Cervical Cancer: Disease burden and Screening Medical Management in Metastatic and Recurrent Cervical Cancer Dr Alok Gupta

Cervical cancer - Role of screening and management of advanced stage cervical cancer
Jan 22, 2018
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Cervical Cancer: Disease burden and Screening
Medical Management in Metastatic and Recurrent Cervical Cancer
Dr Alok Gupta

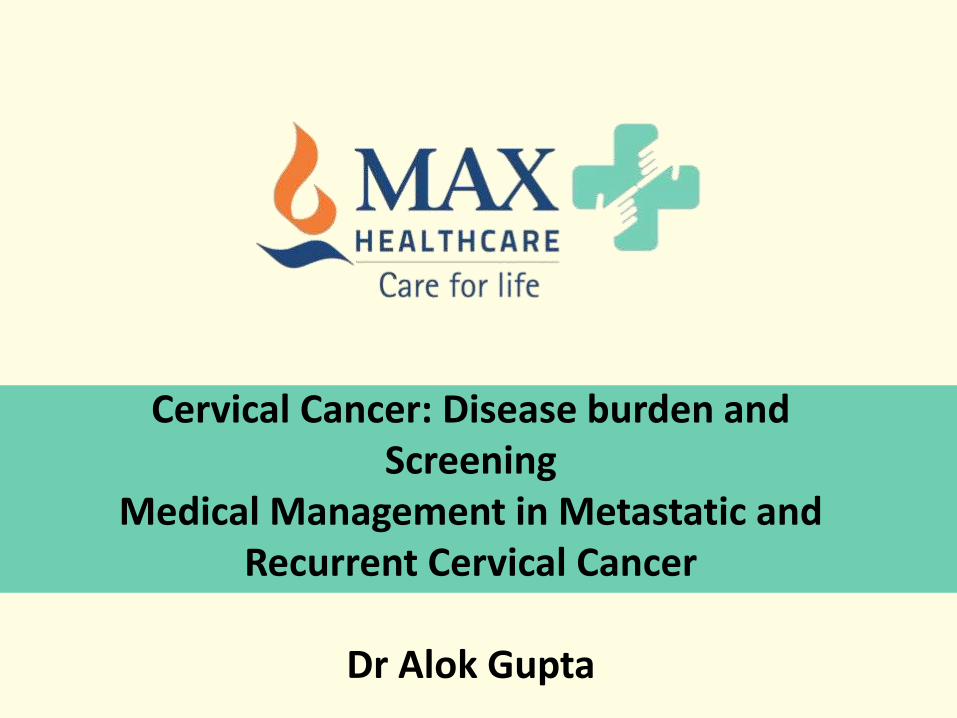
> 500,000diagnosed annually1
> 275,000deaths annually1
CERVICAL CANCER
GLOBAL SCENARIO
>85% of the global burden occurs in
developing countries1
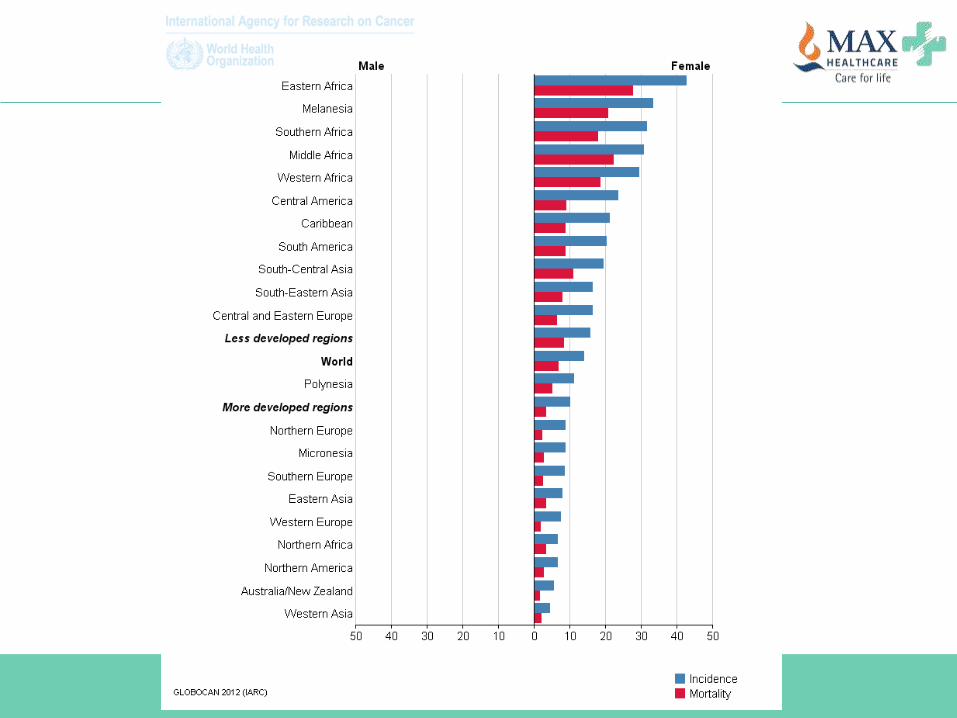
Estimated Cervical Cancer Incidence Worldwide
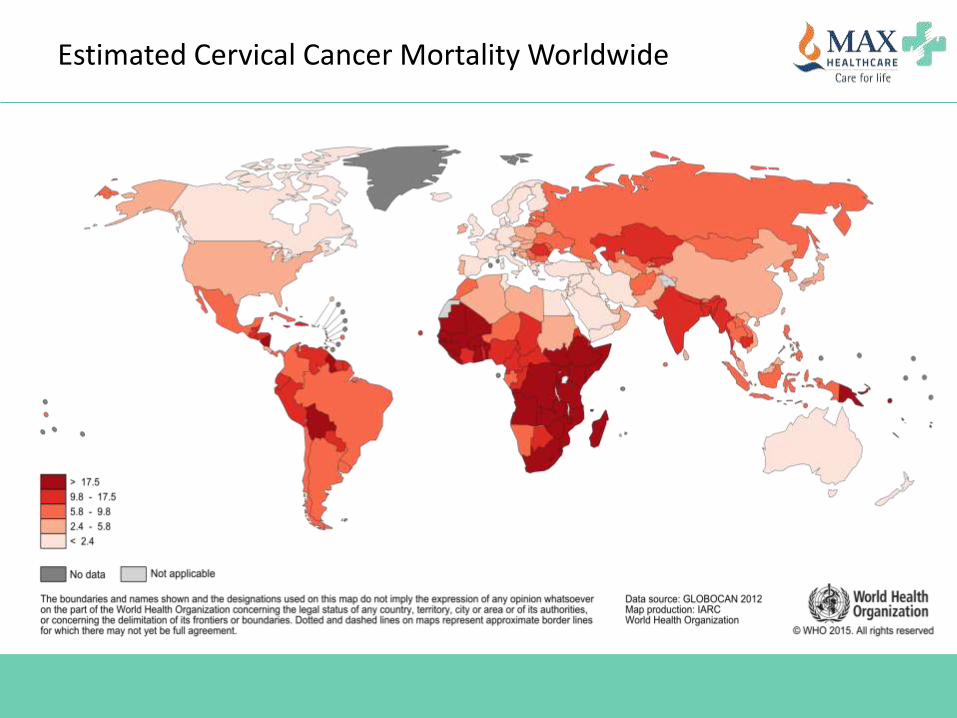
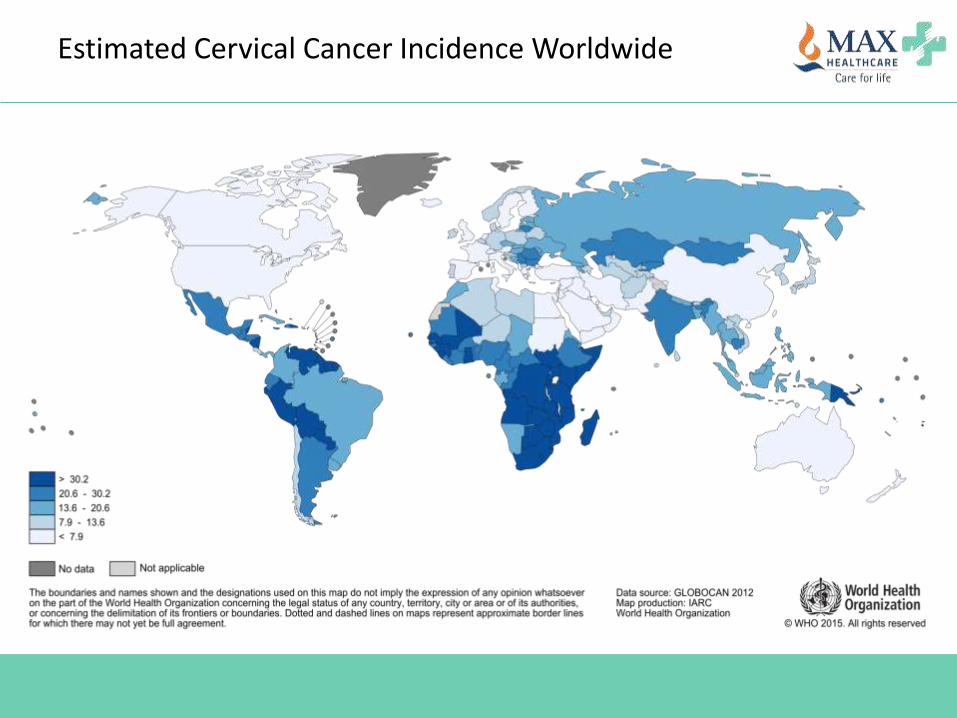
Estimated Cervical Cancer Mortality Worldwide
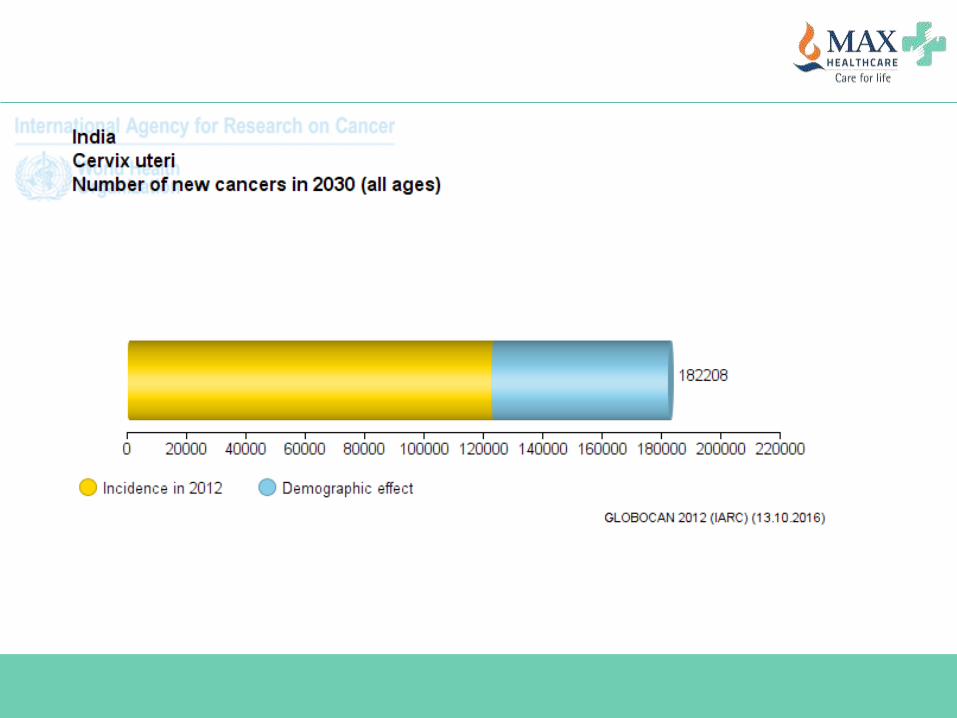
> 120,000diagnosed annually1
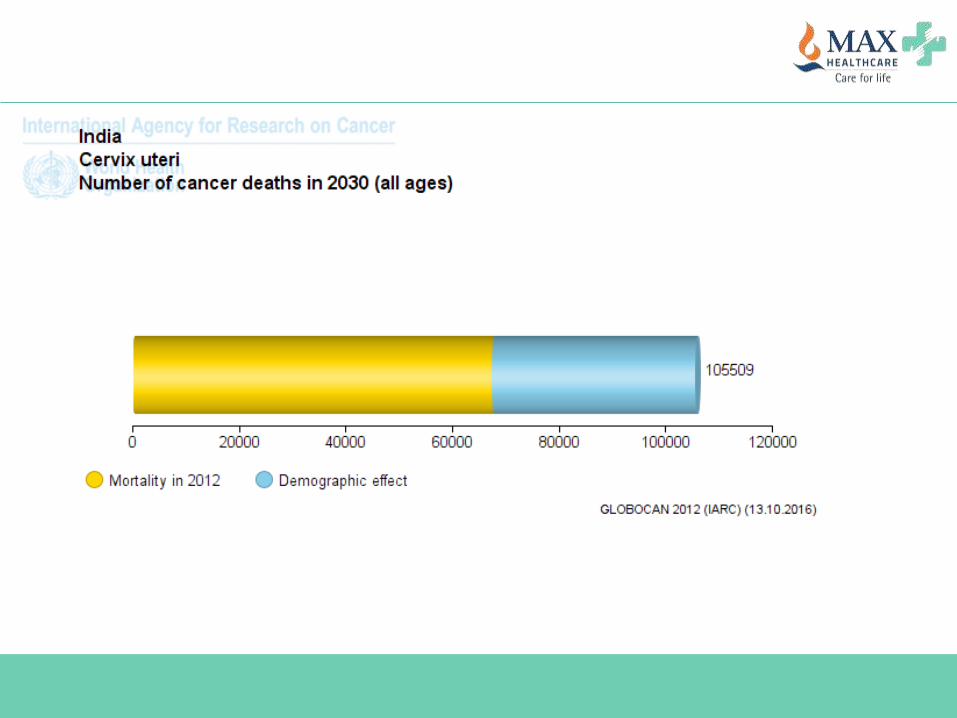
> 67,000deaths annually1
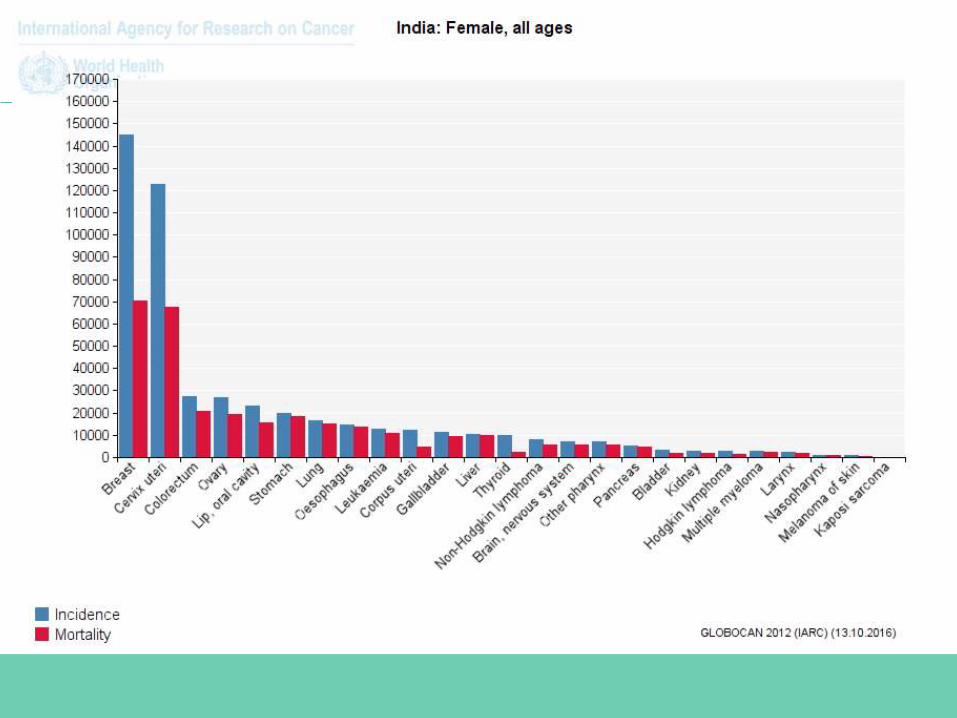
2nd most
common cancer
in Indian
females1
CERVICAL CANCER
INDIAN SCENARIO
1. Globocan, 2008;
CAUSES?
