric Dosing
Weight(lb)
Age(yr)
Dose(mg)
Dose(tsp)
24-35 2-3 100 1
36-47 4-5 150 1 ½
48-59 6-8 200 2
60-71 9-10 250 2 ½
72-95 11 300 3

Nonselective NSAIDs
Acetic Acids– Diclofenac (Voltaren)– Indomethacin– Nabumetone (Relafen)– Sulindac (Clinoril)– Tolmetin (Tolectin)
Oxicams– Piroxicam (Feldene)– Meloxicam (Mobic)
Pyranocarboxylic acid– Etodolac (Lodine)
Pyrrolizine carboxylicacid– Ketorolac (Toradol)
Propionic Acids– Fenoprofen (Nalfon)– Flurbiprofen (Ansaid)– Ibuprofen (Motrin)*– Ketoprofen (Orudis)– Naproxen /Naproxen Na
(Anaprox, Naprosyn)– Oxaprozin (Daypro)
Fenamates– Meclofenamate– Mefenamic acid (Ponstel)
Nonselective NSAIDs GI Effects Nausea
– Most 3-9%
– Ketorolac 12%
– Tolmetin 11%
Diarrhea– Ibuprofen , Piroxicam<3%
– Diclofenac, Etodolac, Flurbiprofen, Ketorolac, Oxaprozin, Sulindac, Tolmetin 3-9%
– Nabumetone 14%
Dyspepsia– Most 3-9%– Etodolac 10%– Ketoprofen 11.5%– Ketorolac 12%– Nabumetone 13%
Stomatitis– Most 1-3%
Additive effects with aspirin– GI toxicity
Nonselective NSAIDs Adverse drug effects and interactions Inhibits platelet
aggregation– reversibly
– normal function when drug eliminated
Potentiates the effects of anticoagulants
– Warfarin (Coumadin)– Anisindione (Miradon)
– Dicumarol Potentiates the effects of
other antiplatelet drugs– Dipyridamole (Persantine)– Ticlodipine (Ticlid)– Anagrelide (Agrylin)– Clopidogrel (Plavix)– Cilostazol (Pletal)
NSAIDs Adverse Effects Cross-hypersensitivity with aspirin allergy
– Contraindication– urticaria, asthma, nasal polyps
NSAIDsAdverse Drug Effects and Drug Interactions
Caution with reduced renal function– Do not prescribe for
renal transplant patients
Lithium– Increased toxicity
Methotrexate– Increased toxicity
Cyclosporine– Increased
nephrotoxicity
NSAIDs Drug Interactions Antihypertensives
– decrease effect– ACE Inhibitors
• Benazepril (Lotensin)• Captopril (Capoten)• Enalapril (Vasotec)• Fosinopril (Monopril)• Lisinopril (Prinivil,
Zestril)• Moexipril (Univasc)• Quinapril (Accupril)• Ramipril (Altace)• Trandolapril (Mavik)
Angiotensin II Receptor Antagonists– Candesartan (Atacand)– Eprosartan (Teveten)– Irbesartan (Avapro)– Losartan (Cozaar)– Telmisartan (Micardis)– Valsartan (Diovan

NSAIDs Drug Interactions
– Beta Blockers• Acebutolol (Sectral), Atenolol (Tenormin),
Betaxalol (Kerlone) Bisoprolol (Zebeta), Metoprolol (Lopressor, Toprol XL),
Carteolol (Cartrol), Nadolol (Corgard), Penbutolol (Levatol), Pindolol (Visken), Propranolol (Inderal) Sotalol (Betapace), Timolol (Blocadren), Labetalol (Normodyne, Trandate)
NSAIDs Drug Interactions Antihypertensives
– decrease effect
– Loop Diuretics• Furosemide (Lasix),
Bumetanide (Bumex), Ethacrynic acid (Edecrin), Torsemide (Demadex)
– Thiazide Diuretics• Bendroflumethiazide
(Naturetin), Benzthiazide (Exna), Chlorothiazide (Diuril), Hydrochlorothiazide (Hydrodiuril, Esidrix, Oretic), Hydroflumethiazide (Diucardin, Saluron), Indapamide (Lozol), Methyclothiazide (Enduron, Aquatensen), Metolazone (Zaroxolyn, Mykrox), Polythiazide (Renese), Quinethazone, (Hydromox) Trichlormethiazide (Metahydrin, Naqua, Diurese)

