Carlos del Rio, MD Hubert Professor and Chair Hubert Department of Global Health Rollins School of Public Health of Emory University Atlanta, Georgia Understanding and Addressing Cultural and Socioeconomic Barriers to Effective HIV Management This program is supported by an educational grant from

Carlos del Rio, MD Hubert Professor and Chair Hubert Department of Global Health Rollins School of Public Health of Emory University Atlanta, Georgia Understanding.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Carlos del Rio, MDHubert Professor and ChairHubert Department of Global HealthRollins School of Public Health of Emory UniversityAtlanta, Georgia
Understanding and Addressing Cultural and Socioeconomic Barriers to Effective HIV Management
This program is supported by an educational grant from

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Faculty Disclosures
Carlos del Rio, MD, has disclosed that he has received consulting fees from Gilead Sciences and Pfizer.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
1. CDC. HIV Surveillance Supplemental Report 2012;17(No. 4). Published December 2012.
Diagnosis of HIV Infection and Population by Race, 2010 (46 States)
Diagnosis of HIV Infection(N = 47,129)
Population, 46 States(N = 292,196,890)
*Hispanic/Latinos can be of any race.Note: Data include persons with a diagnosis of HIV infection regardless of stage of disease at diagnosis. All displayed data have been statistically adjusted to account for reporting delays but not for incomplete reporting.
20%
2%
46%
29%
1% 1% <1%
12%
4%
65%16%
1% 1% <1%
American Indian/Alaska NativeAsianBlack/African AmericanHispanic/Latino*Native Hawaiian/otherPacific IslanderWhiteMultiple races

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
2. CDC. HIV Surveillance Supplemental Report 2012;17(No. 4). Published December 2012.
Diagnosis of HIV Infection Among MSM Aged 13-24 Yrs
