Cerebral Vasospasm Following Subarachnoid Hemorrhage M. Akif Topcuoglu, MD Johnny C. Pryor, MD * Christopher S. Ogilvy, MD † J. Philip Kistler, MD Address Stroke Service, Department of Neurology and Interventional Neuroradiology and Neurosurgery, * Neurovascular Surgery, † Massachusetts General Hospital, 55 Fruit Street, VBK 802, Boston, MA 02114, USA. E-mail: [email protected] Current Treatment Options in Cardiovascular Medicine 2002, 4:373–384 Current Science Inc. ISSN 1092-8464 Copyright © 2002 by Current Science Inc. Introduction The presence of cerebral vasospasm (VSP) has been corre- lated with a 1.5- to threefold increase in mortality and morbidity in the first 2 weeks after subarachnoid hemor- rhage (SAH) from aneurysm rupture [1]. This exceeds that of surgical and endovascular morbidity as well as re- rupture, hydrocephalus, systemic or central nervous system infections, and metabolic complications. Despite many years of extensive research, the underlying molecular mechanism of VSP after SAH has not completely been elucidated. Two contemporary theories are still suggested. The first suggests that morphologic changes or dysfunction of the endothelial and vascular smooth muscle cells (VSMCs) are thought to be at the core. The second suggests that exposure to the blood breakdown products including potassium, oxyhemoglobin, and bilirubin in addition to a variety of paracrine mediators, eg, eicosanoids, free radicals, inflammatory and a vasoactive substance, eg, nitric oxide (NO) and endothelin (ET), initiate vasocon- striction. The spasm in turn stimulates endothelial and VSMC proliferation [2]. Studies performed at our institution in the early 1980s suggest a close relationship between the extent and location of subarachnoid blood noted on CT scan and the severity and location of VSP of the basal arteries Opinion statement Cerebral vasospasm and related ischemic stroke continue to be significant complicating factors in the course of many patients with subarachnoid hemorrhage from berry aneurysm rupture. The risk of this well-recognized but poorly understood complication can be estimated on the basis of patient medical history, neurologic examination, and head CT findings. Every patient with possible risk needs specialized neurologic intensive care unit care after aneurysm obliteration. Surgical and pharmacologic wash-out of subarachnoid blood around the basal arteries, proper management of intracranial pressure and fluid status, hyponatremia, hypomagnesemia, and fever, as well as use of calcium channel blockers, have been considered helpful in patient management prior to and with the symptomatic vasospasm development. Transcranial Doppler (TCD) ultrasound is important in detecting vasospasm before the patient suffers ischemic neurologic deficit or infarct. Elevated TCD velocities often initiate the use of triple-H (HHH: hypertension, hemo- dilution, and hypervolemia) therapy and subsequently guide it. Up to the end of the first 3 weeks after subarachnoid hemorrhage and aneurysm obliteration, development of any focal neurologic deficit or mental deterioration, unless convincingly proven otherwise, is assumed to be from cerebral vasospasm. When a hemodynamically significant vasospasm in the arterial segments of clinical concern is suggested, emergency cerebral angiography with balloon dilatation angioplasty or intra-arterial infusion of vasodilating agents may be helpful in relieving ischemic symptoms.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Cerebral Vasospasm Following Subarachnoid HemorrhageM. Akif Topcuoglu, MDJohnny C. Pryor, MD*
Christopher S. Ogilvy, MD†
J. Philip Kistler, MD
AddressStroke Service, Department of Neurology and Interventional Neuroradiology and Neurosurgery,* Neurovascular Surgery,† Massachusetts General Hospital, 55 Fruit Street, VBK 802, Boston, MA 02114, USA.E-mail: [email protected] Treatment Options in Cardiovascular Medicine 2002, 4:373–384Current Science Inc. ISSN 1092-8464Copyright © 2002 by Current Science Inc.
IntroductionThe presence of cerebral vasospasm (VSP) has been corre-lated with a 1.5- to threefold increase in mortality andmorbidity in the first 2 weeks after subarachnoid hemor-rhage (SAH) from aneurysm rupture [1]. This exceeds thatof surgical and endovascular morbidity as well as re-rupture, hydrocephalus, systemic or central nervous systeminfections, and metabolic complications. Despite manyyears of extensive research, the underlying molecularmechanism of VSP after SAH has not completely beenelucidated. Two contemporary theories are still suggested.The first suggests that morphologic changes or dysfunctionof the endothelial and vascular smooth muscle cells
(VSMCs) are thought to be at the core. The second suggeststhat exposure to the blood breakdown products includingpotassium, oxyhemoglobin, and bilirubin in addition to avariety of paracrine mediators, eg, eicosanoids, freeradicals, inflammatory and a vasoactive substance, eg,nitric oxide (NO) and endothelin (ET), initiate vasocon-striction. The spasm in turn stimulates endothelial andVSMC proliferation [2].
Studies performed at our institution in the early1980s suggest a close relationship between the extentand location of subarachnoid blood noted on CT scanand the severity and location of VSP of the basal arteries
Opinion statementCerebral vasospasm and related ischemic stroke continue to be significant complicating factors in the course of many patients with subarachnoid hemorrhage from berry aneurysm rupture. The risk of this well-recognized but poorly understood complication can be estimated on the basis of patient medical history, neurologic examination, and head CT findings. Every patient with possible risk needs specialized neurologic intensive care unit care after aneurysm obliteration. Surgical and pharmacologic wash-out of subarachnoid blood around the basal arteries, proper management of intracranial pressure and fluid status, hyponatremia, hypomagnesemia, and fever, as well as use of calcium channel blockers, have been considered helpful in patient management prior to and with the symptomatic vasospasm development. Transcranial Doppler (TCD) ultrasound is important in detecting vasospasm before the patient suffers ischemic neurologic deficit or infarct. Elevated TCD velocities often initiate the use of triple-H (HHH: hypertension, hemo-dilution, and hypervolemia) therapy and subsequently guide it. Up to the end of the first 3 weeks after subarachnoid hemorrhage and aneurysm obliteration, development of any focal neurologic deficit or mental deterioration, unless convincingly proven otherwise, is assumed to be from cerebral vasospasm. When a hemodynamically significant vasospasm in the arterial segments of clinical concern is suggested, emergency cerebral angiography with balloon dilatation angioplasty or intra-arterial infusion of vasodilating agents may be helpful in relieving ischemic symptoms.

