Carpal Tunnel Syndrome Oh My Aching Wrist By Jeff Freshour

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Carpal Tunnel SyndromeOh My Aching Wrist
By Jeff Freshour

Definition Carpal Tunnel Syndrome
Chronic pain, numbness, or tingling in the hand, caused by compression of the median nerve in the wrist. It can be caused by repetitive bending and extension of the wrist, as in keyboarding, or by medical conditions such as rheumatoid arthritis and diabetes.
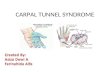
Bound by bones and ligaments, the carpal tunnel is a narrow passageway — about as big around as your thumb — located on the palm side of your wrist. This tunnel protects a main nerve to your hand and nine tendons that bend your fingers. Pressure placed on the nerve produces the numbness, pain and, eventually, hand weakness that characterize carpal tunnel syndrome.

Anatomy
The carpal tunnel is a narrow, tunnel-like structure in the wrist. The bottom and sides of this tunnel are formed by wrist (carpal) bones. The top of the tunnel is covered by a strong band of connective tissue called the transverse carpal ligament.
The median nerve travels from the forearm into the hand through this tunnel in the wrist. The median nerve controls feeling in the palm side of the thumb, index finger, and long fingers. The nerve also controls the muscles around the base of the thumb. The tendons that bend the fingers and thumb also travel through the carpal tunnel. These tendons are called flexor tendons.

Anatomy

Symptoms of PresentationCarpal Tunnel Syndrome
typically starts gradually with a vague aching in your wrist that can extend to your hand or forearm. Other common carpal tunnel syndrome symptoms include:
Tingling or numbness in your fingers or hand, especially your thumb and index, middle or ring fingers, but not your little finger. This sensation often occurs while holding a steering wheel, phone or newspaper or upon awakening. Many people "shake out" their hands to try to relieve their symptoms. As the disorder progresses, the numb feeling may become constant.
Pain radiating or extending from your wrist up your arm to your shoulder or down into your palm or fingers, especially after forceful or repetitive use. This usually occurs on the palm side of your forearm.
A sense of weakness in your hands and a tendency to drop objects.

Diagnosis The diagnosis of carpal tunnel syndrome is suspected based on the symptoms and
the distribution of the hand numbness. Examination of the neck, shoulder, elbow, pulses, and reflexes can be performed to exclude other conditions that can mimic carpal tunnel syndrome. The wrist can be examined for swelling, warmth, tenderness, deformity, and discoloration. Sometimes tapping the front of the wrist can reproduce tingling of the hand, and is referred to as Tinel's sign of carpal tunnel syndrome. Symptoms can also at times be reproduced by the examiner by bending the wrist forward (referred to as Phalen's maneuver).
The diagnosis is strongly suggested when a nerve conduction velocity test is abnormal. This test involves measuring the rate of speed of electrical impulses as they travel down a nerve. In carpal tunnel syndrome, the impulse slows as it crosses through the carpal tunnel. A test of muscles of the extremity, electromyogram(EMG), is sometimes performed to exclude or detect other conditions that might mimic carpal tunnel syndrome.
Blood tests may be performed to identify medical conditions associated with carpal tunnel syndrome. These tests include thyroid hormone levels, complete blood counts, and blood sugar and protein analysis. X-ray tests of the wrist and hand might also be helpful to identify abnormalities of the bones and joints of the wrist.

Treatment Options
For most people, carpal tunnel syndrome will progressively worsen without some form of treatment. It may, however, be modified or stopped in the early stages. For example, if symptoms are clearly related to an activity or occupation, the condition may not progress if the occupation or activity is stopped or modified.
Nonsurgical TreatmentIf diagnosed and treated early, carpal tunnel syndrome can be relieved without surgery. In cases where the diagnosis is uncertain or the condition is mild to moderate, your doctor will always try simple treatment measures first.
Bracing or splinting. A brace or splint worn at night keeps the wrist in a neutral position. This prevents the nightly irritation to the median nerve that occurs when wrists are curled during sleep. Splints can also be worn during activities that aggravate symptoms.
Medications. Simple medications can help relieve pain. These medications include anti-inflammatory drugs (NSAIDs), such as ibuprofen.
Activity changes. Changing patterns of hand use to avoid positions and activities that aggravate the symptoms may be helpful. If work requirements cause symptoms, changing or modifying jobs may slow or stop progression of the disease.
Steroid injections. A corticosteroid injection will often provide relief, but symptoms may come back.

