6/23/2014 1 Celiac Disease: Past, Present and Future BETH ISRAEL DEACONESS MEDICAL CENTER HARVARD MEDICAL SCHOOL Daniel Leffler MD, MS Research Director @ The Celiac Center Beth Israel Deaconess Medical Center Celiac Disease Program @ Harvard Medical School Associate Professor of Medicine Harvard Medical School Celiac Disease in the Past 50 A.D. - Aretaeus the Cappadocian “If the stomach be irretentive of the food and if it pass through undigested and crude, and nothing ascends into the body, we call such persons koeliacs" 1888 - Samuel Gee separates celiac disease from non-diet responsive chronic malabsorption. “On the Coeliac Affection…if the disease is to be cured at all it must be by means of diet” Celiac Disease in the Present: Three Breakthrough Discoveries 1950 - Dicke publishes his medical school thesis: ‘Investigation of the harmful effects of certain cereals on patients with celiac disease’ 1970’s –HLA DQ2 associated th celiac disease/dermatitis herpetiformis 1997 - The role of tissue transglutaminase in celiac disease identified

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
6/23/2014
1
Celiac Disease:Past, Present and Future
BETH ISRAEL DEACONESSMEDICAL CENTER
HARVARD MEDICAL SCHOOL
Daniel Leffler MD, MSResearch Director @ The Celiac CenterBeth Israel Deaconess Medical Center
Celiac Disease Program @ Harvard Medical SchoolAssociate Professor of Medicine
Harvard Medical School
Celiac Disease in the Past 50 A.D. - Aretaeus the Cappadocian “If
the stomach be irretentive of the food and
if it pass through undigested and crude,
and nothing ascends into the body, we
call such persons koeliacs"
1888 - Samuel Gee separates celiac disease
from non-diet responsive chronic
malabsorption. “On the Coeliac Affection…if
the disease is to be cured at all it must be by
means of diet”
Celiac Disease in the Present:Three Breakthrough Discoveries
1950 - Dicke publishes his medical school
thesis: ‘Investigation of the harmful effects of
certain cereals on patients with celiac disease’
1970’s –HLA DQ2 associated
th celiac disease/dermatitis
herpetiformis
1997 - The role of tissue
transglutaminase in celiac disease
