CH. 6 HYPERTENSION AND THE HEALTH BELIEF MODEL GROUP 1 - JASLYN ADAMS, CHERISE CASSELL, MARIA HERNANDEZ, JASON MOORE, JAYME RENTZ, MACKENZY VOLMY PHA 4724 HEALTH CARE & BEHAVIOR SECTION 301 CH. 5- HYPERTENSION OCTOBER 25, 2011 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
CH. 6 HYPERTENSION AND THE HEALTH BELIEF
MODELG R O U P 1 - JAS LYN ADAMS , CHER IS E CAS S ELL , MAR IA HERNANDEZ , JAS ON MOORE , JAYME RENTZ , MAC KENZY VOLMY
PHA 4724 HEALTH CARE & BEHAV IOR S EC T ION 301CH. 5 - HYPERTENS ION OC TOBER 25 , 2011

2
HYPERTENSION STATISTICS
• 32% of U.S. adults had high blood pressure in 2002.• 31% of American adults has pre-hypertension in
2002• Higher than normal blood pressure, but not yet in the
hypertension range.
• Raises your risk for high blood pressure.
• In 2010, high blood pressure will cost the United States $76.6 billion in health care services, medications, and missed days of work.

3
RISK FACTORS
• Stress or Anxiety• Family history of hypertension• Race – African-Americans• Diet – Excessive salt or fat • Drug Use – Smoking, Alcohol• Medications – Pain medication, Decongestants,
etc.• Medical Conditions – Diabetes, Obesity
SYMPTOMS
• No signs or symptoms for hypertension• Severe(Malignant) hypertension• Nosebleeds• Severe headaches • Nausea and vomiting• Changes in vision

TREATMENT
• Usually combines preventative lifestyle modifications with one or more antihypertensive drugs• Can be managed with medications such as
Lopressor®, Ativan®, Toprol®, and Cardura® among others.
6
PREVENTION
• Hypertension can be prevented by:• Exercising regularly• Reducing alcohol intake• Dietary Approach to Stop Hypertension (DASH)• Increases fruits and vegetables, Limits fat and sodium
• Check your blood pressure regularly.• Manage other medical conditions
7
COMPLICATIONS
• When hypertension is left untreated or not well controlled the following conditions can develop:• Heart• Myocardial infarction• Congestive heart failure• Angina Pectoris• Vascular Disease
• Brain • Stroke• Dementia• Vision Problems
• Chronic kidney disease
CH 7 DYSLIPIDEMIA?
• Definition: Increased blood lipid levels and lipoprotein concentrations.
• Caused by:oEnvironmentaloGenetic oPathologic risk factors

DYSLIPIDEMIA
• The major blood lipids involve:o Cholesterol- vital & needed component for
maintaining normal physiologic functioningo Triglycerides- consist of glycerol esterfied with 3 fatty
acids and are the main constituents of stored energy. Present in blood plasma and form plasma lipids when associated with cholesterol.
o Phospholipids- essential for cholesterol and triglyceride transportation in the serum in the form of lipoproteins.
• Elevated lipoprotein concentrations contribute to dyslipidemia.
STATISTICS
• CHD is the number 1 cause of death in the US
• It is reported than nearly 1million Americans experience CHD event annually in which 40% are fatal
• One of the major risk factors is hyperlipidemia
• Approx 18% American have blood cholesterol levels that are too high
RISK FACTORS FOR DYSLIPIDEMIA
• Chronic Heart Disease (CHD)
• Diabetes mellitus
• Metabolic Syndrome
• Severe or poorly controlled CHD factors
PRIMARY FACTORS CONTRIBUTING TO DYSLIPIDEMIA
• Single or multiple gene mutations
•Overproduction or defective clearance of TG and LDL cholesterol
•Underproduction or excessive clearance of HDL
SECONDARY FACTORS CONTRIBUTING TO DYSLIPIDEMIA
• Sedentary lifestyle• Excessive dietary intake of saturated fat,
cholesterol, and trans fat (processed foods).• Diabetes mellitus • Alcohol overuse• Chronic kidney disease• Hypothyroidism• Biliary cirrhosis
DISEASE PREVENTION & TREATMENT (NUTRITION)
Prevention
• Lifestyle changes can involve diet and exercise.
• Dietary changes include: oDecreasing intake of saturated fats and
cholesterol.o Increasing the proportion of dietary fiber,
and complex carbohydrates.
o Maintaining ideal body weight..
DISEASE PREVENTION & TREATMENT CONT…
Treatment
• If the patient has high blood pressure, first step is to lower LDL cholesterol.
• Second step is to manage risk factors for metabolic syndrome & other lipid risk factors
PROGRAM ADHERENCE RECOMMENDATIONS
• Make sure the patient has a clear understanding of therapeutic life changes.• Contact the patient weekly for the first 4 weeks
of the program & then monthly thereafter.• Set achievable goals.• Assess dietary intake.• Identify specific barriers to lifestyle changes.• Design a program that is reasonable, gradual,
and easily implemented.

