Cariology 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cariology
1
Dental caries
“It is an infectious microbiologic disease of the teeth that results in localized dissolution and destruction of the calcified tissues.”
2

Classification
Anatomic site
Pit & fissure Smooth surface Proximal
Cervical
Root surface
Rate of progression Active or Acute
Arrested or Chronic
3
classification
Hard tissue involved Enamel
Dentin
Cementum Etiology Radiation
According to age Nursing bottle Geriatric caries
4

classification
According to researchers G.V. Black
Mount & Hume
5

Rampant caries
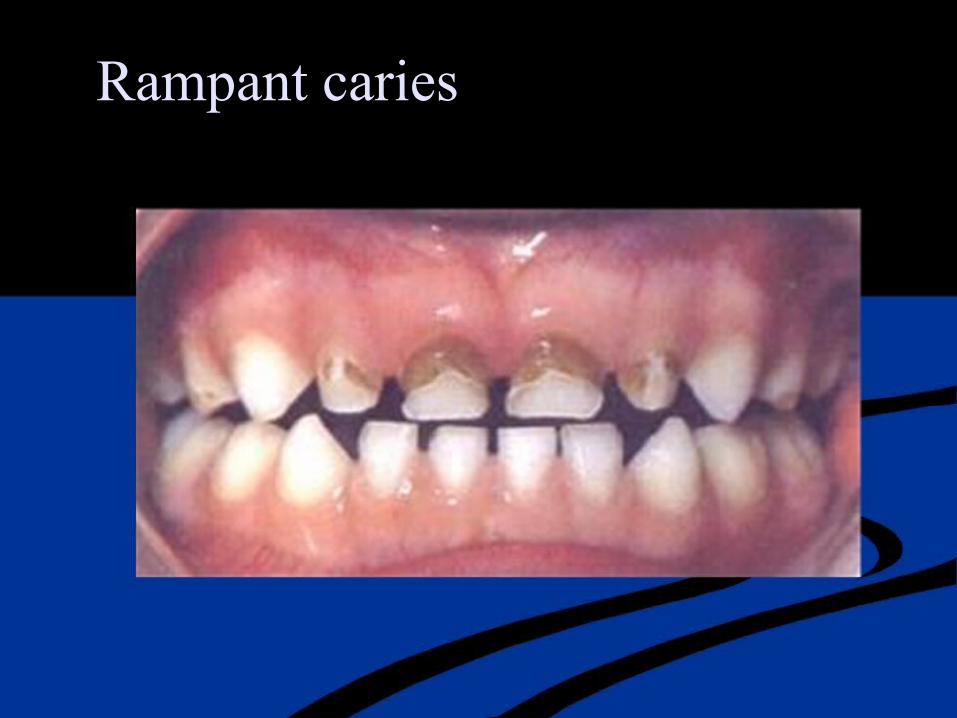
Rampant caries

Few facts
Sucrose greatly stimulates plaque metabolism
Periods of demineralization & remineralization
Some 200 to 300 species of bacteria, yeast & protozoa present in oral cavity
MS----primary organism associated with caries in man
8
Dental plaque
“A gelatinous mass of bacteria adhering to the tooth surface”
9
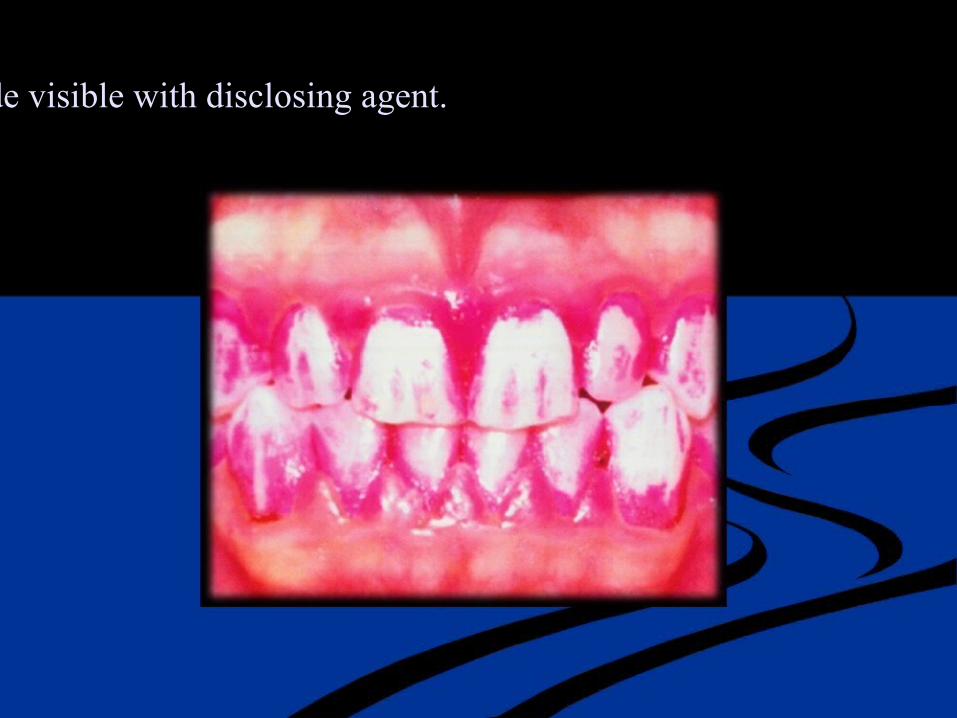
Dental plaque made visible with disclosing agent.
Hypothesis concerning the etiology of caries
Nonspecific plaque hypothesis All plaque is pathogenic
Specific plaque hypothesis
Recognizes plaque as pathogenic only when signs of associated disease are present
11

New Caries Treatment Based on the Medical Model
Etiology MS infection Symptoms Demineralization lesions
Treatment, symptomatic Restoration of cavitated lesions
Treatment, therapeutic Eliminate MS infection
Posttreatment assessment, Examine teeth for new lesions symptomatic
Bacteriologic testing for MS Post treatment assessment,
therapeutic
12

Theories of Cariology
Acidogenic theory
Proteolysis theory
Microbiotic Secretions theory
13
Acidogenic theory
Dental decay is caused by acids produced by microbial enzymatic action on ingested carbohydrates. These acids will decalcify the inorganic portion of the teeth; then the organic portion is disintegrated, creating cavities.
14

Proteolysis theory
Organic portion of the tooth is attacked first by certain lytic enzymes, leaving inorganic portion without a matrix
support, causing it to be washed away, creating cavities
15
Micrbiotic Secretions theory
Metabolic products of MO have the ability to chealate calcium from tooth substances, leaving the organic matrix
to be disintegrated
16

1. A tooth surface without caries. 2. The f irst signs of demineralization.
3. The enamel surface has broken down. 4. A f illing has been made but the demineralization has not been stoppe
5. The demineralization proceeds and undermines the tooth. 6. The tooth has f ractured.
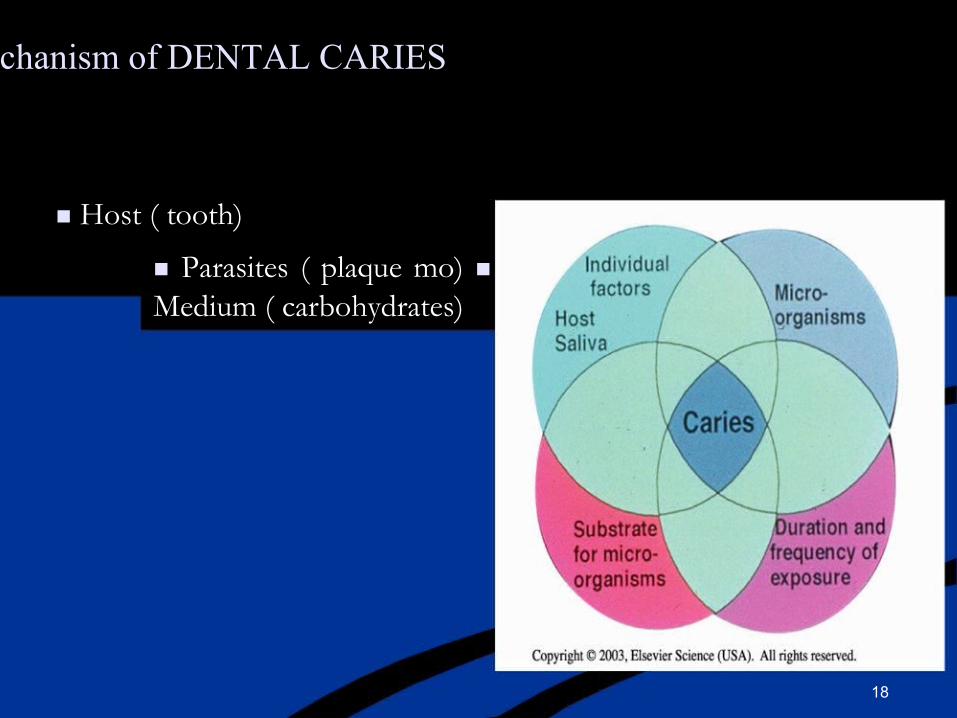
General Mechanism of DENTAL CARIES
Host ( tooth)
Parasites ( plaque mo) Medium ( carbohydrates)
18