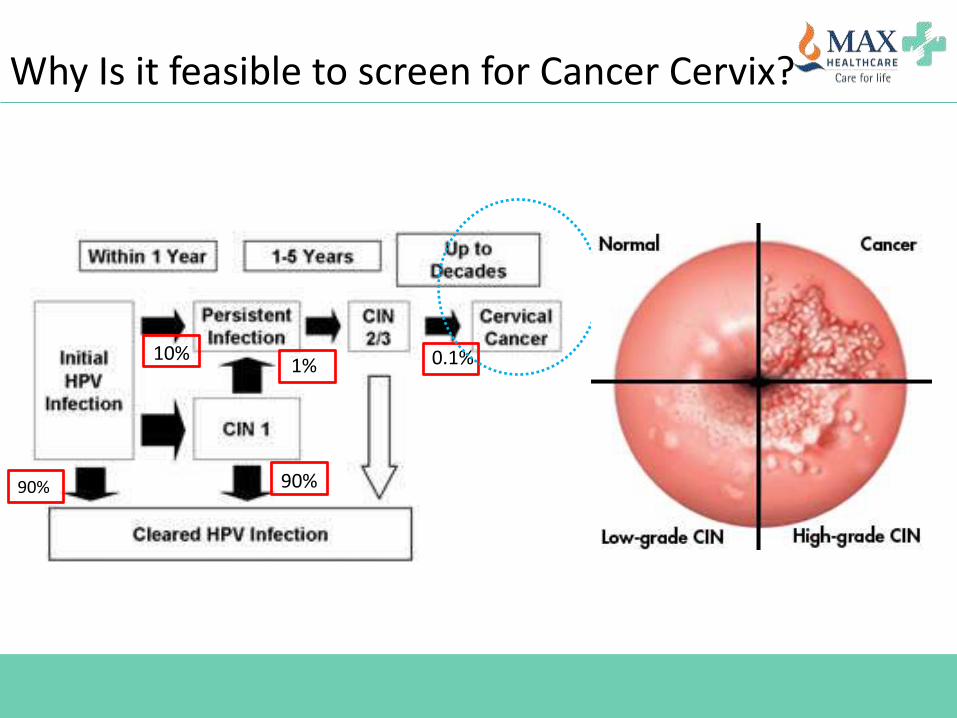
90%
10%
90%
1% 0.1%
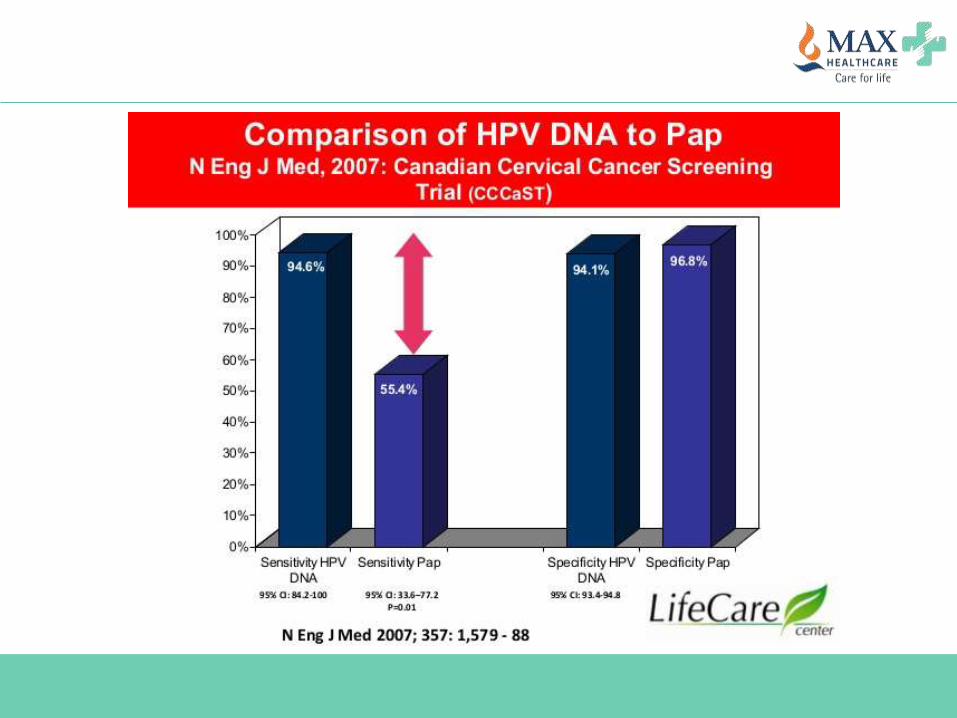
Why Is it feasible to screen for Cancer Cervix?
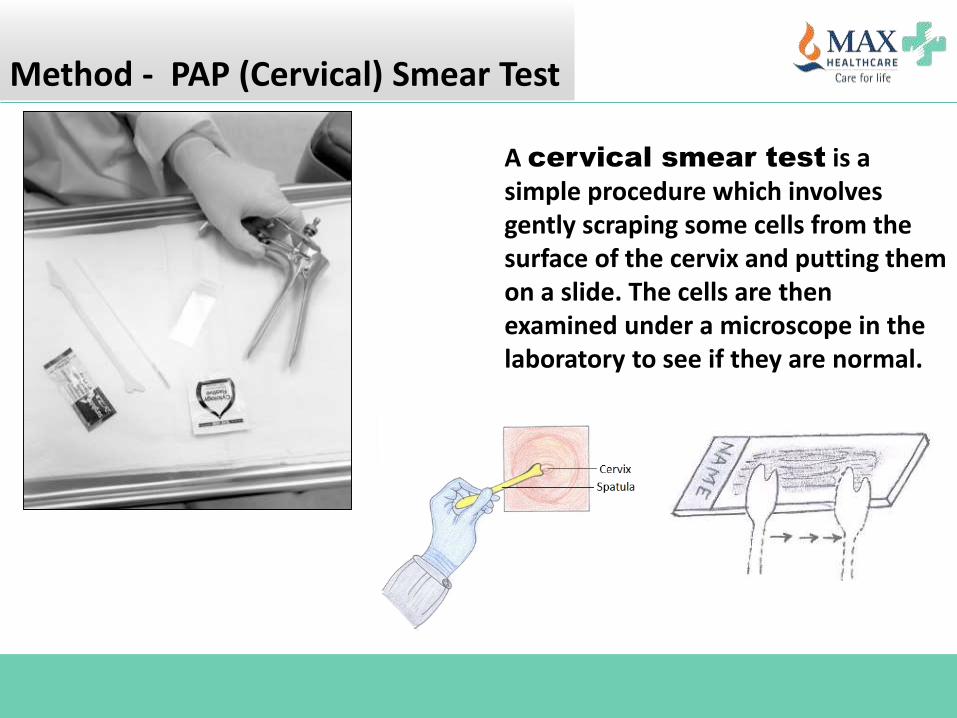
Method - PAP (Cervical) Smear Test
A cervical smear test is a simple procedure which involves gently scraping some cells from the surface of the cervix and putting them on a slide. The cells are then examined under a microscope in the laboratory to see if they are normal.
