Challenges in Management: Solid Organ Transplantation & Tuberculosis Michele I Morris, M.D., FACP, FIDSA Director, Immunocompromised Host Section Associate Professor of Clinical Medicine Division of Infectious Diseases University of Miami Miller School of Medicine Miami, FL, USA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Challenges in Management:
Solid Organ Transplantation &
Tuberculosis
Michele I Morris, M.D., FACP, FIDSA Director, Immunocompromised Host Section
Associate Professor of Clinical Medicine Division of Infectious Diseases
University of Miami Miller School of Medicine Miami, FL, USA
The Nightmare Scenario
• 45 year old female nurse mother of 2 develops active pulmonary TB after work related exposure
• Treated with RIPE, develops hepatic failure 12 weeks into therapy
• Is she a candidate for liver transplant?
• If so, how do you manage her TB post-transplant?

Expert Clinical Opinion

TB in Solid Organ Transplant
(SOT)
• Epidemiology
• Interventions to prevent TB post-transplant
– Screening deceased & living donors
– Screening transplant candidates
– Management of Latent TB in SOT
• Worse Case Scenario – Treating TB post-transplant – How TB providers can help

TB Epidemiology in SOT
• SOT recipients 36-74 fold higher risk for TB than general population
• TB incidence 1.2-6.4%, up to 15% in highly endemic countries
• Risk factors for TB in SOT
– Country of origin
– Older age
– Lung transplant
Morris MI. Amer J Transpl 2012;12:2288-2300.
TB Mortality in SOT
• Mortality of TB in SOT 10-30%
• TB-attributable mortality 9-20%
• Predictors of TB mortality
– Disseminated infection
– Prior rejection
– Increased immunosuppression (anti-T cell antibody therapy)

TB in SOT:
Reasons for Increased Mortality
• Delayed Diagnosis
– Immunocompromised with multiple infection risks
– Unusual clinical presentations
• Drug-drug interactions with transplant immunosuppressants allograft rejection organ loss
– Transplant experts with little TB experience
– TB experts with little transplant experience
Sources of TB in Transplant
Recipients
• Reactivation in recipients with untreated or unrecognized latent or active TB
• Post-transplant exposure – Likely more common in high TB incidence countries – Nosocomial outbreaks – Travel
• Donor-derived – transmitted through organ allograft – ~4% post-transplant TB – Likely more common in lung recipients
• Relapse – history of previously treated active TB with persistent viable bacilli despite clinical cure – 3.5% relapse rate at 2 years with 4 drug/6 month TB therapy

• Only 20-25% of post-transplant TB patients had +TST pre-transplant – End stage organ failure TST anergy/IGRA
indeterminate results
• No gold standard to diagnose LTBI • Sensitivity of IGRAs may be better than TST • Both tests specific, any + should be considered as
evidence of TB infection • Neither TST nor IGRA can distinguish latent from
active TB
TST & IGRA Performance in
Transplant Candidates

QuantiFERON-TB Assay in
Hemodialysis Patients
High rate of indeterminates but none with active TB
Inoue T, Nakamura T, Katsuma A. Nephrol Dial Transplant 2009.

Predictive Value of T-SPOT TB Test
in Kidney Transplant Candidates
Kim S-H, Lee S-O, Park JB. Amer J Transpl 2011.
Rate difference 3.3/100 + vs -/indeterminate P<0.001

Quantiferon-TB Gold Test
Performance in Transplant
Candidates
Transplant Type
Total Positive Test Result
Indeterminate Test Result
Negative Test Result
Liver alone 310 60 (19.4%) 126 (40.6%) 124 (40%)
Kidney alone 541 175 (32.3%) 57 (10.5%) 309 (57.1%)
Liver-Kidney 20 2 (10%) 8 (40%) 10 (50%)
Kidney-Pancreas
31 3 (9.7%) 4 (12.9%) 24 (77.4%)
Heart alone 12 3 (25%) 3 (25%) 5 (50%)
Other 27 2 (7.4%) 8 (29.6%) 17 (63%)
Theodoropoulos N, Lanternier F, Rassiwala J. Transpl Inf Dis 2011.

