CAREGIVER BURDEN IN TREATMENT SEEKING INDIVIDUALS WITH ALCOHOL USE DISORDERS, TAMILNADU Dissertation submitted in partial fulfillment of the requirements for the degree of M.D. (PSYCHIATRY) BRANCH XVIII DEPARTMENT OF PSYCHIATRY 201728551 KARPAGA VINAYAGA INSTITUTE OF MEDICAL SCIENCES AND RESEARCH CENTRE, KANCHIPURAM 603308 THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY, CHENNAI, TAMILNADU MAY 2020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CAREGIVER BURDEN IN TREATMENT SEEKING INDIVIDUALS
WITH ALCOHOL USE DISORDERS, TAMILNADU
Dissertation submitted in partial fulfillment of the
requirements for the degree of
M.D. (PSYCHIATRY)
BRANCH XVIII DEPARTMENT OF PSYCHIATRY
201728551
KARPAGA VINAYAGA INSTITUTE OF MEDICAL SCIENCES
AND RESEARCH CENTRE, KANCHIPURAM 603308
THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY,
CHENNAI, TAMILNADU
MAY 2020
ii
CERTIFICATE
Certified that this dissertation entitled “CAREGIVER BURDEN IN
TREATMENT SEEKING INDIVIDUALS WITH ALCOHOL USE
DISORDERS, TAMILNADU” is a bonafide work done by Dr.
KARPAGALAKSHMI.R, Post graduate student, Karpaga Vinayaga
Institute of Medical Sciences, Madhuranthagam, during the academic year
2017 – 2020.
Signature:
Prof. V. Sethumadhavan, MD, D.P.M.,
Professor & Head,
Department of Psychiatry,
Karpaga Vinayaga Institute of Medical Sciences & Research Centre
Kancheepuram 603308

iii
CERTIFICATE
Certified that this dissertation entitled “CAREGIVER BURDEN IN
TREATMENT SEEKING INDIVIDUALS WITH ALCOHOL USE
DISORDERS, TAMILNADU” is a bona fide work done by
Dr. KARPAGALAKSHMI.R, Post graduate student, Karpaga Vinayaga
Institute of Medical Sciences, Madhuranthagam, during the academic year
2017 – 2020.
Signature:
Dr. Sufala Sunil Viswasrao, MD,
Principal,
Karpaga Vinayaga Institute of Medical Sciences and Research Centre,
Kancheepuram 603308.
iv
CERTIFICATE – II
This is to certify that this dissertation entitled “CAREGIVER
BURDEN IN TREATMENT SEEKING INDIVIDUALS WITH
ALCOHOL USE DISORDERS, TAMILNADU, KANCHEEPURAM,
TAMILNADU” of the candidate Dr. R. Karpagalakshmi, with registration
Number 201728551 for the award of M.D. in the branch Psychiatry. I
personally verified the urkund.com website for the purpose of plagiarism
check. I found that the uploaded thesis file contains from introduction to
conclusion pages and result shows percentage of plagiarism 5% in the
dissertation.
Guide and Supervisor
Sign with Seal
v
DECLARATION BY THE CANDIDATE
I, hereby declare that this dissertation entitled “CAREGIVER
BURDEN IN TREATMENT SEEKING INDIVIDUALS WITH
ALCOHOL USE DISORDERS, TAMILNADU” submitted by me for the
degree of M.D is the record work carried out by me during the period from
July 2017 to May 2020 under the guidance of Prof. V. Sethumadhavan,
Head of the Department of Psychiatry, Karpaga Vinayaga Institute of
Medical Sciences and has not formed the basis of any degree, diploma or
fellowship titles in this or any other university or other similar institution of
higher learning.
Signature:
Dr. R. KARPAGALAKSHMI
Post Graduate Registrar (MD),
Department of Psychiatry,
Karpaga Vinayaga Institute of Medical Sciences and Research Centre,
Kancheepuram 603308.
vi
ACKNOWLEDGEMENT
I sincerely thank Dr. R. ANNAMALAI RAGHUPATHY, Managing
Director, Karpaga Vinayaga Institute of Medical Sciences for his kindness in
helping us with all available resources.
I wish to thank Dr. SUFALA SUNIL VISWAS RAO, Principal,
Karpaga Vinayaga Institute of Medical Sciences for her support and
guidance.
It is beyond words to express my sincere thanks and gratitude to my
Professor and HOD and my guide Dr. V. SETHUMADHAVAN, Professor,
KIMS who consistently guided me in each and every step of my thesis work.
His kind support and encouraging words are great pillars of my success.
I wish to proudly thank my Associate Professor Dr. T. SIVAILANGO
for his valuable advice and support.
I feel happy to thank Dr.S.ARUMUGANATHAN, Assistant Professor
and my co guide for the encouragement, guidance and support rendered by
him all through my works. His passion for the subject and his zeal to share
his immense knowledge and experience with me will always be a source of
inspiration.

vii
It also gives me immense pleasure in thanking Dr. S.
SUMITHRADEVI, Assistant Professor and Dr. S. USAID, senior resident,
for helping me in overcoming difficult situations during this thesis work and
for their valuable guidance. I am also thankful our Clinical Psychologist
Mr.M.Krishnamoorthy, for his assistance in bringing out this project.
I thank my co-postgraduate, my juniors and CRRIs who has been a
source of constant support and help.
I thank my family and my friends for the limitless love, support and
motivation.
I thank the “Almighty” immeasurably, because without HIS blessings I
wouldn’t have been able to complete this dissertation.
Finally, I am immensely thankful and grateful to all the patients and
their caregivers who had involved themselves and participated in this study,
making it a successful completion.

viii
ix
CONTENTS
S NO TITLE PAGE NO
1 INTRODUCTION 1 – 3
2 REVIEW OF LITERATURE 4 –35
3 AIMS AND OBJECTIVES 36 – 38
4 MATERIAL AND METHODS 39 – 48
5 OBSERVATIONS & RESULTS 49 – 72
6 DISCUSSION 73 – 82
7 CONCLUSION 83 – 85
8 REFERENCES 86 – 98
9
ANNEXURES
i. ABBREVIATIONS
ii. CONSENT FORM
iii. STUDY INSTRUMENTS
iv. ETHICS COMMITTEE
APPROVAL CERTIFICATE
v. MASTER CHART
99 – 137
101
102 – 103
104 – 121
122
123 - 137

1
INTRODUCTION

2
INTRODUCTION
Alcohol use disorders not only affect the individual but also their
family members. In the human history alcohol has played a major role
irrespective of the culture, race, traditional background and religion. Many
societies in the world make use of exhilarating, euphoric substances among
which alcohol was believed to be the most common.
Family plays a vital part in the care of the patient with mental illnesses.
In country like India, family is the most important factor due to various
factors like interdependence, culture and concern for the family members1.
Increased consumption of alcohol has been identified as a major risk
factor for global disease burden. According to global status report, overall
5.1% of global disease burden and injury were attributed to alcohol2
Alcohol use disorders are defined as a cluster of behavioral and
physical symptoms which can include withdrawal, tolerance and craving.
Alcohol withdrawal symptoms develop 4-12 hours after reduction of intake
following prolonged, heavy alcohol ingestion. Craving for alcohol is
indicated by a robust desire to drink that produces it troublesome to think
about the rest which usually leads to the onset of drinking. School and job
performance may also suffer either from the after effects of drinking or from
actual intoxication at workplace; childcare or household responsibilities may
be neglected; and alcohol related absences may occur from school or work.
3
Finally individuals with an alcohol use disorder may continue to consume
alcohol despite the knowledge that continued consumption possess
significant physical (blackouts, liver disease), psychological (depression),
social or interpersonal problems (violent arguments with spouse while
intoxicated, child abuse (DSM 5)3
Alcohol use has become one of the major public health problems and
third largest risk factor for disease and disability globally. Since most studies
focused mainly on individuals who consume alcohol and very few on
caregivers, this study is an attempt to assess the pattern of alcohol use,
correlation between the severity of alcohol use and caregiver burden.
4
REVIEW OF LITERATURE
5
REVIEW OF LITERATURE
Alcoholism:
Alcoholism is a bio psychosocial phenomenon par excellence; it results
from the contribution of multiple individual and environmental risk factors.
Theories have taken many disparate considerations, from the effects of policy
to the influence of familial and sociocultural environments across cultures
and over time. Some ethnic groups have traditionally had low rates of
alcoholism (Asians, Jews, and some North American Aboriginals) and the
prevalence is generally higher in males across both age cohorts and
ethnicities.
Another layer of complexity lies in the fact that alcoholism is a
clinically heterogeneous disorder with variable age of onset, drinking
patterns, severity, and comorbidity with other mental disorders. In general,
alcoholics have one or more clinical diagnoses in addition to alcohol
dependence, including drug abuse, antisocial personality disorder, anxiety,
and depression. The course of the disorder is variable with high rates of
remission and relapse; its manifestation changing in pattern and severity in
response to life events (stressors) and other aspects of the environment.
The availability of alcohol and the social promotion of frequent or
heavy drinking are examples of social risk. But environmental facilitation
6
does not explain the genesis of an alcohol dependence disorder in specific
individuals. This disorder is best understood because the results of social
prompting and individual vulnerabilities. There is a variance in drinking and
heavy drinking patterns, alcohol use disorders and treatment for alcoholism
recorded more in men than in women3
Alcohol Use Disorder
Alcohol Use Disorder is a complex, multifaceted cluster of behavioral,
cognitive, and physiological symptoms. The elements represent biological,
psychological (cognitive), and behavioral processes. This helps to explain the
linkages and interrelationships that account for the coherence of signs and
symptoms. The main feature is co-occurrence of signs and symptoms.
Salience means that drinking is given a higher priority than other activities in
spite of its negative consequences.
This is reflected in the emergence of alcohol use as the preferred
activity from a set of available alternative activities. Once drinking to
intoxication goes against the understood social rules governing the time,
place, or quantity usually expected by the user’s family or friends, this might
indicate hyperbolic salience. Salience is when a person continues to drink or
drug use despite of negative consequences.

7
This implies that substance use has become the preferred activity in the
person’s life. One indication of this is the amount of time or effort devoted to
obtaining or using substances or recovering from substance use.
Chronic drinking interferes with the person’s ability to conform to tacit
social rules governing daily activities, such as keeping appointments, caring
for children, or performing a job properly, that are typically expected by the
person’s reference group. Excessive use also results in mental and medical
consequences. Thus, a key aspect of the dependence syndrome is the
persistence of excessive drinking in spite of social, psychological, or physical
harm, such as loss of employment, marital problems, depressive symptoms,
accidents, and liver disease. This indicates that alcohol use is given a higher
priority than other activities, in spite of its negative consequences.
Impaired control refers to the inability to limit the amount or frequency
of alcohol use. Resumption of heavy drinking after receiving professional
help for a drinking problem is evidence of lack of success. The symptom is
considered present if the drinker has repeatedly failed to abstain or has only
been able to control drinking with the help of treatment, mutual-help groups,
or removal to a controlled environment.
Tolerance is a decrease in response to a standard dose of alcohol that
occurs with continued use. Tolerance may be physical, behavioral, or
psychological. Physical tolerance is a change in cellular functioning. The
8
physiological effects of alcohol diminish over time, even though the cells
normally affected by alcohol are subjected to the same concentration.
Psychological tolerance occurs when the drinker no longer experiences a
“high” after the initial drink. Behavioral tolerance is a change in the effect of
a standard dose of alcohol that occurs when the person has learned to
compensate for the impairment.
A withdrawal state is a group of symptoms that occur after cessation of
drinking, usually after repeated and usually prolonged drinking. Withdrawal
symptoms can appear after several hours of abstinence, which explains why
some alcoholics have a need to drink soon after waking in the morning.
Dick & Kendler, 2012 says Alcohol use disorder has long been
recognized to run in families 4. There is substantial evidence from twin
research and adoption studies that a major genetic component is operative in
its development, which prior to DSM-5 was called alcohol dependence.
Nonetheless, the disorder is etiologically complex, in that it there is a
sevenfold risk for alcohol dependence in first-degree relatives of alcohol-
dependent individuals, with male relatives of male alcohol-dependent
individuals having the greatest risk for the disorder 5. This highlights the fact
that environmental factors play a role in developing alcohol use disorders,
In a review of population-based twin studies of alcohol dependence,
heritability estimates (i.e., the proportion of risk attributable to genetic
9
factors) ranged between 0.52 and 0.64, with no substantial sex difference
(Kendler, 2001).
Kendler et al., 1997 conducted a study in Sweden using data from
temperance board registrations showed that the estimate of the genetic
contribution to risk of stability of disorder across decades, despite of
changing society
McGue, 1994 conducted many adoption studies and majority of the
results have shown an excess of alcohol dependence in adopted-away
offspring of biological parents. Alcohol dependence appears to be a
polygenic disorder with multiple genes acting in either additive or interactive
ways. Two molecular genetic approaches that have been used to identify the
genes that influence risk for alcohol dependence are candidate gene studies
and linkage studies.
Candidate gene studies are population-level investigations in which
genetic loci that code for proteins thought to be important in the etiology of
the disorder are examined in samples of unrelated individuals. Candidate
Gene Studies are the best-known example of genetic variation affecting risk
for alcohol dependence involves genes that are not directly relevant to
alcohol’s neuropharmacological effects. (Gelernter, 1995).

10
Thomasson et al., 1991 found that the mechanism depends upon the
metabolism of alcohol, first to acetaldehyde by ADH and then to acetate by
acetaldehyde dehydrogenase. Acetaldehyde is toxic and produces a flushing
reaction characterized by a set of uncomfortable symptoms including facial
flushing, lightheadedness, palpitations, and nausea. Thus, increased
metabolism of ethanol or decreased metabolism of acetaldehyde, either of
which can result in increased acetaldehyde concentrations, produces an
aversive effect which could decrease the risk for alcohol dependence. There
is, in fact, evidence that a variant that greatly reduces or eliminates ALDH
function (occurring mostly in Asian populations) is protective against alcohol
dependence, and ADH variants that increase function may also be protective.
The mechanism of this effect depends upon the metabolism of alcohol, first
to acetaldehyde by ADH and then to acetate by acetaldehyde dehydrogenase.
Work by Chen et al., 1999 and Bierut et al., 2012 concluded some people
metabolize alcohol quickly but have a problem breaking down the in-between
by-product acetaldehyde; people carrying this gene variant may be less likely
to drink and therefore may have a lower risk for alcoholism.
Hesselbrock et al., 2001 conducted two large linkage studies in an
effort to identify chromosomal regions that contain genes that modify the risk
for alcohol dependence12
. The larger of these two projects, the Collaborative
Study on the Genetics of Alcoholism (COGA), included more than 9000

11
adults and nearly 1500 children and adolescents. A genomic scan of the
COGA samples showed that chromosomes 1 and 7 each have a region
containing one or more genes that increase the risk for alcohol dependence.
Reich et al., 1998 found a “protective factor” on chromosome 4 for
alcohol dependence13.
A linkage study has also been reported for a sample of
152 subjects belonging to extended pedigrees in a southwestern American-
Indian tribe (Long et al., 1998)14
. A genome-wide scan was performed on
172 sibling pairs from this sample. Evidence for linkage to alcohol
dependence was obtained for regions on chromosomes 4 and 11. Three
closely linked loci on chromosome 4 map onto the Type I ADH gene cluster
in proximity to the region on this chromosome that was identified as linked to
a “protective factor” by COGA.
Epidemiology
Alcoholism is one of the major health problems globally. More than 3
million people died as a result of harmful use of alcohol in 2016, according a
report released by the World Health Organization (WHO) on September 21,
2018. This represents 1 in 20 deaths and it’s more common among men.
Overall, the harmful use of alcohol causes more than 5% of the global disease
burden is caused by harmful alcohol use

12
Alcohol consumption occurs along a Continuum and drinking patterns
vary considerably among individuals with no clear demarcation between
“social” or “moderate” drinking and problem or “harmful” drinking.
However, as the average amount of reached drinking and the frequency of
intoxication increases so does the incidence of medical and psychosocial
problems. In DSM- 4 (American psychiatric association 1994), the most
commonly identified group of people are those with alcohol abuse or
dependence. A less prominent, but more numerous groups consist of
individuals referred to as problem drinkers or harmful drinkers who do not
need the criteria for alcohol dependence.
In DSM-5 alcohol dependence and abuse have been replaced with a
single category of alcohol use disorder. This is likely to result in “diagnostic
orphans”. For Example individuals with alcohol related problems, but not
receiving an alcohol use disorder diagnosis in DSM-5 (Peer et al.2012).
In the 2009 survey on Drug use and health (NSDUH; Substance
abuse and mental health services administration 2010) the majority of U.S
Population aged 12 years and older (51.9% or 130.6 million people reported
consuming alcohol during the month before the interview nearly a quarter of
such individuals (23.7% age or 59.6 million people) engaged in binge
drinking (5 or more drinks on the same occasion) at least once during this
time. Heavy drinking (five or more drinks on separate occasions during the

13
month) was repeated by 6.8% of population or 17.1 million people. The
prevalence of current alcohol use increased with age up to age group of 21 to
25 years where it reached a peak of 70.2%. This is also the same age group
for which the rates of both binge drinking that is 46.5 % and heavy drinking
16% peaked. The 2009 the NSDUH (Substance Abuse and Mental Health
Services Administration 2010) also showed that men were more likely than
women to drink (57.6% versus 46.5%).
Drinking behavior also differed by race, ethnicity. 56 % of white
people reported drinking during the past month followed by individuals
reporting two or more races (47.6 %) Afro-American persons (42.8 %),
Hispanic persons (41.7 %), Asian persons (37.6 %) and American Indian
Alaska native persons (37.1 %). Binge drinking was most common among
Hispanic individuals. (25.0 %), followed by white (24.8 %) American Indian/
Alaska native (22.2 %), African-American (19.8 %) and Asian (11 %)
individuals.
For many years there has been studies shows life time and past year
prevalence of alcohol use disorders. For example, the national comorbidity
survey NCS, a representative household survey of more than 8,000
individuals ages 15 to 54 years was conducted to assess lifetime and past year
alcohol use disorders using the DSM-3 R criteria (American Association
Psychiatric association 1987). The NCS estimated the lifetime prevalence of

14
alcohol abuse and alcohol dependence for adults aged 18 to 54 years to be 9.4
% and 14.1 % respectively.
Together, these data indicate that more than one in five young to
middle-aged in United States met the criteria for a lifetime alcohol use
disorder. (Kessler et al. 1997) 17
. The 12-month prevalence rates for alcohol
abuse and dependence where 2.5% and 4.4% respectively. The 1992
(National longitudinal alcohol epidemiological Survey) NLAES based on
interviews with the national probability household sample of more than
43,000 adults aged 18 and older, showed the one near prevalence of alcohol
use disorder to be 7.4 percentage ( 3.0 percentage with alcohol abuse and 4.4
percentage with alcohol dependence)18
(Grant et al., 1991-92, 2001-02). The
national epidemiological survey on alcohol and related conditions
(NESARC), also a community based survey of more than 43,000 individuals
(Grant et al. 2004a)20
, permitted an evaluation of trends in alcohol use
disorder prevalence and characteristics because it is used a methodology very
similar to that of 1992 NLEAES.
The NESARC are showed a 12 month prevalence of alcohol abuse and
dependence of 4.7% and 3.8%, respectively, so that an estimated total of 17.6
million adult Americans had an alcoholic use disorder during 2001- 2002 the
prevalence of alcohol abuse in the NESARC was significantly increased over
that NLEAS. Whereas the prevalence of alcohol dependence decreased
15
significantly over the ten-year period between the two surveys consistent
with drinking behavior.
National prevalence data also shows that rates of alcohol use disorders
vary by age gender race, ethnicity socioeconomic status and geographic
location. The prevalence of alcohol use disorders has consistently been higher
among men than among women by at least two fold Substance Abuse and
Mental Health Services Administration 2010, the highest prevalence rates of
alcohol abuse and dependence occur among young adults with rates declining
gradually with increasing age.
Adverse consequences of drinking include a variety of social, legal,
and medical problems (Babor et al., 1987)20
. Overall, alcohol-related
mortality is 98,000 deaths each year, or about 7.6% of all deaths in the United
States, putting it among the three leading lifestyle-related causes of death
(Centers for Disease Control, 2012)21
. The number of alcohol-induced
deaths excluding accidents and homicides in 2010 was 25,692. Of alcohol-
related deaths, 44% were attributable to alcohol-related traumatic injury
(Centers for Disease Control, 2012). Alcohol related mortality declined
during the last few decades of the twentieth century.
The age-adjusted mortality rate from liver cirrhosis in 2011 (4.8 deaths
per 100,000 persons) was almost half the 1993 rate (7.9 deaths per 100,000)
(US Department of Health and Human Services, 2013), and alcohol-
16
related automobile fatalities fell by 24.5% between 1998 and 2009, from 5.3
to 4.0 deaths per 100,000 (National Institutes of Health, 2010). Nonetheless,
age-adjusted rates of liver cirrhosis in 2007 remained more than twice as high
for males (12.7 deaths per 100,000 population) than females (5.9 deaths per
100,000 population). (National Institutes of Health, 2010).
The most frequent co-occurring diagnoses are for other drug use
disorders, mood, anxiety, and personality disorders (Hasin et al., 2007)22
.
The relative risks for different types of disorder vary somewhat by gender
(Kessler et al., 1994)23
. Among women, anxiety and affective disorders are
the most common co-occurring disorders. Among men with a history of
alcohol abuse or dependence, drug disorders and conduct disorder account for
the largest proportion of comorbid cases.
Substance use disorders ranging from mild to severe are common
among both men and women with an alcohol use disorder. In 2001–2002,
13.1% of those with a 12-month alcohol use disorder also had a 12-month
drug use disorder. Of these, 73.9% were men and 26.1% were women
(Stinson et al., 2005)24
.
Results from NESARC showed that 28.6% of those with a current
alcohol use disorder had at least one personality disorder. Similarly, 16.4% of
people with a personality disorder had an alcohol use disorder (Grant et al.,
2004a).
17
Problem drinkers have a significantly increased risk for antisocial personality
disorder (ASPD) compared with those in the population with no alcohol use
disorder. Evidence from multiple studies indicates that individuals with an
alcohol use disorder experience a two- to threefold increased risk for
depressive disorders (Swendsen et al25
., 1998; Grant et al, 2004b). The
NESARC study showed mood disorders to be present in 18.9% of those with
an alcohol use disorder (Grant et al., 2004b)26
.
Conversely, 17.3% of individuals with a mood disorder also had an
alcohol use disorder (Grant et al, 2004b). Of the mood disorders, bipolar
disorder is particularly common among individuals with an alcohol use
disorder, with 5.1% having a form of bipolar disorder. Dysthymic disorder,
although present in 2.93% of individuals with an alcohol use disorder, has an
OR of only 1.7 (Grant et al., 2004b) While considered to be important in the
development of alcoholism, comorbid psychiatric disorders also have
prognostic significance (Meyer, 1986)27
.
Rounsaville et al. (1987) found that psychiatric diagnosis at the time
of treatment intake predicted a variety of 1-year post-treatment outcomes.
Among males, the presence of a comorbid lifetime diagnosis of ASPD, major
depressive disorder, or drug abuse/dependence was associated with poorer
drinking outcomes28
.
18
Other investigators have found no difference in drinking outcomes on
comparing primary alcoholics (i.e., those for whom alcohol dependence is the
first and predominant disorder) and alcoholics with a comorbid mood
disorder (Schuckit, 198529
; O’Sullivan et al., 198830
; Powell et al., 199231
).
India being second populous country in the world, around 1/3rd
of its
population consumes alcohol. Alcohol misuse represents a public health
problem in India that need to receive adequate attention. According to WHO
World Health Organization statistics the annual rise in consumption of
alcohol has been increasing in rapid manner. “Magnitude of Substance Use in
India” is a report submitted by NDDTC (National Drug Dependence
Treatment Centre) of the All India Institute of Medical Sciences, New Delhi,
sponsored by the Ministry of Social Justice and Empowerment to Union
Minister for Social Justice and Empowerment.
The Ministry of Social Justice and Empowerment has conducted a
“National Survey on Extent and Pattern of Substance Use in India”. The
Survey was conducted by a team of NDDTC of AIIMS, New Delhi during
2018. This study provides data regarding alcohol use at national and state
level
At the national level, as many as 19% of current users of alcohol
consume alcohol in a dependent pattern. The prevalence of dependent pattern
of alcohol use in the general population (10—75 years) is estimated to be