identified

6/23/2014
2
PathophysiologyStep 1: Gluten Entry into the Submucosa
Green, Cellier NEJM 2007
Step 2: Deamidation of Gluten by Tissue Transglutaminase (tTG)
Step 3: Immune Activation
Only HLA DQ2 and DQ8 are able to bind gluten!
Step 1
Step 2 Step 3
Serologic tests
Dermatitis Herpetiformis: Model for Celiac Disease Outside the Gut
Zone et al. J. Investigative Dermatology, 2009 Murray, et al. Int. J. Derm, 2003
Antibodies to TG3 or T cells primed to react to TG
Antibodies deposit at Dermal-Epidermal junction
•Complement activation•Cytokine release•Neutrophil infiltrate
Dapsone / sulfapyridine
Celiac Disease is a Multi-System Autoimmune Disorder
Hadjivassiliou et al. Lancet, Neuro 2010
Dermatitis Herpetiformis
Classic Celiac + Manifestations in:
Lung, Liver, Kidney, Blood
Vessels, Placenta, etc
Lane Hamilton Syndrome IgA Nephropathy MPGN Cardiomyopathy, IHD Fertility
+
6/23/2014
3
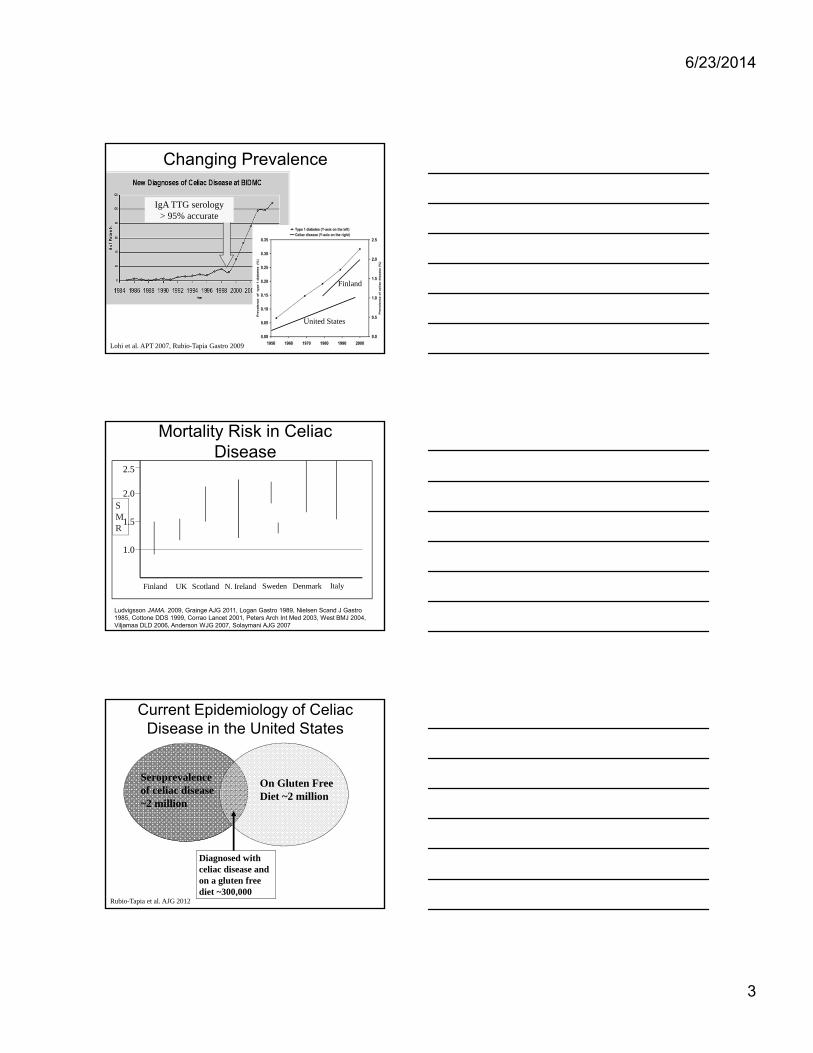
Changing Prevalence
What happened here?IgA TTG serology> 95% accurate
United States
Finland
Lohi et al. APT 2007, Rubio-Tapia Gastro 2009
Mortality Risk in Celiac Disease
Ludvigsson JAMA. 2009, Grainge AJG 2011, Logan Gastro 1989, Nielsen Scand J Gastro 1985, Cottone DDS 1999, Corrao Lancet 2001, Peters Arch Int Med 2003, West BMJ 2004, Viljamaa DLD 2006, Anderson WJG 2007, Solaymani AJG 2007
SMR
DenmarkFinland N. Ireland SwedenUK ItalyScotland
2.5
2.0
1.5
1.0
Current Epidemiology of Celiac Disease in the United States
Rubio-Tapia et al. AJG 2012
On Gluten Free Diet ~2 million
Seroprevalence of celiac disease ~2 million
Diagnosed with celiac disease and on a gluten free diet ~300,000
6/23/2014
4
Current Definitions
• Celiac disease is a chronic small intestinal immune-mediated enteropathy precipitated by exposure to dietary gluten in genetically predisposed individuals.
vs. • Non-Celiac Gluten Sensitivity (NCGS) relates
to one or more of a variety of immunological, morphological or symptomatic manifestations that are precipitated by the ingestion of gluten in people in whom CD has been excluded.
Ludvigsson J. Et al. GUT 2012.
Wahnschaffe U, et al. CGH 2007.
