Cerebral Aneurysm & Subarachnoid Hemorrhage (SAH) ROZMEEN SHIVJI, ACNP-BC

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cerebral Aneurysm &
Subarachnoid Hemorrhage (SAH)
ROZMEEN SHIVJI, ACNP-BC

Objectives:
Define Brain Aneurysm
Recognize different types of aneurysm
List causes and S & S of aneurysm
Identify diagnosis of aneurysm
Discuss treatment of aneurysms
Discuss complications of aneurysm
Understand nursing care of a patient with aneurysm & SAH

What Is An Aneurysm?
A cerebral aneurysm is a
bulge or balloon like
dilatation/swelling of the wall of
a blood vessel in the brain.
Aneurysm develops because of a
weakness in the wall of the
blood vessel, usually at the
bifurcation point.
Also called as intracranial aneurysm
or brain aneurysm.


Demographics
Unruptured Aneurysms are found in 2-4% of the USA population
6 million Americans are affected with Unruptured Aneurysms
More likely to occur in adults of age 40-60 years
They are more common in women
There are as many as 27,000 aneurysms that could be diagnosed and treated per year in the U.S.
The annual rupture rate is approximately 1.5%
Rupture of an aneurysm results in approximately 50% mortality and 25% stroke incidence
Annual incidence of SAH is 15 cases/100,000 or about one hemorrhage every 18 minutes
Brisman, et al (2006), New England Journal of Medicine, 355, 928-939.
Hickey, J.V. (2014). The Clinical Practice of Neurological and Neurosurgical Nursing

Etiology
AV malformation
Connective Tissue Disorder
Family history of brain aneurysms
Smoking
Hypertension
Traumatic head injury
Alcohol use
Use of oral contraception
Post menopausal women
Infection: Bacterial and Fungal
Disorders: Ehler’s syndrome, polycystic kidney disease, Marfan syndrome
Suarez, et al. (2006), New England Journal of Medicine, 354, 387-396.
Familial Intracranial Aneurysm (FIAs)
FIAs : Two or more family members among 1st and 2nd degree relatives with aneurysmal SAH or incidental finding of aneurysm.
Incidence of FIAs among SAH patients is 6% - 20%. Prevalence of FIAs among SAH patients is 7% to 10%.
Patients with FIAs are more likely to have multiple aneurysm and they have higher tendency to rupture even with a small size.
FIA study completed in Nov 2011, 542 families and 2,874 subjects from 26 clinical centers suggests genetic disposition plays an important role in development of cerebral aneurysm.
Screening: Family members should be screened (MRI, MRA, CTA) in their 20s and every 5-10 years thereafter.
Hickey, J.V. (2014). The Clinical Practice of Neurological and Neurosurgical Nursing

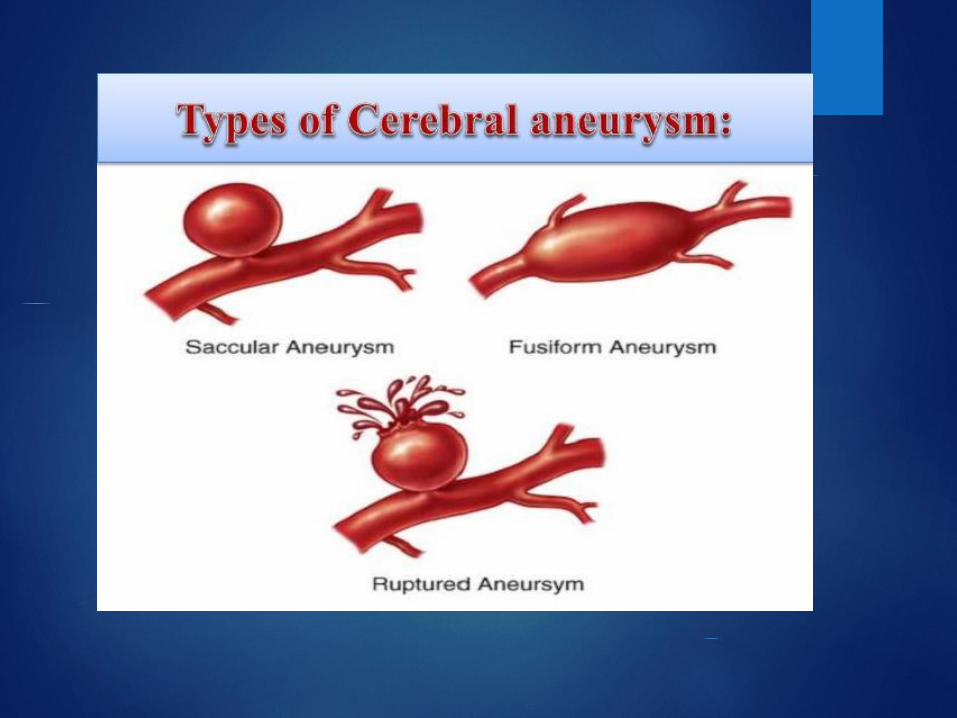
Classification:
Aneurysm are present in various size and shape.
Classification by size
Small: up to 10 mm
Medium: 10 to 15 mm
Large: 15 to 25 mm
Giant: 25 to 50 mm
Super-Giant: >50 mm
Giant Aneurysm
Hickey, J.V. (2014). The Clinical Practice of Neurological and Neurosurgical Nursing

