CASE PRESENTATION Presented by: Dr Nitha George

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CASE PRESENTATION
Presented by: Dr Nitha George
Ajjaiah
14yrs
Male
Hindu
Student (9th grade)
Holakere, Chitradurga

CHIEF COMPLAINTS
Right ear discharge since 3 years
HISTORY OF PRESENTING ILLNESS
Right ear discharge
Since 3years
Insidious in onset
Intermittent ( one episode per month)
Each episode last for 5-7 days
Moderate amount, sticky white with yellow tinge, foul
smelling, not blood stained
Aggravated with episodes of common cold
Relieved with oral medications (details unavailable)
Last episode 1week back lasting for 3days
Relieved temporarily with oral medications

Decreased hearing in right ear
Since 3years
Following onset of right ear discharge
Insidious in onset
Gradually progressive
Was able to appreciate whispers well 3yrs back
At present can only perceive loud noises in right ear
Hearing worsens during episodes of active discharge

Ringing sensation of right ear since 3 years
Insidious in onset
Intermittent
Low pitched humming voice
Lasting throughout the episode of discharge
Aggravated during active discharge and relieved with its
resolution.

No h/o
Fever
Headache / vomiting
Unconsciousness / Neck stiffness
Earache
Visual disturbances
Speech problems
No h/o postaural swelling associated with fever
No h/o
Giddiness
Deviation of angle of mouth
No h/o trauma
Not h/o excessive sneezing/ excessive nasal discharge / postnasal drip/ bleeding from nose/ facial pain.

PAST HISTORY
Chronic adenotonsillitis for which he underwent
ADENOTONSILLECTOMY under general anaesthesia on
3/6/2013
No history of:
Prolonged hospital admissions
Juvenile DM / HTN
Allergy / Bronchial asthma / TB
Previous blood transfusions / drug allergies
Epilepsy

TREATMENT HISTORY
Used oral medications every month for one week during
episodes of ear discharge (Details not available)
One week of postop medications last week
T. Cefpodoxime 100mg BD for 5days
Analgesic Syrup (Aceclofenac 50mg and paracetamol 100mg)10ml
BD

FAMILY HISTORY
No similar complaints in the family

PERSONAL HISTORY
Appetite: Good
Diet: Mixed
Bowel and bladder : Regular
Sleep: Adequate
Habits -Nil
GENERAL EXAMINATION
14yr old male pt
Moderately built n nourished
Conscious, cooperative and well oriented to time, place
and person.
Vitals
Afebrile
BP : 100 / 70mm Hg
PR : 76 bpm
RR : 16/min
Pallor
Icterus
Cyanosis
Clubbing
Lymphadenopathy
Pedal edema
NIL