CHAPTER 8CORONARY HEART
DISEASE
Fantasia Wilburn
Kaitlin Hudson
Ashley Andrews
Shantoria Easton
Jake Shouppe
Saurabh Narkhede
Group #3
November 1, 2011
OVERVIEW OF CORONARY HEART DISEASE
Coronary Heart Disease (CHD), also called ischemic heart disease, is a complex disease process that ultimately results in an imbalance in the amount of oxygen that is available to supply the heart compared to the demand that the heart requires to function properly
PREVALENCE OF CHD
• In 2002, 13 million Americans had CHD, 7.1 million of who had experienced an MI.• White males have the highest incidence of CHD
(8.9%) followed by black females (7.5%), black males (7.4%). Mexican-American males (5.6%), white females (5.4%), and Mexican-American females (4.3%).
PREVALENCE OF CHD CONT.
• Approximately 700,000 Americans would have new coronary attack and that 500,000 would have a recurrent attack was estimated for 2005.• Average age to experience a first heart attack for
American males is 66 years old and for American females is 71 years old.

PREVALENCE OF CHD CONT.
• In 2002, CHD caused 1 out of every 5 deaths in the United States.• CHD is the single largest killer if American males
and females and increasing.
ECONOMIC COSTS
• In 2005, it was estimated that the direct and indirect costs associated with CHD was $142 billion.

ENVIRONMENTAL RISK FACTORS LEADING TO CHD
• Smoking • Hypertension• High total cholesterol• High LDL cholesterol• Low HDL cholesterol
• High triglycerides• Diabetes mellitus• Obesity or overweight• Physical inactivity• Emotional stress• Male gender• Increasing age• Family history of CHD• High lipoprotein• High homocystiene
CHD PREVENTION AND TREATMENT
• Strategies for preventing CHD are approached in two ways, depending on the status of the patient.1. Primary prevention strategies2. Secondary prevention strategies
• Many of the prevention strategies are similar with respect to lifestyle modification
• Drug therapy differs between primary and secondary prevention
PRIMARY CHD PREVENTION
• Pharmacist and healthcare providers can encourage patients to participate in primary prevention strategies.• Excess body weight can lead to diseases that can also
increase CHD risk, such as hypertension, dyslipidemia, type 2 diabetes mellitus, and stroke. Weight-loss programs and activities, even at modest levels, have been shown to decrease the risk for these diseases therefore decrease the risk for CHD.• Nutrition plays an important role not only in weight
loss but also in controlling other risk factors for CHD such as hypertension and dyslipidemia

PRIMARY CHD PREVENTION CONT.
• Eating plans that consist of whole grains, fruits, and vegetables and that are high in fiber, calcium, and potassium and low in saturated fat and cholesterol are associated with decrease risk for CHD.• Physical inactivity is an independent risk factor
for CVD but can also contribute to increasing the incidence of other diseases as type 2 diabetes, hypertension, dyslipidemia, and obesity. Increasing the physical activity and fitness levels of individuals decrease the risk for CHD.
PRIMARY CHD PREVENTION CONT.
• Working with “healthy” patients to avoid risk factors for CHD is at the heart of primary prevention and is an area that all healthcare providers, including pharmacist, should spend more time doing.• Helping patients maintain physical activity
and normal levels of blood pressure, blood lipids, and blood glucose are important concepts in the prevention of diseases.