374 Cerebrovascular Disease and Stroke
[3,4]. Moreover, the method of quantification of localamounts of subarachnoid clot developed in these stud-ies (known as Fisher’s scale) is reliable enough to suggesta risk of delayed symptomatic VSP on a single patient’sbasis. The patients with “thick” clots in the basilarcisterns (Fisher’s group 3) are at high risk of developingsecondary ischemia with symptoms, whereas thepatients with no blood (group 1), or diffuse and thin-layered blood (group 2), or blood outside the subarach-noid space (group 4) are at low risk. It seems likely thatnot only the severity and distribution of angiographiclarge artery VSP, but also the adequacy of collateralsupply contributes to whether and where secondaryischemia and infarction will develop. Parenchymalvessels distal to the basal arteries with angiographic VSPafter SAH, as opposed to those in carotid artery occlu-sion, do not show normal autoregulatory vasodilatationand cerebral blood volume increase [5•]. This may limitthe compensatory effect of the collateral flow.
Some degree of VSP occurs in 70% of all patientswith aneurysmal SAH, but leads to neurologic symp-toms associated with brain ischemia in 35% [6]. VSPafter SAH usually occurs between day 4 and 12 afteronset, with the peak around the end of the first week,but very early (within 3 days) and late manifestations(≤ 3 weeks) may be observed. The clinical manifesta-tions of VSP-related ischemia or infarctions developgradually over several hours, ie, a subacute syndrome.Abrupt onset is rare; other etiologies, especially re-bleeding or embolic stroke, should also be consideredwhen sudden neurologic deterioration occurs. Fluctuat-ing course, in particular worsening with hypotension, ishighly suggestive of VSP.
When VSP is severe enough to lead to ischemia, thepatients may develop a decrease in level of consciousness,abulia, or agitated delirium, or focal neurologic manifesta-tions referable to the territory of the basal or corticalsurface arteries, in which severe VSP reduces the distal flowin the absence of adequate collateral supply [7]. Because ofsubacute development of VSP and the involvement ofmore than one artery, multi-territorial infarcts or ischemiaresulting in complex neurologic syndromes can occur.Many of these syndromes await adequate clinical andpathologic description. Nonetheless, some clinicalsyndromes are often seen and can readily suggest the arteryinvolved [7]. A constellation of abulia, mutism, hypopho-nia, grasping, lip pursuing, eyelid apraxia, urinary inconti-nence, and uni/bilateral leg weakness is typical for anteriorcerebral artery VSP. Hemiparesis, brachiofacial paresis,monoparesis, facial weakness, aphasia or hemineglect,mostly in combination, occurs in middle cerebral arteryspasm. Hemianopia, and sometimes with abulia, developsin the posterior cerebral artery VSP. Vertebrobasilar spasmsgenerally result in encephalopathy, rarely with focal brainstem dysfunction. Persistence or reappearance of previouslysubsided headache is a frequent complaint in low-grade
SAH patients developing VSP. Changes in characteristicsand severity of headache may also be important.Hyponatremia, hypertension, and fever of unknown origincan precede or accompany SAH-related VSP.
In patients with suspicion of VSP after SAH, a varietyof tests are available to document it and to exclude theother possible causes for deterioration (Table 1). Thedevelopment of mass effect and edema surroundingintra-parenchymal hemorrhage, hydrocephalus, or re-bleeding can be easily ruled out by brain CT. Further-more, it shows signs suggestive of ischemia in up to twothirds of deteriorating patients with VSP. As expected,brain magnetic resonance imaging (MRI), in particulardiffusion-weighted imaging, is more sensitive in thedetection of ischemia and infarction in the early period.However, the long acquisition time and in-hospital trans-fer logistics usually preclude its use in these unstable andrestless patients. The obscuring susceptibility artifactsresulting from clip or coil also interferes. But MRI can beextremely helpful in identifying brain-stem abnormali-ties in patients with otherwise unexplainable symptoms.It is clearly the best way to demonstrate it.
Transcranial Doppler (TCD) ultrasonography is non-invasive, inexpensive, and easy to perform at bedside toevaluate blood flow velocities in the basal cerebral arter-ies. Hemodynamic changes representing the developmentof VSP can be reliably detected in almost every case byserial TCD measurements in the course of SAH. TCD hasdirect influence on the management of patients withSAH-related VSP by assessing the success or failure of pro-phylactic and therapeutic interventions. Conventionalangiography remains the gold standard for the diagnosisof VSP. Its invasive nature associated with significant riskof complications must be considered before performing itin these critically ill patients. It is generally reserved forconfirming the diagnosis at the time of consideringneurointerventional methods to relieve symptomatic VSP.CT or magnetic resonance angiography and perfusionscans, single photon emission CT, and xenon-enhancedCT can also demonstrate basal arteries in spasm andassociated areas of decreased perfusion. Experience withtranscranial infrared cerebral oximeter, jugular oxygensaturation monitoring, and direct parenchymal pH,temperature, oxygen and CO2 tension detection bymicrodialysis catheters is also limited. ECG and cardiacenzyme studies (to rule our myocardial infarction), chestradiograph (to evaluate pneumonia, acute pulmonaryedema, atelectasis), blood or urine tests (to excludeelectrolyte imbalances, hypo/hyperglycemia, hepatic andrenal dysfunction, toxicity and sometimes hypo-thyroidism or Addison crisis), cultures of blood, urine,sputum and venous lines (to exclude infections),electroencephalogram (to rule out seizure), and cere-brospinal fluid examination (in patients with ventriculardrain to exclude meningitis and ventriculitis) are allacceptable when indicated.
Cerebral Vasospasm Following Subarachnoid Hemorrhage Topcuoglu et al. 375
Treatment
• All patients with suspected VSP after SAH are best managed in an intensive care surrounding. A central venous line and arterial catheter are often placed. Serial neurologic examination by nurses and physicians to monitor clinical change generally dictates the level of medical management. That together with serial TCD assessment of VSP suggests when to consider neurointerventional therapy with balloon dilatation or vasoactive agents. Hourly or continuous monitoring of blood pressure, heart rate, and temperature are essential as are assessment of the Glasgow coma scale, pupillary responses, strength in all extremities, speech, and orientation. In high-risk or deteriorated patients, more frequent clinical assessments are necessary, as in every 15 minutes. In addition, daily electrolyte and hematologic indices, including arterial blood gases, intracranial pressure (ICP), and cerebrospinal fluid drainage, bladder output, and given fluids are monitored.
