,Catecholamine Depletion in Thyrotoxicosis Effect of Guanethidine on Cardiovascular Dynamics By SIDNEY GOLDSTEIN, M.D., AND THOMAS KILLIP III, M.D. AN INTIMATE relationship between the sympathetic nervous system and the cardiovascular effects of thyroid hormone has been extensively documented during the past several decades.'-9 In hyperthyroidism in both man and the experimental animal there is an increased susceptibility to cardiac arrhythmia after parenteral administration of epineph- rine.2 4, 0 The frequent occurrence of atrial fibrillation in patients with thyrotoxicosis in the apparent absence of organic heart disease is well known. In addition, hyperthyroidism enhances the pressor effect of injected epi- nephrine and norepinephrine.7 8 The similarities between the cardiovascular effects of excess thyroid hormone and epi- nephrine administration have stimulated an evaluation of the therapeutic effects of sym- pathetic blockade in hyperthyroidism. Spinal anesthesia has been reported to prevent hy- perkinetic cardiovascular responses during thyroid surgery.'0 Brewster et al.9 showed that injection of procaine into the epidural space in hyperthyroid dogs reduced the ele- vated oxygen consumption, heart rate, cardiac output, and blood pressure to control levels. In the treated animals, infusion of epinephrine and norepinephrine restored the hyperthyroid state. They assumed that the procaine had blocked spinal autonomic outflow and con- cluded that there is an augmentation of the physiologic actions of epinephrine and norepi- nephrine in thyrotoxicosis. From the Department of Medicine, The New York Hospital, Cornell Medical Center, New York, New York. Supported in part by Research Grant HE-07044, from the National Heart Institute, U. S. Public Health Service, and by FR-47, Division of General Medical Sciences, National Institutes of Health. Presented in part before the Thirty-fifth annual Scientific Sessions of the American Heart Association, Cleveland, Ohio, October 26-28, 1962. Circulation, Volume XXXI, February 1965 The advent of newer drugs that inhibit sympathetic adrenergic functions, has prompt- ed their clinical trial in thyrotoxicosis. Reser- pine decreases pulse, blood pressure, basal metabolic rate, and stare in patients with thyrotoxicosis.1" In normal volunteers made hyperthyroid by the administration of tri- iodothyronine, Gaffney and co-workers12 re- ported that oral guanethidine reduced the tachycardia, basal metabolic rate, systolic blood pressure, and tremor without affecting serum cholesterol or weight loss. Similar ef- fects have been observed by others in spon- taneous thyrotoxicosis.13 Hemodynamic data describing the effect of catecholamine depletion in spontaneous hy- perthyroidism in man are scant. DeGroot et al.'4 administered reserpine or guanethidine orally to thyrotoxic patients and found no significant change in basal metabolism or car- diac output although heart rate decreased. The present study was designed to evaluate the effect of parenteral guanethidine on car- diovascular functions in patients with pre- viously untreated thyrotoxicosis. The data show that after the administration of large doses of guanethidine intramuscularly, the elevated heart rate, blood pressure, cardiac output, and cardiac work return toward nor- mal. Although the cardiovascular responses to exercise were reduced after this therapy, the effects of exercise were qualitatively similar to those observed prior to treatment. Materials and Methods Nine patients with previously untreated thyro- toxicosis were admitted to a metabolic ward and maintained on an isocaloric diet. The diagnosis of hyperthyroidism was initially made on clini- cal grounds and was substantiated by elevation of the basal metabolic rate, increased uptake of orally administered tracer doses of 1131, and in- creased serum protein-bound iodine (table 1). Seven of the patients had no evidence of heart 219 by guest on April 17, 2018 http://circ.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

,Catecholamine Depletion in ThyrotoxicosisEffect of Guanethidine on Cardiovascular Dynamics
By SIDNEY GOLDSTEIN, M.D., AND THOMAS KILLIP III, M.D.
AN INTIMATE relationship between thesympathetic nervous system and the
cardiovascular effects of thyroid hormone hasbeen extensively documented during the pastseveral decades.'-9 In hyperthyroidism in bothman and the experimental animal there is anincreased susceptibility to cardiac arrhythmiaafter parenteral administration of epineph-rine.2 4, 0 The frequent occurrence of atrialfibrillation in patients with thyrotoxicosis inthe apparent absence of organic heart diseaseis well known. In addition, hyperthyroidismenhances the pressor effect of injected epi-nephrine and norepinephrine.7 8The similarities between the cardiovascular
effects of excess thyroid hormone and epi-nephrine administration have stimulated anevaluation of the therapeutic effects of sym-pathetic blockade in hyperthyroidism. Spinalanesthesia has been reported to prevent hy-perkinetic cardiovascular responses duringthyroid surgery.'0 Brewster et al.9 showedthat injection of procaine into the epiduralspace in hyperthyroid dogs reduced the ele-vated oxygen consumption, heart rate, cardiacoutput, and blood pressure to control levels.In the treated animals, infusion of epinephrineand norepinephrine restored the hyperthyroidstate. They assumed that the procaine hadblocked spinal autonomic outflow and con-cluded that there is an augmentation of thephysiologic actions of epinephrine and norepi-nephrine in thyrotoxicosis.
From the Department of Medicine, The New YorkHospital, Cornell Medical Center, New York, NewYork.
Supported in part by Research Grant HE-07044,from the National Heart Institute, U. S. Public HealthService, and by FR-47, Division of General MedicalSciences, National Institutes of Health.
Presented in part before the Thirty-fifth annualScientific Sessions of the American Heart Association,Cleveland, Ohio, October 26-28, 1962.