Classification:Classification by shape
Berry aneurysm: most common, berry or saccular shape with stem
or neck. Develop over time.
Fusiform aneurysm: an outpouching of an arterial wall, without
stem. Common in hypertension, atherosclerosis and advancing age.
Traumatic aneurysm: Infrequent; resulting from trauma
Mycotic aneurysm: rare; resulting from septic emboli due to
infection, such as bacterial endocarditis
Hickey, J.V. (2014). The Clinical Practice of Neurological and Neurosurgical Nursing

Location
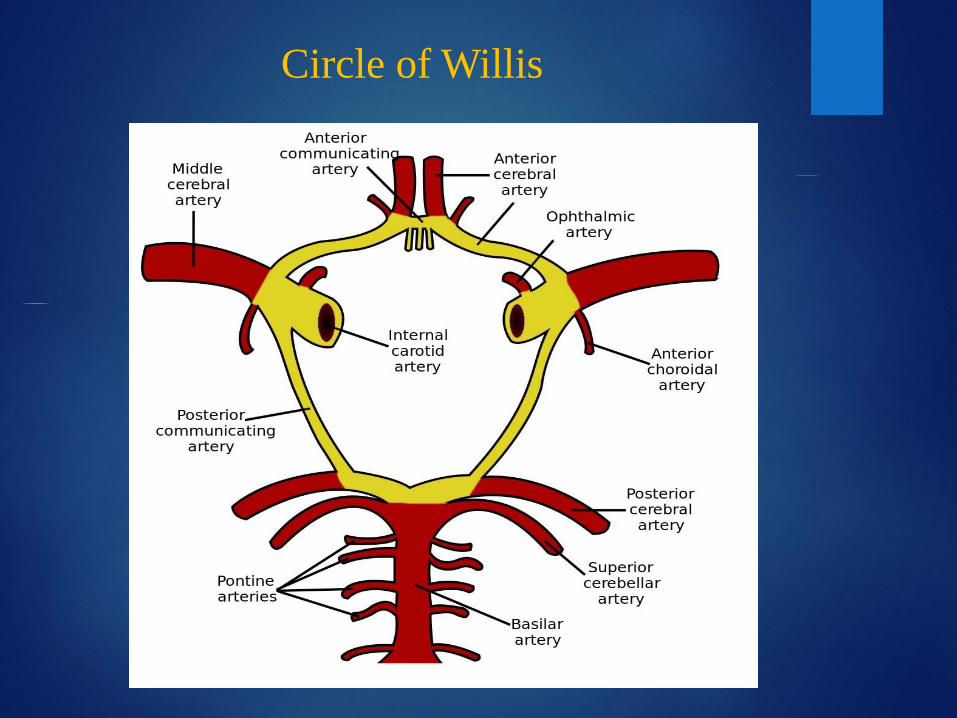
Generally aneurysm occur at the bifurcation and branches of
large arteries at the base of the brain, Circle of Willis.
85% develop in the anterior part of circulation (Carotid
System).
15% are found in posterior circulation (vertebrobasilar
system).
Important to understand Circle of Willis.
Suarez, et al. (2006), New England Journal of Medicine, 354, 387-396.

Circle of Willis
Circle of Willis
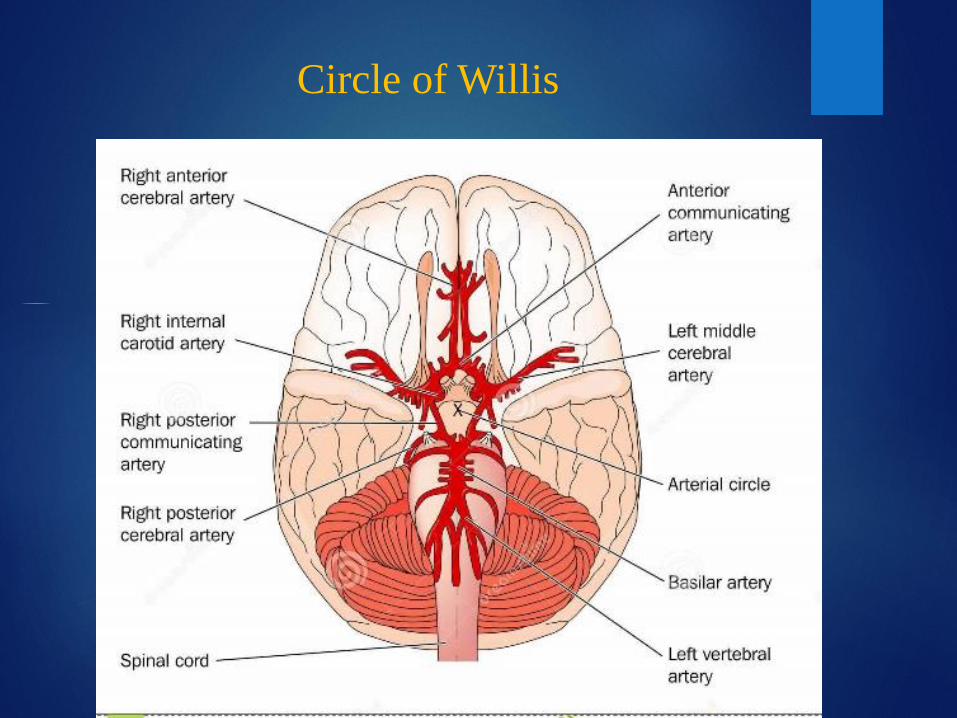
Circle of Willis