Etiology
bacteria food
tooth
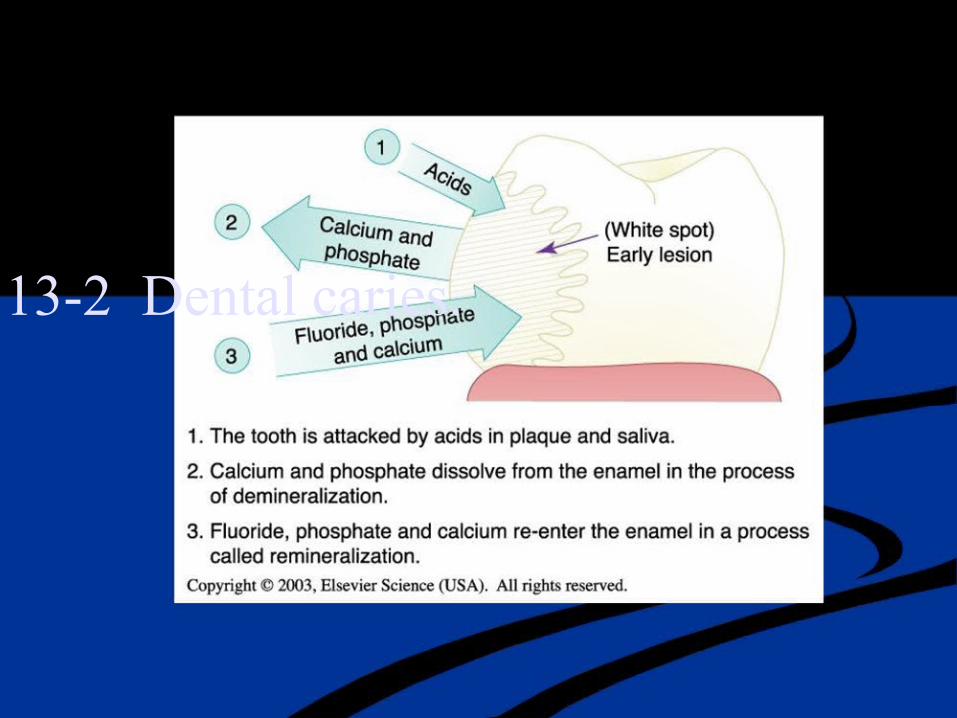
Fig. 13-2 Dental caries.
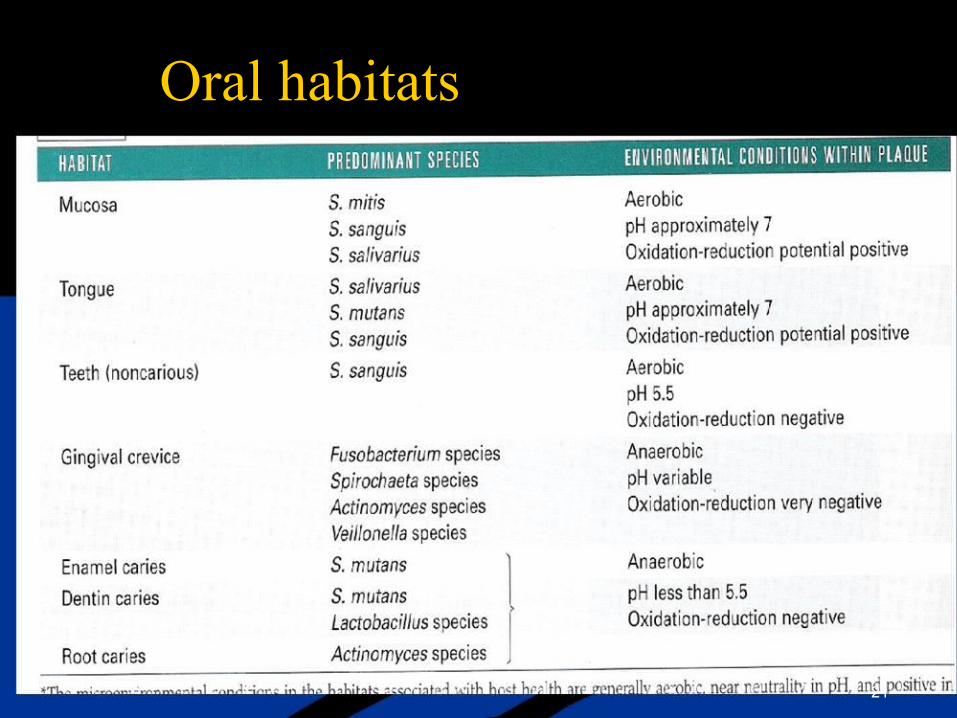
Oral habitats
21

22

Why do you need to restore teeth?
Restoration of damaged tooth structure Maintenance of pulpal vitality
Effective removal of the nidus of infection.
23

24
Stephan’s curve
Demonstrates the acid production of bacteria (pH decrease) with a glucose swallow & the gradual rise due to salivary buffering.
25
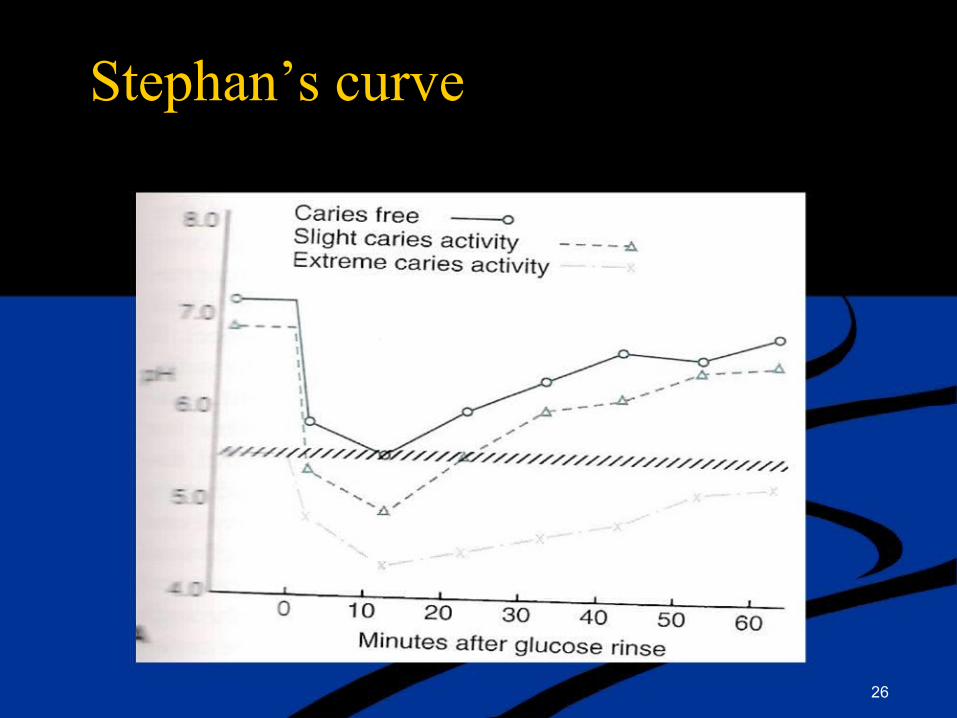
Stephan’s curve
26

Tooth habitats for pathogenic plaque
Pits & fissures
The smooth enamel surfaces Root surfaces
Sub gingival areas
27

