9/7/11 1 Cardiopulmonary Screening September 23, 2011 CPTA Annual Conference Long Beach, CA LeeAnne Carrothers, PT, PhD Why C-P Screening? • CVD responsible for most deaths in the US than any other disease • Although patients may come to us with non-CP problems, many have histories of or current CP diagnoses (Freese, Richter and Burlis (2002) ” Self-reported measurement of heart rate and blood pressure in patients by physical therapy clinical instructors.” Physical Therapy: 82(12): 1192-200.) • Direct Access/Primary Care-You are responsible screening of patients you see off the street Who should be screened? PT Options • Treat • Refer • Treat AND Refer Differential Diagnosis • Definitions: – Medical: The determination of which two or more diseases with similar symptoms is the one from which a patient is suffering based on an analysis of the clinical data. – Physical Therapy: a label encompassing a cluster of signs and symptoms commonly associated with a disorder or syndrome or category of impairment, functional limitation or disability” (APTA HOD, 1995). Differential Diagnosis • Process: – Assess patient (exam, interview, systems review) to determine list of patient findings – Create list of potential causes for a given symptom/signs – Perform further tests that enable the clinician to further delineate the reasons for patient findings. – Once a decision has been reached about the nature/cause of symptoms, the PT’s responsibility is to take appropriate action within the scope of PT practice, i.e., treat, refer, or treat AND refer.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

9/7/11
1
Cardiopulmonary Screening September 23, 2011
CPTA Annual Conference Long Beach, CA
LeeAnne Carrothers, PT, PhD
Why C-P Screening?
• CVD responsible for most deaths in the US than any other disease
• Although patients may come to us with non-CP problems, many have histories of or current CP diagnoses (Freese, Richter and Burlis (2002) ” Self-reported measurement of heart rate and blood pressure in patients by physical therapy clinical instructors.” Physical Therapy: 82(12):1192-200.)
• Direct Access/Primary Care-You are responsible screening of patients you see off the street
Who should be screened? PT Options
• Treat • Refer • Treat AND Refer
Differential Diagnosis
• Definitions: – Medical: The determination of which two or
more diseases with similar symptoms is the one from which a patient is suffering based on an analysis of the clinical data.
– Physical Therapy: a label encompassing a cluster of signs and symptoms commonly associated with a disorder or syndrome or category of impairment, functional limitation or disability” (APTA HOD, 1995).
Differential Diagnosis
• Process: – Assess patient (exam, interview, systems
review) to determine list of patient findings – Create list of potential causes for a given
symptom/signs – Perform further tests that enable the clinician to
further delineate the reasons for patient findings. – Once a decision has been reached about the
nature/cause of symptoms, the PT’s responsibility is to take appropriate action within the scope of PT practice, i.e., treat, refer, or treat AND refer.

9/7/11
2
When you hear hoofbeats… Review of Systems
• The primary symptoms of cardiopulmonary diseases include – Chest pain – Cough
• Sputum Production • Hemoptysis
– Dyspnea/Orthopnea – Cyanosis – Activity Limitations – Peripheral Edema
Some of these symptoms may be so “routine” the patient doesn’t think to volunteer the symptom – you need to ask about all of them in a systematic manner.
Chest pain
• Localized chest pain is a common symptom of pleural disorders (presents as pain with max. inspiration), some pneumonias and even fractured ribs from excessive coughing.
• Asking the patient to localize pain with one or two fingers will guide you to a more careful examination of that area.
Cough
• A cough is a normal defense mechanism. • The most common symptom of lung disease is
cough. • Smoker’s morning cough results from the normal
decrease in coughing during sleep, with buildup of mucus during the night.
• A cough with expelled sputum or other material is termed “productive”.
• A non-productive cough can be due to local irritants, viral infections or even psychological.
Sputum Production
• Sputum production is normal - 75-100 ml is secreted daily by the bronchi.
