Challenge 4: Linking TB & HIV/AIDS Programs Kayt Erdahl, Project HOPE Rodrick Nalikungwi, Project HOPE Malawi December 18, 2008

Challenge 4: Linking TB & HIV/AIDS Programs Kayt Erdahl, Project HOPE Rodrick Nalikungwi, Project HOPE Malawi December 18, 2008.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Challenge 4:Linking TB & HIV/AIDS Programs
Kayt Erdahl, Project HOPERodrick Nalikungwi, Project HOPE Malawi
December 18, 2008
Topics
• Introduction• Why is it important to link TB & HIV Programs?• TB/HIV Interactions• TB/HIV Strategies• Project HOPE TB/HIV Program in Malawi• Challenges • Program activities & progress• Lessons learned/recommendations

Why is it important to link TB & HIV programs?
“Tuberculosis (TB) is a leading cause of HIV-related deaths worldwide. In countries with
high HIV prevalence, up to 80% of people with TB test positive for HIV.
Globally there were 700,000 TB cases among people living with HIV in 2006, and an
estimated 230,000 people living with HIV will die as a result of TB in 2008 despite the fact
that TB is curable.”http://www.who.int/hiv/topics/tb/en/index.html
TB/HIV Interactions
• HIV promotes progression from TB infection to TB disease. People with HIV are up to 50% more likely to develop TB in a given year than HIV-people.
• High rates of mortality among TB/HIV co-infected patients
• TB is more difficult to diagnose in people with HIV• Infection control issues• Treatment coordination for both diseases: drug
interactions, IRIS, system policies
The Three Is
Three key public health strategies focused on decreasing the impact of TB on people living with HIV:
• Isoniazid Preventive Therapy (IPT)• Intensified Case Finding (ICF) for active TB• TB Infection Control (IC)

Examples of areas that NGOs/CBOs can get involved
• Coalition development, coordination between TB and HIV services, PHC and communities
• Incorporate screening and testing for TB within HIV services and for HIV in TB services
• Capacity building, TB/HIV education• Mobilize communities to demand coordinated services,
and to seek diagnosis, treatment and care• Decrease burden of HIV in TB patients: CPT, ART, HIV
prevention, care and support
Mulanjepop. 548,250
Phalombepop. 296,960
Project HOPE TB/HIV Project in Malawi
Tuberculosis Control in Southern Malawi
Child Survival TB & TB/HIV Grant funded by USAID
Dates: Oct 2006-2011
Location: 2 Districts in Southeastern Malawi

Malawi & Program area
Malawi• Country in Southern Africa, 13 million population• Health services provided mainly by Government, also
Mission Hospitals and private sector
Mulanje and Phalombe districts• Shared border with Mozambique• Population over 845,000• Largely rural, with inconsistent distribution of health
facilities• Communicable diseases are common –TB, HIV and Malaria
Malawi TB Goal & Objectives
Sub-objectives:1. Improve treatment outcomes of TB cases and TB
cases with HIV co-infection in Mulanje and Phalombe
2. Increase case detection of TB, including among people with HIV co-infection in Mulanje and Phalombe
Goal: to reduce morbidity and mortality due to TB and TB cases with HIV co-infection in the Mulanje and Phalombe Districts

Baseline, 2006 Year 2, 2008
Indicator Malawi1 2 Districts2 Malawi3 Phalombe4 Mulanje4
Case detection rate, new SS+
39% 29% 42% 34% 41%
Treatment success rate, new SS+
71% 77% 73% 73% 76%
Died, new SS+ 16% 19% 15% 24% 19%
HIV Prevalence 14.1% 18.6% 14%5 20-22%5
HIV prevalence est. in incident TB Cases
50% 70%
TB & HIV Epidemiologic data
1 WHO 2007 Global TB Control Report (2004 cohort)
2 Mulanje & Phalombe District Health Office (TB 08 Q3 2005-Q2 2006)
3 WHO 2007 Global TB Control Report (2005 cohort)
4 Mulanje & Phalombe District Health Office (CD 2007, Treatment outcomes, 2006)
5 2007 AIDS Epidemic Update, Africa (2005 data)
Challenges
• ART accessibility limited for TB/HIV co-infected due to the MOH quota system for ART
• Service Providers and the community are at risk of TB infection due to inadequate infection control
• Not all health facilities have access to microscopy for TB diagnosis
• Existing laboratories need strengthening to improve quality of diagnosis
• Accessibility to HIV testing still limited in remote areas
Challenges
• Link between TB and HIV programs still weak
• Clinical issues– Initiation of ART in TB/HIV co-infected only starts after
two months on TB treatment, by policy– Patients will not come for ART when they start feeling
well – less recruitment on ART and increased risk of dying from
AIDS– ART and TB drug interaction poses risks to patients
Program Activities - Community
• ASCM - Community education campaign– Increase recognition of TB symptoms,
importance of HIV testing, early TB diagnosis, knowledge of TB/HIV interaction, behaviors related to HIV prevention
– Volunteers, community leaders, shop owners, traditional healers, drama groups, families
• Improve TB symptom screening/referral by– Traditional healers & shop-keepers– HIV patients (self-referral)– Household contacts of SS+ TB cases– VCT/HIV Clinical care providers
Program Activities – Health Workers
• Train/mentor health workers (40) and health surveillance assistants (61)
– DOTS, strengthen recording & reporting system– Recognition of TB symptoms & referral for testing, repeat testing for
people with HIV– supervision of guardians, advocacy for TB & ARV treatment
adherence
• Advocate for client-friendly services: hours, confidentiality• Update/improve training manuals & curricula in
collaboration with NTP for HCW, HAS, community groups• Collaboration with national, local and international
organizations and programs