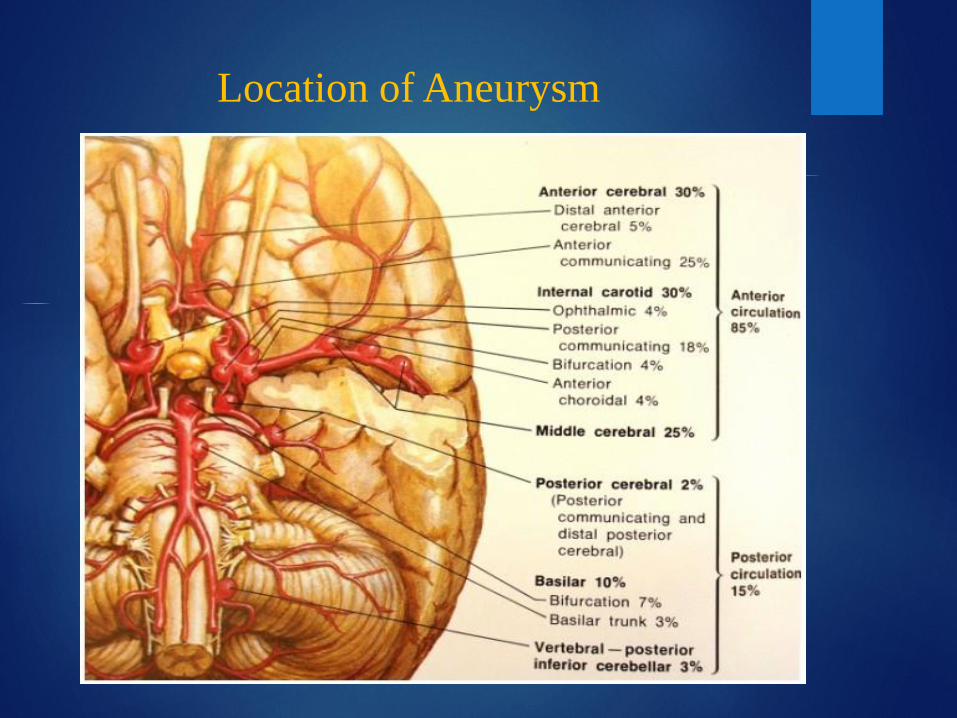
Location of Aneurysm
Anterior Communicating Artery (Acomm) is the single most
common: 30-40%
Posterior Communicating Artery (Pcomm): 25-30%
Middle Cerebral Artery (MCA): 20%
Basilar Artery (BA): general at basilar tip, 10%
20-30% patients who suffer an aneurysm will have multiple
aneurysms
Hickey, J.V. (2014). The Clinical Practice of Neurological and Neurosurgical Nursing

Location of Aneurysm
Location of Aneurysm

Diagnosis of Aneurysm
An unruptured aneurysm is generally asymptomatic thus
incidentally found.
Unruptured are generally diagnosed based on sign and
symptoms.
Aneurysms > 10mm, located at Basilar apex or Posterior
Communicating artery have higher chance to rupture.

Imaging of Aneurysm
CT- Angiography (CTA)
Sensitivity: 0.77-0.97 (reduces if aneurysm is < 3mm)
Specificity: 0.87-1.00
Takes app. 30 mins
Use of contrast: careful with Renal Failure patients
Magnetic Resonance Angiography (MRA)
Sensitivity: 0.69-0.99
Specificity: 1.00
Takes > 30 mins
Imaging of Aneurysm
Cerebral- Angiography
Arterial catheterization (femoral)
Benchmark for diagnosis aneurysms
More invasive and expensive
Three dimensional rotational
Helpful in finding aneurysm: location, shape, size, cerebral
vasculature, and presence of vasospasm

Major Threat of Aneurysm
Subarachnoid Hemorrhage (SAH)
Ruptured arterial aneurysm 95% cases of SAH

SAH
10 % of patients with aneurysmal SAH die prior to reaching
the hospital
25 % die within 24 hours of SAH onset
45 % die within 30 days; only one-third of patients will have a
good outcome after treatment
The most important predictive factors for acute prognosis after
SAH include
Level of consciousness and neurologic grade on admission
Patient age (inverse correlation)
Amount of blood on initial head computed tomography
(CT) scan (inverse correlation)
Signs and Symptoms
The worst headache of the life
Loss of consciousness or decrease LOC
Nausea and vomiting- very common
Stiff neck or neck pain
Blurred or double vision
Pain above and behind eye
Dilated pupils
Sensitivity to light
Loss of sensation
Cerebral edema and Increased ICP (may cause seizure, bradycardia, hypertension, wide pulse pressure).