19
2.7%, or 2.9 crore individuals. States with high prevalence (more than 10%)
of alcohol use disorders are: Tripura, Andhra Pradesh, Punjab, Chattisgarh,
and Arunachal Pradesh. An additional 2.5% of people in the country (about
2.7 crore individuals), consume alcohol in a harmful manner. In other words,
about 5.2% of the population (more than 5.7 crore individuals) are affected
by harmful or dependent alcohol use and need help for their alcohol use
problems. Nearly one in five alcohol users suffers from alcohol dependence
and needs urgent treatment
Patterns of Drinking and Burden of Disease
Alcohol in beverage form is among the most widely used psychoactive
substances in the world. Because of its widespread distribution and the
readiness with which it is consumed in a variety of settings, people do not
generally think of beverage alcohol as a drug. Nonetheless, its complex
pharmacological actions, including panoply of psychoactive effects, have led
societies throughout the world to surround alcoholic beverages with a variety
of rules and regulations to prevent behavioral, social, and psychiatric
problems connected with alcohol misuse (Babor et al., 2010)32
.
Despite these efforts at control, excessive drinking, with its adverse
effects, is widespread. Room et al., 2002 Patterns of drinking and the types
of problems associated with alcohol misuse differ markedly throughout the
world33
. Whereas the highest alcohol consumption rates are generally found
20
among the industrialized countries of Europe and the North American
continent, the lowest consumption rates are found in the predominantly
Islamic countries where the use of alcohol is prohibited or discouraged. The
percentage of drinkers in adult populations ranges from a high of 86% in the
North and Central European countries to less than 10% of adults in Islamic
countries such as Pakistan and Iraq (Room et al., 2002)33
.
According to recent estimates from the World Health Organization’s
Expert Committee (WHO, 2007), the evidence of alcohol’s impact on health
through its intoxicating, dependence-producing, and toxic qualities is
extensive. Alcohol is estimated to cause a net harm of 3.7% of all deaths, and
4.4% of the global burden of disease, as measured in disability-adjusted life-
years (DALYs) lost. Neuropsychiatric disorders, mainly made up of alcohol
use disorders, account for the highest proportion of alcohol attributable
DALYs (Babor et al., 2010).
Sarkar et al., studied socio-demographic characteristics of 187 men
who were alcohol dependent at a de addiction center at west Bengal. They
found that most of the patients were male, married and middle aged. The age
at which they first started drinking and quantity of alcohol intake were
associated significantly with positive family history of alcoholism35
. Strong
familial history in children needs to be evaluated and counseled to prevent
development of alcoholism.

21
In a cross sectional study conducted by Gupta et al34
., concluded that
people consume alcohol much more than the recommended levels often gets
higher rates of binge drinking They also often do not seek treatment for their
alcohol use predisposing them to alcohol related conditions34
.
Sampath et al., conducted a study in a 550-bed teaching hospital in
Kolar, a rural district of Southern India and they found that physical health
issues are common among problem drinkers and there is significant
correlation with smoking and they are likely to prefer local made liquor and
become alcohol dependent.36
John et al.,37
conducted a study at The Department of Community
Health, Christian Medical College, Vellore, Tamil Nadu, Kaniyambadi block
and employed ‘AUDIT’, to assess the use of alcohol. Totally 345 men
interviewed in which 343 were refused to give consent and in that population
One-third sample had used alcohol over last year and one fifth are using
alcohol in a regular basis and about one sixth were hazardous alcohol users.
The study says that it is possible that living in a village which brews alcohol
may encourage positive attitudes towards the consumption of alcohol and
also flagging the risks of illicit liquor. At the same time, the preference for
IMFL, whose availability is widespread in the region, may be a greater risk
for hazardous use.
22
PATTERN OF ALCOHOL USE
A cross-sectional study by Gupta et al34
., on 75 participants with
alcohol use disorders More than half of the participants reported use of
alcohol ‘for relaxation’ or to ‘relieve tension’ and around 40% for
recreational purpose and usual timing for drinking is during night. The most
common place of consuming alcohol was home. Most of the participants
prefer country made liquor followed by Indian made foreign liquor. Around
2/3rd
participants consume alcohol alone and 75% participants would have
something to munch along with drinks and would mix alcohol with water or
soda. More than half of the participants get intoxicated ‘some of the time’
after consuming alcohol in the past three months. In ASSIST scoring, more
than three fourth people scored in high to moderate risk range.
Other studies from different regions of India shows that majority of
population preferred drinking alone and the main reason for drinking is to get
intoxicated and they consume different types of beverages in different
occasion. Beverage type, place where alcohol consumed, manner of
consuming alcohol, proximity of food intake and mixing used with liquor
were often associated with alcohol related complications.(Benegal,200538
;
Vilamovska et al., 200939
, Ronksley , Brien et al40
, Mukamal, & Ghali,
201141
; Turner, Ghosh et al., 201242
; Studer et al., 201543
).
23
CAREGIVER
Steinglass44
studied the impact of alcohol dependence syndrome on the
family in terms of association between extent of alcohol dependence and
psychiatric symptomatology. The sample of the study includes families of
alcohol dependent and non-alcohol dependent spouses. The study showed
that the psychopathology in wives is directly proportional to severity of
alcohol dependence leading to social impairment.
A study from Nepal compared IV drug users and alcohol dependent
individuals and they have found increased caregiver burden in both groups.
However, the caregiver burden was significantly high in IV users. IV drug
abusers showed increased tolerance and less perceived burden in comparison
to other family members.45
About 95 to 100% caregivers of alcohol dependent and opioid
dependent patients had severe burden as reported by a study from
Chandigarh.46
Vaishnavi et al., concluded that severity of alcohol dependence
correlated positively with significant burden in caregivers. It is imperative
that during treatment of alcohol disorder patients alleviating burden of
caregivers is very important to improve treatment effectiveness in alcohol,
use disorder patients.47
24
Srinivasagopalan et al (2015) states that the term Caregiver refers to
anyone who assists to someone else who is in some degree Incapacitated and
needs help. The person who provides unpaid care is called as the informal
caregiver. They may be family member, neighbor or friend. The person who
provides care like a volunteer or being paid for his service that is associated
with the service system is called as formal caregivers48
A hospital based interventional study on burden and quality of life
among caregivers of persons with alcohol dependence syndrome by Swapna
et al., Quality of life has given an approach for management and natural
course of relapse and remission for alcohol dependence.49
It is a dimensional
construct that includes the physical, mental, psychological, social and
religious functioning of the individual. It helps to understand the effects of
the disease on the patient and their caregiver. Among various psychiatric
disorders, alcohol- related disorders significantly affect Quality of life and
extensive studies have to be done on this forum.
Shah et al studied about common mental disorders among spouses of
men with alcohol dependence and he found that 36% depression, anxiety
16%, stress 6% and the risk of self-harm is 2%. This study reveals that
psychiatric comorbities were higher in wives of alcohol dependent men when
compared with wives of non-alcohol dependent men50
. Many studies reported
that women who are married to alcohol dependent men have poor mental and
25
physical health and need for intervention like psychological and social
support to improve the quality of life of affected individuals48
.
Shekhawat et al.,51
conducted a cross sectional study on Caregiver
Burden on Wives of Substance‑dependent Husbands and Its Correlates at a
Tertiary Care Centre in Northern India and it was conducted at Government
Medical College, Kota, Rajasthan and Government Medical College,
Haldwani, Uttrakhand by department of psychiatry and department of
community medicine respectively 50
. Inclusion criteria for patients were those
aged between 18 and 65 years, fulfilled alcohol or heroin (opioid)
dependence criteria as per the WHO ICD‑ 10, duration of heroin or alcohol
dependence for more than 1 year, whose primary caregiver was wife, and
who gave informed consent.
The inclusion criteria for wives were those who gave informed
consent, living with the patient for more than 1 year. There is significance
burden noted in wives of alcohol dependence patients. The burden ranging
from moderate to high and affects the lives of caregivers. On comparing the
mean scores of burden assessment schedule and overall burden between AD
and HD group, there was more burden (in all factors as well as in overall
burden) on wives of HD patients than on wives of AD patients.
Also significant difference was found in the factors of “impact on
marital relationship,” “appreciation of caregiving,” and “impact on relation
with others” but no statistical significant difference was found in the factors

26
of “impact on well‑being” and “perceived severity of disease”. Substance
use in adult phase of life results in the loss of productivity and working
capacity of the patients subsequently disturbing the personal, familial, and
social life as a whole. Present and previous Indian study had shown a higher
prevalence of substance addiction in people from lower socio demographic
status and those who live on daily wages and inability to satisfy the emotional
needs of partner.
Due to lack of appreciation of care given higher burden was perceived
by wives of HD patients as compared to wives of patients of alcohol
dependence. The trend toward the nuclear family system in our country
highlights the importance of wives as the primary care providers and thus
bearing significant caregiver burden. Indian study comparing burden on
caregivers of alcohol‑ and opioid‑dependent patients also found moderate to
severe burden in 95%–100% of the caregivers.
Higher burden in primary caretaker of illiterate patients. Hence,
education becomes an integral part and also important contributor in reducing
burden. As the age of the wife increases, she gets more mature and better
understands the need and care of the patient; hence, she perceives less burden
and more satisfaction because of appreciation and acknowledgment of good
caregiving from family and friends of patients.
Swaroopachary et al52
., conducted a cross sectional of inpatients
attending psychiatry department, SVS Medical college in 2017 for alcohol
27
dependence reported higher caregiver burden in young population and
unemployed group. Care giver burden is high in families with domestic
violence. Severe dependence by married men is associated with poor mental
health and abuse in their wives. Female spouses of persons with alcohol use
disorders experience victimization, mood disorders, anxiety disorders,
subjective to injuries and were often in fair to poor health than spouses of
non-alcohol users. More life stressors were experienced by them. They also
had lower psychological quality of life scores. Partner alcohol problems pose
diverse health threats for women that go beyond their well‑ documented
association with domestic violence.
The quality of marital life of 30 wives of alcohol dependent
individuals and wives of non-dependent control by using Dyadic Adjustment
Scale (DAS) and Social Drinking Scale (SDS) studied by George. Study
results revealed that marital dysfunction among individuals with Alcohol
Dependence Syndrome are related to their drinking habit 53
. The quality of
marital life is influenced by the spouse being dependent prior to or after
marriage. The sample size was small. This was one of the earliest
investigations in the area of the quality of marital life of spouses of alcohol
dependent individuals.

28
Nagalakshmi and Suman conducted a study on 40 families with
fathers having Alcohol Dependence Syndrome and family interaction using
the Family Interaction Scale (FIS) was assessed. They concluded that there
were significant differences between families with fathers having Alcohol
Dependence Syndrome than families with non-alcohol dependent fathers54
.
Families of these individuals were often associated with poor interpersonal
communication, deprivation of mutual warmth and support. The spouse of
the men with Alcohol Dependence Syndrome expressed greater
dissatisfaction in all areas of family functioning than the spouses of men
without Alcohol Dependence Syndrome.
Sabhaney studied 80 families’ individuals with Alcohol Dependence
Syndrome and 30 non-alcohol dependent families55
. He used tools like MMPI
and a semi structured interview to assess the psychiatric disorders in the
families. The MMPI revealed that anxiety, depression, mania, schizophrenia,
and psychopathic deviance were more frequent among wives of alcohol
dependent individuals. Since the study sample was small, conclusion could
not be drawn from the study.
Rao TSS and Kuruvilla K. conducted a study on personality of 30
wives of individuals with Alcohol Dependence Syndrome. They included the
women who satisfied Feighner’s Criteria and simultaneously it was compared
with 30 wives of non-alcohol dependent individuals56
. The tools used are
16PF and Eysenck's Personality Inventory. The results revealed there were no
29
statistically significant differences between the two groups on EPI and the
scores were within normal limits. Similar scores on 16 PF observed in both
the profiles in items of being submissive timid, conventional, conservative,
dependent and poised. These findings were not in favour of the concept of
“pathological wives” causing alcoholism in their husbands as advocated by
other investigators. The results were reliable since the scales used were
standardized but not predictive since the sample size was small.
Sisters of individuals with history of alcohol abuse from high density
multigenerational families were studied to determine the characteristics of
personality. Spousal similarity was assessed in proband and in spouse pairs
from the parental generation, permitting for comparisons of selection versus
contagion as descriptions for this resemblance 57
. Sisters were found to differ
from control women with respect to disaffection and Social nearness from the
MDPQ and Scale 6 (Paranoia) from the MMPI. Only spouses from the
parental generation were similar on estrangement, signifying that exposure
over time (contagion) leads to greater resemblance in parents hailing from
high-risk families.
Correlations of a lesser degree occurring in couples from both
generations reveal that assortative mating for Social nearness occurs among
the parents of these persons from high-risk families, and further expose that a
reduced level of Social intimacy for sisters of alcoholics might be mediated
to a certain extent by the additive genetic variance. It was accomplished that
30
assortative mating for particular traits might attribute to increased risk for
alcohol use. In addition, failure to mate assortatively for other traits may as
well contribute to increased rates in high-risk families. The group of wives of
individuals with Alcohol Dependence Syndrome (N=100) was matched up to
a group of wives of non-alcohol dependent men (N=90). The groups were
indistinguishable in view of their age, employment position and wedded
status.
Eysenck Personality Questionnaire was utilized for determining the
main personality proportions. A structured 38 psychiatric interrogation based
on ICD-10 and DSM-III-R, and assessing behavior of oneself before
matrimony (extraverted vs. introverted) were used as well. The wives of
individuals with Alcohol Dependence Syndrome were found to be less
extraverted than the wives of non-alcohol dependent persons. However there
appeared to be no differences in neuroticism and psychoticism. In respect
with the self-assessment of their behavior before marriage, wives of persons
with Alcohol Dependence Syndrome also manifested less extraverted
behavior before marriage.
Lewis explained the etiology of alcohol use and proposed the
Disturbed Personality Model in 1937. He found that a woman who was in
some way psychologically maladjusted, dependent, hostile, domineering,
masochistic, sadistic, married the man with alcohol dependence syndrome to
fulfill her own neurotic needs58
. Being psychologically disturbed herself; she
31
often contributed to the alcohol use of her husband. He concluded that those
women needed therapeutic help as much as their alcohol dependent husbands.
Idstad et al., conducted a cross sectional study on Mental disorder and
caregiver burden in spouses from Nord-Trøndelag, Norway in the year 1995-
1997. Subjective burden in spouses of persons with mental disorder was
compared with subjective burden in spouses of persons without mental
disorder. Totally 9740 couples were included in the study and the reports
shows that the spouses of these persons with mental disorder shows higher
levels of anxiety and depression and lower levels of subjective wellbeing
when compared with spouses of persons without mental disorder59
. This
study concludes that is an association between mental disorder and one
partner and subjective burden in the spouse, but not to the extent that reaches
a symptom level of anxiety and depression which reflects clinical mental
disorder.
Matoo SK et al (2013) defines family caregivers as “the persons who
gives good care to other family member who needs assistance for his regular
works in illness or disability and those who gives unpaid care to the ill
person with special needs”60
.
Fadden et al61
(1987) in an audit of studies on the family burden of
psychiatric patients have watched that the groups of schizophrenic patients
constituted the main gathering which have been reliably examined, despite
the fact that there was proof that the groups of other patient gatherings were
32
likewise truly influenced. They further note that the families regularly endure
extensive burden without grumbling.
Kuruvilla (1993) recognizes family trouble as a critical examination
range for a creating nation like India. From the accessible writing, it shows
up that so far studies on family burden have been more worried with the
appraisal of psychiatric dismalness among the patients' relatives and that no
significant effort has been made to study their subjective well -being in terms
of positive mental health coping resources62
.
Moos et al in a study on the wives of older individuals with late life
Problem drinking pattern. He found that wives of those individuals whose
drinking problems later remitted reported increased alcohol consumption,
poor general health with symptoms of depression and lack of motivation in
domestic chores, social and religious activities63
.
O’Farell, Harrison and Cutter conducted a study on sixty women
who were married to individuals with alcohol dependent syndrome currently
or formerly with a goal to evaluate the stress involved after their marriage,
stress of their children, and their proximity to marital breakup. It was
generally observed as a common prediction done sociologically that more
stressful the marriage was the faster was the wife was to divorce. Differing to
psychoanalytic prediction s, the disturbances in personality, associated with
stress of childhood, did not show a relationship with proximity to marital
breakup. Factor analytically derived subscales of stressors of marital and

33
childhood exhibited a considerable psychosocial interaction; wives were
more disposed than their more outgoing counterparts to undergo their
husbands' verbal abuse of them and their children67
. In addition, sway by
others to break up, optimistic attitudes toward divorce, fear of violence, and
little or no good period early in marriage all linked absolutely with proximity
to marital breakup64
.
Michael Marshal took sixty studies and did a review on the influence
of alcohol use and marital functioning were taken into consideration that
tested the correlation between alcohol use and one of three domains of the
marital functioning ( the satisfaction, the interaction, and the violence).
Results showed that alcohol abuse is associated with marital discord,
miscommunications and increased levels of marital violence65
.
In a study on alcohol’s influence and marital relations as longitudinal
predictors of marital adjustment the relationships among “married couples”
lifetime alcoholism status, behaviors after marriage, and adjustments after
marriage were tested. The results exhibited that the husbands ' life time
alcohol addictive use resulted in lower levels of their wife's helpful marital
adjustments 3 years later but was not associated with their own or their wife's
marital behaviours 9 years from baseline. Findings indicated that in alcoholic
couples the marital adjustment may be driven more by the wives’ than the
husbands' alcohol abuse and marital behavior.
34
Jayaram studied personality profile of 30 wives of individuals with
Alcohol Dependence Syndrome and 30 controls66
. The tools used were 16PF
and GHQ. He found that wives of individuals with Alcohol Dependence
Syndrome differed from the wives on control on the variable personality on
16PF questionnaire. The two groups differed significantly on 8 of the 16
factors. On GHQ the wives of individuals with Alcohol Dependence
Syndrome had shown marked psychological problems like difficulty to
concentrate, sleep disturbance, worry ad constant strain. The sample used was
small. The investigators used an age-matched control group. This was the
first time GHQ was used for the wives of individuals with Alcohol
Dependence Syndrome. The results possibly indicated the severe trend of
psychopathology in spouses of individuals with Alcohol Dependence
Syndrome
Brennan et al investigated 87 spouses of late life problem drinkers and
87 wives of non-problem drinkers. The spouses of problem drinkers reported
poor health related and social functioning. They also reported more stressful,
less supportive family context in problem drinkers67
.
Ino et al studied ‘addiction trends’ seen among wives of alcohol
dependent individuals. The sample consisted of 162 wives of alcohol
dependent men68
. The addiction screening test for wives of alcohol
dependent men (ASTWA) was used to measure addiction trends. The
ASTWA questionnaire consists of 24 questions, which was designed to make
35
clear views about the wives character trends and their addictions. As for the
character traits, the tendency for obsessiveness and tendency for Among 30
families of alcohol dependent individuals, 9 families showed a family history
of alcoholism. As seen on M.P.Q. test the anxiety, depression, mania,
paranoia, schizophrenia and psychopathic deviation were more common
among wives of alcohol dependent individuals than among the wives of non-
alcohol individuals.
36
AIMS & OBJECTIVES

37
AIM & OBJECTIVES
AIM
1. To study the burden in caregivers of Alcohol use disorders.
OBJECTIVES
Primary Objective
1. To assess the caregiver burden in alcohol use disorder.
2. To study the correlation between severity of alcohol use and the
burden.
Secondary objective
1. To study the drinking pattern of patients with alcohol use disorders.
2. To study the association between drinking pattern and caregiver
burden.
38
RATIONALE
The literature presented suggests that alcohol use disorders and the
patient’s pattern of drinking and severity contributes to significant burden in
caregivers physically and psychologically.
Effects upon the family would be expected due to financial and social
consequences of a patient’s loss of income, role reversal and lack of
emotional bonding with family members.
Very few studies in the past have tried to measure care giver burden in
alcohol use disorder but this study aimed to correlate the pattern of drinking
and severity of alcohol use and burden in caregivers.
39
MATERIALS & METHODS