Fissure anatomy
28
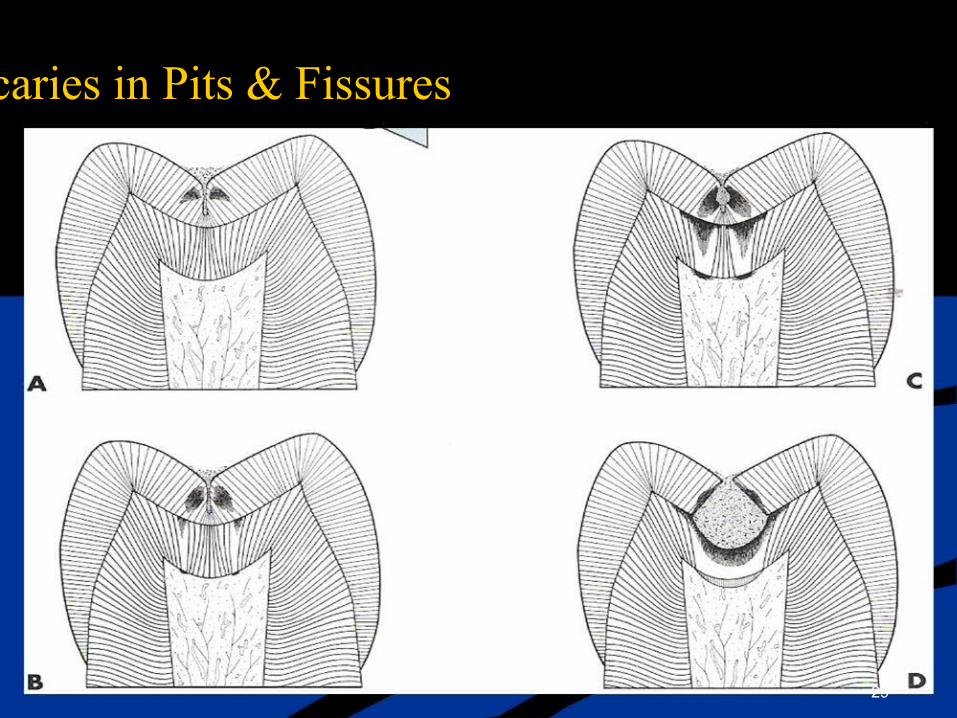
Progression of caries in Pits & Fissures
29
Smooth enamel surfaces
Presence of caries in these areas usually is indicative of a caries active mouth.
The proximal enamel surfaces immediately gingival of the contact area
Col In very young patients, the gingival papilla completely fills
the interproximal space under a proximal contact
30

Initiation & progression on interproximal surfaces
31

Smooth surface caries
32

Cervical Burnout
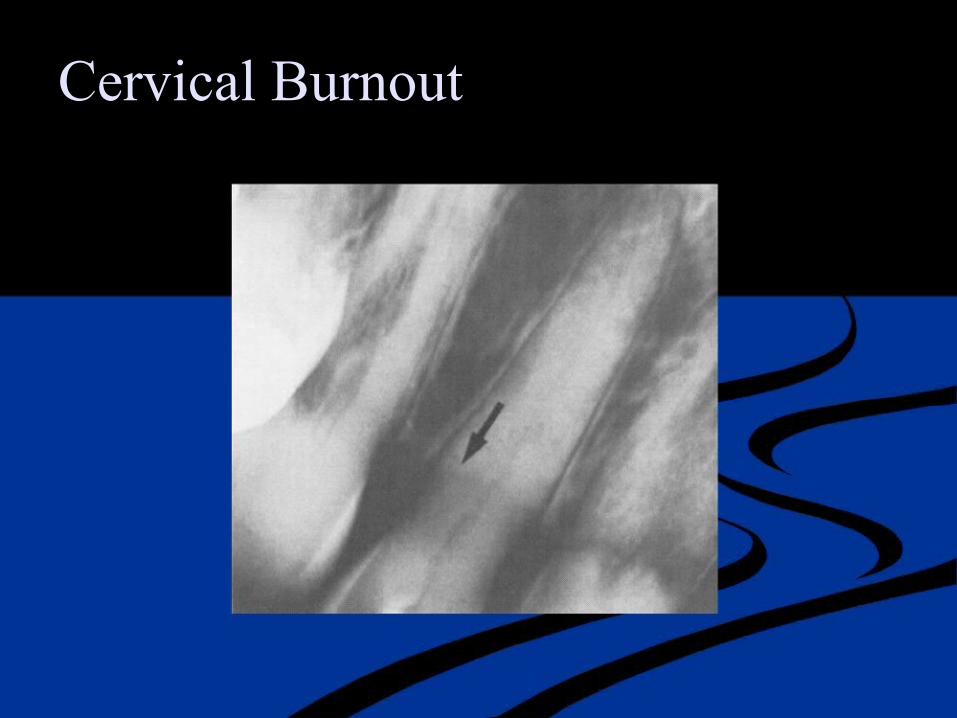
Cervical Burnout
Root surface
Gingival recession
Root caries is alarming b/c rapid progression
Closer to pulp Difficult to restore
Following are more prone to caries Decreased salivary flow
Poor oral hygiene Decreased motivation
35
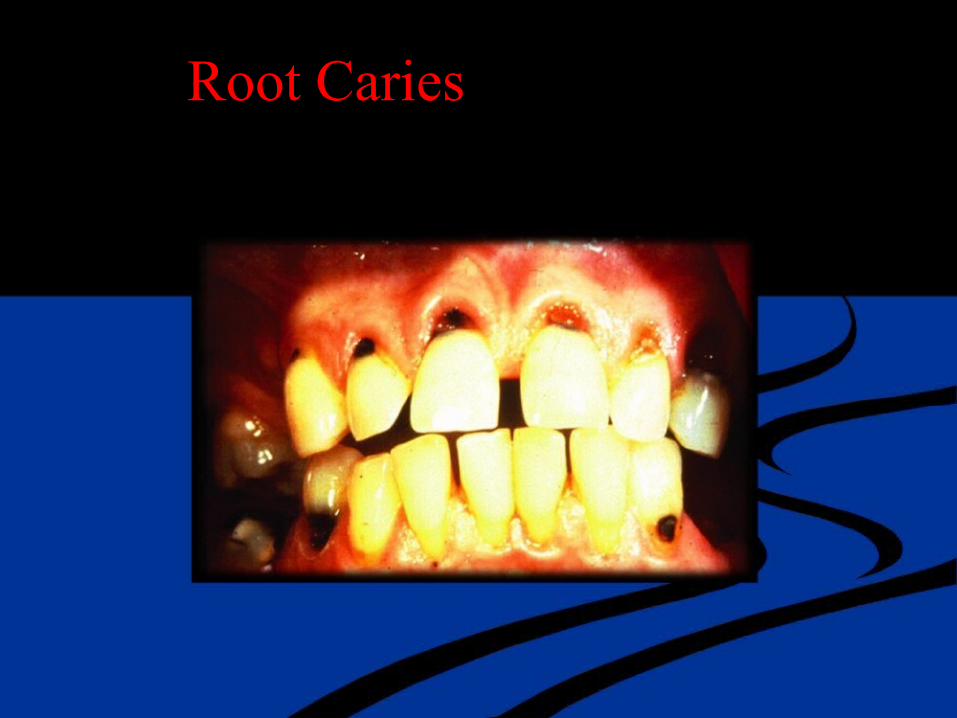
Root Caries
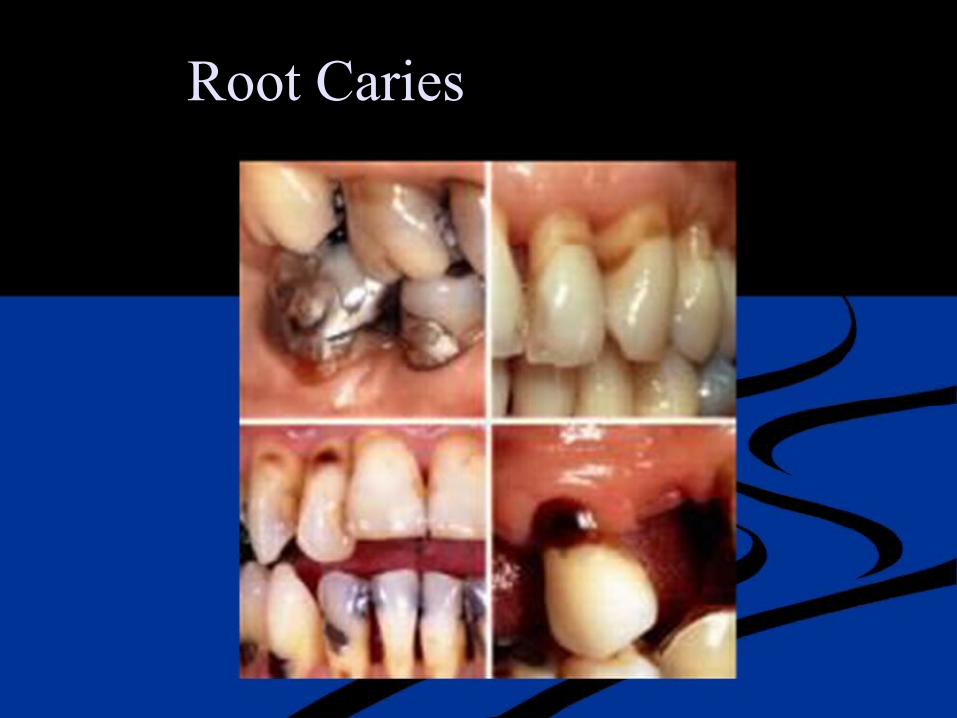
Root Caries