Circle of Willis: Multiple aneurysms Brain: SAH

Hunt and Hess Scale (Clinical Grading of SAH)
Grade & Description
Grade1: Asymptomatic or minimal headache and slight nuchal rigidity
Grade 2: Moderate to severe headache, nuchal rigidity, no neurological deficit other than cranial nerve palsy
Grade 3: Drowsiness, confusion, or mild focal deficit
Grade 4: Stupor, moderate to severe hemiparesis, possible early decerebrate rigidity and vegetative disturbances
Grade 5: Deep coma, decerebrate rigidity, moribund appearance
Modification added:
Grade 0: Unruptured aneurysm
Grade1a: No brain reaction but fixed neurological deficit

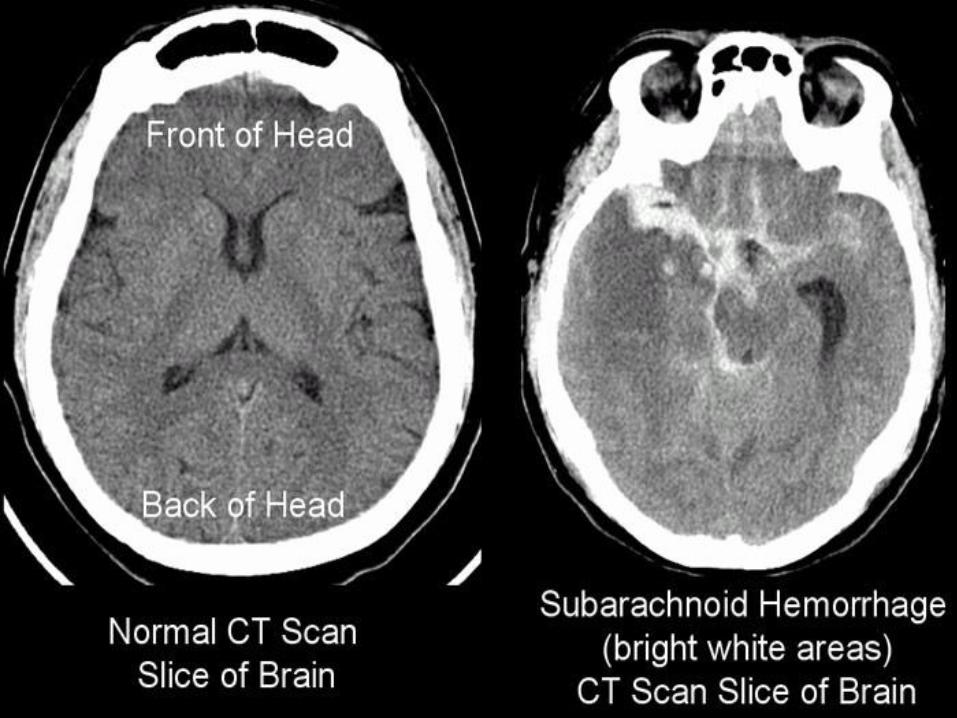
Diagnosis of SAH
Non-Contrast CT Scan
Preferred method of imaging: wider availability, lower cost,
convenient for sicker patient, provider experience with CT
4th generation-CT can detect SAH in 95% if done within 48 hrs.
Blood appears as high density (white) in subarachnoid space.
Lumbar Puncture (LP)
Indicated if clinical presentation suggest SAH and CT is negative
Presence of xanthochromia (the yellow discoloration indicating
the presence of bilirubin in the cerebrospinal fluid)
Presence of erythrocytes
Diagnosis of SAH
CTA
Frequently used
MRA
Not recommend with acute hemorrhage
Cerebral Angiography
Gold standard. May even require repeat study.
Transcranial Doppler (TCD)
Commonly used for patients with SAH to monitor blood flow
velocities in major cerebral arteries to detect early vasospasm.
120 cm/sec: Mild vasospasm
150 cm/sec: Moderate vasospasm
200 cm/sec severe vasospasm

Ruptured Ant CoA
aneurysm

SAH 20 ruptured
right PCA

Normal Circle of Willis 3-D CTA
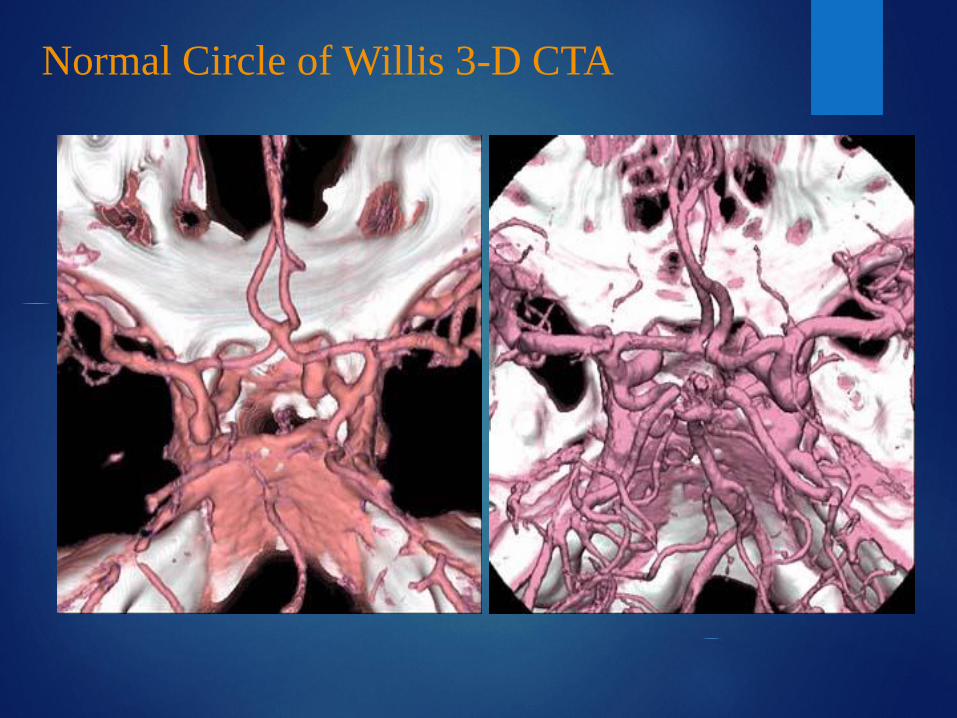
Normal Circle of Willis 3-D CTA

