Inpatient falls and their severity Oct 08 - Sep 09 Degree of harm Acute Mental Health Community Total No Harm 143,591 19,470 24,614 187,675 Low 57,306 15,194 12,047 84,547 Moderate 6,596 1,687 1,785 10,068 Severe 777 124 164 1065 Death 68 7 8 83 Total 208,338 36,482 38,618 283,438 National Patient Safety Agency 2010 Context – falls in hospital

Case study on a fall: dealing with incidents, claims and inquests in an ageing society - Elderly care conference 2015, Jonathan Treml
Jul 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
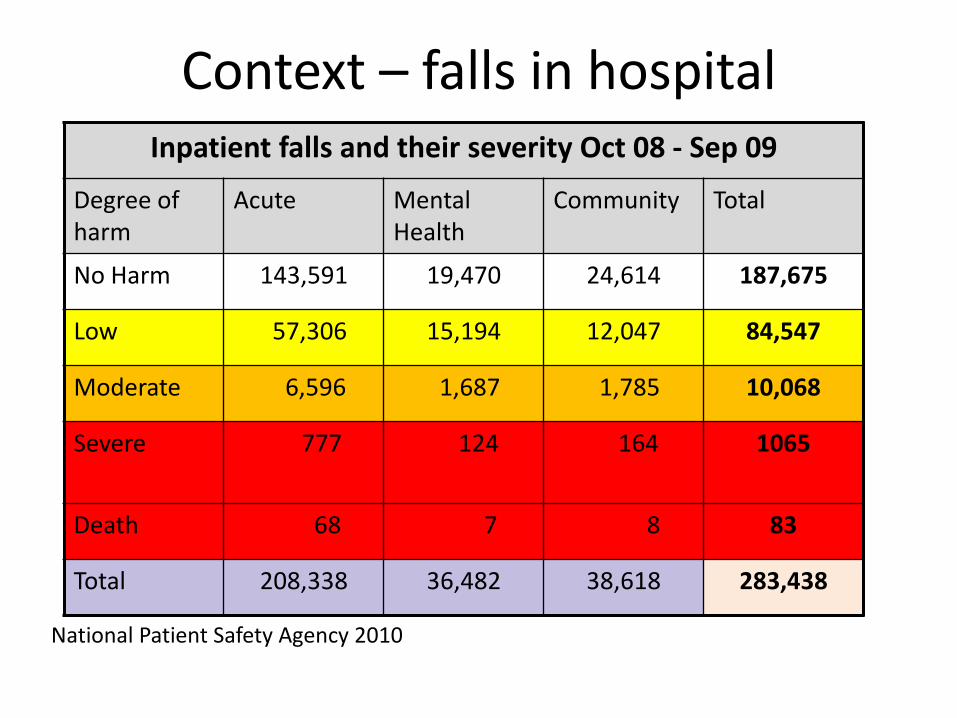
Inpatient falls and their severity Oct 08 - Sep 09
Degree of harm
Acute Mental Health
Community Total
No Harm 143,591 19,470 24,614 187,675
Low 57,306 15,194 12,047 84,547
Moderate 6,596 1,687 1,785 10,068
Severe 777 124 164 1065
Death 68 7 8 83
Total 208,338 36,482 38,618 283,438
National Patient Safety Agency 2010
Context – falls in hospital

1390 fractures (including 840 hip fractures) + 30 brain injuries

Medical Report on the late Mr EH
At the request of HM Coroner, I was asked to review the case of EH and to provide an independent medical opinion regarding the cause of EH’s death on 16/10/2012.
I was specifically asked to consider whether the District General Hospital (DGH) had taken all reasonable steps to minimise the risk of EH suffering a fall and injury while in hospital.
Summary of case

Background
EH was an 82-year-old man with a past history of: • bladder cancer with recent radiotherapy (2012) • TURP for benign prostatic hypertrophy (2011) • amaurosis fugax (2005) • pulmonary tuberculosis (1981) • hearing impairment • hypertension • hypercholesterolemia • impaired glucose tolerance
Background
Regular medications
• pravastatin
• aspirin
• tamsulosin
• solifenacin
He lived at home with his wife. Mobile, no carers

Background
• EH had a previous admission to DGH in November 2010 with a fall, external head injury and delirium
• He also had falls at home requiring calls to the ambulance service in October 2011 and 28/09/12
02/10/12 – Falls, new confusion
EH was seen at home as an emergency by a
nurse practitioner
• He was confused, had suffered falls and was struggling with incontinence and urinary frequency
• He was referred to the district nurses and started on oral antibiotics