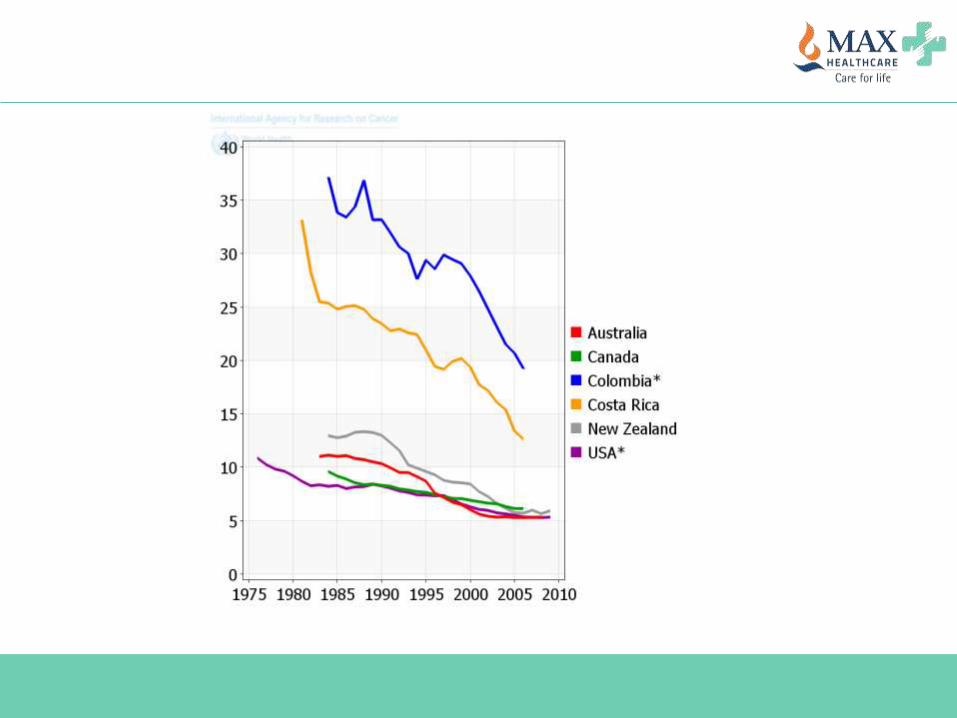
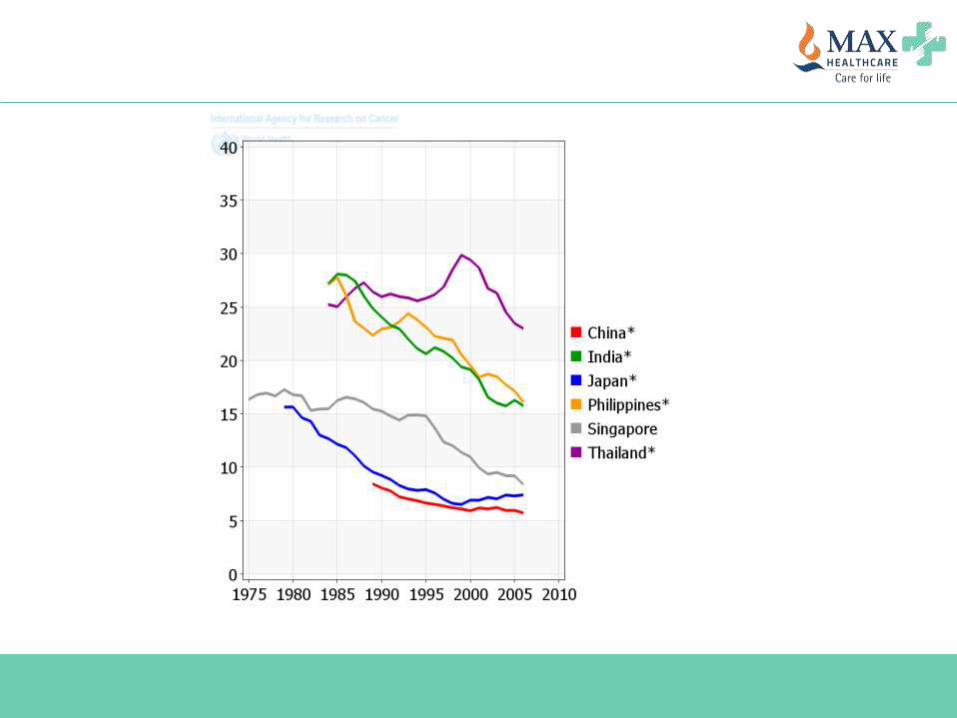
Benefit of screening in cervical cancer
70% reduction in cervical cancer deaths.
Now ranks 14th for cancer deaths in developed
world.
5-year survival rate is approximately 92%.
Screening Recommendations
Screening Recommendations
<21 years: No screening
21-30 years: PAP smear every 3 years
30-65 years: PAP smear every 3 years
30-65 years: PAP smear + HPV testing every 5
years
>65 years: No screening
Some practical points about cervical cancer screening
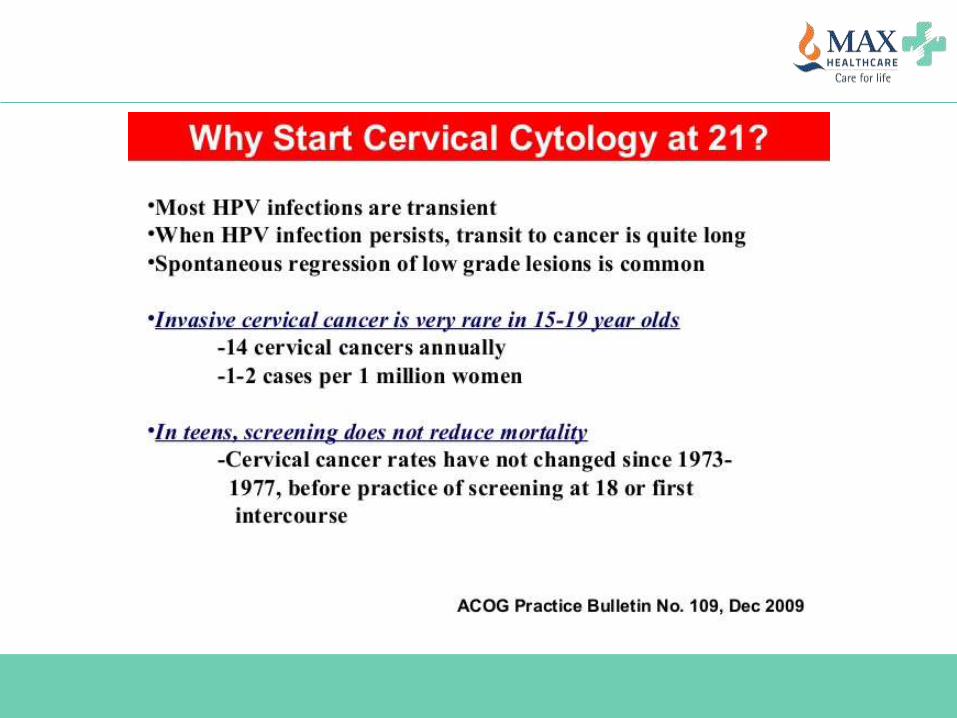
Why to start at 21 years of age?
Why to stop at 65 years of age?
What is the benefit of HPV co-testing?
Can we avoid Pap smear and do only HPV
testing?
Screening in vaccinated individual?
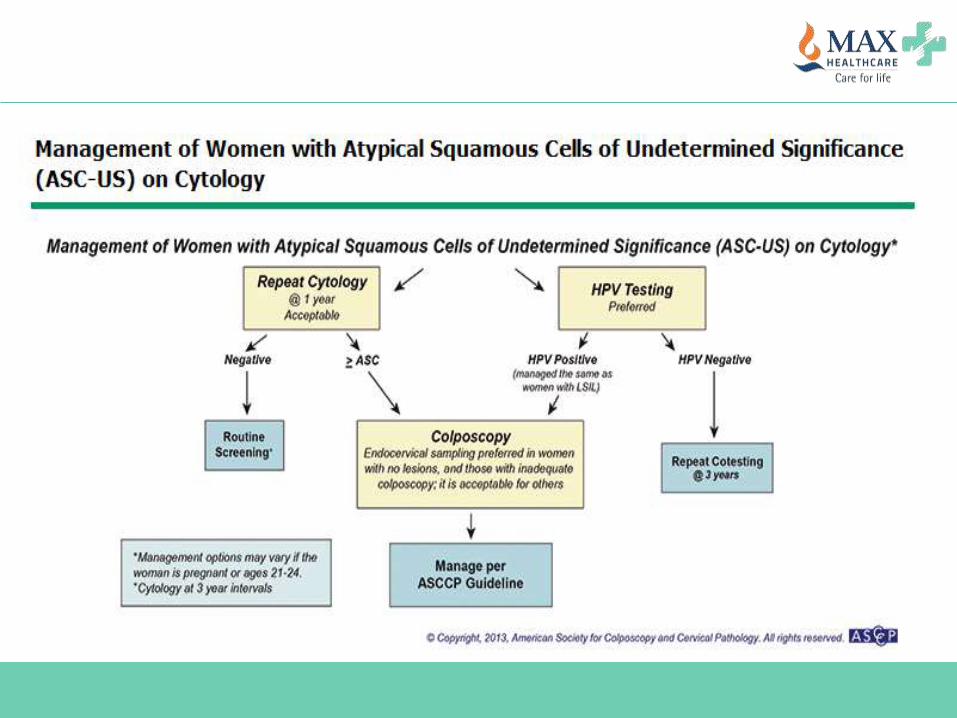
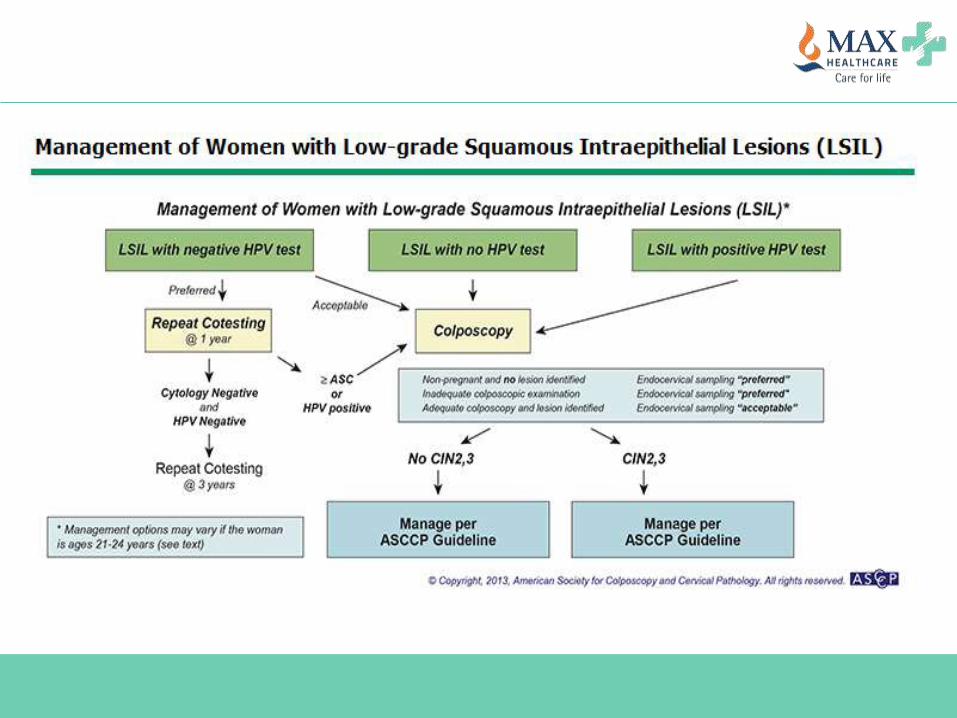
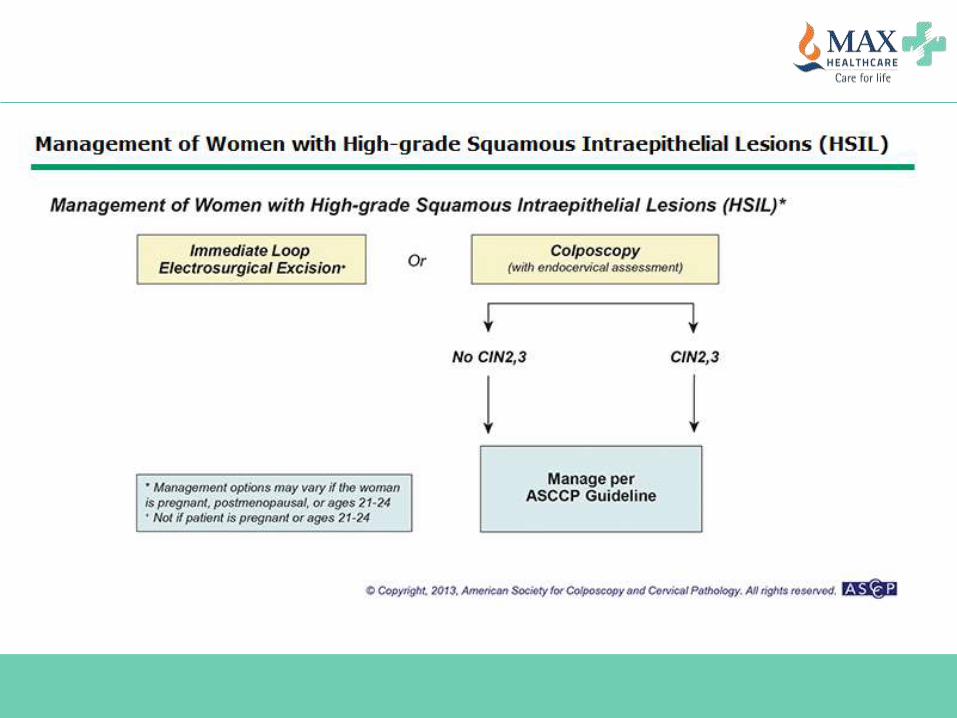
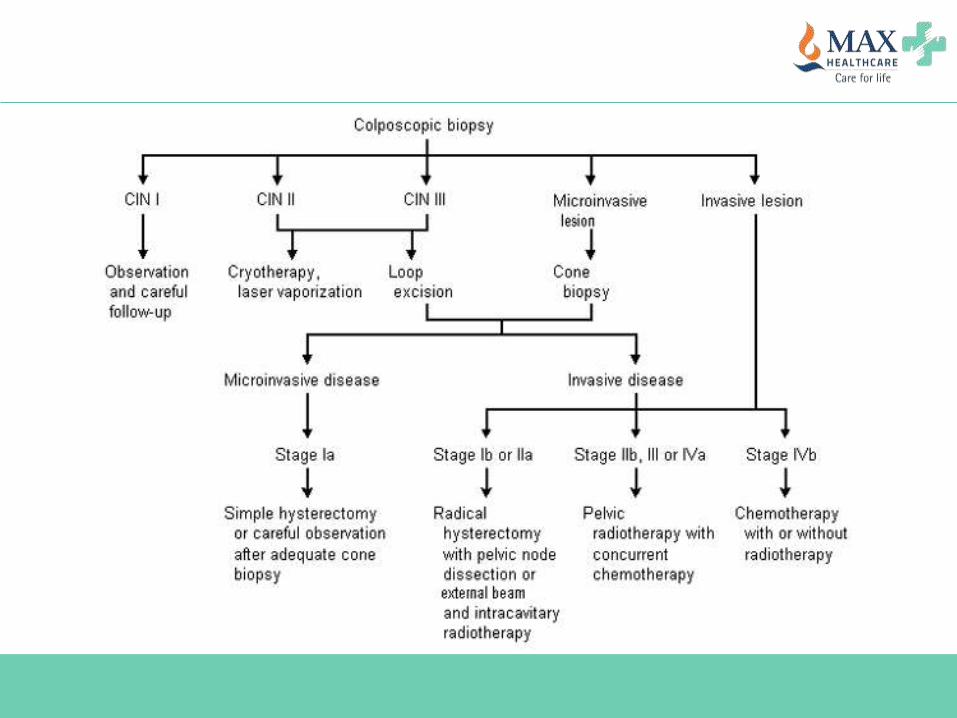
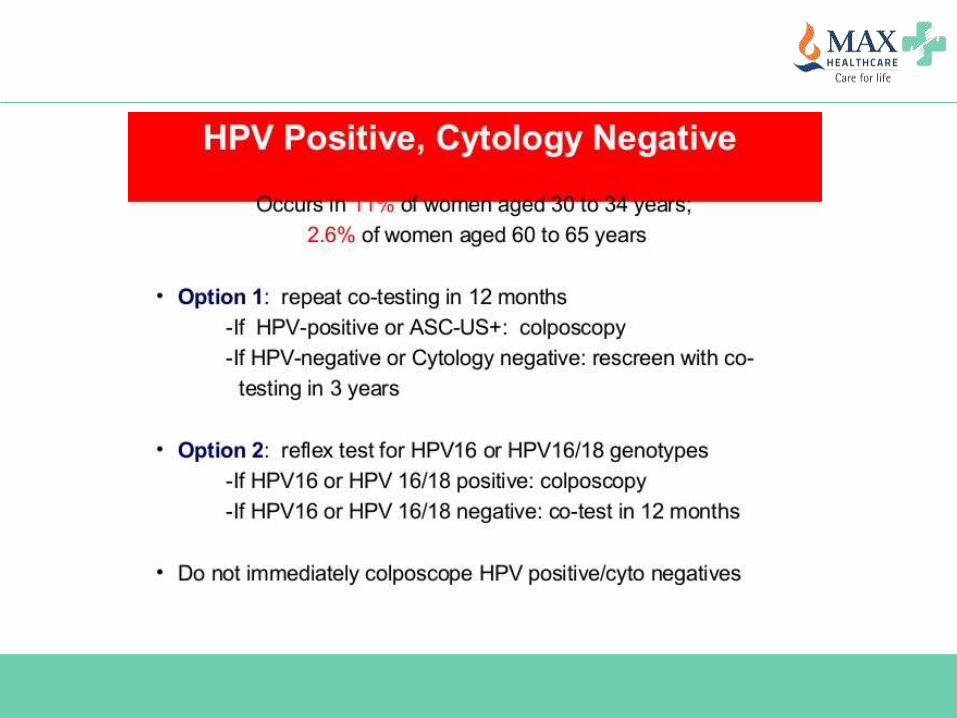
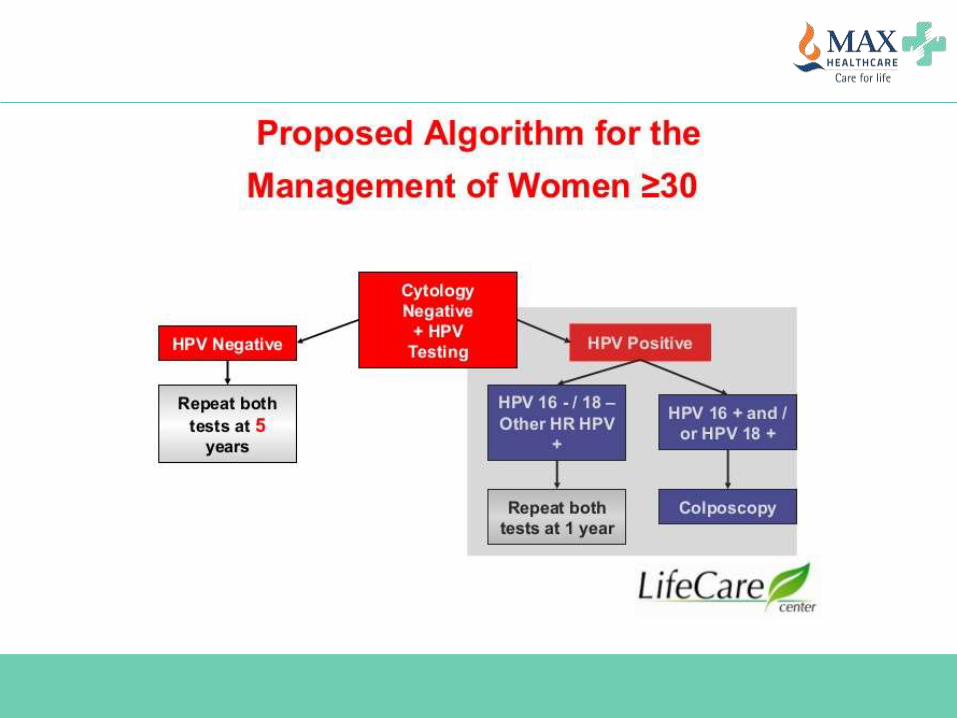
How to act on screening results?
What instructions will you give at the time of
screening?
Some practical points about cervical cancer screening
Why to start at 21 years of age?
Why to stop at 65 years of age?
What is the benefit of HPV co-testing?
Can we avoid Pap smear and do only HPV
testing?
Screening in vaccinated individual?
How to act on screening results?
What instructions will you give at the time of
screening?
Some practical points about cervical cancer screening
Why to start at 21 years of age?
Why to stop at 65 years of age?
What is the benefit of HPV co-testing?
Can we avoid Pap smear and do only HPV testing?
Screening in vaccinated individual?
How to act on screening results?
What instructions will you give at the time of