SAH 20
ruptured
ACA
aneurysm
3-D CTA
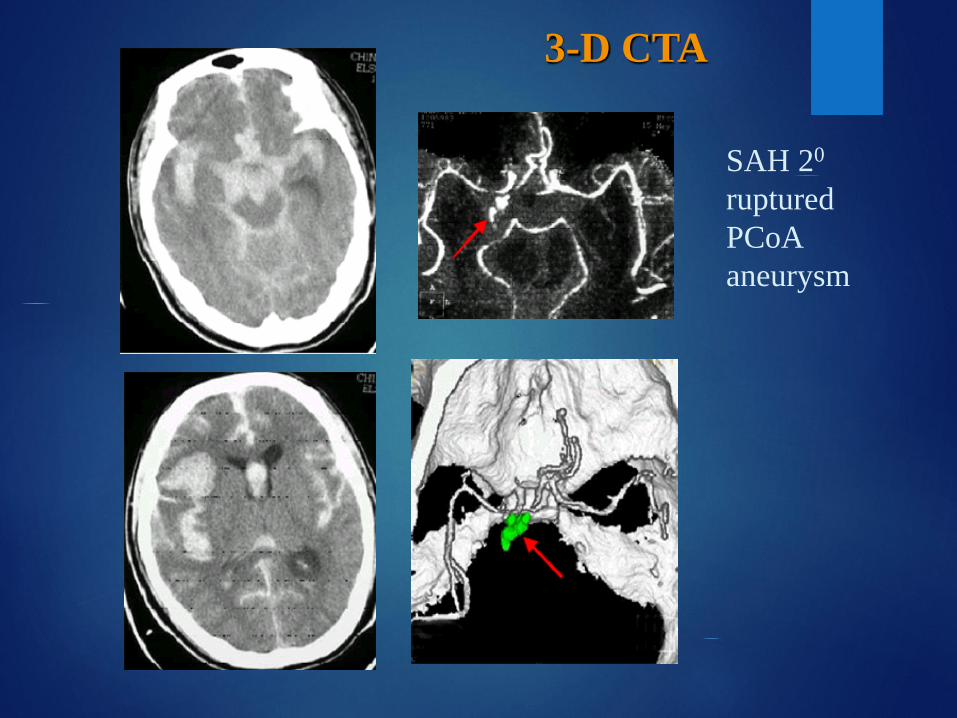
SAH 20
ruptured
PCoA
aneurysm
3-D CTA

Where is the aneurysm?
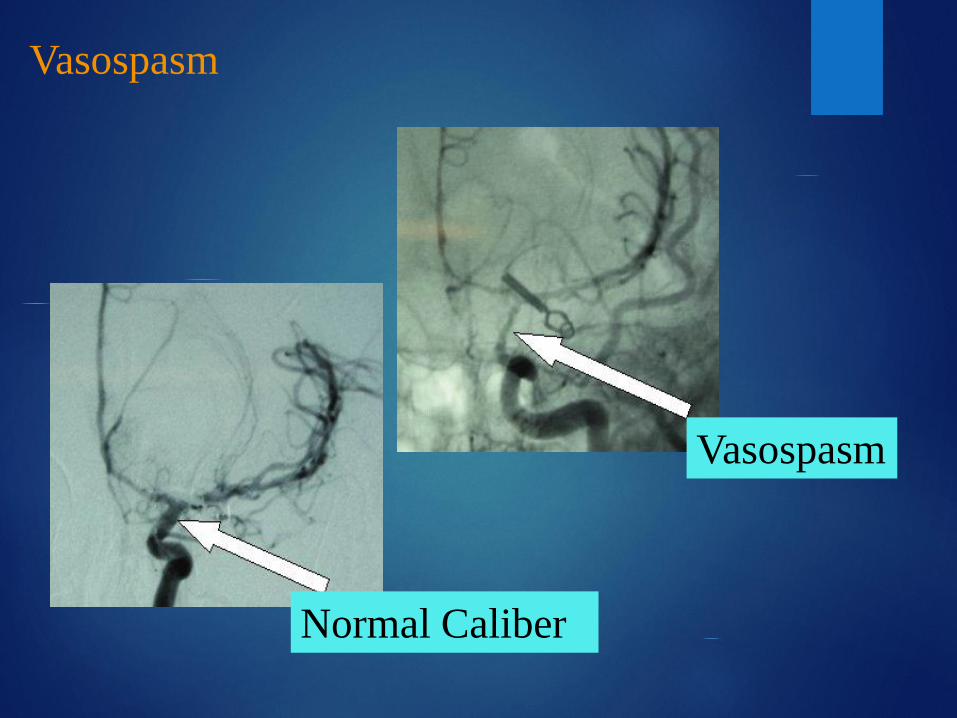
Normal Caliber
Vasospasm
Vasospasm

