Cervical Cancer Screening Past… PRESENT…Future Audrey P. Garrett, MD, MPH Women’s Health Symposium September 7, 2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Cervical Cancer Screening
Past… PRESENT…Future
Audrey P. Garrett, MD, MPH Women’s Health Symposium
September 7, 2012

Disclosure
• On Speaker bureau for Merck for Gardasil • On Speaker bureau for Hologic for Cervista

Objectives
• Review basis for new guidelines • Review platforms for new guidelines • Review guidelines • Convince of the rationale for use of HPV
testing in cervical cancer screening • Review strategies for discussing test results
with patients
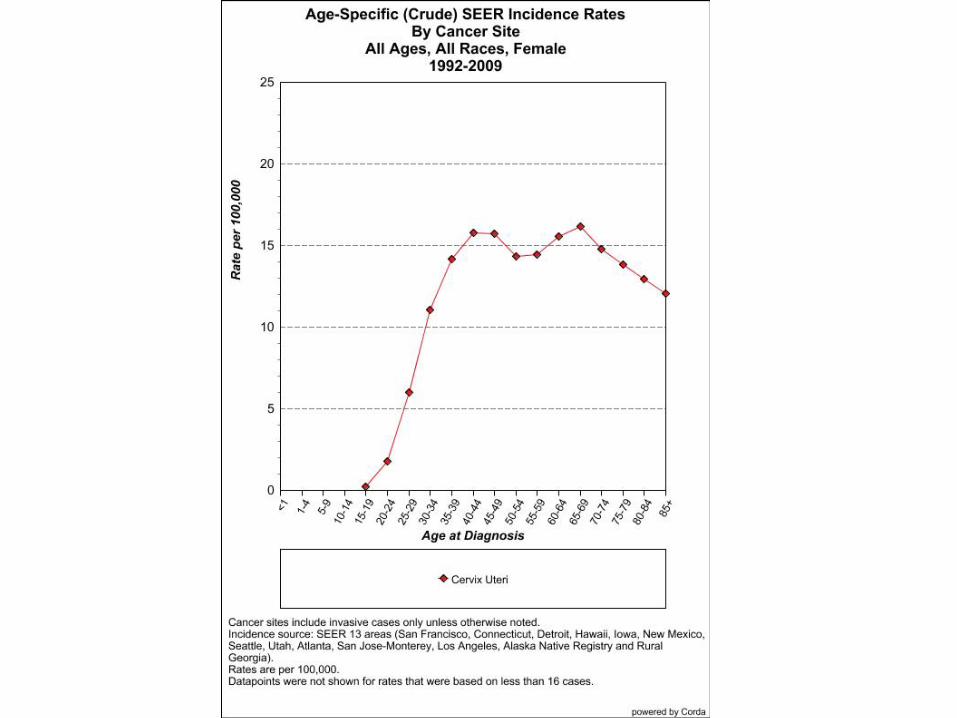
Cervical Cancer
• 500,000 cases annually – 250,000 deaths annually
• Most common cause of cancer death • >80% occur in developing countries • 95% have never had a pap smear
Cervical Cancer: USA
• 12,200 cases annually • 4210 deaths 2010 • >60% have had no recent pap
– 83% population report screening in past year
• Death rate decreasing 4%/year – Decreased 70% since 1955
Cervical Cancer Hero • George Papanicolau: 1883-1962
Mary (wife/ MA)

Cervical Cancer Screening
• 1928 first cancer diagnosis by pap • 1941 paper presented • 1965 American Cancer Society
– Annual pap smear screening

Cervical Cancer Hero: Harald zur Hausen: Nobel Prize in Medicine, 2008

Understanding HPV: timeline
• 1973 zur Hausen hypothesis • 1983 HPV 16 isolated by Southern Blot • 1998 HPV test commercially available • 2001 vaccine trials started • 2006 HPV vaccines commercially available • 2006 HPV testing incorporated into screening • 2009 genotyping available and endorsed • 2011 4 FDA approved HPV testing platforms


HPV testing platforms
• 1998 Digene HC 2 (Qiagen) – Nucleic acid hybridization with signal amplification
using chemiluminescence • Hologic
– Invader technology, first to offer genotyping • Genprobe
– Qualitative detection of E6/E7 viral mRNA • Cobas/Roche
– PCR, uses single throughput technology
BY MIKAELA CONLEY @MIKAELACONLEY FOLLOW ON TWITTER
MAR 15, 2012 12:41PM NEW GUIDELINES DISCOURAGE YEARLY PAP TESTS