Circulation, Volume XXXI, February 1965
The advent of newer drugs that inhibitsympathetic adrenergic functions, has prompt-ed their clinical trial in thyrotoxicosis. Reser-pine decreases pulse, blood pressure, basalmetabolic rate, and stare in patients withthyrotoxicosis.1" In normal volunteers madehyperthyroid by the administration of tri-iodothyronine, Gaffney and co-workers12 re-ported that oral guanethidine reduced thetachycardia, basal metabolic rate, systolicblood pressure, and tremor without affectingserum cholesterol or weight loss. Similar ef-fects have been observed by others in spon-taneous thyrotoxicosis.13Hemodynamic data describing the effect of
catecholamine depletion in spontaneous hy-perthyroidism in man are scant. DeGroot etal.'4 administered reserpine or guanethidineorally to thyrotoxic patients and found nosignificant change in basal metabolism or car-diac output although heart rate decreased.The present study was designed to evaluatethe effect of parenteral guanethidine on car-diovascular functions in patients with pre-viously untreated thyrotoxicosis. The datashow that after the administration of largedoses of guanethidine intramuscularly, theelevated heart rate, blood pressure, cardiacoutput, and cardiac work return toward nor-mal. Although the cardiovascular responses toexercise were reduced after this therapy, theeffects of exercise were qualitatively similarto those observed prior to treatment.
Materials and Methods
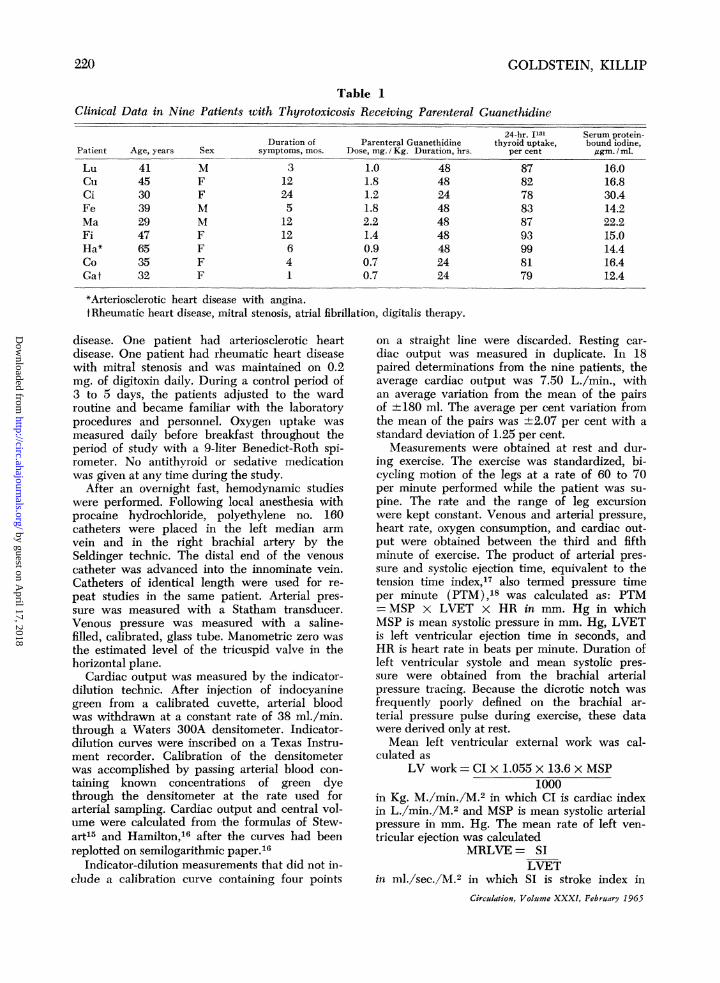
Nine patients with previously untreated thyro-toxicosis were admitted to a metabolic ward andmaintained on an isocaloric diet. The diagnosisof hyperthyroidism was initially made on clini-cal grounds and was substantiated by elevationof the basal metabolic rate, increased uptake oforally administered tracer doses of 1131, and in-creased serum protein-bound iodine (table 1).Seven of the patients had no evidence of heart
219
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from
2DOLDSTEIN, KILLIP
Table 1Clinical Data in Nine Patients with Thyrotoxicosis Receiving Parenteral Guanethidine
Patient
LuCuciFeMaFiHa*CoGat
Duration of Parenteral GuanethidineAge, years Sex symptoms, mos. Dose, mg. i Kg. Duration, hrs.
414530392947653532
MFFMMFFFF
3122451212641
1.01.81.21.82.21.40.90.70.7
484824484848482424
24-hr. I131 Serum protein-thyroid uptake, bound iodine,
per cent jtgm. / ml.
87 16.082 16.878 30.483 14.287 22.293 15.099 14.481 16.479 12.4
*Arteriosclerotic heart disease with angina.tRheumatic heart disease, mitral stenosis, atrial fibrillation, digitalis therapy.
disease. One patient had arteriosclerotic heartdisease. One patient had rheumatic heart diseasewith mitral stenosis and was maintained on 0.2mg. of digitoxin daily. During a control period of3 to 5 days, the patients adjusted to the wardroutine -and became familiar with the laboratoryprocedures and personnel. Oxygen uptake wasmeasured daily before breakfast throughout theperiod of study with a 9-liter Benedict-Roth spi-rometer. No antithyroid or sedative medicationwas given at any time during the study.
After an overnight fast, hemodynamic studieswere performed. Following local anesthesia withprocaine hydrochloride, polyethylene no. 160catheters were placed in the left median armvein and in the right brachial artery by theSeldinger technic. The distal end of the venouscatheter was advanced into the innominate vein.Catheters of identical length were used for re-peat studies in the same patient. Arterial pres-sure was measured with a Statham transducer.Venous pressure was measured with a saline-filled, calibrated, glass tube. Manometric zero wasthe estimated level of the tricuspid valve in thehorizontal plane.
