Cellulitis Timothy F. Brewer, MD, MPH February 24, 2011

Cellulitis Timothy F. Brewer, MD, MPH February 24, 2011.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cellulitis
Timothy F. Brewer, MD, MPH
February 24, 2011
You are in the ER
• 82 year old woman presents with 2 days of fever and inability to walk for 24 hours– Started on ciprofloxacin when fever started for
possible UTI– Yesterday noted redness, swelling pain of left
foot, progressing so that she is unable to bear weight
– PMH: NKA, cellulitis in right leg 4 years ago; trip to Florida 3 months ago, no animal exposures
Physical Examination
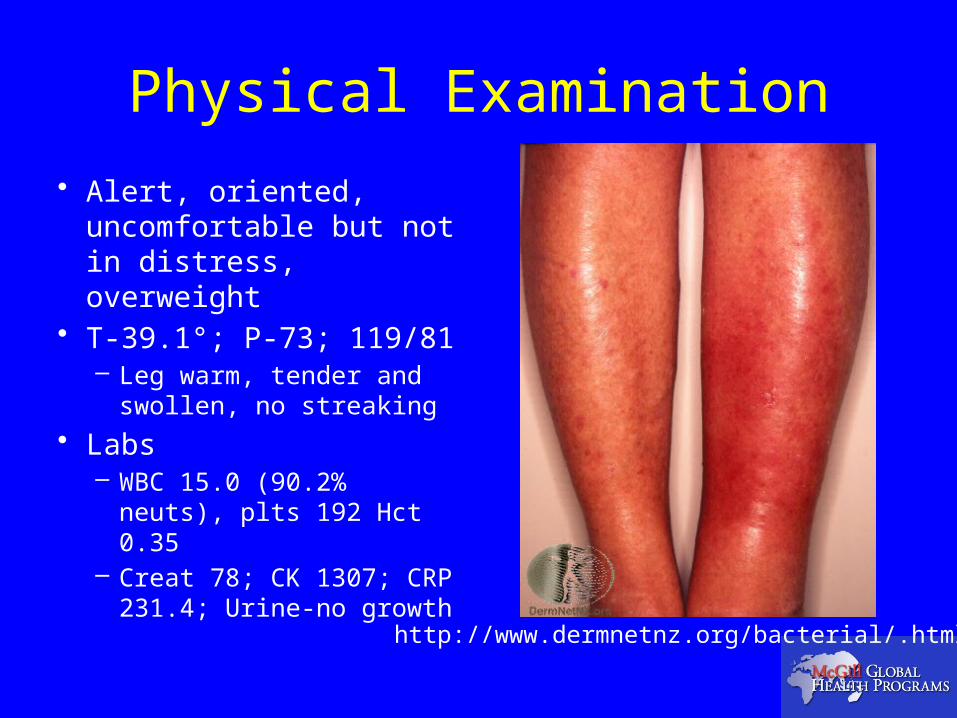
• Alert, oriented, uncomfortable but not in distress, overweight
• T-39.1°; P-73; 119/81– Leg warm, tender and
swollen, no streaking
• Labs– WBC 15.0 (90.2%
neuts), plts 192 Hct 0.35– Creat 78; CK 1307; CRP
231.4; Urine-no growthhttp://www.dermnetnz.org/bacterial/.html
Next steps
• Patient admitted and started on timentin and clindamycin. Appropriate management at this point would include:A. Urgent/emergent surgical consultation
B. Switch to Cefazolin intravenously
C. Continue current antibiotics and add IVIG
D. Continue current antibiotics and get CT scan

Overview of discussion
• Things we will not cover in detail today– Impetigo, folliculitis, boils (abscesses)
• Epidemiology of cellulitis– Frequency, risk factors, organisms
• Management– Blood cultures– Outpatient vs. inpatient; oral vs. IV antibiotics
• Special situations– Unusual exposures, unusual hosts
Definitions
• Cellulitis– Acute pyogenic inflammation of the dermis
and subcutaneous tissue associated with redness, swelling and pain
– Usually lacks a well-demarcated border• Erysipelas
– Superficial cellulitis with prominent lymphatic involvement causing induration “peau d‘ orange” and raised border
– Swartz. New Engl J Med 2004:350:904.