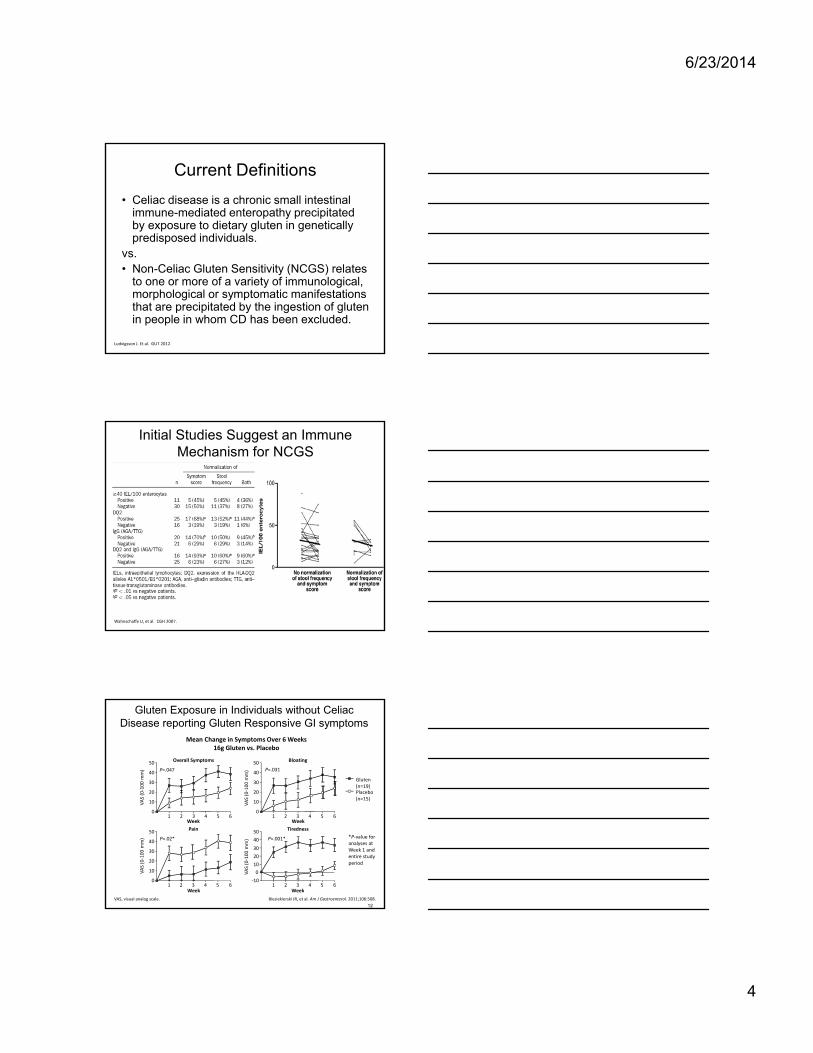
Initial Studies Suggest an Immune Mechanism for NCGS
Gluten Exposure in Individuals without Celiac Disease reporting Gluten Responsive GI symptoms
12
Biesiekierski JR, et al. Am J Gastroenterol. 2011;106:508.VAS, visual analog scale.