40
MATERIALS & METHODS
Study design: Cross-sectional study
Study setting: Inpatient and Outpatient department of Psychiatry in
Karpaga Vinayaga Institute of Medical Sciences
Study duration: from April 2018 to September 2019
Study population: Patients and caregivers of patients with alcohol use
disorder
Sample size & sampling:
n=4pq/d2
P=48%
q=52%
d=10%
n=100
Sampling method: convenient sampling
INCLUSION CRITERIA:
Male patients who met diagnostic criteria for alcohol use disorders as
per DSM-5
Caregivers (male and female) of alcohol use disorder patients
Age above 18 (both patients and caregivers)
41
EXCLUSION CRITERIA:
Caregivers who has alcohol or any other dependence except nicotine
Patients who has any other substance abuse except nicotine
Patients who are not willing to give consent
Caregivers who are not willing to give consent
Presence of medical / psychiatric illness that prevents patient or
caregiver from participating in the interview
42
STUDY INSTRUMENTS
Semi Structured Questionnaire
This questionnaire is used to find the socio demographic parameters of
the patient along with their clinical details of alcohol use, patient’s quantity
of alcohol use and frequency in last 3 months. It also provides the details
about their drinking patterns. It also measures socio-demographic parameters
of the caregiver including relationship to patient and family income
The Severity of Alcohol Dependence Questionnaire (SADQ):
It is a well validated measure of the severity of dependence and was
developed by the Addiction Research Unit of Maudsley Hospital
The SADQ questions cover the following aspects of dependency
syndrome:
Physical withdrawal symptoms
Affective withdrawal symptoms
Relief drinking
Frequency of alcohol consumption
Speed of onset of withdrawal symptoms
General Health Questionnaire-12
GHQ developed by Goldberg in 1970 .GHQ is used to detect psychiatric
disorder in the general population. GHQ-12 has been used to assess
psychological distress in primary care giver for current situation. GHQ-12
43
well recognize and validate instrument for screening purpose in general
population. The 12 item General Health Questionnaire contains 3
factors:
Anxiety and depression
Social Dysfunction
Loss of Confidence
The validity of the GHQ-12 was compared with the GHQ-28 in a
World Health Organization study of psychological disorders in general
health. This version of the GHQ is very quick to administer and score as it
contains only 12 questions. It has comparable psychometric properties to the
longer versions even though it only takes around two minutes to complete.
Given its speed of administration, it is often used in research studies where it
is impractical to administer a longer form.
The GHQ-12 was prepared by removing the items endorsed by
‘physically ill’ respondents from the GHQ-60. All items have a 4 point
scoring system that ranges from a 'better/healthier than normal' option,
through a 'same as usual' and a 'worse/more than usual' to a 'much
worse/more than usual' option.
Likert scoring (0-1-2-3) from left to right is used for every question.
Score range from 0 to 36. Scores vary by study population.
Scores 0-10- No distress
Scores 11-15 - Typical symptoms of distress.
44
Score 16-20- Evidence of distress
Score above 20 suggests severe problems and psychological distress
Family Burden Interview Schedule
It was developed by Shaila Pai and Kapur. Semi structure family
burden assessment schedule was used for measuring burden on family in
different domains. This instrument is widely accepted and used in various
study for measuring burden on family in different types of illness. Economic
and cultural condition in India being vastly different from those of the
Western world and areas of family burden are entirely different. Family
burden assessment schedule considered standardized method of assessing
the burden on the family particularly in Indian context (Pai & Kapur 1981).
This interview schedule assesses the burden placed on families of
psychiatric patients living in the community69
. It contain 24 items in 6
different categories for objective burden: financial burden (loss of income,
expenditure), disruption of routine family activities, family leisure disruption,
disruption of family interaction, effect on physical health of others (illness,
injury) and effect on mental health. It also assess total subjective burden .It is
a three point scale
Severe burden-2; Moderate burden-1; No burden-0
45
The objective burden total scores ranges from 0 to 48. Out of which 0
to 6 indicates no burden, moderate score is between 6 and 24 and severe
burden being above 24.
Procedure:
After obtaining informed consent from patient and caregivers who are
fulfilling the selection criteria were approached for the study and informed
consent was obtained. Clinical and socio demographic details of patient and
caregivers were obtained using semi structured proforma. SAD-Q was
administered to the patient by the investigator. Caregivers were administered
GHQ-12 and FBIS. Assessment was cross sectional and it was done in single
setting.

46
STATISTICAL ANALYSIS
The data collected is analysed by using Statistical Package for Social
Scientists, version twenty (SPSS -20)
Descriptive analyses of socio-demographic variables and scores in the
questionnaires carried out. For continuous data, mean, standard deviation and
range were calculated and frequency distribution was calculated alcohol-
related clinical details, and drinking contexts. Independent ‘t’ test and Chi-
square test were carried out for continuous and categorical variables.
Pearson’s correlation was done to assess the correlations between alcohol use
characteristics in patients and General health status and Family burden in
caregivers. The level of statistical significance will be accepted at p < 0.05
for all tests.
47
ETHICAL CONSIDERATIONS:
After obtaining informed consent from the study participants they
were requested to be spontaneous and truthful with the choices they chose on
the questionnaires. The participants were assured of confidentiality of the
information provided and had the option of refusal to participate in the study.
48
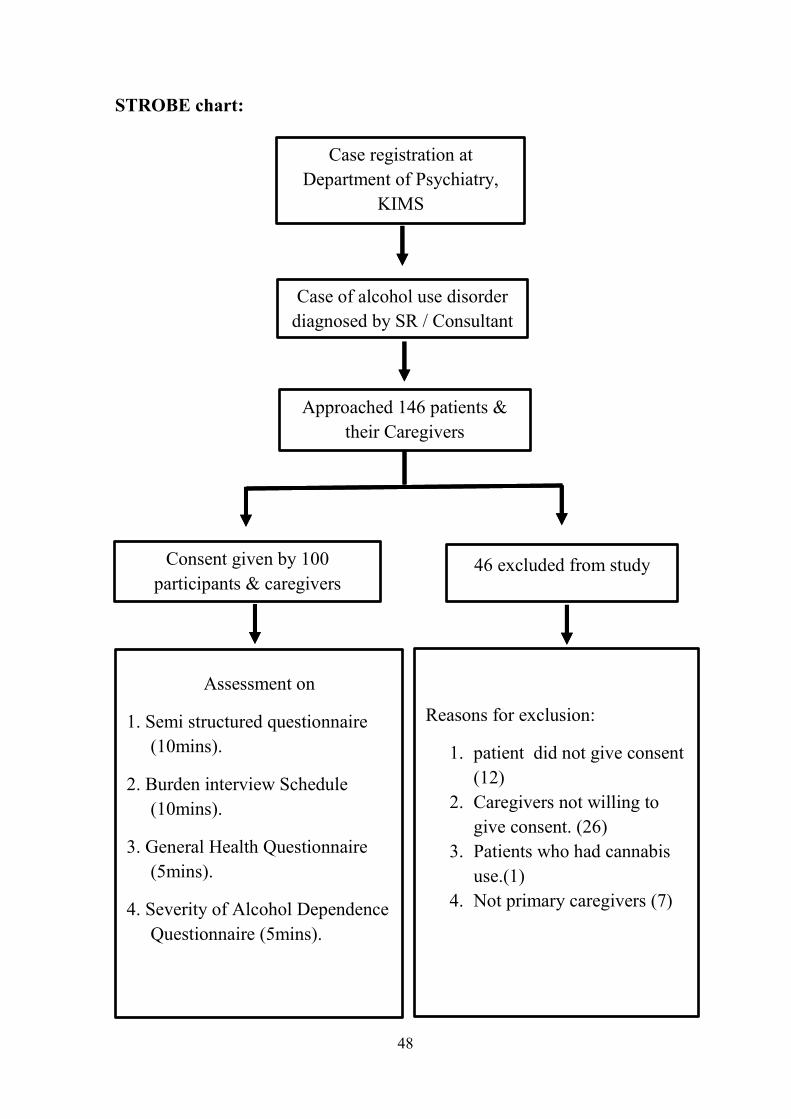
STROBE chart:
Case registration at
Department of Psychiatry,
KIMS
Case of alcohol use disorder
diagnosed by SR / Consultant
Approached 146 patients &
their Caregivers
Consent given by 100
participants & caregivers 46 excluded from study
Assessment on
1. Semi structured questionnaire
(10mins).
2. Burden interview Schedule
(10mins).
3. General Health Questionnaire
(5mins).
4. Severity of Alcohol Dependence
Questionnaire (5mins).
Reasons for exclusion:
1. patient did not give consent
(12)
2. Caregivers not willing to
give consent. (26)
3. Patients who had cannabis
use.(1)
4. Not primary caregivers (7)

49
OBSERVATION & RESULTS

50
OBSERVATION & RESULTS
Socio-demographic profile:
The mean age of the patient was 46.13(± 10.95) years and mean age of
the caregiver 42.03(±10.03) years. All the patients participated in this study
were males and 93 caregivers were females whereas 7 caregivers were males.
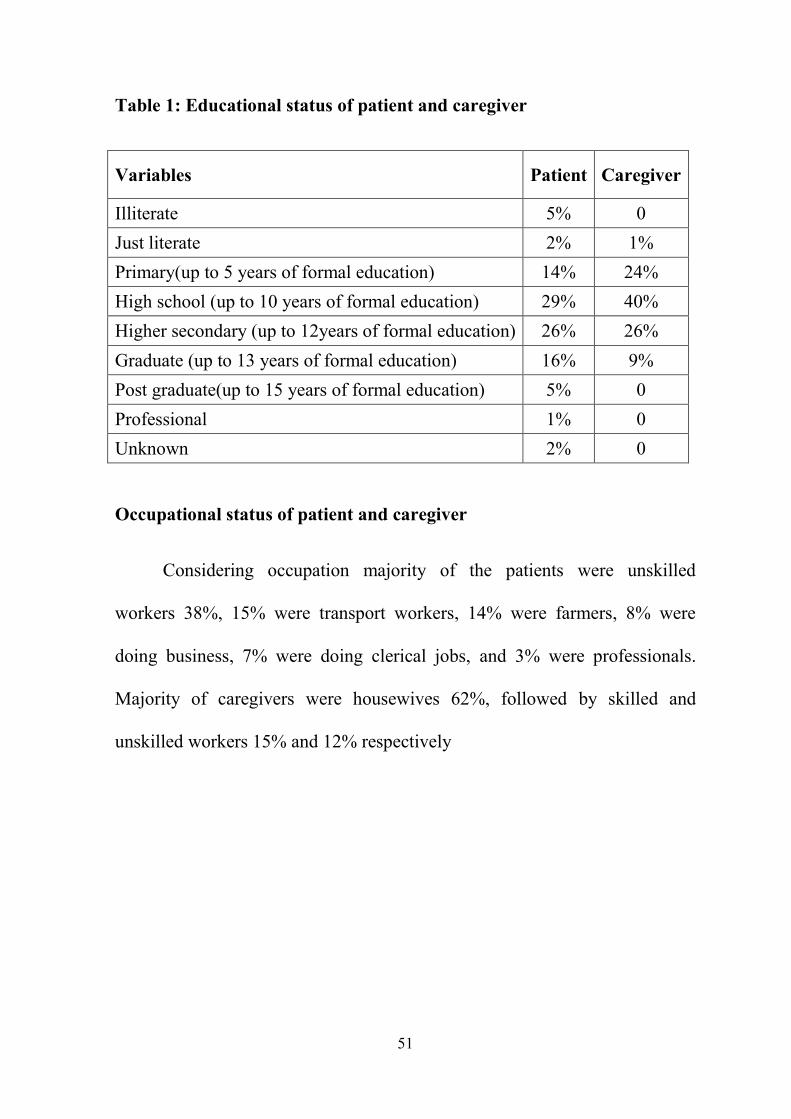
Educational status of patient and caregiver
Among the participants around 5% of the patients were illiterate and
2% of the patients were just literate, 14 percent of the patients completed
primary education up to four five years of formal education, around 29% of
patients completed high school education, 26% studied till 12 years of formal
education, 16% were graduates, 5% completed post-graduation and 1% being
professional, remaining 2% education was unknown. Among caregivers 1%
was just literate, 24% were educated till 5 years of formal education, majority
40% of the caregivers were completed high school (till 10 years of formal
education), 26% were studied till higher secondary and 9% were graduates.
51
Table 1: Educational status of patient and caregiver
Variables Patient Caregiver
Illiterate 5% 0
Just literate 2% 1%
Primary(up to 5 years of formal education) 14% 24%
High school (up to 10 years of formal education) 29% 40%
Higher secondary (up to 12years of formal education) 26% 26%
Graduate (up to 13 years of formal education) 16% 9%
Post graduate(up to 15 years of formal education) 5% 0
Professional 1% 0
Unknown 2% 0
Occupational status of patient and caregiver
Considering occupation majority of the patients were unskilled
workers 38%, 15% were transport workers, 14% were farmers, 8% were
doing business, 7% were doing clerical jobs, and 3% were professionals.
Majority of caregivers were housewives 62%, followed by skilled and
unskilled workers 15% and 12% respectively
52
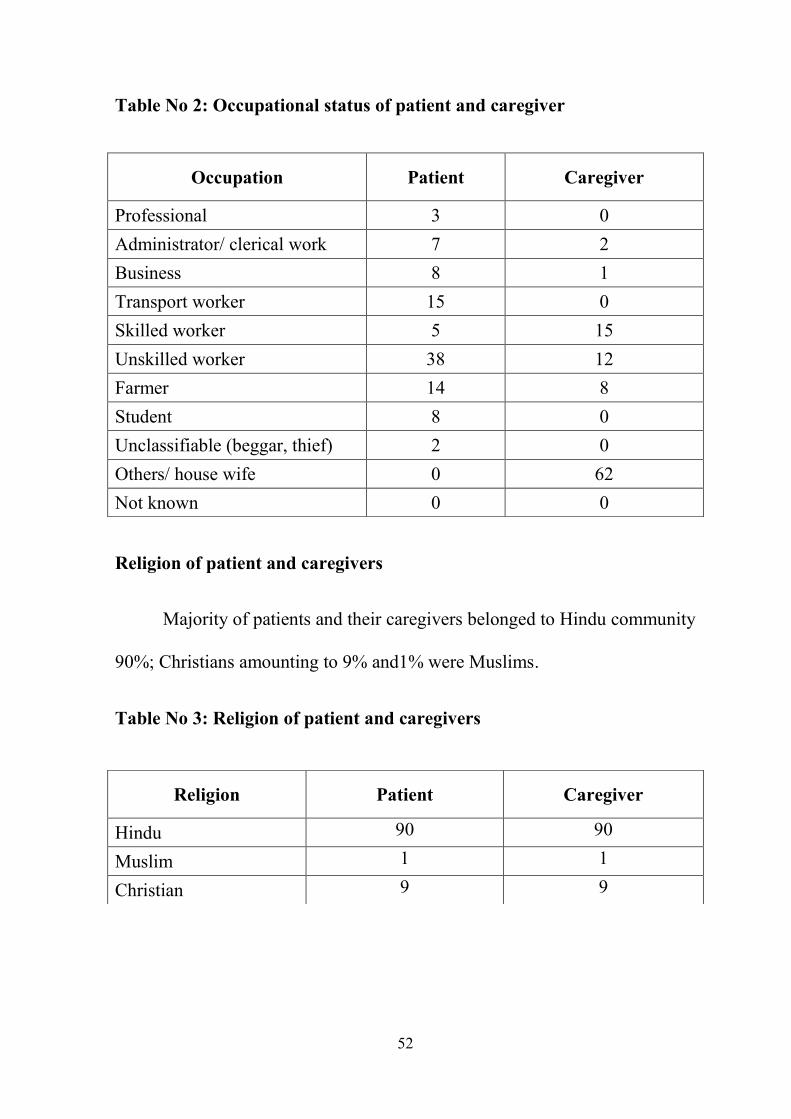
Table No 2: Occupational status of patient and caregiver
Religion of patient and caregivers
Majority of patients and their caregivers belonged to Hindu community
90%; Christians amounting to 9% and1% were Muslims.
Table No 3: Religion of patient and caregivers
Occupation Patient Caregiver
Professional 3 0
Administrator/ clerical work 7 2
Business 8 1
Transport worker 15 0
Skilled worker 5 15
Unskilled worker 38 12
Farmer 14 8
Student 8 0
Unclassifiable (beggar, thief) 2 0
Others/ house wife 0 62
Not known 0 0
Religion Patient Caregiver
Hindu 90 90
Muslim 1 1
Christian 9 9
53
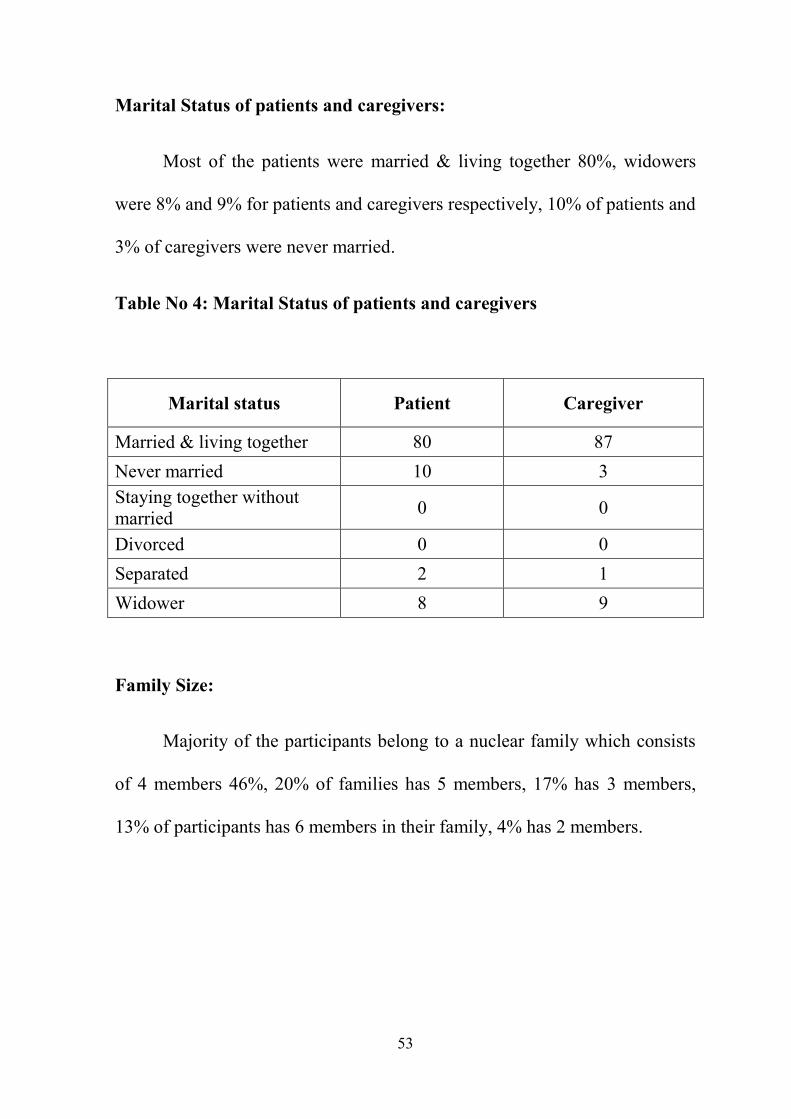
Marital Status of patients and caregivers:
Most of the patients were married & living together 80%, widowers
were 8% and 9% for patients and caregivers respectively, 10% of patients and
3% of caregivers were never married.
Table No 4: Marital Status of patients and caregivers
Family Size:
Majority of the participants belong to a nuclear family which consists
of 4 members 46%, 20% of families has 5 members, 17% has 3 members,
13% of participants has 6 members in their family, 4% has 2 members.
Marital status Patient Caregiver
Married & living together 80 87
Never married 10 3
Staying together without
married 0 0
Divorced 0 0
Separated 2 1
Widower 8 9

