Challenges in the development of immunotherapies Candice Jamois, Clinical Pharmacology, Pharmaceutical Sciences International Workshop of Clinical Pharmacology of AntiCancer Drugs Amsterdam, Friday 22 nd November 2019

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Challenges in the development of immunotherapies
Candice Jamois, Clinical Pharmacology, Pharmaceutical Sciences
International Workshop of Clinical Pharmacology of AntiCancer DrugsAmsterdam, Friday 22nd November 2019

No disclaimer
• Except that I am a Roche employee
2

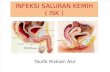
2018 Nobel Prize Awarded for Cancer ImmunotherapyJames P. Allison and Tasuku Honjo : for their discovery of cancer therapy by inhibition of negative immune regulation
3
T cell
Cancer cell
“Their work , the foundation for an entirely novel form of cancer treatment — immune checkpoint therapy — which has been credited with saving thousands of lives within the first few years since its approval.”
• James P. Allison, from the MD Anderson Cancer Center (University of Texas) for his work on CTLA-4 (T-lymphocyte-associated protein 4) blockade,
• Tasuku Honjo, from the Graduate School of Medicine of Kyoto University for his work on PD-1 blockade (programmed cell death protein)

T-cell Checkpoint Regulation, an evolving era since 2011
4
Centanni et al. Clin PK, 2019
6 Check Point Inhibitors approved by FDA, 5 of them by EMA
Improved Survival with Ipilimumab in Patients with Metastatic Melanoma
Hodi FS et al. New England Cancer of Medicine, 2010
gp=glycoprotein 100 peptide vaccine

The Cancer-Immunity Cycle – Activating T-cells against CancerPresentation, recognition, activation, and expansion are key factors for an efficacious tumor response
Chen DS and Mellman I, Immunity, 2013. APC= Antigen-Presenting-Cells; TME= Tumor micro environment; CTL= Cytotoxic T Lymphocytes
Tumour
Lymph node
Blood vessel
Release of cancer
cell antigens
(cancer cell death)
1
Cancer antigen
presentation
(dendritic cells/APCs)
2
Priming and
activation (APCs
and T cells)
3
Infiltration of T cells
into tumours
(CTLs, endothelial cells)
5
Recognition of cancer
cells by T cells
(CTLs, cancer cells)
6
Killing of cancer cells
(immune and cancer
cells)
7
Trafficking of T cells
to tumours (CTLs)4
Ability to create an Antigen-specific T cell response
Ability to infiltrate the TME (Homing and extravasation)
Ability to Kill tumor cells

GeneratorsIncrease number of antigen-specific T-cells
or increase antigen presentation
Examples:
aCD40
“Endogenous” vaccines
ModulatorsAccelerate or remove brakes on T-cell response
Examples:
aPD-L1
CEA-IL2v
aCSF-1R
EngagersBring T-cells in contact with
cancer cells
Examples:
CEA-TCB
Cancer Immunotherapy => Host directed
Adressing the Cancer Challenge with innovative IO agents Generators, Modulators, Engagors

Dosing and Pre-Clinical Model Translation Classical models of Pharmacology Dose Decision Making Process most of the time do not apply for IO agents
7
Cancer immunotherapies (biologics and cell based therapies) are not compatible with conventional pharmacological approaches (NOAEL) when determinig dosing because:
• Efficacy is directly mechanistically linked to immune mediated adverse outcomes
• Immune responses are stochastic and highly dynamic
Human
dose
Apply safety factor
Select appropriate animal species
Convert NOAEL to Human Equivalent Dose
Determine no observed adverse effect levels (NOAEL) in animal species
➢ An in vitro MABEL (minimum anticipated biological effect level) approach is often preferred over the in vivo NOAEL approach
Ch
alle
nge
1: P
re-c
linic
alTr
ansl
atio
n