Cardiac output was measured by the indicator-dilution technic. After injection of indocyaninegreen from a calibrated cuvette, arterial bloodwas withdrawn at a constant rate of 38 ml./min.through a Waters 300A densitometer. Indicator-dilution curves were inscribed on a Texas Instru-ment recorder. Calibration of the densitometerwas accomplished by passing arterial blood con-taining known concentrations of green dyethrough the densitometer at the rate used forarterial sampling. Cardiac output and central vol-ume were calculated from the formulas of Stew-art15 and Hamilton,16 after the curves had beenreplotted on semilogarithmic paper.16
Indicator-dilution measurements that did not in-clude a calibration curve containing four points
on a straight line were discarded. Resting car-diac output was measured in duplicate. In 18paired determinations from the nine patients, theaverage cardiac output was 7.50 L./min., withan average variation from the mean of the pairsof +180 ml. The average per cent variation fromthe mean of the pairs was ±2.07 per cent with astandard deviation of 1.25 per cent.
Measurements were obtained at rest and dur-ing exercise. The exercise was standardized, bi-cycling motion of the legs at a rate of 60 to 70per minute performed while the patient was su-pine. The rate and the range of leg excursionwere kept constant. Venous and arterial pressure,heart rate, oxygen consumption, and cardiac out-put were obtained between the third and fifthminute of exercise. The product of arterial pres-sure and systolic ejection time, equivalent to thetension time index,'7 also termed pressure timeper minute (PTM),18 was calculated as: PTM= MSP x LVET x HR in mm. Hg in whichMSP is mean systolic pressure in mm. Hg, LVETis left ventricular ejection time in seconds, andHR is heart rate in beats per minute. Duration ofleft ventricular systole and mean systolic pres-sure were obtained from the brachial arterialpressure tracing. Because the dicrotic notch wasfrequently poorly defined on the brachial ar-terial pressure pulse during exercise, these datawere derived only at rest.Mean left ventricular external work was cal-
culated asLV work = CI x 1.055 X 13.6 x MSP
1000in Kg. M./min./M.2 in which CI is cardiac indexin L./min./M.2 and MSP is mean systolic arterialpressure in mm. Hg. The mean rate of left ven-tricular ejection was calculated
MRLVE= SILVET
in nml./sec./M.2 in which SI is stroke index inCirculation, Volume XXXI, February 1965
220
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from
GUANETHIDINE IN THYROTOXICOSIS
e
uo -_ 1 S..CC
Y4C cz ; 00
A5. o o
II..v
CF !.m6 v
.. Ez -
., -2 bio,v OZ41a (n
-..51m
v,Z: 7. E" -0--!. ", I
En w>, 0cn I.-
4)P.
'It C'O 1- 1-- 1- 10 0 x01- G0 00 01- Co1- 1-
r-
&04z 00 in m m 0
mO
01l V CO 10 10 01l10 0101l
---I -4 --
0 1- 6 10 10: C
Co 00 co 000OCo 00 Co 001--
c0 1- 0N 00 Co 1- coc 1- o _- Cc 'J
---4--I -1 -- -4 -q --4-
00
00O ,^e*1 < CI-m 't 10 Q0 v 111 lq m
~ ~ 0 qcItv_qz ~
X i X^>. Q o O4 1 6 C~4 C C's
CZ-cl
FwtSC t-ttumet0cqts
~ 0 C o c x .
0: 0 C0 00ts N cot- NC001O 1 O mco0 0qC 00o -0 - C'-.E¢ "4c N s 0 0 C
0-
11
C9 C LO Ci NO
C)l '.H*'~_1C 01 _co 4
=^
Ctl
Ci.ci. ca Volume 00 00Fbr C)165
=0 ~ ~~t m~o4
*0o o t-o o ~o0oCli ce C)-o_ _ m CD
r--4
oo0 CD C) oo C)C*
oo o0 o- o o00_ C 00m
-0 0 0 - - C
co 00 - C5D *^ 00 CO
*
101--iCO v co *R oc000s C m 000
** C-
10C _10 t*- * Co1C
10 0 10CD mO Its
-t3--.~-.j,-j.. * * COC
* *o
0 00 ' m "-- 00 cobVm 10 ":t tv m
~~~- -
co o c o00z 00 c co
cq t- d>q 00 m con
- .4 * *
* 0*00c C t-00 c
o 0 0 co co r-
co co It m It** ** *
ol V 10 clc: cq c
00 .l .-- .I CovUtd t- Cq Ut 10 cq
** *
* *
o 0 C * *
** *
00 C_O0t ~-1--0cX
oo O0C'm _ _ 10- 14
8)
-5.U C C04 .0404- X0 00X XX
CC$- 00= W X=P
0 0~0 00~~~~~~~.
221
04
ct
ct
0
i44
CZ
0
CC
-
c)C4C)
4-o
CZ
C)
"0
0
CV
C)
04
C)
04SCC
.C
0CC04
0C)CCS00C)0C)CE0C)C)
00t0400
0 1C)mC) o04vCC *
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from

GOLDSTEIN, KILLIP
Table 3
Indices of Left Ventricular Function, at Rest, and before andThyrotoxicosis
after Guanethidine in Nine Patients with
Ejection time,see.
Before After
Mean rate ventricularejection, ml. / sec. / M. 'Before After
Pressure timemm. Hg
Before After
Ventricular work,Kg. M/min./M.2Beore After
Group ILuCuCiFeMaFi
Group IIHaCoGa
Mean values:Group IGroup IIGroups I & II
0.240.230.220.250.220.28
0.290.280.220.280.280.30
0.22 0.250.23 0.240.19 0.23
0.24*0.210.23
0.28*0.240.26
230230250190200190
180180100
215153194
200180250190200170
220220120
198187194
41.265.956.449.950.950.3
35.242.041.331.536.931.5
47.9 44.840.9 33.953.9 43.8
52.5**47.550.8
36.4**40.837.9
Note: See footnote table 2.*P< 0.05
**P < 0.025***P< 0.001
ml./M.2 and LVET is left ventricular ejectiontime in seconds.