screening?
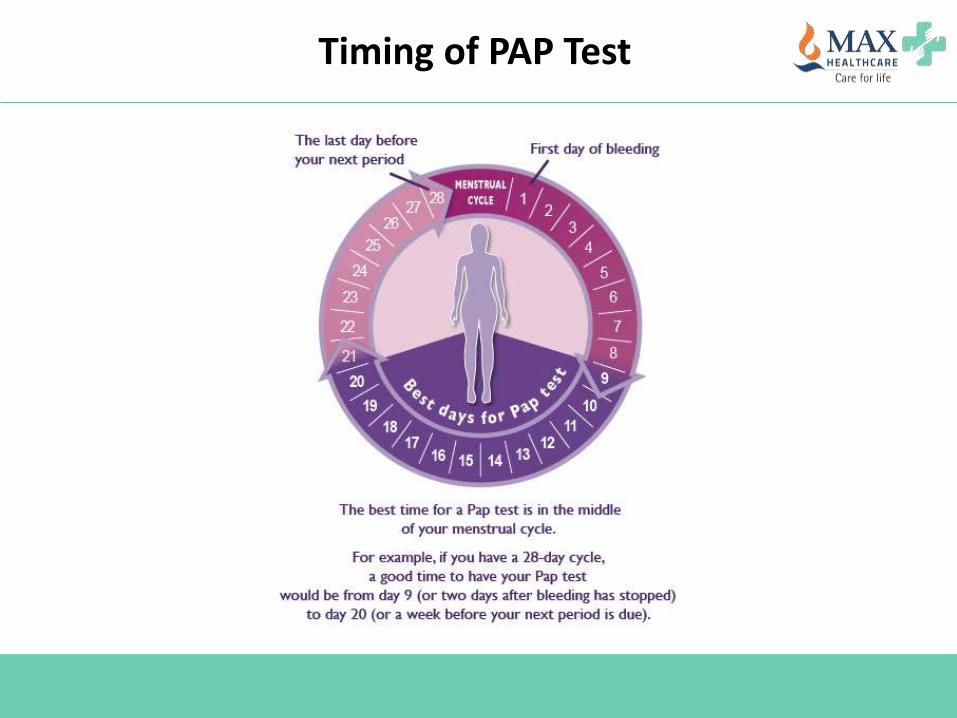
Timing of PAP Test
Instructions at the time of PAP Test
ICMR recommendation
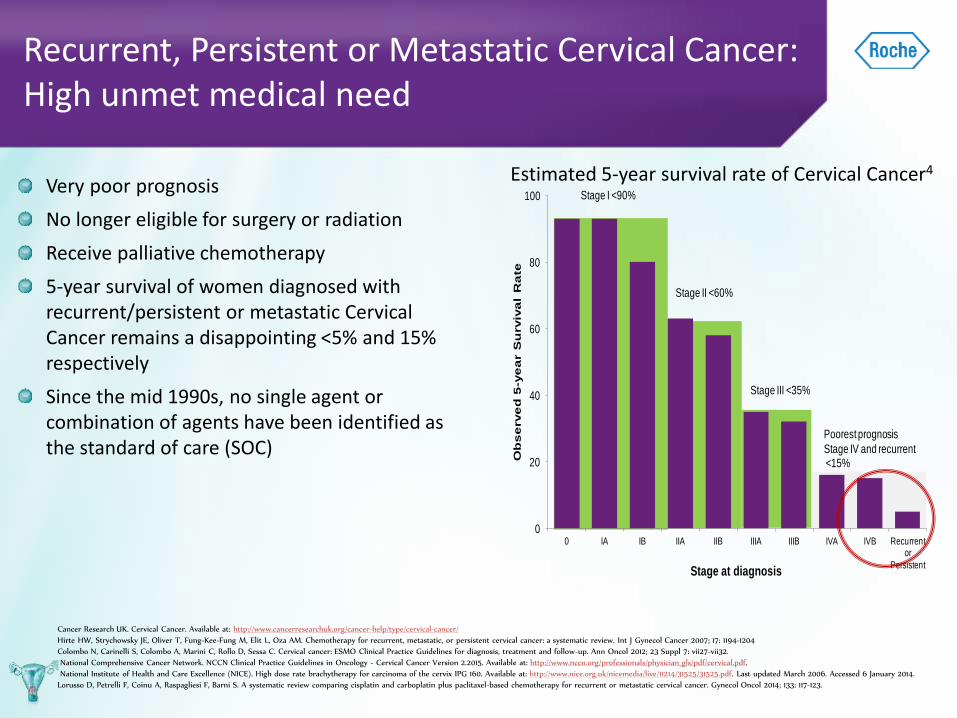
Stage II <60%
Stage III <35%
Poorest prognosis
Stage IV and recurrent<15%
Stage I <90%
0
20
40
60
80
100
0 IA IB IIA IIB IIIA IIIB IVA IVB Recurrent or
Persistent
Ob
se
rve
d 5
-ye
ar S
urviv
al
Ra
te
Stage at diagnosis
Recurrent, Persistent or Metastatic Cervical Cancer:High unmet medical need
Very poor prognosis
No longer eligible for surgery or radiation
Receive palliative chemotherapy
5-year survival of women diagnosed with recurrent/persistent or metastatic Cervical Cancer remains a disappointing <5% and 15% respectively
Since the mid 1990s, no single agent or combination of agents have been identified as the standard of care (SOC)
Estimated 5-year survival rate of Cervical Cancer4
Cancer Research UK. Cervical Cancer. Available at: http://www.cancerresearchuk.org/cancer-help/type/cervical-cancer/
Hirte HW, Strychowsky JE, Oliver T, Fung-Kee-Fung M, Elit L, Oza AM. Chemotherapy for recurrent, metastatic, or persistent cervical cancer: a systematic review. Int J Gynecol Cancer 2007; 17: 1194-1204
Colombo N, Carinelli S, Colombo A, Marini C, Rollo D, Sessa C. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2012; 23 Suppl 7: vii27-vii32.
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology - Cervical Cancer Version 2.2015. Available at: http://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf.
National Institute of Health and Care Excellence (NICE). High dose rate brachytherapy for carcinoma of the cervix IPG 160. Available at: http://www.nice.org.uk/nicemedia/live/11214/31525/31525.pdf. Last updated March 2006. Accessed 6 January 2014.