SYSTEMIC EXAMINATION
CVS : S1 S2 +
No murmers
RS: Bilateral NVBS
No added sounds
P/A: Soft, non tender
No organomegaly
CNS:
Normal
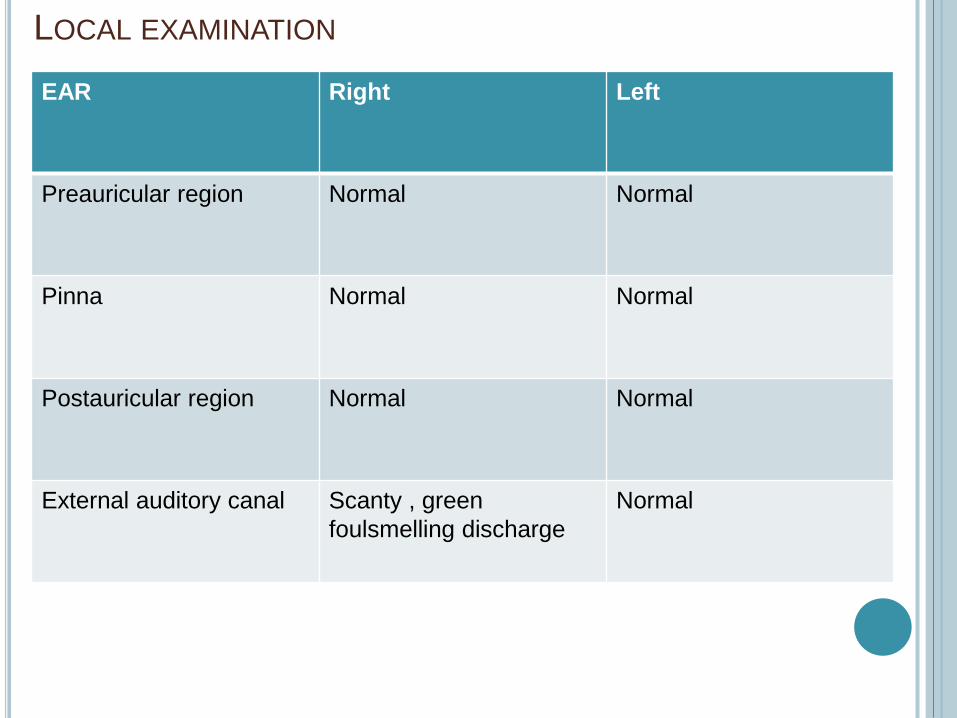
LOCAL EXAMINATION
EAR Right Left
Preauricular region Normal Normal
Pinna Normal Normal
Postauricular region Normal Normal
External auditory canal Scanty , green
foulsmelling discharge
Normal
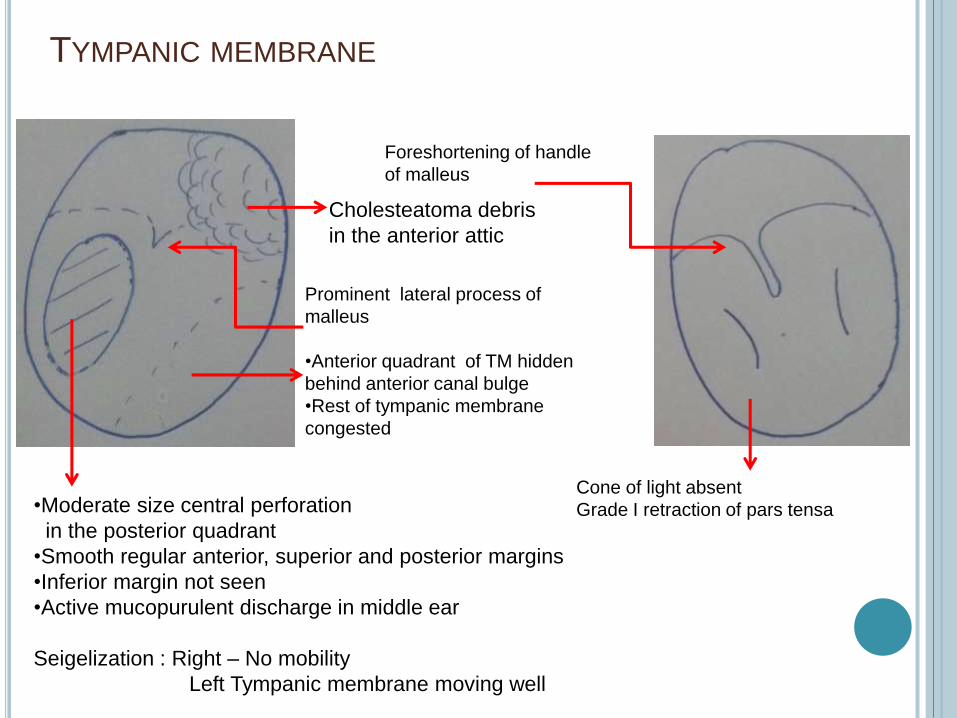
TYMPANIC MEMBRANE
Seigelization : Right – No mobility
Left Tympanic membrane moving well
Cholesteatoma debris
in the anterior attic
•Moderate size central perforation
in the posterior quadrant
•Smooth regular anterior, superior and posterior margins
•Inferior margin not seen
•Active mucopurulent discharge in middle ear
Cone of light absent
Grade I retraction of pars tensa
Prominent lateral process of
malleus
•Anterior quadrant of TM hidden
behind anterior canal bulge
•Rest of tympanic membrane
congested
Foreshortening of handle
of malleus
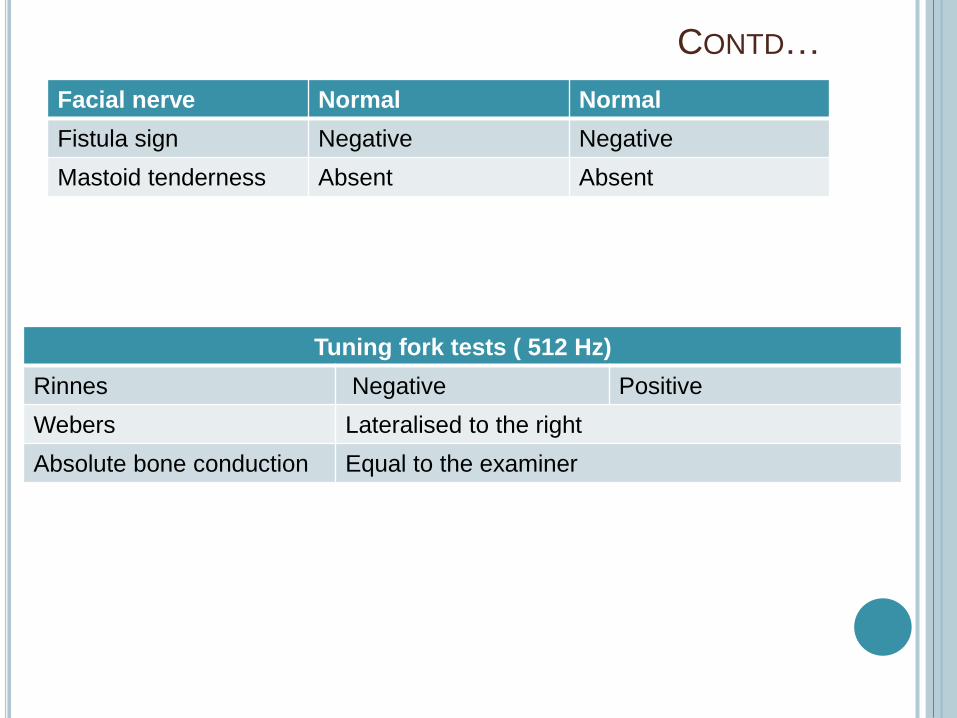
CONTD…
Facial nerve Normal Normal
Fistula sign Negative Negative
Mastoid tenderness Absent Absent
Tuning fork tests ( 512 Hz)
Rinnes Negative Positive
Webers Lateralised to the right