NSAIDs Drug Interactions Cimetidine
– Increased NSAIDs effect/toxicity
Probenecid– Increased NSAIDs effect/toxicity
Codeine Combinations with Acetaminophen (CIII) Tablets (300 mg)
– Tylenol #2,3,4
Capsules (325 mg)– Phenaphen #3,4
– Fioricet w codeine• 50 mg Butalbital
• 40 mg Caffeine
Codeine Dose– #2 15 mg
– #3 30 mg
– #4 60 mg
Acetaminophen Dose– 300 - 325 mg
Codeine Sensitivity– Nausea most prevalent
Codeine Combinations with Acetaminophen (CV) 12 mg codeine/ tsp
(5cc) 120 mg
acetaminophen/ tsp (5cc)
Adult dose: 15 ml (1 tablespoonful q 4 h)
Capital w/Cod susp Tylenol w/Cod elixir Acetaminophen w/cod
sol (various manuf)
Codeine Combinations with Acetaminophen (CV) Analgesic:
– 0.5 – 1 mg codeine/kg/dose every 4-6 hours
– 10-15 mg/kg/dose acetaminophen every 4-6 hours
3-6 yr:– 5 ml (1 tsp)
7-12 yr– 10 ml (2 tsp)
>12 yr– 15 ml (3 tsp)
Hydrocodone Combinations with Acetaminophen (CIII) 2.5/108 Solution
– Hycet 2.5/167 Elixir
– Lortab 2.5/500 tablets
– Lortab 2.5/500 5/325
– Norco 5/400
– Zydone 5/500 tablets
– Co-Gesic, Duocet, Hy-Phen, Lorcet, Lortab 5/500, Anexsia 5/500 Panacet 5/500, Vicodin
5/500 capsules– Bancap HC, Ceta-Plus,
Dolacet, Hydrocet, Hydrogesic, Margesic H, Lorcet HD, Stagesic, T-Gesic, Zydone
7.5/500 Tablets– Lortab 7.5/500
7.5/650 Tablets– Anexsia 7.5/650, Lorcet Plus
7.5/750 Tablets– Vicodin ES
10/650 Tablets– Lorcet 10/650
Hydrocodone
Children < 50 kg– 0.2 mg/kg every 4-6 hours
Children > 50 kg– 5-10 mg every 4-6 hours

Meperidine (CII)
Meperidine (Demerol)– 50, 100 mg tablets
– 50 mg/5cc syrup
– 50 - 150 mg q 3-4 h
– Children• 1-1.5 mg/kg/dose q 3-4
h
Meperidine/Promethazine (Mepergan Fortis)
– 50 mg Meperidine
– 25 mg Promethazine
– 1 q 4-6 h
Contraindications of Meperidine
Patients taking MAOIs within 14 days– Antidepressants
• Phenelzine (Nardil)
• Tranylcypromine (Parnate)
– Antiparkinson– Selegiline (Eldepryl)
– Hyperphenylalaninemia
Meperidine Drug InteractionsSerotonin Syndrome Serotonergic Drugs
– Selective Serotonin Reuptake Inhibitors (SSRIs)
• Fluvoxamine (Luvox)
• Fluoxetine (Prozac)
• Paroxetine (Paxil)
• Sertraline (Zoloft)
• Citalopram (Celexa)
• Escitalopram (Lexipro)
Cognitive-behavioral– Confusion/ disorientation (51%)
– Agitation/irritability (34%)
Autonomic Nervous System– Hyperthermia (45%)
– Diaphoresis (45%)
– Sinus Tachycardia (36%)
– Hypertension (35%)
Neuromuscular– Dilated pupils (28%)
– Tachypnea (26%)
– Nausea (23%)
Opioids
Phenanthrenes – Codeine
– Hydrocodone
– Oxycodone
– Morphine
– Hydromorphone
– Levorphanol
Phenylpiperidines– Meperidine
– (Fentanyl)
Diphenylheptanes– Propoxyphene
– (Methadone)

Opioid Pharmacologic Effects
CNS Effects– Analgesia
– Euphoria
– Sedation
– Respiratory Depression
– Cough Suppression
– Miosis
– Truncal Rigidity
– Nausea and Vomiting
CV System– Hypotension
GI Tract– Constipation
Biliary Tract– Colic
Genitourinary Tract– Urinary Retention– Decreased Renal Function

