MUSCULOSKELETAL SECTION Original Research Article Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability and Improves Neck Movement in Individuals with Chronic Whiplash Ashley Dean Smith, PT,* † Gwendolen Jull, PhD,* Geoff Schneider, PhD, †‡§ Bevan Frizzell, MD, ‡¶ Robert Allen Hooper, MD, †‡ and Michele Sterling, PhD** *Division of Physiotherapy, NHMRC Centre of Clinical Excellence Spinal Pain, Injury and Health, University of Queensland, Brisbane, Queensland, Australia; † Advanced Spinal Care Centre, Calgary, Alberta; ‡ Faculty of Medicine, University of Calgary, Calgary, Alberta; § LifeMark Health, Calgary, Alberta; ¶ Advanced Spinal Care Centre (EFW Radiology), Calgary, Alberta, Canada; **Centre of National Research on Disability and Rehabilitation Medicine, University of Queensland, Brisbane, Queensland, Australia Reprint requests to: Ashley Dean Smith, PT, Evidence Sport & Spinal Therapy, 201, 2000 Veteran’s Place NW, Calgary, AB, Canada T3B 4N2. Tel: 403-210-9969; Fax: 403-210-9084; E-mail: [email protected] Funding: MS receives a fellowship from the National Health and Medical Research Council of Australia. No funding sources were utilized for this study. Conflict of Interest: The authors do not have any conflicts of interest to disclose. Abstract Objective. This study aims to determine if cervical medial branch radiofrequency neurotomy reduces psychophysical indicators of augmented central pain processing and improves motor function in individuals with chronic whiplash symptoms. Design. Prospective observational study of con- secutive patients with healthy control comparison. Setting. Tertiary spinal intervention centre in Calgary, Alberta, Canada. Subjects. Fifty-three individuals with chronic whip- lash associated disorder symptoms (Grade 2); 30 healthy controls. Methods. Measures were made at four time points: two prior to radiofrequency neurotomy, and 1- and 3-months post-radiofrequency neurotomy. Measures included: comprehensive quantitative sensory testing (including brachial plexus provocation test), nociceptive flexion reflex, and motor function (cervi- cal range of movement, superficial neck flexor activ- ity during the craniocervical flexion test). Self-report pain and disability measures were also collected. One-way repeated measures analysis of variance and Friedman’s tests were performed to investigate the effect of time on the earlier measures. Differences between the whiplash and healthy control groups were investigated with two-tailed independent samples t-test or Mann–Whitney tests. Results. Following cervical radiofrequency neu- rotomy, there were significant early (within 1 month) and sustained (3 months) improvements in pain, dis- ability, local and widespread hyperalgesia to pres- sure and thermal stimuli, nociceptive flexor reflex threshold, and brachial plexus provocation test responses as well as increased neck range of motion (all P < 0.0001). A nonsignificant trend for reduced muscle activity with the craniocervical flexion test (P > 0.13) was measured. Conclusions. Attenuation of psychophysical mea- sures of augmented central pain processing and Pain Medicine 2014; 15: 128–141 Wiley Periodicals, Inc. 128

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MUSCULOSKELETAL SECTION
Original Research ArticleCervical Radiofrequency Neurotomy ReducesCentral Hyperexcitability and ImprovesNeck Movement in Individuals withChronic Whiplash
Ashley Dean Smith, PT,*† Gwendolen Jull, PhD,*Geoff Schneider, PhD,†‡§ Bevan Frizzell, MD,‡¶
Robert Allen Hooper, MD,†‡ and Michele Sterling,PhD**
*Division of Physiotherapy, NHMRC Centre of ClinicalExcellence Spinal Pain, Injury and Health, Universityof Queensland, Brisbane, Queensland, Australia;
†Advanced Spinal Care Centre, Calgary, Alberta;
‡Faculty of Medicine, University of Calgary, Calgary,Alberta;
§LifeMark Health, Calgary, Alberta;
¶Advanced Spinal Care Centre (EFW Radiology),Calgary, Alberta, Canada;
**Centre of National Research on Disability andRehabilitation Medicine, University of Queensland,Brisbane, Queensland, Australia
Reprint requests to: Ashley Dean Smith, PT, EvidenceSport & Spinal Therapy, 201, 2000 Veteran’s PlaceNW, Calgary, AB, Canada T3B 4N2.Tel: 403-210-9969; Fax: 403-210-9084;E-mail: [email protected]
Funding: MS receives a fellowship from the NationalHealth and Medical Research Council of Australia.No funding sources were utilized for this study.
Conflict of Interest: The authors do not have anyconflicts of interest to disclose.
Abstract
Objective. This study aims to determine if cervicalmedial branch radiofrequency neurotomy reduces
psychophysical indicators of augmented centralpain processing and improves motor function inindividuals with chronic whiplash symptoms.
Design. Prospective observational study of con-secutive patients with healthy control comparison.
Setting. Tertiary spinal intervention centre inCalgary, Alberta, Canada.
Subjects. Fifty-three individuals with chronic whip-lash associated disorder symptoms (Grade 2); 30healthy controls.
Methods. Measures were made at four time points:two prior to radiofrequency neurotomy, and 1- and3-months post-radiofrequency neurotomy. Measuresincluded: comprehensive quantitative sensorytesting (including brachial plexus provocation test),nociceptive flexion reflex, and motor function (cervi-cal range of movement, superficial neck flexor activ-ity during the craniocervical flexion test). Self-reportpain and disability measures were also collected.One-way repeated measures analysis of varianceand Friedman’s tests were performed to investigatethe effect of time on the earlier measures. Differencesbetween the whiplash and healthy control groupswere investigated with two-tailed independentsamples t-test or Mann–Whitney tests.
Results. Following cervical radiofrequency neu-rotomy, there were significant early (within 1 month)and sustained (3 months) improvements in pain, dis-ability, local and widespread hyperalgesia to pres-sure and thermal stimuli, nociceptive flexor reflexthreshold, and brachial plexus provocation testresponses as well as increased neck range ofmotion (all P < 0.0001). A nonsignificant trend forreduced muscle activity with the craniocervicalflexion test (P > 0.13) was measured.
Conclusions. Attenuation of psychophysical mea-sures of augmented central pain processing and
bs_bs_banner
Pain Medicine 2014; 15: 128–141Wiley Periodicals, Inc.
128

improved cervical movement imply that theseprocesses are maintained by peripheral nocicep-tive input.
Key Words. Whiplash; Radiofrequency Neurotomy;Central Sensitization; Quantitative Sensory Testing;Peripheral Nociception
Introduction
Approximately 50% of individuals who sustain a whiplashinjury will continue to report ongoing neck pain and dis-ability 12 months later [1]. Chronic whiplash-associateddisorder (WAD) is characterized by sensory disturbances(widespread hypersensitivity) [2–4] and heightened spinalcord flexor withdrawal responses [5,6], both indicative ofaugmented central nociceptive processing [7]. Changes inmotor function are also evident with reduced neckrange of movement and altered muscle recruitmentpatterns [8,9].
The processes underlying and contributing to these fea-tures are not clear. While it is generally accepted thatsensory features result from augmented central nocicep-tive processing (central hyperexcitability) [10,11], there ismuch debate as to whether these are driven by anongoing peripheral nociceptive source [12–14] or are self-maintaining due to neuroplastic changes in the centralnervous system [7]. Previous studies of patients withpainful hip or knee osteoarthritis demonstrated improve-ment in sensory measures following successfularthroplastic surgery, indicating that central pain pro-cesses are being maintained by peripheral nociceptiveinput [15,16].
Similarly, persistence of motor changes following whiplashinjury, such as morphometric muscular changes, localmuscular weakness, and loss of range of movement, sug-gests the presence of ongoing peripheral mechanisms[17–21]. However, these changes cannot be separatedfrom changes in central nervous system control, with neu-romotor performance in individuals with neck pain asso-ciated with reorganization of control strategies [22–24].
While tissue damage usually cannot be detected in thepatient with WAD with current imaging techniques, evi-dence to date suggests that a peripheral lesion of somekind is likely to be present [25–27]. Most available evi-dence would support the cervical facet joint as one sourceof nociception in individuals with chronic WAD [28–30].Animal studies have demonstrated that cervical facetjoint injury may be responsible for hypersensitivity andincreased neuronal excitability [31–34]. Injury to the facetjoint has also been implicated in local muscle responses ina cat model [35]. Modulating nociception from facet jointsis possible via medial branch blocks (MBBs) orradiofrequency neurotomy (RFN). There are suggestionsthat MBB or RFN may attenuate sensory hypersensitivity[36–38]; although the evidence is weak, with studies
involving limited subjects, measures or procedures; oronly investigating immediate post-procedure effects.Thus, the role of the cervical facet joint in regard tosensory and motor changes in chronic WAD requiresfurther investigation, with a wider range of measures ofcentral hyperexcitability and inclusion of measures ofmotor function.
The aim of this study was to investigate changes in mea-sures of central hyperexcitability following RFN of cervicalspine facet joints in individuals with chronic WAD. We alsoinvestigated changes in motor function following the sameprocedure. The null hypothesis was that reducingnociception via RFN would not result in changes in psy-chophysical indicators of central hyperexcitability orchanges in motor function.
Methods
Design
A prospective cohort study design was employed at atertiary spinal intervention centre in Calgary, Alberta,Canada. Participants included individuals with chronicWAD who underwent RFN, following a successfulresponse to cervical facet joint blockade. A healthy control(HC) cohort was also investigated to provide comparativedata. Individuals with WAD attended the research labora-tory at four time points: 1 month following cervical facetjoint injections (double blockade procedure), immediatelyprior to receiving RFN, 1 month following RFN, and 3months following RFN. HC individuals attended onesession of laboratory testing.