Location of Infection
Stevens. Ann Intern Med 2009; Jan In the Clinic

Some non-cellulitic skin infections
• Impetigo– Usually Staph aureus or
β-hemolytic Streptococci– More common in children– Blisters, sores, crusting
lesions and exudate– Topical therapy
(mupirocin) for limited lesions or oral antibiotics
– Swartz. New Engl J Med 2004;350:904.
• Folliculitis– Staph aureus
• Candida, M. furfur and non-infectious causes
• Hot tubs: P. aeruginosa
– Pustules in hair follicles & apocrine region
– Lesions at different stages (buttocks, axilla)
– Local care, mupirocin/antifungal cream
– Pasternack. In Mandell’s Principles & Practice of Infectious Diseases 2009.

Impetigo and folliculitis
http://www.dermnetnz.org/bacterial/.html
Epidemiology
• Approximately 28,000 cases of erysipelas and cellulitis in the Netherlands in 2001– Outpatient rate 179.6/100,000– Hospitalization rate 12.1/100,000
• Increased with age (>100/100,000 over 85 yrs old)• Median length of stay 9 days• 1.9% in-patient mortality
» Goettsch. JEADV 2006;20:834.
Epidemiology
• Population-based study of 7438 cellulitis cases among Mormons ≤ 64 yrs old in Western US, 1997-2002 identified through insurance claims – Overall rate of 2,460/100,000
• Increased with age, male > females• 39.9% occurred on the legs
– 32.8% other/unspecified
• 73.8% seen in outpatient clinics; 5.7% hospitalized• 11.1% 1 year recurrence rate
» Simonson. Epidemiol Infect 2006;134:293.

Microbiology of cellulitis
• Approximately 80% of cellulitis cases assumed to be due to Streptococcal species or S. aureus
» Swartz. New Engl J Med 2004;350:904.
• Systematic review of studies of patients with intact skin and cellulitis who underwent punch biopsy or needle aspiration for culture– 127/808 (15.7%) had a positive culture
• 65 positive for Staph aureus (51% of positive cultures)• 35 positive for Group A Strep (28%)• 37 positive for other organisms or mixed cultures (29%)
» Chira. Epidemiol Infect 2010;138:313.
Role of blood cultures
• 757 cases of community-acquired cellulitis from 1995-1998– 553 patients (73%) had blood cultures done
• 11 patients (2%) had positive cultures;– 8 Streptococci, 1 S. aureus, 1 V. vulnificus, 1 M. morganii
• 20 cultures (3.6%) were considered contaminants» Perl. Clin Infect Dis 1999;29:1483.
• 2,678 cases of community-acquired cellulitis from 1997-2004– 308 patients (12%) had blood cultures done
• 57 patients (18.5%) had positive cultures;– 24 Streptococci, 14 gram-negative bacteria1 S. aureus,
• Proximal limb, ≥ 2 comorbid diseases, no recent antibiotics» Peralta. Eur J Clin Microbiol Infect Dis 2006;25;619

Risk factors for disease• 167 patients ≥ 15 years old with leg erysipelas
admitted to 1 of 7 French hospitals in1995-96– Matched with 294 age, sex & hospital controls
Dupuy. BMJ 1999;318:1591.

Risk factors for disease
• 100 patients hospitalized in Iceland between 2000-2004 with acute lower limb cellulitis– 200 controls hospitalized controls matched for age (±
5 years) and sex• Median age 66.5; BMI 27.7 in cases, 25.8 in controls
– History of cellulitis OR 31.04 (95% CI 4.15-232.20)– S. aureus or β-hemolytic Strep in toe webs OR 28.97
(95% CI 5.47-153.48)– Erosions, ulcers or wounds OR 11.80 (2.47-56.33)– Saphenectomy OR 8.49 (1.62-44.52)
» Bjornsdottir. Clin Infect Dis 2005;41:1416.