• Uninfected sputum is odorless, transparent and whitish gray, resembling mucus
• Sputum should be described according to color, consistency, quantity, occurrences during the day and the presence of absence of blood.
Hemoptysis
• Coughing up blood - either clots or blood tinged sputum. • This usually frightens the patient – so it isn’t a “hidden
symptom”. • Clots of blood are very serious – indicating malignancies,
pulmonary emboli or cardiac disease. • Streaks of blood are common in bronchitis, tumors or
pneumonias. • Blood-tinged (i.e., flecks) sputum is commonly seen in
smokers. • Ask how much blood – sometimes the patient will even
bring some in to show you!

9/7/11
3
Difficulty breathing
• Dyspnea is the subjective sensation of shortness of breath.
• Tachypnea is rapid breathing (an objective finding)
• Orthopnea is difficulty breathing while lying flat
• Paroxysmal nocturnal dyspnea is the sudden onset of shortness of breath that occurs at night.
Peripheral vs. Central Cyanosis
Which has a worse prognosis???
Peripheral Central
Causes of Chest Pain
• Cardiac – Ischemic – Stable Angina – Unstable Angina – Printzmetal’s Angina – Coronary Insufficiency/Myocardial
Infarction – Pericarditis
Causes of Chest Pain, cont.
• Pulmonary/Pleural – Pleurisy
– Pneumothorax
– Pulmonary Embolus
Causes of Chest Pain, cont.
• GI • Hiatal Hernia • Reflux Esophagitis • Esophageal Spasm • Cholecystitis • Peptic Ulcer Disease • Pancreatitis
Causes of Chest Pain, cont.
• Psych – Anxiety/Panic Attacks
9/7/11
4
Causes of Chest Pain, cont.
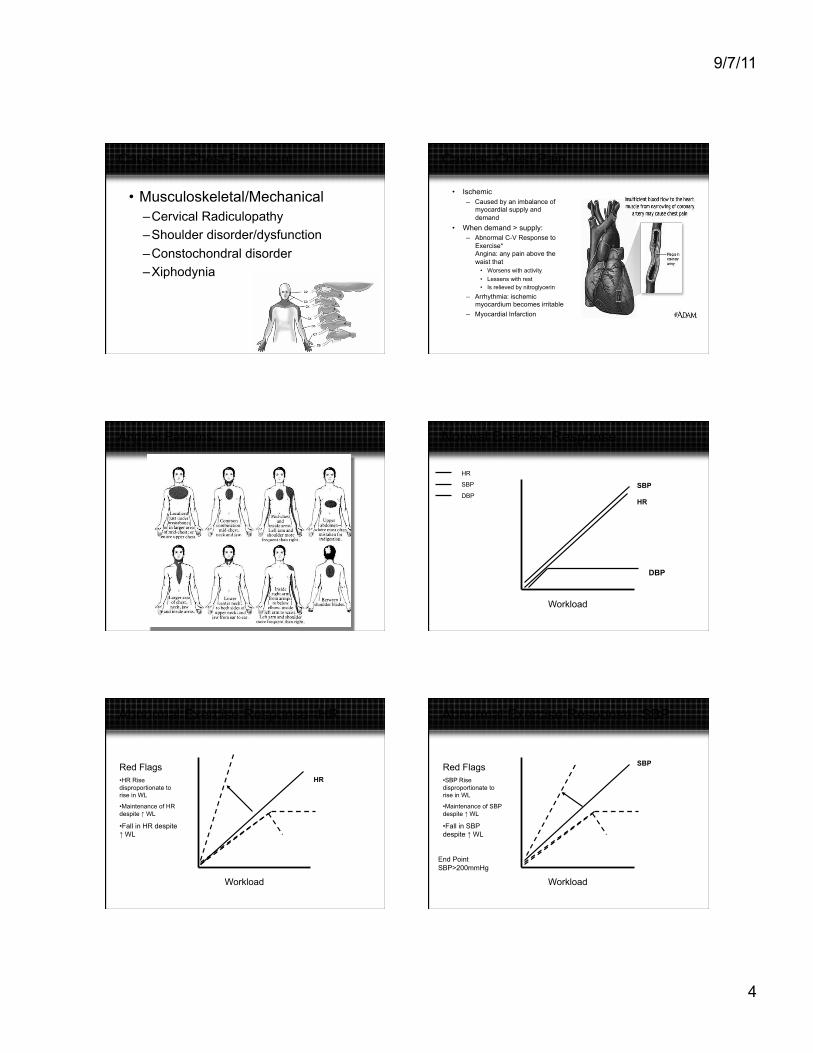
• Musculoskeletal/Mechanical – Cervical Radiculopathy – Shoulder disorder/dysfunction – Constochondral disorder – Xiphodynia
Cardiac Chest Pain
• Ischemic – Caused by an imbalance of
myocardial supply and demand
• When demand > supply: – Abnormal C-V Response to