Participants
Inclusion Criteria
Consecutive participants were recruited from individualsaged 18–65 years with WAD Grade II [39] of a durationgreater than 6 months post-motor vehicle collision (MVC)following successful response (greater than 50% of neckpain relief) to cervical facet joint blockade (intra-articularblock followed by confirmatory MBB) [40], who subse-quently underwent RFN.
HC individuals with no previous history of neck pain, whip-lash injury, or recent treatment for musculoskeletal pain(within previous 2 years) were recruited from advertise-ments placed around the spinal intervention centre.
Exclusion Criteria
Individuals were excluded from the study if they wereclassifiable as WAD Grade III (neurological deficit) or IV(fracture or dislocation) [39], sustained a concussion orloss of consciousness as a result of the trauma, or if theywere not fluent in spoken or written English.
All the participants were unpaid volunteers. Ethical clear-ance for this study was granted from the institutional
129
Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability

medical research ethics committees (University of Calgaryand University of Queensland) in 2009. All participantsprovided informed consent.
Outcome Measures
Quantitative Sensory Tests
Pressure Pain Thresholds. Pressure pain thresholds(PPTs) were measured using a pressure algometer(Somedic AB, Farsta, Sweden). The probe size was 1 cm2,and the rate of application was 40 kPa/s. PPTs weremeasured over the articular pillars of C5/6 bilaterally (whichis the most prevalent facet joint involved in neck pain [notinvolving headaches] following whiplash trauma) [30], overthe median nerve trunks anterior to the elbow bilaterally,and at a bilateral remote site (upper one third of the musclebelly of tibialis anterior) as previously described in inves-tigations of chronic WAD [4]. The participants wererequested to push a button when the sensation of pressurefirst became painful. Three recordings were taken at eachsite and the mean value for each site used in the analysis.
Nociceptive Flexion Reflex. The nociceptive flexion reflex(NFR) is a polysynaptic spinal withdrawal reflex that iselicited following activation of nociceptive A-delta afferents[41]. It was performed via electrical stimulation throughbipolar surface Ag/AgCl electrodes (interelectrode dis-tance approximately 2 cm), which were placed just distalto the left lateral malleolus of the ankle (innervation areaof the sural nerve). Electromyography (EMG) reflexresponses to electrical stimulation were recorded from themiddle of the biceps femoris muscle using Ag/AgCl elec-trodes. The participant lay prone, and a wedge wasplaced under the ankle to obtain 30 degrees knee flexion.The EMG signal was amplified and low-pass filtered0–500 Hz by a multichannel EMG (Noraxon, Scottsdale,AZ, USA). Stimulation and recording was controlled andanalyzed with custom software developed specifically forthis test. A 25-millisecond, train-of-five, 1-millisecond,square-wave impulse (perceived as a single stimulus), wasdelivered by a computer-controlled constant currentstimulator (Digitimer DS7A, Hertfordshire, England).
The current intensity was increased from 2 mA in steps of2 mA until a reflex was elicited. The program delivered theimpulses at random time intervals, so that the participantswere not aware of when the stimulus was going to beapplied. In this way, voluntary muscle contraction due tostimulus anticipation was avoided. A reflex response wasdefined using the standardized peak (NFR interval peak zscore) EMG activity from biceps femoris as recommended[42]. The NFR interval peak z score is the NFR interval peak(EMG activity 90–150 milliseconds post-stimulation inter-val)—baseline mean (60 milliseconds before stimulation)/baseline standard deviation (SD). Rhudy and France [42]suggest an NFR interval peak z score of greater than 10.32be used to define a reflex response. The 90- to 150-millisecond interval was chosen as it avoids possible con-tamination by low threshold cutaneous flexor reflex, startle
reactions, and voluntary movements [43]. The currentintensity required to elicit a reflex response was defined asthe NFR threshold.
Thermal Pain Thresholds. Thermal pain thresholds weremeasured bilaterally over the cervical spine using the TSAII Neurosensory Analyzer (Medoc Advanced MedicalSystems; Minneapolis, MN, USA). The thermode wasplaced over the skin of the mid-cervical region and presetto 32°C, with the rate of temperature change being 1°C/s.To identify cold pain thresholds (CPTs) and heat painthresholds (HPTs), participants were asked to push aswitch when the cold or warm sensation first becamepainful [44]. Triplicate recordings were taken at each site,and the mean value for each site was used in the analysis.
Brachial Plexus Provocation Test. The brachial plexusprovocation test (BPPT) was performed in the followingsequence: gentle shoulder girdle depression, glenohu-meral abduction and external rotation in the coronalplane, forearm supination, wrist and finger extension,and elbow extension [45]. The range of elbow extensionwas measured at the participants’ pain threshold using astandard goniometer aligned along the mid-humeral shaft,medial epicondyle, and ulnar styloid [46]. If the participantdid not experience pain, the test was continued until end ofavailable range. Hypersensitive responses to this test havebeen demonstrated in chronic whiplash [47,48], and thetest has excellent intratherapist reliability [49].
Motor Measures
Range of Motion. Active cervical range of motion (ROM)was measured using electromagnetic motion sensors(Fastrak, Polhemus, Colchester, VT, USA) [8]. One sensorwas placed over the C7 spinous process and the otherattached to the top of a light skull cap firmly fitted to theparticipant’s head, such that the second sensor sat on thevertex. Three trials were performed in each direction(flexion, extension, left and right rotation) and the means ofthe three trials were used in analysis. A computer programwas developed to convert the Euler angles into degrees offreedom of motion of the vertex relative to C7. The Fastrakhas previously been used in trials of neck pain and whip-lash participants [50] and has shown to be accurate within±0.2 degrees [51].
Craniocervical Flexion Test. Surface EMG (Noraxon TeleMyo 900) was used to measure the activity of superficialneck flexor muscles (sternocleidomastoid, SCM) duringthe five incremental stages of the craniocervical flexiontest (CCFT) as described by Jull et al. [9]. The test wasperformed in supine and used a pressure biofeedbackdevice (Stabilizer, Chattanooga, TN, USA) placed suboc-cipitally behind the neck to guide performance. It wasinflated to a baseline of 20 mm Hg, and participants per-formed craniocervical flexion to increase the pressure byfive progressive increments of 2 mm Hg (22–30 mm Hg).Each pressure level was maintained for 10 seconds, andparticipants rested for 15 seconds between each stage.Myoelectric signals were collected from the SCM muscles
130
Smith et al.

using Ag–AgCl electrodes (Noraxon) in a bipolar configu-ration (interelectrode distance approximately 2 cm).
Electrodes were positioned along the lower one-third ofthe muscle bellies of the SCM [52]. Signals were amplifiedand filtered by a 500 Hz low pass filter (Noraxon TeleMyo900) and sampled at 2,000 Hz (National Instruments DAQPCI-6221). EMG data were analyzed as follows: Themaximum root mean square (RMS) value was identified foreach trace using a 1-second sliding window, incrementedin 100-millisecond steps. RMS values were normalized foreach participant, by dividing the 1 second maximum RMSfrom each level of the CCFT by the 1 second maximumRMS during a standardized head lift. The baseline EMGdata (RMS value) obtained at rest (20 mm Hg) was sub-tracted from the measured EMG at each level of this test.The normalized RMS data for the left and right SCMs wereaveraged for analysis [9,50].
Questionnaires
Measures included a description of symptoms, symptomdominance (unilateral or bilateral), and severity, crashparameters, treatments since the crash, compensationstatus, list of medications, and demographic variablesincluding gender, age, marital status, employment status,education level, and duration of neck pain as per a stan-dard clinical examination.
A single item visual analog scale (VAS; 0–10 cm) was usedto measure participants’ current pain intensity in the cer-vical spine (defined as the posterior region of the cervicalspine from the superior nuchal line to the first thoracicspinous process) with (0) described as “No Pain” and (10)as “Worst Pain Imaginable.”
Self-reported pain and disability was measured in whip-lash participants with the Neck Disability Index (NDI) [53].The NDI consists of 10 items addressing functional activi-ties such as personal care, lifting, reading, work, driving,sleeping, and recreational activities and also pain intensity,concentration, and headache, which are rated from nodisability (0) to total disability (5). The overall score (out of100) is calculated by totaling the responses of each indi-vidual item and multiplying by 2. A higher score indicatesgreater pain and disability. It is the questionnaire mostutilized in WAD research [54].
Procedure
Participants were assessed on all outcome measures at thefollowing time points: t(1) at a time period when their familiarbaseline neck pain was present (when symptoms returnedfollowing successful cervical facet joint double blockade)[38]; t(2): immediately prior to receiving RFN; t(3): 1 monthfollowing RFN; and t(4): 3 months following RFN. Atten-dance at two time points prior to receiving RFN allowed usto determine if time alone (t(1) vs t(2)) resulted in improve-ments in measures prior to RFN being performed.
Participants first completed all questionnaires, after whicha standard protocol was used for the order of tests [55].
The participants were seated, the Fastrak sensorsapplied, and ROM was measured. They were instructed toassume a comfortable position looking straight ahead,then to perform each movement three times, moving at acomfortable speed as far as possible and to return to thestart position between each repetition. The order of move-ments assessed were flexion, extension, left rotation, andright rotation. The participants were then positionedsupine, EMG electrodes were applied, and the CCFT wasperformed. For all of the following bilateral tests, the leftside was measured first. PPTs were measured in the fol-lowing order: tibialis anterior, median nerves, and C5/6.Thermal pain thresholds were then measured over thecervical spine, HPTs followed by CPTs. These were fol-lowed by the BPPT. The NFR was the final testing proce-dure. The same examiner tested all participants. Nofeedback or cues were given to the participants regardingtheir performance on any tests.