Treatment OptionsSurgical Treatment
Surgery may be considered if you do not gain relief from nonsurgical treatments. The decision whether to have surgery is based mostly on the severity of your symptoms. In more severe cases, surgery is considered sooner because other nonsurgical treatment options are unlikely to help. In very severe, long-standing cases with constant numbness and wasting of your thumb muscles, surgery may be recommended to prevent irreversible damage. The ligament is cut during surgery. When it heals, there is more room for the nerve and tendons.
Surgical technique. In most cases, carpal tunnel surgery is done on an outpatient basis under local anesthesia. During surgery, a cut is made in your palm. The roof (transverse carpal ligament) of the carpal tunnel is divided. This increases the size of the tunnel and decreases pressure on the nerve. Once the skin is closed, the ligament begins to heal and grow across the division. The new growth heals the ligament, and allows more space for the nerve and flexor tendons.
Endoscopic method. Some surgeons make a smaller skin incision and use a small camera, called an endoscope, to cut the ligament from the inside of the carpal tunnel. This may speed up recovery. The end results of traditional and endoscopic procedures are the same. Your doctor will discuss the surgical procedure that best meets your needs.
Recovery. Right after surgery, you will be instructed to frequently elevate your hand above your heart and move your fingers. This reduces swelling and prevents stiffness. Some pain, swelling, and stiffness can be expected after surgery. You may be required to wear a wrist brace for up to 3 weeks. You may use your hand normally, taking care to avoid significant discomfort. Minor soreness in the palm is common for several months after surgery. Weakness of pinch and grip may persist for up to 6 months. Driving, self-care activities, and light lifting and gripping may be permitted soon after .

Surgical Treatment

Outcome Studies
Long-term outcomes
Most patients' symptoms improve after surgery, but recovery may be gradual. On average, grip and pinch strength return by about 2 months after surgery.
Complete recovery may take up to a year. If significant pain and weakness continue for more than 2 months, your physician may instruct you to work with a hand therapist.
In long-standing carpal tunnel syndrome, with severe loss of feeling and/or muscle wasting around the base of your thumb, recovery is slower and might not be complete.
Carpal tunnel syndrome can occasionally recur and may require additional surgery.

Outcome Studies
Conservative treatment of carpal tunnel syndrome: an outcome study of adjunct exercises.
Seradge H, Parker W, Baer C, Mayfield K, Schall L.Orthopaedic & Reconstructive Center, 1044 SW 44th Street, 6th Floor, Oklahoma City, OK 73109, USA.
AbstractWe conducted a prospective study to evaluate the effect of a new non-surgical protocol for treating carpal tunnel syndrome (CTS). It incorporates the Carpal Tunnel Decompression Exercise Program (Exercise Program) into conventional non-surgical treatment. Twenty-eight patients (33 hands) met the inclusion criteria and were followed for 18 months. The outcome measurement tools used were the Symptom Severity Scale (SSS) and the Functional Status Scale (FSS). The outcome tools were administered at admission and repeated at 1, 2, and 18 months after admission to the treatment program. Using the adjunct treatment, 80% of the hands in the mild category and 71% in the moderate category were successfully treated without surgery. All patients in the severe category required surgery. The average success rate of our adjunct non-surgical treatment protocol was 67%, a substantial improvement over the 18% to 34% success rate reported nationally for conventional treatment methods. Furthermore, improvement in the outcome of carpal tunnel syndrome by the adjunct non-surgical treatment can result in significant savings in human suffering, medical cost, lost work time, and socioeconomic distress.PMID: 11799804 [PubMed - indexed for MEDLINE]