54
Table No 5: Family Size
Number of family members Percentage
Two 4%
Three 17%
Four 46%
Five 20%
Six 13%
Caregiver’s relation to the patient
Majority of the caregivers were wives 76%, 9% were mothers, 7%
were daughters to the patients, 4% were fathers, 2% were sons, grandmother
and nephew was 1%
Table No: 6 Caregivers relation to the patient
Relation to the patient Percentage
Wife 77
Mother 9
Daughter 6
Father 4
Son 2
Grandmother 1
Nephew 1
55
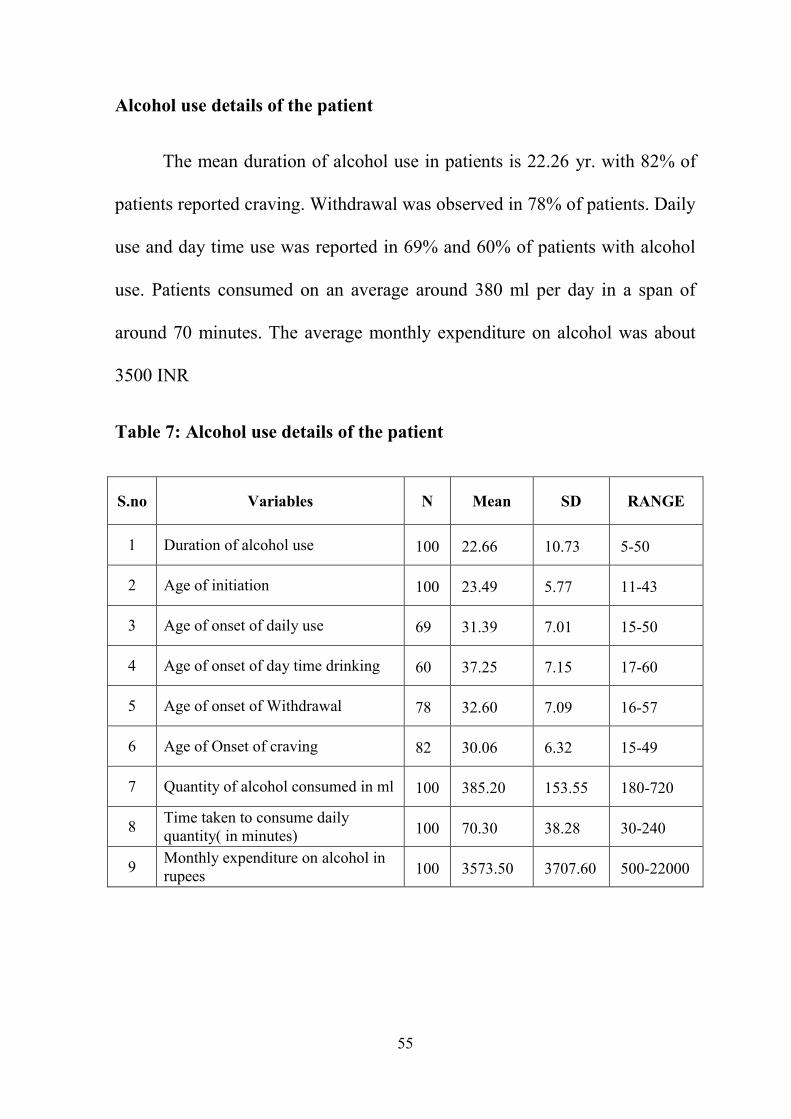
Alcohol use details of the patient
The mean duration of alcohol use in patients is 22.26 yr. with 82% of
patients reported craving. Withdrawal was observed in 78% of patients. Daily
use and day time use was reported in 69% and 60% of patients with alcohol
use. Patients consumed on an average around 380 ml per day in a span of
around 70 minutes. The average monthly expenditure on alcohol was about
3500 INR
Table 7: Alcohol use details of the patient
S.no Variables N Mean SD RANGE
1 Duration of alcohol use 100 22.66 10.73 5-50
2 Age of initiation 100 23.49 5.77 11-43
3 Age of onset of daily use 69 31.39 7.01 15-50
4 Age of onset of day time drinking 60 37.25 7.15 17-60
5 Age of onset of Withdrawal 78 32.60 7.09 16-57
6 Age of Onset of craving 82 30.06 6.32 15-49
7 Quantity of alcohol consumed in ml 100 385.20 153.55 180-720
8 Time taken to consume daily
quantity( in minutes) 100 70.30 38.28 30-240
9 Monthly expenditure on alcohol in
rupees 100 3573.50 3707.60 500-22000
56
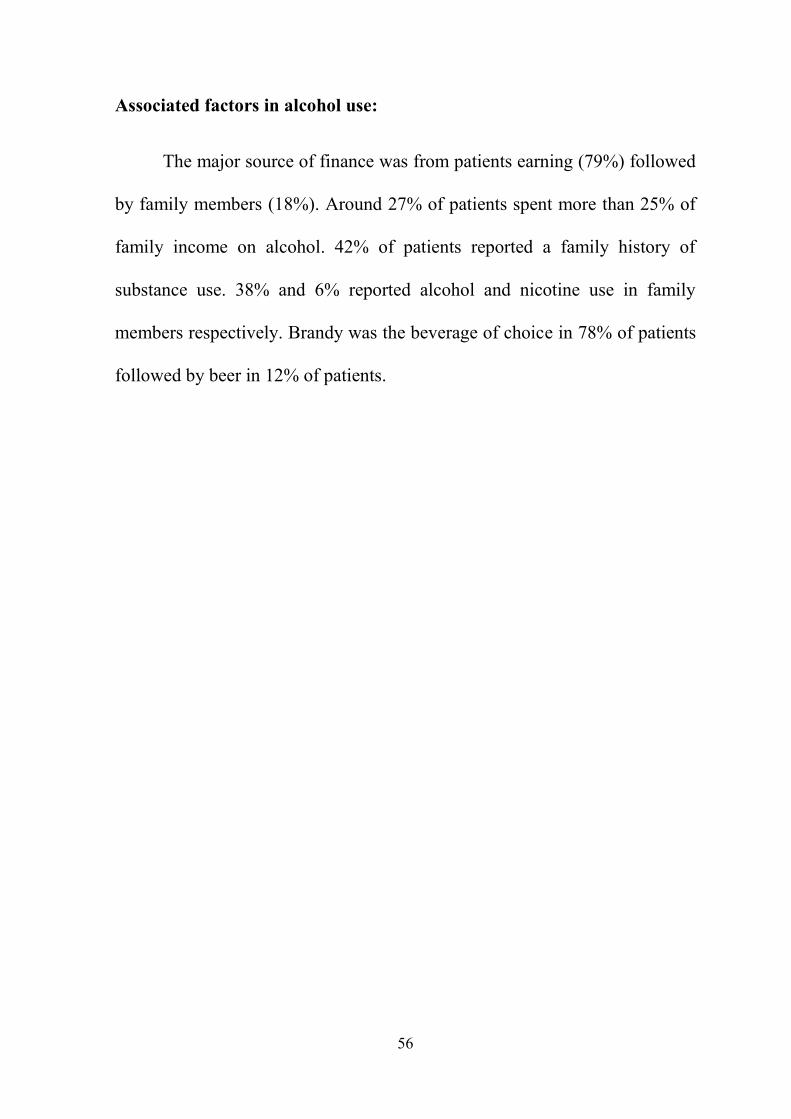
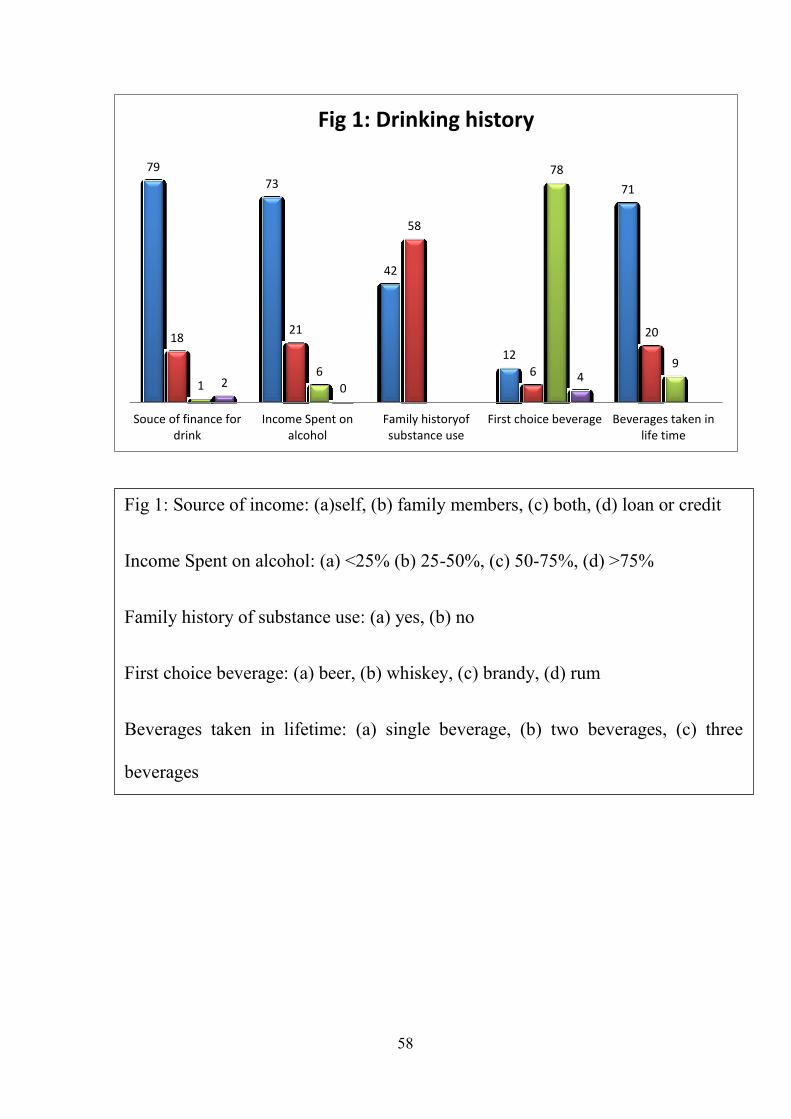
Associated factors in alcohol use:
The major source of finance was from patients earning (79%) followed
by family members (18%). Around 27% of patients spent more than 25% of
family income on alcohol. 42% of patients reported a family history of
substance use. 38% and 6% reported alcohol and nicotine use in family
members respectively. Brandy was the beverage of choice in 78% of patients
followed by beer in 12% of patients.
57
Table No 8: Associated factors in alcohol use:
S.no Variables Frequency in percentage
1 Source of finance for procuring drink
Self 79%
Family members 18%
Both self & family members 1%
Loan / credit 2%
2 Percentage income spend on alcohol
<25% 73%
25-50% 21%
50-75% 6%
>75% -
3 Family history of substance use
Yes 42%
No 58%
Alcohol 38%
Others (Nicotine) 6%
4 Beverages of first choice
Beer 12%
Whiskey 6%
Brandy 78%
Rum 4%
5 Beverages taken in life time
Single beverages 71%
Two beverages 20%
Three beverages 9%
58
79
73
42
12
71
18 21
58
6
20
1 6
78
9
2 0 4
Souce of finance fordrink
Income Spent onalcohol
Family historyofsubstance use
First choice beverage Beverages taken inlife time
Fig 1: Drinking history
Fig 1: Source of income: (a)self, (b) family members, (c) both, (d) loan or credit
Income Spent on alcohol: (a) <25% (b) 25-50%, (c) 50-75%, (d) >75%
Family history of substance use: (a) yes, (b) no
First choice beverage: (a) beer, (b) whiskey, (c) brandy, (d) rum
Beverages taken in lifetime: (a) single beverage, (b) two beverages, (c) three
beverages
59
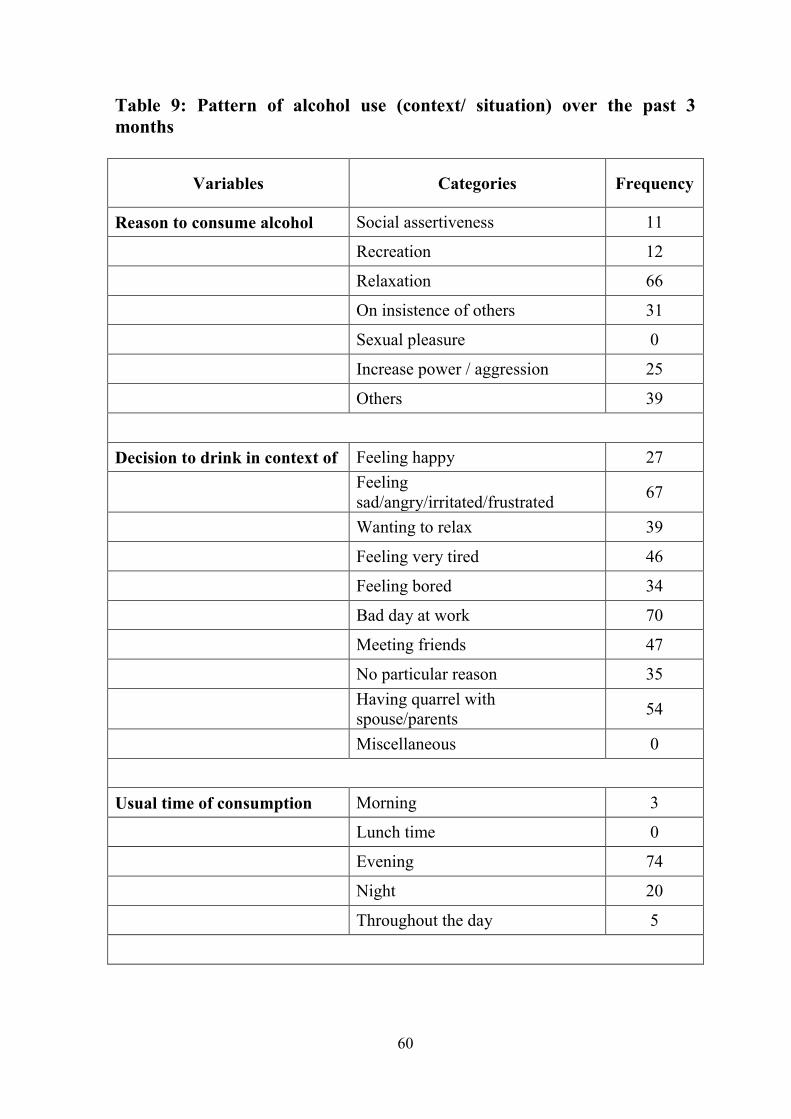
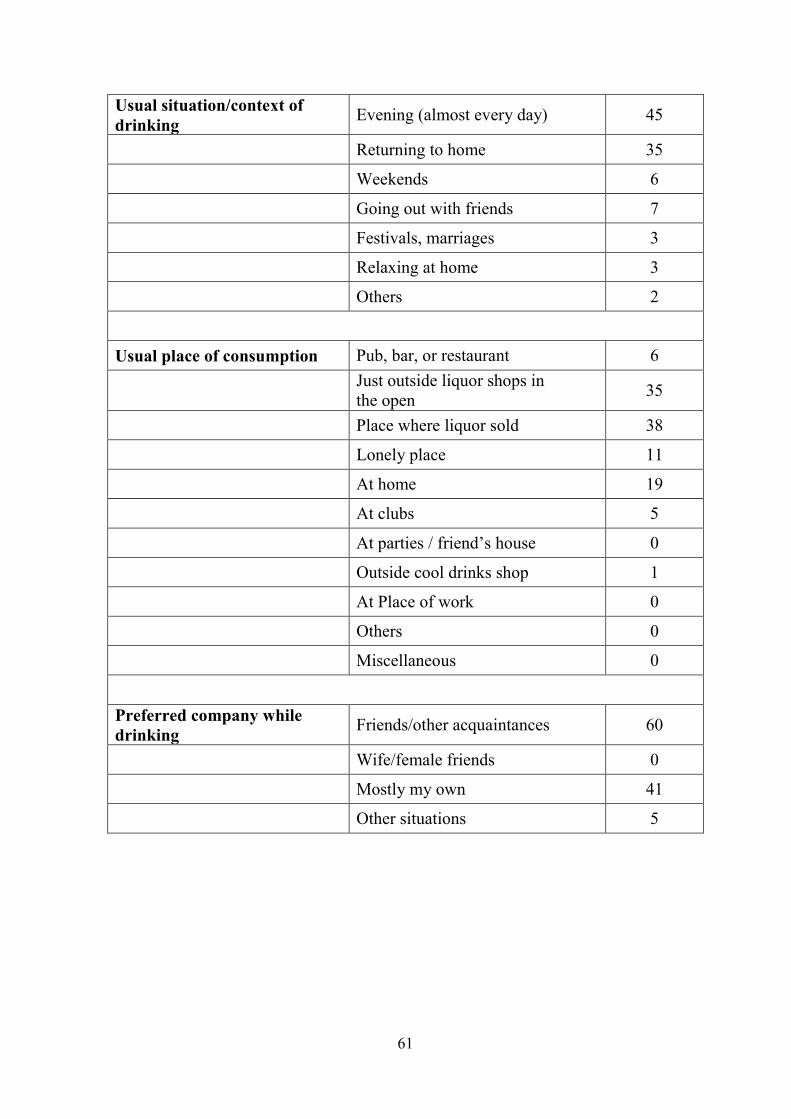
Context & Situation of Alcohol use:
Among patients the major reason to consume alcohol is for relaxation
(66%) followed by others insistence (25%). Negative emotions (67%) and a
bad day at work (70%) are the major drive for alcohol use. 74% of the
population preferred to drink in the evening time. 45% and 35% reported
Evenings and returning to home from job as the more common context of
drinking. 73% of the participants reported to have consumed alcohol either at
or outside the liquor shop. The preferred companion to consume alcohol was
friends (60%).
60
Table 9: Pattern of alcohol use (context/ situation) over the past 3
months
Variables Categories Frequency
Reason to consume alcohol Social assertiveness 11
Recreation 12
Relaxation 66
On insistence of others 31
Sexual pleasure 0
Increase power / aggression 25
Others 39
Decision to drink in context of Feeling happy 27
Feeling
sad/angry/irritated/frustrated 67
Wanting to relax 39
Feeling very tired 46
Feeling bored 34
Bad day at work 70
Meeting friends 47
No particular reason 35
Having quarrel with
spouse/parents 54
Miscellaneous 0
Usual time of consumption Morning 3
Lunch time 0
Evening 74
Night 20
Throughout the day 5
61
Usual situation/context of
drinking Evening (almost every day) 45
Returning to home 35
Weekends 6
Going out with friends 7
Festivals, marriages 3
Relaxing at home 3
Others 2
Usual place of consumption Pub, bar, or restaurant 6
Just outside liquor shops in
the open 35
Place where liquor sold 38
Lonely place 11
At home 19
At clubs 5
At parties / friend’s house 0
Outside cool drinks shop 1
At Place of work 0
Others 0
Miscellaneous 0
Preferred company while
drinking Friends/other acquaintances 60
Wife/female friends 0
Mostly my own 41
Other situations 5

62
Table 10: Pattern of alcohol use (context/ situation) over the past 3 months
11
27
3
45
6
60
12
67
0
35 35
0
66
39
74
6
38 41
31
46
20
7
11
5
0
34
5 3
19
25
70
3 5
39
47
2 1
35
0
54
0
Reason to consume Decision to drink incontext of
Usual time ofconsumption
Usual situation/contextof drinking
Usual place ofconsumption
Preferred companywhile drinking
Fig 2: Pattern of alcohol use (context/ situation) over the past 3 months
Fig 2: 1. reason to consume (a) social assertiveness, (b) recreation, (c) relaxation, (d) others insistence, (e) sexual pleasure, (f) power/ aggression, (g)
others. 2. Decision to drink: (a) feeling happy, (2) negative emotions, (c) to relax, (d) tired, (e) bored, (f) bad day at work, (g) meet friends, (h) no
reasons, (i) quarrels, (j) others. 3. Time of consumption: (a) morning, (b) lunch, (c) evening, (d) night, (e) all time. 4. Place: (a) pub, (b) outside shop, (c)
place where sold, (d) lonely place, (e) home, (f) clubs (g) outside cool drinks shop 4. Company (a) friends, (b) females, (c) alone, (d) others

63
45 44
35 29
80
14 14
33
100
49
21
54
4
20
86 86
67
5
54
11
47
1 1
20
Drinking withfood
Close peoplewho drink
Intoxication Feel after adrink
RestrictionAgainst Drinking
Style of drinking Diluting More than 1beverage in
single occasion
More than 5standard drink
Fig 3:Pattern of alcohol use (style of drinking, social aspect, intoxication) over the past 3 months
Fig 3: 1. Drinking with food: (a) snacks, (b) drink before eat, (c) drink along with meals, (d) doesn’t matter. 2. Close people who drink (a) neighbor, (b)
coworkers, (c) friends (d) others. 3. Intoxication: (a) always, (b) sometimes, (c) never. 4. Feel after a drink: (a) relaxed, (b) guilt, (c) nothing specific, (d)
others. 5. Restriction against drinking: (a) No, (b) yes. 6. Style of drinking: (a) sip, (b) gulp. 7. Diluting (a) neat, (b) mixed. 8. More than 1 beverage in
single time: (a) yes, (b) No. 9. Occasion consumed more than 5 Standard drinks (a) yes
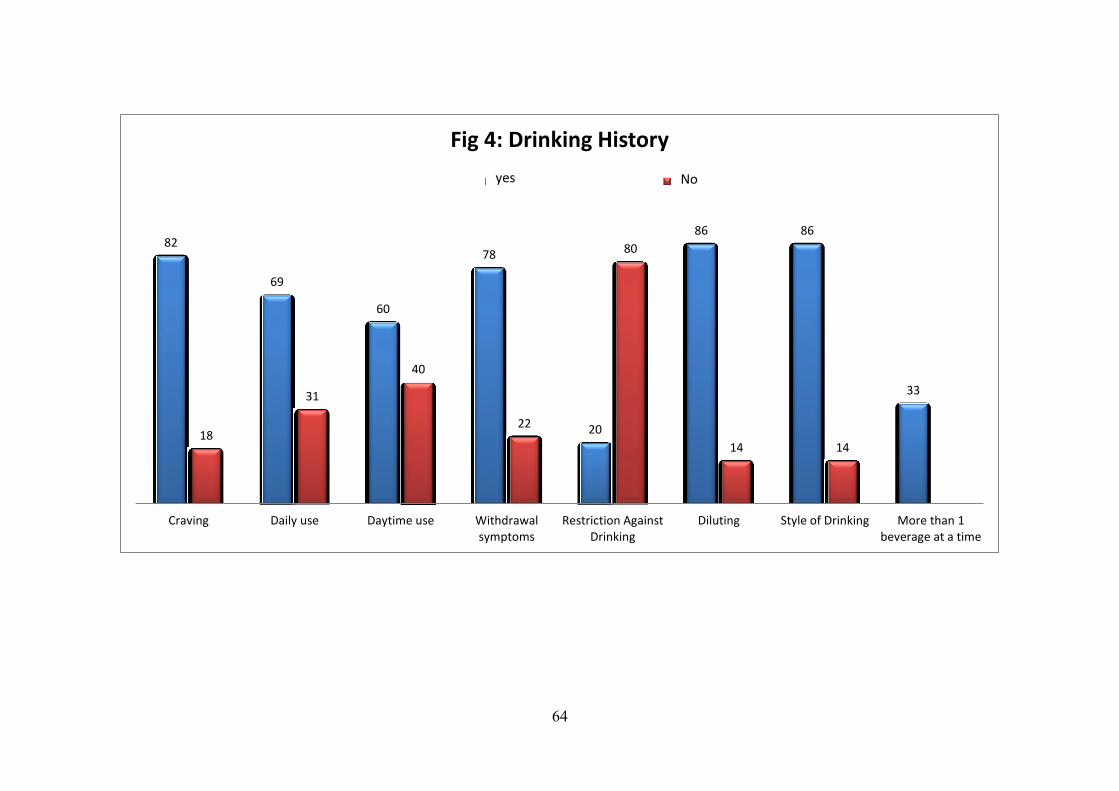
64
82
69
60
78
20
86 86
33
18
31
40
22
80
14 14
Craving Daily use Daytime use Withdrawalsymptoms
Restriction AgainstDrinking
Diluting Style of Drinking More than 1beverage at a time
Fig 4: Drinking History
Series 1 Series 2yes No
65
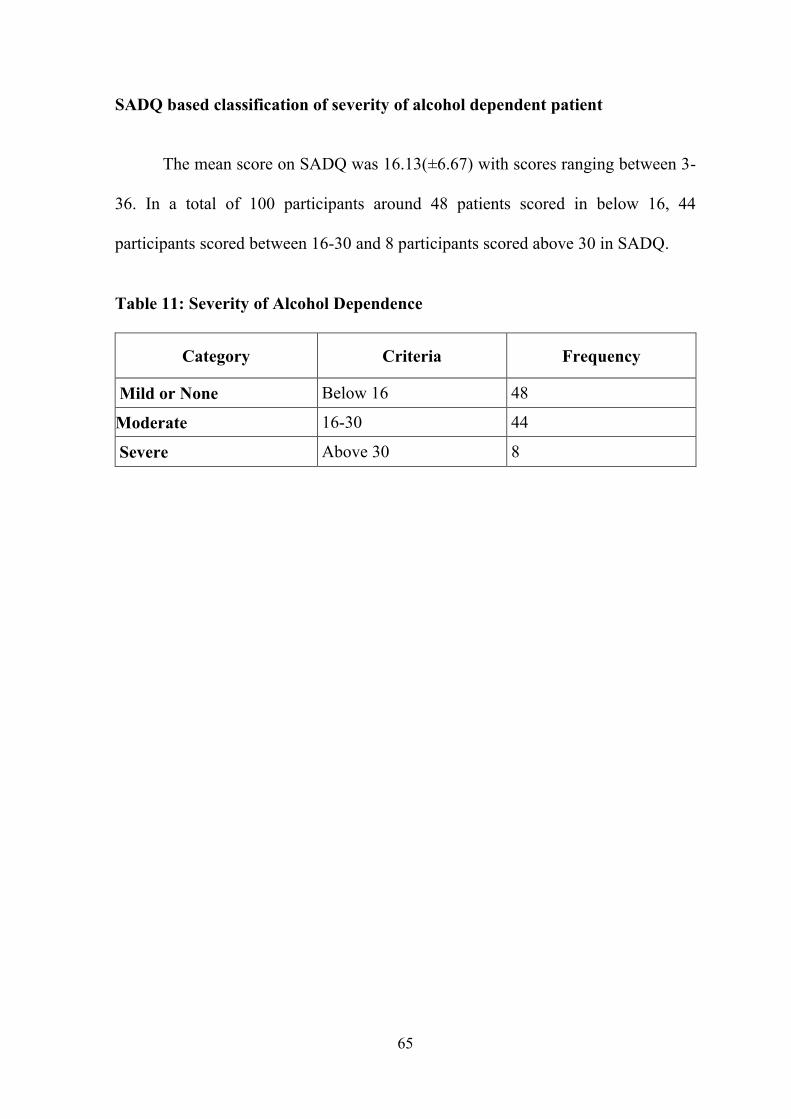
SADQ based classification of severity of alcohol dependent patient
The mean score on SADQ was 16.13(±6.67) with scores ranging between 3-
36. In a total of 100 participants around 48 patients scored in below 16, 44
participants scored between 16-30 and 8 participants scored above 30 in SADQ.
Table 11: Severity of Alcohol Dependence
Category Criteria Frequency
Mild or None Below 16 48
Moderate 16-30 44
Severe Above 30 8