• Fluid management in SAH is critical to prevent plasma volume depletion, which may contribute to the development of cerebral VSP-related ischemia. Almost one third of patients decrease their plasma volume more than 10% because of a negative sodium balance with loss of water and sodium (cerebral salt wasting syndrome). Under careful monitoring for the signs of cardiac failure, 3 ± 0.5 L/d normal saline is advised. This can be powered by adjusting antihypertensive drugs and discontinuing diuretics. Intravenous saline is given in relation to other required parenteral and enteric fluids. Generally, half of the daily fluid requirement is given via the enteric route. Direct monitoring of central venous pressure (CVP) via the subclavian or jugular vein catheter is advised, at least in patients with hyponatremia or negative fluid balance. CVP between 8 to 10 mm Hg is ideal. Pulmonary capillary wedge pressure (PCWP)
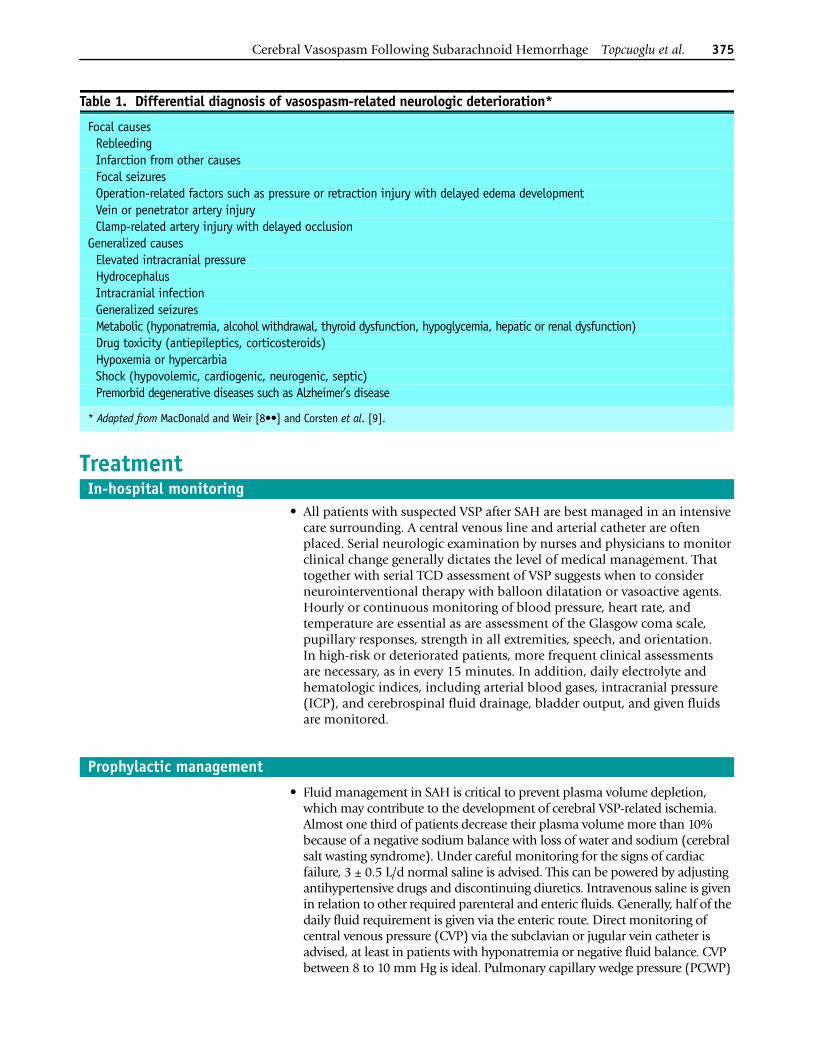
Table 1. Differential diagnosis of vasospasm-related neurologic deterioration*
Focal causesRebleedingInfarction from other causesFocal seizuresOperation-related factors such as pressure or retraction injury with delayed edema developmentVein or penetrator artery injuryClamp-related artery injury with delayed occlusion
Generalized causesElevated intracranial pressureHydrocephalusIntracranial infectionGeneralized seizuresMetabolic (hyponatremia, alcohol withdrawal, thyroid dysfunction, hypoglycemia, hepatic or renal dysfunction)Drug toxicity (antiepileptics, corticosteroids)Hypoxemia or hypercarbiaShock (hypovolemic, cardiogenic, neurogenic, septic)Premorbid degenerative diseases such as Alzheimer’s disease
* Adapted from MacDonald and Weir [8••] and Corsten et al. [9].
In-hospital monitoring
Prophylactic management
376 Cerebrovascular Disease and Stroke
monitoring via pulmonary arterial balloon catheters of the Swan-Ganz type may be needed with cardiopulmonary instability. A PCWP between 7 to 16 mm Hg is ideal. Secondary causes of volume loss, such as fever, should be aggressively managed. Hypervolemic fluid management and true triple-H (HHH: hypertension, hemodilution, and hypervolemia) therapy have not been shown to exert an additional benefit over normovolemic fluid manage-ment in the prophylactic management of VSP (Table 2) [10,11]. Therefore, it is reserved for patients who develop symptomatic VSP, or in asymptomatic patients with TCD changes compatible with VSP.
• Calcium antagonists are usually recommended in prophylactic management (Table 2). The mechanism of action is the inhibition of the VSMC contraction within the small collateral vessels not within the basal conducting arteries. Secondarily, perhaps more importantly, the blocking of calcium influx after the development of cerebral ischemia is thought to be neuroprotective. The evidence to date indicates that oral nimodipine is effective in improving outcomes (but not necessarily mortality) due to VSP [12].
• Aside from the possible effect on prevention or improvement of VSP, magnesium has well-defined neuroprotective properties on the ischemic tissue. Preliminary evidence also suggests that intravenous magnesium sulfate administration with a target serum level of twice the baseline or 2.0 to 2.5 mmol/L may be effective in preventing VSP [13]. A 2- to 4-g (1 mmol = 24 mg) magnesium sulfate daily infusion for the first 3 to 7 days is advised to maintain normomagnesemia. Frequent tendon reflex examination (hyporeflexia suggests hypermagnesemia) and daily serum concentration measurement should be performed.
• The experiences with oral fludrocortisone acetate, tirilazad mesylate, cyclosporine A, and antiplatelet agents have been insufficient to recommend them for routine prophylactic use.