Exercise* Angina: any pain above the waist that
• Worsens with activity
• Lessens with rest • Is relieved by nitroglycerin
– Arrhythmia: ischemic myocardium becomes irritable
– Myocardial Infarction
Anginal Patterns Normal Exercise Response
Workload
HR
SBP
DBP HR
SBP
DBP
Abnormal Exercise Response--HR
Workload
HR Red Flags • HR Rise disproportionate to rise in WL
• Maintenance of HR despite ↑ WL
• Fall in HR despite ↑ WL
Abnormal Exercise Response--SBP
Workload
SBP Red Flags • SBP Rise disproportionate to rise in WL
• Maintenance of SBP despite ↑ WL
• Fall in SBP despite ↑ WL
End Point SBP>200mmHg

9/7/11
5
Abnormal Exercise Response--DBP
Workload
DBP
Red Flags • DBP>15 mmHg over resting, regardless of the increase in workload
• Resting DBP > 95
End Point DBP> 100mmHg
Stable angina
• Has a well-established level of onset
• Can be reliably predicted with a set level of myocardial demand
• Can be controlled with a reduction in intensity of activity or by taking NTG
Unstable Angina
• Definition: Presence of signs/symptoms of inadequate blood supply to the myocardium in the absence of demands that usually provoke this imbalance.
• Clinical Cues: – Angina at rest – Occurrence of the patient’s typical angina at a
significantly lower level of activity than usual. – Deterioration of a previously stable pattern, i.e., angina
occurring several times a day vs. several times a week. – Evidence of loss of previously present myocardial
reserve, such as a drop in blood pressure or increase in heart rate with levels of activity previously well tolerated.
Printzmetal’s Angina
• Angina that is not preceded by an increase in myocardial demand
• Typically occurs at rest; most often in the early morning Caused by coronary artery spasm (due to presence of risk factors)
