Case Presentation: Antenatal USS significance? By Thomas Cromarty ST2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Case
Presentation:
Antenatal USS
significance? By
Thomas Cromarty
ST2

Introduction
Case Presentation
South Africa bites to break it up
Topic learning
Summary


Background 35+3, Primigravida
SROM 36hrs
Steroids (bethamthosone) 2nd dose 13.3 0500
Born @ 2249
Grade I Meconium
No maternal High Temp/Tacchycardia
Mat WCC 21.6, CRP 49. (Erythromycin PO x2)
CMV and CF negative
A/N Bloods – Rubella susceptible (otherwise NAD)
Mum non smoker, no alcohol
Asthma
Surestart
Background

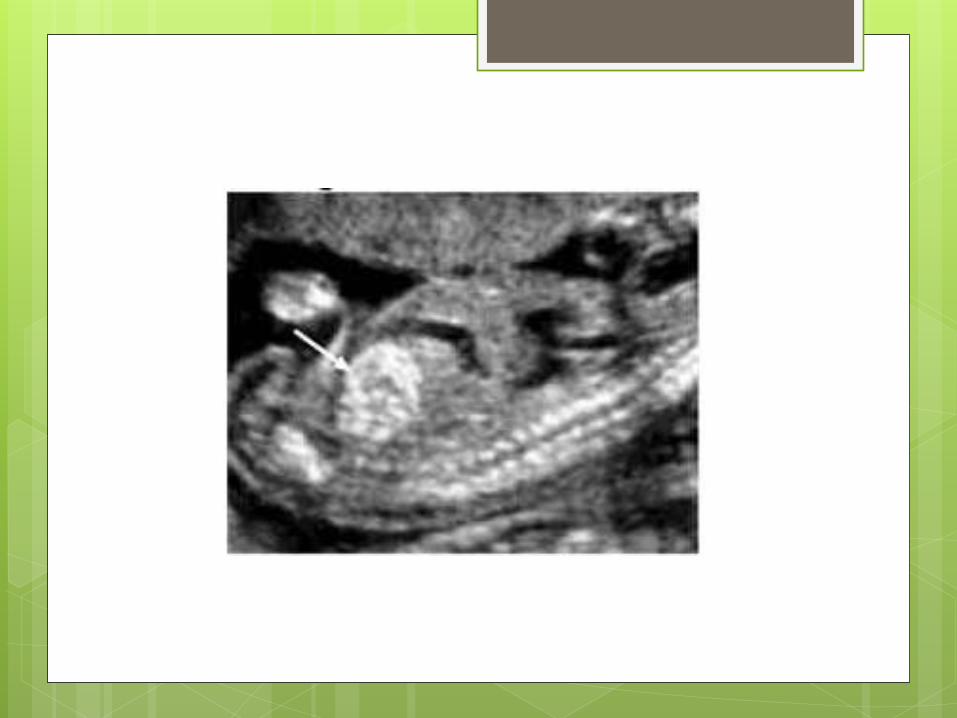
Antenatal Scans 25week
Dilated loop of bowel with maximum diameter of 14mm
Some echogenic bowel noted
31week
Normal growth
No polyhydramnios
Bowel dilation 10.9mm Some areas of echogenic bowel
EDF +ve
Due to see the surgeons on Monday and fetal medicne @ 36 weeks
Delivery
Born by SVD in a good condition
No resus required
HR>100 throghout
Regular Respiration <1min
Normal palate, anus, spine
PREM, PROM, Raised Mat CRP
IV ABX for presumed sepsis
LBW and Mec obs

GI Management
Neonatal and SHO & Reg reviewed Hx
No documentation of FU/Mx
Reg discussed with Surgical Reg ~ 00.00
Continue with normal neonatal care
Feed early as per usual
No dysmorphic features

