Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Dr. A.MOHAN KRISHNA M.S.ORTHO, MCh ORTH(U.K)
Consultant Orthopaedic surgeon ,Trauma, Arthroscopy, Arthroplasty Surgeon Apollo hospitals, Hyderabad
Consultant Orthopaedic Surgeon at
www.drmohankrishna.comwww.healthyjointclub.comwww.bonesandjointsclinic.com
www.drmohankrishna.comwww.healthyjointclub.comwww.bonesandjointsclinic.com

Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist.

Boundaries of carpal tunnel:Volarly : transverse carpal ligamentDorsally : Carpal bones, deep volar carpal ligaments and volar interoseeous ligamentsLaterally : scaphoid tuberosity & TrapeziumMedially : Pisiform & hook of hamate
Contents: 9 Tendons and median nerveTendons: The tendon of Flexor pollicis longus4 tendons of Flexor digitorum profundus4 tendons of Flexor digitorum superficialis
Transverse carpal Ligament : Flexor RetinaculumThick fibrous band from the tuberosity of scaphoid & a portion of trapezium to the Pisiform & hook of hamate.



Aberrant Anatomy
- Anamalous flexor tendons- Congenitally small carpal canal- Ganglion cysts- Lipoma- Proximal lumbrical muscle
insertion- Thrombosed artery
Infections
- Septic arthritis- Mycobacterial infections- Lyme disease
Inflammatory conditions
- Flexor tenosynovitis- Connective tissue diseases- Gout or pseudogout- Rheumatoid arthritis
Meatabolic conditions
- Acromegaly- Hypothyroidism- Amyloidosis- Diabetes
Increased canal volume
- Pregnancy- Obesity- Edema- Congestive heart failure





Sensory disturbance
Weakness in thumb abduction
Thenar atrophy

In this test the wrist is flexed upto 90 degrees for a period of one minute. Patient is then asked for the complaints of tingling, numbness an or pain in the first 3 fingers.This test can be quantified by noting the time taken for the symptoms to appear.There are several ways of positioning the wrist for eliciting the test.

Elicitation: Tap over the median nerve as it passes through the carpal tunnel in the wrist.Positive response: a sensation of tingling in the distribution of the median nerve over the hand.
Elicitation: Tap over the median nerve as it passes through the carpal tunnel in the wrist.Positive response: a sensation of tingling in the distribution of the median nerve over the hand.

Gentle pressure directly over carpal tunnel paresthesias in 30 seconds or lessBetter for wrists with limited motionHighest sensitivity/specificity of all physical exam tests
Gentle pressure directly over carpal tunnel paresthesias in 30 seconds or lessBetter for wrists with limited motionHighest sensitivity/specificity of all physical exam tests

Moberg 1958•Static (nl < 6mm) and Moving (nl = < 3mm)•Abnormal = severe nerve compression
Moberg 1958•Static (nl < 6mm) and Moving (nl = < 3mm)•Abnormal = severe nerve compression

Von Frey hairs (1898)Five selected thresholds:- normal (2.83), - light touch (3.61), - protective (4.31), - loss of protective (4.56),- loss of deep pressure (6.56)- Abnormal > 2.83 (eyes closed)
Von Frey hairs (1898)Five selected thresholds:- normal (2.83), - light touch (3.61), - protective (4.31), - loss of protective (4.56),- loss of deep pressure (6.56)- Abnormal > 2.83 (eyes closed)
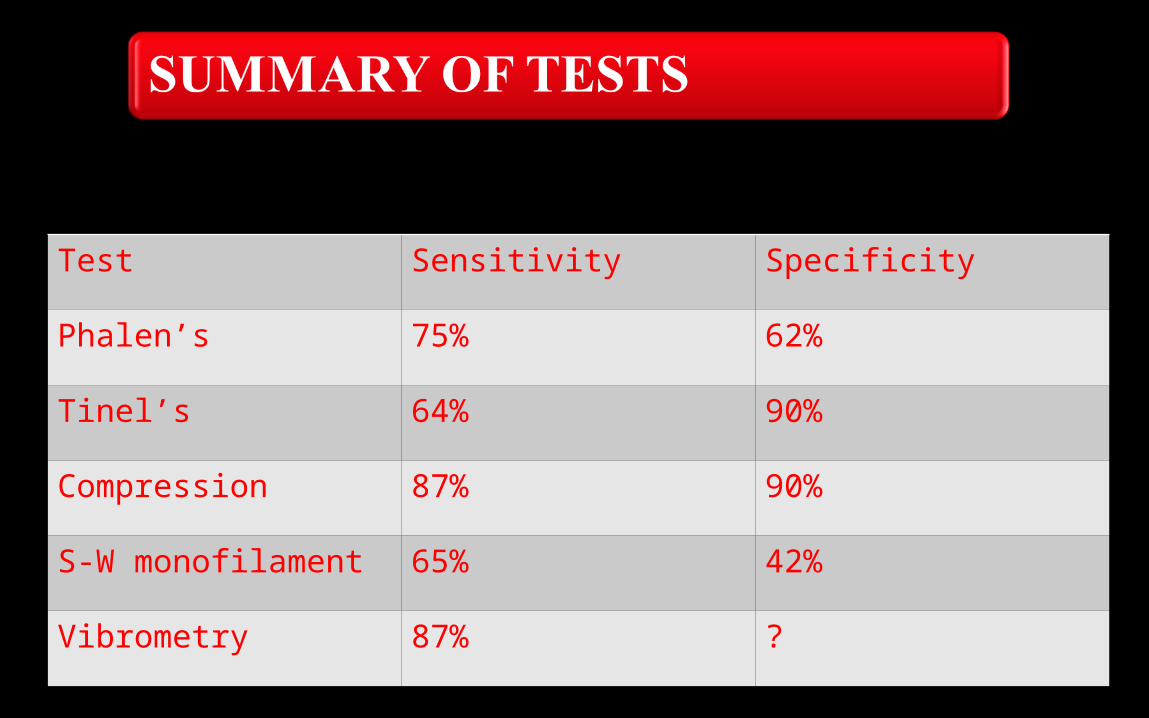
Test Sensitivity Specificity
Phalen’s 75% 62%
Tinel’s 64% 90%
Compression 87% 90%
S-W monofilament 65% 42%
Vibrometry 87% ?

