1 CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014 Canadian Alliance for Regional Risk Factor Surveillance - Quarterly eNewsletter CARRFS Interview Built Environment Dr. David L. Mowat Medical Officer of Health, Region of Peel, Ontario CARRFS Profile Larry Svenson Director, Alberta Ministry of Health CARRFS Feature Built Environment Home is HEALTH

CARRFS eNews Spring 2014
Mar 23, 2016
Online publication for the Canadian Alliance for Regional Risk Factor Surveillance.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
1
CARRFS eNewswww.carrfsenews.ca Volume 4, Issue 2, Spring 2014
Canadian Alliance for Regional Risk Factor Surveillance - Quarterly eNewsletter
CARRFS InterviewBuilt Environment Dr. David L. Mowat Medical Officer of Health, Region of Peel,Ontario
CARRFS ProfileLarry Svenson Director, Alberta Ministry of Health
CARRFS Feature Built EnvironmentHome is HEALTH

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
2
Home is Health! Built Environment as a Risk Factor for Chronic Disease 5 CARRFS eNews examines housing and how built environment has become a risk factor for chronic disease. By PAUL WEBSTER
CARRFS Interview 11 Dr. David L. Mowat, Medical Officer of Health, Region of Peel talks about built environment in the context of social determinants of health. By JOSTEIN ALGROY
Surveillance Facts 16 Dr. Bernard Choi, Public Health Agency of Canada. Part VI of his series about the Evolution of Public Health Surveillance. By BERNARD CHOI
CARRFS Profile 19 The CARRFS Member Profile: Larry Svenson, Director, Alberta Ministry of Health. By JOSTEIN ALGROY
CARRFS eNews Website 21 CARRFS eNews has developed a stand-alone website for the newsletter to serve the readers better. By JOSTEIN ALGROY
Table of ContentsFrom the Editor .......................................................................................................... page 3
News & Trends ......................................................................................................... page 4
Built Environment: Home is Health ........................................................... page 5
A Subtle Subject for Surveillance ............................................................... page 9
Can Design Help Build Transit Culture .................................................... page 10
CARRFS Interview: Dr. David L. Mowat .................................................. page 11
Designing the Built Environment to Improve Public Health ... page 15
Surveillance Facts ....................................................................................................... page 16
Chair’s Message .......................................................................................................... page 18
CARRFS Profile .......................................................................................................... page 19
CARRFS eNews Website ................................................................................. page 21
Updates from Working Groups ................................................................... page 23
Hello & Goodbye .................................................................................................... page 24
CONTRIBUTORS
Jostein Algroy, Editor in ChiefXiaoyan Guo, Copy EditorPaul Webster, Health Science WriterDr. Bernard Choi, Science WriterMary Lou Decou, Senior WriterAhalya Mahendra, CARRFS Working Group Chair
PAN-CANADIAN EDITORIAL ADVISORY BOARD
Jostein Algroy, Editor in ChiefPaul Webster, Health Science WriterAnne Simard, Chief Public Affairs Officer, Public Health OntarioMary Lou Decou, Epidemiologist, Public Health Agency of CanadaDr. Bernard Choi, Senior Research Scientist, Public Health Agency of CanadaDr. Elizabeth Rael, Senior Epidemiologist, Ontario Ministry of Health and Long-Term CareLarry Svenson, Director, Alberta Ministry of HealthDr. Drona Rasali, Director, British Columbia Provincial Health Services Authority
More members to be added to the Board later.
SECRETARIAT SUPPORT
Public Health Agency of CanadaMary Lou Decou
PUBLICATION
CARRFS eNews is a Quarterly Newsletter for the Canadian Alliance for Regional Risk Factor Surveillance (CARRFS) and is published in Winter, Spring, Summer, and Fall.
Photo Credits:Cover Photo: CanStockPhoto_csp8025150Photo page 5: iStockPhoto_11156895Photos page 10: iStockPhoto_37373834, 24539820, 23218833
Disclaimer: CARRFS is a pan-Canadian network of public stakeholders across Canada, working together to enhance the capacity of Regional Risk Factor Surveillance in Canada. CARRFS is supported by the Public Health Agency of Canada (PHAC). The content in the CARRFS eNews does not necessarily reflect the official view of PHAC, Health Canada, the Government of Canada or the employer of its contributors.
CARRFS WEBSITE URL: www.carrfs-acsrfr.ca
CONTENTS in this Issue...

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
3
From the EditorAs CARRFS eNews evolves to deliver better insights and to serve the Canadian risk factor surveillance community better, we’re focusing on key themes in public health. In this issue, we take a closer look at Built Environment.
Depending on where and how you live, your home may just possibly be your most valuable health asset. Which is why it is so worrying that Canadian homes,
neighborhoods, cities and suburbs are so predominantly designed around roads, cars and giant plazas surrounded by vast parking lots. Sadly, for millions of Canadians, the drive-through is a way of life. As a result, walking, bicycling and taking public transit are exotic activities seldom attempted in daily life. As a growing body of evidence indicates, the built environment significantly impacts on healthy lifestyles, environmental safety, and social equality. In this issue of CARRFS eNews, Paul Webster surveys research probing Canada’s built environments as “a cause of causes” for chronic disease. Housing, he reveals, is an especially important risk factor for chronic diseases. Dr. David Mowat, Medical Officer of Health for the Region of Peel in Ontario, has worked for years to help city planners understand the health risks associated with low density built environments. In an interview with CARRFS eNews he underlines the lack of physical activities in routine daily life - or what he calls “utilitarian physical activity”. Such activities, Mowat suggests, have been “engineered” out of our lives and now need to be reintroduced. Not an easy task! But necessary, because we can’t wait any longer. It will cost society way too much if we wait.
To try to reach more readers through a platform offering better service and interactivity, we’ve developed a new website for CARRFS eNews. You can read more about it on page 21, or simply visit www.carrfsenews.ca. Enjoy!
Jostein AlgroyEditor-in-Chief
Volunteers for CARRFS eNewsCARRFS eNews needs volunteers to help with specific sections of the newsletter. We need reviewers who would like to review “Epi” reports and share the information with the network. We are looking for a person who can write up a few blurbs about News & Trends taking place in the “Epi” community – nationally and internationally. If you are interested please contact [email protected].
Send us your StoryWe urge all members of CARRFS to send us articles and ideas for upcoming issues. Please submit your story to [email protected].