Transitional Care Unit Day 1
Feeding well via bottle, some small vomits
PU
Otherwise examines well systemically
Soft, non distended, non tender, BS +ve
R/v at 24 hours old Completed hypoglycaemia protocol
3 hourly bottle feeds, few small vomits
NBO
Normal examination
TCU
Day 2 (36 hours of age)
NBO
1x green vomit
Vomiting after each feed (milky)
Abdo exam
?tinkling bowel sounds?
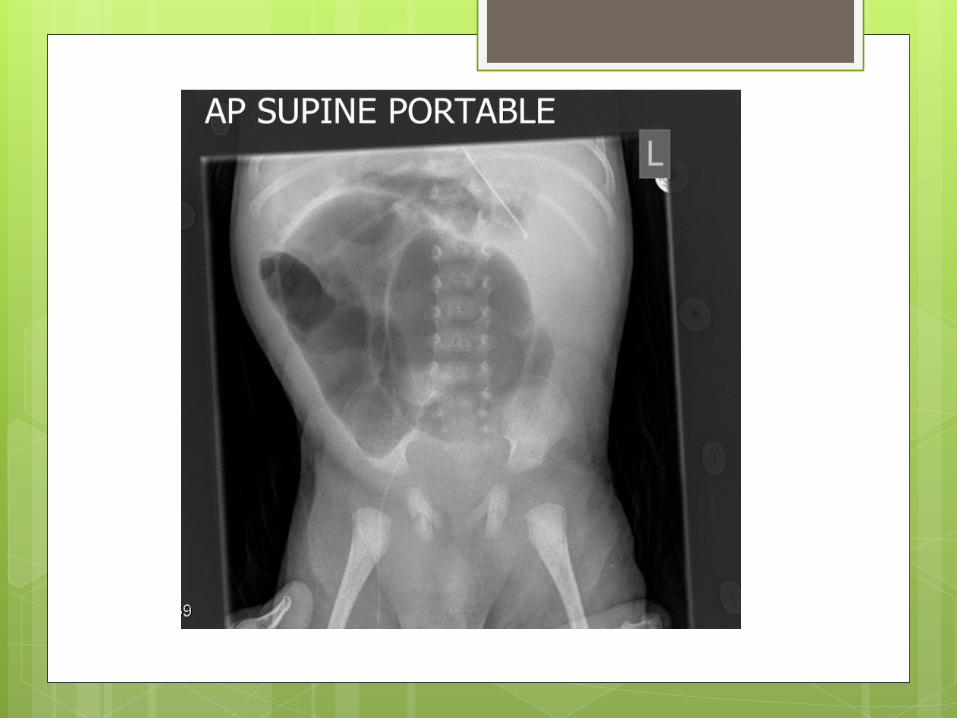
AXR @ 37 hours age
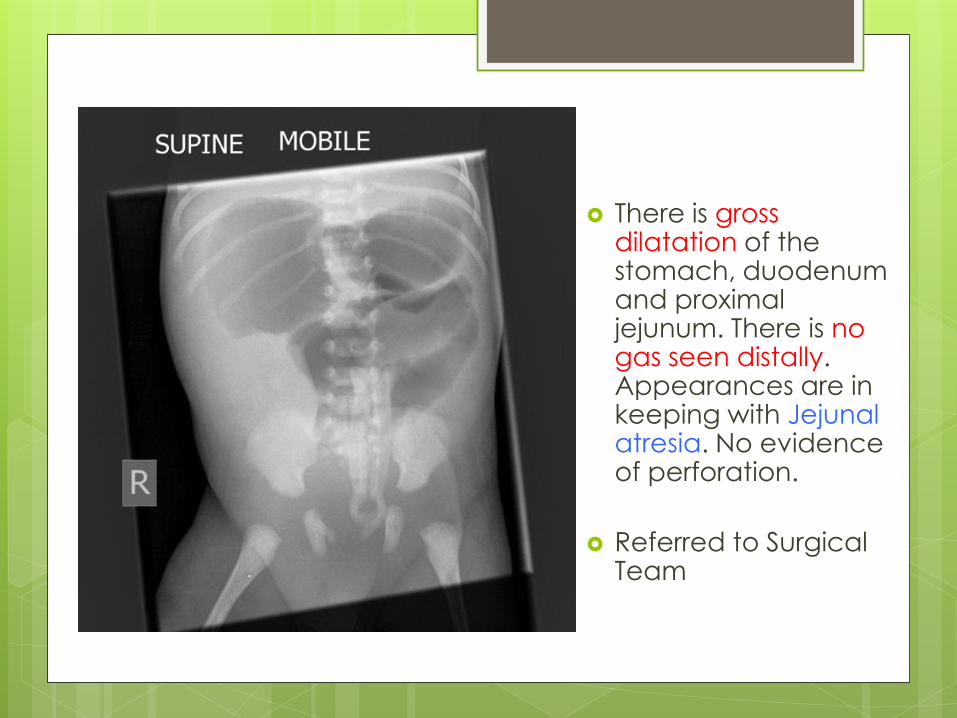
There is gross dilatation of the stomach, duodenum and proximal jejunum. There is no gas seen distally. Appearances are in keeping with Jejunal atresia. No evidence of perforation.
Referred to Surgical Team
Day 2
Admitted to SCBU @ 40 hours of age.
NBM
NGT on free drainage
Surgical r/v
Day 3 - Surgical r/v
2x mucous plugs passed following PR
Testes descended bilaterally
?Small Bowel Atresia
Repeat Xray (no change)

