❖ CASE 2 A 32-year-old man is involved in a motor vehicle accident. He used three-point restraints and was driving a sedan. The driver of a pick-up truck ran a stop sign while going at approximately 45 mph and “T-boned” the patient’s vehicle on the driver’s side. The patient has multiple injuries including a displaced fracture of the left humerus. He complains of an inability to open his left hand and loss of sensation to a portion of his left hand. ◆ What is the most likely diagnosis? ◆ What is the likely mechanism of the injury? ◆ What portion of the left hand is likely to have sensory deficit? ANSWERS TO CASE 2: RADIAL NERVE INJURY Summary: A 32-year-old man is involved in a motor vehicle accident that causes a displaced fracture of the left humerus. He has motor and sensory losses to his left hand. ◆ Most likely diagnosis: Injury to the radial nerve as it spirals around the humerus, resulting in an inability to extend the wrist or fingers and loss of sensation of the hand ◆ Likely mechanism: Stretch or crush injury to the radial nerve as it spirals around the midshaft of the humerus ◆ Likely location of sensory deficit: Radial (lateral) side of the dorsum of the hand and dorsum of the thumb and index and middle digits CLINICAL CORRELATION The radial nerve is at particular risk of injury in its course in the radial groove as it spirals around the midshaft of the humerus. Humeral fractures involving the midshaft region are of particular concern. There is loss of innervation of the posterior extensor muscles in the forearm, resulting in wrist drop and an inability to extend the digits at the metacarpophalangeal joints. The sensory loss on the dorsum of the hand and digits reflects the distal cutaneous distribution of the radial nerve. The triceps muscle (extensor of the elbow) is typically spared; however, the patient usually will not attempt to move the limb due to pain from the fracture. The deep brachial artery has the same path as the radial nerve in the radial groove and has a similar risk for injury. APPROACH TO THE RADIAL NERVE Objectives 1. Be able to describe the origin, course, muscles innervated, and distal cutaneous regions supplied by the radial nerve. 2. Be able to describe the arterial blood supply to the upper limb. 3. Be able to describe the origin, course, muscles innervated, and distal cutaneous regions supplied by the five major terminal branches of the brachial plexus (Cases 1, 2, and 4). Definitions Fracture: A break in the normal integrity of a bone or cartilage. Blunt trauma: Injury due to a crushing force as opposed to a sharp penetrating force. 18 CASE FILES: ANATOMY DISCUSSION The radial nerve is a continuation of the posterior cord of the brachial plexus, and it reaches the posterior compartment of the arm by coursing around the radial groove of the humerus with the deep brachial artery (Figure 2-1). It gives off multiple muscular branches to the triceps muscle in

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
❖ CASE 2 A 32-year-old man is involved in a motor vehicle accident. He used three-point restraints and was driving a sedan. The driver of a pick-up truck ran a stop sign while going at approximately 45 mph and “T-boned” the patient’s vehicle on the driver’s side. The patient has multiple injuries including a displaced fracture of the left humerus. He complains of an inability to open his left hand and loss of sensation to a portion of his left hand.
◆ What is the most likely diagnosis?
◆ What is the likely mechanism of the injury?
◆ What portion of the left hand is likely to have sensory deficit? ANSWERS TO CASE 2: RADIAL NERVE INJURY Summary: A 32-year-old man is involved in a motor vehicle accident that causes a displaced fracture of the left humerus. He has motor and sensory losses to his left hand.
◆ Most likely diagnosis: Injury to the radial nerve as it spirals around the humerus, resulting in an inability to extend the wrist or fingers and loss of sensation of the hand
◆ Likely mechanism: Stretch or crush injury to the radial nerve as it spirals around the midshaft of the humerus
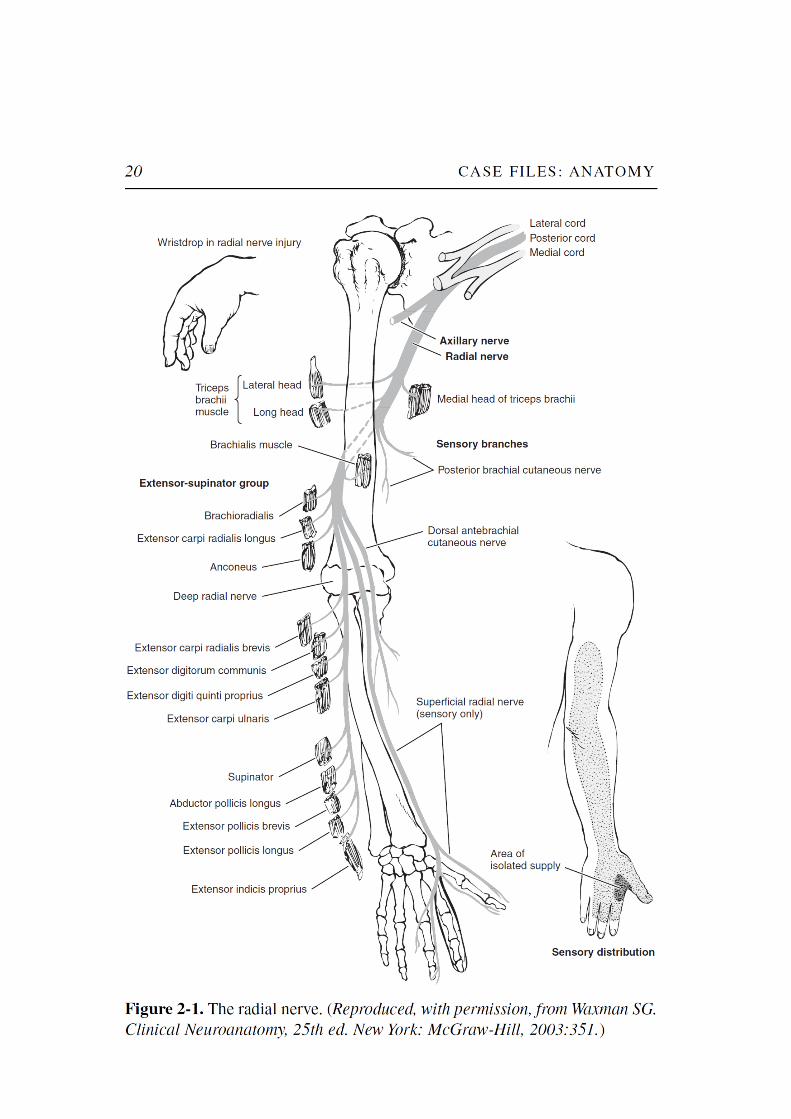