Quantiferon-TB Assay in Liver
Candidates • TST and QFT diagnose latent TB infection at
similar rates pre-liver transplant – consider IGRA followed by TST, esp in high risk
• Candidates with advanced liver disease – Indeterminate results more likely
– QFT performs better than TST
• Approach to indeterminate QFT – Repeat when patient healthier
– Alternative test – T-SPOT TB or TST
Manuel O, Humar A, Preiksaitis J. Amer J Transpl 2007. Casas S, Munoz L, Moure R. Liver Transpl 2011. Theodoropoulos N, Lanternier F, Rassiwala J. Transpl Inf Dis 2011.
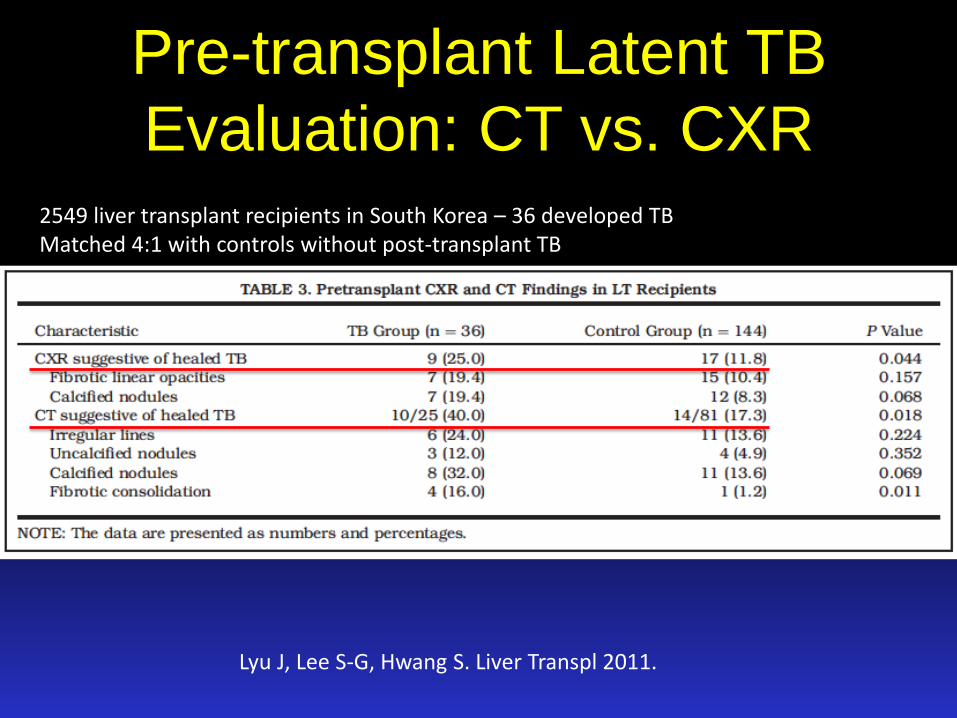
Pre-transplant Latent TB
Evaluation: CT vs. CXR
Lyu J, Lee S-G, Hwang S. Liver Transpl 2011.
2549 liver transplant recipients in South Korea – 36 developed TB Matched 4:1 with controls without post-transplant TB