March 14, 2012
BY MIKAELA CONLEY @MIKAELACONLEY FOLLOW ON TWITTER
MAR 15, 2012 12:41PM NEW GUIDELINES DISCOURAGE YEARLY PAP TESTS
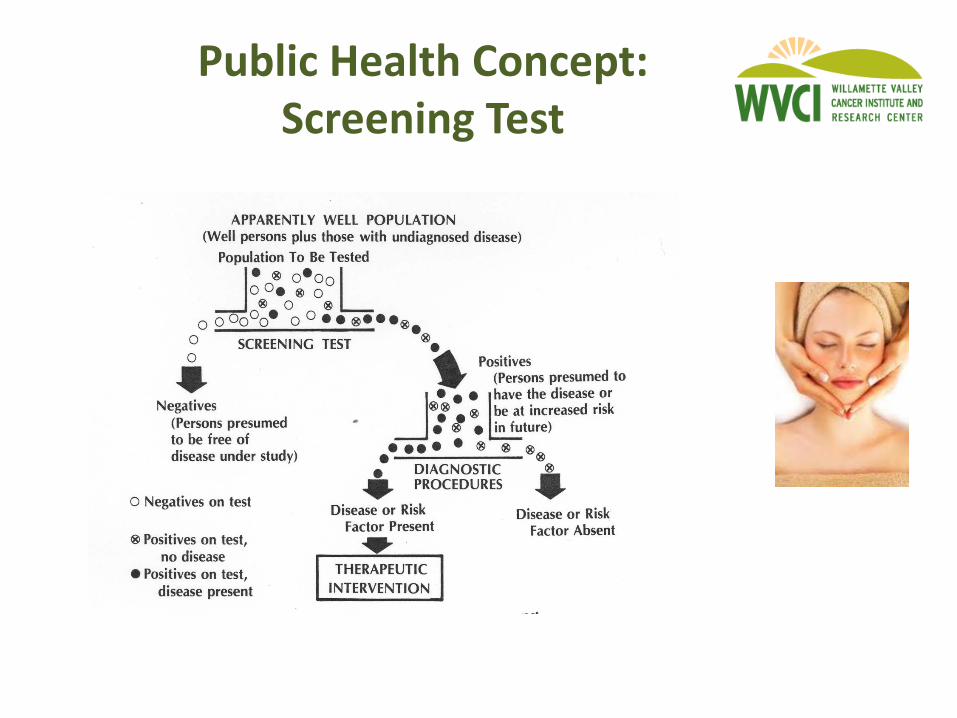

Screening Test
• Cervical cancer was common – 26,000 deaths/yr in early 20th century – 300,000 cases/yr of CIN3 now
• Lengthy pre-invasive process • Testing available
– Cervix accessible – Test inexpensive and “easy”
• Therapeutic intervention

Screening Test • Efficacy of test dependent on epidemiology
– Prevalence – Incidence
• Heavily pre-screened populations – Decrease prevalence – Stable incidence – Smaller incident lesions (lead time bias)
• Altered epidemiology of target lesion
Cervical Cancer and HPV
• HPV is ubiquitous • 100 subtypes identified • 40 predilection for ano-genital mucosa • 15 high risk sub-types • HPV 16, 18 most virulent and persistent
– 50% high grade dysplasias – 70-80% invasive cervical cancers

Cervical Cancer and HPV Biologic Plausibility
• HPV interacts with host genome – E6 and E7 interact P53 and RB
• Archival slides demonstrate presence • Prospective studies link HPV and dysplasia • 99% cervical cancers test positive • Vaccine data demonstrates efficacy