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
4
New
s & T
rends Bernard Choi, Canada’s representative on Pan
American Health Organization (PAHO) Working GroupDr. Bernard Choi, a member of CARRFS, Science Writer for CARRFS eNews and Senior Research Scientist at the Public Health Agency of Canada, has been appointed Canada's representative on the Countries Working Group (CWG) for validation of the Pan American Health Organization (PAHO) 2014-2019 Strategic Plan baselines and targets. The CWG will present its recommendations to the PAHO Executive Committee in June 2014 and the PAHO Directing Council meeting in September 2014. The PAHO CWG has been convened to advance the following: (1) Establish a comprehensive and accountable monitoring and assessment system to report on the implementation of the 2014-2019 Strategic Plan; (2) Complete the Compendium of Indicators and conduct a validation process for baselines and targets of the 2014-2019 Strategic Plan; and (3) Revisit the programmatic priorities stratification methodology in order to improve the methodology and apply its results to future programs and budgets. If you have any comments or suggestions for the PAHO 2014-2019 Strategic Plan, please contact Dr. Choi at [email protected]. <>
by Bernard Choi
Tripling Obesity in CanadaSince the mid-80‘s, the prevalence of obesity in Canada has tr ipled according to a study that was published in the journal CMAJ Open. The study which used data from three Statistics Canada surveys indicated that 18 percent of Canadians were obese in 2011 - up from 6 percent in 1985. In 2019 f ive provinces - Newfoundland and Labrador, Nova Scotia, New Brunswick, Saskatchewan and Manitoba will have more adults classified as overweight and obese than people with healthy weight. <>
by Jostein Algroy
Active Transportation and Health Built EnvironmentsAcross Canada, governments and non-governmental organizations are developing policies and programs that support active transportation and healthy built environments. But a 2012-13 Public Health Agency of Canada (PHAC) consultation showed that there were few opportunities to share the work being done by the different Provinces/Territories. To bridge this knowledge gap, PHAC’c Centre for Chronic Disease Prevention is leading a collaborative project called Mobilizing Knowledge for Active Transport (MKAT) to gather and share knowledge that can accelerate effective approaches to active transportation across Canada. The overall purpose of MKAT is to strengthen evidence that informs active transportation planning. The main findings from this project will be presented through knowledge briefs at a number of webinars and meetings in the first half of 2014. <>
by Ahalya Mahendra
Neighbourhoods module at the Canadian Community Health SurveyThe neighbourhoods in which Canadians live influence behaviour, health, and well-being. Certain community features such as recreational facilities, sidewalks, parks, and stores within walking distance from home have a strong potential to contribute to increased physical activity. In particular, physical activity plays an important role in promoting health and preventing disease among Canadians. People who are physically active live longer, healthier lives and are more likely to avoid illness and injury. In 2011, the Public Health Agency of Canada sponsored a module on neighbourhood environments as part of Statistics Canada’s Canadian Community Health Survey. This module provides new information on the number of Canadians who live in neighbourhoods that promote leisure-time physical activity and active transportation (walking or biking to work or school). <>
by Ahalya Mahendra
The results of these analysis can be found at:Fast Facts about Canada's Neighbourhoods and Physical Activity http://www.phac-aspc.gc.ca/hp-ps/hl-mvs/fast-facts-faits-rapides-eng.php

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
5
BUILT ENVIRONMENT
Home is HEALTH
CARRFS Feature...

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
6
Home is HEALTH Built Environment As a Risk Factor for Chronic DiseasePaul Webster looks at built environment research, focusing on housing as a risk factor for chronic disease.
The homes, neighborhoods, communities and cities we live in – our “built environments” – frame social relations and imprint lifestyles, cultures, and economies. They can also inflict health problems. “When we say the physical and social conditions in which people live have enormous health impacts,” explains Nazeem Muhajarine, a professor of community health and epidemiology at the University of Saskatchewan who heads a multifaceted project probing urban design and health, “it’s often built environment we’re talking about. Built environment is a kind of primordial ‘cause of causes’.” This sounds sensible. But pinpointing the actual health effects caused by built environments can be as maddeningly confusing as urban sprawl itself. Disentangling the role of the built environment from confounding factors such as ethnicity, genetics, and lifestyle is forbiddingly difficult. Many researchers seeking a way out of this maze have settled on housing as a potent focal point for research. A growing number of studies indicate that the design, quality and location of housing all warrant attention in disease risk factor surveillance. In Vancouver, for example, a batch of studies funded by the Mental Health Commission of Canada probing the associations between housing security and health outcomes for homeless people has established that housing yields health benefits that strongly justify investments in housing for the homeless. In the Montérégie region of Quebec, the Public Health Department is probing different aspects of housing and built environment to highlight residential and environmental inequalities. Neighbourhoods are being compared based on the proportion of homeowners, the year the house was constructed, distance to leisure, food and health services, access to cycling paths, social and material deprivation, and the presence of sources of air pollution. Substantial evidence indicates that the location of housing is a key variable in the health conditions of residents: At Carleton University, a team led by bio-statistician Paul Villeneuve investigating associations between non-occupational exposure >>CA
RR
FS F
eatu
re...

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
7
CARRFS Feature...to ambient volatile organic compounds and lung cancer based on a case-control study of 445 incident lung cancers and 948 controls in Toronto between 1997 and 2002 tracked exposures linked to residential addresses. It concluded that long-term exposure to ambient volatile organic compounds and nitrogen dioxide at relatively low concentrations is associated with lung cancer. Similarly, a team of Health Canada researchers probing the relative risk of mortality from all non-accidental, respiratory-, and cardiovascular-related causes, associated with exposure to four air pollutants, by weather type and season, in 10 major Canadian cities for 1981 through 1999 found statistically significant relationships of mortality among urban dwellers due to short-term exposure to carbon monoxide, nitrogen dioxide, sulphur dioxide, and ozone. Not all studies of dwelling locations yield such robust findings. Although a recent review of mental health literature on the linkages between depression and neighborhood types by University of Montreal psychologist Dominic Julien supported the notion that some neighborhood variables – especially those related to poverty and material deprivation – impact on mental health, firm proof is scant. “Thus far, there is limited empirical evidence to fully ascertain this notion, and information is even more scarce on the processes that might explain any relationships between neighborhood variables and depressive mood among older adults,” Julien reported. “Although lack of housing is linked with adverse health outcomes, little is known about the impacts of the qualitative aspects of housing on health,” agrees Sean Rourke, scientific director for the Ontario HIV Treatment Network, who closely investigated the association between structural elements of housing, housing affordability, housing satisfaction and health-related quality of life over a 1-year period for 509
individuals living with HIV in Ontario. “We found significant cross-sectional associations between housing and neighborhood variables – including place of residence, housing affordability, housing stability, and satisfaction with material, meaningful and spatial dimensions of housing – and both physical and mental health-related quality of life,” Rourke and his team reported. These findings, Rourke believes, are broadly applicable to the general population. “Housing is
health,” he’s concluded. Research from the UK indicates that poor housing conditions can increase the risk of severe health issues or disability by up to 25 percent in childhood or early adulthood, notes Housing and Health: Examining the Links, a 2012 study published by Toronto’s Wellesley Institute. In recent years, the relationship between housing and physical activity, body weight and obesity has become a central preoccupation for numerous researchers probing built environment impacts. One of the current buzzwords for researchers in this area is “sedentariness” (a term used to define physical inactivity), notes Muhajardine,
who describes obesity as a “gateway condition” for chronic diseases. The design of homes and neighborhoods can be described as a path leading to that gateway: In Ontario, a study revealed that children with a park or playground within 1 km from home were five times more likely to be at healthy weight than children without such access. And children who live in neighbourhoods with fewer amenities or lacking neighbourhood access to sidewalks, walking paths, parks or playgrounds, or recreation or community centres have 45 percent higher odds of being obese or overweight. “The empirical body of evidence regarding the determinants of obesity – especially those most upstream, such as the built environment, time use >>
“Although lack of housing is linked
with adverse health outcomes,
little is known about the impacts of the qualitative
aspects of housing on health.”