Mean Change in Symptoms Over 6 Weeks16g Gluten vs. Placebo
*P‐value for analyses at Week 1 and entire study period
P=.047
50
40
30
20
10
01 2 3 4 5 6
Week
VAS (0‐100 mm)
Overall Symptoms
P=.03150
40
30
20
10
01 2 3 4 5 6
Week
VAS (0‐100 mm)
Bloating
P=.001*
50
40
30
20
10
‐101 2 3 4 5 6
Week
VAS (0‐100 mm)
Tiredness
0
P=.02*
50
40
30
20
10
01 2 3 4 5 6
Week
VAS (0‐100 mm)
Pain
Gluten(n=19)Placebo(n=15)

6/23/2014
5
Biesiekieski; Gastro 2013
No Effect of Gluten on Symptoms
Role of alpha amylase/trypsin inhibitors (ATIs)
Junker Y, et al. J EX Med, 2013
Current Paradigm
Celiac Disease• Innate and adaptive
immune activation• Auto-antibodies• Destructive mucosal
inflammation
IBS•Visceral Hyperalgesia•↑↓ Altered permeability•1◦ Motility disturbance•? Low grade inflammation
NCGS? Gluten related alterations in:• Intestinal permeability
•Motility• Inflammation
•Innate immune activation•Anti‐gliadin antibodies
Altered intestinal microflora

6/23/2014
6
• Less than 300 cases published from referral centers (10% nonresponsive CD)
• Females (2:1), >50 years old• Population-based cohorts
• 5 (0.7%) of 713 CD patients from Derby (UK)• 3 (1.4%) of 204 CD patients from Olmsted County• 8 (1.7%) of 480 CD patients from Boston• Incidence 0.06 (95% CI: 0.0-0.12) per 100,000
persons years
Rubio-Tapia A et al, Gut 2010
West J. Gastroenterology 2009;136:32
Roshan B, Leffler DA et al AJG 2011
Refractory Celiac Disease
Celiac Disease /Type 1 RefractorySprue
Type 2 Refractory sprue
CD3 CD8
Abnormal IELs (CD3+ CD8-) in refractory sprue
Cellier et al, Lancet 2000
Prognosis by Refractory Celiac Disease Classification
Al-toma et al, Gut 2007
Type 1 RCD