▪ Binds simultaneously with 1 arm to CD3e on T cells and with 2 arms to CEA on tumor cells
▪ Flexible 2- to -1 format enables high-avidity binding and selective killing of high CEA-expressing tumors cells
▪ Extended half-life compared to non-Fc based TCBs
▪ Silent Fc results in reduced risk of FcgR-related cytokine release/ infusion related reactions
CD3 T cell engagement
Silent Fc forhalf-life extension
High avidity binding to tumor antigen
CEA-TCB, first bispecific antibody with a 2- to 1- format leading to T cell mediated killing of tumor cells
8
“2+1” format Fab range of motion in TCB
Bacac M, et al. AACR 2015 and Clin Cancer Res. 2016.; Pr Joseph Tabernero ASCO 2017 CEA=Carcino Embryonic Antigen; TCB = T cell bi specifics
Ch
alle
nge
1: P
re-c
linic
alTr
ansl
atio
n

Determination of the EIH starting-dose of CEA-TCB leveraging 3 MABEL approaches
9
Key Methods for Starting Dose Assessment with Associated CD3e Receptor Occupancies (RO)
In vivo efficacyIn vitro assessment
Tumor Cell LysisReceptor occupancy
403 µg/Kg
(38% RO)
0.736 µg/Kg- EC20
(0.11% RO CD3e)
6.7 µg/Kg
(1% RO CD3e)
Starting dose (52 µg)
o The tumor cell lysis assay was selected for the determination of the starting-dose as the most sensitive
of the three MABEL approaches
o The starting-dose selected was well below the level at which cytokine release was observed in the
Whole Blood Assay (safety factor applied to suggested MABEL dose).
Bacac M, et al. AACR 2015 and Clin Cancer Res. 2016.
Ch
alle
nge
1: P
re-c
linic
alTr
ansl
atio
n

PK properties lead to exposure reduction following multiple dosing Extent of exposure reduction is dependent on the dose and frequency of administration
Grimm H.P., PAGE 2016IL2v cytokine
Tumor target High affinity for tumor antigen (CEA)
Inert Fc part
Modified IL2-variant
Advantages over wild type IL2
• Tumor targeting
• Improved PK properties
• Reduced toxicity
Tumor-targeted immune cytokine
CEA = Carcinoembryonic antigen, IL2=Interleukin 2, cytokine for cell signaling
Grimm et al. PAGE 2016 ; Silber-Baumann et al. PAGE 2017 ; Ribba B, ACOP 2017
Ch
alle
nge
2: C
ho
ice
of
Op
tim
al C
linic
al D
ose
Dose
Frequency Exposure reduction
Drug concentration
Receptor concentration
AUC by treatment cycle
QW
Q2W
Q3W
Time (days) Time (days) Cycle

A quantitative model integrating PK and PET imaging data was developed to predict the impact of Dosing Regimen on Antibody Tumor Uptake and identify the best schedule
PET imaging study with radiolabeled CEA-IL2v
Drug in
interstitial
space
Bound drugDose
Drug in
plasma
Drug in tumor
Predicted tumor uptake QWPredicted tumor uptake Q2W
PET data were incorporated into a model for tumor uptake
Intensifying the dosing frequency is predicted to significantly improve tumor uptake despite peripheral target expansion and reduced exposure
Ribba B et al. CCR, 2018
• Specific tumor uptake after the 1st dose
• Reduced uptake following repeated dosing (Q2W)C
hal
len
ge 2
: Ch
oic
e o
fO
pti
mal
Clin
ical
Do
se

Bell-Shape Kinetics of the tri-molecular synapse between bi-specific Ab, T cell, and Tumor cell : a new Challenge for Clinical Development
12
• Too much bispecific Ab may saturateantigens, and limit cross-linking
• Too little bispecific Ab may not enhanceTarget Cells and T cells cross-linking
Structure of the Target cell-Biologics-Effector Cell complex –based cell killing model
Xiling Jiang et al. MABS, 2018
Bell Shape Kinetics - Illustration
Ch
alle
nge
2: C
ho
ice
of
Op
tim
al C
linic
al D
ose