RFN Procedure
Details of the RFN procedure are provided in Appendix 1.
Data Analysis
Data were analyzed with Stata 9.0 statistical software.Based on our previous research [38], utilizing the SD ofchanges observed (in distal PPT pre-/post-interventionalprocedure), our statistical calculations indicated that thisstudy required 26 participants (with 80% power at 5%level of significance) to adequately detect a minimally clini-cally important difference for the primary outcome mea-sures (change in PPT in tibialis anterior, change in CPT, orchange in NFR threshold). Extra participants wererecruited in the whiplash group to power a further study.
Assumptions of normality, nonmulticollinearity, andhomoscedasticity were tested through examination of his-tograms, box plot graphs, correlation matrices, and a plotof predicted to residual values, respectively. If the datawere not normally distributed, transformation of thedata was applied. PPT, BPPT, NFR threshold, and CCFTdata required log transformation. Despite various transfor-mations being attempted, normality for CPT and HPT wasunable to be achieved (primarily due to floor and ceilingeffects). A paired t-test was used to determine withinparticipant side-to-side differences for all measures andfollowed by the exploratory analysis for all the measures.As no side-to-side differences were found (PPT, CPT, HPT,and BPPT), the data from each side were averaged andthe mean data used for analysis.
All assumptions for repeated measures analysis of vari-ance (ANOVA) were satisfied, except for HPT and CPT.One-way repeated measures ANOVA was performed toinvestigate the effect of time (four levels: 1 month followingcervical facet blockade; 1 month prior to receiving RFN; 1month following RFN, and 3 months following RFN) on thefollowing log-transformed measures: PPT, BPPT, NFR,and CCFT, and normally distributed ROM. NonparametricFriedman’s repeated measures test was used to analyze
131
Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability

the effects of time on CPT and HPT. The baseline data foreach dependent measure was entered into each ANOVA(but not Friedman’s) analysis as a covariate. As this did notalter the significance of any of the results, further mentionof baseline adjustment will not be made.
For ease of interpretation, results are presented usingnontransformed data for medians and interquartile ranges,with probability estimates taken from analyses usingtransformed data. Where there was a significant differenceover time, post-hoc tests of simple effects were per-formed to determine where these differences occurred.Significance level was set at 0.05 with Bonferroni adjust-ments used where appropriate. When the Friedman testwas significant, multiple Wilcoxon signed-rank tests wereperformed with Bonferroni adjustment (P < 0.008) utilizedto determine where those differences occurred. Differ-ences between the whiplash and HC groups were inves-tigated with two-tailed independent samples t-test orMann–Whitney tests (for CPT and HPT, respectively).
The data were assessed for effect size using Cohen’s d fornormally distributed data and Cliff’s Delta for nonparamet-ric analyzed data [56]. The established convention rateswere used. A Cohen’s d effect size of 0 < 0.50 is small, asize of 0.50 to <0.80 is moderate, and >0.80 is large [57].The corresponding effect sizes for Cliff’s Delta are: <0.147is small; between 0.148 and 0.33 is moderate, and >0.33is large [58]. Effect size was calculated utilizing t(4), beingthe primary end point of this study; and t(2), the timeperiod immediately prior to receiving RFN.
Results
Participants
Fifty-eight individuals had a successful response to thecervical facet joint blockade (intra-articular block followedby MBB) and agreed to participate in the study. Fourindividuals subsequently withdrew before undergoing RFN(three individuals declined to proceed with RFN, and oneindividual sustained other traumatic injuries from a skiingaccident). Thus, 54 individuals underwent RFN.
At the 1 month review period following RFN (t(3)), oneindividual sustained neuritis (this was the only side effectnoted for the duration of the study), and thus was unableto attend for further analysis. Thus, 53 individuals (36female, 17 male; mean age = 44.7 ± 10.9 [SD] years) wereincluded in the study. Three individuals were unable toattend the 3-month review (one pregnancy, two lost tofollow-up), although all data until that point was included inthe analysis.
The collision vectors reported were: rear-end impacts(51%), frontal impacts (23%), side impacts (21%), andcombined (6%) vectors. Twenty-eight participants (53%)were involved in ongoing compensation claims, 30 (57%)reported the presence of other musculoskeletal symp-toms (i.e., headaches [44%], low back pain [34%], tho-racic spine pain [21%], shoulder/arm pain [21%], and jaw
pain [8%]), 27 (51%) were university educated, 41 (77%)were fully employed throughout the course of the study,and 39 (74%) reported that they were married or in along-term supportive relationship.
The median (range) duration of symptoms post-whiplashinjury was 43 (9–195) months. Following the initial cervicalfacet double blockade procedure, there was a mean (±SD)wait of 10.4 (±4.5) months until RFN was performed. Allparticipants received treatment following the MVC. Thirty-one participants (58%) were receiving conservative treat-ment at the time of participation in the study. Twenty-sixparticipants (49%) had previously attended the local healthauthority multidisciplinary chronic pain centre.
The most common facet joint implicated was C2/3 (41%),followed by C6/7 (28%) and C5/6 (24%). C3/4 (11%) andC4/5 (4%) were less common. Bilateral facet joints wereidentified in 31% of individuals, while in 36%, both anupper cervical (C2–4) and lower cervical intervertebralsegment (C4–7) were involved.
Following RFN, medication usage decreased as follows:anti-inflammatory medication (from 45% of individuals to36%), simple over-the-counter analgesics (from 34% to23%), various narcotic medications (from 26% to 19%),anticonvulsants (from 19% to 13%), selective serotoninreuptake inhibitors (from 13% to 8%), and tricyclic antide-pressants (from 13% to 6%), with slight increase in usageof selective norepinephrine reuptake inhibitors (8–13%).
Table 1 presents the demographic, pain, and disabilitycharacteristics for the participants at the four measure-ment time points.
Pain and Disability
Repeated-measures ANOVA revealed a significant maineffect of time for VAS (Table 1). Post-hoc tests of simpleeffects showed no significant difference in pain scoresbefore RFN (t(1) and t(2)), with early (t(3): 1 month followingRFN), and sustained (t(4): 3 months after receiving RFN)reductions in pain following RFN with no differencebetween t(3) and t(4). Similarly, there was a main effect oftime for NDI scores (Table 1). Post-hoc tests mirrored theresults for VAS scores, with reductions in self-reporteddisability following RFN, with no significant differences inthe time periods prior to or following RFN, respectively.The effect sizes were large for both pain (Cohen’s d: 1.34[95% confidence interval {CI} 1.13–1.55]) and disabilitymeasures (Cohen’s d: 1.00 [95% CI 0.79–1.21]).
PPTs
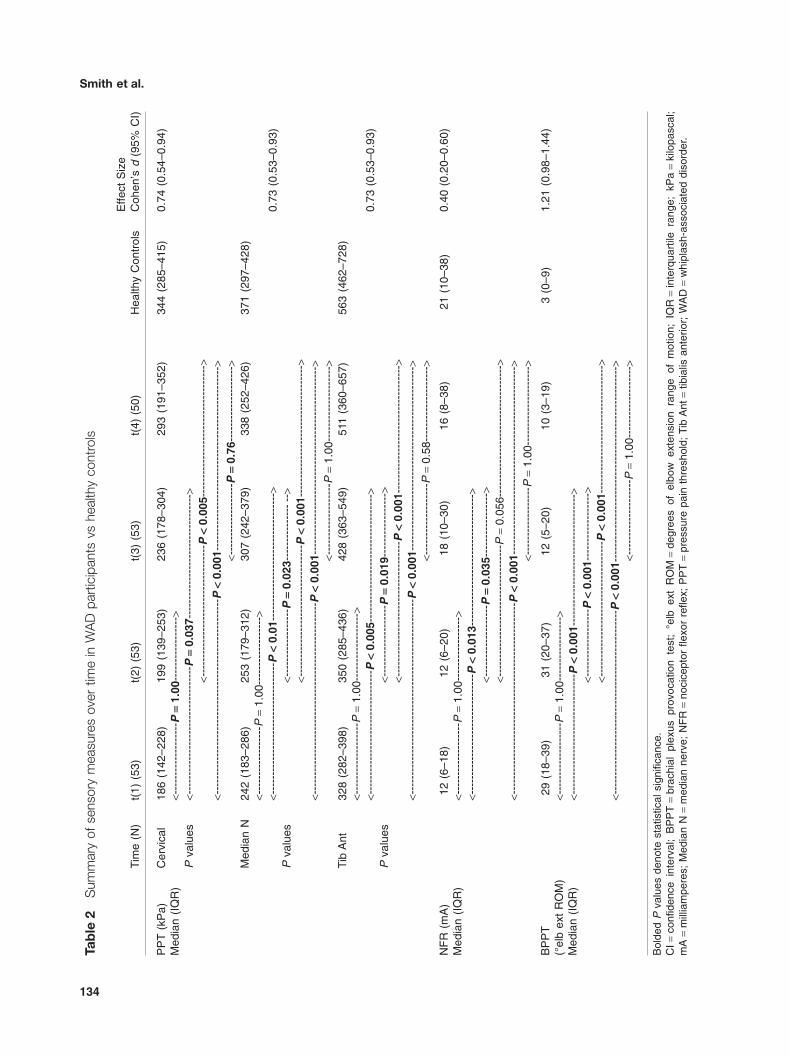
There was a significant main effect of time for PPT at allsites (Table 2). PPTs at tibialis anterior and median nervesites demonstrated early and sustained increases follow-ing RFN, with no difference in PPTs prior to or followingRFN. Similar results (early and sustained increasesfollowing RFN with no differences prior to or followingRFN) were demonstrated at the cervical spine site, with
132
Smith et al.