Treatments for Cerebral Aneurysms
Surgical Clipping
Endovascular Coiling

Surgical clipping (approximately 60-65% in the United States)
Endovascular coiling (approximately 30-35% in the United States)
In certain countries such as Finland, Great Britain and France, close to 90% of aneurysms are treated with endovascular coiling
Aneurysm Therapy
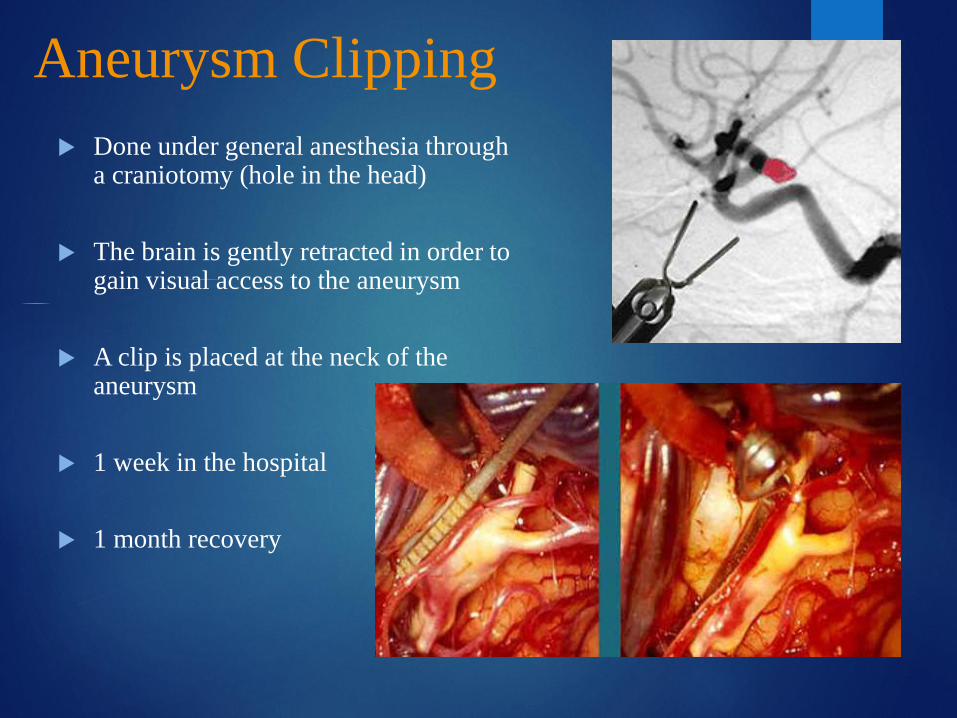
Aneurysm Clipping
Done under general anesthesia through a craniotomy (hole in the head)
The brain is gently retracted in order to gain visual access to the aneurysm
A clip is placed at the neck of the aneurysm
1 week in the hospital
1 month recovery
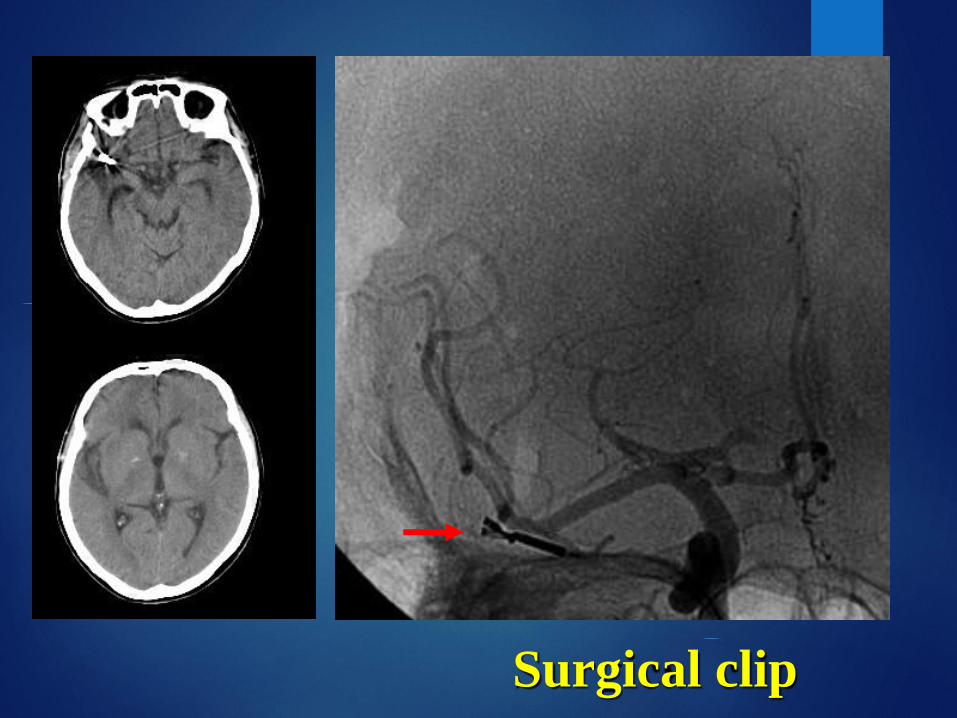
Surgical clip

ANEURYSM COILING
A minimally invasive procedure
Performed under general anesthesia
Performed by an interventional neuroradiologist
A microcatheter is threaded from the groin to the aneurysm
Coils (platinum threads ) are inserted into the aneurysm
The catheter is then removed
For an unruptured aneurysm, the patient is discharged home within 24 to 48 hours