66
General Health Questionnaire for Caregivers
The mean total score on GHQ12 administered to caregivers was
18.42(±6.09) with the range of 3 to 32. Caregivers had higher mean score in
questions assessing feeling depressed (1.94), loss of sleep (1.92), constantly
under strain (1.91).
Table 12: General Health Questionnaire results of caregivers
GHQ 12 Questions Minimum Maximum Mean Std.
Deviation
Been able to concentrate on whatever
you’re doing? 0 3 1.32 0.60
Lost much sleep over worry? 0 3 1.92 0.88
Felt that you are playing a useful part
in things? 0 3 1.19 0.68
Felt capable of making decisions
about things? 0 3 1.32 0.74
Felt constantly under strain? 0 3 1.91 0.92
Felt you couldn’t overcome your
difficulties? 0 3 1.46 0.81
Been able to enjoy your normal day-
to-day activities? 0 3 1.57 0.86
Been able to face up to your
problems? 0 3 1.52 0.81
Been feeling unhappy and depressed 0 3 1.94 0.95
Been losing confidence in yourself? 0 3 1.44 0.82
Been thinking of yourself as a
worthless person? 0 3 1.43 0.83
Been feeling reasonably happy all
things considered? 0 3 1.37 0.65
GHQTOTAL 3.0 32.0 18.42 6.09

67
Family burden scores
The mean scores of each questions in Family burden interview
schedule is calculated and the overall mean scores is computed. The mean
scores were observed to be higher in the expenditure incurred due to patients
illness(1.19), loans or savings spent(1.01), putting off planned activity due to
financial pressures(1.01) in the Financial Burden domain. There was higher
mean score in interaction domain mainly in arguments with others (1.09) and
effects on relationship (1.11). Physical health domain showed higher mean
scores on both variables and psychological help seeking in caregivers (1.05)
in the mental health burden domain of FBIS. The total FBIS mean score was
19.93 with the range of 4-44.

68
Table 13: Family Burden scores in caregivers
S.no Family Burden Questionnaire Range Mean SD
1 Loss of patient's income 0 - 2 0.50 0.56
2 Loss of income of any other family member 0 - 2 0.38 0.53
3 Expenditure incurred due to patient's illness and
treatment 0 - 2 1.19 0.65
4 Expenditure incurred due to extra arrangements 0 - 2 0.15 0.39
5 Loans taken or savings spent 0 - 2 1.01 0.63
6 Any other planned activity put off because of the
financial pressure of the patient's illness 0 - 2 1.01 0.69
7 Patient not going to work, school, college, etc.:
How inconvenient is this for the family? 0 - 2 0.94 0.57
8 Patient not helping in the household work: How
much does this affect the family? 0 - 2 0.99 0.46
9 Disruption of activities of other members of the
family 0 - 2 0.77 0.60
10 Patient's behaviour disrupting activities 0 - 2 0.83 0.62
11 Neglect of the rest of the family due to patient's
illness 0 - 2 0.93 0.59
12 Stopping of normal recreational activities 0 - 2 0.85 0.58
13 Patient's illness using up another person's holiday
and leisure time 0 - 2 0.92 0.56
14 Patient's lack of attention to other members of the
family 0 - 2 0.72 0.64
15 Has any other leisure activity had to be abandoned
owing to the patient's illness or incapacity 0 - 2 0.90 0.58
16 Any ill effect on the general atmosphere in the
house 0 - 2 0.35 0.54
17 Do other members get into argument over this 0 - 2 1.09 0.68
18 Have relatives and neighbours stopped visiting the
family 0 - 2 0.42 0.55
19 Has the family become secluded 0 - 2 0.59 0.59
20 Has the patient's illness had any other effect on
relationships within the family or between the
family and neighbours or relative
0 - 2 1.11 0.65
21 Have any other members of the family suffered
physical ill health, injuries, etc. due to the patient's
behaviour
0 - 2 1.11 0.83
22 Has there been any other adverse effect on health 0 - 2 1.13 0.83
23 Has any other family member sought help for-
psychological illness brought on by the patient's
behaviour
0 - 2 1.05 0.61
24 Has any other member of the family lost sleep,
become depressed or weepy, expressed suicidal
wishes, become excessively irritable, etc.
0 - 2 0.99 0.66
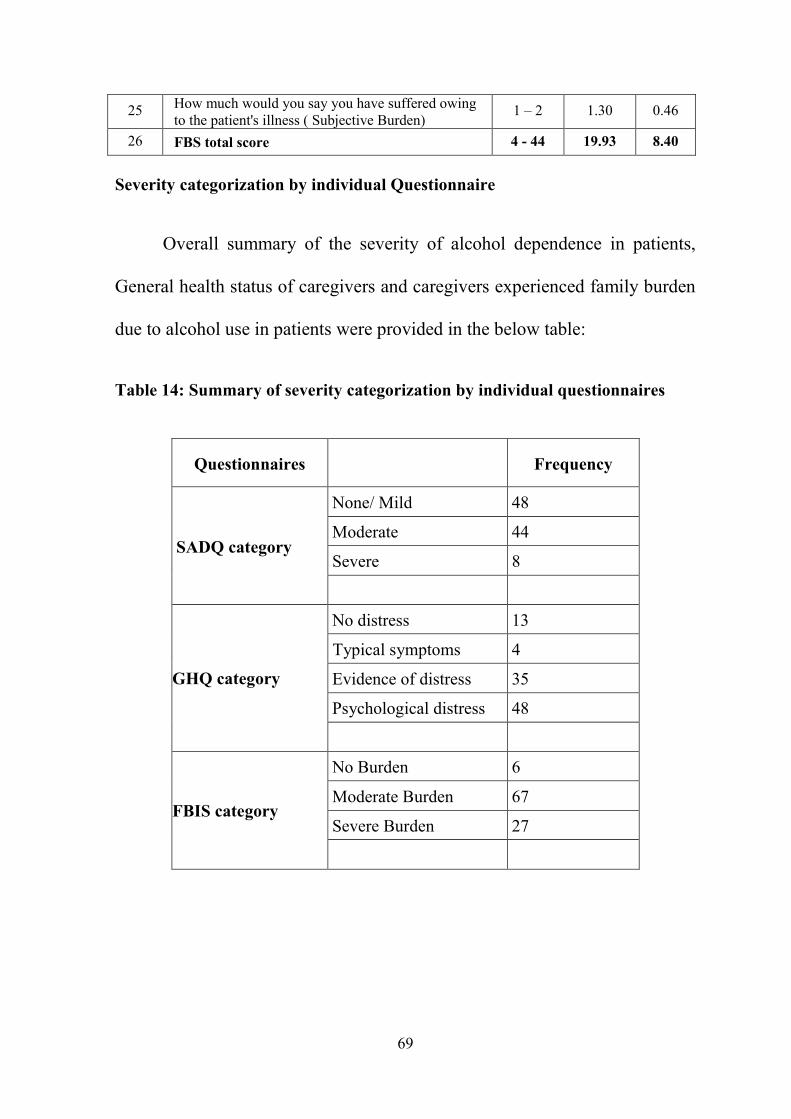
69
25 How much would you say you have suffered owing
to the patient's illness ( Subjective Burden) 1 – 2 1.30 0.46
26 FBS total score 4 - 44 19.93 8.40
Severity categorization by individual Questionnaire
Overall summary of the severity of alcohol dependence in patients,
General health status of caregivers and caregivers experienced family burden
due to alcohol use in patients were provided in the below table:
Table 14: Summary of severity categorization by individual questionnaires
Questionnaires Frequency
SADQ category
None/ Mild 48
Moderate 44
Severe 8
GHQ category
No distress 13
Typical symptoms 4
Evidence of distress 35
Psychological distress 48
FBIS category
No Burden 6
Moderate Burden 67
Severe Burden 27

70
Correlations between Alcohol use characteristics in patients and General
health status and Family burden in caregivers:
Age of the patient is positively correlated with SADQ, age of
caregiver, GHQ and FBIS scores and negatively correlated with family
income. Duration of alcohol use is positively correlated with SADQ, GHQ
and FBIS score. There seems to be a positive association between monthly
expenses on alcohol with SADQ, GHQ, FBIS and subjective burden scores.
Quantity of alcohol consumed is positively correlated with SADQ, GHQ, FBIS and
subjective burden. SADQ scores are positively correlated with GHQ, FBIS and
subjective burden scores. GHQ scores are positively correlated with FBIS and
Subjective burden scores.
SADQ Category GHQ Category FBIS Category Subjective Burden
48
13
6 0
44
4
67 70
8
35
27 30
48
Fig 5:Severity categorization on individual Questionnaire
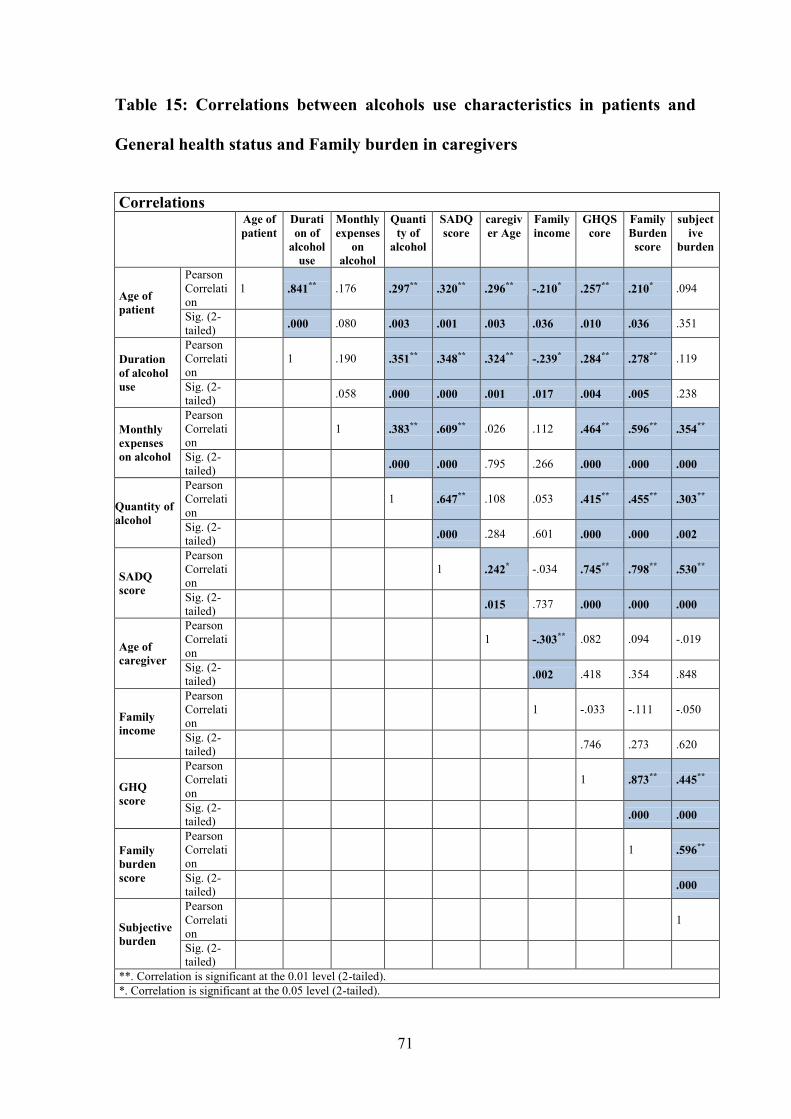
71
Table 15: Correlations between alcohols use characteristics in patients and
General health status and Family burden in caregivers
Correlations
Age of
patient
Durati
on of
alcohol
use
Monthly
expenses
on
alcohol
Quanti
ty of
alcohol
SADQ
score
caregiv
er Age
Family
income
GHQS
core
Family
Burden
score
subject
ive
burden
Age of
patient
Pearson
Correlati
on
1 .841** .176 .297** .320** .296** -.210* .257** .210* .094
Sig. (2-
tailed) .000 .080 .003 .001 .003 .036 .010 .036 .351
Duration
of alcohol
use
Pearson
Correlati
on 1 .190 .351** .348** .324** -.239* .284** .278** .119
Sig. (2-
tailed) .058 .000 .000 .001 .017 .004 .005 .238
Monthly
expenses
on alcohol
Pearson
Correlati
on
1 .383** .609** .026 .112 .464** .596** .354**
Sig. (2-
tailed) .000 .000 .795 .266 .000 .000 .000
Quantity of
alcohol
Pearson
Correlati
on 1 .647** .108 .053 .415** .455** .303**
Sig. (2-
tailed) .000 .284 .601 .000 .000 .002
SADQ
score
Pearson
Correlati
on 1 .242* -.034 .745** .798** .530**
Sig. (2-
tailed) .015 .737 .000 .000 .000
Age of
caregiver
Pearson
Correlati
on 1 -.303** .082 .094 -.019
Sig. (2-
tailed) .002 .418 .354 .848
Family
income
Pearson
Correlati
on 1 -.033 -.111 -.050
Sig. (2-
tailed) .746 .273 .620
GHQ
score
Pearson
Correlati
on 1 .873** .445**
Sig. (2-
tailed) .000 .000
Family
burden
score
Pearson
Correlati
on 1 .596**
Sig. (2-
tailed) .000
Subjective
burden
Pearson
Correlati
on
1
Sig. (2-
tailed)
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).

72
Spouse vs. others as caregivers
77 patients had spouse as caregivers and in 23 patients the caregivers were
mother, father, daughter, son, grandmother and nephew. There was no significant
difference observed between the groups in the severity of alcohol use in patients,
GHQ scores and Family burden score
Table: Spouse vs. others as caregivers
S. no Criteria Category Spouse as
caregivers
(n= 77)
Others as
caregivers
(n= 23)
χ2
/ ‘t’
value
“p”
value
1 SAD Q Mild/ none 37 11 3.87 0.14
Moderate 36 8
Severe 4 4
Mean Score(SD) 15.64(5.95) 17.78(8.6) -1.36 0.17
2 GHQ No distress 11 2 2.36 0.50
Typical symptoms 2 2
Evidence of distress 28 7
Psychological
distress 36 12
Mean Score(SD) 18.16(5.93) 19.30(6.64) -0.75 0.46
3 FBIS No Burden 6 0 2.48 0.29
Moderate Burden 52 15
Severe Burden 19 8
Mean Score(SD) 19.22(7.95) 22.30(9.57) -1.41 0.17
Chi square test for categorical variable and independent‘t’ test for continuous
variables

73
DISCUSSION
74
DISCUSSION
Alcohol use disorder not only affects the patients but also the
individuals who are taking care of them. It affects the family in various levels
like social issues, occupational dysfunction physical health problems, mental
stress and financial burden.
This study was conducted to know about the pattern of alcohol use and
its severity and also how it contributes to care giver burden. This study was
carried out in outpatient and inpatient setting in the department of psychiatry
in a tertiary hospital in Maduranthagam Taluk.
A total of 100 participants and their caregivers were included in this
study. The study comprises of socio demographic details such as age,
education, marital status, occupation, monthly income and residing
background.
Duration of alcohol use:
The mean age of onset of alcohol consumption was 23.49 years in our
study, which is similar to the mean age of onset of alcohol use in the study
conducted by Gupta et al34
which was 21.5 years.
In a cross sectional study conducted by Gupta et al34
found the
participants were problem alcohol users and non-treatment seekers. Whereas
75
our study sample includes individuals who were seeking treatment for
alcohol use disorders
Drinking pattern:
In our study 100 adult males with alcohol use disorders were recruited
and interviewed using questionnaire and standard instruments. Drinking
pattern and style of drinking along with its severity was assessed by severity
of alcohol dependence questionnaire and a semi structured questionnaire. In
our study the participants had a long history of alcohol use with the presence
of features of physical dependence such as withdrawals as well as features of
psychological dependence such as craving for more than a decade which is
similar to Gupta et al34
study. Additionally, it took the participants around 70
minutes to consume their quantity of alcohol. Not surprisingly, almost all of
the participants reported drinking more than 5 standard drinks in the past
3months. Most of our participants spent more than 25% amount of money for
alcohol from their family income.
Caregivers
Poor social performance of one member reciprocally affects the
performance of any other member of the family, who has to compensate the
deficiencies, experiencing burden. This led to the differentiation of burden
into subjective and objective (Hoenig et al70
, 1966).
76
Oldridge et al71
(1992) reported that psychological distress (anxiety,
depression, and insomnia) was twice as high in caregivers as in the general
population.
In our study, caregivers experienced burden in financial domain and in
family interaction domain. They also showed significant burden in physical
and mental health. The above findings matched with Vaishnavi et al47
study.
This is probably because in a country like India males are considered to be
the bread winners of the family (Kiran et al72
).
Our study reveals that majority of the caregivers were females. Among
them most of the caregivers were spouses of patients with alcohol use
disorders Majority of caregivers were not employed and it is similar to
Lennox et al73
study.
A study conducted by Devi et al74
in a nursing college with sample of
70 alcoholic’s wives reveals that around 43% had moderate stress levels and
they average coping strategies which is similar to our GHQ scorings and
caregiver burden scores.
When considering caregiver burden in alcohol use disorder individuals
we have not only focused on spouses but also included other caregivers and
assessed the burden as similar to Rospenda et al75
study in a community
sample within the Chicago city.
77
Domestic violence is the major problem in spouses of alcohol
dependent individuals which is found in a study conducted by
Nanjundaswamy et al76
at NIMHANS whereas our study focusing on
different domains of caregiver burden in alcohol use disorders that includes
financial burden, disruption in family routine and family leisure, disruption in
family interaction, effects of physical health and mental health also showed
high mean score on questions pertaining to injuries sustained due to patient’s
behaviour
Similar study on family members with alcohol dependent people
showed an increase in the risk of the emergence of mental disorders in
spouses, and a greater frequency of physical assaults, deaths of family
members and involvement with the police in those homes. This issue affects
their Quality of life, and predisposes them to the emergence of depressive
symptoms
Presence of alcohol dependence in patient is an important factor which
influences caregiver’s psychiatric morbidity and quality of life and severity
of alcohol dependence in patients was positively correlated with psychiatric
morbidity in caregivers. With increasing dose, duration and severity of
alcohol use results in significant increase in psychological morbidity in
caregivers
78
Quality of life of was found to be significantly poor among caregivers
with psychiatric illness than caregivers without psychiatric illness. We found
that there is a positive correlation between the subjective burdens in
caregivers of individuals with alcohol use disorders
Our study shows more burden among caregivers of higher alcohol
dependence scores which is similar to the findings by Swaroopachary et
al52
., which concluded more burden is seen in seen in severe alcohol
dependence patients.
Based on our study there is a positive correlation found between
SADQ, subjective burden and GHQ 12 and thus caregivers of men with
alcohol use disorder have significantly greater chances of developing anxiety,
depression and other psychiatric morbidities when compared with wives of
men who do not consume alcohol. This is a major problem because increased
psychiatric morbidity in women affects not only them but the entire family
unit, with long-standing consequences. The finding is similar to the study
conducted by Gandhi et al77
., but that was a comparative study. They
compared the group of caregivers of men with alcohol use disorder and men
without alcohol use disorders
Alcohol abuse is associated with marital conflicts, violence against
family members, assault and high risk of committing criminal offences. A
person who uses alcohol can disrupt the routine life of caregivers that leads to
79
harmful consequences which affects their physical and mental health that can
last long their lifetime. The finding is similar to Vishal et al50
but in their
study 50 cases (spouses of alcohol dependence patients) versus 50 controls
(spouses of non-alcohol dependence patients but some other illness)
80
STRENGTHS OF THE STUDY:
Though many studies showed correlation between alcohol use and the
burden in care givers, our study measured the positive correlation with
severity of alcohol dependence with general health of the caregivers and their
burden in different aspects
LIMITATIONS:
There were certain limitations in this study.
The causality could not be explained since this is a cross sectional
study.
This study was conducted in a tertiary setting and it cannot be
generalized to community
There is no comparison group in our study
All the patient population were males who are above 18. So, the results
cannot be generalized to adolescent male and female patient
population.
Most of the caregivers were females and there were less male care
givers. And also the study was predominantly populated by spouses as
caregivers but other caregiver population subgroups were less.
81
SUMMARY
In our study the mean age of the patient was 46.13(± 10.95) years and
mean age of the caregiver 42.03(±10.03) years. All the patients
participated in this study were males and 93 caregivers were females
whereas 7 caregivers were males.
Mean duration of alcohol use in patients is 22.26 year with daily use in
69% of patients. 82% of patients reported craving. Withdrawal was
observed in 78% of patients
Average alcohol consumed per day is 380 ml
Average monthly expenditure on alcohol was about 3500 INR
Most of the patients consumed alcohol for relaxation (66%),
preferably in the evening time (74%) and in the company of friends
(60%).
In SAD Q about 48% had mild/ no dependence, 44% had moderate
dependence and 8% had severe dependence
87% of caregivers expressed distress as measured by GHQ 12
In FBIS, All caregivers experienced subjective burden (mild/none-0,
moderate burden- 70% and severe burden- 30%), Whereas 94% of
caregivers experienced objective burden (6%- none, 67% - moderate,
27%- severe burden)

82
Severity of dependence, duration of alcohol use, monthly expenditure
on alcohol, quantity of alcohol use, impacts the general health status
and perceived burden (family as well as subjective burden) of the
caregivers.