one slight difference, that being no significant differencemeasured between t(2) and t(3) (P = 0.27). The effect sizeswere moderate for all sites measured (Table 2).
In comparison with the HC group, PPTs at all sites werelower in the whiplash group prior to undergoing RFN (81df, P < 0.0001). Following RFN (t(4)), there were no differ-ences between the WAD group and controls at themedian nerve and tibialis anterior sites (78 df, P > 0.18),but PPT at the cervical spine remained lower in the WADgroup (t78 = 2.26, P = 0.013).
NFR
There was a significant main effect of time for NFR thresh-old (Table 2). Post-hoc tests showed that there was nosignificant difference in NFR thresholds before RFN. Therewas a significant increase in NFR thresholds between thetime periods prior to RFN, and following RFN (except fort(2) to t(4): P = 0.056). There were no significant differ-ences in NFR thresholds following RFN. The effect sizewas small: Cohen’s d = 0.40 (Table 2).
There was no significant difference between the HC groupand the whiplash group at t(4): t78 = 0.67, P = 0.51, butNFR threshold was lower in the WAD group prior to RFN(t(2): t81 = 2.97, P = 0.004).
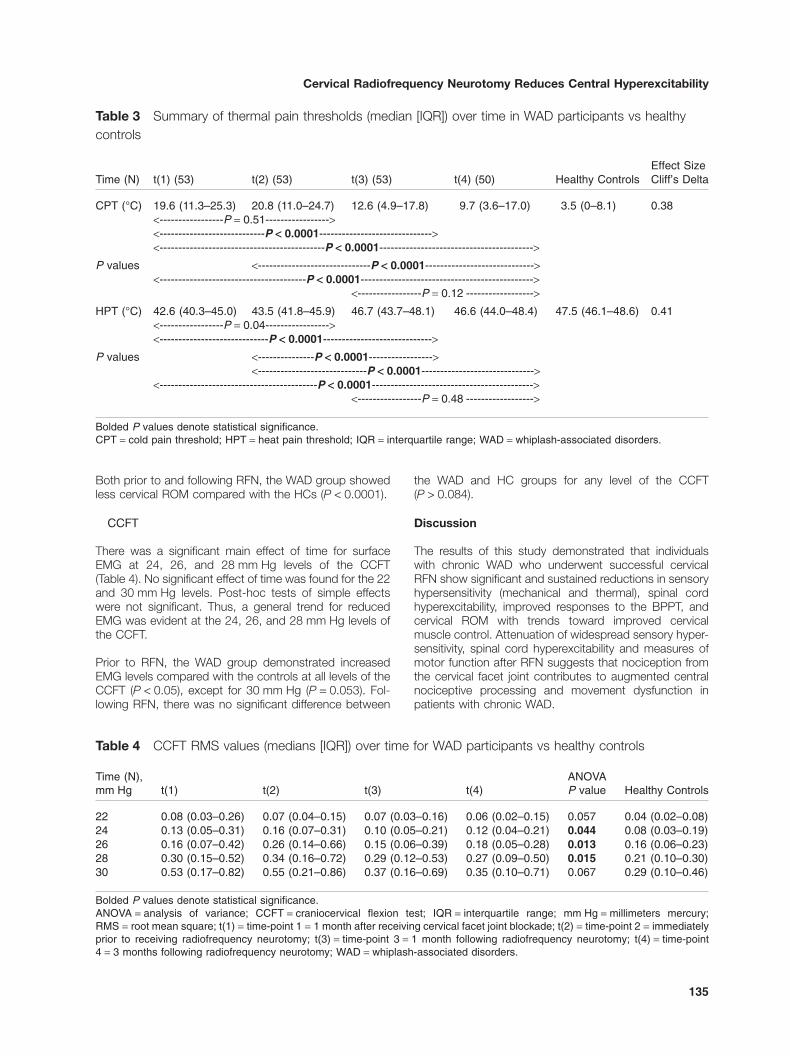
CPTs
There was a significant effect of time for CPT (Table 3).Post-hoc analyses revealed that significant reductions incold hyperalgesia (lower CPTs) were measured post-RFN.There were no significant differences in CPTs measuredbefore receiving RFN or following RFN. Effect sizes werelarge: Cliff’s Delta = 0.38.
Prior to undergoing RFN, the WAD group demonstrated asignificantly elevated CPT (20.8°C) compared withthe HCs (3.5°C, Table 2; Mann–Whitney U = −4.89,nWAD = 53, nHC = 30, P < 0.0001). At t(4), median CPTs in
the whiplash group were significantly higher than those ofcontrols (P = 0.003; Table 3).
HPTs
There was a significant time effect for HPT (Table 3). Post-hoc analysis revealed that significant increased HPTs fol-lowed RFN. There were no significant differences in HPTsmeasured in the time periods prior to or following RFN.The effect sizes were large: Cliff’s Delta = 0.41 (Table 3).
Prior to undergoing RFN, the WAD group showed lowerHPT compared with controls (Mann–Whitney U = 4.43,nWAD = 53, nHC = 30, P < 0.0001; Table 2), but therewas no difference between the groups following RFN(P = 0.17; Table 3).
BPPT
There was a significant main effect of time for elbowextension ROM with the BPPT (Table 2). Post-hoc analysisrevealed that there were no significant differences mea-sured prior to RFN. Elbow extension ROM increased fol-lowing RFN, but there were no significant differences inthe two time points following RFN. The effect size waslarge: Cohen’s d: 1.21 (Table 2).
The WAD group showed less elbow extension ROM com-pared with controls both prior to (t81 = −9.2, P < 0.0001)and following RFN (t67 = −2.61, P = 0.011; Table 2).
ROM
There were significant differences over time for cervicalROM (F3,153 = 104.4, P < 0.0001). Post-hoc analysisshowed no change in cervical ROM between t(1) and t(2)(P = 1.00), but cervical ROM significantly improved follow-ing RFN (both early: t(3) [P < 0.0001]; and 3 months later:t(4); P < 0.0001). No significant differences in ROM weremeasured between t(3) and t(4) (P = 1.00). A large effectsize was present: Cohen’s d: 1.78 (95% CI 1.52–2.04).
Table 1 Demographics of participants and changes in pain and disability over time in the WADparticipants
Gender (F/M) Age (yrs ± SD)
Duration of Symptoms VAS NDIMonths (median) (±SD) (±SD)(25–75) (0–100 mm) (%)
WAD: 36/17HC: 21/9
WAD: 44.7 (10.9)HC: 44.2 (9.7)
43 (30–69) t(1): 58 (19)‡ t(1): 42 (15)‡
t(2): 55 (19) t(2): 43 (16)t(3): 25 (20)*† t(3): 29 (16)*†
t(4): 25 (21)*†‡ t(4): 27 (16)*†‡
* P < 0.0001 (between t(1) and t(x)); † P < 0.0001 (between t(2) and t(x)); ‡ P = 1.00 (between t(1 and 2), or t(3 and 4), orpost-RFN).HC = healthy control; NDI = Neck Disability Index; SD = standard deviation; t(1) = time-point 1 (admission to study following cervicalfacet joint injection double blockade); t(2) = time-point 2 (immediately prior to receiving radiofrequency neurotomy); t(3) = time-point3 (1 month following radiofrequency neurotomy); t(4) = time-point 4 (3 months following radiofrequency neurotomy); VAS = visualanalog scale; WAD = whiplash-associated disorder.
133
Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability
Tab
le2
Sum
mar
yof
sens
ory
mea
sure
sov
ertim
ein
WA
Dpa
rtic
ipan
tsvs
heal
thy
cont
rols
Tim
e(N
)t(
1)(5
3)t(
2)(5
3)t(
3)(5
3)t(
4)(5
0)H
ealth
yC
ontr
ols
Effe
ctS
ize
Coh
en’s
d(9
5%C
I)
PP
T(k
Pa)
Med
ian
(IQ
R)
Cer
vica
l18
6(1
42–2
28)
199
(139
–253
)23
6(1
78–3
04)
293
(191
–352
)34
4(2
85–4
15)
0.74
(0.5
4–0.
94)
<---
----
----
----
----
P=
1.00
----
----
----
----
->P
valu
es<-
----
----
----
----
----
----
----
----
-P=
0.03
7---
----
----
----
----
----
----
----
-->
<---
----
----
----
----
----
----
----
----
P<
0.00
5---
----
----
----
----
----
----
----
----
><-
----
----
----
----
----
----
----
----
----
----
----
----
---P
<0.
001-
----
----
----
----
----
----
----
----
----
----
----
----
><-
----
----
----
----
--P
=0.
76--
----
----
----
----
-->
Med
ian
N24
2(1
83–2
86)
253
(179
–312
)30
7(2
42–3
79)
338
(252
–426
)37
1(2
97–4
28)
<---
----
----
----
---P
=1.
00--
----
----
----
----
><-
----
----
----
----
----
----
----
----
--P
<0.
01--
----
----
----
----
----
----
----
----
>0.
73(0
.53–
0.93
)P
valu
es<-
----
----
----
----
-P=
0.02
3---
----
----
----
-->
<---
----
----
----
----
----
----
----
----
P<
0.00
1---
----
----
----
----
----
----
----
----
><-
----
----
----
----
----
----
----
----
----
----
----
----
--P
<0.
001-
----
----
----
----
----
----
----
----
----
----
----
----
-><-
----
----
----
----
--P
=1.
00--
----
----
----
----
-->
Tib
Ant
328
(282
–398
)35
0(2
85–4
36)
428
(363
–549
)51
1(3
60–6
57)
563
(462
–728
)<-
----
----
----
----
--P
=1.
