Centre for Brain and Mental Health Research University of Newcastle, AUSTRALIA APSAD Skills-based Workshop: Managing mental health issues in AOD settings Amanda Baker [email protected] u.au

Centre for Brain and Mental Health Research University of Newcastle, AUSTRALIA APSAD Skills-based Workshop: Managing mental health issues in AOD settings.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Centre for Brain and Mental Health ResearchUniversity of Newcastle, AUSTRALIA
APSAD Skills-based Workshop:Managing mental health issues in
AOD settingsAmanda Baker

Overview
• Brief introduction
• Key features of mental health issues
• A useful model of care • PsyCheck exercise (Lee et al 2007)
• Goals from today
Centre for Brain and Mental Health ResearchUniversity of Newcastle, AUSTRALIA

References
Key features
Kavanagh, D.J., Mueser, K.T. & Baker, A. (2003) Management of comorbidity. In M. Teesson & H. Proudfoot (Eds.) Comorbid mental disorders and substance use disorders. Canberra: Commonwealth of Australia.
www.nationaldrugstrategy.gov.au/publications/index.htm

References
Assessment
Dawe, S. et al. (2002). Review of diagnostic and screening instruments for alcohol and other drug use and other psychiatric disorders (2nd ed). Canberra: Commonwealth of Australia.
www.nationaldrugstrategy.gov.au/publications/index.htm

References
Innovations in treatment
A. Baker & R. Velleman (2007) Clinical Handbook of Co-existing Mental Health and Drug and Alcohol Problems. London: Brunner-Routledge.
References
Training
Lee, N. et al. (2007) PsyCheck: Responding to mental health issues within alcohol and drug treatment. Canberra, ACT: Commonwealth of Australia

Introduction: group activity
• What mental health issues are common in the setting in which you work?
• What are the advantages & disadvantages of addressing the mental health issues issues?
• What barriers are there to addressing mental health issues?
• How important is it to address mental health issues?
(10 minutes)
What mental health issues are we talking about?
• Multiple, co-existing conditions• No typical presentation• Anxiety & depression very common • May meet criteria for DSM• However, co-existing issues/problems may
be present and impact on client functioning and other domains

10 key features
1. Frequencies are high2. Highest risk vs highest frequency3. Greatest health impact is from tobacco4. Higher rates in treatment settings5. Correlates may differ across substances6. Co-existing problems = poorer outcomes7. Variety of causal relationships
(Kavanagh et al 2003)

Models
(i) MH problems led to D&A problems
(ii) D&A problems led to MH problems
(iii)Bidirectional models: multiple different factors trigger both
(iv) Common factor model: one or more factors independently increase the risk of both
(v) Two conditions unrelated
(Kavanagh et al 2003)
10 key features (cont’d)
8. Different intervention structures for different subgroups (psychosis – integrated; ?anxiety & depression)
9. A set of interventions required rather than a single intervention format
10. Comorbidity is under-serviced (Kavanagh et al 2003)
Who’s responsibility is it to address mental health issues?

Who is responsible?
Clinicians’ responsibility to work towards generation of commitment to change co-existing problems of substance use and mental disorder
Exclusion of people using substances or with unstable mental health symptoms from treatment abrogates responsibility for eliciting motivation and assisting the person in the hardest stages of change
(Kavanagh & Connolly, 2007)

What Works for You?• Working individually complete the worksheet,
identifying which models you have an affinity with
• Then circle the main model you work with
• Now find someone else in the room that uses a DIFFERENT model to the one you typically work with and discuss with your partner– Why you use this model/strategies you do?– How you know it’s working ?
• Group discussion
Mod
ule
2
Stepped Care Model
• Tiered interventions• Recommended for:
Depression (Scogin et al, 03)
Anxiety (Baillie & Rapee, 04)
Alcohol (Sobell & Sobell, 00)
Smoking (Smith et al, 01)
Heroin (King et al, 2002)

Stepped care
• Advantages– Facilitate a larger number into treatment– Low-cost, least intrusive and simple first
interventions as a first step maximises treatment resources
– Sufficient to improve motivation, engagement & some mental health symptoms

Stepped care
• Competent assessment – suicidality, risk of harm to others,
intoxication, possible withdrawal effects, accommodation requirements, mental health and other comorbidity
• Brief psychoeducation/mi, progress monitored
• Increase intensity of treatment or change focus of treatment (Sobell & Sobell, 2000)