Surgery @1300 on 16.3.14
(62 hours of age)
Fresh blood in abdomen (15-20ml)
Very Dilated twisted duodenojejunal loop (blind ending)
Apple peel atresia with nonviable (proximal part)
Absent Right & Transverse colon/Appedix/IC valve
Descending (Left)colon patent but curled
Ladd’s band twisting the D2-D3 creating a blind end.

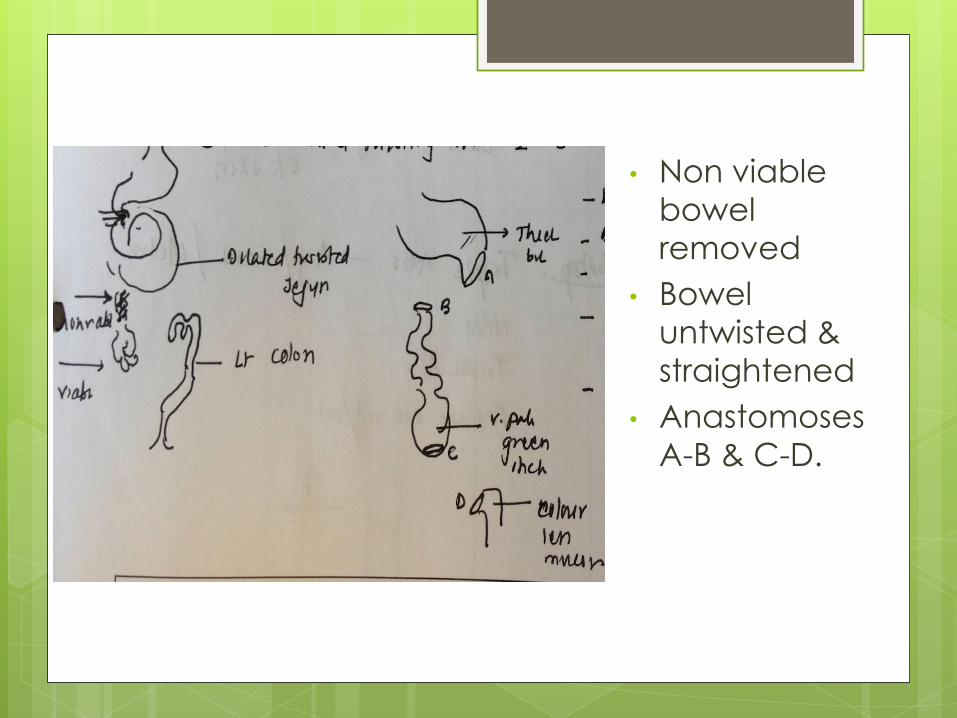
• Non viable
bowel
removed
• Bowel
untwisted &
straightened
• Anastomoses
A-B & C-D.
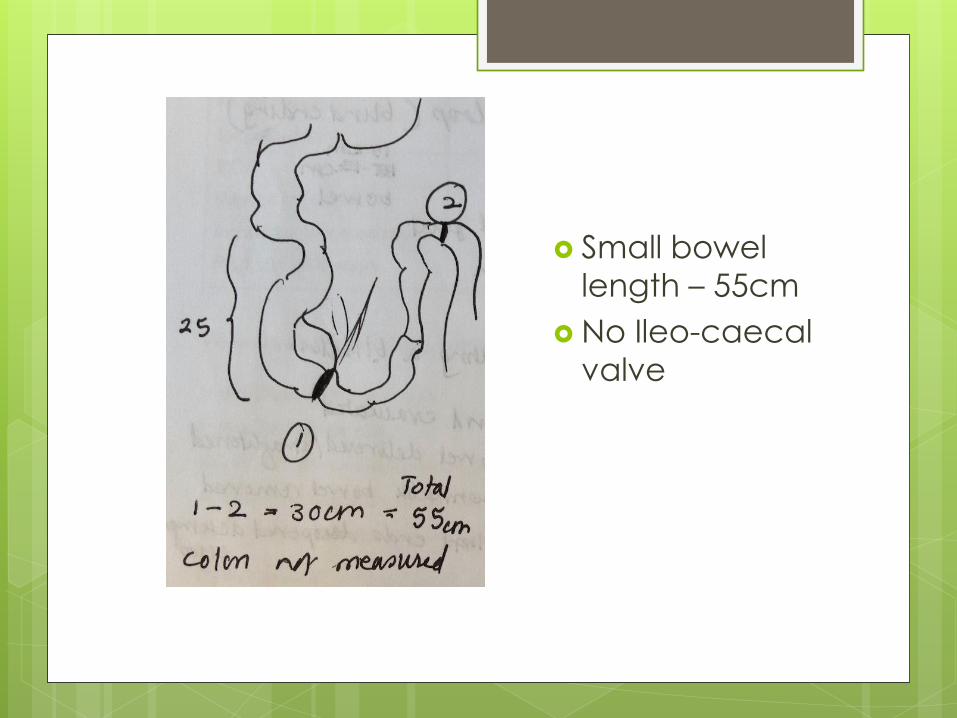
Small bowel
length – 55cm
No Ileo-caecal
valve
Post op complication
Not passed urine since operation (12 hrs)
Catheter passed, balloon inflated but ?not in
bladder.
Balloon deflated and fresh blood into
catheter. Catheter removed.
Post op information
Operation D3
Triple ABX (Gent, Co-Amox, Metroni)
TPN initiated (Standard initially)
PICC Day 5 (Prescribed TPN Day 6)
Extubated Day 7 to SVIA
Day 9 – completed 5/7 triple ABX
Trophic feeds 1ml hourly initiated Day 11
BO with Meconium on Day 12
Day 14 – Up to 3ml hourly
2x Vomits with green aspirates (up to 8mls)
Day 15 – Returned to low reflux
Echogenic Bowel First described in 1985
Poorly understood, Consequences for parents, obstetricians, radiologists,
neonatologists and paediatric surgeons.
Definition:
Foetal bowel with homogenous areas of
echogenicity equal to or greater than
surrounding bone. It can be focal or
multifocal.
There is associated considerable debate as
there is much intraobserver variability. Difficult to introduce objective measures
Echogenic Bowel
Timing
Physiological midgut herniation in the first
trimester precludes assessment of foetal
bowel in the first trimester.
In normal foetuses, it is a rare finding in T2 and
resolves with no adverse sequelae.
<20/40 usually transient, disappearing on
serial scans during the next few weeks
Foetal bowel is often echogenic in the third
trimester and is not considered to be clinically
significant.
It is often considered a soft sign for
aneuploidic anomalies.