00--
----
----
----
----
><-
----
----
----
----
----
----
----
----
P<
0.00
5---
----
----
----
----
----
----
----
--->
0.73
(0.5
3–0.
93)
Pva
lues
<---
----
----
----
----
P=
0.01
9---
----
----
----
-->
<---
----
----
----
----
----
----
----
----
-P<
0.00
1---
----
----
----
----
----
----
----
--->
<---
----
----
----
----
----
----
----
----
----
----
----
----
-P<
0.00
1---
----
----
----
----
----
----
----
----
----
----
----
-->
<---
----
----
----
----
P=
0.58
----
----
----
----
----
>
NF
R(m
A)
Med
ian
(IQ
R)
12(6
–18)
12(6
–20)
18(1
0–30
)16
(8–3
8)21
(10–
38)
0.40
(0.2
0–0.
60)
<---
----
----
----
----
P=
1.00
----
----
----
----
-><-
----
----
----
----
----
----
----
---P
<0.
013-
----
----
----
----
----
----
----
----
-->
<---
----
----
----
----
P=
0.03
5---
----
----
----
-->
<---
----
----
----
----
----
----
----
----
P=
0.05
6---
----
----
----
----
----
----
----
----
><-
----
----
----
----
----
----
----
----
----
----
----
----
--P
<0.
001-
----
----
----
----
----
----
----
----
----
----
----
----
-><-
----
----
----
----
-P=
1.00
----
----
----
----
----
->
BP
PT
(°el
bex
tR
OM
)M
edia
n(I
QR
)
29(1
8–39
)31
(20–
37)
12(5
–20)
10(3
–19)
3(0
–9)
1.21
(0.9
8–1.
44)
<---
----
----
----
----
P=
1.00
----
----
----
----
-><-
----
----
----
----
----
----
----
---P
<0.
001-
----
----
----
----
----
----
----
----
-->
<---
----
----
----
---P
<0.
001-
----
----
----
----
-><-
----
----
----
----
----
----
----
----
---P
<0.
001-
----
----
----
----
----
----
----
----
-><-
----
----
----
----
----
----
----
----
----
----
----
----
P<
0.00
1---
----
----
----
----
----
----
----
----
----
----
----
----
-><-
----
----
----
----
---P
=1.
00--
----
----
----
----
->
Bol
ded
Pva
lues
deno
test
atis
tical
sign
ifica
nce.
CI=
confi
denc
ein
terv
al;
BP
PT
=br
achi
alpl
exus
prov
ocat
ion
test
;°e
lbex
tR
OM
=de
gree
sof
elbo
wex
tens
ion
rang
eof
mot
ion;
IQR
=in
terq
uart
ilera
nge;
kPa
=ki
lopa
scal
;m
A=
mill
iam
pere
s;M
edia
nN
=m
edia
nne
rve;
NF
R=
noci
cept
orfle
xor
refle
x;P
PT
=pr
essu
repa
inth
resh
old;
Tib
Ant
=tib
ialis
ante
rior;
WA
D=
whi
plas
h-as
soci
ated
diso
rder
.
134
Smith et al.
Both prior to and following RFN, the WAD group showedless cervical ROM compared with the HCs (P < 0.0001).
CCFT
There was a significant main effect of time for surfaceEMG at 24, 26, and 28 mm Hg levels of the CCFT(Table 4). No significant effect of time was found for the 22and 30 mm Hg levels. Post-hoc tests of simple effectswere not significant. Thus, a general trend for reducedEMG was evident at the 24, 26, and 28 mm Hg levels ofthe CCFT.
Prior to RFN, the WAD group demonstrated increasedEMG levels compared with the controls at all levels of theCCFT (P < 0.05), except for 30 mm Hg (P = 0.053). Fol-lowing RFN, there was no significant difference between
the WAD and HC groups for any level of the CCFT(P > 0.084).
Discussion
The results of this study demonstrated that individualswith chronic WAD who underwent successful cervicalRFN show significant and sustained reductions in sensoryhypersensitivity (mechanical and thermal), spinal cordhyperexcitability, improved responses to the BPPT, andcervical ROM with trends toward improved cervicalmuscle control. Attenuation of widespread sensory hyper-sensitivity, spinal cord hyperexcitability and measures ofmotor function after RFN suggests that nociception fromthe cervical facet joint contributes to augmented centralnociceptive processing and movement dysfunction inpatients with chronic WAD.
Table 3 Summary of thermal pain thresholds (median [IQR]) over time in WAD participants vs healthycontrols
Time (N) t(1) (53) t(2) (53) t(3) (53) t(4) (50) Healthy ControlsEffect SizeCliff’s Delta
CPT (°C) 19.6 (11.3–25.3) 20.8 (11.0–24.7) 12.6 (4.9–17.8) 9.7 (3.6–17.0) 3.5 (0–8.1) 0.38<-----------------P = 0.51-----------------><----------------------------P < 0.0001------------------------------><--------------------------------------------P < 0.0001----------------------------------------->
P values <------------------------------P < 0.0001-----------------------------><---------------------------------------P < 0.0001---------------------------------------------->
<-----------------P = 0.12 ------------------>
HPT (°C) 42.6 (40.3–45.0) 43.5 (41.8–45.9) 46.7 (43.7–48.1) 46.6 (44.0–48.4) 47.5 (46.1–48.6) 0.41<-----------------P = 0.04-----------------><-----------------------------P < 0.0001----------------------------->
P values <---------------P < 0.0001-----------------><-----------------------------P < 0.0001------------------------------>
<------------------------------------------P < 0.0001-------------------------------------------><-----------------P = 0.48 ------------------>
Bolded P values denote statistical significance.CPT = cold pain threshold; HPT = heat pain threshold; IQR = interquartile range; WAD = whiplash-associated disorders.
Table 4 CCFT RMS values (medians [IQR]) over time for WAD participants vs healthy controls
Time (N),mm Hg t(1) t(2) t(3) t(4)
ANOVAP value Healthy Controls
22 0.08 (0.03–0.26) 0.07 (0.04–0.15) 0.07 (0.03–0.16) 0.06 (0.02–0.15) 0.057 0.04 (0.02–0.08)24 0.13 (0.05–0.31) 0.16 (0.07–0.31) 0.10 (0.05–0.21) 0.12 (0.04–0.21) 0.044 0.08 (0.03–0.19)26 0.16 (0.07–0.42) 0.26 (0.14–0.66) 0.15 (0.06–0.39) 0.18 (0.05–0.28) 0.013 0.16 (0.06–0.23)28 0.30 (0.15–0.52) 0.34 (0.16–0.72) 0.29 (0.12–0.53) 0.27 (0.09–0.50) 0.015 0.21 (0.10–0.30)30 0.53 (0.17–0.82) 0.55 (0.21–0.86) 0.37 (0.16–0.69) 0.35 (0.10–0.71) 0.067 0.29 (0.10–0.46)
Bolded P values denote statistical significance.ANOVA = analysis of variance; CCFT = craniocervical flexion test; IQR = interquartile range; mm Hg = millimeters mercury;RMS = root mean square; t(1) = time-point 1 = 1 month after receiving cervical facet joint blockade; t(2) = time-point 2 = immediatelyprior to receiving radiofrequency neurotomy; t(3) = time-point 3 = 1 month following radiofrequency neurotomy; t(4) = time-point4 = 3 months following radiofrequency neurotomy; WAD = whiplash-associated disorders.
135
Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability

Post-mortem studies have previously demonstrated thatcervical facet joints are injured in MVCs [59–62], withclinical studies confirming the facet joint as a candidate forongoing nociception in patients with chronic WAD [28,30].Biomechanical studies of cadavers and human volunteershave demonstrated how these injuries may occur [63–70].Animal studies have shown that facet joint capsule stretchresulting from whiplash loading [71] has the potential toinitiate physiological and behavioural responses includingnociceptive afferent activation and after-discharge [31,71–75], release of inflammatory mediators resulting inperipheral sensitization [32], and alterations in neuronalexcitability in the spinal cord [33,73,76–78]. The results ofour study, where hyperalgesic responses were effectivelymodulated following the reduction of facet jointnociception, would support the results of these animalstudies demonstrating a relationship between the facetjoint and ongoing hyperalgesic responses in WAD.
Other studies in humans with chronic musculoskeletalpain have attempted to elucidate the relationship betweenperipheral mechanisms (persistent nociception) and aug-mented central processes. In studies of painful osteoar-thritis, participants demonstrated central nervous systemhyperexcitability prior to undergoing arthroplasty of the hipor knee that was reversed after arthroplastic surgery andsubsequent pain relief [15,16], implicating the role ofongoing afferent nociception in augmentation of centralpain processes. The influence of peripheral mechanismsdriving central mechanisms was also demonstrated in arecent study involving individuals with chronic low backpain [79]. Following successful reduction in pain withsurgery or facet joint injections, functional magnetic reso-nance imaging scans demonstrated a reversal of func-tional and structural brain abnormalities, which did notoccur in those who did not respond to treatment [79].Thus, it appears that successfully reducing nociceptionresults in changes in central pain processing mechanisms.