SECONDARY CHD PREVENTION
• Approximately 70% of deaths from CHD and one half of MIs occur in patients with previously established CHD.• Instituting strategies for secondary CHD
prevention is major opportunity to reduce the risk for cardiovascular disease.• The Pharmacist’s role in the secondary
prevention of patients with CHD who have not yet attended a cardiac rehabilitation program is to encourage such participation and help monitor drug therapy associated with the disease

BEHAVIOR THERAPY
• Strategies to enhance program adherence for patients risk for CHD and for those who currently have CHD largely focus around patient education.
• Most individuals who do not currently have CHD do not understand the importance of implementing strategies such as lifestyle modification.
• Spreading the word about primary disease prevention can be a part of every healthcare providers’ responsibilities.
• Pharmacist can support both primary and secondary CHD prevention by educating patients about their importance

NUTRITION AND CHD
• The goal is to adopt the necessary dietary changes to decrease the risk for CHD.
• The dietary recommendation primarily focus on the promoting health and reducing risk for CHD and other chronic diseases by lowering low-density lipoprotein cholesterol (LDL) and blood pressure.
• Lowering the LDL cholesterol through dietary modifications can most successfully be accomplished by reaching the dietary intake of saturated of saturated fats, trans fatty acids, and cholesterol.
• The overarching themes are to rat fewer calories, be more physically active, and make wiser food choices.
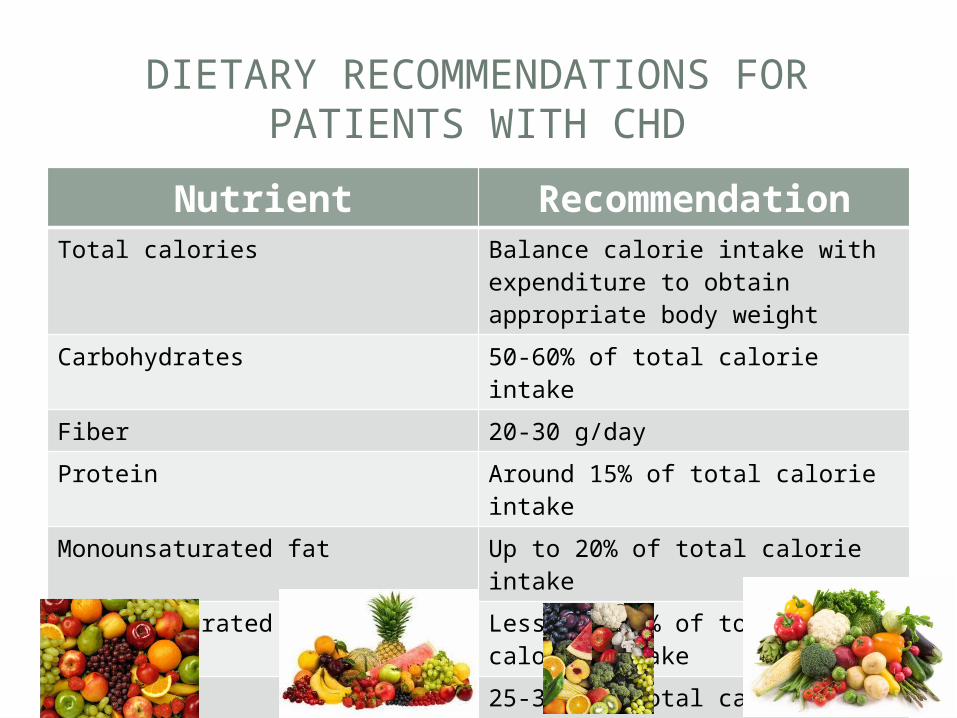
DIETARY RECOMMENDATIONS FOR PATIENTS WITH CHD
Nutrient RecommendationTotal calories Balance calorie intake with
expenditure to obtain appropriate body weight
Carbohydrates 50-60% of total calorie intake
Fiber 20-30 g/day
Protein Around 15% of total calorie intake
Monounsaturated fat Up to 20% of total calorie intake
Polyunsaturated fat Less than 7% of total calorie intake
Total fat 25-35% of total calorie intake
Dietary cholesterol Less than 200 mg/day