You are called back to the ER
• 78 yr old man presents with 1 month history of a swollen, itchy left ankle and 3 weeks of progressive redness, swelling pain of ankle & calf; still able to walk– PMH Type II diabetes, hypothyroidism, CABG
x 4 in 2008, Lt hip prosthesis, hernia repair, ex-smoker, allergic to penicillin (? Reaction as child)
– No recent hospitalizations or travel

Physical Examination
• Alert, no distress• T-36.4°; P-89; 124/89
– Decreased breath sounds bilaterally, ventral hernia
– Lt ankle and calf warm, tender and swollen, no streaking, excoriations on skin
• Labs– WBC 6.7, plts 187, Hb 122– Creat 79; CK 1433; lactate
1.2– CXR bilateral pleural
effusions http://www.dermnetnz.org/bacterial/.html
What now?
• Patient started on timentin (? Penicillin stress test). Appropriate next steps include:A. Switch to oral therapy and arrange outpatient
follow-up
B. Switch to IV ertapenem and arrange to see in the medical day clinic tomorrow
C. Switch to IV vancomycin and admit to the hospital
D. Switch to IV cefazolin and admit to the hospital

Whose at risk for bad outcomes?
• 332 cases of community-acquired cellulitis from 1995-2000 in Spanish hospital– Mean age 59.7, 52% women
• 82 (25%) with diabetes, 66 (20%) with cancer, 41 (12%) with cirrhosis, 21 (6%) with necrotizing soft tissue infection
• Mean duration of hospitalization 11.8 days• 8 early deaths (<72 hours); 5% (16) 1 month mortality• Mortality associated with multiple comorbid conditions,
CHF, renal insufficiency, obesity, shock and P. aeruginosa infection
» Carratala. Eur J Clin Microbiol Infect Dis 2003;22:151.

Summary so far
• Cellulitis is common– 2-24 cases/1,000 person-years
• Age, lymphedema, obesity, previous cellulitis, saphenectomy/mastectomy, leg edema, ulcers, wounds and fungal infections increase risk
– Most commonly caused by S. aureus or Strep species• But many bacteria and fungi capable of causing cellulitis
– Majority (approximately 70-80%) can be treated as outpatient
– Increased risk of mortality with• Co-morbid conditions, heart failure, obesity, gram-negative
infections

Treatment recommendations
• Erysipelas– Penicillin
• Cellulitis– 1st generation cephalosporin
• Cephalexin, cefazolin
– Penicillinase-resistant semi-synthetic penicillin• Dicloxacillin, nafcillin, oxacillin
– Penicillin allergic patients• Clindamycin, erythromycin or vancomycin
• Treatment based on clinical response– Ranges from 5-14 days (average 7 days)
» Stevens. IDSA Practice Guidelines. Clin Infect Dis 2005;41:1373.

IDSA treatment guidelines
Stevens. IDSA Practice Guidelines. Clin Infect Dis 2005;41:1373.
Ancillary treatments
• Elevation• Treatment of leg edema• Compression dressings once acute
inflammation diminished• Treatment of interdigital dermatophyic
infections with topical antifungals– Clotrimazole, miconazole, terbinafine, ciclopirox
» Swartz. New Engl J Med 2004:350:904.» Stevens. IDSA Practice Guidelines. Clin Infect Dis
2005;41:1373.