*Hispanic/Latinos can be of any race.Note: Data include persons with a diagnosis of HIV infection regardless of stage of disease at diagnosis. All displayed data have been statistically adjusted to account for reporting delays and missing risk-factor information, but not for incomplete reporting. Data exclude men who reported sexual contact with other men and injection drug use.
By Race, 2007-201046 States and 5 US Dependent Areas
American Indian/Alaska Native Asian
Black/African American
Hispanic/Latino*
Native Hawaiian/otherPacific Islander
White
Multiple races
Dia
gn
ose
s (n
)
Yr of Diagnosis2007 2008 2009 2010
5000
4500
3500
3000
2500
2000
1500
1000
500
0
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
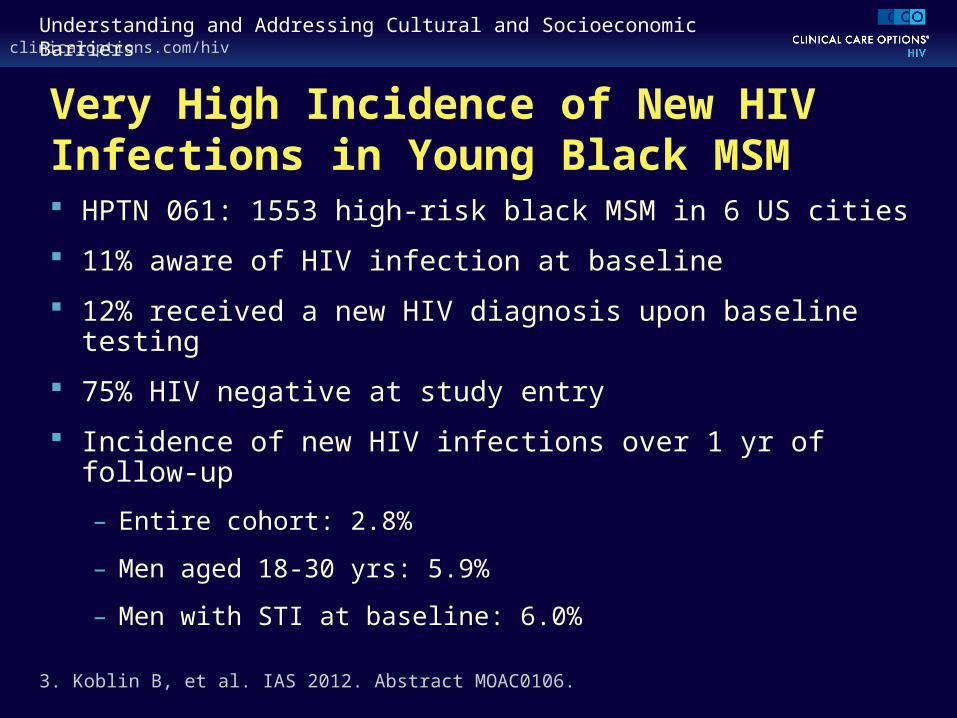
Very High Incidence of New HIV Infections in Young Black MSM HPTN 061: 1553 high-risk black MSM in 6 US cities
11% aware of HIV infection at baseline
12% received a new HIV diagnosis upon baseline testing
75% HIV negative at study entry
Incidence of new HIV infections over 1 yr of follow-up
– Entire cohort: 2.8%
– Men aged 18-30 yrs: 5.9%
– Men with STI at baseline: 6.0%
3. Koblin B, et al. IAS 2012. Abstract MOAC0106.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
4. CDC. HIV Surveillance Supplemental Report 2012;17(No. 4). Published December 2012.
Trends in Age-Adjusted* Annual Rates of Death due to HIV Disease
*Standard: age distribution of 2000 US population.†Hispanic/Latinos can be of any race.The racial/ethnic categories other than Hispanic/Latino are all non-Hispanic/non-Latino. Note: For comparison with data for 1999 and later yrs, data for 1990-1998 were modified to account for ICD-10 rules instead of ICD-9 rules.
By Race, United States, 1990-2008
Dea
ths
per
100
,000
P
op
ula
tio
n
60
50
40
30
20
10
090 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08
Black/African AmericanHispanic/Latino†
American Indian/Alaska NativeWhiteAsian/Pacific Islander