PHYSICAL ACTIVITY AND CHD
• It is well established that regular amounts of aerobic physical produce cardiovascular changes that increase exercise capacity, endurance, and muscular strength.
• Regular exercise also prevents the incidence of CHD and helps to decrease the symptoms associated with cardiovascular disease.
• Exercise can decrease the risk for and aid in controlling chronic diseases that can lead to CHD such as obesity, type 2 diabetes, hypertension, and dyslipidemia ,as well as other diseases such as osteoporosis. Depression, breast cancer, and colon cancer.

PHYSICAL ACTIVITY AND CHD CONT.
• The studies have shown that individuals who participate in physical activity generally experience a CHD rate that is half of sedentary individuals.• Individuals should engage in 30 minutes or more a
day of moderate intensity physical activity on most(preferably all) days of the week.• Patients with existing CHD should perform exercise
under supervision of cardiac rehabilitation facility as these patients may pose additional risks while exercising compared with individuals without CHD.

PHYSICAL ACTIVITY RECOMMENDATIONS FOR PATIENTS WITH CHD
Exercise RecommendationGoals Decrease risk for CHD and CVD
Decrease risk factors for CHD and CVD such as elevated blood pressure, insulin resistance and glucose intolerance, elevated triglyceride concentrations, low HDL-C concentrations, obesity, stroke, myocardial functionIncrease exercise peak workload and endurance
Type Aerobic exercises such as walking, jogging, running, cycling, or individual aerobic exercise preferenceResistance running can be adjunctive to aerobic exercises
Intensity Moderate-intensity endurance activity
Duration 30 minutes or more continuous or intermittent exercise per day
Frequency Most, preferably all, days of week
Lifestyle activity Increase overall daily activity through the duration of activities of daily living

35
CH 9 CANCER
G R O U P 9A N D R I A F RA Z I E RS H A N I C E WA L L E R
T O S H A B R O W NC H I N E LO O KA N YA LV I N L L A N O SC H A P T E R 1 5
N OV E M E B E R 1 5 , 2 0 1 1