The History of Coiling
1987-1989: Dr. Guido Guglielmi(University of Rome) visits DrViñuela (Interventional Neuroradiologist) at UCLA and research work on coiling concept started
1989: Dr Guglielmi came permanently to UCLA
1989-1990: Animal research
March 6, 1990: First clinical use of Guglielmi Detachable Coil
FDA approval in 1995

ANEURYSM COILING
Video
https://www.youtube.com/watch?v=kCE1zSM1TaA
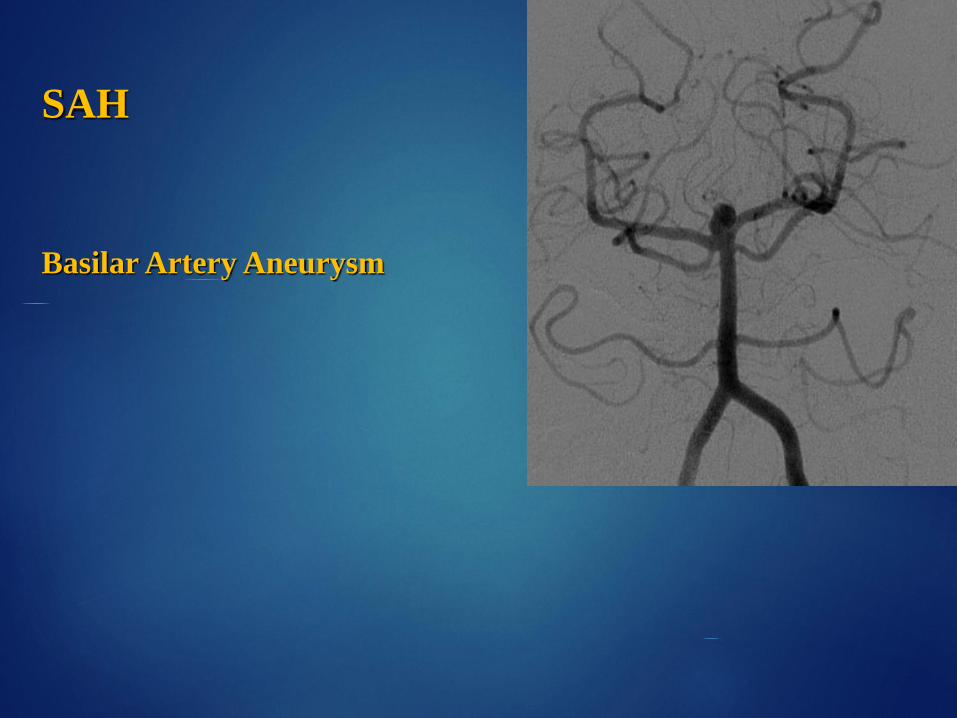
SAH
Basilar Artery Aneurysm



before after
Pros and Cons of Coiling
PROS
Minimally invasive
Short recovery
Safer than surgery
Cheaper than surgery
CONS
Shorter track record
Possibly less durable
Requirement for follow-
up angiography

What about Aneurysms with Wide Necks?
Aneurysms with wide necks must be treated in a slightly
different manner.
The use of a Neuroform stent or some similar stent must
first be placed across the base or neck of the aneurysm.
This is done so that the coils will remain within the
aneurysm sac.

Wide neck mid basilar aneurysm
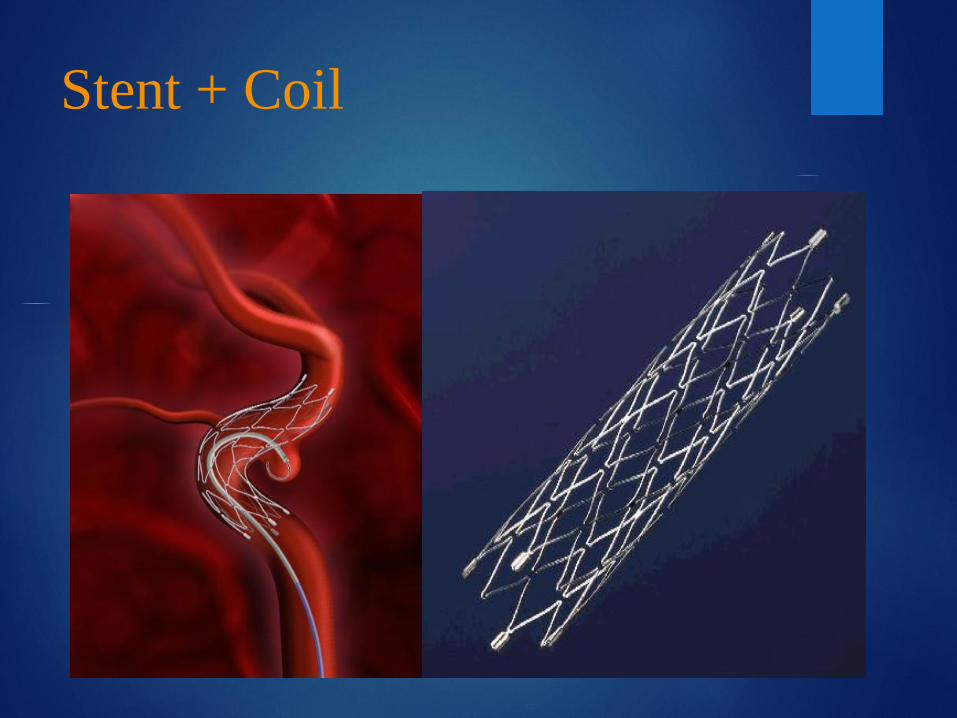
Stent + Coil