• Treated with drugs to manage vasomotor tone, e.g., calcium antagonists
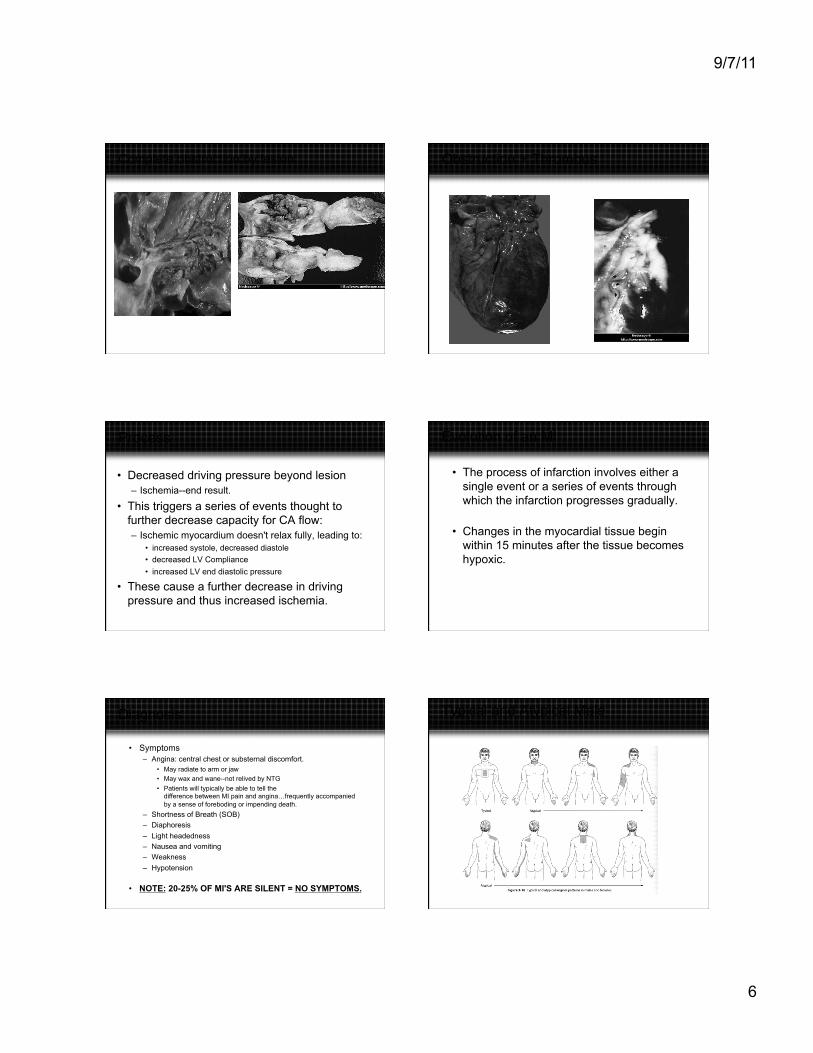
Myocardial Infarction Mechanisms of Coronary Artery Obstruction
• Complete obstruction by lesion
• Obstruction + Thrombus--result is total occlusion
• Obstruction + Coronary Artery Spasm
• Near total obstruction + high MVO2
9/7/11
6
Complete obstruction by lesion Obstruction + Thrombus
Process
• Decreased driving pressure beyond lesion – Ischemia--end result.
• This triggers a series of events thought to further decrease capacity for CA flow: – Ischemic myocardium doesn't relax fully, leading to:
• increased systole, decreased diastole • decreased LV Compliance • increased LV end diastolic pressure
• These cause a further decrease in driving pressure and thus increased ischemia.
Evolution of an MI
• The process of infarction involves either a single event or a series of events through which the infarction progresses gradually.
• Changes in the myocardial tissue begin within 15 minutes after the tissue becomes hypoxic.
Diagnosis
• Symptoms – Angina: central chest or substernal discomfort.
• May radiate to arm or jaw • May wax and wane--not relived by NTG
• Patients will typically be able to tell the difference between MI pain and angina…frequently accompanied by a sense of foreboding or impending death.
– Shortness of Breath (SOB) – Diaphoresis – Light headedness – Nausea and vomiting – Weakness – Hypotension
• NOTE: 20-25% OF MI'S ARE SILENT = NO SYMPTOMS.
Typical and Atypical Male Irwin and Tecklin, 4th Ed.

9/7/11
7
Typical and Atypical Female Irwin and Tecklin, 4th ed.
Serum Enzymes
• Based on several assumptions: – elevation of enzymes occurs with cell death
and not just prolonged ischemia. – enzyme rise is not attributable to rise in other
organs
– size of infarct is proportional to amount of rise.