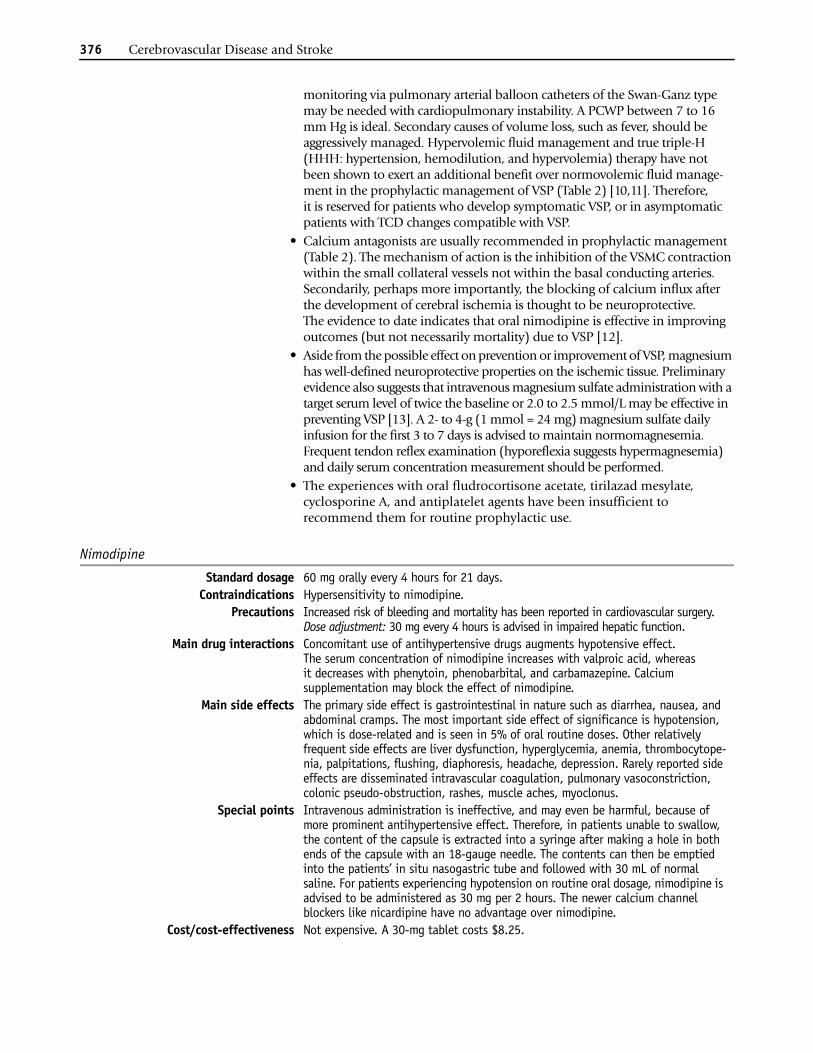
Nimodipine
Standard dosage 60 mg orally every 4 hours for 21 days.Contraindications Hypersensitivity to nimodipine.
Precautions Increased risk of bleeding and mortality has been reported in cardiovascular surgery. Dose adjustment: 30 mg every 4 hours is advised in impaired hepatic function.
Main drug interactions Concomitant use of antihypertensive drugs augments hypotensive effect. The serum concentration of nimodipine increases with valproic acid, whereas it decreases with phenytoin, phenobarbital, and carbamazepine. Calcium supplementation may block the effect of nimodipine.
Main side effects The primary side effect is gastrointestinal in nature such as diarrhea, nausea, and abdominal cramps. The most important side effect of significance is hypotension, which is dose-related and is seen in 5% of oral routine doses. Other relatively frequent side effects are liver dysfunction, hyperglycemia, anemia, thrombocytope-nia, palpitations, flushing, diaphoresis, headache, depression. Rarely reported side effects are disseminated intravascular coagulation, pulmonary vasoconstriction, colonic pseudo-obstruction, rashes, muscle aches, myoclonus.
Special points Intravenous administration is ineffective, and may even be harmful, because of more prominent antihypertensive effect. Therefore, in patients unable to swallow, the content of the capsule is extracted into a syringe after making a hole in both ends of the capsule with an 18-gauge needle. The contents can then be emptied into the patients’ in situ nasogastric tube and followed with 30 mL of normal saline. For patients experiencing hypotension on routine oral dosage, nimodipine is advised to be administered as 30 mg per 2 hours. The newer calcium channel blockers like nicardipine have no advantage over nimodipine.
Cost/cost-effectiveness Not expensive. A 30-mg tablet costs $8.25.
Cerebral Vasospasm Following Subarachnoid Hemorrhage Topcuoglu et al. 377
• With the new-onset of a neurologic deficit, prompt detection of VSP and evaluation for other causes are essential. Hydrocephalus and recurrent hemorrhage are excluded by emergent head CT. Prompt treatment of infection, metabolic and electrolyte disturbances, and seizure is obvious. Triple-H therapy is applied to the highest tolerable level, in order to reverse or at least reduce any ischemic deficit. ICP should be normalized. Supple-mentary oxygen and effective fever treatment are considered helpful. At this point, TCD guides the management. If TCD shows changes consistent with VSP and maximal medical treatment is not associated with clinical and
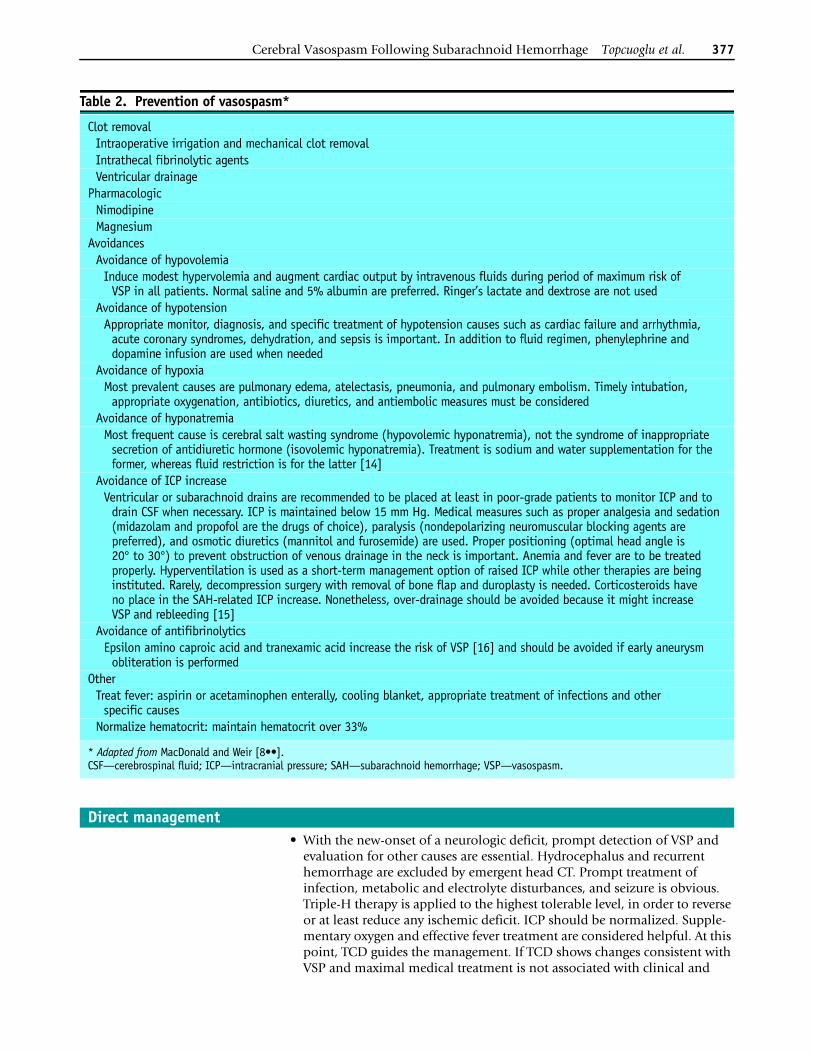
Table 2. Prevention of vasospasm*
Clot removalIntraoperative irrigation and mechanical clot removalIntrathecal fibrinolytic agentsVentricular drainage
PharmacologicNimodipineMagnesium
AvoidancesAvoidance of hypovolemia
Induce modest hypervolemia and augment cardiac output by intravenous fluids during period of maximum risk of VSP in all patients. Normal saline and 5% albumin are preferred. Ringer’s lactate and dextrose are not used
Avoidance of hypotensionAppropriate monitor, diagnosis, and specific treatment of hypotension causes such as cardiac failure and arrhythmia,
acute coronary syndromes, dehydration, and sepsis is important. In addition to fluid regimen, phenylephrine and dopamine infusion are used when needed
Avoidance of hypoxiaMost prevalent causes are pulmonary edema, atelectasis, pneumonia, and pulmonary embolism. Timely intubation,
appropriate oxygenation, antibiotics, diuretics, and antiembolic measures must be consideredAvoidance of hyponatremia
Most frequent cause is cerebral salt wasting syndrome (hypovolemic hyponatremia), not the syndrome of inappropriate secretion of antidiuretic hormone (isovolemic hyponatremia). Treatment is sodium and water supplementation for the former, whereas fluid restriction is for the latter [14]
Avoidance of ICP increaseVentricular or subarachnoid drains are recommended to be placed at least in poor-grade patients to monitor ICP and to
drain CSF when necessary. ICP is maintained below 15 mm Hg. Medical measures such as proper analgesia and sedation (midazolam and propofol are the drugs of choice), paralysis (nondepolarizing neuromuscular blocking agents are preferred), and osmotic diuretics (mannitol and furosemide) are used. Proper positioning (optimal head angle is 20° to 30°) to prevent obstruction of venous drainage in the neck is important. Anemia and fever are to be treated properly. Hyperventilation is used as a short-term management option of raised ICP while other therapies are being instituted. Rarely, decompression surgery with removal of bone flap and duroplasty is needed. Corticosteroids have no place in the SAH-related ICP increase. Nonetheless, over-drainage should be avoided because it might increase VSP and rebleeding [15]