Root Surface Caries

Subgingival areas
Gingival sulcus habitat is unique
Initial occupants of the sulcus are only an extension of the plaque community on the immediately adjacent surface of the
tooth
Immunologic materials may change some characteristics of the adjacent plaque by removing the most susceptible organisms.
Plaque changes progressively from cocci in the supragingival plaque to filamentous bacteria & spirochetes in subgingival
plaque
39

Factors that serve as ecologic determinants
Oral hygiene
Available nutrients Sulcular fluid
Saliva Bacterial clearance
Direct antibacterial activity Buffers
Remineralization
40
Enamel caries
41

Incipient caries/white spot lesion
Initial carious lesion
limited to enamel intact surface but a porous subsurface. Chalky white, opaque Seen only when the surface is desiccated
42
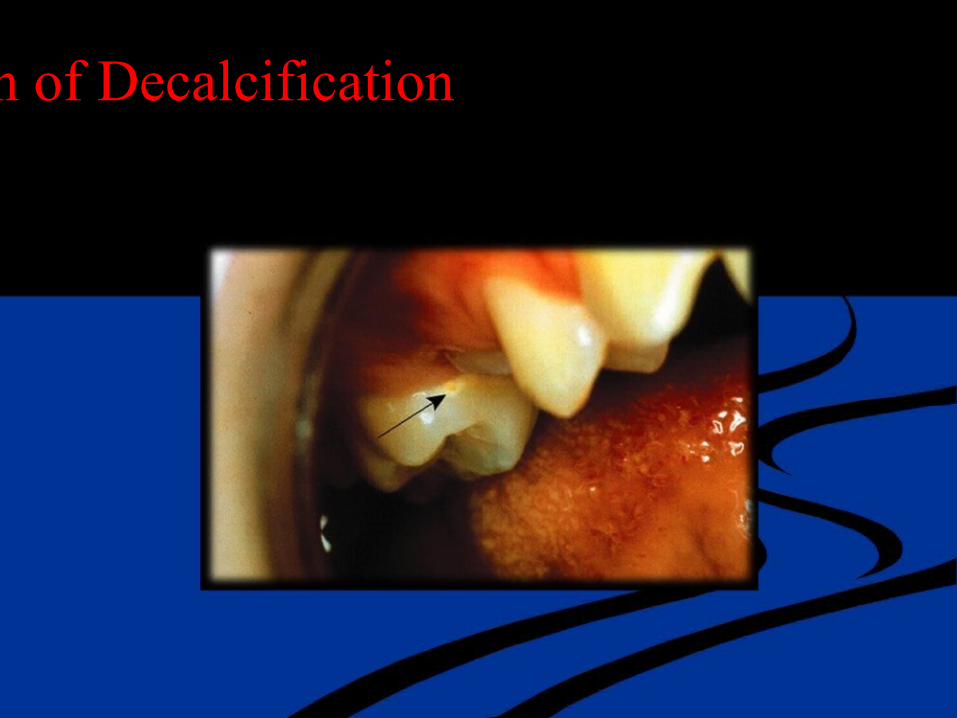
Earliest Sign of Decalcification

Earliest Sign of Decalcification
44

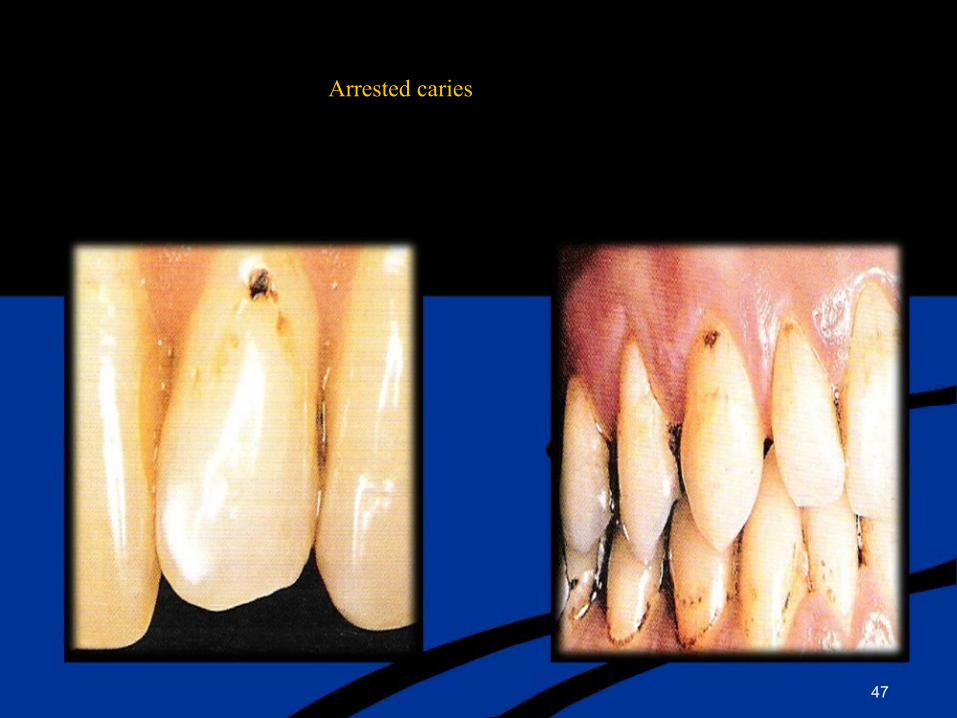
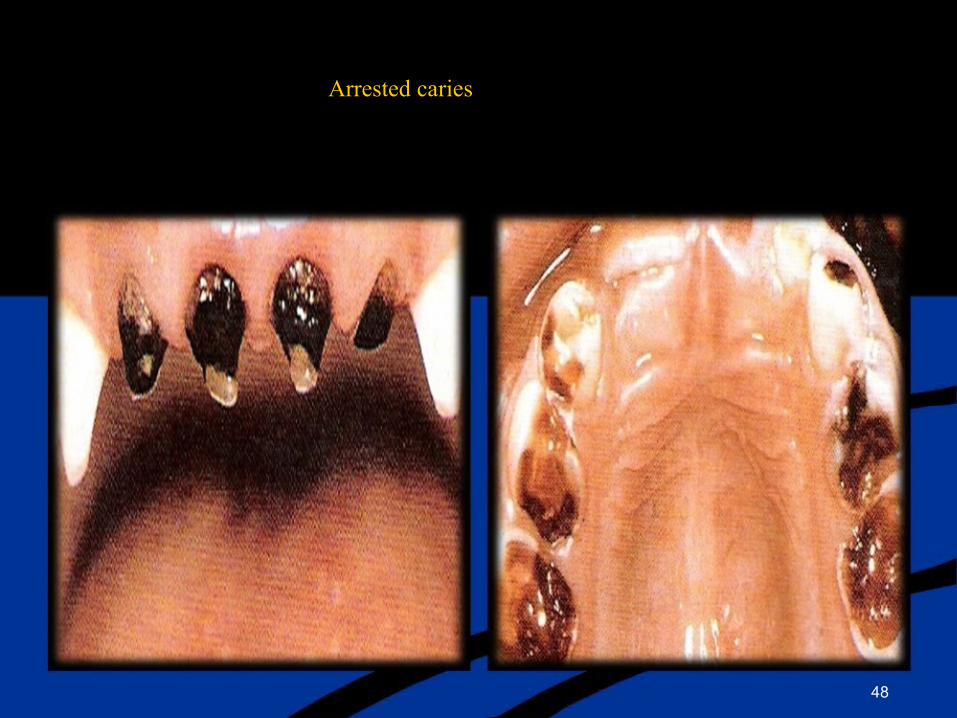
Arrested lesion
It is an intact, but discolored, usually brown or black spot
Shiny surface, hard on excavation
Should not be restored unless esthetically objectionable
45