Serum Enzymes
• CK (AKA CPK) – CK-MB
• LDH • Troponin • Myoglobin
Transmural vs. Subendocardial
Pericarditis
• Description: Inflammation of the pericardium
• May develop either as a primary condition or due to a number of other circumstances/conditions
• Frequently follows MI, CABG Surgery, valve replacement
• May be acute or chronic – Chronic form can result in
accumulation of fluid in pericardium that interferes with diastolic filling (cardiac tamponade) or restriction due to formation of fibrinous tissue between visceral and parietal layers.
Pericarditis
• Signs: – Fever – Chills – Malaise
– Pericardial Friction Rub
9/7/11
8
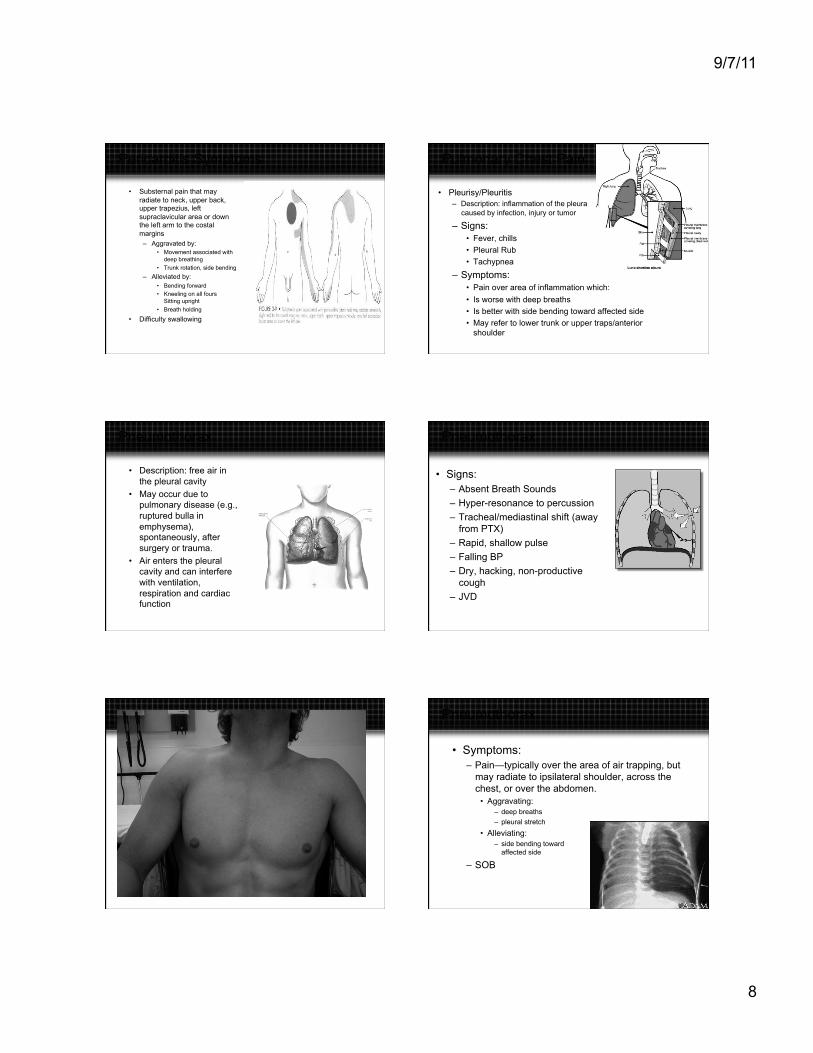
Pericarditis Symptoms
• Substernal pain that may radiate to neck, upper back, upper trapezius, left supraclavicular area or down the left arm to the costal margins – Aggravated by:
• Movement associated with deep breathing
• Trunk rotation, side bending
– Alleviated by: • Bending forward • Kneeling on all fours
Sitting upright • Breath holding
• Difficulty swallowing
Pulmonary Chest Pain
• Pleurisy/Pleuritis – Description: inflammation of the pleura
caused by infection, injury or tumor
– Signs: • Fever, chills • Pleural Rub • Tachypnea
– Symptoms: • Pain over area of inflammation which: • Is worse with deep breaths • Is better with side bending toward affected side • May refer to lower trunk or upper traps/anterior
shoulder
Pneumothorax
• Description: free air in the pleural cavity
• May occur due to pulmonary disease (e.g., ruptured bulla in emphysema), spontaneously, after surgery or trauma.