Some special situationsRisk factor/Exposure Organisms Treatment
Diabetic ulcers S. aureus, gram-negative bacteria, anaerobes
Piperacillin-tazobactam, meropenem
Abscesses, boils S. aureus Drainage in addition to antibiotics
Human bites Eikenella corrodens; anaerobic Strep, Bacteroides
Amoxicillin-clavulanate
Cat bites Pasteurella multocida Amoxicillin-clavulanate, doxycycline
Dog bites Pasteurella multocida, Capnocytophaga canimorsis
Amoxicillin-clavulanate
Salt water, shellfish Vibrio vulnificus Doxycycline
Fish handlers Erysipelothix rhusiopathiae Amoxicillin, ciprofloxacin
Fresh water Aeromonas species Ciprofloxacin
Neutropenia Pseudomonas aeruginosa Meropenem, Piperacillin-tazobactam
Swartz. New Engl J Med 2004:350:904. Stevens. Ann Intern Med 2009; Jan In the Clinic

Day 3, things are no better
• Right diagnosis, correct but insufficient treatment– Elevation, time, inadequate antibiotics
• Correct diagnosis, wrong treatment– Unusual or resistant organisms (MRSA)
• Wrong diagnosis

Failure in outpatient treatment
• Retrospective review of 405 outpatients treated with oral antibiotics (aged 18-86 years old) between 2005-2007– 70 (17%) had treatment failure at follow-up visit; risk
factors for failure included:• upper limb cellulitis (OR 2.06),• moderately severe disease (OR 3.74),• antibiotic not active against MRSA (OR 4.22)• Lack of drainage when abscess present (OR 4.38)
– 134/180 (74%) successfully treated with cephalexin– 138/152 (91%) success with TMP-SMX– 34/40 (855) success with clindamycin
» Khawcharoenporn. Amer J Med 2010;123:924.
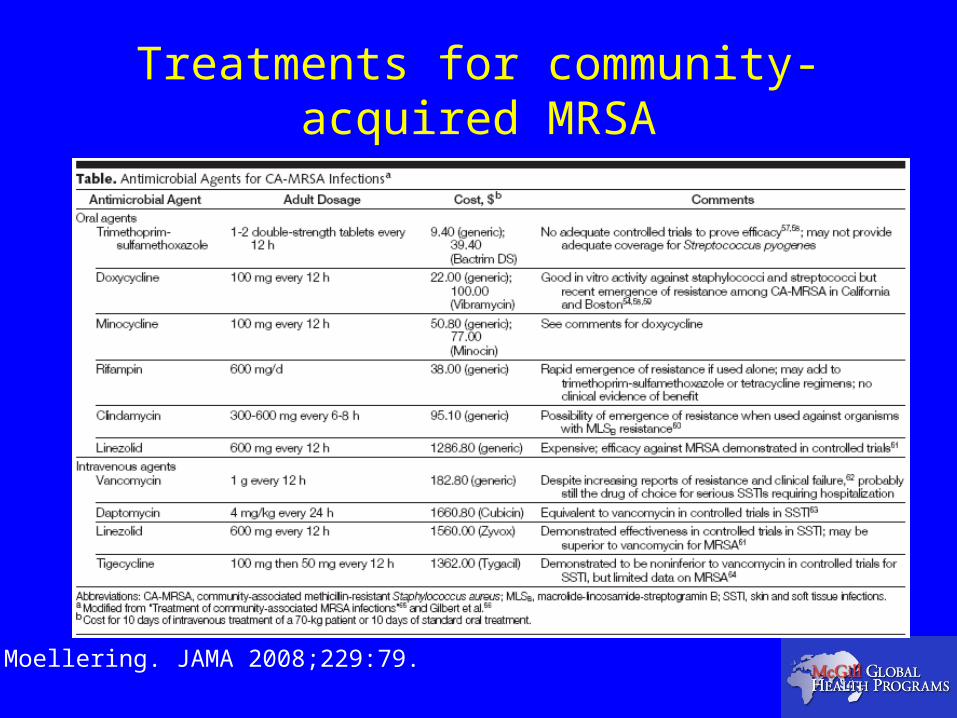
Treatments for community-acquired MRSA
Moellering. JAMA 2008;229:79.
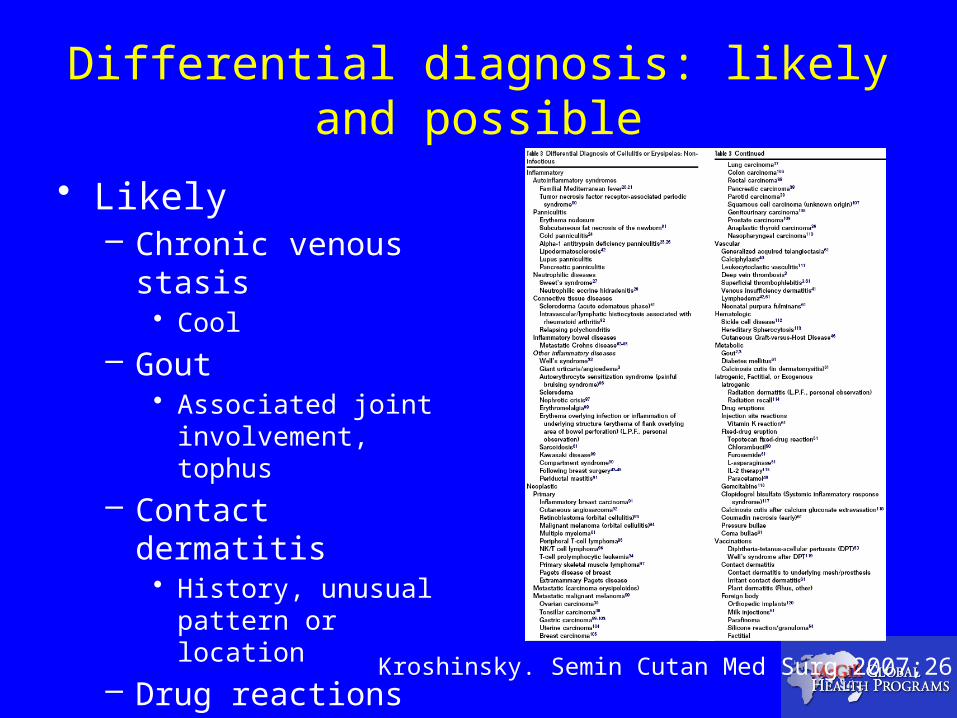
Differential diagnosis: likely and possible
• Likely– Chronic venous stasis
• Cool
– Gout• Associated joint
involvement, tophus
– Contact dermatitis• History, unusual pattern
or location
– Drug reactions• history
Kroshinsky. Semin Cutan Med Surg 2007;26:168.