Arrested caries
46
Arrested caries
47
Arrested caries
48
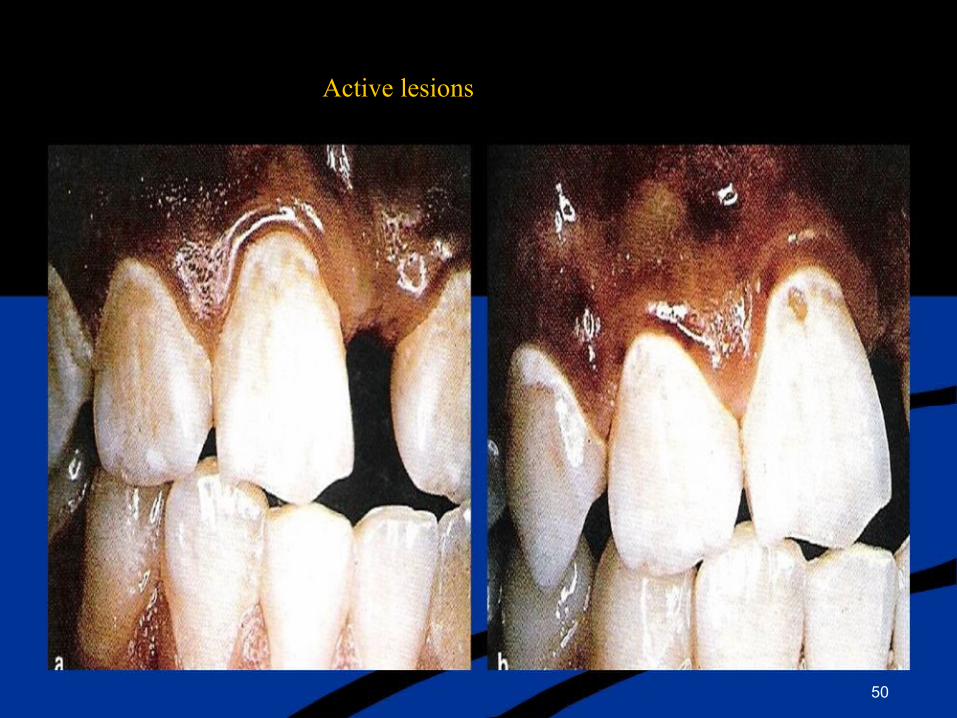
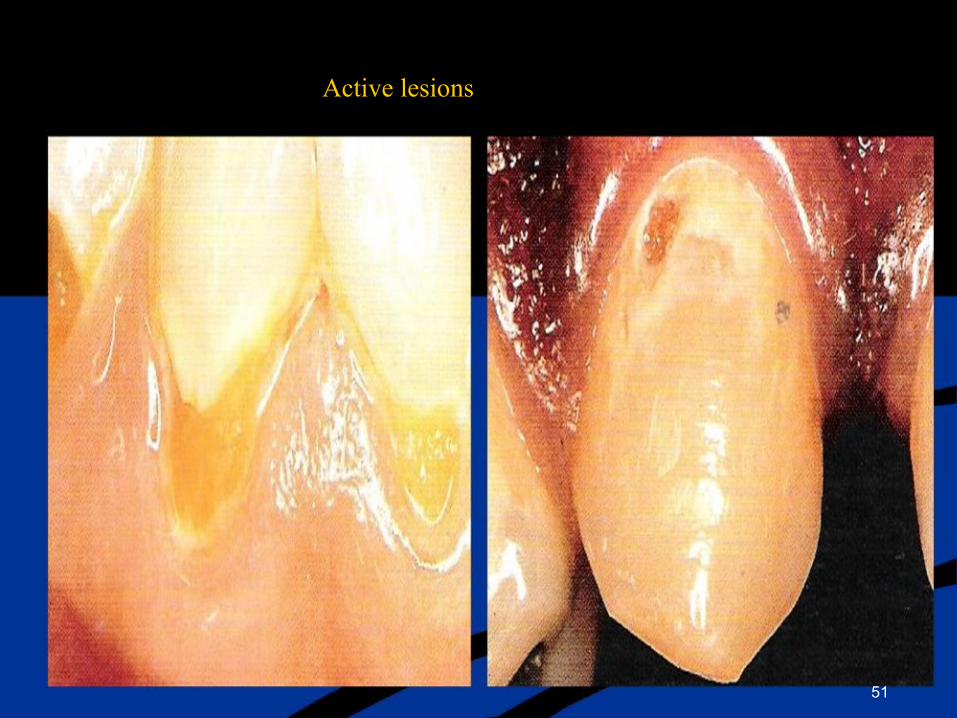
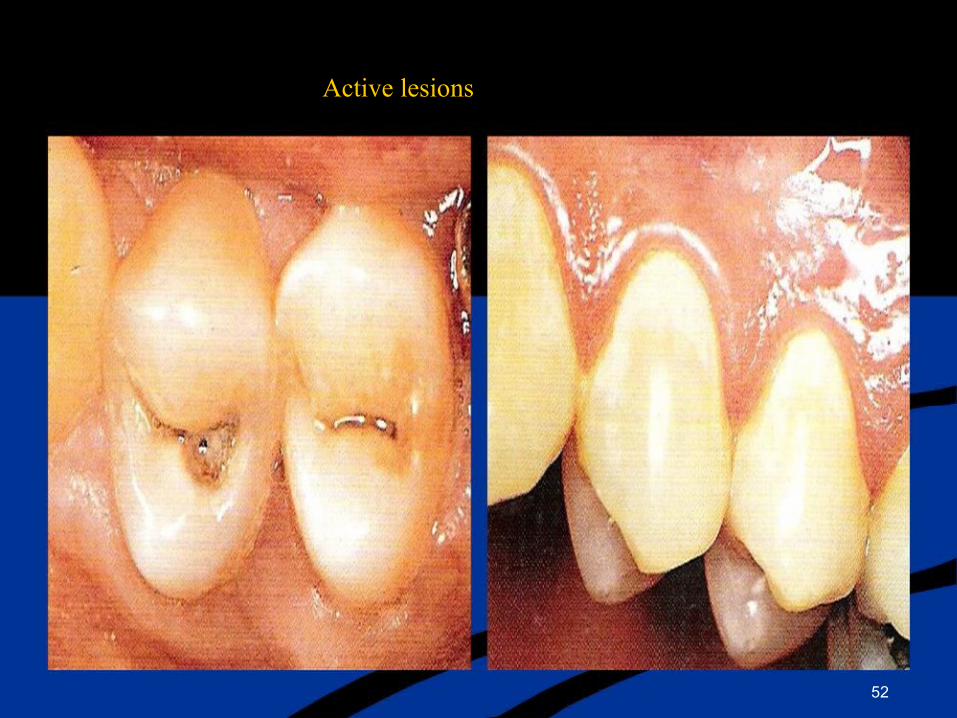
Active lesions
White spot lesions that have a matte or visibly frosted surface or are plaque covered after drying or application of a disclosing agent. Cavitated lesions, including micro cavities as well as cavities exposing dentin.
Soft or leathery in consistency
Lesions visible in dentin on bitewing radiograph
49
Active lesions
50
Active lesions
51
Active lesions
52
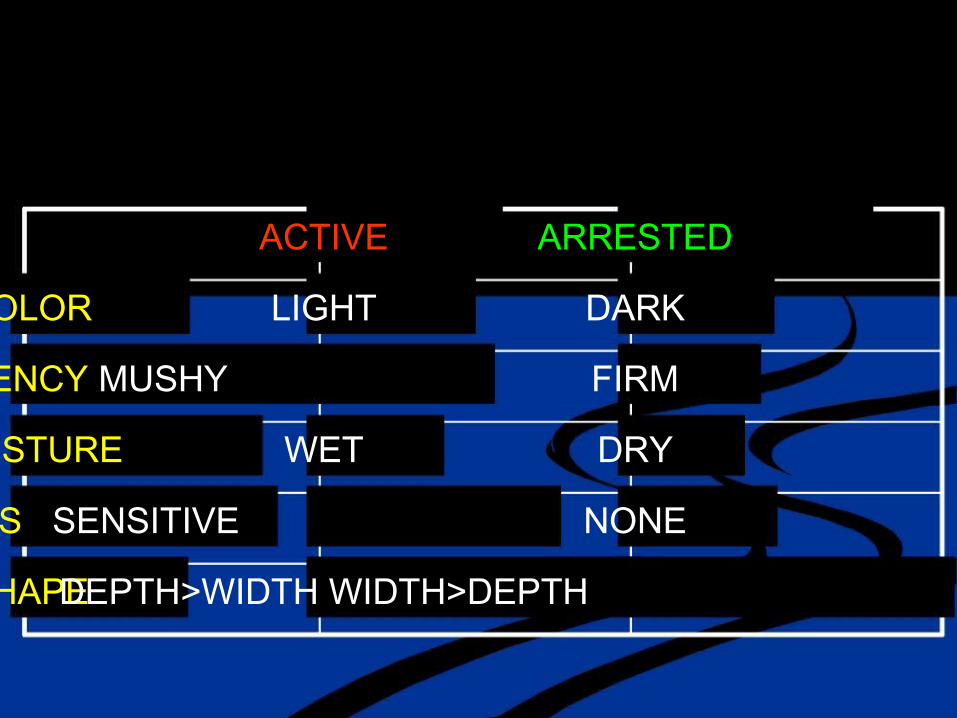
ACTIVE ARRESTED
COLOR LIGHT DARK
CONSISTENCY MUSHY FIRM
MOISTURE WET DRY
SYMPTOMS SENSITIVE NONE
SHAPE DEPTH>WIDTH WIDTH>DEPTH