ResultsClinical data and the dose of parenteral
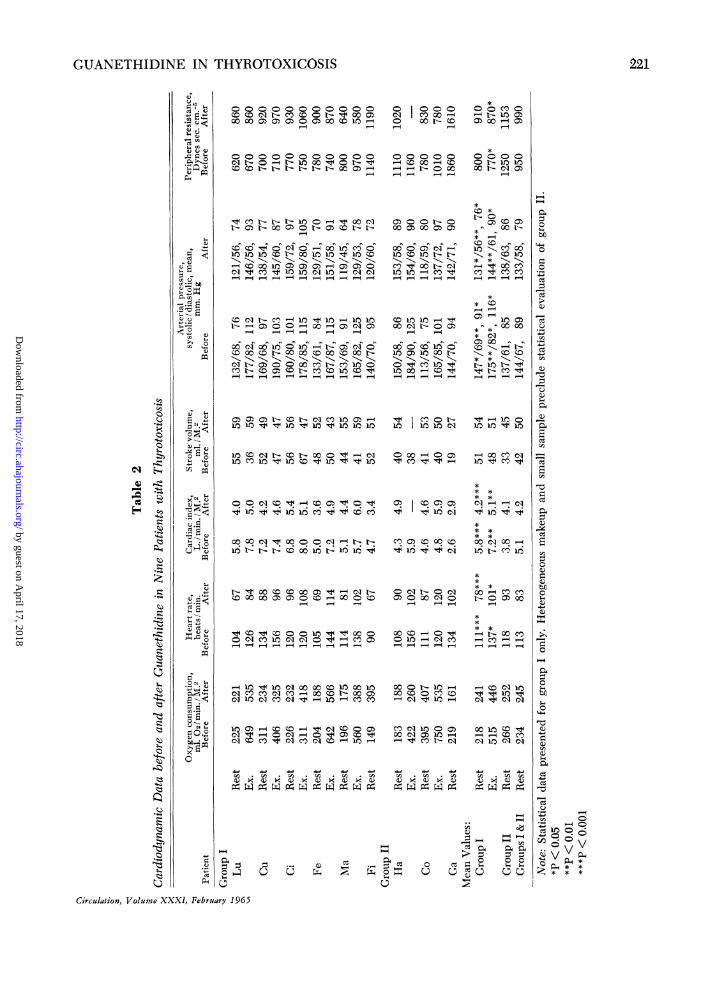
guanethidine for nine patients with previouslyuntreated thyrotoxicosis are recorded in table1. For purposes of analysis the patientshave been divided into two groups. GroupI comprises six patients who received 1.0mg./Kg. or more of guanethidine (total pa-tient dose ranged from 60 to 147 mg.) be-tween the first and second tests. Group II
comprises the three patients who receivedless than 1.0 mg./Kg. of guanethidine (pa-tient total dose ranged from 35 to 42 mg.)before the second set of measurements. Allpatients in group I but one (Ma) devel-oped postural hypotension after guanethidineadministration prior to the second set ofmeasurements. None of the patients in groupII developed postural hypotension. Data ob-tained before and after guanethidine are
presented in tables 2 and 3.
Group I. Data during Rest
Resting oxygen consumption obtained at
the time of the cardiovascular measurements,was not significantly different from the con-
trol values after guanethidine administration,averaging 218 ml./min./M.2 before and 241ml./min./ M.2 after therapy. Daily oxygen con-
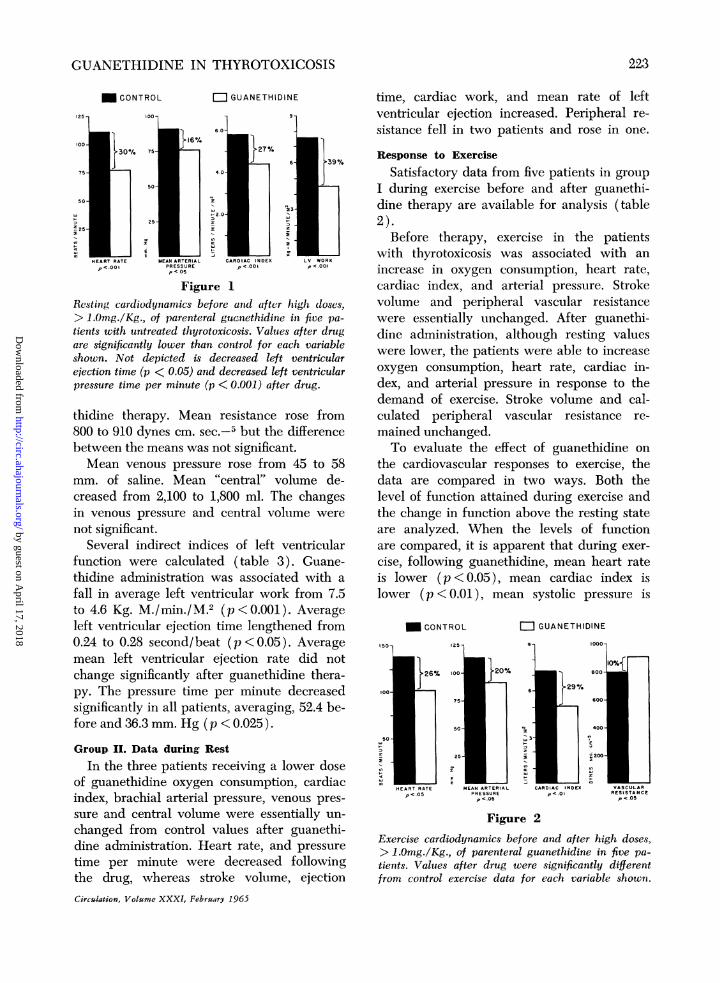
sumptions showed considerable individualvariability, but no trend was apparent eitherbefore or after therapy.Heart rate fell significantly, averaging 111
beats/min. before and 78 beats/min. afterguanethidine (p < 0.001) (fig. 1).Mean, systolic, and diastolic brachial arte-
rial pressures fell significantly with adminis-tration of guanethidine, averaging 91 and147/69 mm. Hg before, and 76 and 131/56mm. Hg after therapy (p<0.05 for systolicand mean, p <0.01 for diastolic pressures ).The average cardiac index decreased sig-
nificantly from a value of 5.8 L./min./M.2before to 4.2 L./min./M.2 after guanethidine(p<0.001). Mean stroke volume index rose
slightly from 51 ml./beat/M.2 to 54 ml./beat/M.2, but the difference between the means
was not statistically significant.Calculated peripheral resistance tended to
rise as the blood pressure fell after guane-
Circulation, Volume XXXI, February 1965
6.410.09.86.06.66.4
5.34.93.5
7.5**4.66.5
4.24.87.53.64.13.5
6.25.33.7
4.6*5.14.8
222
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from
GUANETHIDINE IN THYROTOXICOSIS
CONTROL GUANETHIDINE
125 1 10 75t 9% 9
HEART RATE MEAN ARTERIAL CARDIAC INDEX LV WORK~oool PRESSURE pV<OOi pH<001
Figure 1Resting cardio)dynarnics before and after high doses,> 1.0mg/Kg., of parenteral guanethidine in five pa-tients with untreated thyrotoxicosis. Values after drugare signilficantly lower than control for each variableshown. Not depicted is decreased left ventricularejection time (p < 0.05) and decreased left ventricularpressure time per minute (p <0.001) after drug.