Differential diagnosis: things that look like cellulitis but are not
Swartz. New Engl J Med 2004:350:904.

Rashes of Sweet’s and Wells Syndromes
Ratzinger. Amer J Dermatopath 2007;29:125.
Katoulis. Clin Exper Derm 2009;34:e375.

Risk factors for recurrence
• Case-control study of 47 male patients with recurrent cellulitis followed in a VA center 1998-2002, median age 59 yrs old– 94 age, sex matched controls with 1 episode cellulits
• Leg edema (OR 4.43, 95% CI 1.82-10.82)• BMI (OR 1.09, 95% CI 1.03-1.16)• Tobacco use (OR 3.12, 95% CI 1.18-8.23)• Homelessness (OR 3.62, 95% CI 1.03-12.69)
» Lewis. Amer J Med Sci 2006;332;304h.
• Case-control study of 90 patients with cellulitis, 2004-2005, 44 with a history of previous disease, median age 58 yrs old– 46 patients with single episode
• Obesity (OR 9.5, 95% CI 2.2-40.8)• Previous operation (OR 3.4, 95% CI 1.3-9.2)
» Karppelin. Clin Microbiol Infect 2010;16;729.
You are back in the ER
• 36 year old man presents with 2 days of right hand swelling and pain, no history of trauma– 24 hours of fever, chills, nausea and vomiting– PMH unremarkable except for seasonal
allergies and hernia repair, no recent travel, lived on farm with horses, dogs and cats
– Smokes, occasional ETOH, no other drug use

Physical Examination
• Acutely ill and confused• T-37.9°; P-145; 73/25,
R-30 with 100% O2 on 6L– Rt hand mottled, cool
and swollen, no crepitus
• Labs– WBC 17.9 (24% bands),
plts 133 Hct 0.44– Creat 211; CK 2,934;
Lactate 2.3Filbin. New Engl J Med 2009;360:281.