◆ Likely location of sensory deficit: Radial (lateral) side of the dorsum of the hand and dorsum of the thumb and index and middle digits CLINICAL CORRELATION The radial nerve is at particular risk of injury in its course in the radial groove as it spirals around the midshaft of the humerus. Humeral fractures involving the midshaft region are of particular concern. There is loss of innervation of the posterior extensor muscles in the forearm, resulting in wrist drop and an inability to extend the digits at the metacarpophalangeal joints. The sensory loss on the dorsum of the hand and digits reflects the distal cutaneous distribution of the radial nerve. The triceps muscle (extensor of the elbow) is typically spared; however, the patient usually will not attempt to move the limb due to pain from the fracture. The deep brachial artery has the same path as the radial nerve in the radial groove and has a similar risk for injury. APPROACH TO THE RADIAL NERVE Objectives 1. Be able to describe the origin, course, muscles innervated, and distal cutaneous regions supplied by the radial nerve. 2. Be able to describe the arterial blood supply to the upper limb. 3. Be able to describe the origin, course, muscles innervated, and distal cutaneous regions supplied by the five major terminal branches of the brachial plexus (Cases 1, 2, and 4). Definitions Fracture: A break in the normal integrity of a bone or cartilage. Blunt trauma: Injury due to a crushing force as opposed to a sharp penetrating force. 18 CASE FILES: ANATOMY DISCUSSION The radial nerve is a continuation of the posterior cord of the brachial plexus, and it reaches the posterior compartment of the arm by coursing around the radial groove of the humerus with the deep brachial artery (Figure 2-1). It gives off multiple muscular branches to the triceps muscle in

the posterior compartment. The nerve then pierces the lateral intermuscular septum to return to the anterior compartment of the arm and descends to the level of the lateral epicondyle of the humerus; at this level, it lies deep to the brachioradialis muscle, where it divides into its two terminal branches. The deep branch of the radial nerve is entirely motor to the muscles of the posterior compartment of the forearm. The other terminal branch, the superficial branch of the radial nerve, is sensory to the dorsum of the hand and to the dorsum of the thumb, index finger, and the radial side of the middle finger. The radial nerve also has cutaneous sensory branches to the posterior and lateral arm and to the posterior forearm. The blood supply to the upper limb is derived from the brachial artery, a direct continuation of the axillary artery. It begins at the lower border of the teres major muscle and accompanies the median nerve on the medial aspect of the humerus, where its pulsations can be palpated or the artery occluded to control hemorrhage. In its descent toward the elbow, it gives off the deep brachial artery, which supplies the posterior compartment of the arm, and passes around the radial groove of the humerus with the radial nerve. It also has ulnar collateral branches to the elbow joint. The brachial artery shifts anteriorly as it enters the forearm, lying just medial to the tendon of the biceps brachii muscle in the cubital fossa. At about the level of the neck of the radius, it divides into the ulnar and radial arteries, the main arteries of the forearm and hand. Near their origin, each sends recurrent arterial branches to supply the elbow joint. The radial artery supplies the lateral aspects of the forearm and at the wrist passes dorsally (deep) through the anatomical snuff box (see Case 3) to become the deep palmar arch. The ulnar artery is the larger branch of the brachial, and it supplies the medial aspect of the forearm. A branch close to its origin, the common interosseous artery, divides into anterior and posterior interosseous arteries. The latter artery is the main blood supply to the posterior compartment. At the wrist, the ulnar artery enters the hand to form the superficial palmar arch. The superficial and deep palmar arches form an arterial anastomosis and give rise to arteries to the digits. Also see Case 1.
Related Documents