thidine therapy. Mean resistance rose from800 to 910 dynes cm. sec.-6 but the differenceebetween the means was not significant.Mean venous pressure rose fom 45 to 58
mm. of saline. Mean KA etrl" volume de-creased from 2,100 to 1,800 ml. The changesin venous pressure and central volume werenot significant.
Several indirect indices of left ventricularfunction were calculated (table 3). Guane-thidine administration was associated with afall in average left ventricular work from 7.5to 4I.6 Kg. M./min./M ,2 (p<O.OOl ) . Averageleft ventricular ejection time lengthened from0.24 to 0.28 second/beat (p <0.05). Averagemean left ventricular ejection rate did notchange significantly after guanethidine thera-py. The pressure time per minute decreasedsignificantly in all patients, averaging, 52.4 be-fore and 36.3 mm. Hg (p <0.025).
Group. II. Data during RestIn the three patients receiving a lower dose
of guanethidine oxygen consumption, cardiacindex, brachial arterial pressure, venous pres-sure and central volume were essentially un-changed from control values after guanethi-dine administration. Heart rate, and pressuretime per minute were decreased followvingthe drug, whereas stroke volume, ejectionCirculation, Volume XXXJ, Februry 1965
time, cardiac work, and mean rate of leftventricular ejection increased. Peripheral re-sistance fell in two patients and rose in one.
Response to ExerciseSatisfactory data from five patients in group
I during exercise before and after guanethi-dine therapy are available for analysis (table2).
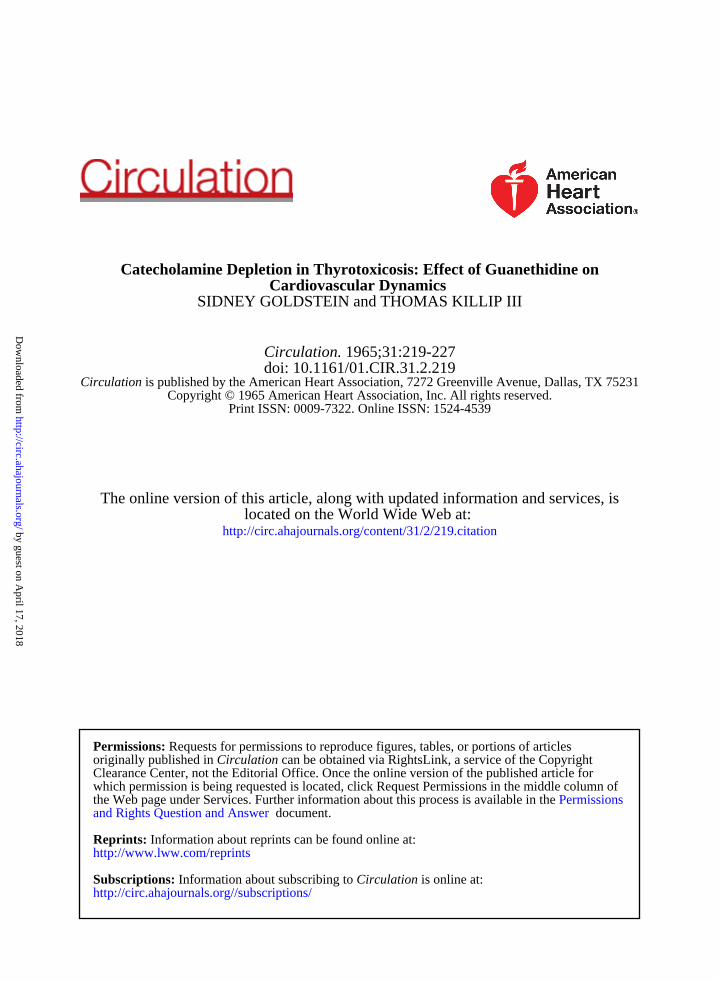
Before therapy, exercise in the patientswith thyrotoxicosis was associated with anincrease in oxygen consumption, heart rate,cardiac index, and arterial pressure. Strokevolume and peripheral vascular resistancewere essentially unchanged. After guanethi-dine administration, although resting valueswere lower, the patients were able to increaseoxygen consumption, heart rate, cardiac in-dex, and arterial pressure in response to thedemand of exercise. Stroke volume and cal-culated peripheral vascular resistance re-mained unchanged.To evaluate the effect of guanethidine on
the cardiovascular responses to exercise, thedata are compared in two ways. Both thelevel of function attained during exercise andthe change in function above the resting stateare analyzed. When the levels of functionare compared, it is apparent that during exer-cise, following guanethidine, mean heart rateis lower (p <0.05), mean cardiac index islower (p <0.01), mean systolic pressure is
M CONTROL
100 2%
75
MEAN ARTERIALPRESSUREp C.05
= GUANETHIDINE
CARDIAC INDEXpc OI
Figure 2Exercise cardiodynamics before and after high doses,> 1.Omg./Kg., of parenteral guanethidine in five pa-tients. Values after drug were significantly differentfrom control exercise data for each variable shown.