Aguado JM, Torre-Cisneros J. Clin Infect Dis 2009.
TB Screening Algorithm for Transplant Candidates
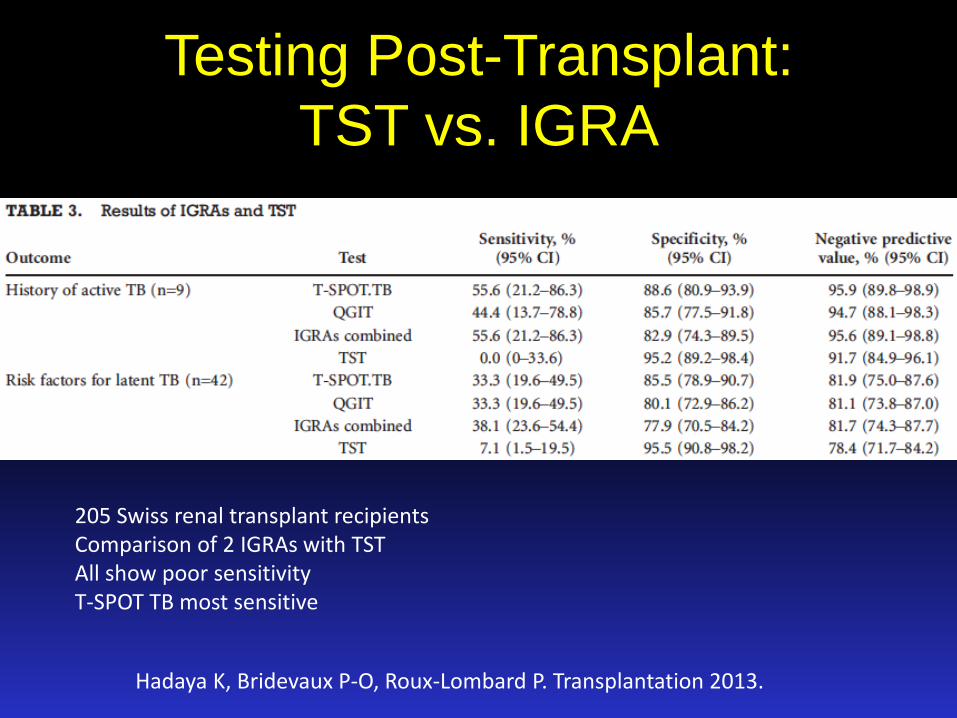
Testing Post-Transplant:
TST vs. IGRA
Hadaya K, Bridevaux P-O, Roux-Lombard P. Transplantation 2013.
205 Swiss renal transplant recipients Comparison of 2 IGRAs with TST All show poor sensitivity T-SPOT TB most sensitive

TB Screening of Deceased Donors
Detailed History is Key, but Complex
End Stage Organ Failure +/- ICU Care
Required Screening for
Multiple Infectious Diseases
Reliance on Diagnostic Tests with Variable
Sensitivity
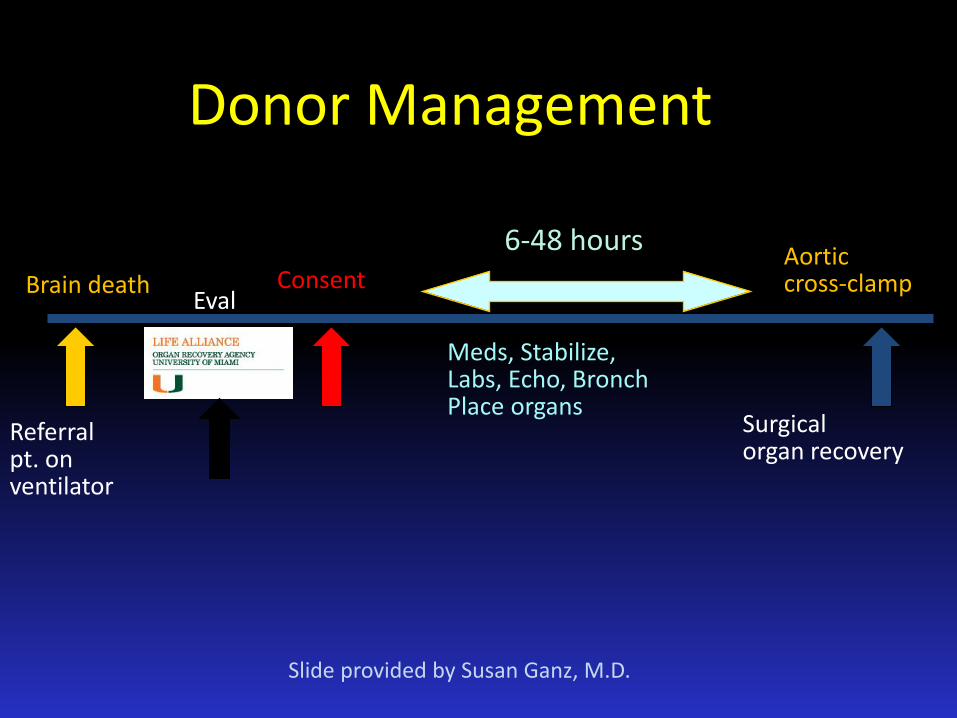
Brain death Consent
6-48 hours
Surgical organ recovery
Meds, Stabilize, Labs, Echo, Bronch Place organs
Referral pt. on ventilator
Aortic cross-clamp
Donor Management
Eval
Slide provided by Susan Ganz, M.D.