Next steps
• Patient started on early goal-directed therapy for sepsis including 10 L fluid, pressors, ceftriaxone, piperacillin-tazobactam, steroids and Benadryl. CT scan shows subcutaneous fluid without gas, abscess or bone involvement. Optimal management at this point would be:A. Switch piperacillin-tazobactam to clindamycinB. Add vancomycin IVC. IVIGD. Emergent surgical debridement

Next steps
• Emergent surgical debridement
Filbin. New Engl J Med 2009;360:281.
Necrotizing fasciitis and gas gangrene
• Type I– Mixed infections with Staph, Strep, gram-negative bacteria and anaerobes
• Portal of entry often obvious (recent surgery), gas usually present, bulla and necrosis of skin
– Diabetes is risk factor– Fournier’s gangrene when involving the groin
• Type II– Streptococcus pyogenes (Group A Strep, “flesh-eating bacteria”)
• Acute, may not have clear portal of entry, gas absent, severe systemic symptoms and shock, pain out of proportion to appearance of skin
• Anaerobic myonecrosis (Type III or gas gangrene)– Clostridium perfringens and other species
• Usually associated with previous injury or trauma, crepitus and extensive gas in tissues, marked edema and bulla; C. septicum associated with occult colonic tumors
» Swartz. New Engl J Med 2004;350:904.» Stevens. Ann Intern Med 2009; Jan In the Clinic

Necrotizing fasciitis treatment
• Type I– Broad-spectrum antibiotics (meropenem & vancomycin)
• Type II– Penicillin (ceftriaxone or vancomycin) and clindamycin
• Clindamycin to interfere with toxin production, more active against non-replicating bacteria
• Myonecrosis– Penicillin (vancomycin) and clindamycin
• All require emergent surgical evaluation, septic shock treatment as appropriate
• Value of IVIG unproven, but used sometimes in Type II» Swartz. New Engl J Med 2004;350:904.» Stevens. Ann Intern Med 2009; Jan In the Clinic» Stevens. IDSA Practice Guidelines. Clin Infect Dis 2005;41:1373

Bringing it all home-outpatients
• Cellulitis usually treated as an outpatient– Dicloxacillin, cefadroxil, clindamycin
• Gram-positive fluoroquinolones (levofloxacin) also okay
– Abscess or boil think Staph aureus• Need incision and drainage
– Antibiotics not needed if no cellulitis
• For CA-MRSA, TMP-SMX (not great for Strep), doxycycline or clindamycin (can be resistance)
– Usually treat for 5-7 days
In the hospital
• Consider admitting– Older patients, those with co-morbid diseases
such as heart or renal failure, those with significant edema, recurrent disease
• Inpatient therapy (simple cellulitis)– Cefazolin, nafcillin, oxacillin, vancomycin– Think MRSA in recent hospitalizations,
antibiotics, treatment failures• Vancomycin, daptomycin, linezolid
– Elevation, elevation, elevation
When to get ID Consult
• Orbital cellulitis• Suspected necrotizing fasciitis or gas
gangrene• Cellulitis with sepsis• Immunocompromised hosts• Unusual exposures• When you are not sure what is going on

A final note
Patients are not canvases
If you feel the need to draw, do it in the medical chart.
http://www.manyirons.com/Puker/Drawings/picasso_stravinsky_1920.jpg
Related Documents