Stent + coils

Balloon Remodeling
Balloon remodeling is the use of a
balloon while placing coils within the
aneurysm.
The balloon is inflated while the coil
is placed and then deflated once coil
is in place.
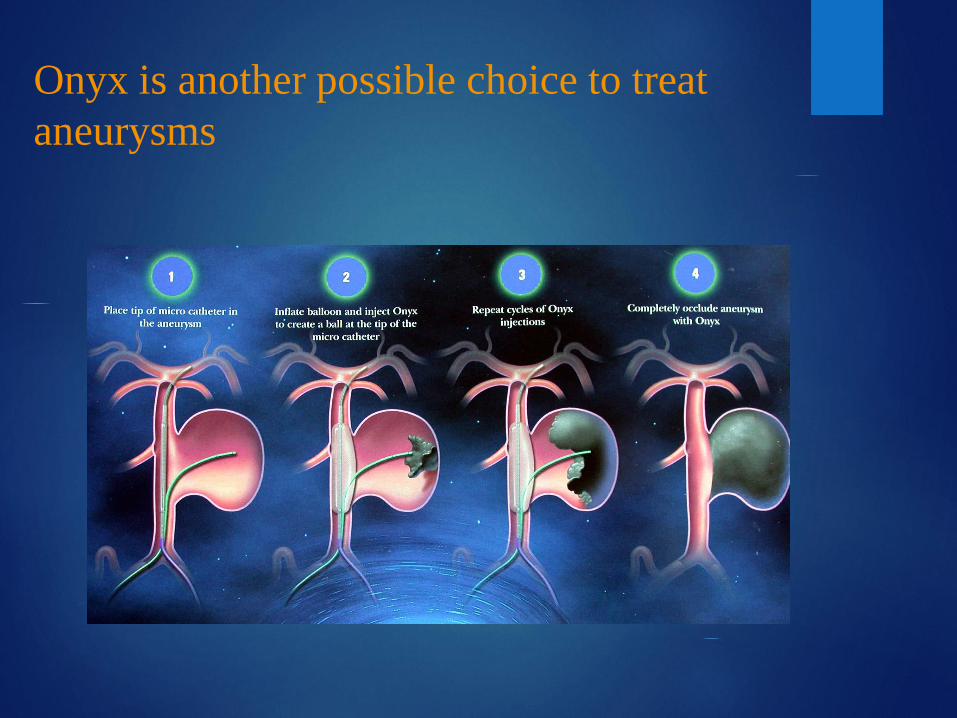
Onyx is another possible choice to treat
aneurysms
Complications of Aneurysm
Rebleeding:
4% chance on day 1, post rupture of aneurysm
1.5% daily for 13 days (15-20% within 14 days)
50% within 6 months
3% / year and mortality rate of 2% /year
Acute Hydrocephalus
Caused by obstruction of CSF and reabsorption Ischemic
Neurological deficit due to vasospasm
Seizures
DVT and PE
Hyponatremia and Hypovolemia

Goals of Treatment
Maintaining Hemodynamics
Close Cardiac Monitoring; NICU admission
A-Line
PAC (Hunt-Hess grade 111 or higher)
Euvolemic State (0.9 NS/Albumin)
Strict I/O
Maintaining Blood Pressure – Goal SBP: 120-150 mm Hg
(labetalol, nitroprusside or nicardipine)
Airway Protection
Intubation
Oxygenation optimization

Goals of Treatment Neuroprotection
HOB > 30 and patient must be bed rest
Neuro check q 1
Optimizing Cerebral Blood Flow (CBF)
Maintaining Cerebral Perfusion Pressure (CPP)
Maintaining Intracranial Pressure (ICP)- (use of Mannitol of ICP)
Preventing from vasospasm – Nimodipine (Nimotop)
Maintaining Blood Pressure (labetalol, nitroprusside or nicardipine)
Preventing seizures- Keppra
Treat Cerebral Edema- Steroids (Decadron)- controversial
Avoid activities that increases ICP- Stool Softener
Pain control- Analgesic (Dilaudid, Morphine, Codeine)
Avoid agitation- Sedative (Haldol, Seroquel)

Goals of Treatment
General Care
GI Prophylaxis (PPI)
Prevent DVT (Heparin or Lovenox)
Glycemic Control (Accu Checks and sliding scale)
Electrolyte Replacements
Skin Ulcer Prevention Care
Nutrition (Sooner the better)
Family Support
Rehabilitation

References
Brisman, J.L., Song, J.K., & Newell, D. W. (2006). Cerebral Aneurysms. New
England Journal of Medicine, 355, 928-939.
Hickey, J.V. (2014). The Clinical Practice of Neurological and Neurosurgical
Nursing (7th ed). New York, NY: Lippincott Williams & Wilkins.
Suarez, J.L., Tarr, R. W., & Selman, W. R. (2006). Aneurysmal Subarachnoid
Hemorrhage. New England Journal of Medicine, 354, 387-396.
Related Documents