• Air enters the pleural cavity and can interfere with ventilation, respiration and cardiac function
Pneumothorax
• Signs: – Absent Breath Sounds
– Hyper-resonance to percussion
– Tracheal/mediastinal shift (away from PTX)
– Rapid, shallow pulse
– Falling BP
– Dry, hacking, non-productive cough
– JVD
Pneumothorax
• Symptoms: – Pain—typically over the area of air trapping, but
may radiate to ipsilateral shoulder, across the chest, or over the abdomen.
• Aggravating: – deep breaths – pleural stretch
• Alleviating: – side bending toward
affected side
– SOB

9/7/11
9
Pulmonary Embolus
• Description: pulmonary vasculature becomes occluded by a displaced thrombus, an air bubble, a fat globule, clump of bacteria, vegetations from infected heart valves or other particulate matter
• Most common is due to DVT
Pulmonary Embolus, cont.
• Three major risk factors: – Blood stasis, – endothelial injury, – hypercoagulable states
• Other risks: – > 50 – Previous history – Malignant disease – Inactivity – Obesity – Pregnancy – Clotting abnormality – OCA use
• Embolism causes a blockage of blood flow to the lung tissue resulting in pulmonary infarct
Pulmonary Embolus, cont.
• Signs: Vary greatly, depending on the extent of tissue necrosis – Hemoptysis – Tachypnea – Tachycardia – Fever
• Symptoms: – Pleuritic pain – Diffuse chest discomfort – Apprehension – Cough
Chest pain of GI origin
• Description – Most pain of GI
origin results from ulceration or infection of the GI mucosa
– Typically has a vague onset
– Unrelated to degree of physical activity
Pain behavior
• Location: corresponds to dermatomes from which the diseased organ receives its innervation
• Aggravating: – Positional, i.e., lying flat – Food consumption (foods high in acids, fats) – Palpation over involved organ
• Alleviating: – Antacids – Consumption of food – Release of gas (burp)
Chest Pain from Psych Causes
• Description: Chest pain occurs frequently associated with Panic / Anxiety disorders
• Signs – Tachycardia – Dyspnea – Diaphoresis