Incidence
Echogenic bowel is present in 0-6% to 1-4% of
all second trimester foetuses.
Foetal small bowel becomes progressively
more visible by ultrasound scan during the
second trimester as relatively ‘bright’
meconium accumulates within its lumen from
about 16 weeks’ gestation.
Persistently hyper echogenic small bowel in
the third trimester is more likely to reflect
underlying pathology even though a normal
outcome is still possible.

Differential Diagnosis
35% of foetuses with echogenic bowel will
have underlying pathology (65% Normal)
1. Foetal aneuploidy Most commonly Trisomy 21: (bowel
hypotonia)
Includes Trisomy 13,18 and the sex
chromosomes
Isolated finding in 9% of foetuses with
aneuploidy.
2. Non chromosomal
Cystic fibrosis risk 2%: (meconium)
Congenital infection: CMV, Toxoplasmosis,
Parvovirus
Intra-amniotic bleeding: swallowing of blood Congenital malformations of the bowel: atresia,
perforation, meconium.
3. IUGR and increased risk perinatal morbidity and mortality: (mesenteric ischemia)
4. Other: foetal alcohol syndrome, alpha
thalassaemia homozygous
Differential Diagnosis
Relevant PMHx
Past obstetric history and any anomalies
Any family history of note. In particular
cystic fibrosis, aneuploidy, syndromes
History of bleeding (swallowed blood)
Viral/bacterial illness
A prior risk for aneuploidy

Scanning: Isolated or Other
Structural Anomalies
Detailed review of anatomy, growth and
placenta
Assess markers for aneuploidy Other major structural abnormality
Nuchal thickening Short femur / humerus
Intracardiac echogenic foci
Hypoplastic/absent nasal bone
Mild foetal pyelectasis Choroid plexus cyst
Assess markers of infection
Microcephaly, ventriculomegaly,
calcifications
Hydrops
IUGR
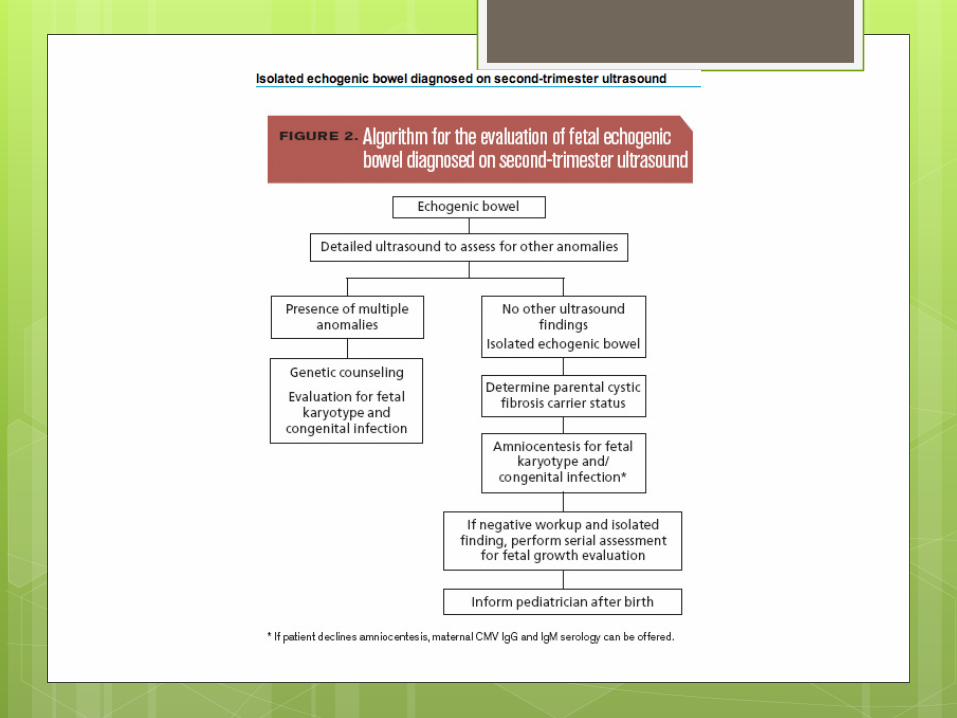
Scanning: Isolated or Other
Structural Anomalies
Investigation Amniocentesis
Karyotype
PCR for virology: Toxoplasma, Rubella,
Parvovirus, CMV DNA analysis: Cystic fibrosis
Maternal factors Virology screen : Toxoplasma, Rubella,
Parvovirus, CMV
Maternal AFP (associated IUGR)
Parental cystic fibrosis carrier status
screening detects 80% of carriers.
Not all mutations can be identified and this
does not exclude the possibility.
Main Causes (5)
Mechanism: Hypoperistalsis and/or decreased fluid content of the
meconium.
Foetal aneuploidy mostly Trisomy 21 (trisomy
18/13, Turner’s syndrome and triploidy)
It is thought to be due to decreased bowel motility
with increased water absorption from the meconium.
There appears to be decreased microvillar enzymes
activity in the amniotic fluid of aneuploid fetuses.
Causes
Small bowel obstruction proximally
(especially duodenal atresia) can
produce hyper echogenic bowel
by reducing the meconium fluid content.
Oligohydramnios.
due to decreased amniotic fluid content of
meconium.