Avoidance of antifibrinolyticsEpsilon amino caproic acid and tranexamic acid increase the risk of VSP [16] and should be avoided if early aneurysm
obliteration is performedOther
Treat fever: aspirin or acetaminophen enterally, cooling blanket, appropriate treatment of infections and other specific causes
Normalize hematocrit: maintain hematocrit over 33%
* Adapted from MacDonald and Weir [8••].CSF—cerebrospinal fluid; ICP—intracranial pressure; SAH—subarachnoid hemorrhage; VSP—vasospasm.
Direct management
378 Cerebrovascular Disease and Stroke
sonographic improvement, the patient should be considered for the cere-bral angiography with possible transluminal balloon or chemical angio-plasty. If TCD does not show changes consistent with VSP, distal arterial spasm becomes a likely diagnosis. In this situation, medical management or chemical angioplasty are the therapeutic options.
• Triple-H therapy is the mainstay of the medical treatment of VSP. PCWP and CVP monitoring are very helpful in guiding this therapy. Volume expansion (hypervolemia) is given initially. If there is not enough improvement after desired PCWP is achieved, vasopressor drips (hypertension) are initiated. Vasopressors alone may not be successful in improving cerebral blood flow in dehydrated patients. In addition, systemic vasoconstriction puts the end organs, ie, kidneys, at risk for ischemia if hydration is not enough. If a patient is found to be euvolemic after Swan-Ganz placement, volume expansion and vasopressors are usually instituted simultaneously [9].
Problems with triple-H therapy• The most common complications are fluid overload and congestive heart
failure. Other serious complications are rupture of unsecured aneurysm, intracerebral hemorrhage, pulmonary edema, respiratory distress syndrome, and myocardial infarction. Dilutional hyponatremia, coagulopathy, cardiac arrhythmias, severe peripheral vasoconstriction, renal medullary wash-out, aggravation of cerebral edema, and hemorrhagic transformation of cerebral infarction can be observed. Various complica-tions related to central catheterization (in particular pneumothorax) are not rare. Iatrogenic hypertensive encephalopathy has been reported.
• The inability to produce and to maintain hypertension in the advocated range is frequent even with a normal functioning cardiovascular system. Tachyphylaxis to the sympathomimetic agents is a common problem. Invasiveness and inability to show volume status via the commonly used monitoring methods (CVP and PCWP) are usually confounding.
• Triple-H treatment is associated with significantly higher cost [11].• Triple-H therapy is not evidence-based.• At present there are no randomized controlled clinical trials with adequate
methodology that have assessed the effect of triple-H therapy (or any of its components) on clinical outcome [17].
Hypervolemia• In spite of the absence of a general consensus, most guidelines for volume
loading include 5% albumin and crystalloid solutions. Packed erythrocytes and fresh frozen plasma are sometimes used. Dextran 40 and hydroxyethyl starch (Hetastarch) use has recently been abandoned because of concerns about potential hemorrhagic complications [18]. However, albumin has also been shown to have anticoagulant properties [19].
• Albumin can distribute easily across the capillary membrane and can cause tissue edema. On the other hand, it lowers the renal glomerular filtration rate and facilitates sodium retention. When albumin is added to the regimen, the amount of crystalloids can be decreased [20]. This fluid-saving effect helps balance its edema-promoting effect.
Triple-H therapy
Cerebral Vasospasm Following Subarachnoid Hemorrhage Topcuoglu et al. 379
• The volume expansion is titrated by CVP and PCWP monitoring. Serum colloid oncotic pressure (COP) is a practical way to estimate the maximum tolerable PCWP upper limit. COP in mm Hg can be calculated by serum total protein (TP) by the formula of COP = 2.1 TP + 0.16 TP2 + 0.009 TP3. The suggested PCWP is less than this value [9].
Albumin
Standard dosage 5% albumin 250 to 500 mL three to four times per day is given if the CVP is less than 10 mm Hg.
Contraindications Hypersensitivity to albumin.Main drug interactions None.
Main side effects Congestive heart failure, fever, rash.Special points Albumin should be held if the CVP is more than 15 mm Hg. Albumin is weaned by
250 to 500 mL/d following the resolution of ultrasonographic VSP.Cost/cost-effectiveness Very expensive. A 250-mL intravenous solution of 5% albumin costs $75.00. The
addition of human albumin to the regimen increases the cost over 30 times [21].