36
WHAT IS CANCER
• Cancer is characterized as an uncontrolled growth and spread of abnormal cells• Most are categorized by their development such
as• Carcinoma• Leukemia• Lymphoma• Sarcoma
37
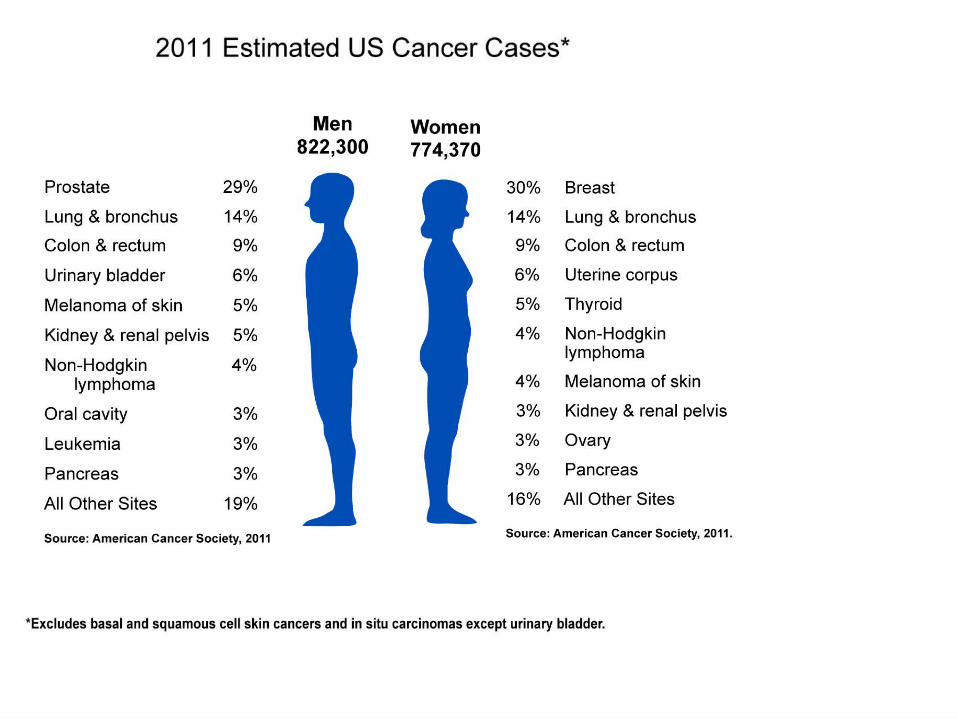
PREVALENCE
• Cancer is the 2nd most common cause of death in the US• Cancer accounted for 564,000 death is 2006• The most commonly diagnosed types• Prostate• Breast• Lung• Colon
38
RISK OF CANCER
• Men • Developing cancer 46%• Dying from cancer 24%
• Women• Developing cancer 38%• Dying from cancer 20%
40
RISK FACTORS
• Genetics• Environmental• Occupational• Medication• DES, diethylstilbestrol and cervical cancer
• Lifestyle activity factors
41
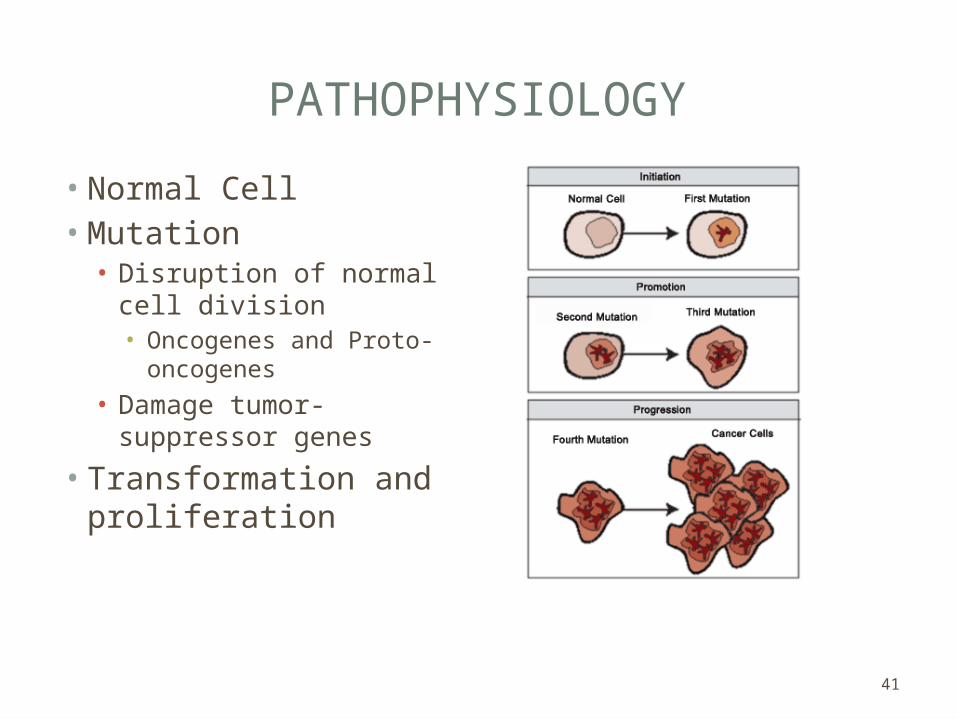
PATHOPHYSIOLOGY
• Normal Cell• Mutation• Disruption of normal cell
division • Oncogenes and Proto-
oncogenes
• Damage tumor-suppressor genes
• Transformation and proliferation