05/10/12 – Worsening confusion
• EH was reported to have pain on passing urine and GP prescribed tramadol for pain
• District nurses reported that EH’s wife was not able to cope with his increased confusion and was worried he might fall
• District nurses requested admission to a GP-led intermediate care centre (ICC)
06/10/12 – Admission to ICC
• Change of antibiotics for a presumed UTI
• Add paracetamol and dihydrocodeine for pain
• 40 mg enoxaparin for DVT prophylaxis
• EH was in a bed with ‘cot sides’ (bed rails)
• Constipation, treated with laxatives
08/10/12 – Transfer to DGH
• EH increasingly confused and unwell
• Referred from ICC for admission to DGH
• Transfer document from ICC summarised EH’s condition and care
• In particular, it records that EH had ‘cot sides’ (bed rails) in place, that he may require a low bed and that he had experienced one fall in the last 6 months
Seen by junior doctor
• History of intermittent and worsening confusion, dysuria and constipation
• On examination - drowsy, confused and having occasional hallucinations
• Clinically dehydrated, low oxygen levels and increased respiratory rate
• Abbreviated mental test score 8/10
• No evidence of weakness in any limbs
Seen by junior doctor
• Working diagnosis was of acute confusion/ delirium and acute kidney injury, possibly due to urinary or respiratory infection
• Intravenous antibiotics and fluids
• Oxygen
• Laxatives
• 40 mg enoxaparin was prescribed
• (20 mg subsequently given due to renal function)

On-call Consultant review
• No additional information
• Plan to repeat bloods after 24h treatment
• Consider CT scan of head if not improving
Review on ward
• Confused and agitated
• 2.5 mg haloperidol intramuscularly
• Continue treatment as agitation permits
• Critical care outreach review

First night
• Abnormal ECG, possibly acute coronary syndrome
• 300 mg aspirin, 200 mg clopidogrel
• Transferred to Coronary Care
– All single room accommodation
– Incomplete use of trust falls care bundle
• Consultant Cardiologist review in morning
• Surgical review due to ?bowel obstruction
Second night
• Confused and agitated, removing monitoring leads and urosheath
05:30 – Fall reported ?witnessed by one nurse
On floor face down, cut on nose, black eye
06:00 – seen by doctor on-call
Half-hourly neurological observations advised
08:30 – Reduced level of consciousness,
right-sided weakness
10:10 - CT scan of head
• An acute sub-dural intracranial haematoma adjacent to the falx cerebri, falx cerebella and cerebral hemisphere on the left and causing mass effect
• Also external bruising on the right frontal region of the scalp, a nasal fracture and blood in the left maxillary sinus
• No sign of any chronic sub-dural haematoma
Transfer to Critical Care
• Intubated and ventilated
• Neurosurgical advice was obtained from the regional centre
• Decision that surgical intervention would not improve EH’s outcome and he was treated conservatively
• Extubated later that day
• Family told that “the bleed may have caused the fall”
Final days
• Remained comatose
• Became febrile, chesty
• Clinical diagnosis of bronchopneumonia
• Treated symptomatically, no antibiotics
16/10/12 – EH died in the presence of his wife
• Case referred to Coroner

Autopsy report
• Bronchopneumonia, considered to be the terminal event
• External head injuries consistent with the fall described on 10/10/12
• Traumatic subdural haematoma with compression of the underlying brain
• Severe atheroma of the coronary arteries
• Dilated, infected gallbladder
• Scarring consistent with treated bladder cancer
For discussion
• Could the fatal fall have been prevented?
• What is reasonable practice in reducing falls risk?
• Should ‘blood-thinning’ medication be used in patients with increased falls risk?
• Was the use of 2.5 mg haloperidol important?
• Should bed rails have been used?
• What will the Coroner conclude?
Summary of NICE Clinical Guideline 161 (June 2013)
• Do NOT screen/stratify for falls risk
• Assessment for falls risk factors and targeted interventions on • All patients aged 65+
• Patients aged 50-64 clinically judged to be at high risk of falling
Assess for:
• cognitive impairment
• continence problems
• falls history and fear of falling
• footwear that is unsuitable or missing
• health problems that may increase falls risk
• medication
• postural instability, mobility, balance problems
• syncope syndrome
• visual impairment

• Multifactorial interventions – Targeted to risk factors
• “Promptly” address the patient's identified individual risk factors for falling in hospital
• Take into account whether the risk factors can be treated, improved or managed during the patient's expected stay • i.e. Providing a walking aid – Yes
Delivering a 12+ week exercise programme - No

The verdict
Accidental death

Thank you
Related Documents




![Inquests arising from the deaths in the Westminster Terror ... · 10/4/2018 · October 4, 2018 Inquests arising from the deat [...] Terror Attack of 22 March 2017 Day 17.2 1 2 3](https://static.cupdf.com/doc/110x72/5f9648de9dac984bdf54a69e/inquests-arising-from-the-deaths-in-the-westminster-terror-1042018-october.jpg)