Hypertension• Hypertensive therapy is titrated according to the baseline systolic and mean
arterial blood pressure and the baseline cardiac output. The systolic blood pressure may be raised to the level the deficit recedes but not higher than 240 mm Hg. In the presence of unsecured aneurysm, the highest limit we tolerate is 180 mm Hg. Clinical response is usually rapid, occurring in minutes. If improvement is observed, pressor therapy is continued. If there is no neurologic improvement after blood pressure elevation and optimiza-tion of cardiac output, pressor infusion is stopped [9]. Dopamine and phenylephrine are the most commonly used vasopressor agents [22].
Dopamine
Standard dosage The recommended dilution is 5 mL of 200 mg/mL dopamine solution diluted with 250 or 500 mL of sodium chloride or dextrose solutions (final concentration is 800 µg/mL and 400 µg/mL, respectively). The diluted dopamine is initially admin-istered at 2 to 5 µg/kg/min and then increased by 5 to 10 µg/kg/min until appropriate response or 20 to 50 µg/kg/min is reached.
Contraindications Hypersensitivity to dopamine products, ventricular tachyarrhythmias, pheochromocytoma.
Precautions Angina pectoris, allergy to sulfide, patients with atherosclerotic or spastic peripheral vascular disease, Parkinson disease.
Main drug interactions Concurrent use of intravenous phenytoin can decrease blood pressure.Main side effects Cardiovascular: Tachycardia, palpitations, arrhythmia, ventricular premature beats,
extrasystoles, anginal pain. Gastrointestinal: Nausea and vomiting.Genitourinary: Nephrotoxicity, polyuria, dysuria, diabetes insipidus.Skin: Gangrene or necrosis at the injection site and extravasation.
Special points Onset of activity is 5 minutes and the duration is 10 minutes. When discontinuing the infusion, it may be necessary to gradually decrease the dopamine dose because abrupt cessation may cause severe hypotension. Proper monitoring of renal function particularly during high doses (dopamine 20 to 40 µg/kg/min) is required because decreased renal blood flow can occur at these dose levels. Every patient is to be monitored for decreased perfusion in the extremities, which may occur with either high or low doses (coldness, cyanosis, pulses).
Cost/cost-effectiveness Not expensive. A 400-mg/250-cm3 intravenous dopamine solution costs $21.25.
380 Cerebrovascular Disease and Stroke
Phenylephrine
Standard dosage The recommended dilution is 10 mg of phenylephrine, which is diluted with 250 mL of sodium chloride (final concentration is 40 µg/mL). Infusion should begin as 0.1 to 0.5 µg/kg/min (usually 40 µg/min) and then titrate up to 300 µg/min to achieve blood pressure goal.
Contraindications Hypersensitivity to adrenergic agents, narrow angle glaucoma, ventricular tachyarrhythmia.
Main drug interactions Tricyclic antidepressants increase the pressor response.Main side effects Reflex bradycardia, peripheral vasoconstriction, headache, reduced urine output,
respiratory distress.Special points Onset of activity is several minutes and the duration is 15 minutes.
Cost/cost-effectiveness Not expensive. A 5-g vial costs $8.75.
Hemodilution• Hemodilution is obtained by infusion of a plasma volume expander that
decreases hematocrit and whole blood viscosity and increases cerebral blood flow. The relationship between hematocrit and net oxygen carrying capacity is U-shaped. If hematocrit is reduced below a critical value, oxygen delivery starts to diminish. Data from normal tissue studies suggest that a hematocrit range of 30% to 33% is advisable.
• A persisting or deteriorating neurologic deficit referable to VSP and refractory to aggressively employed medical treatment is the indication for transluminal balloon angioplasty (TBA). All accessible arterial segments with evidence of more than 50% luminal narrowing are suggested for this treatment [23•].
• The mechanism of action of TBA in the treatment of cerebral VSP is not totally understood. After TBA, morphologic changes of partial tearing of internal elastic lamina, flattening of VSMCs, and denudation of endo-thelium as well as functional changes of impairment in vasodilatatory responses of VSMCs have been demonstrated. Experimental evidence indi-cates that each resolves within 3 weeks, at least in animal experiments [24].
• On average, if the infarction is not too large, 70% (31% to 86%) of patients show significant clinical improvement within hours [23•,25]. The anatomic response is sustained, but VSP can develop in previously undilated segments and vessels.
• The periprocedural mortality rate varies from 2% to 5%. Therefore, TBA is not recommended for asymptomatic patients [26].
Problems with transluminal balloon angioplasty• High technological and personnel demand: TBA is technically demanding, a
fact that limits its successful use to highly skilled and experienced endo-vascular specialists and to advanced centers.
• Limited to proximal and segmental VSP: TBA is only applicable to segmental VSP within the middle and anterior cerebral artery stems, the supraclinoid internal carotid arteries, and the vertebral and basilar arteries.
• Sedation: Required to keep patients absolutely motionless during the procedure, may mask clinical signs of improved ischemia.
Transluminal balloon angioplasty
Cerebral Vasospasm Following Subarachnoid Hemorrhage Topcuoglu et al. 381
Procedure of transluminal balloon angioplasty
Standard procedure Transluminal balloon angioplasty is performed in the angiography suite under intubation and appropriate sedation, often with a paralytic agent or general anesthe-sia. First, a guiding catheter with appropriate luminal size is placed into the supracli-noid internal carotid artery or vertebral artery. For the standard balloons, a 5F guiding catheter is suitable. At this point, the patient is anticoaguled with intravenous heparin targeting activated coagulation time as twice the baseline. Then, a flow-directed or over-the wire balloon is placed to the most proximal area of VSP carefully. A small guidewire is placed in the catheter lumen to stiffen the shaft for ease of positioning. Angioplasty is performed from proximal to distal as the vessels dilates. All balloon inflations are performed by hand injection of a 50% or less contrast/saline mixture. A gradual dilatation is performed till the pre-VSP size is achieved. Over-the-wire balloons can be better for the anterior cerebral arteries.
Precautions Unsecured aneurysms in the targeted territory. Infarct with CT evidences in the territory of the vessel to be dilated.
Complications Procedure related: Vascular rupture (approximately 5%), balloon detachment, unsecured aneurysm rupture, dissection of intracranial or cervical arteries, femoral hematoma, retroperitoneal hematoma, contrast-induced nephropathy.Other: Intracerebral hemorrhage, hyperperfusion injury.
Special points The timing of TBA has crucial importance on not only prognosis but also technical success. However, in most institutes, TBA has been reserved for the patients with failure of maximal medical therapy or complications that ensue. This widely accepted approach rarely avoids the need, and may lead to delay in definitive treatment. Because TBA is only effective if it is performed within 6 to 12 hours (and perhaps as short as 2 hours [27]), consideration of early TBA should be encouraged. Not only the vessels of clinical concern based on the patient’s symptoms, but also other spastic vessels are plastied during the procedure. The possibility of TBA-related perforation is higher in the posterior cerebral artery than the other vessels.