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
8
CARRFS Feature (cont’d) and technology change – is only now taking shape,”Muhajarine explains. “We’re at the point now where we need to start doing systematic surveillance. But before we do that we need to agree on common indicators to measure.” Karen Lee, an adjunct professor at the University of Alberta’s School of Public Health who has advised numerous cities on healthy housing, sees the role of housing in health as an emerging literature in Canada. “A lot of the built environment research in Canada has focused on the role of transportation and land use planning” she explains, while noting that much new work has been seeded since the 2009 launch of Healthy Canada by Design Coalitions Linking Science and Action for Prevention, a national network for collaboration in built environment health research and interventions funded by the Canadian Partnership Against Cancer, the Public Health Agency of Canada (PHAC), and the Heart and Stroke Foundation. As part of this project, Toronto Public Health produced software for planners to model how urban planning and transportation planning affect health outcomes. To increase the momentum, the Canadian Institutes of Health Research has adopted built environment as a strategic research area, and the PHAC is working to coordinate the development of a pan-Canadian framework identifying which indicators of built environment health effects warrant surveillance. These may include “urbanization, proximity and accessibility to recreational facilities and parks, neighbourhood walkability, transportation, food production and quality and safety” according to a summary of the issue from PHAC. A growing body of evidence “shows a link between the built environment and its impact on maintaining healthy lifestyles, safer and less polluted communities, and on social inequalities” the
Agency says. “In order to document and follow the trends associated with health and the built environment, a solid evidence base is vital; surveillance systems need to be established based on survey and administrative data.” In Ontario, newly-revised Public Health Standards emphasise that built environment should be viewed as a chronic disease risk factor. To back that up, the
Standards contain a surveillance protocol requiring Boards of Health to collect data on physical environment factors. The province’s Public Health Sector Strategic Plan prioritizes built environment as one of five action areas, stating that it can “play a significant role in improving health and reducing health and social costs, particularly by promoting healthy physical activity and reducing the risk of injuries and social isolation – which lead to better physical and mental health.” Alberta, British Columbia and Quebec have also recognized that built environment matters to public health. Alberta has adopted a Built Environment Health Promotion
Strategy to promote physical activity, nutrition, injury prevention, and environmental safety, as well as to identify common built environment disease risk indictors. In Québec, work is underway to develop surveillance indicators based on six classes of built environment indicators – including density, and land use, road networks, non-motorized transport, and transit infrastructure, and urban design with specific regard to recreational facilities and food shops. <>
“We’re at the point now where we need to start
doing systematic surveillance. But
before we do that we need to agree
on common indicators to measure.”
Built Environment ToolkitBC Provincial Health Services Authority has just launched their Healthy Built Environment Linkages: A Toolkit for Design, Planning, & Health. Read more about the it on CARRFS eNews website.
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
9
Built Environment:
A SUBTLE SUBJECT FOR SURVEILLANCE“The built environment is strongly related to health – but often in quite subtle ways,” argues Candace Nykiforuk, a health geographer and population health researcher at the University of Alberta who has investigated obesity, asthma, smoking, cancer as well as other chronic diseases as the Head of a lab known as the Policy, Location, and Access in Community Environments (PLACE) Laboratory.
“Built environment is a container for how people behave,” Nykiforuk argues. “It helps determine if and when people eat healthy foods, socialize, and exercise. By promoting incidental changes in behavior through changes to the built environment, we can see small changes that may have large impacts.”
For Nykiforuk, although the case is clear for bolstered surveillance, the absence of commonly accepted measurable indicators retards researchers from unravelling how modifications to the built environment can lead to health improvements. “The Canadian evidence is still emerging,” she cautions. “Part of the problem is that the same people finding out how best to measure are also trying to figure out how to intervene.”
Donald Schopflocher, a University of Alberta statistician who frequently co-publishes with Nykiforuk warns against overstating findings from research into built environment impacts.
At the outcome of a 2006–2009 community-based intervention for obesity and chronic disease prevention in four Alberta communities in which “environmental determinants of obesity amenable to intervention” were identified and implemented, the findings were underwhelming, Schopflocher notes.
“Self-reported body mass index showed no change, and neither were there significant changes in behaviors,” reported this study about whether changes to the built environment improved health. “Health outcome indicators at the community level may not be sufficiently sensitive to capture changes which, over a relatively short term, would only be expected to be incremental.”
Donald Schopflocher, University of Alberta
Candace Nykiforuk, University of Alberta
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
10
Built Environment:
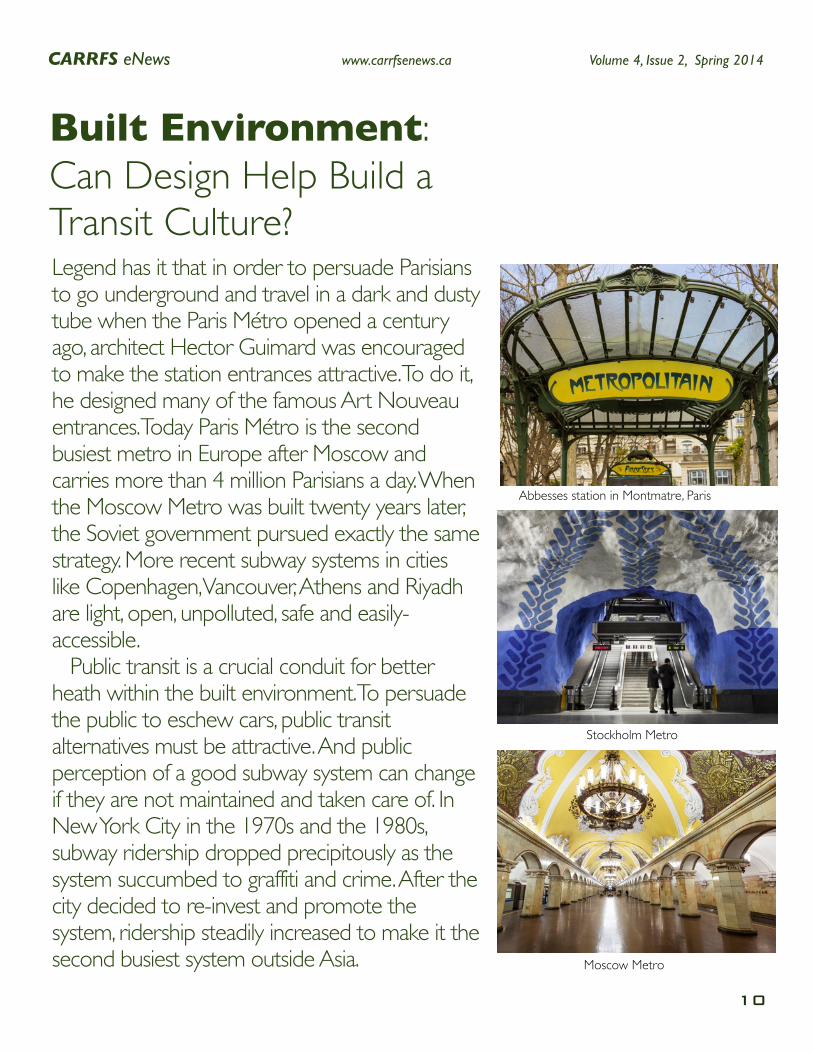
Legend has it that in order to persuade Parisians to go underground and travel in a dark and dusty tube when the Paris Métro opened a century ago, architect Hector Guimard was encouraged to make the station entrances attractive. To do it, he designed many of the famous Art Nouveau entrances. Today Paris Métro is the second busiest metro in Europe after Moscow and carries more than 4 million Parisians a day. When the Moscow Metro was built twenty years later, the Soviet government pursued exactly the same strategy. More recent subway systems in cities like Copenhagen, Vancouver, Athens and Riyadh are light, open, unpolluted, safe and easily-accessible. Public transit is a crucial conduit for better heath within the built environment. To persuade the public to eschew cars, public transit alternatives must be attractive. And public perception of a good subway system can change if they are not maintained and taken care of. In New York City in the 1970s and the 1980s, subway ridership dropped precipitously as the system succumbed to graffiti and crime. After the city decided to re-invest and promote the system, ridership steadily increased to make it the second busiest system outside Asia.