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
WIHS: Black HIV+ Women Twice as Likely to Die of AIDS Than White HIV+ Women
Black race predicted reduced adherence to HAART but remained associated with AIDS death after adjusting for adherence
5. Murphy K, et al. CROI 2012. Abstract 1045.
N = 1471 women on continuous HAART
0
20
0 5 13
4
8
12
16
12111098764321Yr
White
Other
Black
0
20
0 5 13
4
8
12
16
12111098764321Yr
White
Other
Black
AIDS Death Non-AIDS Death
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
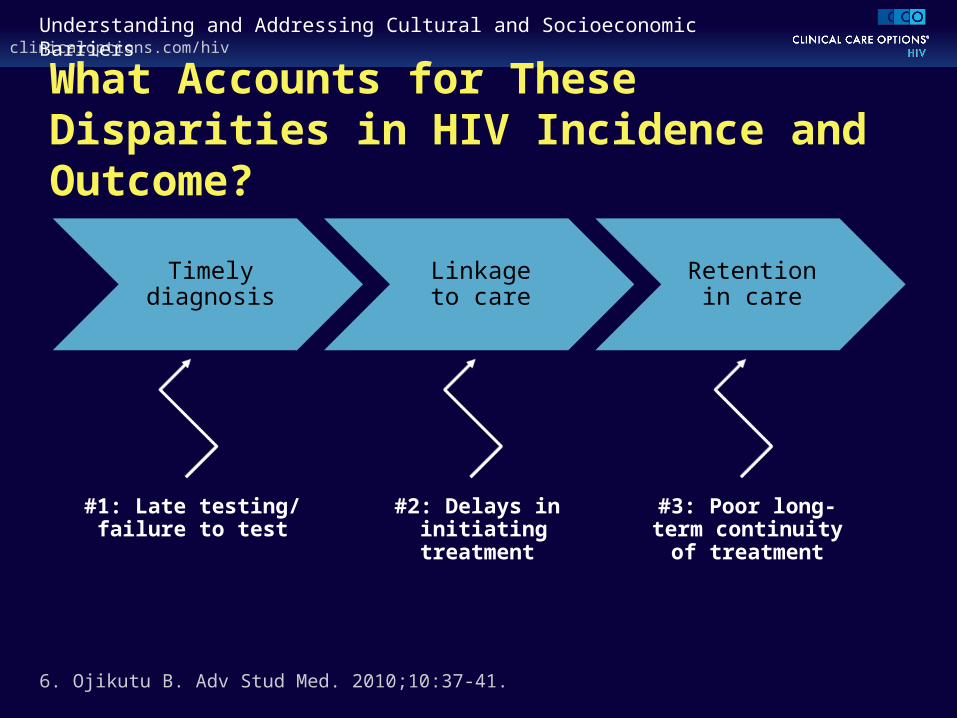
What Accounts for These Disparities in HIV Incidence and Outcome?
#1: Late testing/failure to test
#2: Delays in initiating treatment
#3: Poor long-term continuity of
treatment
6. Ojikutu B. Adv Stud Med. 2010;10:37-41.
Timely diagnosis
Linkage to care
Retention in care
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
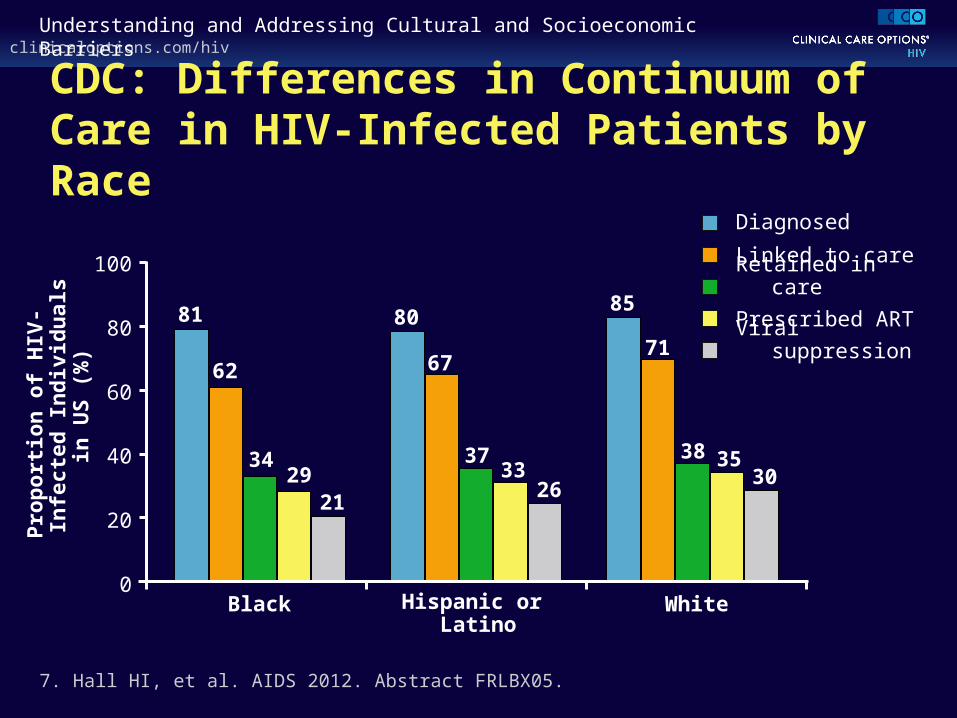
CDC: Differences in Continuum of Care in HIV-Infected Patients by Race
7. Hall HI, et al. AIDS 2012. Abstract FRLBX05.
100
80
60
40
20
0Black Hispanic or
LatinoWhite
81
62
80
67
3733
26
85
71
38 3530
3429
21
Pro
po
rtio
n o
f H
IV-I
nfe
cted
In
div
idu
als
in U
S (
%)
Diagnosed
Linked to care
Retained in care
Prescribed ART
Viral suppression