• Symptoms: – Substernal Chest Pain – Does not radiate – Not aggravated by respiratory or M-S Movements – Associated with hyperventilation and claustrophobia – Accompanied by subjective sense of impending death
9/7/11
10
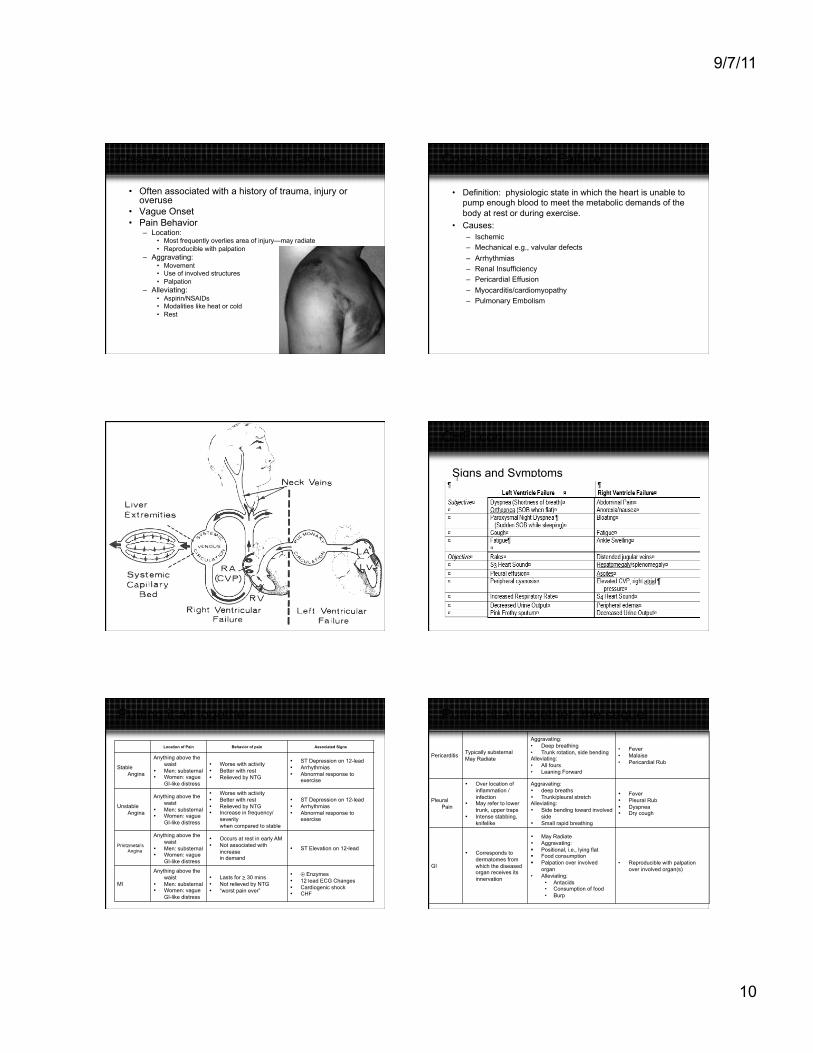
Chest Pain from M-S / Mechanical Causes
• Often associated with a history of trauma, injury or overuse
• Vague Onset • Pain Behavior
– Location: • Most frequently overlies area of injury—may radiate • Reproducible with palpation
– Aggravating: • Movement • Use of involved structures • Palpation
– Alleviating: • Aspirin/NSAIDs • Modalities like heat or cold • Rest
Congestive Heart Failure
• Definition: physiologic state in which the heart is unable to pump enough blood to meet the metabolic demands of the body at rest or during exercise.
• Causes: – Ischemic – Mechanical e.g., valvular defects – Arrhythmias – Renal Insufficiency – Pericardial Effusion – Myocarditis/cardiomyopathy – Pulmonary Embolism
CHF, cont.
Signs and Symptoms
Putting it all together
Location of Pain Behavior of pain Associated Signs
Stable Angina
Anything above the waist
• Men: substernal • Women: vague
GI-like distress
• Worse with activity • Better with rest • Relieved by NTG
• ST Depression on 12-lead • Arrhythmias • Abnormal response to
exercise
Unstable Angina
Anything above the waist
• Men: substernal • Women: vague
GI-like distress
• Worse with activity • Better with rest • Relieved by NTG • Increase in frequency/
severity when compared to stable
• ST Depression on 12-lead • Arrhythmias • Abnormal response to
exercise
Printzmetal’s Angina
Anything above the waist
• Men: substernal • Women: vague
GI-like distress
• Occurs at rest in early AM • Not associated with
increase in demand
• ST Elevation on 12-lead
MI Anything above the
waist • Men: substernal • Women: vague
GI-like distress
• Lasts for > 30 mins • Not relieved by NTG • “worst pain ever”
• ⊕ Enzymes • 12 lead ECG Changes • Cardiogenic shock • CHF
Putting it all together, the sequel.