Can Design Help Build a Transit Culture?
Abbesses station in Montmatre, Paris
Stockholm Metro
Moscow Metro
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
11
CARRFS Interview...
Social Determinants
of Health & Built
Environment Dr. David L.
Mowat Medical Officer of
Health, Region of Peel
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
12
CARRFS Interview...How would you describe or define “built environment”? Within the determinants of health, we have a number of environments – political, social, and economic. To this list, I would add the built environment. These environments overlap, of course, and consist of factors that go beyond the individual. In built environment, we have housing and the infrastructure that supports it – transportation, workplaces, and public spaces. In other words, everything that we have built in and around our cities. All of these influence health. And, the natural environment also plays a role. Within cities, we have playgrounds, open spaces, parks, trees, and so on. They also play a part of the urban form. All these have an impact on health in a number of complex and intertwined ways.
As you know - what’s measured gets attention. Region of Peel has defined built environment around seven elements: density; proximity to services and transit; land use mix; street connectivity; road networks and sidewalk characteristics; parking; aesthetics and human scale. How did you select these elements? We developed these elements in partnership with Dr. Jim Dunn at the Centre for Research on Inner City Health, St. Michael's Hospital. His team reviewed the empirical evidence connecting the elements of land use planning using the “realist review” methodology. They identified seven elements most strongly linked to health outcomes and constructed the index around them. They then developed quantitative measures of each element after a strength-of-evidence analysis was done for each. Research-based benchmarks, expert recommendations and similar indices (such as LEED-ND) were used to help set targets. Then there was a consultation process to assess feasibility and test its validity in existing communities in Peel. We know that population density is really important. You need a certain level of density to be able to have viable basic public transit – say a local bus route. For other forms of transit, like an LRT [Light Rail Transit] or subway, you need greater density. The mix of land use, together with density, is reflected in proximity – how close you are to the places you need to go – work, school, stores, services, and so on. Active transportation requires destinations to be close enough to walk or cycle. And not
a lot of people are going to walk or cycle in a low-density environment which is 100% residential. It won’t happen. Unfortunately we have, for a long time, built low-density car-dependent urban environments which can’t support transit and active means of transportation.
Should we care? Yes! In order to solve or prevent potential future health care crisis in the form of obesity, cardiovascular diseases, or diabetes, physical activity, has become an important factor for improving the health status of a population. Normally, when I say physical activity people’s immediate reactions are: “I have to hit the gym” or “We should build more bike paths.” Most people think first of recreational physical activity. I would group physical activity into four types: physical activity at home; physical activity at work; physical activity getting between home and work; and recreational activity. The only one that has not gone
down over the last 30-40 years is recreational activity. In other words, recreational activity is not the problem. The problem is that we have lost the physical activity from our day-to-day life. Our days don’t contain enough physical activity. And most Canadians do not engage enough in regularly recreational activities either. It is a great thing and should be encouraged, but it’s not the problem. The problem is utilitarian physical activity – the physical activity we do going about our daily life. It has been engineered out of our lives and we need to put it back in. >>
“The physical activity we do going about our daily life
has been engineered out of our lives and we
need to put in back in.”
The Regional Transportation Plan (2008)Following 4 of the 10 strategies in the plan are relevant for Heath:Strategy #1: Build a Comprehensive Regional Rapid Transit Network.Strategy #2: Enhance and Expand Active Transportation.Strategy #7: Build Communities that are Pedestrian, Cycling and Transit-Supportive.Strategy #8: Plan for Universal Access.
Source: Health Background Study. Development of Health Background Study Framework. May 27, 2011

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
13
CARRFS Interview (cont’d)How have you, as a medical officer of health in the Region of Peel, managed to get health on the agenda for the city planners? It has been an interesting journey. We started out thinking “what on earth are these planners doing?” After starting to talk to them, we realized that they knew a lot more about this than we did. What gets built is the result not just of what constitutes good planning, but also of political and economic forces that have to be balanced. Planners are interested in having us talk about what you might call the “health justification” for complete and compact communities because people believe that health issues are important. This adds to the other reasons why we need good planning – environmental sustainability, economic sustainability, social cohesion, and quality of life. Another issue is building communities for all ages: it’s much better if there is a mix of ages and people can age without having to move when, for example, they can’t drive any longer. Our elected officials here in Region of Peel – the Council, are very engaged in this issue. They have directed Public Health to work with the regional planning department and municipalities. The political support is there. But it is still a huge challenge – the planning process takes a long time, and in the meantime the GTA is growing fast. In the next 20 years, the GTA’s population will grow by the size of Montreal and Vancouver combined. A lot of that is going to be built on current farmland. At the same time, places like Mississauga and York region are saying “Can’t we improve what we have”? The Province now has rules which force municipalities to intensify and increase density and provide more transportation options rather than only building for cars. So, how do we actually get this solved? One thing we have done in Peel is to develop a health index which is based on the seven elements we discussed. The index has been adopted by our municipalities. What they can do now is to take a developer’s plan for a new subdivision and run it through the index and say – how does your plan score in supporting healthy living?