Recurrent Caries
Recurrent caries
“ Lesion observed under or around the margins or surrounding walls of an existing restoration”
54

Recurrent caries
55
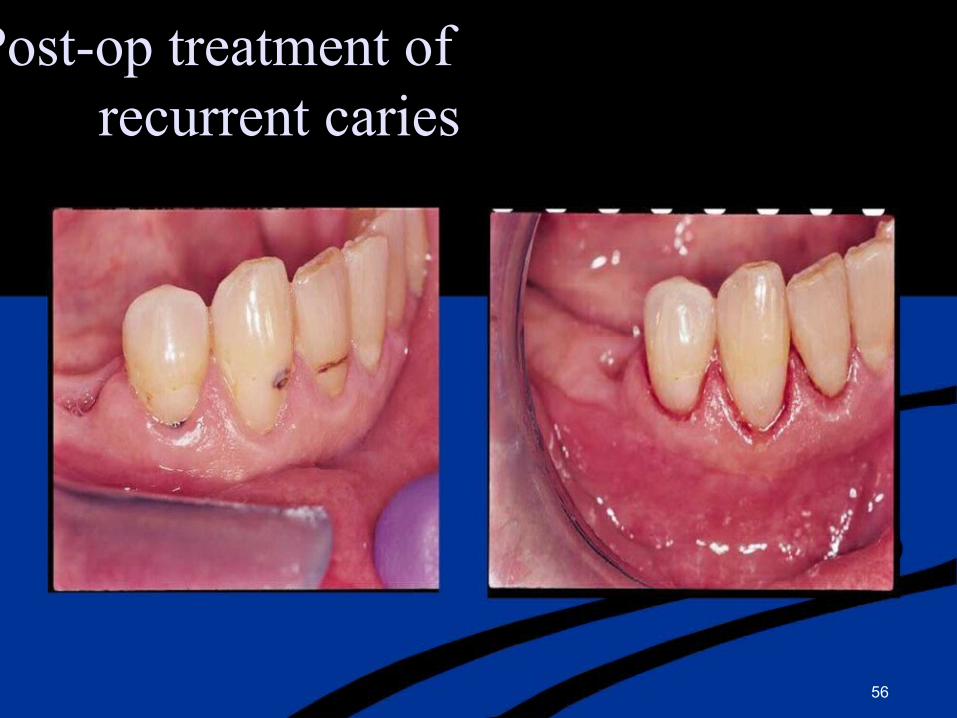
Pre & Post-op treatment of recurrent caries
56

Recurrent lesion
Residual caries
“ Lesion which is not removed during the restorative procedure, either by accident, neglect or intention”
58
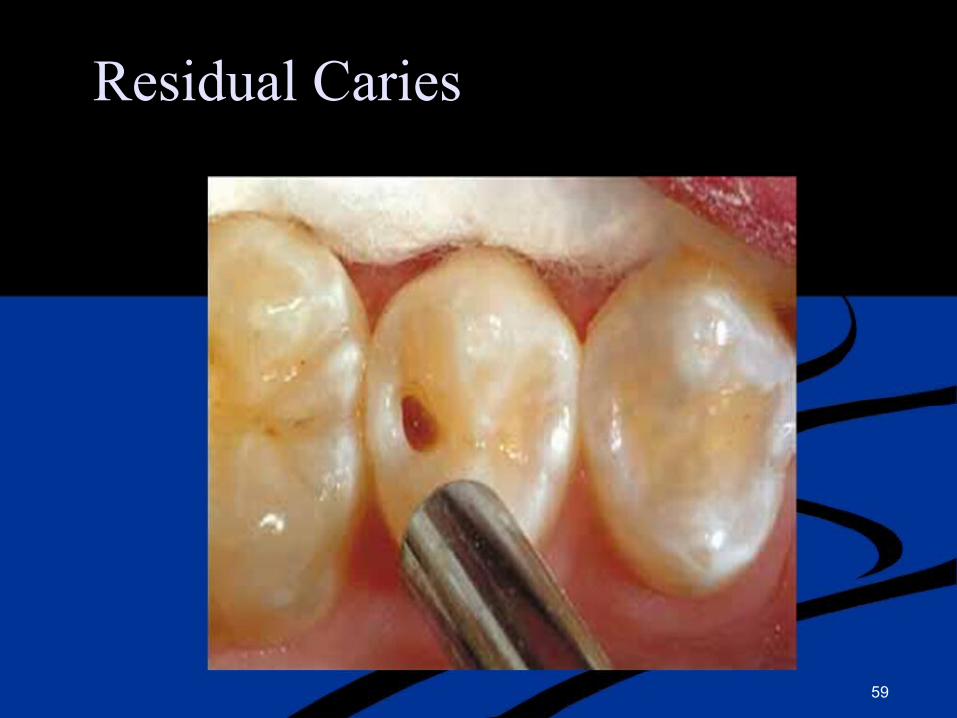
Residual Caries
59
Dentinal caries
60
Dentinal caries
Zone 1: Normal Dentin Deepest area
Normal odontoblastic processes No crystals are in the lumen
Intertubular dentin has normal cross banded collagen
Normal dense apatite crystals No bacteria
Stimulation of dentin produces a sharp pain
61

Zone 2: Subtransparent Dentin
Demineralization of the intertubular dentin Initial formation of very fine crystals in tubule lumen
Damage to the odontoblastic process is evident No bacteria are found
Stimulation of the dentin produces pain Dentin is capable of remineralization
62
Zone 3: Transparent Dentin
Zone of carious dentin softer than normal Shows further loss of mineral from intertubular dentin Large crystals in the lumen
Stimulation of this region produces pain No bacteria
This region remains capable of self repair provided the pulp remains vital.
63
Zone 4: Turbid Dentin
Zone of bacterial invasion
Distortion of dentinal tubules which are filled with bacteria
Very little mineral present & collagen is irreversibly denatured
No self repair
Must be removed before restoration
64

Zone 5: infected Dentin
Consist of decomposed dentin teeming with bacteria No recognizable structure to dentin & collagen Mineral seem to be absent
Removal is essential
Wet & mushy in appearance.
65
Dentin
Infected dentin Contaminated with bacteria
Includes superficial granular necrotic tissue, & softened, dry, leathery dentin
Affected dentin
Comparatively hard, demineralized dentin that is not yet invaded by bacteria
66


Infected Dentine

Affected Dentine
Pain (toothache) that may be associated with caries
♦Sweet -sharp, last seconds
♦Hot & cold -sharp, lasts seconds
♦Hot & cold -lingers, “throbbing”
♦Constant throb -pain starts off by itself
♦Painful on biting
Severity does not always relate to extent and “toothache” can present as any one of the above
Clinically, how would you treat the different types of carious dentin ?
71