TB Screening of Deceased Donors
• TST not feasible • IGRAs often indeterminant
– Head injury patients known to have cellular immunity
– Screening cattle for M. bovis pre/post mortem demonstrated ~50% decrease in gamma interferon after slaughter
• IGRA evaluated in 105 deceased donors – Quantiferon TB Gold - 56/105 (53%) indeterminant – FACS (research assay) - 13/104 (12.5%) indeterminant – ELISPOT 0/97 - (0%) indeterminant
Schmidt T, Schub D, Wolf M. Amer J Transpl 2014.

TB Screening of Deceased Donors
History Obtained from relatives, sometimes distant or uninformed, often inaccurate
Imaging CXR often obscured by trauma,
pulmonary edema. Unspecified lung nodules/granulomas may not be identifiable as TB pre-transplant
Micro Standard AFB smear and culture results not ready prior to transplant. Rapid molecular
methods not universally available at all centers
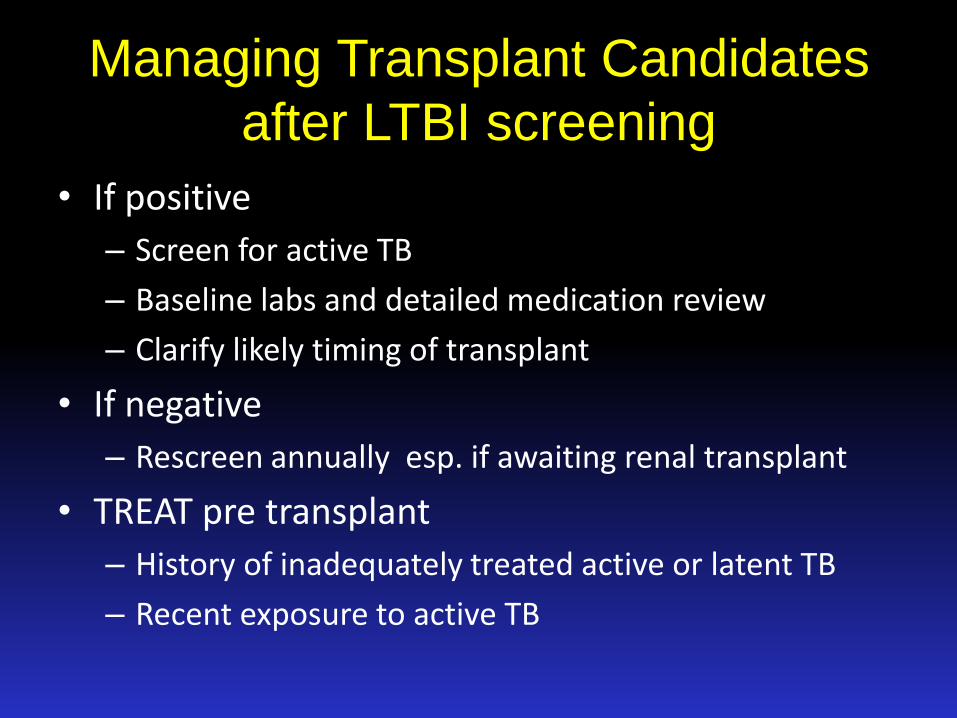
Managing Transplant Candidates
after LTBI screening
• If positive
– Screen for active TB
– Baseline labs and detailed medication review
– Clarify likely timing of transplant
• If negative
– Rescreen annually esp. if awaiting renal transplant
• TREAT pre transplant
– History of inadequately treated active or latent TB
– Recent exposure to active TB