What are the concrete steps that the Region of Peel is taking? The prevalence of diabetes is rising very fast. We know that in 2006, one in ten adults in Peel had diabetes. By 2026, it is going to be one in six. A lot is due to aging, some due to ethno-cultural make-up – we know that South Asian and people from the Caribbean have higher risks of diabetes and they are an increasing part of our population. We have to turn this around. Individual
behavioural change on its own is not going to do it. We have to change the environment to one that makes healthy behaviours, especially physical activity, possible. We are working with planners and politicians to look at increasing density, doing better on land-use mix, on connectivity, having better infrastructure for cycling and walking with better sidewalks and bike trails. The other thing is that we have to invest in public transit. The typical transit user is going to walk 19 minutes on the outbound journey and another 19 minutes on the home journey. We know that if people use active means of transportation - including transit to get to and from work, we would take a huge step in meeting the recommendation for physical activity of 150 minutes a >>
Seven Core Elements
DensityDensity refers to a measurement of the number of families, individuals, employees, dwelling units, households or housing structures per unit of land area.Higher residential densities not only result in a more efficient use of land, but also increase a community’s ability to support a variety of services and facilities within proximity, which in turn support walkability and physical activity outcomes.
Service ProximityService proximity refers to the optimal distance between particular uses to maximize their accessibility (i.e. living near jobs and services, or even better, to have jobs and services provided where one lives).
Land Use MixLand Use Mix refers to the mix of uses either within a building or an area of land.The achievement of mixed use forms of development can contribute to positive health outcomes by promoting service/use proximity, more compact urban development and subsequent walkability.
Street ConnectivityStreet connectivity is defined as a system of streets with multiple routes and connections serving the same origins and destinations.
Road Network and Sidewalk CharacteristicsThe overall framework for transportation mobility as it specifically relates to roads and their hierarchy. The road network provides access and allows for the movement of people, goods and services through an area. It also includes opportunities for alternative modes of transportation such as bicycle lanes and pedestrian pathways.
ParkingRefers to a prescribed level of parking (both car and bicycle) that must be provided for a specific development.
Aesthetics and Human ScaleRefers to a development that is of a human scale in its size, position and details relate to passersby in a way that makes them feel comfortable rather than intimidated.
Source: Health Background Study. Development of Health Background Study Framework. May 27, 2011
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
14
CARRFS Interview (cont’d) week - something the majority of the Canadian do not meet today. But if we can get people out of the single occupancy car, we have made a huge impact. Having said that, it is really difficult and definitely a long-term enterprise. There has been some progress. In the last 10 years, a lot of high-rise development has been built around Square One in Mississauga . Of the population growth that occurs from now on – 40 percent are going to be housed within the existing built boundaries. The goal is to achieve a density of 50 residences plus jobs per hectare over all. In designated city centres like Square One, it has to hit 200 - for downtown Toronto it is already 700. We will see a change with more storefronts on the street, more mixed developments and LRT. Central Brampton will be developed in the same direction.
What role do you see epidemiologists having today and how do you think the profession will evolve over the next 5-10 years? We are fortunate to have excellent epidemiologists here. I am excited about what they can do for us. There are four epidemiologists, a supervisor, a manager and five data analysts. There are another three epidemiologists and two data analysts for the infectious diseases section. My experience talking to academics is that they are very keen to have the opportunity to solve real problems. We have worked with people from many universities on projects we have funded or received grants, to look at initiatives such as the development of our health index. Another project has been to build “what if ” scenarios around e.g. diabetes:
What would be the likely impact of increasing physical activity? I find that the information we have been given by the epidemiologists - especially when it has been put into graphic form, can be very persuasive. We need that kind of information to influence stakeholders and politicians. Scenario analysis combined with visualized data is very powerful. Stakeholders listen when you show them – “if
you do this, then this will likely happen.” Epidemiologists can go beyond producing data to provide communication tools for decision making. It is not enough to just work in terms of risk factors or mortality/morbidity data but to show: What is this costing us in dollars? How can this be visualized in the form of an info-graphic? Why do we need better transit in the GTA? Some of the data have we develop ourselves. But we find it helpful if we can link up with epidemiologists in academia and with e.g. Statistics Canada. Statistics Canada is excellent to work with and they have access to datasets which we cannot access ourselves. The Institute for Clinical Evaluative Sciences (ICES) is another example. But again, producing data costs money. We can’t practice public health without data. It is fundamental. Of a budget of approximately $82 million, we spend about 1.8% on data collection and analysis. It’s a good investment. <>
By Jostein Algroy
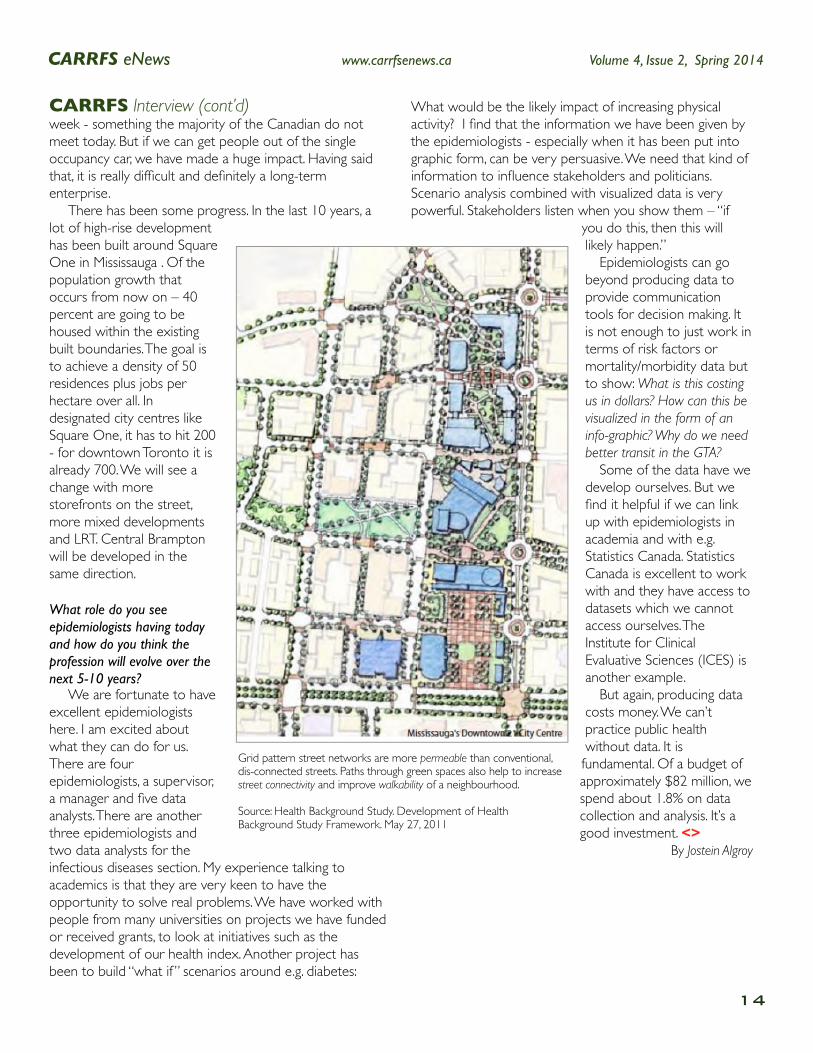
Grid pattern street networks are more permeable than conventional, dis-connected streets. Paths through green spaces also help to increase street connectivity and improve walkability of a neighbourhood.