CaCx screening and HPV
• Pap swipes the ectocervix – Can miss endocervical lesions – Can miss very small lesions
• HPV represents risk of disease – Much stronger negative predictive value – Allows us to focus on those at risk – Allows us to reassure those at less risk
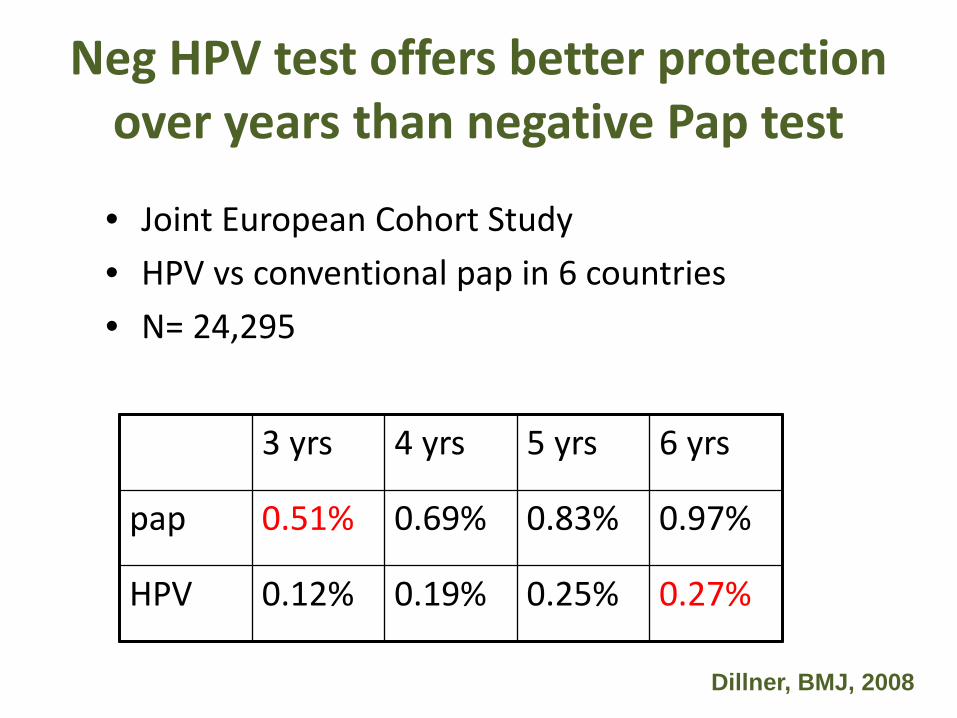
Neg HPV test offers better protection over years than negative Pap test
• Joint European Cohort Study • HPV vs conventional pap in 6 countries • N= 24,295
Dillner, BMJ, 2008
3 yrs 4 yrs 5 yrs 6 yrs
pap 0.51% 0.69% 0.83% 0.97%
HPV 0.12% 0.19% 0.25% 0.27%


Cervical Cancer: HPV
Cervical Cancer: Prevention
• Pap test: – 20% false negative rate – Compensate with frequent paps – 1 in 5 will have an abnormal pap
• Pap test 2012: – Changing epidemiology – Better testing available – Changing recommendations

Cervical Cancer Prevention: Get with the times…
“This dial phone has always worked for me…” “My patients would never be able to understand a more modern test…”

Cervical Cancer Prevention: HPV
• HPV testing is more sensitive and specific – 3 successive paps at 20% false neg: 3/1000 – Pap and HPV at 3 yrs: 1/1000
• HPV is highly predictive of disease – If HPV 16 pos, 17% risk at 10 yrs – If HPV 16/18 neg, <4% risk at 10 yrs
• HPV testing can decrease mortality from cervical cancer – NEJM Apr, 2009

Cervical Cancer: HPV

How much protection do we lose by not doing Pap tests every year?
• Percentage reduction in rate of invasive cacx in cohort of women aged 35-64 with different frequencies of screening – Next pap 1 year: 93.5%
• 30 paps required over 30 years – Next pap 2 years: 92.5%
• 15 paps over 30 years – Next pap 3 years: 90.8%
• 10 paps over 30 years – Next pap 5 years: 83.6%
• 6 paps required over 30 years – 3 well timed paps in a lifetime
• South Africa: 95% reduction in cacx mortality
IARC BMJ 293: 1986
How many cancers do we prevent:
• Assuming at least 3 consecutive neg paps • Cancers prevented by doing annual pap rather
than Q 3 yr – Age 30-44: 3/100,000 women – Age 45-59: 1/100,000 women
• Additional testing necessary to find each cancer – Age 30-44: 69,665 paps plus 3861 colpos – Age 45-59: 209,324 paps plus 11,502 colpos
Sawaya et al, NEJM, 2003
Rate of progression CIN3-> CA
• Increases with age – 80: 10% per year – 20-24: 0.5% per year – Adolescents: negligible
Moscicki, Cox, et al, JLGTD, 2010

Cervical Cancer Screening: ASCCP/ACOG guidelines
• No paps under 21 – Controversial but Public Health based – Difference between pap and pelvic exam – STD screens if sexually active
• HPV testing not useful under 21 – High prevalence – 90% infections resolve

Cervical Cancer Screening: ASCCP/USPSTF guidelines
• Primary cytology screening 21-29
– Triennial screening – REFLEX HPV testing for ASCUS
• Women 30-65: lengthened intervals – Triennial screening with cytology – Cotesting every FIVE years – CANNOT risk assess without HPV
Cervical Cancer Screening: Women over 30
• Cytology with HPV testing
– Pap NIL, HR HPV neg: retest 5 yrs
• Pap abnormal, regardless of HPV – Triage appropriately