Treatment Options Pre-SOT
Subramainian AK, Morris MI. Amer J Transpl 2013;13:68-76.

LTBI Treatment of SOT candidates
• INH/Rif 12 week regimen - 17 patients preSOT
– 83% dose compliance, 76% completion rate
– No transaminase elevations > 2x baseline, 4x ULN
Lopez de Castilla D, Rakita RM, Spitters CE. Transplantation 2014.
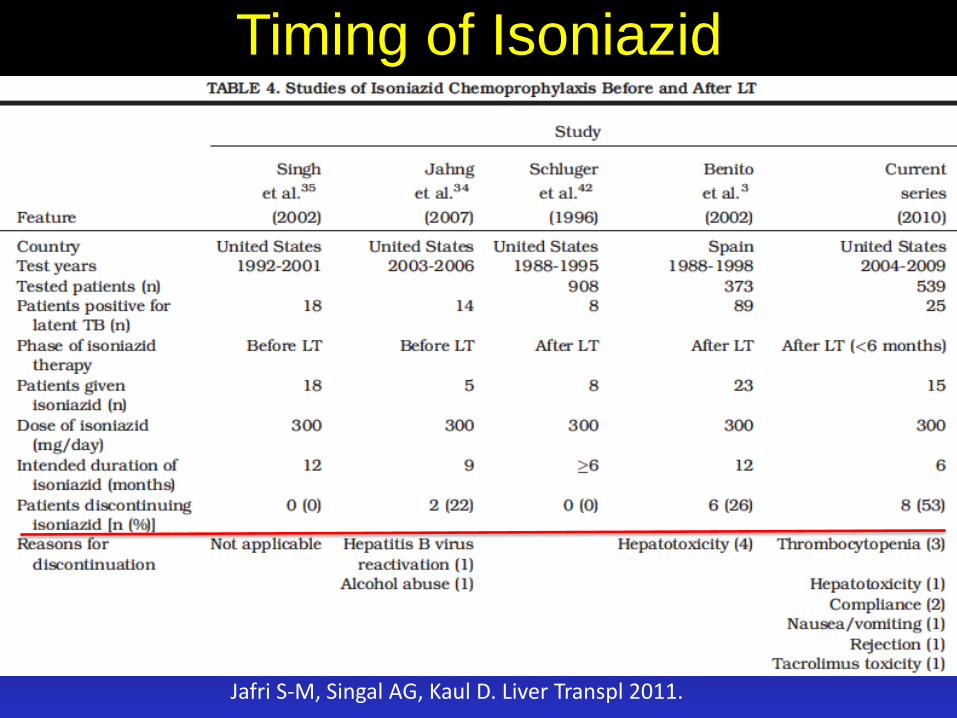
Timing of Isoniazid
Jafri S-M, Singal AG, Kaul D. Liver Transpl 2011.