Source: Health Background Study. Development of Health Background Study Framework. May 27, 2011
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
15
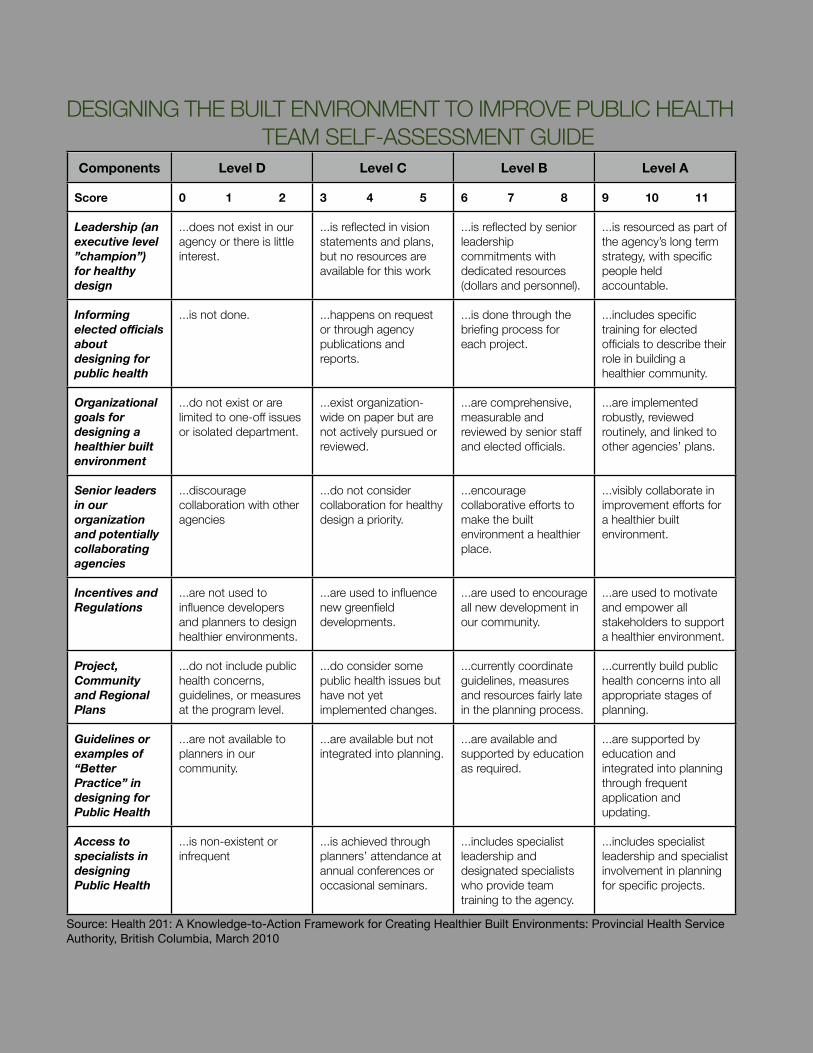
DESIGNING THE BUILT ENVIRONMENT TO IMPROVE PUBLIC HEALTH TEAM SELF-ASSESSMENT GUIDE
Components Level D Level C Level B Level A
Score 0 1 2 3 4 5 6 7 8 9 10 11
Leadership (an executive level ”champion”) for healthy design
...does not exist in our agency or there is little interest.
...is reflected in vision statements and plans, but no resources are available for this work
...is reflected by senior leadership commitments with dedicated resources (dollars and personnel).
...is resourced as part of the agency’s long term strategy, with specific people held accountable.
Informing elected officials about designing for public health
...is not done. ...happens on request or through agency publications and reports.
...is done through the briefing process for each project.
...includes specific training for elected officials to describe their role in building a healthier community.
Organizational goals for designing a healthier built environment
...do not exist or are limited to one-off issues or isolated department.
...exist organization-wide on paper but are not actively pursued or reviewed.
...are comprehensive, measurable and reviewed by senior staff and elected officials.
...are implemented robustly, reviewed routinely, and linked to other agencies’ plans.
Senior leaders in our organization and potentially collaborating agencies
...discourage collaboration with other agencies
...do not consider collaboration for healthy design a priority.
...encourage collaborative efforts to make the built environment a healthier place.
...visibly collaborate in improvement efforts for a healthier built environment.
Incentives and Regulations
...are not used to influence developers and planners to design healthier environments.
...are used to influence new greenfield developments.
...are used to encourage all new development in our community.
...are used to motivate and empower all stakeholders to support a healthier environment.
Project, Community and Regional Plans
...do not include public health concerns, guidelines, or measures at the program level.
...do consider some public health issues but have not yet implemented changes.
...currently coordinate guidelines, measures and resources fairly late in the planning process.
...currently build public health concerns into all appropriate stages of planning.
Guidelines or examples of “Better Practice” in designing for Public Health
...are not available to planners in our community.
...are available but not integrated into planning.
...are available and supported by education as required.
...are supported by education and integrated into planning through frequent application and updating.
Access to specialists in designing Public Health
...is non-existent or infrequent
...is achieved through planners’ attendance at annual conferences or occasional seminars.
...includes specialist leadership and designated specialists who provide team training to the agency.
...includes specialist leadership and specialist involvement in planning for specific projects.
Source: Health 201: A Knowledge-to-Action Framework for Creating Healthier Built Environments: Provincial Health Service Authority, British Columbia, March 2010

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
16
Surveillance Facts...Part VI in a series about the Past, Present and Future of Public Health Surveillance. Written by Dr. Bernard Choi, Senior Research Scientist, Chronic Disease Surveillance, Public Health Agency of Canada and CARRFS eNews science writer.
PastLegislation for surveillance was first introduced in 1741 in the Americas, when the colony in Rhode Island passed an act
requiring tavern keepers to report contagious disease among their patrons. In 1743, the colony passed a law requiring the reporting of smallpox, yellow fever, and cholera. This started the concept of compulsory reporting of infectious diseases. In 1776, Johann Peter Frank in Germany advocated that surveillance needs to link to policy development. He suggested a comprehensive form of public health surveillance which dealt with school health, injury prevention, maternal and child health, and public water and sewage treatment. Frank formulated comprehensive health policy which had considerable impact both within Germany and in countries such as Hungary, Italy, Denmark, and Russia that had close cultural contact with Germany.