Lorusso D, Petrelli F, Coinu A, Raspagliesi F, Barni S. A systematic review comparing cisplatin and carboplatin plus paclitaxel-based chemotherapy for recurrent or metastatic cervical cancer. Gynecol Oncol 2014; 133: 117-123.
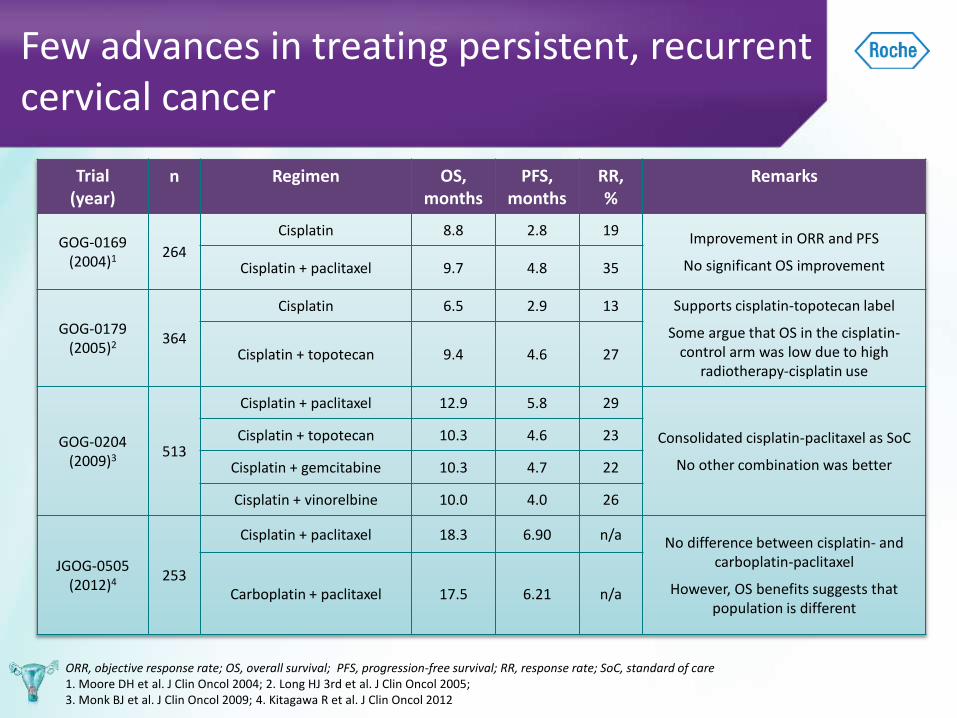
Few advances in treating persistent, recurrent cervical cancer
Trial (year)
n Regimen OS, months
PFS, months
RR, %
Remarks
GOG-0169 (2004)1 264
Cisplatin 8.8 2.8 19Improvement in ORR and PFS
No significant OS improvementCisplatin + paclitaxel 9.7 4.8 35
GOG-0179 (2005)2 364
Cisplatin 6.5 2.9 13 Supports cisplatin-topotecan label
Some argue that OS in the cisplatin-control arm was low due to high
radiotherapy-cisplatin useCisplatin + topotecan 9.4 4.6 27
GOG-0204 (2009)3 513
Cisplatin + paclitaxel 12.9 5.8 29
Consolidated cisplatin-paclitaxel as SoC
No other combination was better
Cisplatin + topotecan 10.3 4.6 23
Cisplatin + gemcitabine 10.3 4.7 22
Cisplatin + vinorelbine 10.0 4.0 26
JGOG-0505 (2012)4 253
Cisplatin + paclitaxel 18.3 6.90 n/a No difference between cisplatin- and carboplatin-paclitaxel
However, OS benefits suggests that population is different
Carboplatin + paclitaxel 17.5 6.21 n/a
ORR, objective response rate; OS, overall survival; PFS, progression-free survival; RR, response rate; SoC, standard of care 1. Moore DH et al. J Clin Oncol 2004; 2. Long HJ 3rd et al. J Clin Oncol 2005; 3. Monk BJ et al. J Clin Oncol 2009; 4. Kitagawa R et al. J Clin Oncol 2012
CERVICAL CANCER:EMERGING THERAPIES
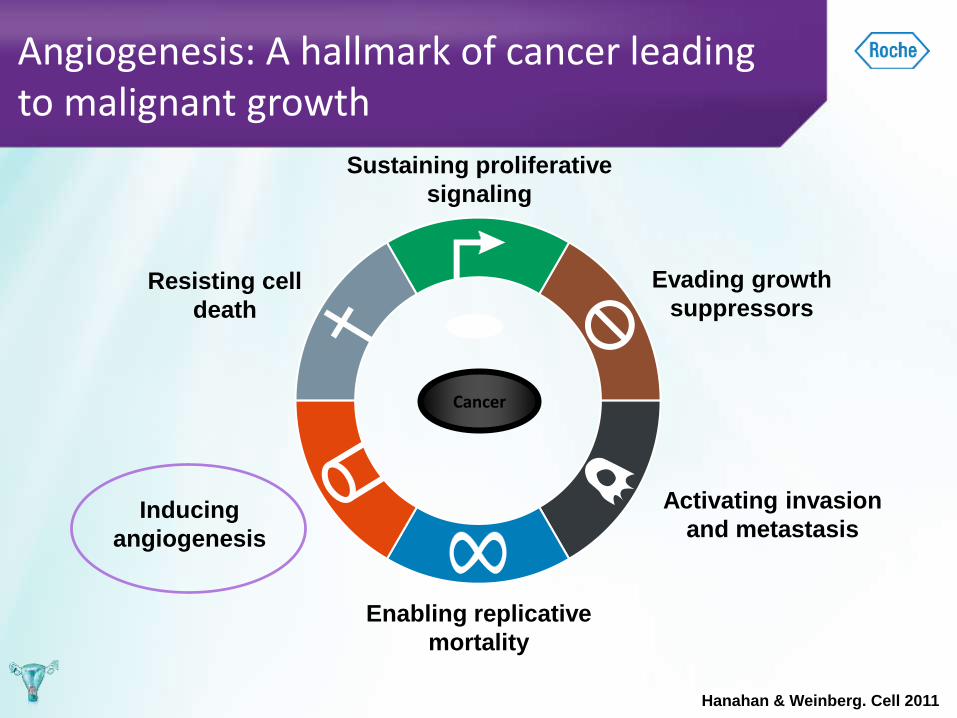
Inducing
angiogenesis
Angiogenesis: A hallmark of cancer leading to malignant growth
Cancer
Sustaining proliferative
signaling
Evading growth
suppressors
Activating invasion
and metastasis
Enabling replicative
mortality
Resisting cell
death
Hanahan & Weinberg. Cell 2011
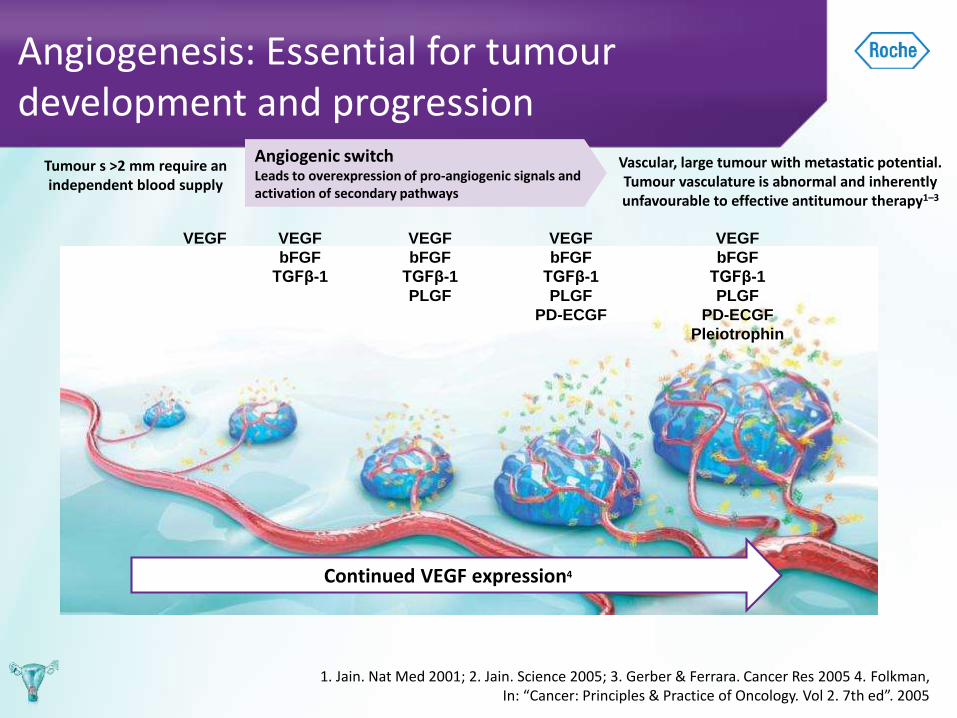
Angiogenesis: Essential for tumour development and progression
1. Jain. Nat Med 2001; 2. Jain. Science 2005; 3. Gerber & Ferrara. Cancer Res 2005 4. Folkman, In: “Cancer: Principles & Practice of Oncology. Vol 2. 7th ed”. 2005
Tumour s >2 mm require an independent blood supply
Angiogenic switchLeads to overexpressionof pro-angiogenic signalsand activation of secondary pathways
Continued VEGF expression4
VEGF VEGF
bFGF
TGFβ-1
VEGF
bFGF
TGFβ-1
PLGF
VEGF
bFGF
TGFβ-1
PLGF
PD-ECGF
VEGF
bFGF
TGFβ-1
PLGF
PD-ECGF
Pleiotrophin
Vascular, large tumour with metastatic potential. Tumour vasculature is abnormal and inherently unfavourable to effective antitumour therapy1–3
Angiogenic switchLeads to overexpression of pro-angiogenic signals and activation of secondary pathways
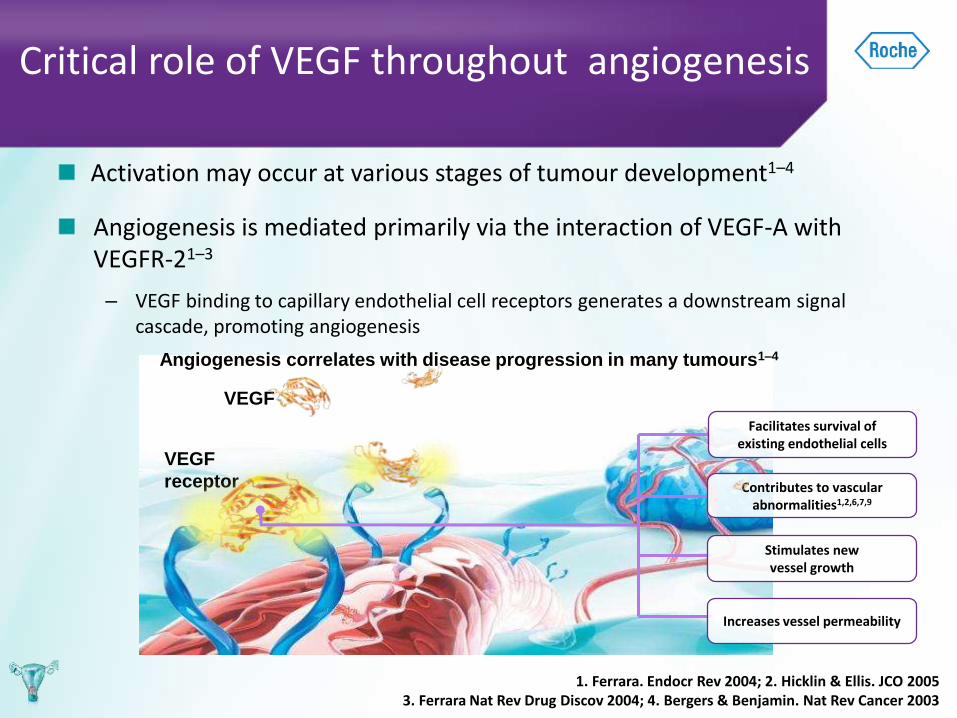
Activation may occur at various stages of tumour development1–4
Angiogenesis is mediated primarily via the interaction of VEGF-A with VEGFR-21–3
– VEGF binding to capillary endothelial cell receptors generates a downstream signal cascade, promoting angiogenesis
Critical role of VEGF throughout angiogenesis