Type 2 RCD
De Novo EATL
Secondary EATL

6/23/2014
7
Let Thy Food Be Thy Medicine
• Strict gluten free diet is the only accepted treatment for celiac disease
• The GFD is one of the more challenging treatments we assign patients
• Involves avoidance of all wheat, rye and barley products
• Less than 50 mg of gluten (1/30th of a slice of bread) can cause significant, sustained mucosal inflammation
• Untreated celiac disease increases risk of malignancy, infection, and results in a 2-3 fold increase in mortality
GFD
Hippocrates, 400 AD
Patient Satisfaction with the GFD is Low
• Controversial in the past• Better scientific data and a more diverse
celiac population → general acceptance
Sanders JGLD 2011
Treatment Burden is Second Only to Hemodialysis
*VAS: 0=Very Easy
100=Very Difficult
VAS*
Shah S, Leffler DA, AJG 2014
6/23/2014
8
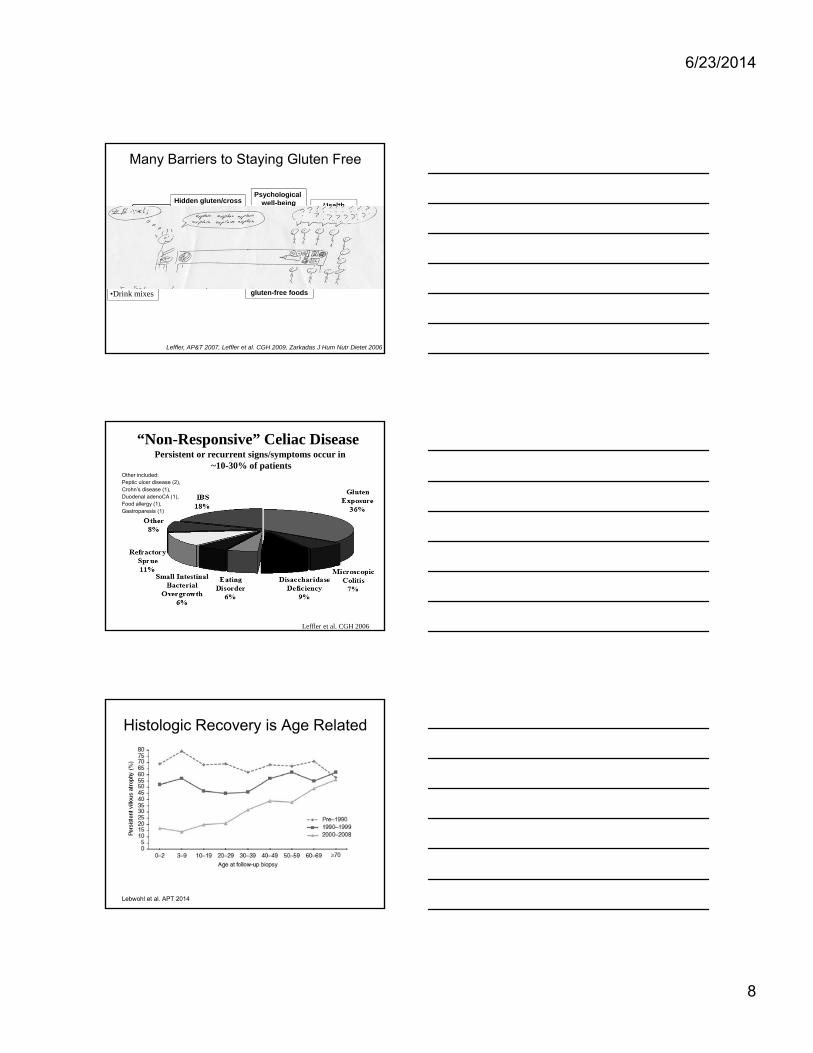
Many Barriers to Staying Gluten Free
Impact
Hidden gluten/cross contamination Health
concerns
Cost
Label readingAccess to
gluten-free foods
Nutritional Content
Social and professional
life
Psychological well-being
Leffler, AP&T 2007, Leffler et al. CGH 2009, Zarkadas J Hum Nutr Dietet 2006
•Medications•Supplements•Processed meats •Frozen Vegetables•Soy Sauce•Seasonings•Drink mixes
Other included: Peptic ulcer disease (2), Crohn’s disease (1), Duodenal adenoCA (1), Food allergy (1), Gastroparesis (1)
Leffler et al. CGH 2006
“Non-Responsive” Celiac DiseasePersistent or recurrent signs/symptoms occur in
~10-30% of patients
Histologic Recovery is Age Related
Lebwohl et al. APT 2014
6/23/2014
9
Current Recommendations for Celiac Monitoring