INH vs. Rifampin for LTBI
Page KR. Arch Int Med 2006.
Retrospective cohort study of 2255 patients in MD treated for LTBI

Risks of Latent TB Treatment
• Drug related hepatotoxicity
– HBV, HCV coinfections
– Liver transplant candidates with ESLD
• Multiple drug-drug interactions
– Heart transplant candidates on coumadin, amiodarone
– Renal transplant candidates with oral hypoglycemics, antihypertensives
Transplant Candidates with History
of Latent or Active TB
• No need for repeat TST or IGRA • Need reliable documentation of adequate
therapy or repeat treatment pre/post SOT • RE-EVALUATE
– Assess for signs/symptoms of active TB – CXR with consideration for other imaging/testing – Microbiology prn
• Culture – slow if smear negative • Nucleic acid amplification
– rapid, automated – may be false negative with few mycobacteria present

TB Post Transplant • Clinical presentations atypical
– FUO
– Allograft dysfunction
– Uncommon sites of involvement – GI tract, Kidney, Bone, Skin
• 33-50% of post-transplant disease is disseminated or extrapulmonary – 15% in normal hosts
• Symptom onset within 1 year of transplant – median 11.2 months
Muñoz P, Rodriguez C, Bouza E. Clin Infect Dis 2005. Lopez de Castilla D, Schluger NW. Transpl Infect Dis 2010.

TB Post Liver Transplant
Holty J-EC, Gould MK, Meinke L. Liver Transpl 2009.
Seen in almost half of patients

Active TB & SOT 2009
• Unrecognized active TB at time of SOT
• Liver transplant in patients with hepatic failure due to TB treatment (our nightmare scenario)
Aguado JM, Torre-Cisneros J. Clin Infect Dis 2009.

Rifampin Sparing Regimens
Increased Risk of TB Recurrence
High TB Resistance Rates
No Difference in Post-TB Rejection Rate
No Difference in Mortality
Meije Y, Piersimoni C, Torre-Cisneros J. Clin Microbiol Infect 2014.
Transplant TB Treatment Tips 2015
• Rifampin-containing regimens may be preferred – Increase immunosuppressants 3-5 fold, esp. tacrolimus,
cyclosporine, sirolimus, everolimus
– Increase corticosteroids
– Closely monitor immunosuppressant levels
• Dose adjustments often needed in renal transplant recipients – INH, Ethambutol, Streptomycin
• ? Treat longer – 2004 - Better outcomes with treatment duration >12
months even rifampin-free
– 1997 - Treatment < 9 months associated with mortality
Meije Y, Piersimoni C, Torre-Cisneros J. Clin Microbiol Infect 2014. Aguado JM, Herrera JA, Gavalda J. Transplantation 1997. Park YS, Choi JY, Cho CH. Yonsei Med J 2004.
Treatment of TB post-SOT
• Do NOT treat alone – need transplant team clinician involvement – Complex drug-drug interactions
– Potential loss of organ allograft
• Do NOT use standard DOT – Daily dosing strongly preferred due to impact on other
medications (and medication levels)
• Do NOT give up on the organ allograft or the patient – Frequent visits with both transplant clinician managing TB
and TB provider essential for successful outcome

Immune Reconstitution Syndrome
(IRS) in Post-SOT TB • Increased inflammatory response seen in HIV patients • Occurs in 14% of TB post-transplant • Risk Factors
– Liver transplant – Cytomegalovirus (CMV) infection – Rifampin therapy
• Complicates monitoring of clinical response to treatment – Need to distinguish from progressive infection – Median onset 47 days after starting anti-TB therapy
• Increased 1 year Mortality (33% IRIS vs 17% no IRIS)
Sun HY. Prog Transplant 2014;24:37-43.
Take Home Messages • Transplant recipients are at high risk for TB related
morbidity and mortality
• Available diagnostics do not work optimally in deceased donors & critically ill transplant candidates
• Diagnose & treat LTBI pre-transplant if possible
• Post-transplant TB treatment requires close teamwork

Questions? [email protected]
Related Documents