73
Caries diagnosis
Primary objectives of caries diagnosis are to identify those
lesions that require surgical treatment
lesions that require nonsurgical treatment persons who are at high risk of developing lesions.
74
Clinical risk assignment for caries
High MS counts are found
Any two of the following are found Two or more active lesions
Large no of restorations Poor dietary habits Low salivary flow
75

LOW RISK PATIENT
No cavitated lesions
May have inactive white spots (smooth shiny). Bacteria MS levels are low
Diet is normal sugar levels low Normal Saliva levels
Low DMF

MODERATE RISK PATIENT
No cavitated lesions
Some active white spot lesions (rough/chalky) Bacterial MS levels elevated
Moderate sugar use
Saliva normal or reduced (xerostomia) Moderate DMF

HIGH RISK PATIENT
One or more cavitated lesions
May have white spot lesions (active or inactive) Bacterial MS levels are very high
Sugar intake very high
Saliva levels low (xerostomia) High DMF
Assessment tools
Patient history
Clinical examination Nutritional analysis Salivary analysis
Radiographic assessment
79

Medical history factors associated with increased caries risk
Age
Gender
Fluoride exposure Smoking
Alcohol
General health Medications
80
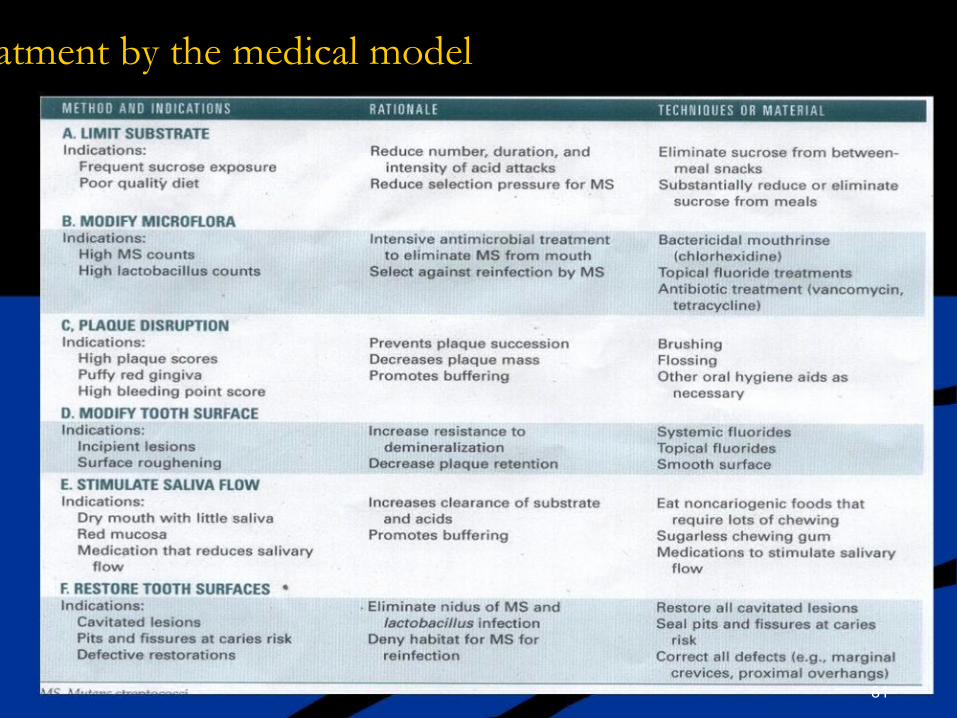
Methods of caries treatment by the medical model
81

Fluoride treatment modalities
82
Antimicrobial Agents
Antibiotics
Vancomycin Kanamycin actinobolin Bis Biguanides chlorhexidine Halogens Fluoride
83

Caries Prevention
General health
Fluoride exposure Immunization
Salivary functioning Antimicrobial agents Diet
Oral hygiene Xylitol gums
Pit & fissure sealant Restorations
84

What can we do about caries?
1.Prevent ♦Frequency (and amount) of “substrates”(sugars)
♦Fluoride (water, tablets, mouthrinse, salt)
♦Regular visits to dentist, including placement of fissure sealants
♦Effective plaque removal
2.Treat ♦Drilling & Filling
♦Extract

Caries Management
Noncavitated caries Preventive measures Sealant, PRR, F-/Obs
Cavitated caries Restoration
Pulpitis, Apical RCT or Extraction Abscess

Think before ………………….
Two Difficulties
1) When to place an initial restoration?
Breakdown of the outer enamel is an important clinical indicator of the treatment
2) How to deal with severe caries?
Protection of dental pulp is the primary goal

Management of Fissured Surface
No Caries or Arrested Enamel Demineralization Cavitation or Caries in Fissures with or Questionable Caries in Caries in Dentin
Susceptible Morphology Dentin
Low High Low High Open fissures Caries Caries with round bur Risk? Risk?
enamel Demineralization dentin involve
No treatment Sealant Restoration Enamel PRR

Treatment Modalities
The results of diagnosis :
Pulp Exposure No exposure
Non-vital Conventional Vital (carious) restoration (traumatic)ex exposure
posure
RCT Direct pulp capping

Preventive Resin restoration


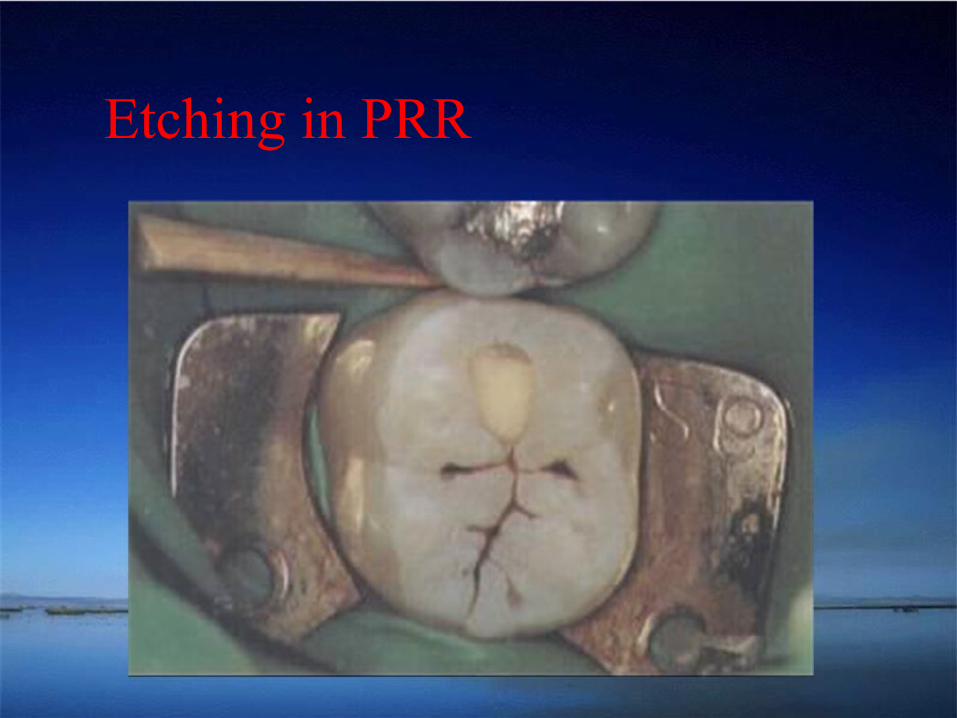
Etching in PRR

PRR-Composite

PRR-Final restoration

Caries control restoration
The goal is elimination of the source of cariogenic organisms by removal of caries from all deep lesions and placement of temporary restorations early in the treatment.
Caries Control Restoration
Cavity preparation is done quickly without definitive cavity preparation.
Undermined enamel be left to aid in retention of these treatment restorations, especially if restoratives are used that bond
to tooth structure.

Caries Control Restoration
Restorative materials used for caries control restoration.
CaOH
Reinforced Zinc Oxide-eugenol Glass ionomer
Amalgam

Deep Lesions
indirect pulp-capping procedure stepwise excavation
Indirect pulp capping
All infected dentin is excavated with large round burs and excavators, being careful not to expose the pulp. Basic fuchsin effectively identifies infected dentin.
A small amount of firm caries (affected dentin) is left over sites of potential exposure.