Warnings for Opioids
Asthma and Other Respiratory Conditions– Use with extreme caution with acute asthma,
bronchial asthma, COPD or cor pulmonale
Hypotensive Effect– Increased with coadministration of
phenothiazines or general anesthesia
Opioid Drug InteractionsDental Implications Phenothiazines
– Acetophenazine (Tindal)
– Chlorpromazine (Thorazine)
– Fluphenazine (Prolixin)
– Mesoridazine (Serentil)
– Perphenazine (Trilafon)
– Prochlorperazine (Compazine)
– Promazine (Sparine)
– Promethazine (Phenergan)
– Thioridazine (Mellaril)
– Trifluoperazine (Stelazine)
Additive Pharmacologic Effects– CNS Depression
– Respiratory Depression
– Orthostasis
Inhibitors of CYP3A4 increase opioid effects
Antifungals– Fluconazole– Itraconazole– Ketoconazole– Miconazole
Metronidazole Macrolides
– Erythromycin– Clarithromycin

Narcotic Antagonist
Naloxone (Narcan)– 0.4 mg/ml, 1 mg/ml– For OD:
• 0.4 - 2 mg IV q 2-3 minutes
– Partial reversal• 0.1-0.2 mg IV q 2-3 minutes repeat every 1-2 hrs
– Children:• 0.01 mg/kg IV, may repeat q 2-3 min
Treating Nausea
Anti-emetics Hydroxyzine
– Atarax, Vistaril Phenothiazines
– Chlorpromazine– Perphenazine
• Trilafon– Prochlorperazine
• Compazine– Promethazine
• Phenergan– Triflupromazine
• Vesprin– Triethylperazine
• Torecan
Metoclopramide – Reglan
Anticholinergics– Cyclizine
• Marezine– Meclizine
• Antivert, Bonine– Dimenhydrinate
• Dramamine Trimethobenzamide
– Tigan
Anti-emetics
5-HT3 Receptor Antagonists– Dolasetron
• Anzemet
– Gransetron• Kytril
– Ondansetron• Zofran
Droperidol– Inapsine
Dronabinol– Marinol
Anti-emetics
Hydroxyzine– 25-100 mg– Children: 1.1 mg/kg
Promethazine– 12.5 - 25 mg q 4-6 h– Children 0.25 - 0.5 mg/kg q 4-6 h– do not adm < 2 yo
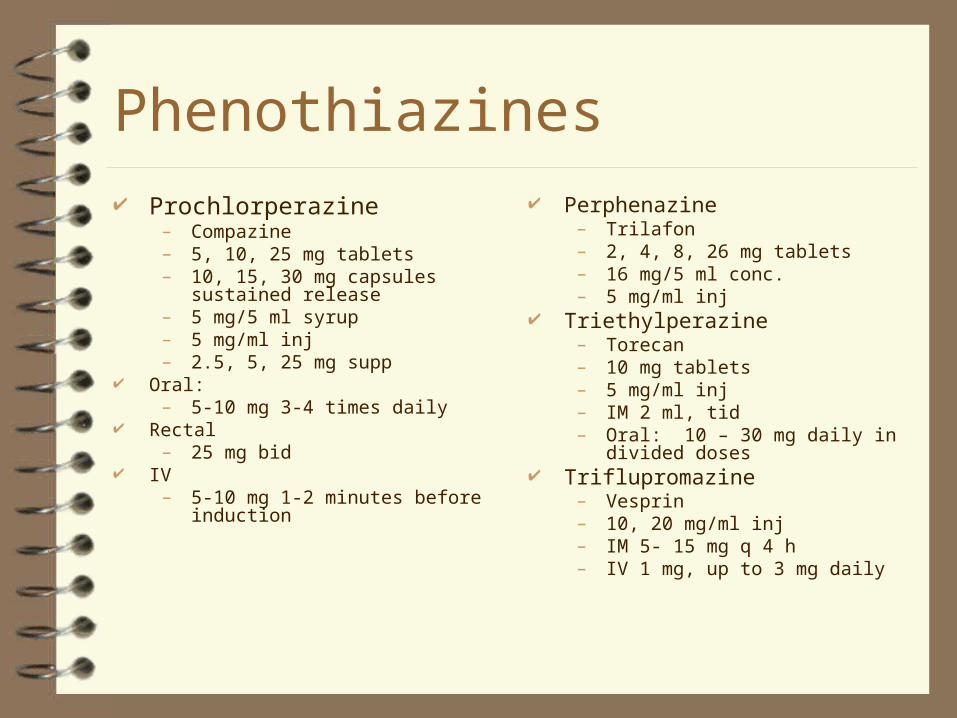
Phenothiazines Prochlorperazine
– Compazine– 5, 10, 25 mg tablets– 10, 15, 30 mg capsules sustained
release– 5 mg/5 ml syrup– 5 mg/ml inj– 2.5, 5, 25 mg supp
Oral:– 5-10 mg 3-4 times daily
Rectal– 25 mg bid
IV – 5-10 mg 1-2 minutes before induction
Perphenazine– Trilafon– 2, 4, 8, 26 mg tablets– 16 mg/5 ml conc.– 5 mg/ml inj
Triethylperazine– Torecan– 10 mg tablets– 5 mg/ml inj– IM 2 ml, tid– Oral: 10 – 30 mg daily in divided doses
Triflupromazine– Vesprin– 10, 20 mg/ml inj– IM 5- 15 mg q 4 h– IV 1 mg, up to 3 mg daily