Outcome Studies A Prospective, Longitudinal Outcome Study of Patients with Carpal Tunnel
Surgery and the Relationship of Body Mass Index
Venkata KrishnaRao Bodavula,1 Frank D. Burke,2 Norman H. Dubin,1 Mary J. Bradley,2 and E. F.Shaw Wilgis 11The Curtis National Hand Center, Union Memorial Hospital, 3333 N. Calvert Street, #200, Baltimore, MD 21218 USA 2The Pulvertaft Hand Centre, Derbyshire Royal Infirmary, Derby, DE1 2QY UK E. F.Shaw Wilgis, Phone: +1-410-2618413 begin_of_the_skype_highlighting +1-410-2618413 end_of_the_skype_highlighting, Fax: +1-410-554-4363, Email: [email protected].
AbstractThis study investigated whether body mass index (BMI) was associated with effectiveness of carpal tunnel release as measured by physical and self-assessment tests. This prospective, longitudinal study was conducted from March 2001 to March 2003 using 598 cases (hands) diagnosed with carpal tunnel syndrome and scheduled for surgery at The Curtis National Hand Center, Baltimore, Maryland, and at the Pulvertaft Hand Centre, Derby, England. Body mass index was calculated, and demographic, clinical, and functional data were collected preoperatively and at 6-month follow-up. Grip, pinch, and Semmes–Weinstein scores were measured preoperatively and at 6-month follow-up. Levine–Katz self-assessment scores for symptom severity and functional status were measured preoperatively and at 6-month follow-up. Grip and pinch increased, whereas Semmes–Weinstein, symptom severity, and functional scores decreased by 6-month follow-up. Cases with BMI >35 had lower grip strength and higher symptom severity in males and higher functional status in both sexes pre- and postoperatively compared to normal-weight BMI cases. BMI had no relationship to patient satisfaction. Although morbidly obese cases did worse on some physical and self-assessment tests compared to normal BMI cases preoperatively, all improved to the same extent postoperatively regardless of BMI.

Outcome Studies
Carpal tunnel syndrome: cross-sectional and outcome study in Ontario workers Purpose
To carry out an analytic cross-sectional study of Ontario workers with carpal tunnel syndrome (CTS) and to assess workers’ symptoms, functional disabilities, recreational difficulties, and work capability 4 years after treatment of their CTS.
MethodsData were obtained by review of Ontario Workers Safety and Insurance Board (WSIB) files and by completion of self-assessment questionnaires. Inclusion criteria included all workers registered with the Ontario WSIB who were off work with newly diagnosed carpal tunnel syndrome in 1996.
ResultsThere are 3 million workers covered by the WSIB in the province of Ontario. In 1996, 964 of them developed work-related CTS that required time off for treatment. Of these patients 53% were women and 75% had bilateral CTS. Eighty-one percent of the unilateral cases involved the dominant extremity. The average age at the time of claim was 41 years and workers were at the same job type for an average of 7.4 years (unilateral) and 8.5 years (bilateral), respectively. Thirty-nine percent of workers had a history of another tendonitis or epicondylitis. Seventy-five percent of workers had surgery and on average returned to work 3 months later. Four years after treatment, outcome was assessed by self-administered questionnaires, for which there was a 73% response rate. Forty-six percent of workers experienced moderate to severe pain, 47% had moderate to severe numbness, and 40% had difficulty grasping and using small objects. Only 14% were symptom free. Successful return to work was considered to be a return to the same job with or without modifications, and it occurred in 64% of cases. Better clinical outcome scores were found to occur with surgery and abnormal nerve conduction study results. Worse clinical outcome scores were present with repeat surgery and surgical complications. Concurrent diagnoses of either tendonitis or epicondylitis also resulted in worse clinical outcome scores and worse return-to-work outcomes. The average total cost in Canadian dollars to the WSIB exceeded $13,700 per worker for a total cost in excess of $13,200,000 per year. (In 1996, $1 Canadian = $1.365 US.)
ConclusionsThese outcomes indicate that Canadian workers have a large amount of permanent pain and suffering, a large loss of work productivity, and incur a considerable financial cost as a result of work-related CTS.

Thank You
Questions and Comments
Related Documents