Indirect pulp capping
Calcium hydroxide liner is placed in the deepest areas. The high pH of the CaOH will neutralize acid, kill bacteria and stimulate formation of restorative
dentin.
The rein-forced ZOE, glass ionomer or amalgam restoration is placed

Stepwise excavation


Methods Of Caries Excavation

Classification of Various Tooth-Cutting Techniques

Ideal Properties Of Cutting Instruments
Comfort & ease of use
Discriminate & remove disease tissue Painless, silent, req. minimal pressure No heat or vibration
Affordable
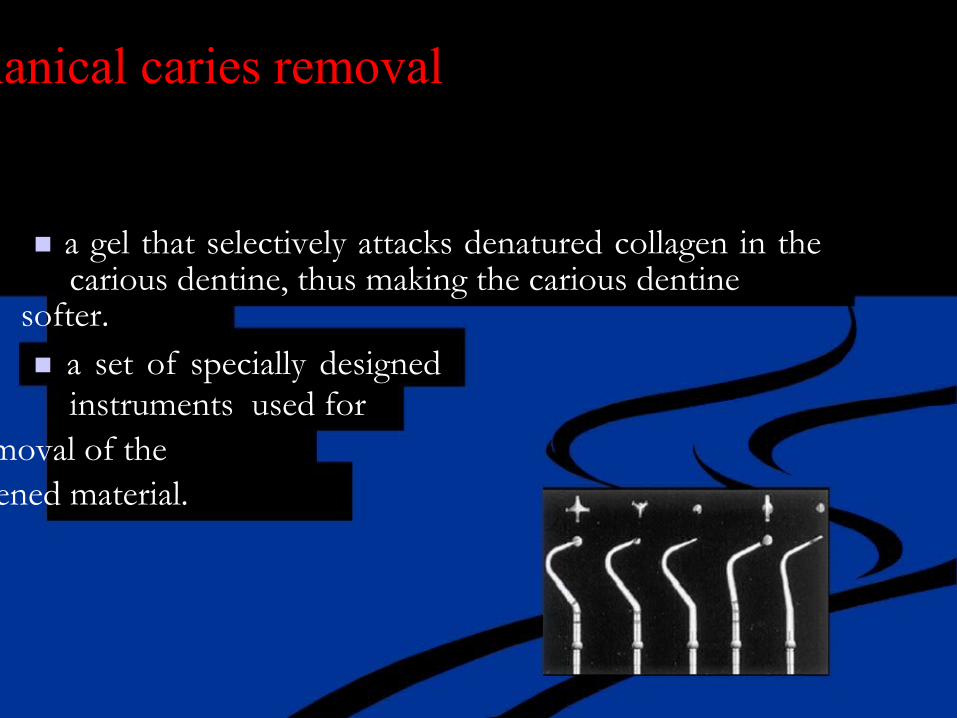
Chemo-mechanical caries removal
a gel that selectively attacks denatured collagen in the carious dentine, thus making the carious dentine
softer. a set of specially designed
instruments used for removal of the
softened material.
Carisolv gel consists of two carboxymethylcellulose based gels:
a red gel containing : amino acids (glutamic acid, leucine and lysine), NaCl
NaOH Erythrosine (added in order to make the gel visible during use ).
and a second containing sodium hypochlorite
The gels are mixed & then applied onto the exposed carious dentine and left for 30 to 60 seconds then the
softened dentine is gently but firmly abraded away leaving a hard, caries-free cavity
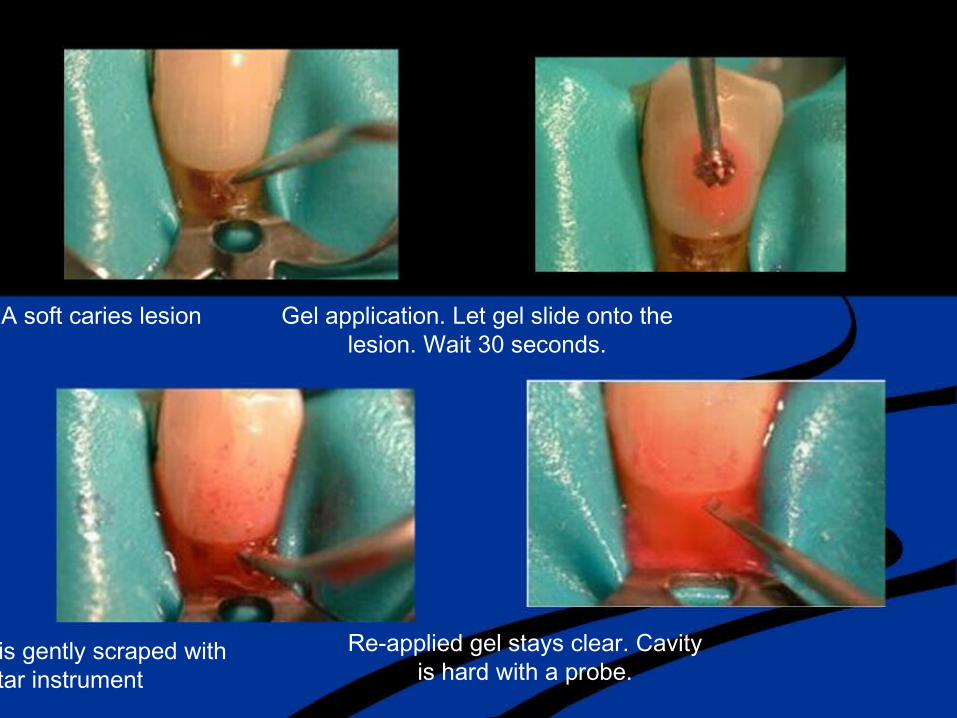
A soft caries lesion Gel application. Let gel slide onto the lesion. Wait 30 seconds.
Re-applied gel stays clear. Cavity The lesion is gently scraped with is hard with a probe. a star instrument

The gel is removed with a Complete caries removal is dry pellet checked with an explorer
The cavity is cleaned with Finished cavity wet pellets
Advantages :
Conserve healthy tooth structure,
Virtually no risk of inadvertent pulp exposure, Reduce the need for anesthesia and allow for same-visit cavity preparations on multiple quadrants,
Designed to reduce post-operative sensitivity.
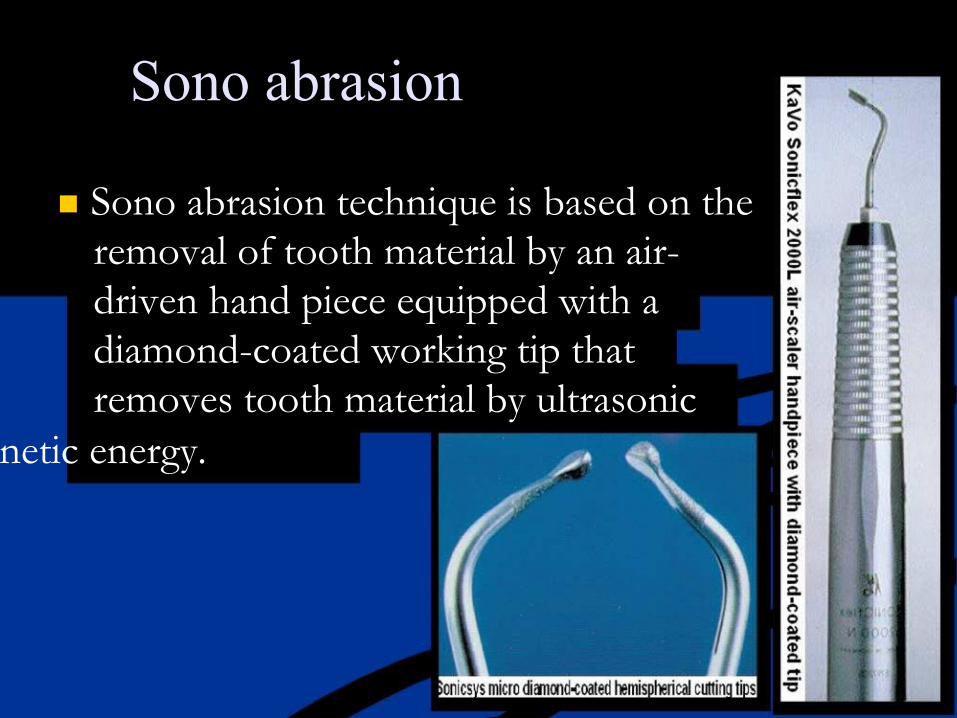
Sono abrasion
Sono abrasion technique is based on the removal of tooth material by an air- driven hand piece equipped with a diamond-coated working tip that removes tooth material by ultrasonic
kinetic energy.
Related Documents