Pericarditis Typically substernal May Radiate
Aggravating: • Deep breathing • Trunk rotation, side bending Alleviating: • All fours • Leaning Forward
• Fever • Malaise • Pericardial Rub
Pleural Pain
• Over location of inflammation / infection
• May refer to lower trunk, upper traps
• Intense stabbing, knifelike
Aggravating: • deep breaths • Trunk/pleural stretch Alleviating: • Side bending toward involved
side • Small rapid breathing
• Fever • Pleural Rub • Dyspnea • Dry cough
GI • Corresponds to
dermatomes from which the diseased organ receives its innervation
• May Radiate • Aggravating: Positional, i.e., lying flat Food consumption Palpation over involved
organ • Alleviating:
• Antacids • Consumption of food • Burp
• Reproducible with palpation over involved organ(s)
9/7/11
11
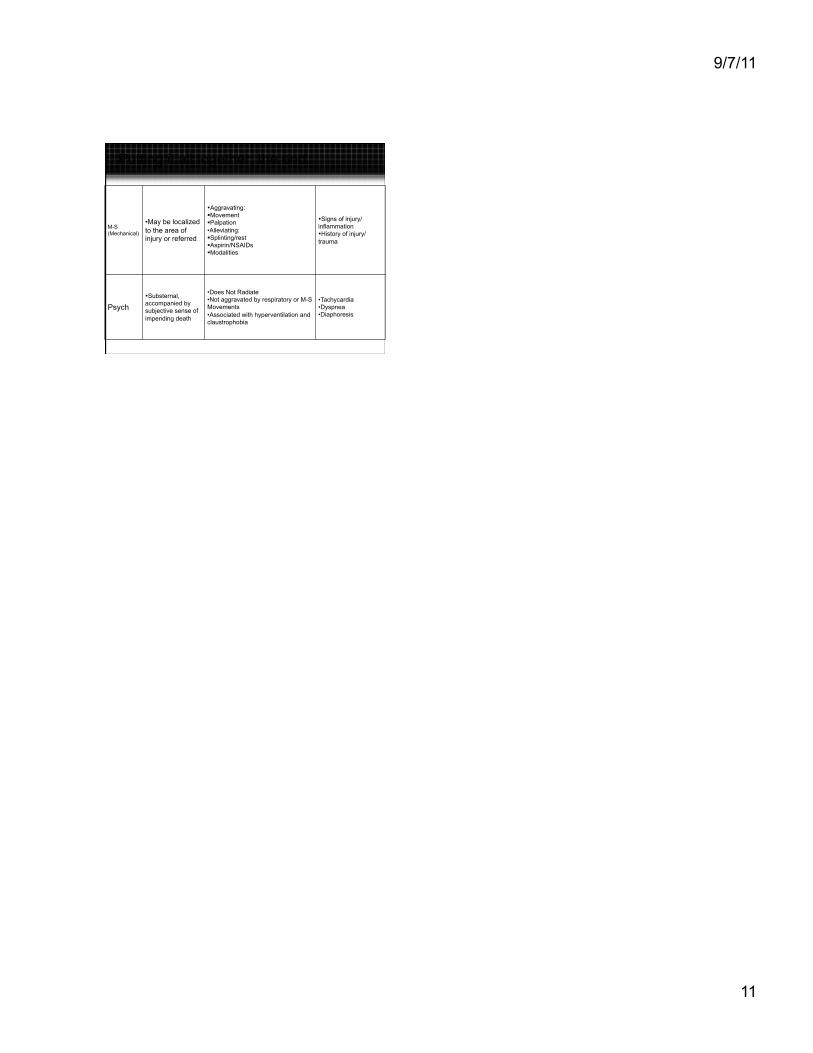
Putting it all together, the end.
M-S (Mechanical)
• May be localized to the area of injury or referred
• Aggravating: Movement Palpation • Alleviating: Splinting/rest Aspirin/NSAIDs Modalities
• Signs of injury/ inflammation • History of injury/trauma
Psych • Substernal, accompanied by subjective sense of impending death
• Does Not Radiate • Not aggravated by respiratory or M-S Movements • Associated with hyperventilation and claustrophobia
• Tachycardia • Dyspnea • Diaphoresis
Related Documents