• Currently: No standard practice regarding need for and timing of clinical, serologic and histologic follow up
• Commonly recommended: – Clinical and serologic follow up Q3-6
months until normal than Q1-2 years
– Histologic follow up: variable from repeat biopsy at 4-6 months to never if clinical and serologic response
– DXA at least once
Available Biomarkers
• Excellent for diagnosis– tTG/DGP are >90% accurate– Biopsy confirmatory– Response to therapy supportive and typical
• Imperfect for monitoring– Drop in serologic titers after diagnosis is helpful– Repeat histology can be reassuring– Symptomatic improvementBUT– Serology and symptoms are not predictive of mucosal
healing– Histologic changes can be patchy and misleading and
have differing responsiveness
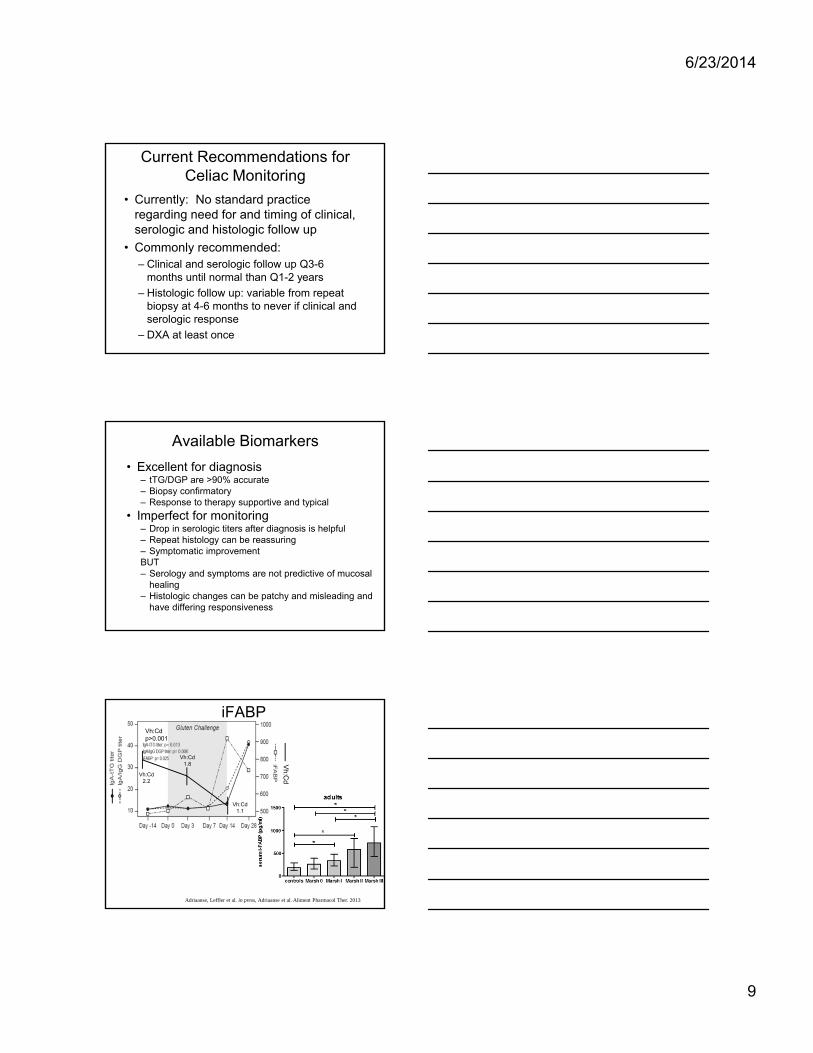
iFABP
Adriaanse, Leffler et al. in press, Adriaanse et al. Aliment Pharmacol Ther. 2013
Vh:Cdp>0.001
Vh
:CdVh:Cd
2.2
Vh:Cd1.8
Vh:Cd1.1
6/23/2014
10
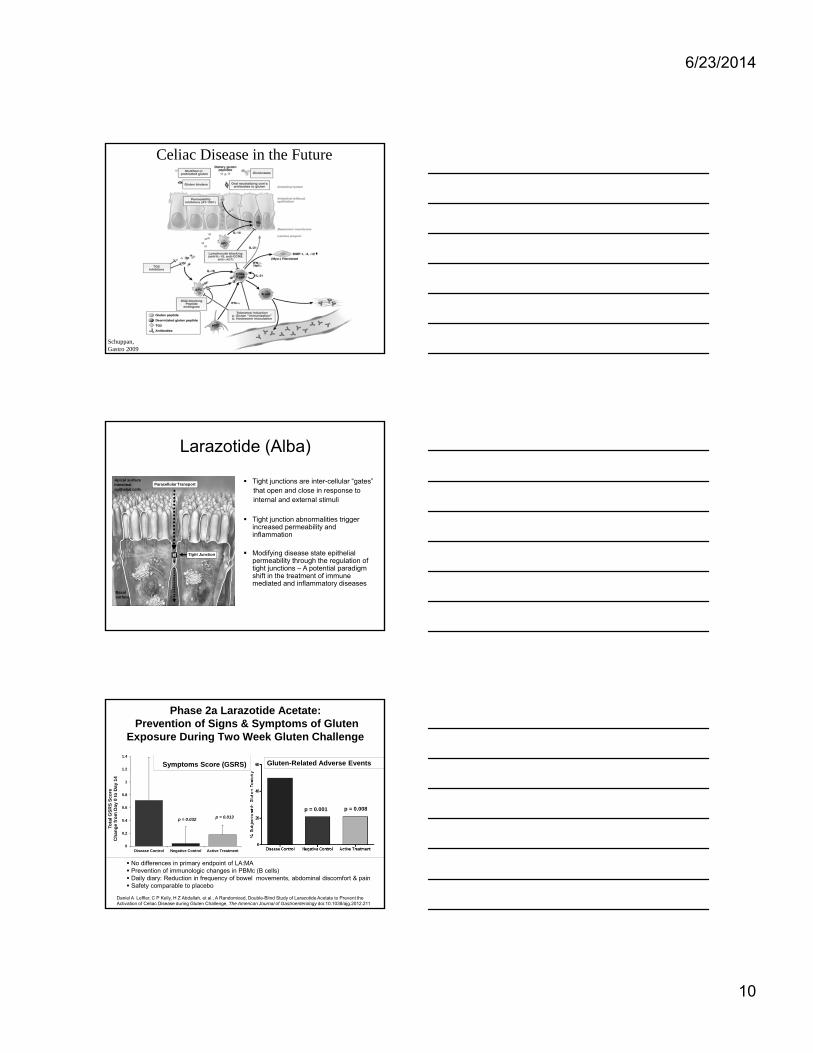
Schuppan, Gastro 2009
Celiac Disease in the Future
Larazotide (Alba)
Tight junctions are inter-cellular “gates” that open and close in response to internal and external stimuli
Tight junction abnormalities trigger increased permeability and inflammation
Modifying disease state epithelial permeability through the regulation of tight junctions – A potential paradigm shift in the treatment of immune mediated and inflammatory diseases
Apical surfaceIntestinal epithelial cells
Basal surface
Tight Junction
Paracellular Transport
Gluten-Related Adverse Events
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Disease Control Negative Control Active Treatment
Tota
l GS
RS
Sc
ore
Ch
an