1. Ferrara. Endocr Rev 2004; 2. Hicklin & Ellis. JCO 2005 3. Ferrara Nat Rev Drug Discov 2004; 4. Bergers & Benjamin. Nat Rev Cancer 2003
VEGF
VEGF
receptor
Angiogenesis correlates with disease progression in many tumours1–4
Increases vessel permeability
Contributes to vascular abnormalities1,2,6,7,9
Facilitates survival of existing endothelial cells
Stimulates new vessel growth

AVASTIN: MECHANISM OF ACTION
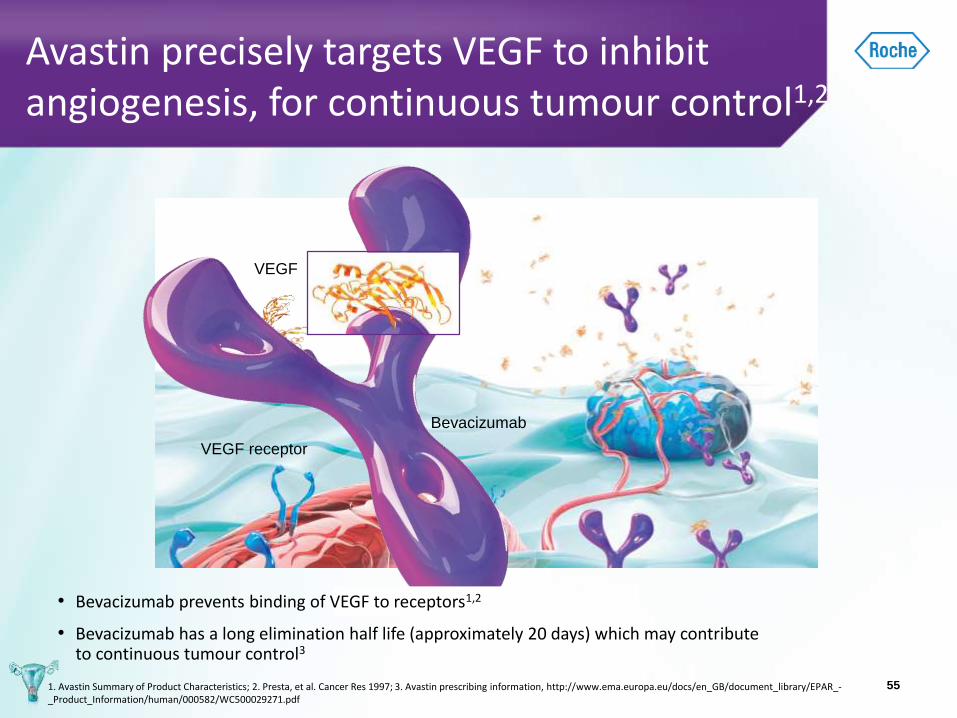
Avastin precisely targets VEGF to inhibit angiogenesis, for continuous tumour control1,2
55
Bevacizumab
VEGF receptor
VEGF
1. Avastin Summary of Product Characteristics; 2. Presta, et al. Cancer Res 1997; 3. Avastin prescribing information, http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000582/WC500029271.pdf
• Bevacizumab prevents binding of VEGF to receptors1,2
• Bevacizumab has a long elimination half life (approximately 20 days) which may contribute to continuous tumour control3
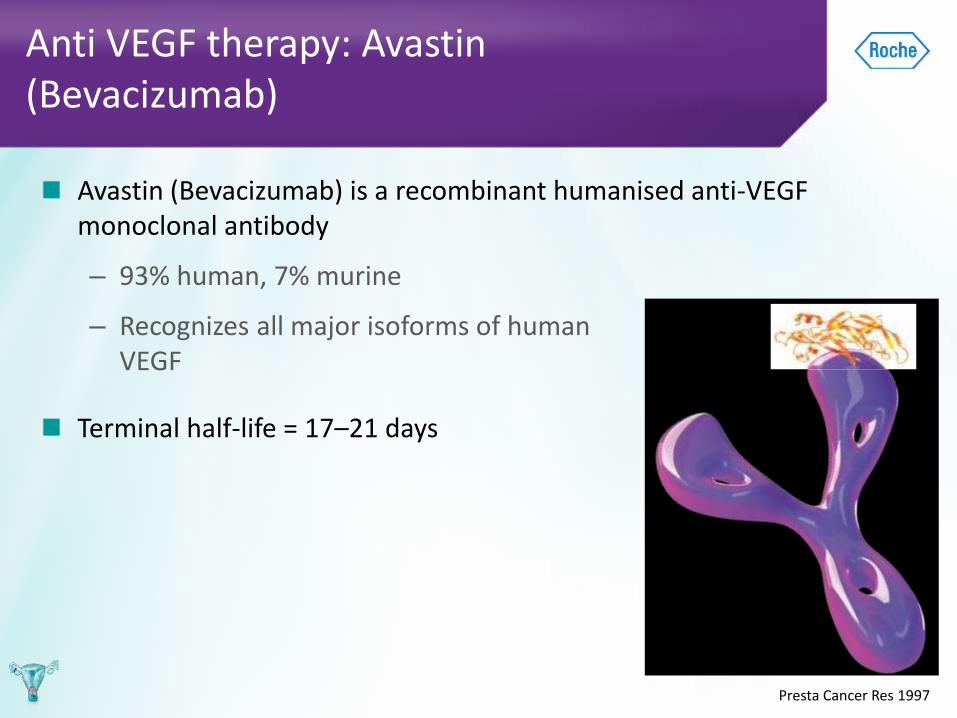
Avastin (Bevacizumab) is a recombinant humanised anti-VEGF monoclonal antibody
– 93% human, 7% murine
– Recognizes all major isoforms of human VEGF
Terminal half-life = 17–21 days
Anti VEGF therapy: Avastin (Bevacizumab)
Presta Cancer Res 1997
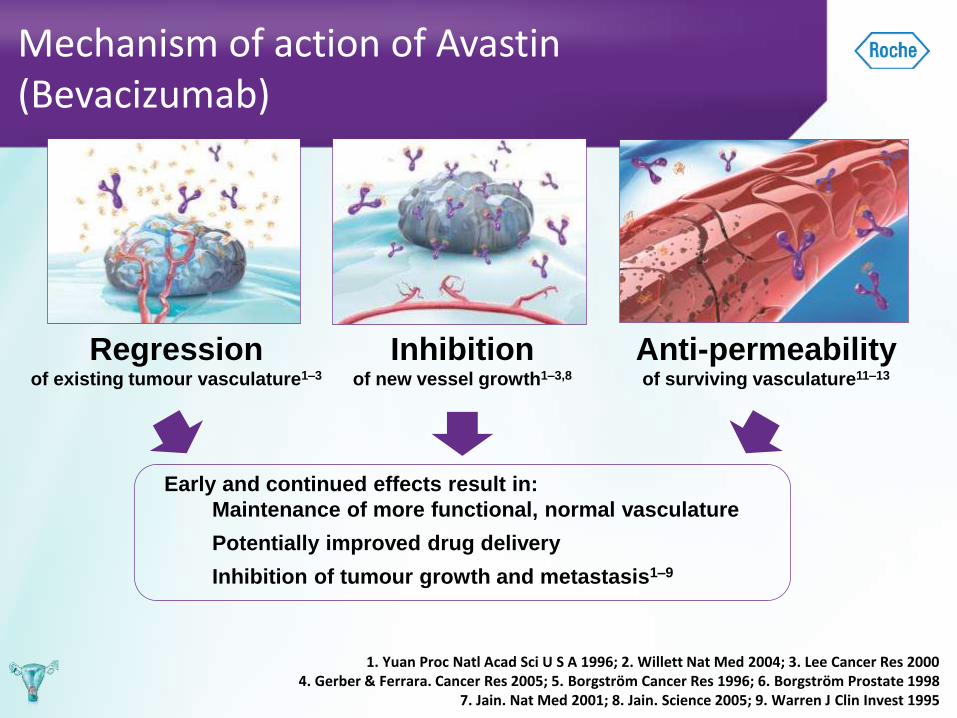
Mechanism of action of Avastin (Bevacizumab)
1. Yuan Proc Natl Acad Sci U S A 1996; 2. Willett Nat Med 2004; 3. Lee Cancer Res 2000 4. Gerber & Ferrara. Cancer Res 2005; 5. Borgström Cancer Res 1996; 6. Borgström Prostate 1998
7. Jain. Nat Med 2001; 8. Jain. Science 2005; 9. Warren J Clin Invest 1995
Regressionof existing tumour vasculature1–3
Inhibitionof new vessel growth1–3,8
Early and continued effects result in:
Maintenance of more functional, normal vasculature
Potentially improved drug delivery
Inhibition of tumour growth and metastasis1–9
Anti-permeabilityof surviving vasculature11–13
CERVICAL CANCER:AVASTIN IN TREATMENT LANDSCAPE
Improved Survival with Bevacizumab in Advanced Cervical Cancer1
GOG 240 study
1. Tewari KS, et al. N Engl J Med 2014;370:734-43.
GOG, Gynecologic Oncology Group;
PS, performance status
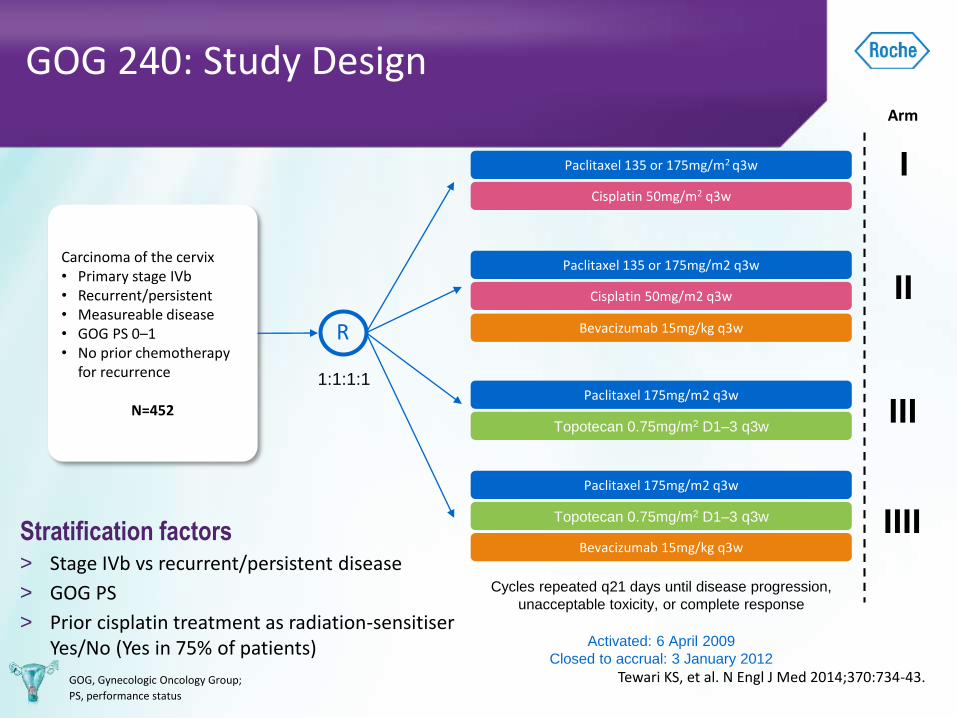
Carcinoma of the cervix• Primary stage IVb• Recurrent/persistent • Measureable disease • GOG PS 0–1• No prior chemotherapy
for recurrence
N=452
1:1:1:1
Arm
Activated: 6 April 2009
Closed to accrual: 3 January 2012
Stratification factors> Stage IVb vs recurrent/persistent disease
> GOG PS
> Prior cisplatin treatment as radiation-sensitiserYes/No (Yes in 75% of patients)
R
Paclitaxel 135 or 175mg/m2 q3w I
II
III
Cisplatin 50mg/m2 q3w
Paclitaxel 135 or 175mg/m2 q3w
Cisplatin 50mg/m2 q3w
Paclitaxel 175mg/m2 q3w
Topotecan 0.75mg/m2 D1–3 q3w
Topotecan 0.75mg/m2 D1–3 q3w
Bevacizumab 15mg/kg q3w
IIII
Bevacizumab 15mg/kg q3w
Paclitaxel 175mg/m2 q3w
Cycles repeated q21 days until disease progression,
unacceptable toxicity, or complete response
Tewari KS, et al. N Engl J Med 2014;370:734-43.