Immune related Adverse Events (IrAEs), inflammatory side effects caused by IO agents
13Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur J of Cancer, 2016
C. Lee Ventola. Cancer Immunotherapy, Part 2: Efficacy, Safety, and Other Clinical Considerations. 2017
Immune related adverse events with Check Point blockers
Ch
alle
nge
3: R
isk
Mit
igat
ion
Mea
sure
s

Harnessing the Host Immune System while still Controlling it : Cytokine Release Syndrome, a Major Challenge with T cells engaging IO therapies
14
Engineered T cells - Chimeric antigen receptor (CARs)
▪ Outstanding clinical efficacy with CD19 CARs in B-cells malignancies
▪ Activity associated with high toxicity (such as CRS)
Ch
alle
nge
3: R
isk
Mit
igat
ion
Mea
sure
s

Managing immune mediated adverse events : a Challenge Some safety measures may compromise efficacy potential
15
Maude S.L., Barrett D., Teachey D.T., Grupp S.A. Managing cytokine release syndrome associated with novel T cell-engaging therapies. Cancer J. 2014;20:119–122
• Corticosteroids may control some of these toxicities, however their potential to block T cell activation/proliferation and abrogate clinical benefit is a concern
• Tocilizumab , anti IL6R, an alternative to manage patients’ safety without compromising efficacy
Kaplan-Meier curves of OS according to the use of steroids
Nivolumab
Giovanni Fuca et al. ESMO 2019
Nivolumab + steroids
Early use of steroids, associated with poor disease control in patients with mNSCLC
Ch
alle
nge
3: R
isk
Mit
igat
ion
Mea
sure
s

Obinutuzumab (Gazyva®) pre-treatment to mitigate the risk of CRS. Shared target : when CD20 molecular format and receptor occupancy (RO%) drive the response
• G pre-treatment is given as 1000 mg IV, on Cycle Day -7
• CD20-TCBa,b RO% determined in the presence of circulating G pre-treatment using standard approachesc
• Average RO% (AvgRo%) used to examine relationships with efficacy and safety and inform RP2D
16
https://www.biooncology.com/pipeline-molecules/cd20-tcb.html
aBacac M et al. Blood. 2016;128:1836. bBacac M et al. Clin Cancer Res. 2018.cSaji Salahudden M et al. Saudi Pharm J. 2017. ASH 2019
-assumes binding equilibrium and serum RO% correlates with response
-does not account for absolute number of receptors
Ch
alle
nge
3: R
isk
Mit
igat
ion
Mea
sure
s

Rationale framework to design and assess combination therapy
17
• > 2300 FDA registered clinical trials are on-going based on targeting PD-1 pathway
• Most large pharma companies in IO would have up to 15,00-20,00 combination therapies
• Modeling can help identify dosing, combinations, timing, mixing cell based therapies & vaccines with biologics….
From Tang J et al., Nature Reviews Drug Discovery 17, 854-85, 2018
Despite impressive clinical outcomes, RR for all CPIs administered as single agents < 50 % regardless of tumor type
Combotherapy Landscape
Ch
alle
nge
4: C
om
bin
atio
nth
erap
y

Multi-trial platform - Novel way to test Cancer Immunotherapy Combinations
18
How to identify optimal clinical dose?
How to identify optimal sequencing?
For each combinationThrough understanding
of drug response variability
Ch
alle
nge
4: C
om
bin
atio
nth
erap
y

Some Perspectives The success of combination immunotherapy will depend on our ability to manage development hurdles
• Design of the right preclinical experiments and the translation of those into the clinic,
• Optimization of the dose and schedule of the combination regimen,
• Safety management (risk of overlapping toxicities with immunotherapies).
19
The application of Quantitative Clinical Pharmacology Approaches in the translational space and throughout clinical development may help to address these challenges; in collaboration with System Pharmacology
and Machine Learning

Doing now what patients need next
Related Documents