83
CONCLUSION
84
CONCLUSION:
The severity of alcohol use measured by SADQ is positively correlated
with impairment in general health status of caregivers as measured in
GHQ-12.
The severity of alcohol use is also positively correlated with subjective
burden as well as objective burden in FBIS scores (all six domains)
The duration of alcohol use is positively correlated with impairment in
general health status and perceived family burden of the caregivers
In addition, monthly expenditure on alcohol and quantity of alcohol
consumed in a day are positively correlated with impairment in general
health status of caregivers, family burden scores and subjective burden.
Overall, severity of dependence, duration of alcohol use, monthly
expenditure on alcohol, quantity of alcohol use, impacts the general
health status and perceived burden (family as well as subjective
burden) of the caregivers
85
FUTURE DIRECTIONS:
Studies focused on community setting with comparison group for
better results. Researchers should consider doing cohort study so that the
causality can be explained clearly. The future studies can consider including
adolescent population and their care giver burden.
86
BIBLIOGRAPHY

87
BIBLIOGRAPHY
1. Avasthi A. Preserve and strengthen family to promote mental health.
Indian journal of psychiatry. 2010; 52 (2):113-126.
2. World Health Organization, Global Status Report on Alcohol, World
Health Organization, Geneva, Switzerland, 2014
3. Diagnostic and Statistical Manual of mental disorders, Substance-
Related and Addictive Disorders, Alcohol-Related disorders
4. Dick DM & Kendler KS (2012) The impact of gene–environment
interaction on alcohol use disorders. Alcohol Research, 34(3), 318–
324.
5. Gelernter J (1995) Genetic factors in alcoholism: evidence and
implications. In Kranzler HR(ed.) The Pharmacology of Alcohol
Abuse. NewYork,NY: Springer, pp. 297–313.
6. Kendler KS (2001) Twin studies of psychiatric illness. Archives of
General Psychiatry, 58, 1005–1014.
7. Kendler KS, Prescott CA, Neale MC, et al. (1997) Temperance board
registration for alcohol abuse in a national sample of Swedish male
twins born 1902–1949. Archives of General Psychiatry, 54, 178–184.
8. McGue M (1994) Genes, environment, and the etiology of alcoholism.
In Zucker R, Boyd G, & Howard J (eds.) The Development of Alcohol
Problems: Exploring the Biopsychosocial Matrix of
Risk.NIAAAResearch Monograph No. 26. Rockville, MD: US
Department of Health and Human Services, pp. 1– 40.
88
9. Thomasson HR, Crabb DW, Edenberg HJ, et al. (1993) Alcohol and
aldehyde dehydrogenase polymorphins and alcoholism. Behavior
Genetics, 23, 131–136.
10. Chen C-C, Lu R-B, Chen Y-C, et al. (1999) Interaction between the
functional polymorphisms of the alcohol-metabolism genes in
protection against alcoholism. American Journal of Human Genetics,
65(3):795–807.
11. Bierut LJ, Goate AM, Breslau N, et al. (2012) ADH1B is associated
with alcohol dependence and alcohol consumption in populations of
European and African ancestry. Molecular Psychiatry, 17(4), 445–450.
12. Hesselbrock VM, Foroud T, Edenberg H, et al. (2001) Genetics and
alcoholism: the COGA Project. In Agarwal DP & Seitz HK (eds.)
Alcohol in Health and Disease. New York, NY: Marcel Dekker, pp.
103–124.
13. Reich T, Edenberg HJ, Goate A, et al. (1998) Genome-wide search for
genes affecting the risk for alcohol dependence. American Journal of
Medical Genetics, 81, 207–215.
14. Long JC, KnowlerWC,Hanson RL, et al. (1998) Evidence for genetic
linkage to alcohol dependence on chromosomes 4 and 11 from an
autosomewide scan in an American Indian population. American
Journal of Medical Genetics, 81, 216–221.

89
15. WHO 2018 report, Global strategy to reduce the Harmful use of
Alcohol, World Health Organization, September 21, 2018, Geneva
16. Peer K, Rennert L, Lynch K, et al; prevalence of DSM- IV alcohol,
cocaine, opioid and cannabis use disorders in a largely substance
dependent sample. Drug Alcohol Depend Aug 9, 2012.
17. Kessler RC, Crum RM, Warner LA, et al. (1997) Lifetime co-
occurrence of DSM-III-R alcohol abuse and dependence with other
psychiatric disorders in the National Comorbidity Survey. Archives of
General Psychiatry, 54, 313–321
18. Grant BF, Dawson DA, Stinson FS, et al. (2006) The 12-month
prevalence and trends in DSM-IV alcohol abuse and dependence:
United States, 1991–1992 and 2001–2002. Alcohol Research and
Health, 29(2), 79–91.
19. Grant BF, Stinson FS, Dawson DA, et al. (2004a). Co-occurrence of
12- month alcohol and drug use disorders and personality disorders in
the United States: results from the National Epidemiologic Survey on
Alcohol and Related Conditions. Archives of General Psychiatry,
61(4), 361–368.
20. Babor TF, Kranzler HR & Lauerman RL (1987) Social drinking as a
health and psychosocial risk factor: Anstie’s limit revisited. In Galanter
M (ed.) Recent Developments in Alcoholism, Vol.5 New York, NY:
Plenum Press, pp. 373–402.

90
21. Centers for Disease Control and Prevention (2012) Alcohol and Public
Health: Alcohol Related Disease Impact (ARDI), http://apps.nccd.cdc.
22. Hasin DS, Stinson FS, Ogburn E, et al. (2007) Prevalence, correlates,
disability, and comorbidity of DSM-IV alcohol abuse and dependence
in the United States: results from the National Epidemiologic Survey
on Alcohol and Related Conditions. Archives of General Psychiatry,
64(7), 830–842.
23. Kessler RC, McGonagle KA, Zhao S, et al. (1994) Lifetime and 12-
month prevalence of DSM-III-R psychiatric disorders in the United
States. Archives of General Psychiatry, 51, 8–19.
24. Stinson FS, Grant BF, Dawson DA, et al. (2005) Comorbidity between
DSM-IV alcohol and specific drug use disorders in the United States:
results from the national epidemiologic survey on alcohol and related
conditions. Drug and Alcohol Dependence, 80(1), 105–116.
25. Swendsen JD, Merikangas KR, Canino GJ, et al. (1998) the
comorbidity of alcoholism with anxiety and depressive disorders in
four geographic communities. Comprehensive Psychiatry, 39, 176–
184.
26. Grant BF, Stinson FS, Dawson DA, et al. (2004b) Prevalence and co-
occurrence of substance use disorders and independent mood and
anxiety disorders. Archives of General Psychiatry, 61(8), 807–816.
91
27. MeyerRE(1986) Howto understand the relationship between
psychopathology and addictive disorders: another example of the
chicken and the egg. In Meyer RE (ed.) Psychopathology and
Addictive Disorder. New York, NY: Guilford Press, pp. 3–16.
28. Rounsaville BJ, Dolinsky ZS, Babor TF, et al. (1987) Psychopathology
as a predictor of treatment outcome in alcoholics. Archives of General
Psychiatry, 44, 505–513.
29. SchuckitMA(1983) Alcoholic patients with secondary depression.
American Journal of Psychiatry, 140, 711–714.
30. O’Sullivan K, Rynne C, Miller J, et al. (1988) A follow-up study on
alcoholics with and without co-existing affective disorder. British
Journal of Psychiatry, 152, 813–819.
31. Powell BJ, Penick EC, Nickel EJ, et al. (1992) Outcomes of comorbid
alcoholic men: a 1-year follow-up. Alcoholism, Clinical and
Experimental Research, 16, 131–138
32. Babor T, Caetano R, Casswell S, et al. 2010 alcohol: No ordinary
commodity- Research and public policy. NewYork, Oxford University
Press
33. Room R, Jernigan D & Carline-Marlatt B (2002) Alcohol in
Developing Societies. Helsinki: Finnish Foundation for Alcohol
Studies
92
34. Gupta S, Lal R, Rao R, Mishra AK, Ambekar A. Pattern of alcohol use
among problem alcohol users in a community-based setting in India: A
cross-sectional study. J Substance Use. 2018 Mar 4 [cited 2019 Aug
3];23(2):130–5. https://doi.org/10.1080/14659891.2017.1366557
35. Sarkar AP, Sen S, Mondal S, Singh OP, Chakraborty A, Swaika B. A
study on socio-demographic characteristics of alcoholics attending the
de-addiction center at Burdwan medical college and hospital in West
Bengal. Indian J Public Health 2013;57:33-5.
36. S. K. Sampath, P. K. Chand, and P. Murthy, “Problem drinking among
male inpatients in a rural general hospital,” Indian Journal of
Community Medicine, vol. 32, article 93, 2007.
37. John, A. Barman, D. Bal et al., “Hazardous alcohol use in rural
southern India: nature, prevalence and risk factors,”
38. Benegal, V. (2005). India: Alcohol and public health. Addiction,
100(8), 1051–1056. doi:10.1111/j.1360-0443.2005.01176.x
39. Vilamovska, A.-M., Brown Taylor, D., & Bluthenthal, R. N. (2009).
Adverse drinking-related consequences among lower income, racial,
and ethnic minority drinkers: Cross-sectional results. Alcoholism:
Clinical and Experimental Research, 33(4), 645–653. doi:10.1111/
j.1530-0277.2008.00879.x

93
40. Brien, S. E., Ronksley, P. E., Turner, B. J., Mukamal, K. J., & Ghali,
W. A. (2011). Effect of alcohol consumption on biological markers
associated with risk of coronary heart disease: Systematic review and
meta-analysis of interventional studies. BMJ, 342, d636.
doi:10.1136/bmj.d636
41. Mukamal, K. J., Maclure, M., Muller, J. E., & Mittleman, M. A.
(2005). Binge drinking and mortality after acute myocardial infarction.
Circulation, 112 (25), 3839–3845.
doi:10.1161/CIRCULATIONAHA.105.574749
42. Ghosh, S., Samanta, A., & Mukherjee, S. (2012). Patterns of alcohol
consumption among male adults at a slum in Kolkata, India. Journal of
Health, Population and Nutrition, 30(1), 73.
43. Studer, J., Baggio, S., Deline, S., N’Goran, A. A., Henchoz, Y.,
Mohler- Kuo, M. Gmel, G. (2015). Drinking locations and alcohol-
related harm: Cross-sectional and longitudinal associations in a sample
of young Swiss men. The International Journal on Drug Policy, 26(7),
653–661. doi:10.1016/j.drugpo.2014.11.004
44. Steinglass.P : The impact of alcoholism on the family relationship
between degree of alcoholism and psychiatric symptomatology;
Journal of studies on Alcohol 1981; 42:288-303.
94
45. P. M. Shyangwa, B. M. Tripathi, and R. Lal, “Family burden in opioid
dependence syndrome in tertiary care centre,” Journal of the Nepal
Medical Association, vol. 47, no. 171, pp. 113–119, 2008.
46. K. Chandra, Burden and coping in caregivers of men with alcohol and
opioid dependence [MD dissertation], Postgraduate Institute of
Medical Education & Research, Chandigarh, India, 2004
47. Vaishnavi R, et al Journal of Addiction, vol 2017, Article ID 8934712,
http://doi.org\10.1155\2017\8934712
48. Srinivasagopalan., Nappinai. Solayappan(2015 march) A Comparative
Study of Caregiver Burden in Cancer Cervix and Breast cancer
illnesses., IJPS.
49. Mrs.Sapna Ganesh "Burden and Quality of Life among Care Givers of
Persons with Alcohol Dependence Syndrome - A Hospital based
Interventional Study.” IOSR Journal Of Humanities And Social
Science (IOSR-JHSS). vol. 22 no. 12, 2017, pp. 20-28.
50. Vishal shah, Behere P, Mishra KK, Sharma A, Kumar K. Psychiatriv
Morbidity among Spouses of Men with Alcohol Dependence. Int J
Recent Surg Med Sci 2017;3(1):10-14
51. Shekhawat BS, Jain S, Solanki HK. Caregiver burden on wives of
substance-dependent husbands and its correlates at a Tertiary Care
Centre in Northern India. Indian J Public Health 2017;61:274-7.
95
52. Swaroopachary RS, Kalasapati LK, Ivaturi SC, Reddy CM. Caregiver
burden in alcohol dependence syndrome in relation to the severity of
dependence. Arch Ment Health 2018;19:19-23.
53. George S: A comparative study of the quality of marital life among
alcohol dependents: unpublished dissertation; Bangalore
university.1986
54. Nagalakshmi S.V., Suman L.N.: Family interaction patterns in
alcoholic families; NIMHANS Journal.1995;13(1);47-52
55. Sabhaney, J: A study of family and social background of alcoholic
addicts, MD thesis, Bangalore University.1974
56. Rao T.S.S. and Kuruvilla K. : A study in the personality characteristics
of wives of alcoholics; Indian Journal of Psychiatry.1991;33(3),359-
365
57. Hill SY : Personality characteristics of sisters and spouses of male
alcoholics; Alcoholism: Clinical and Experimental Research. 1993
Aug;17(4):733-9.
58. Lewis M.G : Alcoholism and family case work: The Family.1937;18,
39-44
59. Idstad et al. BMC Public Health 2010, 10:516
http://www.biomedcentral.com/1471-2458/10/516
60. S. K. Mattoo, N. Nebhinani, B. N. Anil Kumar, D. Basu, and P.
Kulhara, “Family burden with substance dependence: a study from
96
India,” Indian Journal of Medical Research, vol. 137, no. 4, pp. 704–
711, 2013.
61. Fadden, G., Bebbington, P.,& Kuipers, L. (1987). Caring and its
burdens. British Journal of Psychiatry, 151, 660–667
62. Kuruvilla, K. (1993) Towards more rational and responsible patient
care. Indian Journal of Psychiatry, 35,71-72.
63. Moos R , Brennan P.L, Schutte K, Moos B.S: Spouses of Older Adults
With Late-Life Drinking Problems: Health, Family, and Social
Functioning; Journal of Studies on Alcohol and Drugs. 2010 July;
71(4): 506–514
64. O'Farrell TJ, Harrison RH, Schulmeister CA, Cutter HS: A Closeness
to Divorce Scale for wives of alcoholics; Drug and Alcohol
Dependence. 1981;7(4):319-24.
65. Marshal P : For better or for worse? The effects of alcohol use on
marital functioning; Clinical Psychology Review. 2003 December;
23(7): 959–997.
66. Jayaram G: 16PF Profile of wives of alcoholics; unpublished
dissertation,Bangalore university.1988
67. Moos R , Brennan P.L, Schutte K, Moos B.S: Spouses of Older Adults
With Late-Life Drinking Problems: Health, Family, and Social
Functioning; Journal of Studies on Alcohol and Drugs. 2010 July;
71(4): 506–514
97
68. Ino, A; Sugino, K. and Shmiura, M. (1994). The "addiction trends"
seen among the wives of alcoholics, Report 2, Arukom Kenkyuto
Yuhbutsu Ison, April, 29 (2), 121-138
69. Pai, S. & Kapur, R.L. (1981) The burden on the family of a psychiatric
patient: development of an interview schedule. British Journal of
Psychiatry, 138, 332-335
70. Hoenig, J. & Hamilton, M.W. (1966) The schizophrenic patient in the
community and his effect on the household. International Journal of
Social Psychiatry, 12,165-176
71. Oldridge, M., & Hughes, I. (1992). Psychological well-being in
families with a member suffering from schizophrenia. British Journal
of Psychiatry, 161, 249–251.
72. M. Kiran and M. Senthil, “Family burden among caregivers of patients
with epilepsy and alcohol dependence,” Global Journal for Research
Analysis, vol. 5, no. 3, pp. 296–300, 2016.
73. R. D. Lennox, J. A. Scott-Lennox, andH. D. Holder, “Substance abuse
and family illness: evidence from health care utilization and cost-offset
research,”The Journal of Mental Health Administration, vol. 19, no. 1,
pp. 83–95, 1992.
74. Devi C. G., Rajasekar, N. Kokilavani (2013). A Study to Assess the
Level of Stress and Coping Strategies among Wives of Alcoholics at

98
Selected Settings, Chennai, Tamil Nadu. International Journal of
Nursing Education and Research. 1(1), Page 12-14.
75. Rospenda R., & Doman, K (2001). Partner enabling of alcoholic:
Critical review and future directions. American Journal of family
Therapy, 29(4) 257 -270.
76. Nanjundaswamy, M,P.A. Sreedevi , H.M. Gangadharaiah. B.
Viswanath, V. Benegal (2016). A study to assess the stress, coping
strategies and domestic violence in wives of alcohol dependent
individuals, NIMHANS, Psychiatry, Bangalore, India. https://doi.org/
10.1016/S0924-9338(13)77350-4.
77. Rakesh R. Gandhi1, Mahesh A. Suthar1, Sutanaya Pal1 Ankit J.
Rathod2: Archives of Psychiatry and Psychotherapy, 2017; 4: 51–56
99
ANNEXURES
100
ANNEXURES
1. LIST OF ABBREVIATIONS
2. CONSENT FORM (ENGLISH)
3. CONSENT FORM (TAMIL)
4. SOCIO DEMOGRAPHIC QUESTIONNAIRE- PATIENT AND
CAREGIVER
5. SEMI STRUCTURED QUESTIONNAIRE– PATIENT AND
CAREGIVER
6. SAD Q ( Severity Of Alcohol Dependence Questionnaire)
7. GHQ-12 (General Health Questionnaire 12)
8. FBIS (Family Burden Interview Schedule)
9. ETHICAL COMMITTEE CLEARANCE CERTIFICATE
10. MASTER CHART

101
ABBREVATIONS
1 ADH Alcohol Dehydrogenase
2 ADS Alcohol Dependence Syndrome
3. ALDH Aldehyde Dehydrogenase
4. ASPD Antisocial Personality Disorder
5. ASSIST Alcohol, smoking and substance Involvement Screening Test.
6. ASTWA Addiction Screening Test for Wives of Alcohol Dependence Men
7. COGA Collaborative Study On The Genetics Of Alcoholism
8. DALY Disability Adjusted Life Years
9. DAS Dyadic Adjustment Scale
10. DSM Diagnostic and Statistical Manual
11. FAD Family Assessment Device
12. FBIS Family Burden Interview Schedule
13. FIS Family Interaction Scale
14. GHQ General Health Questionnaire
15. HED Heavy Episode Drinking
16. ICD10 International statistical Classification of Diseases
17. MDPQ Mobile Device Proficiency Questionnaire
18. MMPI Minnesota Multiphasic Personality Inventory
19. NCS Family Interaction Scale
20. NDDTC National Drug Dependence Treatment Centre
21. NESARC National Epidemiology Survey On Alcohol And Related Conditions
22. NIMHANS National Institute Of Mental Health And Neuro Sciences
23. NLEAS National Longitudinal Alcohol Epidemiology Survey
24. NSDUH National Survey On Drug Use And Health
25. 16 PQ 16 Personality Factor Questionnaire
26. SAD Q Severity Of Alcohol Dependence Questionnaire
27. SDS Social Drinking Scale
28. SPSS Statistical Package For Social Scientist Version
29. WHO World Health Organisation
102
Informed Consent:
Title: STUDY ON CAREGIVER BURDEN IN TREATMENT
SEEKING INVIDUALS WITH ALCOHOL USE DISORDERS
Principal Investigator
Dr. KARPAGALAKSHMI.R
Department of Psychiatry
Karpaga Vinayaga Institute of Medical Sciences & RC,
Madhuranthakam.
A structured questionnaire will be administered to get necessary
information for the study. The participation in the study will require
approximately 30 minutes of your valuable time and it does/ does not include
any invasive procedure. There are no risks involved in the study.
Participation in the study is completely voluntary and confidentiality will be
maintained. Your consent is required before you can participate in this study
and you have the right to refuse / withdraw from this study.
I have read this consent form and I fully understand the content of this
document and voluntarily consent to participate in the study. All of my
questions concerning this study have to be answered. If I have any questions
in the future about this study the investigator listed above will answer them. I
understand that this consent ends at the conclusion of this study. By signing
this form, I agree to participate in this study.
Date: Caregivers Name & Signature Participants Name &
Signature
CERTIFICATION OF INFORMED CONSENT
I certify that I have explained the nature and purpose of this study to the
above named individual and I have discussed the potential benefits of this
study participation. The questions, the individual had about this study have
been answered and we will always be available to address future questions.
Date: Signature of person obtaining consent
103
. . , .
ந
ந ந
ந ந
+91 9600441233
ந CAREGIVER BURDEN IN TREATMENT SEEKING INDIVIDUALS WITH ALCOHOL
USEDISORDERS
ந ந
. ந ந
. .
ந
.
ந
.
ந
ந :
:

104
SOCIO DEMOGRAPHIC QUESTIONNAIRE- PATIENT
Unique ID :
Age:
Sex:
Religion:
Education:
Residence: rural/urban
Family income\month:
No. of family members:
SOCIO DEMOGRAPHIC PROFILE OF CAREGIVERS
Unique ID :
Age:
Sex:
Relation to patient:
Religion:
Education:
Residence: rural/urban
Family income\month:
No. of family members:

105
SEMI STRUCTURED QUESTIONNAIRE FOR ALCOHOL USE
DISORDER PATIENTS
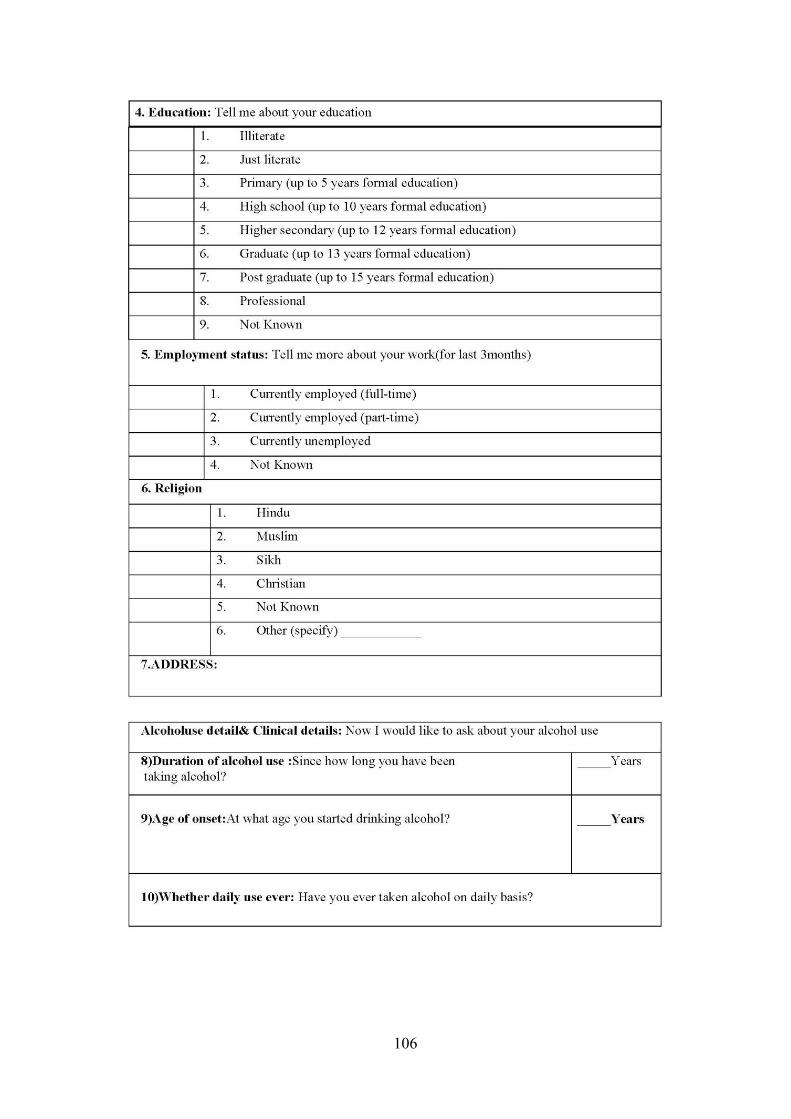
106
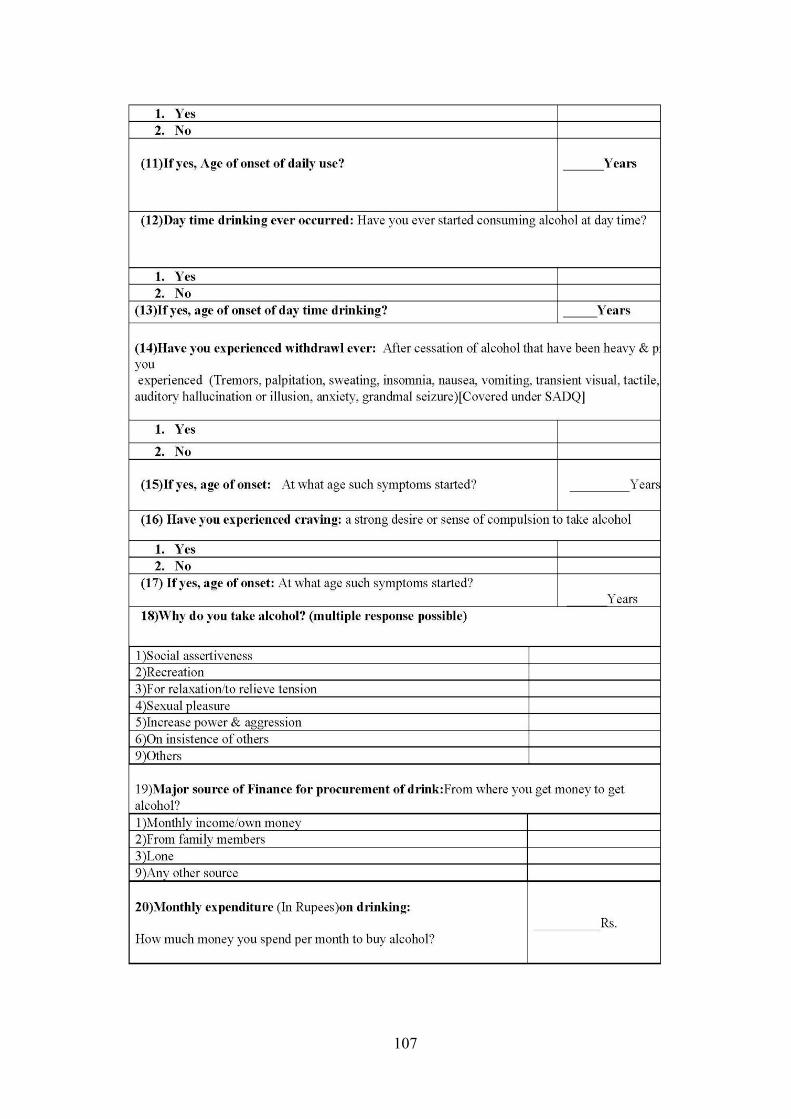
107

108
109
110
111

112
113
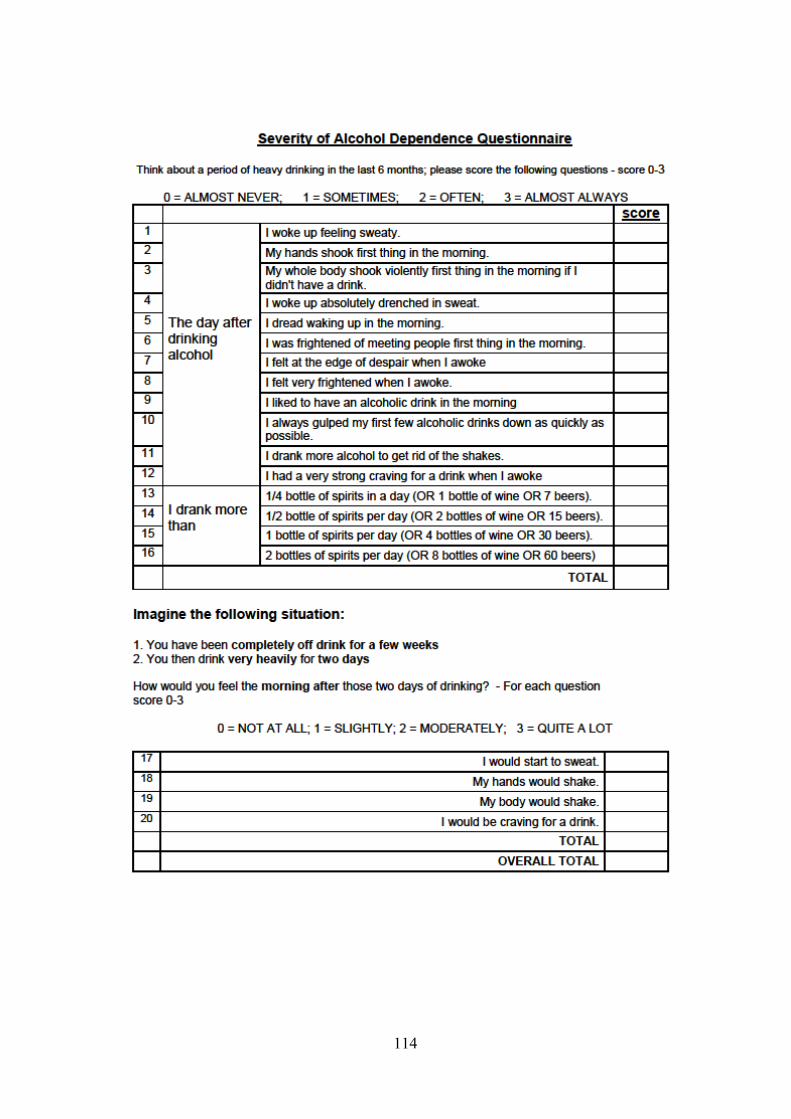
114
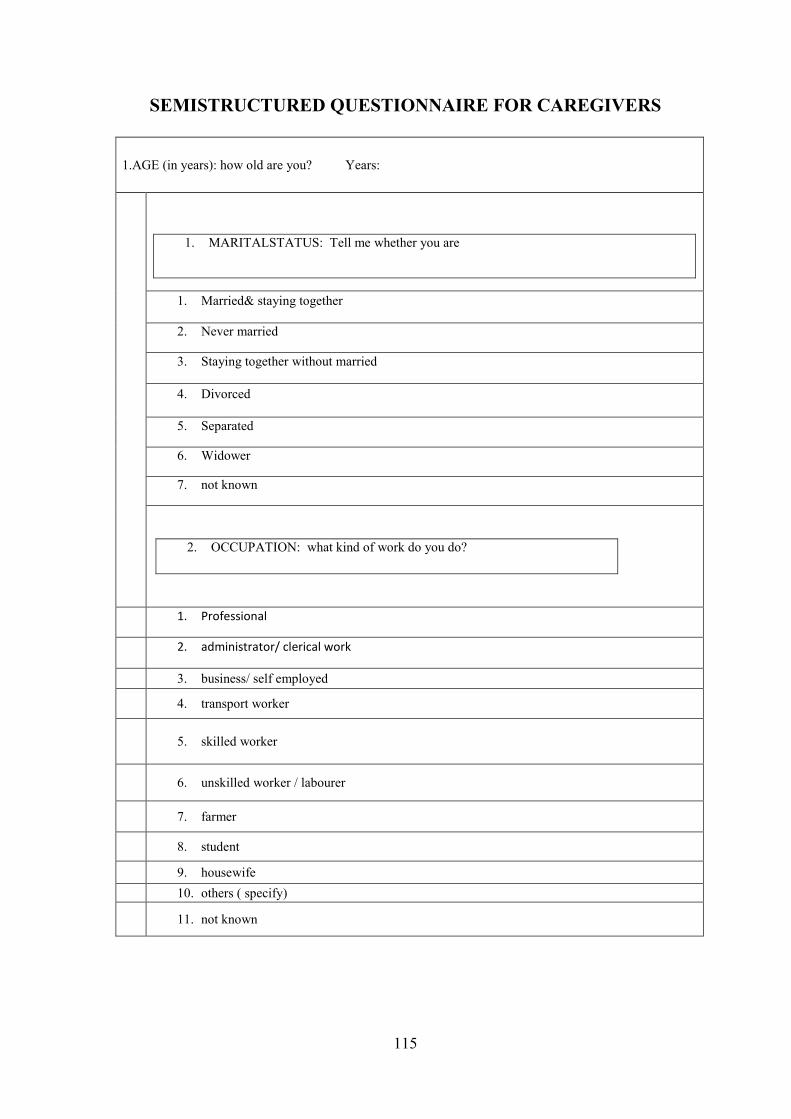
115
SEMISTRUCTURED QUESTIONNAIRE FOR CAREGIVERS
1.AGE (in years): how old are you? Years:
1. MARITALSTATUS: Tell me whether you are
1. Married& staying together
2. Never married
3. Staying together without married
4. Divorced
5. Separated
6. Widower
7. not known
2. OCCUPATION: what kind of work do you do?
1. Professional
2. administrator/ clerical work
3. business/ self employed
4. transport worker
5. skilled worker
6. unskilled worker / labourer
7. farmer
8. student
9. housewife
10. others ( specify)
11. not known
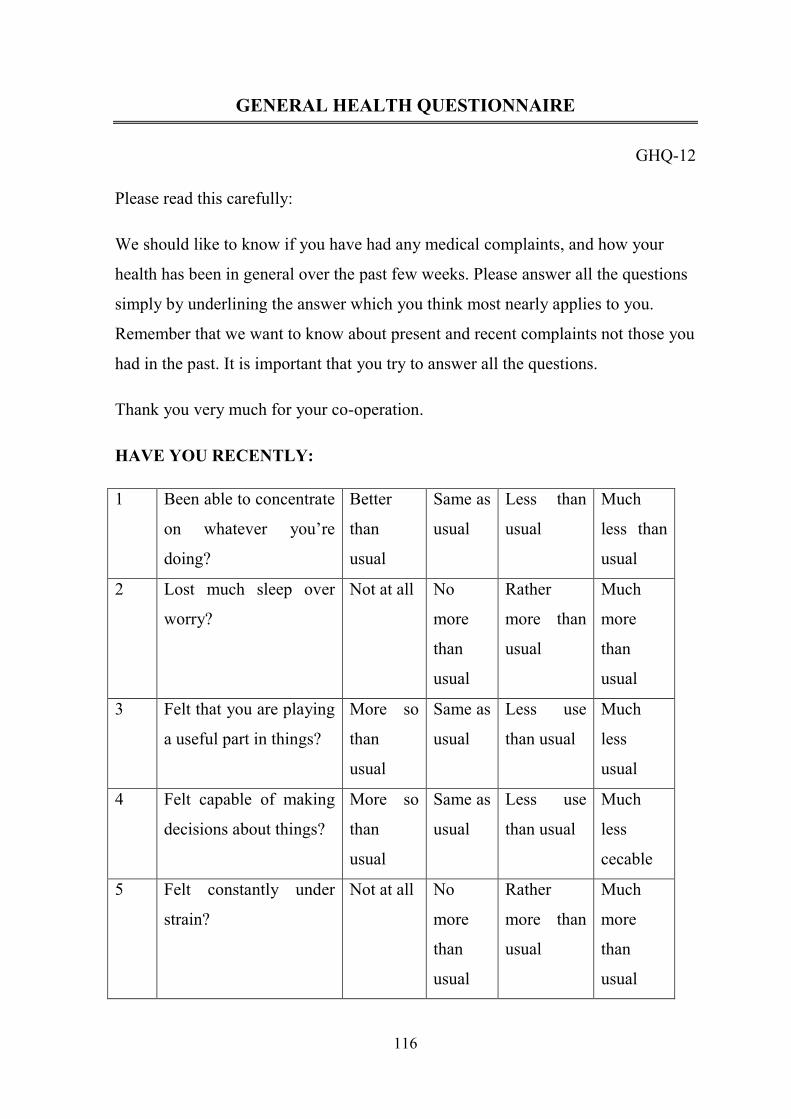
116
GENERAL HEALTH QUESTIONNAIRE
GHQ-12
Please read this carefully:
We should like to know if you have had any medical complaints, and how your
health has been in general over the past few weeks. Please answer all the questions
simply by underlining the answer which you think most nearly applies to you.
Remember that we want to know about present and recent complaints not those you
had in the past. It is important that you try to answer all the questions.
Thank you very much for your co-operation.
HAVE YOU RECENTLY:
1 Been able to concentrate
on whatever you’re
doing?
Better
than
usual
Same as
usual
Less than
usual
Much
less than
usual
2 Lost much sleep over
worry?
Not at all No
more
than
usual
Rather
more than
usual
Much
more
than
usual
3 Felt that you are playing
a useful part in things?
More so
than
usual
Same as
usual
Less use
than usual
Much
less
usual
4 Felt capable of making
decisions about things?
More so
than
usual
Same as
usual
Less use
than usual
Much
less
cecable
5 Felt constantly under
strain?
Not at all No
more
than
usual
Rather
more than
usual
Much
more
than
usual
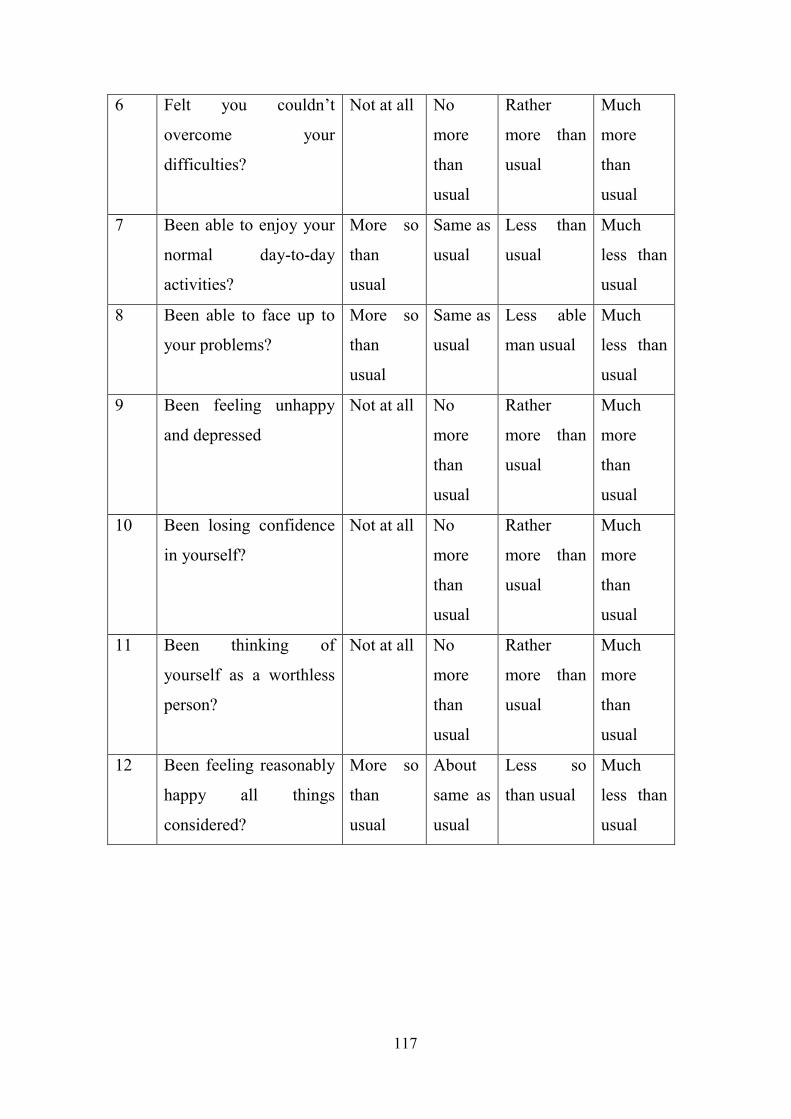
117
6 Felt you couldn’t
overcome your
difficulties?
Not at all No
more
than
usual
Rather
more than
usual
Much
more
than
usual
7 Been able to enjoy your
normal day-to-day
activities?
More so
than
usual
Same as
usual
Less than
usual
Much
less than
usual
8 Been able to face up to
your problems?
More so
than
usual
Same as
usual
Less able
man usual
Much
less than
usual
9 Been feeling unhappy
and depressed
Not at all No
more
than
usual
Rather
more than
usual
Much
more
than
usual
10 Been losing confidence
in yourself?
Not at all No
more
than
usual
Rather
more than
usual
Much
more
than
usual
11 Been thinking of
yourself as a worthless
person?
Not at all No
more
than
usual
Rather
more than
usual
Much
more
than
usual
12 Been feeling reasonably
happy all things
considered?
More so
than
usual
About
same as
usual
Less so
than usual
Much
less than
usual
118
FAMILY BURDEN INTERVIEW SCHEDULE
Instructions to relative: We are trying to assess the various difficulties felt by
the family of a psychiatric patient, and will ask you a few questions about these.
Please do not hesitate to express your true feelings.
Instructions to raters: Please interview the relative on the following
guidelines. You may probe further in order to assess a particular item if you feel it
necessary. During the interview note your rating for each general category, as well
as for each individual item, on a three-point scale, viz Severe burden -2, Moderate
burden-1, No burden-0
After completing the interview please assess the burden on the family as a
whole, and give the rating on a similar three-point scale.
A. Financial burden
1. Loss of patient's income: (Has he lost his job? Stopped doing the work
which he was doing before? To what extent does it affect the family
income?)
2. Loss of income of any other member of the family due to patient's illness:
(Has anybody stopped working in order to stay at home, lost pay, lost a job?
To what extent are the family finances affected?)
3. Expenditure incurred due to patient's illness and treatment:(Has he spent or
lost money irrationally due to his illness? How much has this affected the
family finances? How much has been spent on treatment, medicines,
transport, accommodation away from home and so on? How much has been
spent on other treatments such as temples and native healers? How has this
affected family finances?)