42
PREVENTION AND TREATMENT
• Genetic predisposition• Lifestyle modifications• Smoking 30% of cancer deaths annually• Physical inactivity, obesity, improper nutrition 30% of
cancer deaths
• Treatment and recommended adherence programs
43
WEIGHT
• Obesity results from a diet high in saturated fats and inactivity • It is linked to • Risk of endometrial cancer• High estrogens levels• Polycystic ovary syndrome (PCOS)
• Postmenopausal women• Primary source of estrogens is from the conversion of
androgens to estrogens within adipose tissue.
44
• Rich fruits and vegetables diet• Vegetarians
• Vitamin recommendations• Multi-vitamin pill• Vitamin E (400 IU daily)• Has both a cancer reducing as well
as a heart protective effect.
DIET
45
PHYSICAL ACTIVITY
• Exercise should be a PRIORITY throughout your treatment and recovery• improves quality of life • reduces fatigue • increases physical functioning.
• Exercise can improve mental health• improve self-image• decreases stress and anxiety • gives you a sense of control over cancer.
46
CHAPTER 10:PERIPHERAL
ARTERIAL DISEASE
S E C T I O N 3 0 1G R O U P 5
L AT R I C E W I L S O NT R E V E N A FAVO R SA M E T H Y S T S M I T HA M B E R B A L BO S A
D O N N I E RAY J O H N S O NM O N I C A N I C O L A
November 8, 2011
47
WHAT IS PERIPHERAL ARTERIAL DISEASE (PAD)?
• Also known as • Atherosclerosis of the Lower Extremity Arteries• Peripheral Vascular Disease• Lower Extremity Arterial Disease
• Narrowing of the arteries as a result of plaque formation• A systemic disease• Traditionally diagnosed as the presence of lower
extremity pain with exertion, often called claudication, absent or markedly diminished pulses on physical examination

48
SYMPTOMS
• May Be Asymptomatic• Claudication• Painful cramping in your hip, thigh or calf
muscles after activity, such as walking or climbing stairs• Leg numbness or weakness• Hair loss or slower hair growth on your feet
and legs• No pulse or a weak pulse in your legs or
feet• Sores on your toes, feet or legs that won't
heal
49
PREVALENCE
• PAD: 3.9% of men and 3.3% of women between the ages of 55 to 64 years and 65 to 74 years respectively
• Claudication: 1.9% of men and 0.8% of women
• 20% of people have PAD by 75 years of age

50
RISK FACTORS
• Age- 40 and older• Gender• Family History • Racial Background
51
MODIFIABLE RISKS FACTORS
• Smoking• Diabetes• Dyslipidemia• Hypertension• Physical Inactivity
52
RISKS FOR PATIENTS WITH PAD
• Cardiovascular Disease• Myocardial Infarction• 4x greater than people without PAD
• Stroke• 2-3x greater risk than those without Pad
• 85% have coronary heart disease• 60% have cerebrovascular disease• Carotid Artery Stenosis

53
BEHAVIOR CHANGES RELEVANT TO PAD
• Exercise• Aerobic, such as walking, jogging, running, or cycling• At least 30 minutes of continuous or intermittent activity
• Proper Nutrition• Balance caloric intake with expenditure to obtain
appropriate body weight • Carbohydrates: 50-60% of caloric intake• Fiber: 20-30g/day• Protein: 15% of total caloric intake • Total Fat: 25-35% of total caloric intake

54
PRIMARY PREVENTION
• Patients who do not have PAD, but possess risk factors for the disease• Strategies:• Smoking cessation programs (for smokers)• Weight loss programs• Nutrition regiments
55
SECONDARY PREVENTION
• Patients who currently have PAD• Strategies include:• Smoking cessation programs (for smokers)• Weight loss programs• Nutrition regiments• Drug Regiments• Blood glucose, blood pressure, and blood lipid
management
56
PREVENTION:PROGRAM ADHERENCE RECOMMENDATIONS
• Ensure patient’s understanding of PAD and prevention components• Multiple adherence strategies work better
than a single approach• Weekly contact with patients for the first
weeks, and then continually assess monthly progress• Set achievable goals to manage and
prevent PAD
57
COMPLICATIONS
• Critical Limb Ischemia• This condition begins as open sores that don't heal, an
injury, or an infection of your feet or legs. Critical limb ischemia (CLI) occurs when such injuries or infections progress and can cause tissue death (gangrene), sometimes requiring amputation of the affected limb.
• Stroke • Heart Attack
58
TREATMENT
• Exercise• Proper Nutrition• Medications• Anti-hypertensives• Lipid lowering drugs• Diabetes therapies• Smoking Cessation• Anti-platelet drugs
• Angioplasty• Bypass Surgery• Thrombolytic Surgery
Related Documents