PresentEvaluation of Surveillance Systems - Limitations have been identified for current surveillance systems: (1) The current surveillance practice is unable to address adequately either current or new potential challenges to public health. (2) The current approach to public health surveillance is fragmented,
as the various systems are not well coordinated. Ongoing public health information systems are not always integrated with public health surveillance and prevention activities. Instead, over time, a collection of independent and poorly coordinated surveillance systems has evolved in response to various needs. (3) It is difficult to address a new emerging health problem because surveillance for the specific problem usually does not exist. New health problems are not detected through the collection of routine surveillance data. (4) Existing surveillance systems may not provide timely data. (5) Inadequate funding has been a problem with current systems of surveillance. Evaluation of Public Health Actions and Practice - When surveillance information is used to plan and implement public health practice (policies, programs), the surveillance system should also serve to evaluate the success of the public health practice. The objective of program evaluation is to determine as systematically and objectively as possible the relevance, effectiveness, and impact of programs with respect to their objectives. The basic principles of program evaluation involve information, expectation, and attribution. Step-by-step guides for program evaluation are available.
FutureImproving Methods of Epidemiologic and Statistical Analysis - Post-survey adjustments are becoming an increasingly important means of maintaining the representativeness of survey data. New
weighting methods have been developed for adjusting the data for sex, age, race, education, marital status, and telephone coverage, and for non-telephone coverage. A number of methodological research areas to improve data analysis in the 21st century include application of capture-recapture methodology to identify missing cases in routine data; conditions in which age-standardized techniques can be used for time trend and geographic comparisons; development of economic analysis models; methodology for multilevel analyses. Improving Methods of Information Dissemination - Since the latter part of the 19th century, the dissemination of surveillance information generally has been done by “weekly reports” of diseases of critical health or strategic importance. In the United States, the Weekly Abstract of Sanitary Reports, published since 1886, has included morbidity and mortality information for most cities and ports of the United States and many countries of the world. Until recently, surveillance information was disseminated as written documents published periodically by government agencies. Although printed paper reports will continue to be produced, there is a need to explore new methods of information dissemination, such as paperless or electronic media. Associated with ready electronic access to detailed personal information from surveillance are ethical and legal concerns that might constrain access to data of potential public health importance. <>
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
17
> MESSAGE > PROFILE > UPDATE >
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
18
Chair’s MessageBetty Reid-White, Chair for the Canadian Coordination Committee, (CCC) gives a status update on CARRFS achievements over the last quarter and what is in store for CARRFS over the months ahead.CARRFS has been steadily moving forward to support and strengthen regional risk factor surveillance across Canada. This work is completed by a network of volunteer professionals who support this agenda.
At the end of January, 2014 the Canadian Coordinating Committee of CARRFS held a face to face meeting in Toronto. Members of the committee were updated on the progress of the individual working groups. Highlights from these groups are as follows:
Training Working Group continues to works toward its goal to develop, promote and deliver opportunities for members to enhance their capacity for risk factor surveillance. They have planned and delivered several e-learning sessions as well as an Eastern Regional Workshop on “Small Area Analysis Using R” in Moncton, New Brunswick in March, 2013.
Tools and Resources Working Group is continuing its work to foster and support the sharing of information, tools and resources. Current activities include the development and maintenance of a searchable inventory of risk factor surveillance tools and resources, initiatives, projects and activities and the development of a social media strategy for membership engagement.
The Surveillance Innovation task group is currently in the process of drafting a discussion paper on “Innovation in Regional Risk Factor Surveillance”. Stay tuned!
Members of the Coordinating Committee also identified deliverables for the fiscal year 2014. Key ideas were brought forward and discussion ensued as how best to move forward. Some of these ideas and discussions included communication strategies, membership engagement, linkages with other agencies, performance measurement and evaluation. In upcoming meetings, the Committee will continue discussion on these ideas and develop a plan of action to enhance the work of CARRFS as we continue to move surveillance forward.
We also added a new member to the Coordinating Committee: Tannis Erickson, Epidemiologist, Cancer Care Manitoba. Welcome Tannis!
Thank you for your continued interest in and support of regional risk factor surveillance as together we continue to work to improve the health of all Canadians.
Betty Reid-White Chair, Canadian Coordination Committee, CCC
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
19
CARRFS Profile...To help build our community, the CARRFS eNews profiles a leading member in each issue. In this issue we profile Larry Svenson, Director, Alberta Ministry of Health.
What is your background? Oddly enough it is not in epidemiology. While I did take a number of courses in epidemiology, I was trained in psychology with a focus on neuroscience. While an undergraduate, I had a particularly good introductory statistics professor. I approached her with an idea to conduct a survey on campus related to knowledge, attitudes and behaviours related to AIDS. I suggested we replicate a study done at Lakehead University. She agreed and managed to obtain funding. We wrote up the results and had them published in the Canadian Journal of Public Health in 1990. Because this was only the second such study in Canada, we were invited to conduct similar surveys with high school students. The University of Alberta used the results to inform a new peer education program that they had set up to try and reduce the risk of HIV/AIDS on campus. The subsequent research we did with high school students led to the St. Albert Protestant School Board voting to place condom vending
machines in their High School. This was the first school in Canada to do so. This sequence of events not only provided me with graduate level training as an undergrad, it showed me the value of evidence and how it could drive actions. What inspired you to become a health professional? I have always been interested in understanding risk factors for various diseases as well as their temporal and spatial distribution. I wanted to better understand the role of things in the environment and how they interacted with one's biology to kick in the disease process. My hope was that by gaining a better understanding of the factors that increased risk or actually determining factors that were in the causal chain, this information could be used to reduce the burden of illness. I liked the challenge of trying to figure out complex interactions, but always with the desire to discover or shine a light on ways to prevent illness. My interests were primarily related to chronic disease with a special interest in neurological disorders like Parkinson’s disease and multiple sclerosis. >>

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
20
CARRFS Profile (cont’d)What do you spend the most time on in your current position? I manage a team for the Alberta Ministry of Health that has responsibility for providing evidence on a range of topics including communicable disease, non-communicable disease, injury, mental health, public health economics, health determinants, risk factors, and other things. Any given day results in needing to consider a diverse set of questions or issues. A lot of time is spent making sure data are available to support analyses that are needed. I also spend a fair bit of time providing updates and advice to senior people in the organization. A large part of the job involves explaining complex issues in simple terms with clear actionable advice. The range of topics makes the job a challenge some days, but also keeps it very interesting. It is not uncommon to be talking about vaccine preventable diseases, infectious disease outbreaks, risk factors for stroke and the burden of injuries all within the same day.
What was your motivation to become a member of the CARRFS? It is hard to say if there is one single reason for joining CARRFS. I believe in the enhancement of capacity to collect and use data for preventing disease and promoting health. CARRFS is about just that. How can we ensure the people that need evidence to act have what they need and are informed of the things they may not have thought about? There is also merit to sharing experiences and approaches in a collaborative manner. It helps to not only gain efficiencies, but to elevate the quality and utility of the work.
How do you see the current role of the CARRFS in Canada today? It may be better to ask CARRFS colleagues that question. I guess I would see it as providing advice and context, particularly to newer members. I have been involved in a number of studies and initiatives over the years and without realizing that it became a bit of the holder of corporate memory and historical developments related to surveillance in Canada. I hope that I bring ideas to the table that others find valuable.