EMG/NCV criteria:-Sensory latencies (DSL)>3.2ms (most sensitive), -motor latencies(DML)>4.2ms.
EMG conduction delay: -distal motor latency >4.5ms for 8cm study; -distal peak sensory latency >4.0ms for 14cm distance; -distal peak compound nerve latency >2.4ms for 8cm study. (AMA Guides 6th ed.)
However:- 8-22% of patients with –ve Electrodiagnostics and +ve clinical signs improve with carpal tunnel release.- In some cases Electrodiagnostics + ve for asymptomatic and –ve for symtomatic
EMG/NCV criteria:-Sensory latencies (DSL)>3.2ms (most sensitive), -motor latencies(DML)>4.2ms.
EMG conduction delay: -distal motor latency >4.5ms for 8cm study; -distal peak sensory latency >4.0ms for 14cm distance; -distal peak compound nerve latency >2.4ms for 8cm study. (AMA Guides 6th ed.)
However:- 8-22% of patients with –ve Electrodiagnostics and +ve clinical signs improve with carpal tunnel release.- In some cases Electrodiagnostics + ve for asymptomatic and –ve for symtomatic
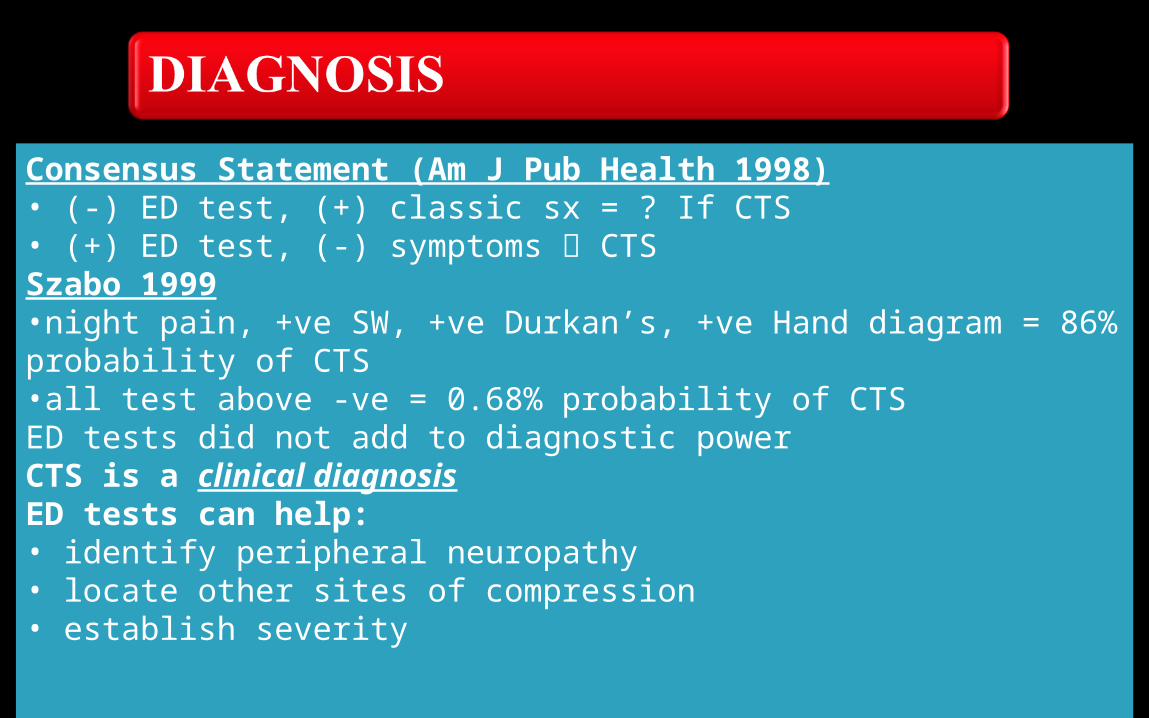
Consensus Statement (Am J Pub Health 1998)• (-) ED test, (+) classic sx = ? If CTS• (+) ED test, (-) symptoms CTSSzabo 1999•night pain, +ve SW, +ve Durkan’s, +ve Hand diagram = 86% probability of CTS•all test above -ve = 0.68% probability of CTSED tests did not add to diagnostic powerCTS is a clinical diagnosisED tests can help:• identify peripheral neuropathy• locate other sites of compression• establish severity






•May be beneficial in the long term management •More studies are needed to confirm it’s usefulness

JBJS Evidence-Based Orthopaedics*“Decompressive Surgery Was Better Than Steroid Injection for Symptomatic and Neurophysiologic Outcomes in Carpal Tunnel Syndrome ”PRCT, ED-proven CTS, 20wk f/uAll injection patients had improvement of Pain, NCV better with surgery (not grip)
McCallister, Trumble JBJS (Am) 2006







Dr.A.MOHAN KRISHNAM.S.Ortho., MCh Ortho(U.K).,Consultant Orthopaedic Surgeon,Apollo Hospitals, Hyderabad.Appointments: Secretary : 09247258989 09441184590 08332936085 www.drmohankrishna.comwww.healthyjointclub.comwww.bonesandjointsclinic.comEmail: [email protected]
Related Documents