GOG 240: Study Design
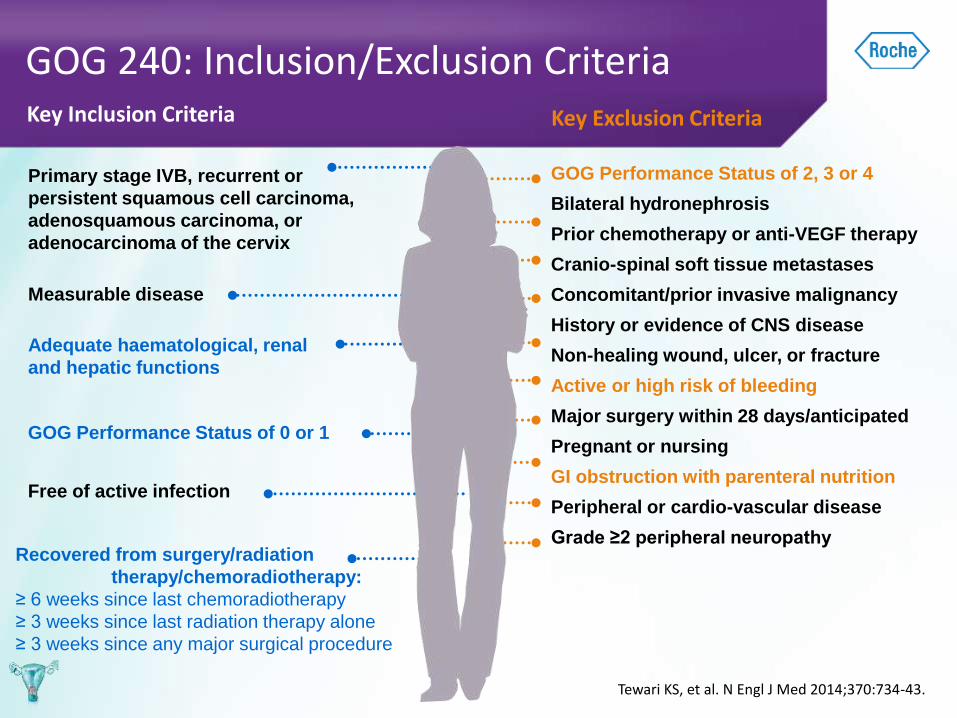
Recovered from surgery/radiation
therapy/chemoradiotherapy:
≥ 6 weeks since last chemoradiotherapy
≥ 3 weeks since last radiation therapy alone
≥ 3 weeks since any major surgical procedure
Free of active infection
GOG Performance Status of 0 or 1
Measurable disease
Primary stage IVB, recurrent or
persistent squamous cell carcinoma,
adenosquamous carcinoma, or
adenocarcinoma of the cervix
Adequate haematological, renal
and hepatic functions
Key Inclusion Criteria
GOG Performance Status of 2, 3 or 4
Bilateral hydronephrosis
Prior chemotherapy or anti-VEGF therapy
Cranio-spinal soft tissue metastases
Concomitant/prior invasive malignancy
History or evidence of CNS disease
Non-healing wound, ulcer, or fracture
Active or high risk of bleeding
Major surgery within 28 days/anticipated
Pregnant or nursing
GI obstruction with parenteral nutrition
Peripheral or cardio-vascular disease
Grade ≥2 peripheral neuropathy
Key Exclusion Criteria
Tewari KS, et al. N Engl J Med 2014;370:734-43.
GOG 240: Inclusion/Exclusion Criteria
Pro
po
rtio
n S
urv
ivin
g
Months on Study
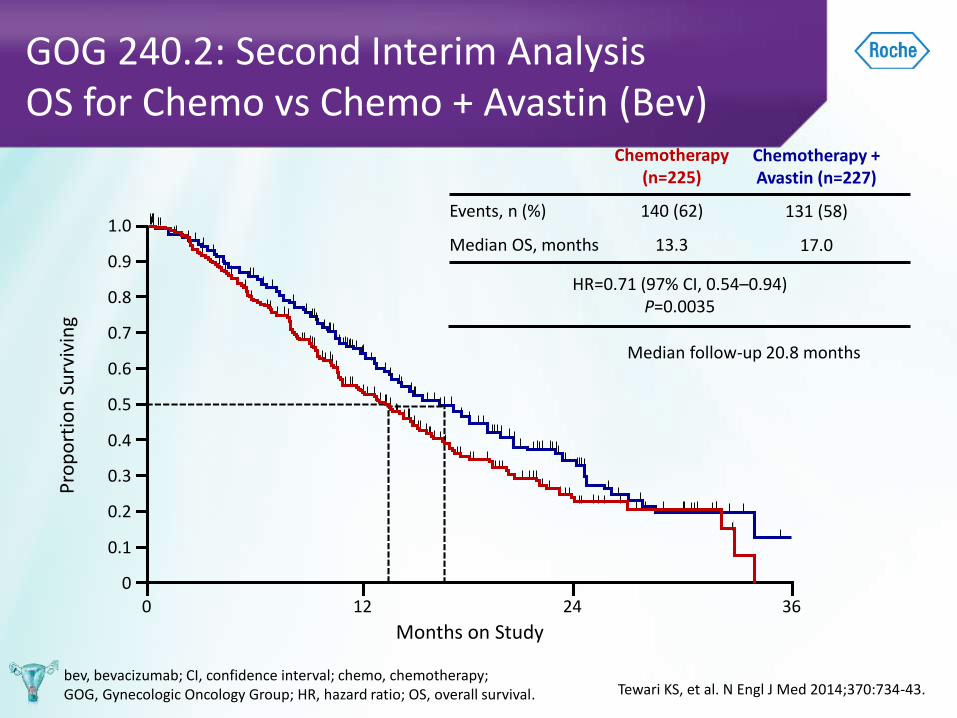
Median follow-up 20.8 months
GOG 240.2: Second Interim AnalysisOS for Chemo vs Chemo + Avastin (Bev)
bev, bevacizumab; CI, confidence interval; chemo, chemotherapy; GOG, Gynecologic Oncology Group; HR, hazard ratio; OS, overall survival.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3612 24
Chemotherapy(n=225)
Events, n (%) 140 (62)
Median OS, months 13.3
Chemotherapy + Avastin (n=227)
131 (58)
17.0
HR=0.71 (97% CI, 0.54–0.94)P=0.0035
Tewari KS, et al. N Engl J Med 2014;370:734-43.
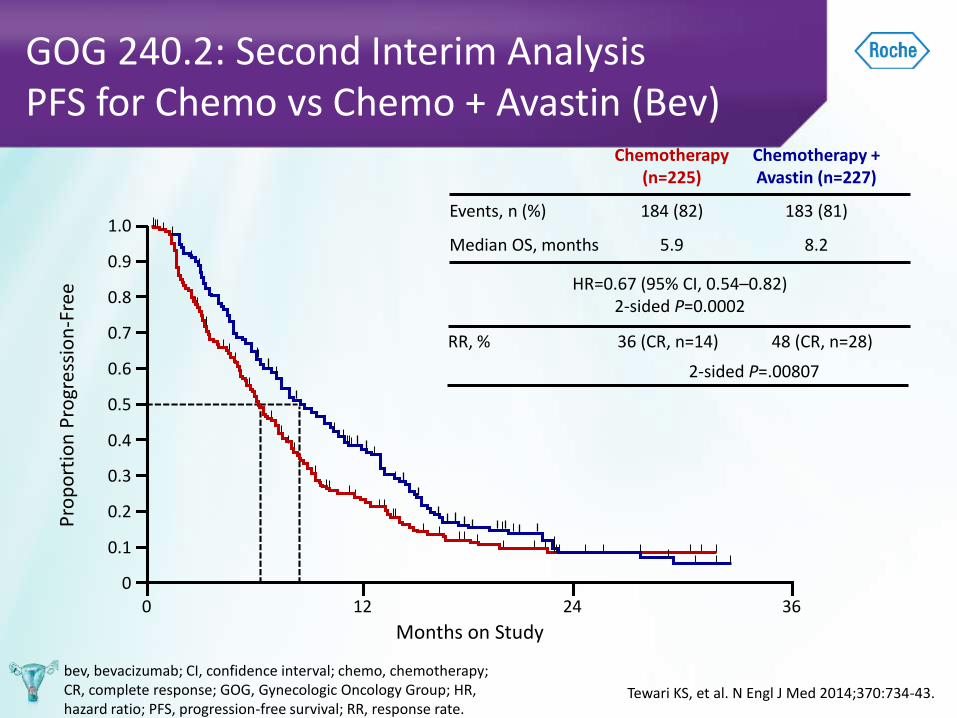
GOG 240.2: Second Interim AnalysisPFS for Chemo vs Chemo + Avastin (Bev)
bev, bevacizumab; CI, confidence interval; chemo, chemotherapy; CR, complete response; GOG, Gynecologic Oncology Group; HR, hazard ratio; PFS, progression-free survival; RR, response rate.
Pro
po
rtio
n P
rogr
essi
on
-Fre
e
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3612 24
Chemotherapy(n=225)
Events, n (%) 184 (82)
Median OS, months 5.9
RR, % 36 (CR, n=14) 48 (CR, n=28)
2-sided P=.00807
Months on Study
Chemotherapy + Avastin (n=227)
183 (81)
8.2
HR=0.67 (95% CI, 0.54–0.82)2-sided P=0.0002
Tewari KS, et al. N Engl J Med 2014;370:734-43.
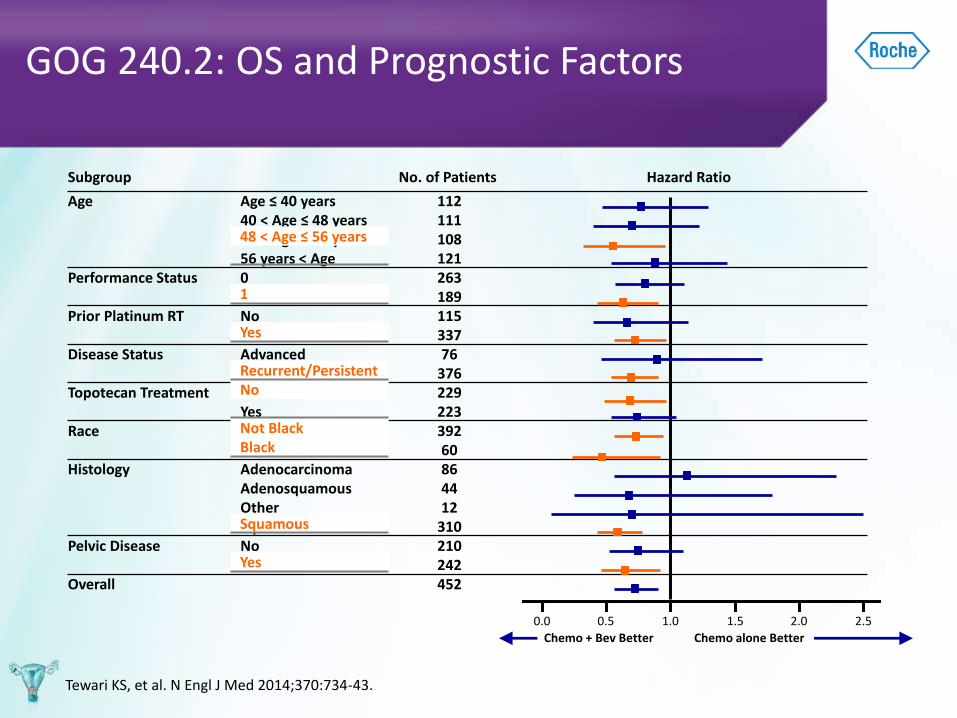
Subgroup No. of Patients Hazard Ratio
Age Age ≤ 40 years 11240 < Age ≤ 48 years 11148 < Age ≤ 56 years 10856 years < Age 121
Performance Status 0 2631 189
Prior Platinum RT No 115Yes 337
Disease Status Advanced 76Recurrent/Persistent 376
Topotecan Treatment No 229Yes 223
Race Not Black 392Black 60
Histology Adenocarcinoma 86Adenosquamous 44Other 12Squamous 310
Pelvic Disease No 210Yes 242
Overall 452
GOG 240.2: OS and Prognostic Factors
0.0 0.5 1.0 1.5 2.0 2.5
Chemo + Bev Better Chemo alone Better
48 < Age ≤ 56 years
1
Yes
Recurrent/PersistentNo
Not BlackBlack
Squamous
Yes
Tewari KS, et al. N Engl J Med 2014;370:734-43.