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Addressing Specific Aspects of Care: Late Diagnosis and Missed Testing Minorities less likely than whites to receive HIV testing
45% first tested within 1 yr of AIDS diagnosis
Characteristics of these late testers
– Younger
– Exposed through heterosexual contact
– Less educated
– Black or Hispanic
8. CDC. MMWR Morb Mortal Wkly Rep. 2003;52:581-586.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Potential Barriers to Testing in Minorities
Patient-Related Factors Provider-Related Factors
Financial constraints Discomfort with healthcare Limited access HIV-related stigmatization and
discrimination Lack of knowledge about HIV/AIDS Fear of AIDS diagnosis Drug or alcohol use Mental illness
Complacency about risk Feelings of incompetence or
discomfort about high-risk behavior Missed opportunities to offer testing
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Tools to Increase HIV Testing
Opt-out testing
Incorporate testing into routine care
Use reminder mechanism to prompt testing
Increase outreach, education
Work with community business organizations that have the trust of the minority community
– eg, churches, barber shops, nail salons
Assure patients of confidentiality
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Addressing Specific Aspects of Care: Delays in Initiating HIV Care Characteristics associated with delay to HIV care or treatment
– Black,[10,11] Hispanic[12]
– No insurance[11]
– Less education[11]
Delays in HIV care > 3 mos[12]
– 56% more likely in black vs white patients
– 53% more likely in Hispanic vs white patients
Among patients with access to care, no disparity in outcomes by race, despite lower adherence in minorities[13]
10. Bhatta MP, et al. Am J Med Sci. 2010;339:133-140. 11. Anthony MN et al. AIDS Care. 2007;19:195-202. 12. Turner BJ, et al. Arch Intern Med. 2000;160:2614-2622. 13. Silverberg MJ, et al. J Gen Intern Med. 2009;24:1065-1072.
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Clinicians’ Attitudes May Result in Withholding or Delay of ART in Minorities Minority race often associated with perceived nonadherence;
may led to withholding/delay of ART[14-16]
In earlier study (1996-1998), 89% of HCPs said adherence an important factor in decision to prescribe PIs[17]
– Explained delayed use of PIs in minorities, women, poor
In MACH14, lower adherence among black patients not explained by differences in demographics, depression, or substance abuse[17]
– Possible contributing factors: mistrust of HCPs, health illiteracy, healthcare system inequities
14. Bogart LM, et al. Med Decis Making. 2001;21:28-36. 15. Thrasher AD, et al. J Acquir Immune Defic Syndr. 2008;49:84-93. 16. Simoni JM, et al. J Acquir Immune Defic Syndr. 2012;60:466-472. 17. Wong MD, et al. J Gen Intern Med. 2004;19:366-374.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Delay of ART in Substance Abusers
18. Westergaard RP, et al. J Int AIDS Soc. 2012;15:10.
CD4+ Cell Count200 cells/mm3
CD4+ Cell Count 350 cells/mm3
Pro
vid
ers
Lik
ely
to D
efer
AR
T (
%) No injection drug use
Abstinent x 3 mos
Occasional injecting
Daily injecting
CD4+ Cell Count 500 cells/mm3
100
80
60
40
20
0
90
70
50
30
10
*
*
P = .03*
*
*
*
*P < .001