223
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from

4GOLDSTEIN, KILLIP
CONTROL GUANETHIDINE
50
40-
301-
200-I
RATE
Figure 3
Changes in cardiodynamics from resting levels duringexercise before and after high doses, > 1.Omg/Kg., ofguanethidine in six patients with untreated thyrotoxi-cosis. Resting (fig. 1) and exercise (fig. 2) indicesof cardiac function are lower after guanethidine.However, the changes from resting level induced dur-ing exercise after the drug are not significantly differ-ent from control for each variable shown.
lower (p <0.01), mean diastolic pressure islower (p < 0.05), average mean arterial pres-
sure is lower (p <0.05), and the calculatedperipheral vascular resistance is higher (p <0.05) than under control conditions (table 2,fig. 2).Comparison of the change in cardiovascular
function induced by exercise before and afterguanethidine reveals, however, that the differ-ences between the mean change in heartrate, oxygen consumption, cardiac index, di-astolic and mean arterial pressure and cal-culated peripheral vascular resistance fromthe resting state are not statistically signifi-cant (fig. 3). These data suggest that guane-thidine does not inhibit a relatively normalqualitative response to exercise in thyrotoxi-cosis.Values measured during exercise are lower
after treatment because function is at a lowerbase. The increment above the base inducedby the exercise is similar before and afterguanethidine (fig. 3).
Satisfactory measurements during exercisewere obtained from only one patient in group
II (table 2).
DiscussionThe cardiovascular alterations found in thy-
rotoxicosis are strikingly similar to the re-sponses following epinephrine administration.Since adrenergic autonomic blockade inhibitsthe hemodynamic alterations of hyperthyroid-ism, it has been postulated that many of theeffects of catecholamines are augmented bythyroid hormone. Wurtman et al. studiedthe distribution and metabolism of catechola-mines in the heart of hyperthyroid rats. Theyfound that the hypertrophied hearts had adecreased ability to inactivate by binding cir-culating epinephrine, which is delivered inlarger amounts than normal because of theshunting of an increased fraction of the cardi-ac output to the myocardium. They concludedthat the increased sensitivity of the cardio-vascular system to epinepbrine in thyrotoxico-sis was due to increased availability of "free"epinephrine to act on physiologic receptors.Whether this mechanism can be invoked inrnan is unclear. Rowe et al.'9 found an identi-cal fractional increase in both coronary andsystemic blood flow in patients with thyro-toxicosis.The present study has shown that depletion
of catecholamines with large doses of guane-thidine partially depresses the hyperkineticcirculation in thyrotoxicosis. The elevatedheart rate, blood pressure, cardiac output,and cardiac work are reduced by the drugin patients with untreated thyrotoxicosis.These observations are in contrast to the effectof guanethidine on normal subjects, in whomonly the pulse rate falls.20 Although the dos-age schedules varied between the presentstudy and Kahler's et al.,20 in both studies thedrug was given to the point of postural hypo-tension, suggesting that maximal doses wereused.The depression of the hyperkinetic circula-
tion in thyrotoxicosis by guanethidine is com-patible with the thesis that many of the car-diovascular effects of excess thyroid hormoneare mediated by catecholamines. Guanethi-dine is a potent adrenergic blocking agentwhich selectively blocks the reflex responsesto sympathetic stimulation, inhibits the up-take of circulating norepinephrine, enhancesthe action of injected catecholamines, releases
Circulation, Volume XXXI, February 1965
224
& CARDIAC NDEX
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from

GUANETHIDINE IN THYROTOXICOSIS
norepinephrine from bound tissue stores, andcauses a slow but continuous release of nor-epinephrine.21 The mechanism responsible forthe guanethidine response in thyrotoxicosismay be (1) blockade of the effect of tonicsympathetic discharge on the heart, (2) re-duction in myocardial catechol content, or(3) reduction of myocardial response to cir-culating catechols.Evidence for a relationship between cate-
cholamines and the metabolic effects of thy-roid hormone is conflicting.22 In the presentstudy guanethidine did not reduce significant-ly the elevated oxygen consumptions. Bothsimilar and opposite results have been re-ported by others. 12, 14, 23 Bray22 found thatreserpine inhibits the oxygen consumption invitro in liver but not in myocardium fromtriiodothyronine-treated rats.One might postulate a reduction in venous
tone (increase in compliance) with venous"'pooling" as partial explanation for the fall incardiac output. Lack of significant changein either "central" volume or venous pressureafter administration of guanethidine arguesagainst such a postulation. In descriptiveterms, cardiac output fell after high doses ofguanethidine because stroke volume remainedunchanged despite the sharp decline in heartrate. Although maximally tolerated doses ofguanethidine were administered, resting car-diac output and stroke volume remained abovenormal, but pulse returned to a normal rate.