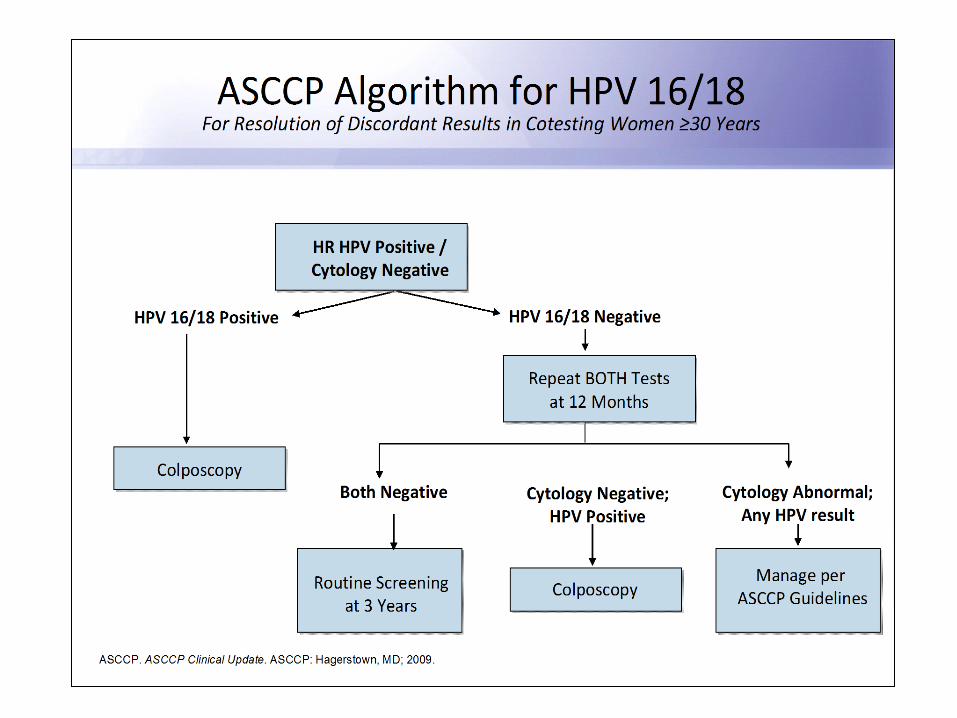
Cervical Cancer Screening: Women over 30
• Pap normal, HR HPV positive
– Repeat both 12 months • If HPV persistently positive, colpo
• Pap normal, HR HPV positive – Immediate reflex to HPV 16/18
• If positive, colpo • If negative, repeat

Cervical Cancer Screening: Women over 30
• Cytology with HPV testing
– May require alteration/ attention to req – May require patient education – May require EMR tickler system – Does NOT mean that patient does not need
annual exam – This is the stronger test
Cervical Cancer Screening: “other” guidelines
• Women over 65 – If adequate prior testing, cessation of screening
• Women who have had hysterectomy – If for non-HPV related causes, no screening
• Women who have had vaccination – Routine screening
• Women with new sexual partners – Routine screening

Cervical Cancer Screening: “higher risk women”
• Immunocompromise – HIV – Transplant recipient
• DES exposure in utero • Women with symptoms
– Aka not SCREENING
• Women with prior HPV related disease/treatment
The Changing Landscape of Cervical Cancer Screening
• New epidemiology – Understanding other HPV strains
• New vaccines – To cover that new understanding
• New recommendations – To accommodate that new
understanding


Cervical Cancer: Vaccines GARDASIL (Merck)
16, 18, 6, 11 2006 for girls 9-26, 2009 for boys 9-26 2010 gained indication for anal cancer
Cervarix (GSK) 16,18
2009 for girls 9-26 34% of eligible patients are vaccinated
ACOG recommends documenting vaccine status at each visit

Risk Stratification with HPV Types 16 and 18 in Women ≥ 30 Years of Age with Negative Cytology
HPV 16 positive HPV 18 positive Non-HPV 16/18 positive HPV-negative
In women ≥ 30 years of age, 10-year cumulative incidence of ≥ CIN 3 was 20% and 18% for HPV 16/18, respectively
Khan MJ, et al. J Natl Cancer Inst. 2005;87(14):1072-1079.
Follow-up Time (Years)
Cum
ulat
ive
Inci
denc
e Ra
te o
f ≥
CIN
3 (%
)
0
5
10
15
20
25
0.4 1.25 2.25 3.25 4.25 5.25 6.25 7.25 8.25 9.25 9.95

Smith J, et al. Int J Cancer. 2007;121:621-632.
16 alone
16 + 18
+ 35
+ 31
+ 33
+ 45
+ 52
+ 58
+ 59
54.7%
76.4%
83.7%
87.6%
91.0%
93.6%
94.2%
94.4%
94.5%
Cumulative Prevalence Incremental Prevalence
> 75% of Squamous Cancers in the United States Are Caused by HPV 16/18
HPV
Type
s
Proportion of Cancers Associated with HPV Types
Why Are HPV 16/18 Important?
Related Documents