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Discrimination, Distrust, and Adherence
Responses in a midwestern survey[19]
– 71% reported discrimination in HIV treatment based on race
– 66% reported discrimination based on socioeconomics/class
HIV Cost and Services Utilization Study[20]
– 40% of respondents reported discriminatory healthcare
– 24% of respondents reported some mistrust of HCPs
– More discrimination → greater distrust, weaker beliefs regarding treatment benefit → poorer adherence
19. Bird ST, et al. AIDS Patient Care STDS. 2004;18:19-26.20. Thrasher AD, et al. J Acquir Immune Defic Syndr. 2008;49:84-93.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Challenging Stereotypes Regarding Readiness for and Adherence to ART Assessing ART readiness is critically important
Provide adherence support
Understand the patient’s social situation and challenges
Other possible strategies
– Support groups
– Peer educators
– Treatment buddies
– Case managers

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Addressing Specific Aspects of Care: Poor Long-term Continuity of Treatment Single-center study from Vanderbilt Clinic[21]
– Lower percentage of time on ART for black vs nonblack patients (47% vs 76%; P < .001)
– Higher mortality in black patients; difference gone after adjusting for time on ART
Single-center study from UAB-Birmingham[22]
– Black race associated with higher risk of missed clinic visit within first yr of HIV care (OR: 2.74; 95% CI: 1.77-4.23)
– Missed visit within first yr of care associated with higher mortality risk (HR: 2.90; 95% CI: 1.28-6.56)
21. Lemly DC, et al. J Infect Dis. 2009;199:991-998. 22. Mugavero MJ, et al. Clin Infect Dis. 2009;48:248-256.
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
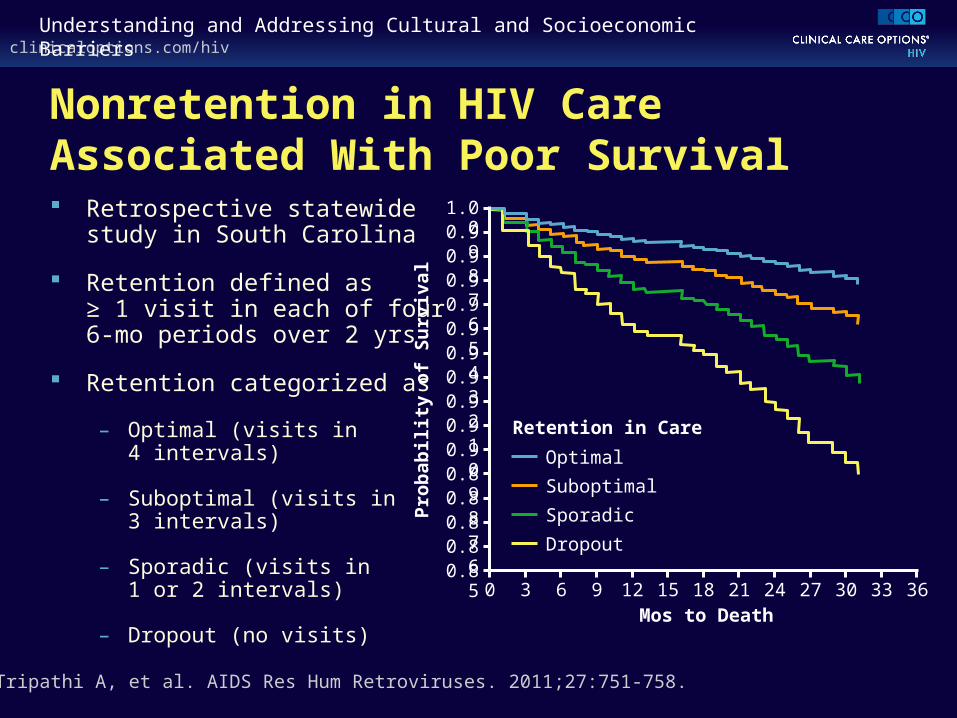
Nonretention in HIV Care Associated With Poor Survival Retrospective statewide
study in South Carolina
Retention defined as ≥ 1 visit in each of four 6-mo periods over 2 yrs
Retention categorized as
– Optimal (visits in 4 intervals)
– Suboptimal (visits in 3 intervals)
– Sporadic (visits in 1 or 2 intervals)
– Dropout (no visits)
23. Tripathi A, et al. AIDS Res Hum Retroviruses. 2011;27:751-758.
1.000.990.980.970.960.950.940.930.920.910.900.890.880.870.860.85
360 3 6 9 12 15 18 21 24 27 30 33Mos to Death
Pro
bab
ilit
y o
f S
urv
ival
Retention in Care
Optimal
Suboptimal
Sporadic
Dropout