Heart rate fell in the patients receivingthe lower doses of guanethidine althoughcardiac output did not change. With higherdoses cardiac output was reduced. Becausethe number of patients studied is small, thedifferences in response must be interpretedwith caution. A two-stage effect, dependingon dosage, may be postulated. Guanethidinehas been shown to block the response tosympathetic stimulation (cardio-acceleratornerve) prior to a reduction in myocardialcatechol content.24 Neither the mechanism ofaction nor the completeness of the catechola-mine depletion can be accurately delineatedfrom the present study.
In normal human subjects, guanethidineCirculation, Volume XXXI, February 1965
impairs the expected increase in cardiac out-put, arterial pressure, and cardiac work dur-ing exercise.20 Despite the high resting values,both cardiac output and heart rate increasedduring exercise prior to therapy in the pa-tients with thyrotoxicosis. After high doses ofguanethidine the resting values were lower,but heart rate and cardiac output still in-creased during exercise by approximately thesame amount as during the control study.These observations suggest that either the de-pletion or blockade caused by guanethidinewas incomplete or that nonadrenergic factorscontinued to sustain cardiac hyperfunctionboth at rest and during exercise.
Guanethidine reduced left ventricular workand the product of mean arterial systolic pres-sure, ejection time, and heart rate. The latterhas been shown to correlate with myocardialoxygen consumption in acute preparations.17' 18A reduction in cardiac work and oxygen de-mand might improve cardiac function in pa-tients with thyrotoxicosis and heart disease.Reversion of atrial fibrillation to sinus rhythmafter guanethidine administration has beenreported.'3
In patients severely ill with thyrotoxicosis,catecholamine depletion may provide imme-diate respite and allow time for standardforms of medical therapy directed towardthyroid hyperfunction itself to become effec-tive. The narrowed arterial-mixed venous oxy-gen difference in thyrotoxicosis indicates thatcardiac output is increased out of proportionto total body metabolic needs. However,splanchnic arteriovenous oxygen differencewidens in thyrotoxicosis despite an increasedsplanchnic blood flow which is not sufficientto meet the increased oxygen demand.25 Cen-tral necrosis of the liver, a sign of hepatic cir-culatory insufficiency,26 has been reported inpatients dying from thyroid storm.25
Guanethidine has been reported to reducethe fraction of systemic blood flow perfusingthe splanchnic bed in hypertensive subjects.27It is possible that in thyrotoxicosis guanethi-dine may reduce blood flow to certain vas-cular beds out of proportion to any change inoxygen demand. Since such an imbalance
225
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from

GOLDSTEIN, KILLIP
may have adverse effects, we suggest thatsympathetic blockade be utilized in thyro-toxicosis with caution.
Summary and Conclusions
The effect of catecholamine depletion oncardiovascular dynamics has been studied innine patients with untreated thyrotoxicosis.Measurements were made at rest and duringexercise before and after large doses of paren-teral guanethidine. Six patients received max-imally tolerated doses of guanethidine (1.0mg./Kg. or more). Three patients receivedlesser amounts.
In the patients receiving the higher doses,heart rate, cardiac index, arterial pressure,left ventricular ejection time, left ventricularpressure time per minute, and left ventricularwork were significantly reduced, from 16 to39 per cent, at rest after guanethidine. Theelevated oxygen consumption was not signifi-cantly changed. Despite maximally tolerateddoses of guanethidine, cardiac index andstroke volume remained above normal, sug-gesting that either catecholamine depletion orblockade was incomplete or that nonadrener-gic factors continued to maintain a hyper-kinetic circulatory state.
In the patients receiving the lower doseof guanethidine heart rate fell, but cardiacindex was not changed.During exercise cardiovascular response was
significantly lower in the patients receivingthe higher doses of guanethidine than con-trol for heart rate, cardiac index and ar-terial pressure; peripheral vascular resistancewas higher. However, the resting values afterdrug therapy were lower, and the changesfrom baseline resting cardiac function inducedby exercise were similar before and afterguanethidine. Hence catecholamine depletiondid not inhibit a relatively normal qualitativeresponse to supine exercise in thyrotoxicosis.The reduction of left ventricular work and
pressure time by guanethidine suggests thatthe drug may be useful as a short-term aid inthe occasional patient with severe heart fail-ure and thyrotoxicosis. A note of caution issounded, however, since it is possible that
guanethidine may reduce blood flow to somevascular beds out of proportion to change inoxygen demand.
AcknowledgmentDr. David V. Becker and Dr. Eugene D. Furth
provided invaluable assistance in the selection, labora-tory evaluation, and management of the patientsreported in this study.
References1. PRIESTLY, J. T., MARKOWITZ, J., AND MANN,
F. C.: The tachyeardia of experimental hyper-thyroidism. Am. J. Physiol. 98: 357, 1931.
2. GOETSCHE, E.: Newer methods in the diagnosisof thyroid disorders: Pathological and clinical.New York State J. Med. 18: 259, 1918.
3. SAWYER, M. E. M., AND BROWN, M. G.: Theeffect of thyroidectomy and thyroxine on theresponse of the denervated heart to injectedand secreted adrenine. Am. J. Physiol. 110:620, 1935.
4. MCDONALD, C. H., SHEPEARD, W. L., GREEN,M. F., AND DEGROAT, A. F.: Response of thehyperthyro.d heart to epinephrine. Am. J.Physiol. 112: 227, 1935.
5. BARKER, S. B., FAZIKAS, J. F., AND HIMwIcH,H. E.: Metabolic aspects of thyroid-adrenalinterrelationship. Am. J. Physiol. 115: 415,1936.
6. RoSENBLum, H., HAHN, R. G., AND LEVINE,S. A.: Epinephrine: Its effect on the cardiacmechanism in experimental hyperthyroidismand hypothyroidism. Arch. Int. Med. 51: 279,1933.