ge
fro
m D
ay
0 t
o D
ay
14
p = 0.032 p = 0.013
No differences in primary endpoint of LA:MA Prevention of immunologic changes in PBMc (B cells) Daily diary: Reduction in frequency of bowel movements, abdominal discomfort & pain Safety comparable to placebo
Symptoms Score (GSRS)
Phase 2a Larazotide Acetate:Prevention of Signs & Symptoms of Gluten
Exposure During Two Week Gluten Challenge
p = 0.001 p = 0.008
Daniel A Leffler, C P Kelly, H Z Abdallah, et al., A Randomized, Double-Blind Study of Larazotide Acetate to Prevent the Activation of Celiac Disease during Gluten Challenge, The American Journal of Gastroenterology doi:10.1038/ajg.2012.211

6/23/2014
11
ALV-003 (Alvine)
DigestivelyResistant GlutenFragments Gluten Peptide
Processed in the Mucosa
T-Cell ActivationCauses Inflammatory Response
Celiac Specific
Antigen Presentation
Celiac Patient
Immune ReactionCausesInflammation
Normal
No ImmuneReaction
IntestinalMucosa
GLUTENINGESTEDGLUTENINGESTED
11 REACTIONREACTION22
TRIGGERS IMMUNE RESPONSE AMD INFLAMMATION IN SMALL INTESTINETRIGGERS IMMUNE RESPONSE AMD INFLAMMATION IN SMALL INTESTINE
33
Phase 2a ALV-003: Prevention of Gluten Induced Mucosal Injury Exposure During 6 Week Gluten Challenge
Lahdeaho ML, Kaukinen K, et al., Gastro 2014
Nexvax (ImmunosanT)
• Treatment shifts T cells from pro-inflammatory to tolerant response to gluten
• Induces tolerance in a celiac mouse model• Phase 2a trials underway• Nexvax administration → symptoms mimicking
oral gluten exposure
Peptide library:
18,117 12mers
2,922 20mers 3 16AA Proteins
Dominant peptides
6/23/2014
12
Non-Dietary (non-behavioral) Therapies:Transformative for Celiac Disease?