Absolute bone conduction Equal to the examiner
NOSE
External appearance: Normal
Vestibule : Normal
Anterior rhinoscopic examination:
Mucosa normal
Septum normal with septal spur on left side
Lateral wall –HIT
Floor - Normal
Cold spatula test : Bilaterally equal fogging
Paranasal sinus : Non tender
PRE : Normal

ORAL CAVITY
Normal

OROPHARYNX
Posterior pharyngeal wall : Normal
Indirect laryngoscopy: Normal
NECK:
Bilateral jugulodigastric lymph nodes palpable
Right Left
Anterior pillar Normal Normal
Tonsil Healthy tonsillar fossae
Posterior pillar Normal Normal
Right Left
2 in number
2*1 cms each
2 in number
2*1 cms each
Non tender , firm , mobile

PROVISIONAL DIAGNOSIS
Right chronic otitis media, active squammous , with
conductive hearing loss without any complications
with bilateral hypertrophy of inferior turbinates.

INVESTIGATIONS
Otoscope
Otomicroscopy
PTA:
Right 66.6db (Moderately severe CHL)
Left 21.66 db
Xray B/L mastoid (Schullers view)
Xray PNS (Waters view)
Blood
Urine routine
ECG
Chest Xray PA view

FURTHER MANAGEMENT
Tympanoplasty with intact canal wall / canal wall
down mastoidectomy (intraop )
THANK YOU
Related Documents