5-HT3 Receptor Antagonists
Ondansetron– Zofran– 4, 8, 24 mg tablets– 4 mg/5ml solution– 2 mg/ml inj– 32 mg/50ml premixed– IV (prevention)
• 4 mg undiluted over > 30 seconds
– Oral• 16 mg 1 hr before procedure
– Zofran ODT• 4, 8 mg
Dolasetron– Anzemet– 50, 100 mg tablets– 20 mg/ml inj– IV
• 12.5 mg• Children: 0.35 mg/kg
– Oral (prevention)• 100 mg 2 h before surgery• Children: 1.2 mg/kg
within 2 hr of surgery– Caution in patients with
QTc abnormalities
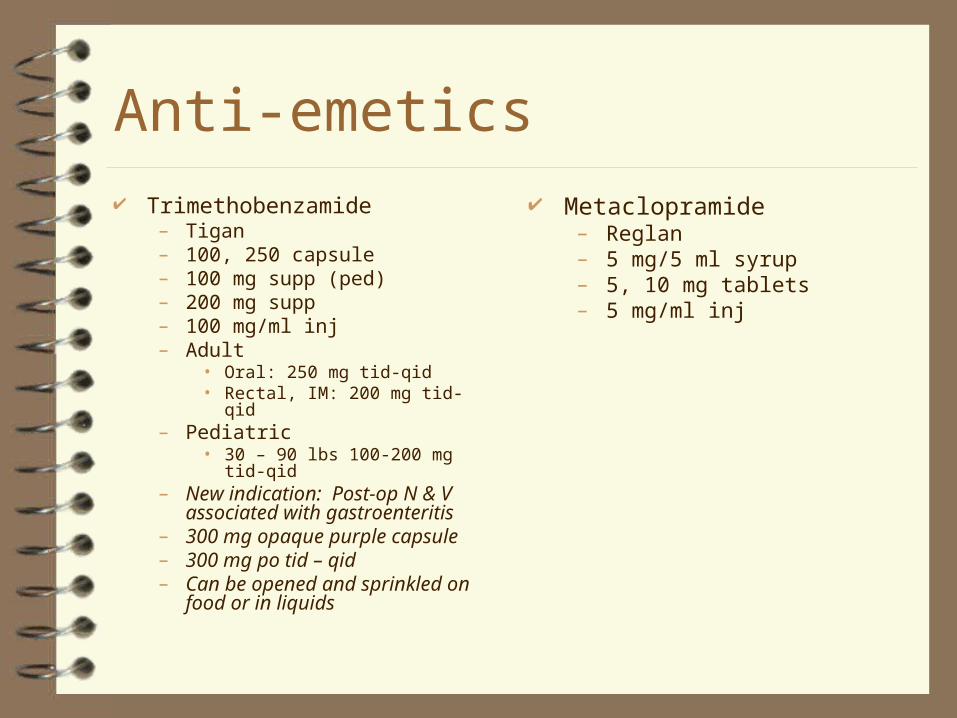
Anti-emetics Trimethobenzamide
– Tigan– 100, 250 capsule– 100 mg supp (ped)– 200 mg supp– 100 mg/ml inj– Adult
• Oral: 250 mg tid-qid• Rectal, IM: 200 mg tid-qid
– Pediatric• 30 – 90 lbs 100-200 mg tid-qid
– New indication: Post-op N & V associated with gastroenteritis
– 300 mg opaque purple capsule– 300 mg po tid – qid– Can be opened and sprinkled on
food or in liquids
Metaclopramide– Reglan– 5 mg/5 ml syrup– 5, 10 mg tablets– 5 mg/ml inj

Antiemetic Dental Implications
Increased CNS Depression– Sedation– Respiratory depression
Extrapyramidal effects Vasodilation
– Orthostatic hypotension Lower seizure threshold Increase cardiac arrhythmias Interaction with vasoconstrictors Anticholinergic effects
– dry mouth
Related Documents