Previous studies have investigated the effects of RFN onsensory measures in patients with WAD to some extent.Consistent with our findings, Prushansky et al. [37] andChua et al. [36] demonstrated that PPTs measured overthe cervical spine increased following RFN, and this mayreflect local hypoalegsia related to the anesthetic proce-dure to the neck and decreased focal sensitization ofperipheral structures. Our finding of decreased heathyperalgesia may also support this proposal, as heathyperalgesia is thought to reflect nociceptor sensitizationand also be an indicator of peripheral sensitization [80,81].Chua et al. [36] found no change in PPTs at remote sites.In contrast, we found that PPTs at sites remote to the neckalso increased, indicating that RFN has the capacity tomodulate central as well as peripheral nociceptive pro-cessing. This discrepancy in study findings could beexplained by the low sample size (N = 9) of Chua’s study[36] in view of large variance in distal PPT measurements[38,82]. We previously demonstrated immediate (withinhours) increases in PPTs at sites away from the site ofinjury (neck) in patients with chronic WAD [38]. The currentstudy replicated these findings but demonstrated that
these effects were sustained to at least 3 months post-procedure and exceeded published minimal detectablechanges [83]. The current study findings also differed fromthose of our previous study. In the former study, PPTmeasures of the whiplash group remained lower than thatof controls post-MBB, while in the current study, mea-sures largely returned to those of the HC group. This maybe due to the duration of pain relief in this study (3 monthscompared with 1–2 hours) or possibly due to participantvariability in their health characteristics.
In addition to changes in PPT, we found sustainedincreases in NFR threshold following RFN, indicatingreduced excitability of the spinal cord reflexes andreduced hyperalgesic response to the BPPT, together withdecreased cold and heat hyperalgesia. Cold sensitivityhas been postulated to occur as a result of sensitizedafferent fibers or dorsal horn neurons, with possible under-lying insular cortex dysfunction [84,85]. Dorsal horn sen-sitization has also been suggested as an underlyingmechanism of heat hyperalgesia [16], while BPPT reactiv-ity has been interpreted to reflect hyperalgesic motor andsensory responses as a consequence of central sensiti-zation [86,87]. Thus, reduction of cold hyperalgesia, con-comitant improvements in PPT at distal sites of uninjuredtissues (tibialis anterior and median nerves), especiallywhen combined with reduction of spinal cord hyperexcit-ability (increased NFR threshold) and improvement inBPPT hyperalgesia, would suggest that peripheralnociception contributes to these processes. Most of thesensory measures of the WAD group were no longerdifferent from control data following RFN. The exceptionsto this were CPT and BBPT responses, which remainedmore sensitive than the HCs at the follow-up time points,although the values for these two measures were within95% CIs of published normative data [4,88].
Individuals with chronic WAD consistently demonstratethe presence of persistent motor dysfunction [8,17,50,89–91], most noticeable in those with increased levels of painand disability [8,50]. In longitudinal studies, motor dys-function has remained unchanged over time [50,92], withonly modest improvements in ROM, pain and disabilitydemonstrated following a course of multimodal physio-therapy [93]. The changes measured were not significantlydifferent to a self-management group (advice booklet andexercise) [93]. In contrast, our study demonstrated a largeand significant improvement in ROM following RFN withconcurrent large reductions in pain and disability. Therewas also a trend toward improvement in performance ofthe CCFT, with changes not quite reaching statistical sig-nificance. However, following RFN, no significant differ-ence in test performance was measured between the HCand WAD groups, indicating that the improvements mea-sured were relevant. Hence, the reduction of nociceptionresulted in certain CCFT improvements occurring. Giventhat individuals continued to report ongoing mild levels ofpain, further improvement could be postulated to occur iffurther pain reduction was possible. However, theseresults are also consistent with findings in previousresearch, where despite resolution of pain and disability in
136
Smith et al.

some participants, deficits in performance of the CCFTremained [50]. Thus, the remaining motor impairment inthis group with chronic neck pain probably reflects bothlocal changes in muscle properties as well as changes incentral neuromotor control [19,22–24].
Individuals in our study continued to present with mild-to-moderate levels of pain and disability, 1–3 months follow-ing RFN. These results are consistent with other studies,when comparing similar time periods post-RFN [37,94]. Atfirst glance, these results may not seem as promising asLord et al. [95], where complete relief of pain was reportedin the days following the procedure. In our study, fourpatients reported complete relief of pain 1 month followingRFN, and an additional 10 reported ≤1/10 pain. However,when comparing results at 3 months post-RFN, they aresimilar, with both studies finding that approximately 60%of participants reported relief of pain of at least 50% [95].Pain reported at 1 and 3 months may be as a result ofongoing nociception from structures other than the facetjoints influenced by RFN [96]. Additionally, ongoing disabil-ity found in our study could be related to factors such aspersistent motor dysfunction (ongoing reduced ROMwhen compared with the HC participants and impairedmotor control demonstrated via the CCFT) and persistentpsychological distress [97].
There are some limitations in this study. We investigated54 consecutive individuals undergoing RFN after success-ful response to facet joint double blockade. Selection ofpatients for and performance of RFN differed slightly fromthe stringent guidelines established by the InternationalSpine Intervention Society [98,99]. Another limitation ofthe study was that it was not possible to blind the asses-sor to the status of the patient or the aims of the study.This may have introduced bias, thus indicating somecaution with interpretation of study findings.
Conclusions
Cervical RFN resulted in increased NFR thresholds,increases in local (mechanical and thermal) and remote(mechanical) pain thresholds as well as improvement incervical ROM. These results indicate that augmentedcentral nociceptive processes, and movement loss aremaintained by peripheral nociception arising from the cer-vical facet joints.
Acknowledgment
The authors would like to acknowledge Ms MeaghanBuisson for her assistance with participant recruitment.
References1 Carroll LJ, Holm LW, Hogg-Johnson S, et al. Course
and prognostic factors for neck pain in whiplash-associated disorders (WAD): Results of the Bone andJoint Decade 2000–2010 Task Force on neck painand its associated disorders. Spine 2008;33(suppl4):S83–92.
2 Curatolo M, Petersen-Felix S, Arendt-Nielsen L, et al.Central hypersensitivity in chronic pain after whiplashinjury. Clin J Pain 2001;17(4):306–15.
3 Koelbaek Johansen M, Graven-Nielsen T,Schou Olesen A, Arendt-Nielsen L. Generalised mus-cular hyperalgesia in chronic whiplash syndrome. Pain1999;83(2):229–34.
4 Sterling M, Jull G, Vicenzino B, Kenardy J. Sensoryhypersensitivity occurs soon after whiplash injury andis associated with poor recovery. Pain 2003;104(3):509–17.
5 Banic B, Petersen-Felix S, Andersen OK, et al. Evi-dence for spinal cord hypersensitivity in chronic painafter whiplash injury and in fibromyalgia. Pain2004;107(1–2):7–15.
6 Sterling M, Hodkinson E, Pettiford C, Souvlis T,Curatolo M. Psychologic factors are related to somesensory pain thresholds but not nociceptive flexionreflex threshold in chronic whiplash. Clin J Pain2008;24(2):124–30.
7 Woolf CJ. Central sensitization: Implications for thediagnosis and treatment of pain. Pain 2012;152(suppl3):S2–15.
8 Dall’Alba PT, Sterling MM, Treleaven JM, Edwards SL,Jull GA. Cervical range of motion discriminatesbetween asymptomatic persons and those with whip-lash. Spine 2001;26(19):2090–4.
9 Jull G, Kristjansson E, Dall’Alba P. Impairment in thecervical flexors: A comparison of whiplash and insidi-ous onset neck pain patients. Man Ther 2004;9(2):89–94.
10 Curatolo M, Arendt-Nielsen L, Petersen-Felix S. Evi-dence, mechanisms, and clinical implications ofcentral hypersensitivity in chronic pain after whiplashinjury. Clin J Pain 2004;20(6):469–76.
11 Sterling M, McLean SA, Sullivan MJ, et al. Potentialprocesses involved in the initiation and maintenance ofwhiplash-associated disorders: Discussion paper 3.Spine (Phila Pa 1976) 2012;36(suppl 25):S322–9.
12 Chien A, Eliav E, Sterling M. The development ofsensory hypoesthesia after whiplash injury. Clin J Pain2010;26(8):722–8.
13 Curatolo M, Arendt-Nielsen L, Petersen-Felix S.Central hypersensitivity in chronic pain: Mechanismsand clinical implications. Phys Med Rehabil Clin N Am2006;17(2):287–302.
14 Staud R, Nagel S, Robinson ME, Price DD. Enhancedcentral pain processing of fibromyalgia patients ismaintained by muscle afferent input: A randomized,
137
Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability
double-blind, placebo-controlled study. Pain 2009;145(1–2):96–104.
15 Graven-Nielsen T, Wodehouse T, Langford RM,Arendt-Nielsen L, Kidd BL. Normalization of wide-spread hyperesthesia and facilitated spatial summa-tion of deep-tissue pain in knee osteoarthritis patientsafter knee replacement. Arthritis Rheum 2012;64(9):2907–16.
16 Kosek E, Ordeberg G. Abnormalities of somatosen-sory perception in patients with painful osteoarthritisnormalize following successful treatment. Eur J Pain2000;4(3):229–38.
17 Dumas JP, Arsenault AB, Boudreau G, et al. Physicalimpairments in cervicogenic headache: Traumatic vs.nontraumatic onset. Cephalalgia 2001;21(9):884–93.
18 Elliott J, Jull G, Noteboom JT, et al. Fatty infiltration inthe cervical extensor muscles in persistent whiplash-associated disorders: A magnetic resonance imaginganalysis. Spine 2006;31(22):E847–55.
19 Falla D, Bilenkij G, Jull G. Patients with chronic neckpain demonstrate altered patterns of muscle activationduring performance of a functional upper limb task.Spine 2004;29(13):1436–40.
20 Falla D, Jull G, Rainoldi A, Merletti R. Neck flexormuscle fatigue is side specific in patients with unilat-eral neck pain. Eur J Pain 2004;8(1):71–7.