Stepped care
• Flexible treatment plan– Guided by client progress and functioning– Rather than predetermined set of symptoms or
characteristics– So far virtually impossible to predict who with
coexisting problems will respond
• Common in clinical practice: regular, thorough assessment

Stepped care recommendations
• Step 1 (assessment/minimal intervention)– Screening, assessment, feedback and self-help
• AOD, mh, medical, QoL, current stressors, readiness to change
• Feedback • Self-help material• Refer on if necessary

Stepped care recommendations
• Step 2 (brief interventions, integrated psychoeducation, motivational interviewing)
• Assess (eg, 1-month later)• Continue monitoring or if not responded,
offer more

Stepped care recommendations
• Step 3– Monitor, intensive integrated CBT intervention– Could include pharmacotherapy and longer
psychosocial treatment
Integrated CBT recommended
• Various MH & D&A problems:– Anxiety (Baillie & Sannibale)
– Depression (Kay-Lambkin et al)
– Psychosis (Barrowclough et al)
– Bipolar (Whicher & Abou-Saleh)
– Eating disorders (Coelho et al)
– Personality disorder (McGovern et al)
– Learning difficulties (Barter)
Baker & Velleman, 2007

Further intervention
• Steps 4, 5 6 etc: – Longer-term, more intensive interventions– More specific interventions (eg, trauma,
relationship counselling)– Can transfer to monitoring and crisis
roundabouts at any time
PsyCheck as an example
• PsyCheck Screening Tool– The PsyCheck Mental health Screen for AOD
clients– Suicide/Self-harm risk assessment– Self-Reporting Questionnaire (SRQ)
Lee et al 2007

Interpreting the PsyCheck Screening Tool
• Intervention or further assessment is required if– The client reaches 5 or more on the SRQ– The client is at risk of suicide/self-harm– The client has a mental health history
• Consider– Readiness to change– Current symptoms Lee et al 2007
Mod
ule
1

SRQ Interpretation Lee et al 2007Total Score Interpretation Action
0 No symptoms present. Re-screen using the PsyCheck after 4 weeks
1-4 Some symptoms of depression, anxiety and/or somatic complaints indicated.
Offer Session 1
Re-screen after 4 weeks
Provide self-help material
5
or above
Considerable symptoms of depression, anxiety and/or somatic complaints indicated
Offer Sessions 1-4
Re-screen after 4
If no improvement after re-screening, consider referral
Mod
ule
1