Cost/cost-effectiveness Although formal cost-effectiveness studies have not been done, TBA seems very expensive.
• Although still a matter of debate and treatment with intra-arterial papaver-ine (IAP) hydrochloride infusion has been abandoned in some institutes [9,28•], IAP and other vasodilating agents such as verapamil, nicardipine, and trinitroglycerine can be used in selected cases, especially those with symptomatic VSP in the inaccessible distal parts of the cerebral circulation.
• Although the exact mechanism is unknown, papaverine appears to inhibit cyclic AMP and cyclic GMP in VSMCs, resulting in direct vasodilatation.
• Nicardipine, with a similar mechanism of action, may be at least as effec-tive as IAP with a longer duration of action and less severe elevation in ICP. Trinitroglycerine is known to cause intracranial hypertension and should not be used in people with elevated ICP.
Problems with intra-arterial papaverine• The effect of IAP is transient [28•]. Angiographic recurrence of VSP can
occur within 24 hours or less, often requiring serial procedures.• The angiographic improvement after IAP application (67% to 98%) may
not be associated with clinical improvement (33% to 80%) [23•]. One study reported only a 26% significant clinical improvement despite a 78% angiographic success rate [29].
• In the arterial territory of severe VSP, IAP may further disturb perfusion deficit. First, because of poor blood flow in severely spastic arteries the effective local papaverine concentration may not be achieved. Papaverine
Intra-arterial papaverine
382 Cerebrovascular Disease and Stroke
paradoxically causes capillary constriction if its concentration is less than 5 × 10-5 mol/mL [1]. Second, more profound dilatation response of the ves-sels in moderate spasm results in a steal effect from less responsive severely spastic vessels. IAP, therefore, is not advised in cases with severe VSP.
• The IAP alone is less effective than the TBA [25,30], but both techniques can be used additively (with 67% to 98% anatomic success) because angioplasty is effective for proximal vessel VSP and papaverine for distal arterial VSP. Moreover, IAP prior to TBA may make VSP more responsive to the angioplasty [23•].
Procedure of intra-arterial papaverine
Standard procedure Direct infusion via microcatheter as close as possible to the affected spastic artery delivered 200 to 300 mg of papaverine in 100 mL of normal saline over 20 minutes (up to 60 minutes) [31].
Contraindications Hypersensitivity to papaverine, complete atrioventricular block.Precautions Glaucoma, liver disease, Parkinsonian patients on levodopa.
Complications Serious: Transient brain stem depression, tonic-clonic convulsions, paradoxical VSP or aggravation of previous VSP, cardiopulmonary arrest, ICP elevation.Other: Dose-related hypotension, mydriasis, unilateral blindness, headache, transient neurologic deficits such as drowsiness, vertigo, thrombocytopenia, lactic acidosis, abdominal discomfort, nausea, vomiting, skin rash with pruritus.Theoretic: Precipitation in microcrystal form and subsequent distal embolization.
Special points Although the patients with high baseline ICP are significantly more likely to experience further ICP elevations, the increases cannot always be predicted by rate of papaverine infusion, patients age, clinical state, and the subarachnoid blood detected on head CT. During the procedure, ICP should, therefore, be monitored in all patients to reduce or stop when significant increases are detected [32] and intraventricular drains should be placed if the ICP is above 12 cm H2O. Papaverine concentrations higher than 0.3% form precipitates when mixed with saline. Crystal in 50 to 100 µm size can cause distal embolism. Concentrations higher than 0.8% are direct vasculotoxic. Papaverine should not be mixed with some specific contrast agents, such as ioxaglate meglumine.
Cost/cost-effectiveness Unproven, but seems very expensive.
• Antioxidants and free radical scavengers (eg, superoxide dismutase, tropolone, nicaraven, ebselen), lipid peroxidation inhibitors (eg, tirilazad mesylate), and iron-chelating agents (eg, deferoxamine) have been studied in phase II and III studies. Overall, no apparent benefit was observed. Similar experience has been obtained with immunosuppressive agents (eg, cyclosporine A) and high-dose intravenous methylprednisolone, serine protease inhibitors (eg, nafamostat mesylate), and with thromboxane-A2 synthetase inhibitors (eg, nizofenone and cataclot).
• Inhibition of ET by actinomycin D (nonspecific), bosentan (ETA/ETB receptor antagonist), PD 155080 (ETA receptor antagonist), and CGS26303 (ET-converting enzyme inhibitor) has been found very effective in reducing experimental VSP. No human studies have been published to date.
• Augmentation of NO by intracisternal nitroprusside (NO donor), intra-carotid infusion of proli-NO, glucantime-NO, or L-arginine has shown some improvement in experimental VSP. Preliminary human experience with intraventricular and intrathecal sodium nitroprusside show some promise [33,34].
• Potassium channel openers such as cromakalim may have some potential in the VSP reversal [35].
Other treatment perspectives
Cerebral Vasospasm Following Subarachnoid Hemorrhage Topcuoglu et al. 383
• Intracisternal administration of prolonged-release preparations of papaver-ine and nicardipine has been tried but further studies are needed [36].
• Calcitonin gene-related peptide was found ineffective in a large random-ized clinical trial [37].
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Treggiari-Venzi MM, Suter PM, Romand JA: Review of medical prevention of vasospasm after aneurysmal subarachnoid hemorrhage: a problem of neuro-intensive care. Neurosurgery 2001, 48:259–262.
2. Dietrich HH, Dacey RG: Molecular keys to the problems of cerebral vasospasm. Neurosurgery 2000, 46:517–530.
3. Fisher CM, Kistler JP, Davis JM: Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computed tomographic scanning. Neurosurgery 1980, 6:1–9.
4. Kistler JP, Crowell RM, Davis KR, et al.: The relation of cerebral vasospasm to the extent and location of subarachnoid blood visualized by CT scan: a prospective study. Neurology 1983, 33:424–436.
5.• Yundt KD, Grubb Rl, Diringer MN, et al.: Auto-regulatory vasodilatation of parenchymal vessels is impaired during cerebral vasospasm. J Cereb Blood Flow Metab 1998, 18:419–424.
Demonstrated that parenchymal vessels distal to arteries with angiographic spasm after SAH do not show normal auto-regulatory vasodilatation unlike the similar conditions of tissue hypoxia, eg, patients with carotid occlusion, that produce cerebral blood volume increase.6. Biller J, Godersky JC, Adams HP Jr: Management of
aneurysmal subarachnoid hemorrhage. Stroke 1988, 19:1300–1305.