21 Uhlig Y, Weber BR, Grob D, Muntener M. Fiber com-position and fiber transformations in neck musclesof patients with dysfunction of the cervical spine.J Orthop Res 1995;13(2):240–9.
22 Falla D, Farina D, Dahl MK, Graven-Nielsen T. Musclepain induces task-dependent changes in cervicalagonist/antagonist activity. J Appl Physiol 2007;102(2):601–9.
23 Falla D, Farina D, Graven-Nielsen T. Experimentalmuscle pain results in reorganization of coordinationamong trapezius muscle subdivisions during repetitiveshoulder flexion. Exp Brain Res 2007;178(3):385–93.
24 Falla D, Jull G, Hodges PW. Feedforward activity of thecervical flexor muscles during voluntary arm move-ments is delayed in chronic neck pain. Exp Brain Res2004;157(1):43–8.
25 Curatolo M, Bogduk N, Ivancic PC, et al. The role oftissue damage in whiplash-associated disorders: Dis-cussion paper 1. Spine (Phila Pa 1976) 2011;36(suppl25):S309–15.
26 Linnman C, Appel L, Fredrikson M, et al. Elevated[11C]-D-deprenyl uptake in chronic whiplash associ-
ated disorder suggests persistent musculoskeletalinflammation. PLoS ONE 2011;6(4):e19182.
27 Gerdle B, Lemming D, Kristiansen J, et al. Biochemi-cal alterations in the trapezius muscle of patients withchronic whiplash associated disorders (WAD)—Amicrodialysis study. Eur J Pain 2008;12(1):82–93.
28 Barnsley L, Lord SM, Wallis BJ, Bogduk N. The preva-lence of chronic cervical zygapophysial joint pain afterwhiplash. Spine 1995;20(1):20–5; discussion 26.
29 Gibson T, Bogduk N, Macpherson J, McIntosh A.Crash characteristics of whiplash associated chronicneck pain. J Musculoskelet Pain 2000;8:87–95.
30 Lord SM, Barnsley L, Wallis BJ, Bogduk N. Chroniccervical zygapophysial joint pain after whiplash.A placebo-controlled prevalence study. Spine1996;21(15):1737–44; discussion 1744-1735.
31 Lee K, Thinnes J, Gokhin D, Winkelstein B. A novelrodent neck pain model of facet-mediated behaviouralhypersensitivity: Implications for persistent pain andwhiplash injury. J Neurosci Methods 2004;137:151–9.
32 Lee KE, Davis MB, Winkelstein BA. Capsular ligamentinvolvement in the development of mechanical hyper-algesia after facet joint loading: Behavioral andinflammatory outcomes in a rodent model of pain. JNeurotrauma 2008;25(11):1383–93.
33 Lee KE, Winkelstein BA. Joint distraction magnitude isassociated with different behavioral outcomes andsubstance P levels for cervical facet joint loading in therat. J Pain 2009;10(4):436–45.
34 Winkelstein BA, Santos DG. An intact facet capsularligament modulates behavioral sensitivity and spinalglial activation produced by cervical facet joint tension.Spine 2008;33(8):856–62.
35 Thunberg J, Hellstrom F, Sjolander P, et al. Influenceson the fusimotor-muscle spindle system from chemo-sensitive nerve endings in cervical facet joints in thecat: Possible implications for whiplash associated dis-orders. Pain 2001;91:15–22.
36 Chua NH, Vissers KC, Arendt-Nielsen L, Wilder-SmithOH. Do diagnostic blocks have beneficial effects onpain processing? Reg Anesth Pain Med 2011;36(4):317–21.
37 Prushansky T, Pevzner E, Gordon C, Dvir Z. Cervicalradiofrequency neurotomy in patients with chronicwhiplash: A study of multiple outcome measures.J Neurosurg Spine 2006;4(5):365–73.
38 Schneider GM, Smith AD, Hooper A, et al. Minimizingthe source of nociception and its concurrent effect on
138
Smith et al.
sensory hypersensitivity: An exploratory study inchronic whiplash patients. BMC Musculoskelet Disord2010;11:29.
39 Spitzer WO, Skovron ML, Salmi LR, et al. Scientificmonograph of the Quebec Task Force on Whiplash-Associated Disorders: Redefining “whiplash” and itsmanagement. Spine 1995;20(suppl 8):1S–73S.
40 Smith A, Jull G, Schneider G, et al. Responders andNon-Responders of Cervical Facet Blocks for ChronicWhiplash Show Similar Physical and PsychologicalFeatures Canadian Physiotherapy Association Con-gress; Whistler, British Columbia, Canada; 2011.
41 Sandrini G, Serrao M, Rossi P, et al. The lower limbflexion reflex in humans. Prog Neurobiol 2005;77(6):353–95.
42 Rhudy JL, France CR. Defining the nociceptive flexionreflex (NFR) threshold in human participants: A com-parison of different scoring criteria. Pain 2007;128(3):244–53.
43 French DJ, France CR, France JL, Arnott LF. Theinfluence of acute anxiety on assessment of nocicep-tive flexion reflex thresholds in healthy young adults.Pain 2005;114(3):358–63.
44 Hurtig IM, Raak RI, Kendall SA, Gerdle B, Wahren LK.Quantitative sensory testing in fibromyalgia patientsand in healthy subjects: Identification of subgroups.Clin J Pain 2001;17(4):316–22.
45 Elvey R. Brachial plexus tension test and thepathoanatomical origin of arm pain. In: Glasgow E,Twomey L, eds. Aspects of Manipulative Therapy.Melbourne: Lincoln Institute of Health Sciences;1979:105–10.
46 Balster SM, Jull GA. Upper trapezius muscle activityduring the brachial plexus tension test in asymptom-atic subjects. Man Ther 1997;2(3):144–9.
47 Ide M, Ide J, Yamaga M, Takagi K. Symptoms andsigns of irritation of the brachial plexus in whiplashinjuries. J Bone Joint Surg Br 2001;83(2):226–9.
48 Sterling M, Treleaven J, Edwards S, Jull G. Pressurepain thresholds in chronic whiplash associated disor-der: Further evidence of altered central pain process-ing. J Musculoskelet Pain 2002;10(3):69–81.
49 Coppieters M, Stappaerts K, Janssens K, Jull G. Reli-ability of detecting “onset of pain” and “submaximalpain” during neural provocation testing of the upperquadrant. Physiother Res Int 2002;7(3):146–56.
50 Sterling M, Jull G, Vicenzino B, Kenardy J, Darnell R.Development of motor system dysfunction followingwhiplash injury. Pain 2003;103(1–2):65–73.
51 Pearcy M, Hindle R. New method for the non-invasivethree-dimensional measurement of human backmovement. Clin Biomech (Bristol, Avon) 1989;4:73–9.
52 Falla D, Dall’Alba P, Rainoldi A, Merletti R, Jull G.Location of innervation zones of sternocleidomastoidand scalene muscles—A basis for clinical andresearch electromyography applications. ClinNeurophysiol 2002;113(1):57–63.
53 Vernon H, Mior S. The Neck Disability Index: A study ofreliability and validity. J Manipulative Physiol Ther1991;14(7):409–15.
54 Macdermid JC, Walton DM, Avery S, et al. Measure-ment properties of the neck disability index: A system-atic review. J Orthop Sports Phys Ther 2009;39(5):400–17.
55 Sterling M, Jull G, Vicenzino B, Kenardy J. Character-ization of acute whiplash-associated disorders. Spine2004;29(2):182–8.
56 Macbeth G, Razumiejczyk E, Ledesma R. Cliff’s DeltaCalculator: A non-parametric effect size program fortwo groups of observations. Univ Psychol 2011;10(2):545–55.
57 Kazis LE, Anderson JJ, Meenan RF. Effect sizes forinterpreting changes in health status. Med Care1989;27(suppl 3):S178–89.
58 Cohen J. Statistical Power Analysis for the BehaviouralSciences, 2nd edition. Hillsdale, NJ: LawrenceErlbaum Associates; 1988.
59 Jonsson H Jr, Bring G, Rauschning W, Sahlstedt B.Hidden cervical spine injuries in traffic accident victimswith skull fractures. J Spinal Disord 1991;4(3):251–63.
60 Taylor J, Taylor M. Cervical spine injuries: An autopsystudy of 109 blunt injuries. J Musculoskelet Pain1996;4(4):61–79.
61 Taylor J, Twomey L. Acute injuries to cervical joints: Anautopsy study of neck sprain. Spine 1993;18(9):1115–22.
62 Uhrenholt L, Grunnet-Nilsson N, Hartvigsen J. Cervicalspine lesions after road traffic accidents: A systematicreview. Spine 2002;27(17):1934–41; discussion 1940.
63 Ivancic PC, Ito S, Tominaga Y, et al. Whiplash causesincreased laxity of cervical capsular ligament. ClinBiomech (Bristol, Avon) 2008;23(2):159–65.
64 Kaneoka K, Ono K, Inami S, Hayashi K. Motion analy-sis of cervical vertebrae during whiplash loading.Spine 1999;24(8):763–9; discussion 770.
139
Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability
65 Panjabi MM, Cholewicki J, Nibu K, Grauer J, VahldiekM. Capsular ligament stretches during in vitrowhiplash simulations. J Spinal Disord 1998;11(3):227–32.
66 Panjabi MM, Pearson AM, Ito S, Ivancic PC, Wang JL.Cervical spine curvature during simulated whiplash.Clin Biomech (Bristol, Avon) 2004;19(1):1–9.
67 Pearson A, Ivancic P, Ito S, Panjabi M. Facet jointkinematics and injury mechanism during simulatedwhiplash. Spine 2004;29(4):390–7.