Program activities - System
• Technical assistance for integration of HIV testing into TB system, and strengthening referral system between diagnostic and treatment services for TB and HIV
• Establish Coordinating Committees for case management• Enhance quality assurance and standard operating
procedures in collaboration with local health care authorities– Supportive supervision training– Monitoring visits with district or zonal TB officers
• Work with NTP to correctly implement WHO TB guidelines and reporting/recording system
Program Activities -Laboratories
• Laboratory assessment done - determined microscopy system needed strengthening
• Train/retrain laboratory staff in microscopy and recording system
• Enhance external quality assurance for microscopy - Development of QA monitoring tools
• Equip new laboratories for sputum microscopy – 3 new peripheral sites established in last year
Program activities – new developments
• New NTP policy of Universal Access to TB Diagnosis – Project HOPE is assisting in implementation of Community Sputum Collection Points in Mulanje and Phalombe
• High mortality rates among TB and TB/HIV patients - Death audits
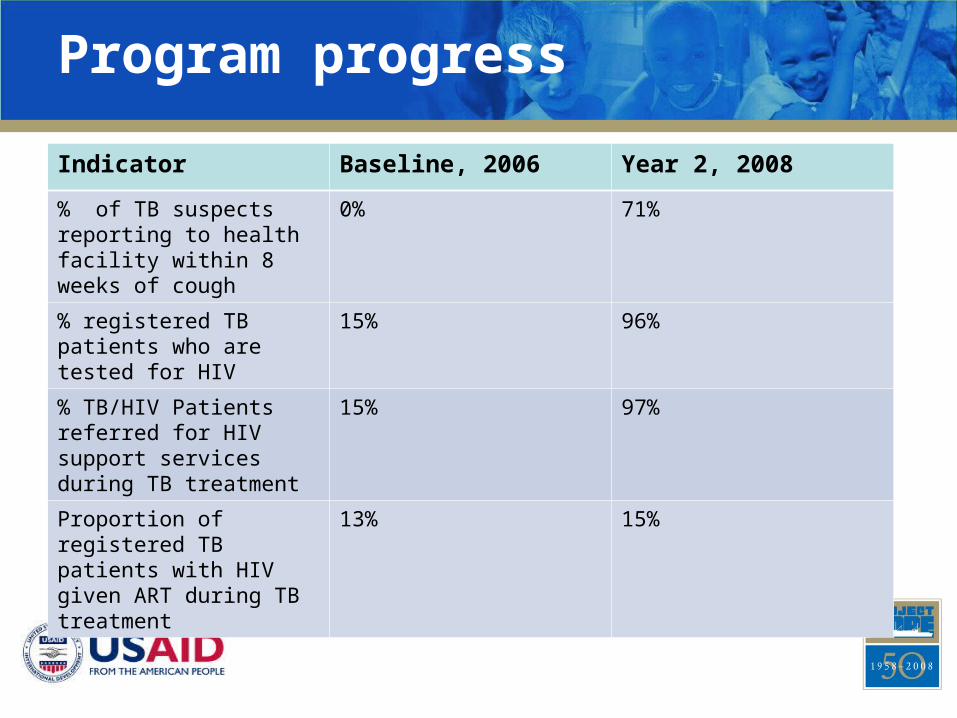
Program progress
Indicator Baseline, 2006 Year 2, 2008
% of TB suspects reporting to health facility within 8 weeks of cough
0% 71%
% registered TB patients who are tested for HIV
15% 96%
% TB/HIV Patients referred for HIV support services during TB treatment
15% 97%
Proportion of registered TB patients with HIV given ART during TB treatment
13% 15%
Lessons learned/recommendations
• TB/HIV management capacity building for health workers is particularly important: Health Surveillance Assistants are often allocated to work on TB/HIV with minimal knowledge
• HIV Counseling and testing done during the TB admission period has increased awareness and access to testing
• NTP and National AIDS Program should standardize approaches to TB and TB/HIV

Lessons learned/recommendations
• It is important for Programs to make strong links with other groups implementing activities in the community, e.g. nutrition-providing partners, Village health banks, etc.
• Programs/activities that put focus on community TB interventions are the most effective strategies in controlling TB, e.g. Decentralized microscopy, sputum points and transmission of results
• Proper data collection and documentation of activities important for sharing information at different levels.

Lessons learned/recommendations
• While clinical interventions are important, community health education is equally important
• Programs doing community interventions in TB/HIV co-infection should not be short term since they target behavior change that needs adequate time to have impact.
Thank you!Any questions?
Related Documents