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Evidence-Based Recommendations for Entry Into and Retention in HIV Care Systematic monitoring of successful entry into HIV care
recommended for all individuals diagnosed with HIV
Brief, strengths-based case management recommended for individuals with a new HIV diagnosis
– ATRAS: evidence-based intervention
Consider intensive outreach for individuals not engaged in medical care within 6 mos of new HIV diagnosis
Consider using peer or paraprofessional patient navigators
24. Thompson MA, et al. Ann Intern Med. 2012;156:817-833.
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
ARTAS: Best Practice for Linkage to Care
CDC-sponsored multicenter, controlled intervention study
– Conducted in university[25] and community[26] settings
Intensive, short duration, time limited
Interventions client centered/strengths based
79% (497/626) entered medical care within first 6 mos[26]
Median time spent per client: 5.8 hrs (mean: 7.2 hrs)
25. Gardner LI, et al. AIDS. 2005;19:423-431. 26. Craw JA, et al. J Acquir Immune Defic Syndr. 2008;47:597-606.
Manual available at:http://www.cdc.gov/hiv/topics/cba/pdf/artas_implementation_manual.pdf

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
HIV in the New Millennium: A Social/ Medical Nexus
Mental Illness
Poverty Drugs
Infectious Diseases
HIV

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
What Might Patients Need to Stay in Care?
Common needs
– Mental health services
– Substance abuse treatment
– Benefits advocacy
– Childcare
– Transportation
– Companion services
– Respite care
27. Stone V, et al. HIV/AIDS in US Communities of Color. Springer. 2009.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Culturally Competent Care May Improve Communication, Trust Know the culture personally
Provider interpreter services
Recruit, retain staff representative of patient community
Recognize role of traditional healers
Provide culturally appropriate pamphlets, activities in relevant languages
Include family, community in care
Ask patients what they need and address those needs
– Make the clinic a desirable place to go28. Stone V, et al. HIV/AIDS in US Communities of Color. Springer. 2009.
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Examples of Considerations That May Improve Communication/Trust Some patients prefer to be called by formal name[29]
Direct eye contact important for some patients[29]
Explain why information is needed before asking; be aware of potential mistrust[29]
Be aware of importance of religion, spirituality[29]
– Allow religious items at bedside
– Be aware of importance of prayer, including group prayer
Some patients may be less comfortable with psychosocial talk[30]
29. Cichicki M. Living With HIV: A Patient’s Guide. McFarland & Co Inc Publishers. 2009.30. Beach MC, et al. J Gen Intern Med. 2010;25:682-687.
clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Specific Considerations for Latino Patients “Latino” applies to a heterogeneous ethnic group representing
different countries, cultures, lifestyles, norms[31]
Within Latino population, there is variability in[31]
– HIV exposure risk factors
– Education level
– Access to medical, psychosocial care
Less acculturation among Latinos associated with[32]
– Less testing for HIV, HCV
– Greatly likelihood of testing HIV positive
31. Corales RB. AIDS Read. 2007;17:87. 32. Kelley CF, et al. AIDS Read. 2007;17:73-88.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Disparities Can Be Overcome: The Ryan White HIV/AIDS Program Integrated federally funded multidisciplinary program
designed to deliver comprehensive HIV care for the economically disadvantaged
Program components
– Primary care
– Specialty care (substance abuse, mental health)
– Supportive care (case management, nutrition, adherence, emergency assistance, transportation)
33. Moore RD, et al. Clin Infect Dis. 2012;55:1242-1251.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Effective HIV Care Overcomes Disparities
Outcomes in 6366 patients treated in Baltimore, Maryland, between 1995 and 2010
87% of patients receiving ART
Median HIV-1 RNA: < 200 copies/mL
Median CD4+ cell count: 475 cells/mm3
OIs: 2.4/100 patient-yrs; mortality 2.1/100 person-yrs
Expected longevity for HIV-infected patients: 73 yrs
No differences in outcomes by demographic group
34. Moore RD, et al. Clin Infect Dis. 2012;55:1242-1251.

clinicaloptions.com/hivUnderstanding and Addressing Cultural and Socioeconomic Barriers
Conclusions
Nature of HIV epidemic continues to change
Cultural factors can significantly affect access, retention in HIV care
Culturally competent care can reduce barriers
Comprehensive HIV care improves outcomes, reduces disparities

Go Online to Earn CME Credit for This Activity on Overcoming Cultural and
Socioeconomic BarriersClinical Focus: concise online CME-certified module with large slide thumbnails paired with supporting text discussion by Carlos del Rio, MD, and interactive polling questions
clinicaloptions.com/CulturalBarriers
Related Documents