Case Study: Erectile DysfunctionThough 1980 ED was considered an uncommon psychological disorder “all sexual dysfunctions are caused by a single factor: anxiety”
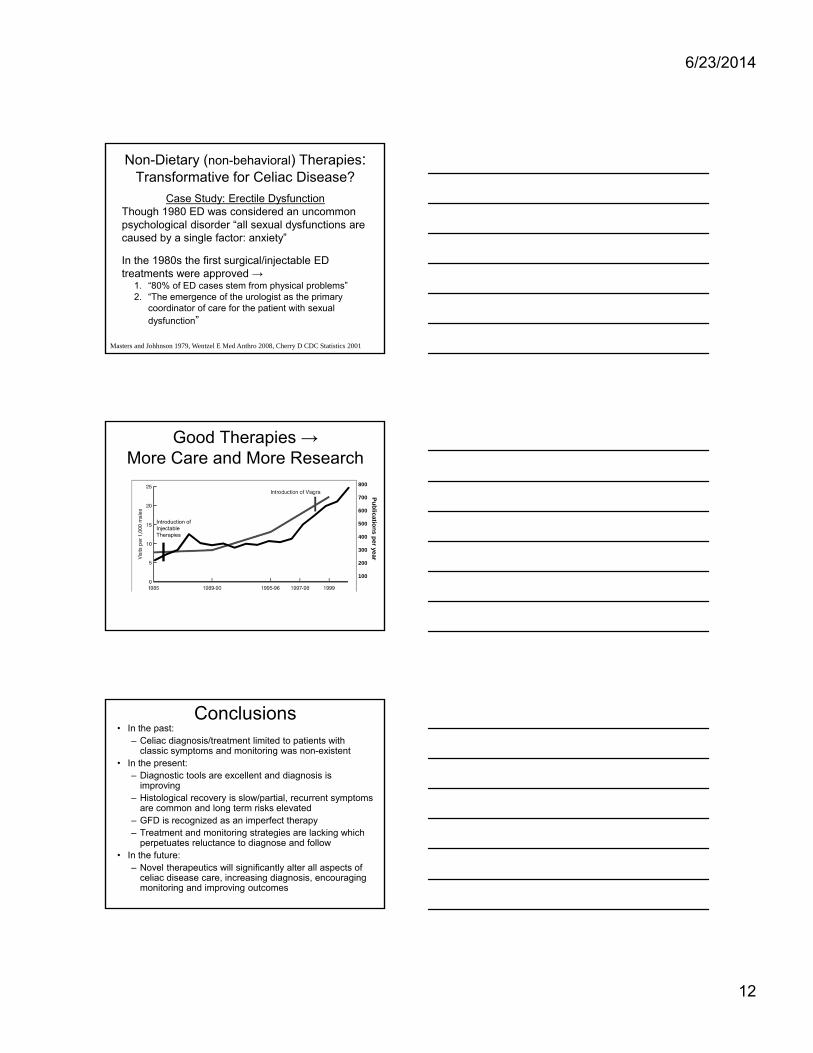
In the 1980s the first surgical/injectable ED treatments were approved →
1. “80% of ED cases stem from physical problems” 2. “The emergence of the urologist as the primary
coordinator of care for the patient with sexual dysfunction”
Masters and Johhnson 1979, Wentzel E Med Anthro 2008, Cherry D CDC Statistics 2001
Good Therapies → More Care and More Research
Introduction of Injectable Therapies
800
700
600
500
400
300
200
100
Pu
blicatio
ns p
er year
Conclusions• In the past:
– Celiac diagnosis/treatment limited to patients with classic symptoms and monitoring was non-existent
• In the present: – Diagnostic tools are excellent and diagnosis is
improving – Histological recovery is slow/partial, recurrent symptoms
are common and long term risks elevated – GFD is recognized as an imperfect therapy– Treatment and monitoring strategies are lacking which
perpetuates reluctance to diagnose and follow• In the future:
– Novel therapeutics will significantly alter all aspects of celiac disease care, increasing diagnosis, encouraging monitoring and improving outcomes
Related Documents









![Pemphigus Herpetiformis [Print] - eMedicine Dermatology Herpetiformis .pdf · • Etiology in the neutrophil-dominant subset of pemphigus herpetiformis includes the following: o In](https://static.cupdf.com/doc/110x72/603eff65c1246c599955258c/pemphigus-herpetiformis-print-emedicine-herpetiformis-pdf-a-etiology-in.jpg)