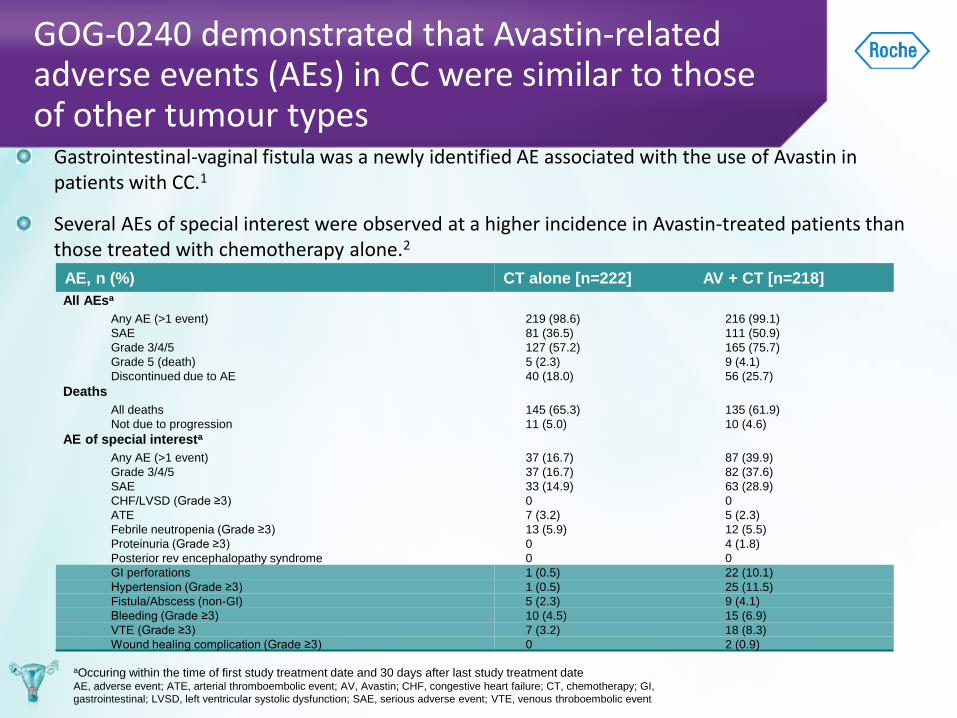
GOG-0240 demonstrated that Avastin-related adverse events (AEs) in CC were similar to those of other tumour types
aOccuring within the time of first study treatment date and 30 days after last study treatment dateAE, adverse event; ATE, arterial thromboembolic event; AV, Avastin; CHF, congestive heart failure; CT, chemotherapy; GI,
gastrointestinal; LVSD, left ventricular systolic dysfunction; SAE, serious adverse event; VTE, venous throboembolic event
AE, n (%) CT alone [n=222] AV + CT [n=218]
All AEsa
Any AE (>1 event) 219 (98.6) 216 (99.1)
SAE 81 (36.5) 111 (50.9)
Grade 3/4/5 127 (57.2) 165 (75.7)
Grade 5 (death) 5 (2.3) 9 (4.1)
Discontinued due to AE 40 (18.0) 56 (25.7)
Deaths
All deaths 145 (65.3) 135 (61.9)
Not due to progression 11 (5.0) 10 (4.6)
AE of special interesta
Any AE (>1 event) 37 (16.7) 87 (39.9)
Grade 3/4/5 37 (16.7) 82 (37.6)
SAE 33 (14.9) 63 (28.9)
CHF/LVSD (Grade ≥3) 0 0
ATE 7 (3.2) 5 (2.3)
Febrile neutropenia (Grade ≥3) 13 (5.9) 12 (5.5)
Proteinuria (Grade ≥3) 0 4 (1.8)
Posterior rev encephalopathy syndrome 0 0
GI perforations 1 (0.5) 22 (10.1)
Hypertension (Grade ≥3) 1 (0.5) 25 (11.5)
Fistula/Abscess (non-GI) 5 (2.3) 9 (4.1)
Bleeding (Grade ≥3) 10 (4.5) 15 (6.9)
VTE (Grade ≥3) 7 (3.2) 18 (8.3)
Wound healing complication (Grade ≥3) 0 2 (0.9)
Gastrointestinal-vaginal fistula was a newly identified AE associated with the use of Avastin in patients with CC.1
Several AEs of special interest were observed at a higher incidence in Avastin-treated patients than those treated with chemotherapy alone.2
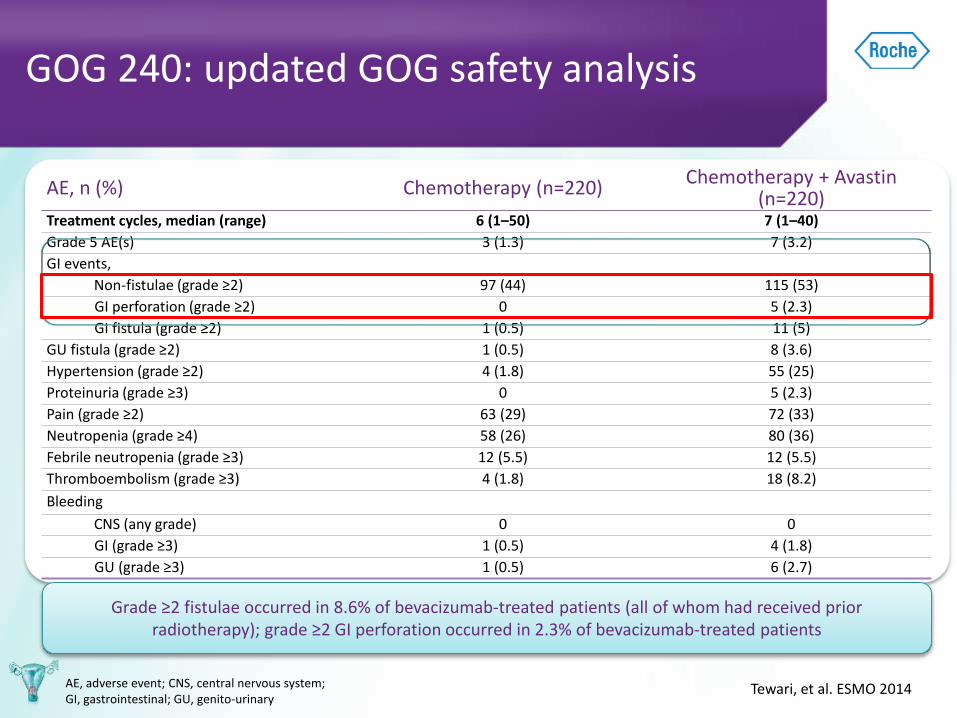
AE, n (%) Chemotherapy (n=220)Chemotherapy + Avastin
(n=220)Treatment cycles, median (range) 6 (1–50) 7 (1–40)
Grade 5 AE(s) 3 (1.3) 7 (3.2)
GI events,
Non-fistulae (grade ≥2) 97 (44) 115 (53)
GI perforation (grade ≥2) 0 5 (2.3)
GI fistula (grade ≥2) 1 (0.5) 11 (5)
GU fistula (grade ≥2) 1 (0.5) 8 (3.6)
Hypertension (grade ≥2) 4 (1.8) 55 (25)
Proteinuria (grade ≥3) 0 5 (2.3)
Pain (grade ≥2) 63 (29) 72 (33)
Neutropenia (grade ≥4) 58 (26) 80 (36)
Febrile neutropenia (grade ≥3) 12 (5.5) 12 (5.5)
Thromboembolism (grade ≥3) 4 (1.8) 18 (8.2)
Bleeding
CNS (any grade) 0 0
GI (grade ≥3) 1 (0.5) 4 (1.8)
GU (grade ≥3) 1 (0.5) 6 (2.7)
GOG 240: updated GOG safety analysis
Tewari, et al. ESMO 2014AE, adverse event; CNS, central nervous system; GI, gastrointestinal; GU, genito-urinary
Grade ≥2 fistulae occurred in 8.6% of bevacizumab-treated patients (all of whom had received prior radiotherapy); grade ≥2 GI perforation occurred in 2.3% of bevacizumab-treated patients
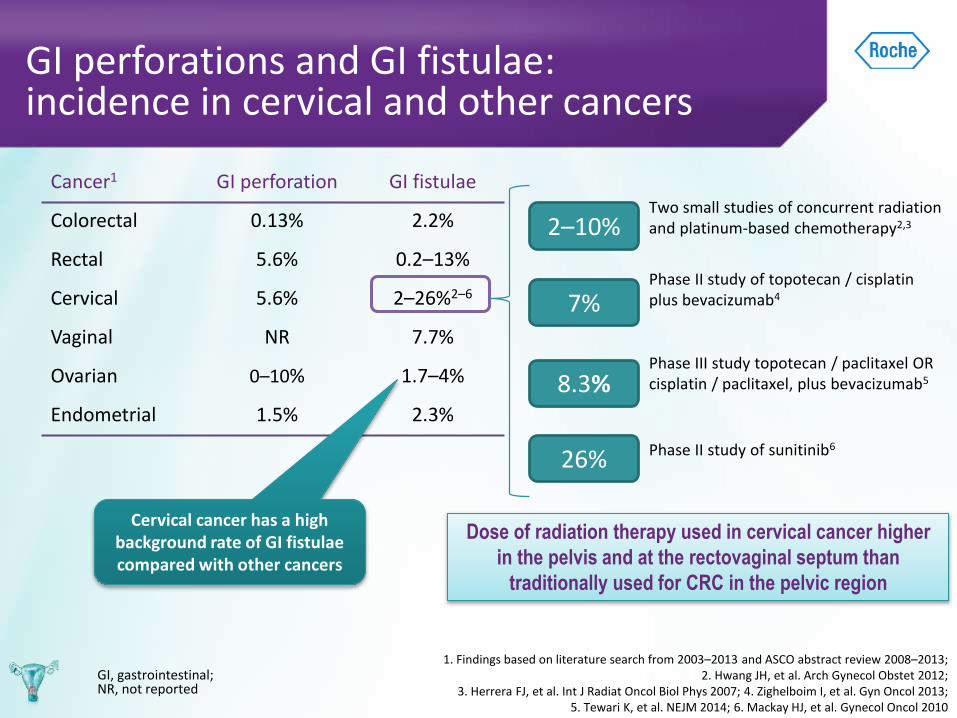
GI perforations and GI fistulae: incidence in cervical and other cancers
1. Findings based on literature search from 2003–2013 and ASCO abstract review 2008–2013;2. Hwang JH, et al. Arch Gynecol Obstet 2012;
3. Herrera FJ, et al. Int J Radiat Oncol Biol Phys 2007; 4. Zighelboim I, et al. Gyn Oncol 2013; 5. Tewari K, et al. NEJM 2014; 6. Mackay HJ, et al. Gynecol Oncol 2010
GI, gastrointestinal; NR, not reported
Cancer1 GI perforation GI fistulae
Colorectal 0.13% 2.2%
Rectal 5.6% 0.2–13%
Cervical 5.6% 2–26%2–6
Vaginal NR 7.7%
Ovarian 0–10% 1.7–4%
Endometrial 1.5% 2.3%
Cervical cancer has a high background rate of GI fistulae compared with other cancers
Dose of radiation therapy used in cervical cancer higher
in the pelvis and at the rectovaginal septum than
traditionally used for CRC in the pelvic region
7%Phase II study of topotecan / cisplatinplus bevacizumab4
2–10%Two small studies of concurrent radiation and platinum-based chemotherapy2,3
26% Phase II study of sunitinib6
8.3%Phase III study topotecan / paclitaxel OR cisplatin / paclitaxel, plus bevacizumab5
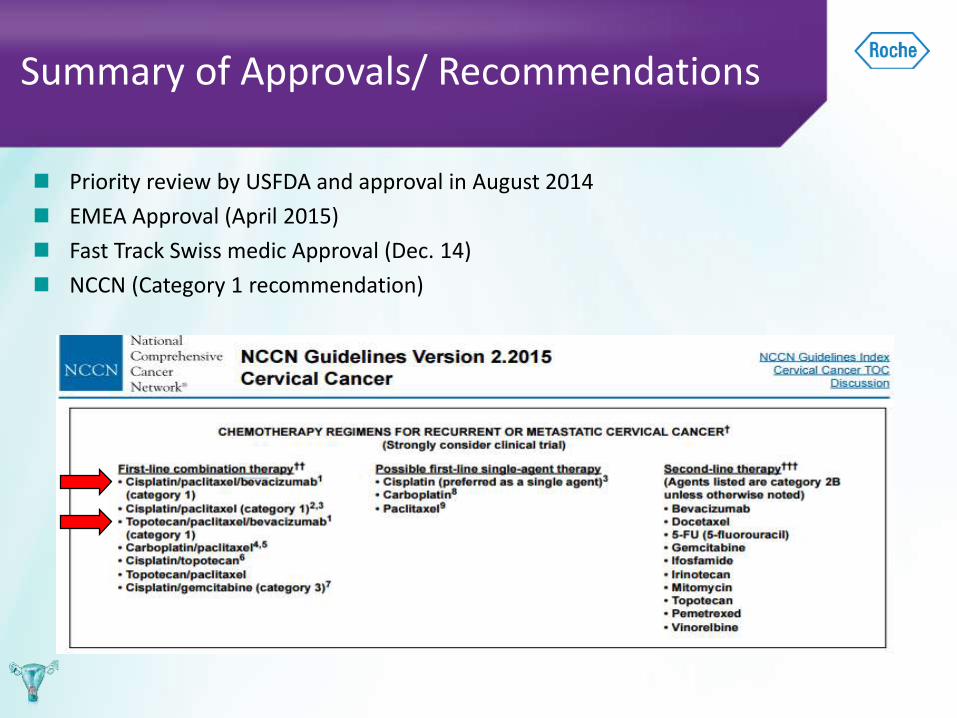
Summary of Approvals/ Recommendations
Priority review by USFDA and approval in August 2014
EMEA Approval (April 2015)
Fast Track Swiss medic Approval (Dec. 14)
NCCN (Category 1 recommendation)

THANK YOU!!
Related Documents