68 Siegmund G, Myers B, Davis M, Bohnet H,Winkelstein B. Mechanical evidence of cervical facetjoint capsule injury during whiplash: A cadaveric studyusing combined shear, compression, and extensionloading. Spine 2001;26(19):2095–101.
69 Stemper B, Yoganandan N, Gennarelli T, Pintar F.Localized cervical facet joint kinematics under physi-ological and whiplash loading. J Neurosurg Spine2005;3:471–6.
70 Winkelstein BA, Nightingale RW, Richardson WJ,Myers BS. The cervical facet capsule and its role inwhiplash injury: A biomechanical investigation. Spine2000;25(10):1238–46.
71 Quinn KP, Winkelstein BA. Cervical facet capsularligament yield defines the threshold for injury and per-sistent joint-mediated neck pain. J Biomech 2007;40(10):2299–306.
72 Chen C, Lu Y, Kallakuri S, Patwardhan A, CavanaughJ. Distribution of A-delta and C-fiber receptors in thecervical facet joint capsule and their response tostretch. J Bone Joint Surg Am 2006;88(8):1808–16.
73 Dong L, Odeleye AO, Jordan-Sciutto KL, WinkelsteinBA. Painful facet joint injury induces neuronalstress activation in the DRG: Implications for cellularmechanisms of pain. Neurosci Lett 2008;443(2):90–4.
74 Lee KE, Franklin AN, Davis MB, Winkelstein BA.Tensile cervical facet capsule ligament mechanics:Failure and subfailure responses in the rat. J Biomech2006;39(7):1256–64.
75 Lu Y, Chen C, Kallakuri S, Patwardhan A, CavanaughJ. Neurophysiological and biomechanical character-ization of goat cervical facet joint capsules. J OrthopRes 2005;23:779–87.
76 Dong L, Quindlen JC, Lipschutz DE, Winkelstein BA.Whiplash-like facet joint loading initiates glutamatergicresponses in the DRG and spinal cord associated withbehavioral hypersensitivity. Brain Res 2012;1461:51–63.
77 Dong L, Winkelstein BA. Simulated whiplash modu-lates expression of the glutamatergic system in thespinal cord suggesting spinal plasticity is associatedwith painful dynamic cervical facet loading. JNeurotrauma 2011;27(1):163–74.
78 Quinn KP, Dong L, Golder FJ, Winkelstein BA.Neuronal hyperexcitability in the dorsal horn afterpainful facet joint injury. Pain 2010;151(2):414–21.
79 Seminowicz DA, Wideman TH, Naso L, et al. Effectivetreatment of chronic low back pain in humans reversesabnormal brain anatomy and function. J Neurosci2011;31(20):7540–50.
80 Kilo S, Schmelz M, Koltzenburg M, Handwerker HO.Different patterns of hyperalgesia induced by experi-mental inflammation in human skin. Brain 1994;117(Pt 2):385–96.
81 Rolke R, Baron R, Maier C, et al. Quantitative sensorytesting in the German Research Network on Neuro-pathic Pain (DFNS): Standardized protocol and refer-ence values. Pain 2006;123(3):231–43.
82 Sterling M, Jull G, Carlsson Y, Crommert L. Arecervical physical outcome measures influenced by thepresence of symptomatology? Physiother Res Int2002;7(3):113–21.
83 Walton DM, Macdermid JC, Nielson W, et al. Reliabil-ity, standard error, and minimum detectable change ofclinical pressure pain threshold testing in people withand without acute neck pain. J Orthop Sports PhysTher 2011;41(9):644–50.
84 Berglund B, Harju EL, Kosek E, Lindblom U. Quanti-tative and qualitative perceptual analysis of cold dys-esthesia and hyperalgesia in fibromyalgia. Pain 2002;96(1–2):177–87.
85 Craig AD, Chen K, Bandy D, Reiman EM.Thermosensory activation of insular cortex. NatNeurosci 2000;3(2):184–90.
86 Quintner JL. A study of upper limb pain andparaesthesiae following neck injury in motor vehicleaccidents: Assessment of the brachial plexus tensiontest of Elvey. Br J Rheumatol 1989;28(6):528–33.
87 Sterling M, Treleaven J, Jull G. Responses to a clinicaltest of mechanical provocation of nerve tissue in whip-lash associated disorder. Man Ther 2002;7(2):89–94.
88 Magerl W, Krumova EK, Baron R, et al. Referencedata for quantitative sensory testing (QST): Refinedstratification for age and a novel method for statisticalcomparison of group data. Pain 2010;151(3):598–605.
140
Smith et al.
89 Elert J, Kendall SA, Larsson B, Mansson B, Gerdle B.Chronic pain and difficulty in relaxing postural musclesin patients with fibromyalgia and chronic whiplashassociated disorders. J Rheumatol 2001;28(6):1361–8.
90 Heikkila H, Astrom PG. Cervicocephalic kinestheticsensibility in patients with whiplash injury. Scand JRehabil Med 1996;28(3):133–8.
91 Nederhand MJ, IJzerman MJ, Hermens HJ, Baten CT,Zilvold G. Cervical muscle dysfunction in the chronicwhiplash associated disorder grade II (WAD-II). Spine2000;25(15):1938–43.
92 Nederhand MJ, Hermens HJ, IJzerman MJ, Turk DC,Zilvold G. Chronic neck pain disability due to an acutewhiplash injury. Pain 2003;102(1–2):63–71.
93 Jull G, Sterling M, Kenardy J, Beller E. Does the pres-ence of sensory hypersensitivity influence outcomes ofphysical rehabilitation for chronic whiplash?—A pre-liminary RCT. Pain 2007;129(1–2):28–34.
94 Sapir DA, Gorup JM. Radiofrequency medial branchneurotomy in litigant and nonlitigant patients with cer-vical whiplash: A prospective study. Spine 2001;26(12):E268–73.
95 Lord SM, Barnsley L, Wallis BJ, McDonald GJ,Bogduk N. Percutaneous radio-frequency neurotomyfor chronic cervical zygapophyseal-joint pain. N Engl JMed 1996;335(23):1721–6.
96 Bogduk N, Aprill C. On the nature of neck pain, dis-cography and cervical zygapophysial joint blocks. Pain1993;54(2):213–7.
97 Sterling M, Kenardy J, Jull G, Vicenzino B. The devel-opment of psychological changes following whiplashinjury. Pain 2003;106(3):481–9.
98 Bogduk N. International Spinal Injection Society guide-lines for the performance of spinal injection proce-dures. Part 1: Zygapophysial joint blocks. Clin J Pain1997;13(4):285–302.
99 International Spine Intervention Society. Percutaneousradiofrequency cervical medial branch neurotomy. In:Bogduk N, ed. Practice Guidelines for Spinal Diagnos-tic and Treatment Procedures. San Francisco, CA:International Spine Intervention Society; 2004:249–84.
Appendix
Diagnostic Pathway:
Individuals who reported greater than 50% relief offamiliar neck pain following cervical facet joint blockade
(intra-articular block [IAB] followed by confirmatory medialbranch block [MBB]) were referred for RFN.
Clinically, this diagnostic pathway (IAB followed by MBB)is used prior to consideration for radiofrequency neu-rotomy. Although the scientific literature is varied, there issome evidence to suggest that a subset of individualswith suspected cervical facet joint pain might experiencea therapeutic benefit from an intra-articular injection,with respect to a decrease in pain intensity over a periodof 3 months or greater (Kim et al., 2005). As our publicly-funded center provides pain management services to alarge catchment area, we possess a long (∼6 month)waitlist for interventional techniques including diagnosticfacet joint procedures. Historically, the clinic utilized atriple-injection procedure for the diagnosis of facetjoint pain consisting of an intra-articular facet joint injec-tion, followed by controlled, comparative MBB proce-dures when needed. Our unpublished data revealed thatit was nearly universal, in that individuals that respondedpositively to both an intra-articular facet joint injectionand the first MBB, responded positively to the secondMBB. By eliminating the second MBB, we were able toreduce patient wait-time by approximately 15–20%,decrease the cost to the system, and manage selectpatients with IAB alone thereby decreasing the demandfor RF neurotomies.
RFN Procedure:
Local anesthetic, fluoroscopic guidance, and sterile tech-nique were utilized for placing 21 gauge RF cannulae tothe expected location of the medial branches of the dorsalrami at the appropriate sites, depending on the levels tobe treated. Cannulae were placed parallel to expectedcourse of the nerves, along the lateral aspect of the articu-lar pillars. A grounding pad was placed on the patient andconnected to the RF lesion generator. Once the RF can-nulae were in proper position based on the AP, oblique,and lateral fluoroscopic imaging, an RF probe wasinserted into each cannula for determination of the tissueimpedance and then motor stimulation. When it wasdetermined that there was no motor nerve stimulation andthe cannulae were considered in proper position, 2% lido-caine was injected through each cannula. After anesthe-tizing with lidocaine, RF thermocoagulation lesions weremade at each site using an RF probe with a 5 mm activetip, heating to the tissue at the tip of the probe to 80degrees centigrade for 75 seconds. For the C2–3 joint thethird occipital nerve (TON) was included along with themedial branch at C3, making at least three lesions alongthe possible craniocaudal extent of the TON. For jointsbelow C2–3, both medial branches that innervated thejoint were targeted, with one to two lesions created ateach site. A small amount (2 mg) of Celestone Soluspanwas injected at each neurotomy site at the conclusion ofthe procedure to reduce the chance of a post-procedureneuritis. The patient was given post-procedure writteninstructions and phone numbers to reach the radiologistif necessary.
141
Cervical Radiofrequency Neurotomy Reduces Central Hyperexcitability
Related Documents