7. SCHNECKLOTH, R. E., KURLAND, G. S., ANDFREEDBERG, A. S.: Effect of variation in thy-roid function on the pressor response to nor-epinephrine in man. Metabolism 2: 546, 1953.
8. WURTMAN, R. J., KOPIN, I. J., AND AXELROD,J.: Thyroid function and the cardiac disposi-tion of catechol amines. Endocrinology 73:63, 1963.
9. BREWSTER, W. R., JR., ISAACS, J. P., OSGOOD,P. F., AND KING, T. L.: The hemodynamicand metabolic interrelationships in the activ-ity of epinephrine, norepinephrine and thethyroid hormones. Circulation 13: 1, 1956.
10. KNIGHT, R. T.: The use of spinal anesthesia tocontrol sympathetic over activity in hyper-thyroidism. Anesthesiology 6: 225, 1945.
1 1. CANARY, J. J., SCHAAF, M., DUFFY, B. J., JR.,AND KYLE, L. H.: Effects of oral and intra-muscular administration of reserpine in thyro-toxicosis. New England J. Med. 257: 435,1957.
12. GAFFNEY, T. E., BRAUNWALD, E., AND KAHTLER,R. L.: Effects of guanethidine on tri-iodothy-
Circulation, Volume XXXI, February 1965
1226
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from

GUANETHIDINE IN THYROTOXICOSIS
ronine-induced hyperthyroidism in man. NewEngland J. Med. 265: 16, 1961.
13. LEE, W. Y., BRONSKY, D., AND WALDSTEIN, S. S.:Studies of thyroid and sympathetic nervoussystem interrelationships. II. Effects of guane-thidine on manifestations of hyperthyroidism.J. Clin. Endocrinol. 22: 879, 1962.
14. DEGROOT, W. J., LEONARD, J. J., PALEY, H. W.,JOHNSON, J. E., AND WARREN, J. V.: The im-portance of autonomic integrity in maintainingthe hypercirculatory dynamics of human hyper-thyroidism. Abstract, J. Clin. Invest. 40:1033, 1961.
15. STENVART, G. N.: The pulmonary circulationtime, the quantity of blood in the lungs andthe output of the heart. Am. J. Physiol. 58:20, 1921.
16. KINSMAN, J. M., MOORlE, J. W., AND HAMILTON,W. F.: Studies on the circulation. I. Injectionmethod: physical and mathematical consider-ations. Am. J. Physiol. 89: 322, 1929.
17. SARNOFF, S. J., BRAUNWALD, E., WELCH, G. H.,JR., CASE, R. B., STAINSBY, W. N., AND MA-cRuz, R.: Hemodynamic determinants ofoxygen consumption of the heart with specialreference to the tension-time index. Am. J.Physiol. 192: 148, 1958.
18. NEILL, W. A., LEVINE, H. J., WAGMAN, R. J.,AND GORLIN, R.: Left ventricular oxygenutilization in intact dogs: Effect of systemichemodynamic factors. Circulation Research 12:163, 1963.
19. ROWE, G. G., HuSTON, J. H., WEINSTEIN, A. B.,TUCHMAN, H., BROWN, J. F., AND CRUMPTON,C. W.: The hemodynamics of thyrotoxicosisin man with special reference to coronary
blood flow and myocardial oxygen metabol-ism. J. Clin. Invest. 35: 272, 1956.
20. KAHLER, R. L., GAFFNEY, T. E., AND BRAUNWALD,E.: The effects of autonomic nervous systeminhibition on the circulatory response to mus-cular exercise. J. Clin. Invest. 41: 198, 1962.
21. AXELROD, J.: The formation, metabolism, uptakeand release of noradrenaline and adrenaline.In Varley, H. and Gowenlock, A. H., ed. TheClinical Chemistry of Monamines. Amster-dam, Elsevier 1963, p. 5.
22. BRAY, G. A.: Studies on the interactions of thy-roid hormone and catecholamines. J. Clin.Invest. 43: 285, 1964.
23. DEGROOT, W. J., LEONARD, J. J., AND KROET:Z,F. W.: The role of catechol amines as media-tors of thyroid hormone activity. Abstract,Program of the Annual Meeting of the Ameri-can Thyroid Association, 1962, p. 22.
24. GAFFNEY, T. E., CHIDSEY, C. A., AND BRAUN-WALD, E.: Study of the relationship betweenthe neurotransmitter store and adrenergicnerve block induced by reserpine and guane-thidine. Circulation Research 12: 264, 1963.
25. MYERS, J. D., BRANNON, E. S., AND HOLLAND,B. C.: A correlatIve study of the cardiac out-put and the hepatic circulation in hyper-thyroidism. J. Clin. Invest. 29: 1069, 1950.
26. KILLIP, T., III, AND PAYNE, M. A.: High serumtransaminase activity in heart disease. Circula-tory failure and hepatic necrosis. Circulation21: 646, 1960.
27. COHN, J. N., LIPTAK, T. E., AND FREis, E. D.:Hemodynamic effects of guanethidine in man.Circulation Research 12: 298, 1963.
The History of Science
They that know the entire course of the development of science will, as a matter ofcourse, judge more freely and more correctly of the significance of any present scien-tific movement than they, who limited in their views to the age in which their ownlives have been spent, contemplate merely the momentary trend that the course ofintellectual events takes at the present moment.-ERNST MACH in Science of Mechanics.
Circulation, Volume XXXI, February 1965
227
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from
SIDNEY GOLDSTEIN and THOMAS KILLIP IIICardiovascular Dynamics
Catecholamine Depletion in Thyrotoxicosis: Effect of Guanethidine on
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1965 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.31.2.219
1965;31:219-227Circulation.
http://circ.ahajournals.org/content/31/2/219.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on April 17, 2018
http://circ.ahajournals.org/D
ownloaded from
Related Documents