7. Fisher CM, Roberson GH, Ojemann RG: Cerebral vasospasm with ruptured saccular aneurysm: the clinical manifestations. Neurosurgery 1977, 3:245–248.
8.•• MacDonald RL, Weir B: Medical aspects of vasospasm. In Cerebral Vasospasm. Edited MacDonald RL, Weir B. San Diego, CA: Academic Press; 2001:353–428.
This very important and peerless work, the first VSP textbook, covers all details one needs to know about VSP.9. Corsten L, Raja A, Guppy K, et al.: Contemporary
management of subarachnoid hemorrhage and vasospasm: the UIC experience. Surg Neurol 2001, 56:140–150.
10. Lennihan L, Mayer SA, Fink ME, et al.: Effect of hyper-volemic therapy on cerebral blood flow after subarachnoid hemorrhage: a randomized controlled trial. Stroke 2000, 31:383–391.
11. Egge A, Waterloo K, Sjoholm H, et al.: Prophylactic hyperdynamic postoperative fluid therapy after aneurysmal subarachnoid hemorrhage: a clinical, prospective, randomized, controlled study. Neurosurgery 2001, 49:593–606.
12. Feigin VL, Rinkel GJE, Algra A, et al.: Calcium antago-nist for aneurysmal subarachnoid hemorrhage. Cochrane Database Syst Rev 2002, 2:CD000277.
13. Boet R, Mee E: Magnesium sulfate in the management of patients with Fisher grade 3 subarachnoid hemor-rhage: a pilot study. Neurosurgery 2000, 47:602–607.
14. Harrigan MR: Cerebral salt wasting syndrome: a review. Neurosurgery 1996, 38:152–160.
15. Kasuya H, Shimizu T, Kagawa M: The effect of continu-ous drainage of cerebrospinal fluid in patients with subarachnoid hemorrhage: a retrospective analysis of 108 patients. Neurosurgery 1991, 28:56–59.
16. Ross YB, Rinkel GJ, Vermeulen M, et al.: Antifibrinolytic therapy for aneurysmal subarachnoid hemorrhage. Cochrane Database Syst Rev 2002, 2:CD001245.
17. Feigin VL, Rinkel GJE, Algra A, et al.: Circulatory vol-ume expansion for aneurysmal subarachnoid hemor-rhage. Cochrane Database Syst Rev 2002, 2:CD000483.
18. Trumble ER, Muizelaar JP, Myseros JS, et al.: Coagulopathy with the use of hetastarch in the treatment of vasospasm. J Neurosurg 1995, 82:44–47.
19. Soni N: Wonderful albumin. BMJ 1995, 310:887–888.20. Mayer SA, Solomon RA, Fink ME, et al.: Effect of 5%
albumin solution on sodium balance and blood volume after subarachnoid hemorrhage. Neurosurgery 1998, 42:759–768.
21. Alderson P, Bunn F, Lebepvre C, et al.: Human albumin solution for resuscitation and volume expansion in critically ill patients. Cochrane Database Syst Rev 2002, 1:CD001208.
22. McDonald CT, Carter BS, Putman C, et al.: Subarach-noid hemorrhage. Curr Treatment Options Cardiovasc Med 2001, 3:429–439.
23.• Smith TP, Enterline D: Endovascular treatment of cerebral vasospasm. State of the art. J Vasc Interv Radiol 2000, 11:547–559.
A very well written detailed description of the contemporary interventional VSP treatment.24. Megyesi JF, Vollrath B, Cook DA, et al.: Long-term
effects of in vivo angioplasty in normal and vasospas-tic canine carotid arteries. Pharmacological and morphological analyses. J Neurosurg 1999, 91:100–108.
25. Polin RS, Coenen VA, Hansen CA, et al.: Efficacy of transluminal angioplasty for the management of symptomatic cerebral vasospasm following aneurysmal subarachnoid hemorrhage. J Neurosurg 2000, 92:284–290.
384 Cerebrovascular Disease and Stroke
26. Muizelaar JP, Zwienenberg M, Rudisill NA, et al.: The prophylactic use of transluminal balloon angio-plasty in patients with Fisher grade 3 subarachnoid hemorrhage: a pilot study. J Neurosurg 1999, 91:51–58.
27. Rosenwasser RH, Armonda RA, Thomas JE, et al.: Therapeutic modalities for the management of cerebral vasospasm: Timing of endovascular options. Neurosurgery 1999, 44:975–980.
28.• Vajkoczy P, Horn P, Bauhuf C, et al.: Effect of intra-arterial papaverine on regional cerebral blood flow in hemodynamically relevant cerebral vasospasm. Stroke 2001, 32:498–505.
Study using thermal diffusion probes in humans, which elegantly demonstrates that the beneficial effect of IAP on cerebral hypoperfusion vanishes within 3 hours after treatment.29. Firlik KS, Kaufmann Am, Firlik AD, et al.: Intra-arterial
papaverine for the treatment of cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Surg Neurol 1999, 51:66–74.
30. Elliot JP, Newell DW, Derek JL, et al.: Comparison of balloon angioplasty and papaverine infusion for the treatment of vasospasm following aneurysmal sub-arachnoid hemorrhage. J Neurosurg 1998, 88:277–284.
31. Mathis JM, Jensen ME, Dion JE: Technical consider-ations on intra-arterial papaverine hydrochloride for cerebral vasospasm. Neuroradiology 1997, 39:90–98.
32. Giardano MJ, Pryor JC, Moran CJ, et al.: Intra-arterial papaverine may significantly increase intracranial pressure [meeting abstract]. Presented at theCongress of Neurological Surgeons. Chicago, IL: 1994.
33. Thomas JE, Rosenwasser RH: Reversal of severe vasoconstriction in three patients after aneurysmal subarachnoid hemorrhage: initial observations regarding the use of intraventricular sodium nitro-prusside in humans. Neurosurgery 1999, 44:48–58.
34. Thomas JE, Rosenwasser RH, Armonda AR, et al.: Safety of intrathecal sodium prusside for the treat-ment and prevention of refractory cerebral vasospasm and ischemia in humans. Stroke 1999, 30:1409–1416.
35. Kwan AL, Lin CL, Yanamoto H, et al.: Systemic administration of the potassium channel activator cromakalim attenuates cerebral vasospasm after experimental subarachnoid hemorrhage. Neurosurgery 1998, 42:347–351.
36. Kasuya H, Onda H, Takeshita M, et al.: Efficacy and safety of nicardipin prolonged-release implants for preventing vasospasm in humans. Stroke 2002, 33:1011–1015.
37. Effect of calcitonin-gene-related peptide with delayed postoperative cerebral ischemia after aneurysmal subarachnoid hemorrhage [no authors listed]. Lancet 1992, 339:831–834.
Related Documents