Evidenced Based Practice Lee et al 2007
• Best evidence for CBT compared to other types of therapies– Most high level research (RCTs) and the most
positive research– Effective for a wide range of mental health
problems including AOD, anxiety and depression
BUT
Whatever framework you use, you can create your own evidence through measuring individual outcomes – CBT emphasises this
Mod
ule
2
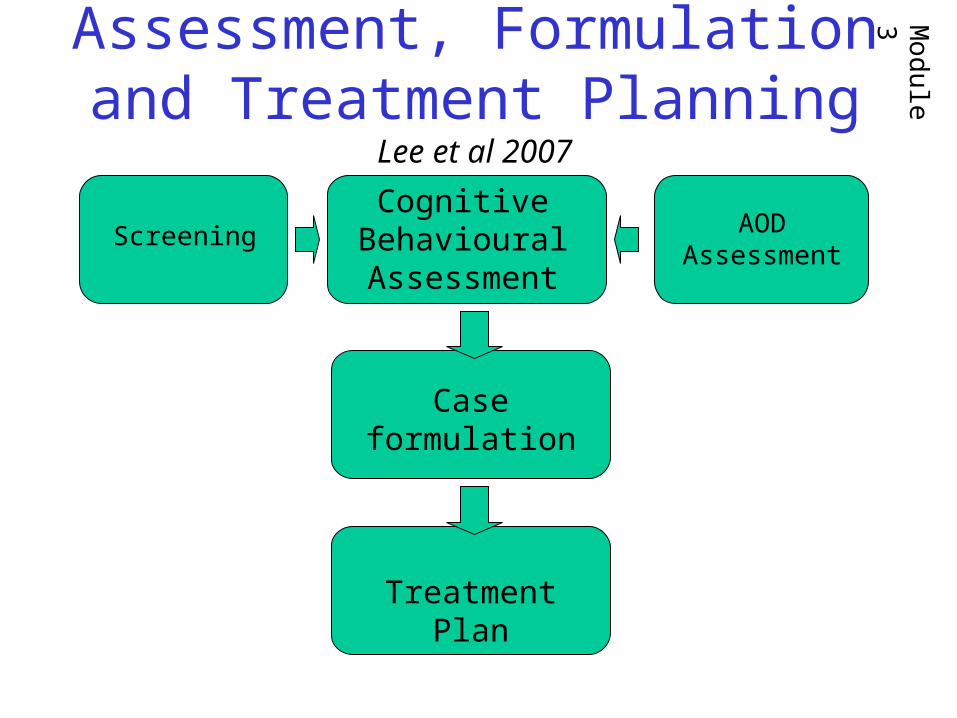
Assessment, Formulation and Treatment Planning Lee et al 2007
ScreeningCognitive
Behavioural Assessment
Case formulation
Treatment Plan
AOD Assessment
Mod
ule
3
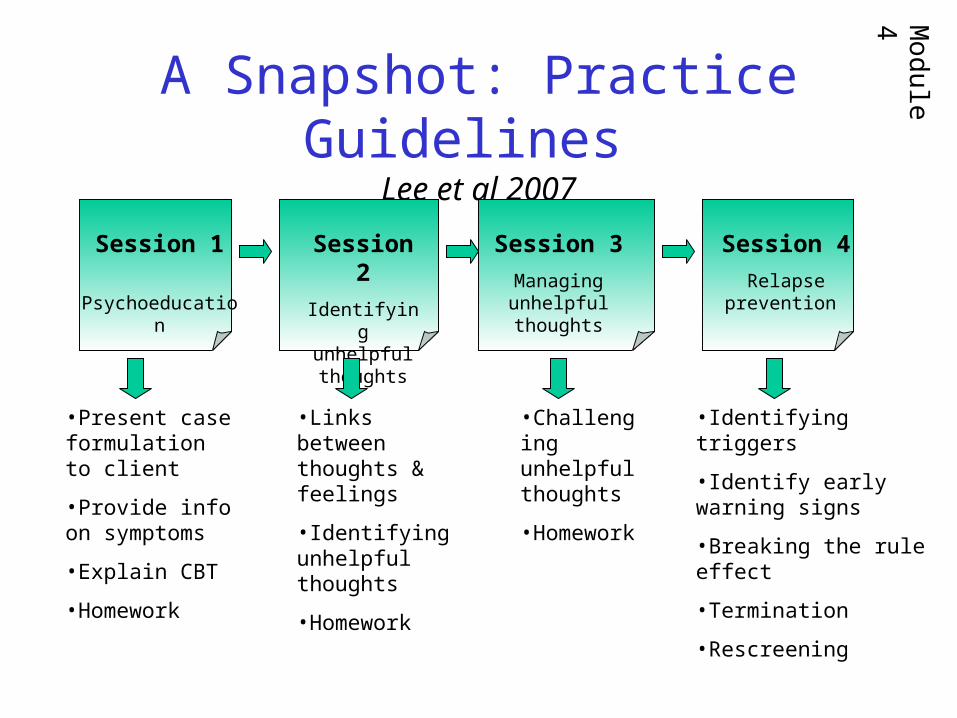
A Snapshot: Practice Guidelines Lee et al 2007
Session 1
Psychoeducatio
n
Session 2
Identifying unhelpful thoughts
Session 3
Managing unhelpful thoughts
Session 4
Relapse prevention
•Present case formulation to client
•Provide info on symptoms
•Explain CBT
•Homework
•Links between thoughts & feelings
•Identifying unhelpful thoughts
•Homework
•Challenging unhelpful thoughts
•Homework
•Identifying triggers
•Identify early warning signs
•Breaking the rule effect
•Termination
•Rescreening
Mod
ule
4

Conclusions
• Screening & assess MH & AOD issues
• Consider a stepped care approach
• PsyCheck may help guide you
• Provide integrated interventions where necessary

Your Goal
What small goal can you set after attending this brief workshop?
(eg, reading, discussion with colleagues, try some mental health screening instruments,
link up with a psychologist)
Related Documents