Causes Hirschsprung’s disease (increased
frequency in foetuses with Down
syndrome) due to hypoperistalsis.
Intra-amniotic haemorrhage Swallowed blood products result in a
hypercellular meconium, probably with small
clots within the bowel lumen which is very
echogenic.
Bowel atresia. Decreased amniotic fluid content of the
meconium.
Causes – Cystic Fibrosis 0.8% - 13.3% of foetuses with echogenic
CF
Echogenic bowel in 50% to 78%
Abnormalities in pancreatic enzyme
secretion changes in meconium
consistency.
Focal echogenic bowel with calcifications
A hyper echoic mass
Bowel dilation.
Causes - IUGR
IUGR
Most don’t have echogenic bowel.
The suggested mechanism is bowel ischemia due
to haemodynamic redistribution and subsequent
mesenteric ischemia.
The presence of IUGR or elevated maternal serum
alpha-fetoprotein in the second trimester in
association with echogenic bowel seems to be
associated with a particularly poor foetal
prognosis.
Other Rarer Causes
Viral Infections 0% to 10%
Cytomegalovirus (Most common)
Toxoplasmosis
Parvovirus Mechanism is unclear, ?caused by direct
intestinal damage from inflammation or
meconium peritonitis or indirectly by ascites,
anaemia, or growth restriction
Thalassemia

Outcomes
5 large North American Studies combined
60% had no abnormalities
Aneuploidy (3-27%)
IUGR in 15%
Rare mechanical associations
Congenital infections
Antenatal haemorrhage
CF

Management
Detailed parental history
?links with karyotype anomalies, intrauterine
infection, and CF.
Complete USS to exclude associated
structural problems
Serial ultrasound assessments
Persistently hyper echogenic bowel
Especially those with IUGR and/or
documented abnormalities of umbilical
artery blood flow are at risk of functional
neonatal intestinal obstruction.
Prognosis
Usually resolves but still requires
investigation
Better prognosis if does resolve but
underlying disease still present in 15%
Outcome in those with no prenatal
diagnosis – probably normal, no clear
evidence long-term bowel problems


Summary
Algorithm
Main causes
1. Intra-amniotic bleeding
2. Cystic Fibrosis
3. Aneuploidy
4. Congenital Infection
5. Primary GI pathology
?Associated with IUGR
Related Documents