What are the future opportunities for the CARRFS? A big opportunity and challenge for CARRFS will be demonstrating the value of data in improving lives. Getting people excited about data and concerned about disparities and wanting to know how to address issues. CARRFS could simply help share information on surveys and methods, but it could also raise the bar on how data is collected, understood, and used to act. <>
By Jostein Algroy
Call for Interest
Are you interested in and available to contribute to setting strategy for CARRFS ? Do you have time to volunteer? We are looking for members for the working groups (training, tools & resources, and surveillance innovation) and the coordinating committee. These are two-year terms. Each group has a specific focus. The Training Working Group coordinates opportunities including bi-monthly e-Learning sessions and an e-Forum which will be informed by an updated needs assessment. The Tools and Resources Working Group identifies what tools and resources are out there and how to link those who “have” with those who “need”. They are looking at creative ways to make it easier to connect – including more use of our Twitter account and other networking options. The Surveillance Innovation Working Group is still in its initial stages, and there are opportunities to influence the direction that this group takes. The Coordinating Committee provides advice on the operation of CARRFS, and takes the lead in specific areas including the e-Newsletter and web presence. We have openings and would be pleased to hear from you if you want additional information, would like to nominate a colleague, or volunteer yourself. The strength of CARRFS lies in its membership: We encourage your contributions! <>

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
21
CARRFS eNews Website...CARRFS eNews new Website is here to serve the readers of CARRFS eNews.
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
22
The Home page - or the website’s opening page. The home page has three columns: News; Interview; and Feature. The link under each column takes you directly to the selected tab.
The News is the place where short articles that are not published in the newsletter reside. These articles can either be a follow-up on an article/theme that previously has been published or a stand-alone article that comes from the reader or from the editors.
The Interview is where we post the quarterly interviews in the CARRFS eNews.
The Feature is where we post the feature stories in the CARRFS eNews. These stories will incorporate hyperlinks to resource materials for additional information.
The Profile is where we post the quarterly profile of a CARRFS member in the CARRFS eNews.
The Review is where critical reviews of books or reports relevant for the CARRFS community are posted.
The Magazine is where you will find the current as well as back issues of the CARRFS eNews - in both English and French.
The Editorial is information about the editors, writers, the pan-Canadian Editorial Advisory Board and how to get in contact with us and give us feedback on how we are doing
Twitter - We also have established a twitter account @carrfsenews. You can sign up and follow us on twitter. Every new article, news/blog post etc. will be notified on Twitter.
A form will be developed to send feedback to the editors.
And as we move along, the website will be developed to serve our readers better.
We have decided to establish a stand-alone website for CARRFS eNews for three reasons.1: To give the reader easy access to the articles posted on the CARRFS eNews and to make it easy to download the newsletter so as to be able to read the articles directly from the website or a tablet or a smartphone as easily as you would read a print magazine. 2: To allow for interactivity through open dialogue with the readers and between readers in the news section as well as being able to frequently update new information about a topic published in the CARRFS eNews.3: To have a platform to publish articles that have been sent to us from readers and have not found their way into the newsletter due to subject or timing. The website allows us to publish content much more frequently.The CARRFS eNews website is structured with following tabs:
CARRFS eNews Website...
CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
23
Update...Updates from each CARRFS Working Group Chairs on recent activities. All working groups need members. Please get in touch with the Chair or a member of the working group and join!Training Working Group
The last several months have found the Training Working Group busy. At the end of January, we were fortunate to have an e-learning session led by Dr. Valerie Tarasuk from the University of Toronto titled “Food Insecurity in Canada: Health and Policy Implications”. It was very interesting and included an overview of measuring hunger on national surveys, the relationship between food bank statistics and food insecurity prevalence rates, the relationship between food insecurity and health, and demographic factors which impact outcomes. If you would like additional information, get in touch and we will assist you. <>
CARRFS CommitteesCARRFS CommitteesCARRFS CommitteesCARRFS CommitteesCARRFS CommitteesCARRFS CommitteesCanadian Coordination Committee
(CCC)Canadian Coordination Committee
(CCC)Tools and Resources Working Group
(TRWG)Tools and Resources Working Group
(TRWG) Training Working Group (TWG)Training Working Group (TWG)
Chair: Betty Reid-White Chair: Ahalya Mahendra Chair: M. Nawal LutfiyyaCo-Chair: Ali Artaman Co-Chair: Vacant Co-Chair: Audrey Layes
Tools and Resources Working Group
The Tools and Resources Working Group is working on a number of projects that will look at how comparable the different youth health surveys that have been conducted in the different regions are. As part of this work, the TRWG will be hosting a panel at the next CARRFS e-forum on youth surveys. We will have three panelist who have worked on a different youth surveys and we will have an opportunity to have an interesting dialogue on how they developed and what other partners they engaged in order to make their survey a success. <>
Invitation: Training Needs AssessmentThe Training Working Group has invited CARRFS members to complete a training needs assessment using Fluid Survey. We have preliminary data which will help to guide the direction in what training to provide over the next several years. This is the second needs assessment and the group felt the time was right to get input from the network with respect to needs, opportunities and experts who could present on specific topics. If you wish to provide your input, use the following link: http://fluidsurveys.com/surveys/carrfs-4/carrfs-training-needs-assessment/

CARRFS eNews www.carrfsenews.ca Volume 4, Issue 2, Spring 2014
24
Hello & Goodbye...This is the place to welcome new members to the CARRFS Steering Committee - The Canadian Coordination Committee (CCC) and honour those who have to leave the committee to pursue or fulfill other commitments.
Send us your StoryWe urge all members to send us articles for upcoming editions. Since we are promoting a bilingual newsletter, articles will be published in the language they are submitted - English or French. Please submit your story to the CARRFS eNews Editor-in-Chief at [email protected]
Tannis EricksonWe welcome Tannis Erickson as a new member of the Canadian Coordination Committee (CCC). Tannis has been with CARRFS since the very beginning – in the 2008 Think Tank Forum where the idea of CARRFS started. She was involved with the 2009 Symposium as well as the Environmental Scan project and a range of other initiatives. Tannis is an epidemiologist at the CancerCare Manitoba. She has a Masters of Science degree from the Community Health Sciences Department of the Faculty of Medicine at the University of Manitoba. At the CancerCare Manitoba, she works on implementation, analysis and knowledge translation from the Manitoba Youth Health Survey. Tannis sees a huge need for sharing risk factor resources and expertise across the country. She believes that we can learn a lot from each other and that CARRFS is a great
platform from which to accomplish this. She would like to see consistency across jurisdictions in the tools used to collect surveillance data and the indicators that are developed using these tools. This will allow cross-jurisdictional comparability and trend monitoring.
By Jostein Algroy
CARRFS is a network of public health stakeholders interested in working together to build
capacity for regional/local area chronic disease risk factor
surveillance in Canada that will be used for chronic disease
prevention and control.
MANDATE
A sustainable and effective regional/local collection,
analysis, interpretation and use of risk factor data to
inform program and policy decisions in Canada.
VISION
To build and strengthen the capacity for regional/
local risk factor surveillance in Canada.
MISSION
Related Documents