119
4. Expenditure incurred due to extra arrangements:(For instance, any other
relative coming to stay with the patient; appointing a nurse or servant;
boarding out children. How have these affected the family finances?)
5. Loans taken or savings spent: (How large a loan? How do they plan to pay it
back? How much does it affect the family? Did they spend from savings?
Were these used up? How much is the family affected?)
6. Any other planned activity put off because of the financial pressure of the
patient's illness: (For instance, postponing a marriage, a journey or a
religious rite. How far is the family affected?)
B. Disruption of routine family activities
1. Patient not going to work, school, college, etc: How inconvenient is this for
the family?
2. Patient not helping in the household work: How much does this affect the
family?
3. Disruption of activities of other members of the family: (Has someone to
spend time looking after the patient, thus abandoning another routine
activity? How inconvenient is this?)
4. Patient's behaviour disrupting activities: (Patient insisting on someone being
with him, not allowing that person to go out, etc? Patient becoming violent,
breaking things, not sleeping and not allowing others to sleep? How much
does it affect the family?)
5. Neglect of the rest of the family due to patient's illness: (Is any other
member missing school, meals, etc? How serious is this?)
C. Disruption of family leisure
1. Stopping of normal recreational activities: (Completely, partially, not at all?
How do the family members react?)
120
2. Patient's illness using up another person's holiday and leisure time: (How is
this person affected by it?)
3. Patient's lack of attention to other members of the family, such as children,
and its effect on them.
4. Has any other leisure activity had to be abandoned owing to the patient's
illness or incapacity e.g. a pleasure trip or family gathering? How do the
family members feel about it?
D. Disruption of family interaction
1. Any ill effect on the general atmosphere in the house: (Has it become dull,
quiet? Are there a lot of misunderstandings, etc? How do the family
members view this?)
2. Do other members get into argument over this (for instance over how the
patient should be treated, who should do the work, who is to blame, etc)?
How are they affected?
3. Have relatives and neighbours stopped visiting the family or reduced the
frequency of their visits because of the patient's behaviour or the stigma
attached to his illness? How does the family feel about this?
4. Has the family become secluded? Does it avoid mixing with others because
of shame or fear of being misunderstood? How do the members feel about
this?
5. Has the patient's illness had any other effect on relationships within the
family or between the family and neighbours or relative e.g. separation- of
spouses, quarrels between two families, property feuds, police intervention,
embarrassment for Family members,etc? How does the family feel about it?
121
E. Effect on physical health of others
1. Have any other members of the family suffered physical ill health, injuries,
etc due to the patient's behaviour? How has this affected them?
2. Has there been any other adverse effect on health (e.g. someone losing
weight or an existing illness being exacerbated)? How severe is it?
F. Effect on mental health of others
1. Has any other family member sought help for- psychological illness brought
on by the patient's behaviour (for instance by the patient's suicide bid, or his
disobedience, or worry about his future)? How severe is this?
2. Has any other member of the family lost sleep, become depressed or weepy,
expressed suicidal wishes, become excessively irritable, etc? How severely?
3. Finally, is there any other burden on the family about which we have not
asked you? If so, what is it? How badly does it affect you?
Subjective burden on the family:
This is to be assessed by asking the following standard question and scoring
the relative's answer: How much would you say you have suffered owing to the
patient's illness: severely, a little or not at all?

122
ETHICAL COMMITTEE CLEARANCE CERTIFICATE
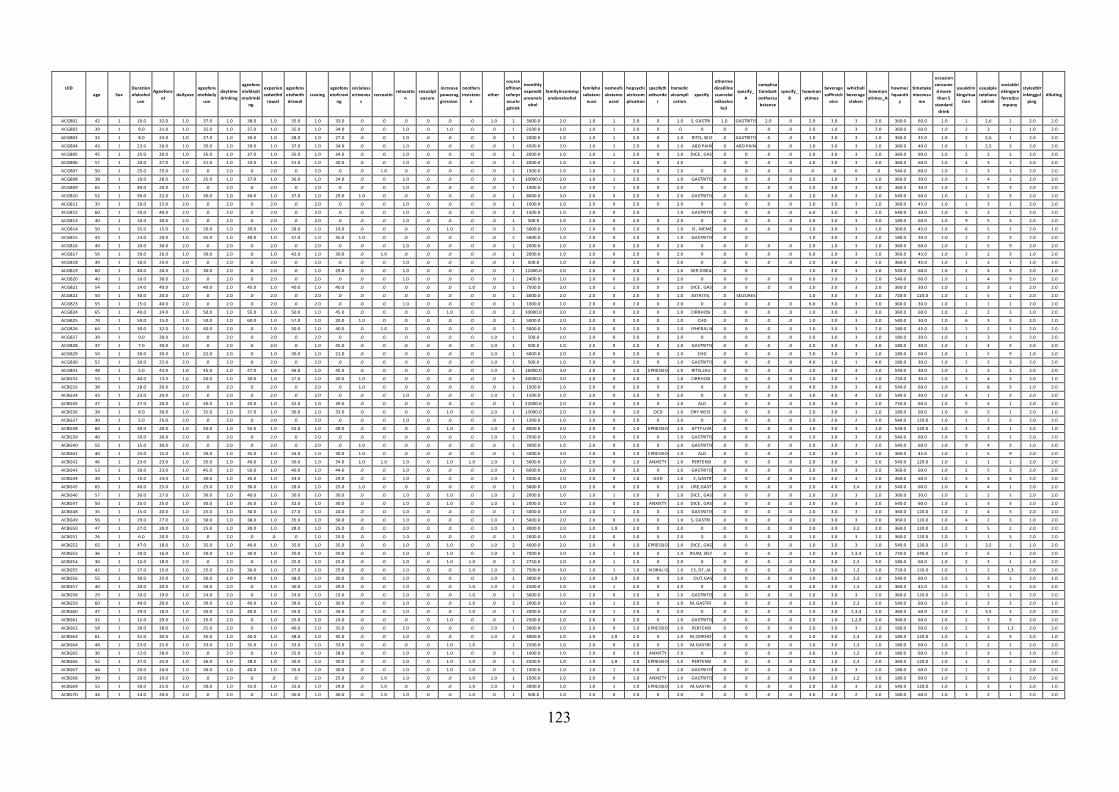
123
UID
age
Sex
Duration
ofalcohol
use
Ageofons
et
dailyuse
ageofons
etofdaily
use
daytime
drinking
ageofons
etofdayti
medrinki
ng
experien
cedwithd
rawal
ageofons
etofwith
drawal
craving
ageofons
etofcravi
ng
socialass
ertivenes
s
recreatin
relaxatio
n
sexualpl
easure
increase
powerag
gression
onothers
insistenc
e
other
source
offinan
ceforpr
ocurin
gdrink
monthly
expendit
ureonalc
ohol
familyincomesp
endonalcohol
familyho
substanc
euse
nameofs
ubstance
used
hopsychi
atriccom
plication
specifyth
edisorde
r
homedic
alcompli
cation
specify
otherme
dicalillne
ssunrelat
edtoalco
hol
specify_
A
complica
tionduet
oothersu
bstance
specify_
B
howman
ytimes
beverage
soffirstch
oice
whichall
beverage
staken
howman
ytimes_A
howmuc
hquantit
y
timetake
ntoconsu
me
occasion
consume
d more
than 5
standard
drink
usualdrin
kingsitua
tion
usualpla
cetohave
adrink
socialdri
nkingpre
ferredco
mpany
styleofdr
inkinggul
ping
diluting
ACGB01 42 1 10.0 32.0 1.0 37.0 1.0 38.0 1.0 35.0 1.0 33.0 .0 .0 .0 .0 .0 .0 1.0 1 3000.0 2.0 1.0 1 2.0 0 1.0
S, GASTRI
1.0 GASTRITIS 2.0 .0 2.0 3.0 3 2.0 360.0 60.0 1.0 1 2,6 1 2.0 2.0
ACGB02 39 1 8.0 31.0 1.0 35.0 1.0 37.0 1.0 35.0 1.0 34.0 .0 .0 1.0 .0 1.0 .0 .0 1 2500.0 1.0 1.0 1 2.0 0 .0
0
.0 0 .0 .0 2.0 1.0 3 2.0 360.0 60.0 1.0 2 3 1 1.0 2.0
ACGB03 32 1 8.0 24.0 1.0 27.0 1.0 30.0 1.0 28.0 1.0 27.0 .0 .0 1.0 .0 .0 .0 .0 1 2000.0 1.0 1.0 1 2.0 0 1.0
RITIS, SEIZ .0 GASTRITIS .0 .0 1.0 3.0 3 1.0 360.0 45.0 1.0 2 2,6 1 2.0 2.0
ACGB04 43 1 23.0 20.0 1.0 35.0 1.0 39.0 1.0 37.0 1.0 34.0 .0 .0 1.0 .0 .0 .0 .0 1 4500.0 2.0 1.0 1 2.0 0 1.0
ABD PAIN
.0 ABD PAIN .0 .0 1.0 3.0 3 1.0 360.0 40.0 1.0 1 2,5 3 2.0 2.0
ACGB05 45 1 25.0 20.0 1.0 35.0 1.0 37.0 1.0 35.0 1.0 34.0 .0 .0 1.0 .0 .0 .0 .0 1 2000.0 1.0 1.0 1 2.0 0 1.0
DICE , GAS
.0 0 .0 .0 2.0 3.0 3 2.0 360.0 90.0 1.0 2 2 1 2.0 2.0
ACGB06 57 1 20.0 27.0 1.0 31.0 1.0 33.0 1.0 31.0 1.0 30.0 .0 .0 1.0 .0 .0 .0 .0 1 2000.0 1.0 1.0 1 1.0 0 2.0
.0 0 .0 .0 2.0 3.0 3 3.0 360.0 60.0 1.0 4 3 1 2.0 2.0
ACGB07 50 1 25.0 25.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 1.0 .0 .0 .0 .0 .0 1 1500.0 1.0 1.0 1 2.0 0 2.0
0
.0 0 .0 .0 .0 .0 0 .0 540.0 60.0 1.0 2 3 1 2.0 2.0
ACGB08 38 1 10.0 28.0 1.0 35.0 1.0 37.0 1.0 36.0 1.0 34.0 .0 .0 1.0 .0 .0 .0 .0 1 10000.0 2.0 1.0 1 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 1.0 3 1.0 360.0 30.0 1.0 3 4 1 2.0 2.0
ACGB09 65 1 40.0 20.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 1000.0 1.0 1.0 1 2.0 0 2.0
0
.0 0 .0 .0 2.0 3.0 3 3.0 360.0 30.0 1.0 1 5 3 2.0 2.0
ACGB10 52 1 30.0 22.0 1.0 30.0 1.0 40.0 1.0 37.0 1.0 29.0 1.0 .0 .0 .0 .0 .0 .0 1 8000.0 3.0 2.0 0 2.0 0 2.0
GASTRITIS
.0 0 .0 .0 1.0 3.0 3 2.0 540.0 60.0 1.0 1 2 3 2.0 2.0
ACGB11 35 1 10.0 25.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 1000.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 3.0 3.0 3 1.0 360.0 45.0 1.0 1 3 1 2.0 2.0
ACGB12 60 1 20.0 40.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 2 1500.0 1.0 2.0 0 2.0
1.0
GASTRITIS
.0 0 .0 .0 6.0 3.0 3 2.0 540.0 30.0 1.0 5 3 1 2.0 2.0
ACGB13 40 1 10.0 30.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 500.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 2.0 3.0 3 3.0 180.0 60.0 1.0 9 5 3 2.0 2.0
ACGB14 50 1 35.0 15.0 1.0 20.0 1.0 30.0 1.0 28.0 1.0 19.0 .0 .0 .0 .0 1.0 .0 .0 3 5000.0 1.0 2.0 0 2.0 0 1.0
IS , MEMO
.0 0 .0 .0 1.0 3.0 3 1.0 360.0 45.0 1.0 6 5 1 2.0 1.0
ACGB15 43 1 23.0 20.0 1.0 35.0 1.0 40.0 1.0 37.0 1.0 35.0 1.0 .0 .0 .0 .0 .0 .0 2 5000.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0
1.0 3.0 3 2.0 180.0 30.0 1.0 2 2 3 2.0 2.0
ACGB16 40 1 10.0 30.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 2000.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 2.0 1.0 3 1.0 360.0 60.0 1.0 1 5 9 2.0 2.0
ACGB17 56 1 30.0 26.0 1.0 30.0 2.0 .0 1.0 42.0 1.0 30.0 .0 1.0 .0 .0 .0 .0 .0 1 2000.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 6.0 2.0 3 1.0 360.0 45.0 1.0 3 2 3 1.0 2.0
ACGB18 30 1 10.0 25.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 500.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 2.0 3.0 3 1.0 360.0 45.0 1.0 1 3 1 1.0 2.0
ACGB19 60 1 40.0 20.0 1.0 30.0 2.0 .0 2.0 .0 1.0 29.0 .0 .0 1.0 .0 .0 .0 .0 1 11000.0 2.0 2.0 0 2.0 0 1.0
VER DISEA
.0 0
1.0 3.0 3 1.0 540.0 60.0 1.0 2 4 3 2.0 1.0
ACGB20 40 1 10.0 30.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 2400.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 6.0 3.0 3 2.0 540.0 60.0 1.0 1 4 9 2.0 2.0
ACGB21 54 1 14.0 40.0 1.0 40.0 1.0 45.0 1.0 40.0 1.0 40.0 .0 .0 .0 .0 .0 1.0 .0 1 7500.0 2.0 1.0 1 2.0 0 1.0
DICE , GAS
.0 0 .0 .0 1.0 3.0 3 2.0 360.0 30.0 1.0 1 3 1 2.0 2.0
ACGB22 50 1 30.0 20.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 .0 .0 .0 .0 .0 1 4000.0 2.0 2.0 0 2.0 0 1.0
ASTRITIS,
.0 SEIZURES
1.0 3.0 3 2.0 720.0 120.0 1.0 1 5 1 2.0 2.0
ACGB23 55 1 15.0 40.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 1000.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 6.0 3.0 3 3.0 360.0 30.0 1.0 1 1 1 2.0 2.0
ACGB24 65 1 40.0 24.0 1.0 50.0 1.0 55.0 1.0 50.0 1.0 45.0 .0 .0 .0 .0 1.0 .0 .0 2 10000.0 3.0 2.0 0 2.0 0 1.0
CIRRHOSI
.0 0 .0 .0 1.0 3.0 3 3.0 360.0 60.0 1.0 2 2 3 1.0 2.0
ACGB25 70 1 50.0 15.0 1.0 50.0 1.0 60.0 1.0 57.0 1.0 20.0 1.0 .0 .0 .0 .0 .0 .0 2 5000.0 2.0 2.0 0 2.0 0 1.0
CHD
.0 0 .0 .0 1.0 3.0 3 2.0 540.0 30.0 1.0 6 3 3 2.0 1.0
ACGB26 64 1 30.0 32.0 1.0 40.0 2.0 .0 1.0 50.0 1.0 40.0 .0 1.0 .0 .0 .0 .0 .0 1 5000.0 1.0 2.0 0 2.0 0 1.0
IPHERAL N
.0 0 .0 .0 1.0 3.0 3 2.0 180.0 45.0 1.0 1 2 1 2.0 2.0
ACGB27 39 1 9.0 30.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 .0 .0 .0 .0 1.0 1 500.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 2.0 3.0 3 1.0 180.0 30.0 1.0 1 3 3 2.0 2.0
ACGB28 37 1 7.0 30.0 2.0 .0 2.0 .0 2.0 .0 1.0 45.0 .0 .0 .0 .0 .0 .0 1.0 1 500.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 3.0 3 4.0 180.0 30.0 1.0 1 4 3 2.0 2.0
ACGB29 50 1 30.0 20.0 1.0 22.0 2.0 .0 1.0 30.0 1.0 21.0 .0 .0 .0 .0 .0 .0 1.0 1 6000.0 2.0 2.0 0 2.0 0 1.0
CHD
.0 0 .0 .0 3.0 3.0 3 1.0 180.0 60.0 1.0 1 5 9 1.0 2.0
ACGB30 52 1 30.0 22.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 .0 .0 .0 .0 1.0 1 500.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 4.0 1.0 1 4.0 180.0 30.0 1.0 2 2 3 2.0 2.0
ACGB31 48 1 5.0 43.0 1.0 45.0 1.0 47.0 1.0 46.0 1.0 45.0 .0 .0 .0 .0 .0 .0 1.0 1 16000.0 3.0 2.0 0 1.0 EPRESSIO 1.0
RITIS,JAU
.0 0 .0 .0 1.0 3.0 3 1.0 540.0 30.0 1.0 1 3 1 2.0 2.0
ACBG32 53 1 40.0 13.0 1.0 20.0 1.0 30.0 1.0 27.0 1.0 20.0 1.0 .0 .0 .0 .0 .0 .0 3 20000.0 3.0 2.0 0 2.0 0 1.0
CIRRHOSI
.0 0 .0 .0 1.0 3.0 3 1.0 720.0 30.0 1.0 3 4 3 2.0 1.0
ACBG33 38 1 18.0 20.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 1.0 .0 .0 .0 .0 .0 .0 1 1500.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 4.0 3.0 3 4.0 540.0 60.0 1.0 1 8 3 1.0 2.0
ACBG34 43 1 23.0 20.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 1.0 1 1500.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 3.0 4.0 4 3.0 540.0 30.0 1.0 4 1 3 2.0 2.0
ACBG35 47 1 27.0 20.0 1.0 40.0 1.0 45.0 1.0 42.0 1.0 39.0 .0 .0 .0 .0 .0 .0 .0 1 22000.0 2.0 2.0 0 2.0 0 1.0
ALD
.0 0 .0 .0 2.0 3.0 3 2.0 720.0 60.0 1.0 5 4 1 2.0 2.0
ACBG36 38 1 8.0 30.0 1.0 35.0 1.0 37.0 1.0 36.0 1.0 33.0 .0 .0 .0 .0 1.0 .0 1.0 1 15000.0 2.0 2.0 0 1.0 OCD 1.0
ORY WEIS
.0 0 .0 .0 2.0 3.0 3 1.0 180.0 60.0 1.0 6 5 1 2.0 1.0
ACBG37 30 1 5.0 25.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 .0 1 1200.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 2.0 2.0 2 2.0 540.0 120.0 1.0 1 2 3 2.0 2.0
ACBG38 60 1 40.0 20.0 1.0 50.0 1.0 55.0 1.0 52.0 1.0 49.0 .0 .0 .0 .0 1.0 .0 1.0 2 8000.0 2.0 2.0 0 1.0 EPRESSIO 1.0
ATTY LIVE
.0 0 .0 .0 1.0 3.0 3 1.0 540.0 120.0 1.0 4 3 1 2.0 1.0
ACBG39 40 1 10.0 30.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 .0 .0 .0 .0 1.0 1 2500.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 3.0 3 2.0 540.0 60.0 1.0 5 2 1 2.0 2.0
ACBG40 55 1 15.0 30.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 1.0 .0 .0 .0 .0 .0 .0 1 3000.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 3.0 3 2.0 540.0 60.0 1.0 9 4 3 1.0 2.0
ACBG41 40 1 25.0 15.0 1.0 30.0 1.0 35.0 1.0 34.0 1.0 30.0 1.0 .0 .0 .0 .0 .0 .0 1 5000.0 3.0 2.0 0 1.0 EPRESSIO 1.0
ALD
.0 0 .0 .0 1.0 3.0 3 1.0 360.0 45.0 1.0 1 5 9 2.0 2.0
ACBG42 46 1 23.0 23.0 1.0 35.0 1.0 40.0 1.0 30.0 1.0 34.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1 5000.0 1.0 2.0 0 1.0 ANXIETY 1.0
PERTENSI .0 0 .0 .0 2.0 3.0 3 2.0 540.0 120.0 1.0 1 1 1 2.0 2.0
ACBG43 53 1 30.0 23.0 1.0 45.0 1.0 50.0 1.0 40.0 1.0 44.0 .0 .0 1.0 .0 .0 .0 1.0 1 6000.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 3.0 3 2.0 360.0 60.0 1.0 2 5 3 2.0 2.0
ACBG44 39 1 15.0 24.0 1.0 30.0 1.0 35.0 1.0 33.0 1.0 29.0 .0 .0 1.0 .0 .0 .0 1.0 1 5000.0 2.0 2.0 0 1.0 GAD 1.0
2, GASTR
.0 0 .0 .0 2.0 3.0 3 2.0 360.0 60.0 1.0 3 3 3 2.0 2.0
ACBG45 65 1 40.0 25.0 1.0 25.0 1.0 30.0 1.0 28.0 1.0 25.0 1.0 .0 .0 .0 .0 .0 .0 1 3000.0 1.0 2.0 0 2.0 0 1.0 URE,GAST
.0 0 .0 .0 2.0 4.0 3,4 2.0 540.0 60.0 1.0 4 4 1 2.0 2.0
ACBG46 57 1 30.0 27.0 1.0 30.0 1.0 40.0 1.0 30.0 1.0 30.0 .0 .0 1.0 .0 1.0 .0 1.0 2 2000.0 1.0 1.0 1 1.0 0 1.0
DICE , GAS
.0 0 .0 .0 2.0 3.0 3 2.0 360.0 30.0 1.0 2 2 1 2.0 2.0
ACBG47 50 1 25.0 25.0 1.0 30.0 1.0 35.0 1.0 32.0 1.0 30.0 .0 .0 1.0 .0 1.0 .0 1.0 1 2000.0 1.0 2.0 0 1.0 ANXIETY 1.0
DICE , GAS
.0 0 .0 .0 2.0 3.0 3 2.0 540.0 60.0 1.0 1 3 3 2.0 2.0
ACBG48 35 1 15.0 20.0 1.0 25.0 1.0 30.0 1.0 27.0 1.0 24.0 .0 .0 1.0 .0 .0 .0 .0 1 5000.0 1.0 1.0 1 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 3.0 3 2.0 360.0 120.0 1.0 2 4 3 2.0 2.0
ACBG49 56 1 29.0 27.0 1.0 30.0 1.0 38.0 1.0 35.0 1.0 30.0 .0 .0 1.0 .0 .0 .0 1.0 1 5000.0 2.0 2.0 0 2.0 0 1.0
S, GASTRI
.0 0 .0 .0 2.0 3.0 3 2.0 360.0 120.0 1.0 4 2 3 1.0 2.0
ACBG50 47 1 27.0 20.0 1.0 25.0 1.0 30.0 1.0 28.0 1.0 25.0 .0 .0 2.0 .0 .0 .0 1.0 1 3000.0 2.0 1.0 1,9 2.0 0 2.0
0
.0 0 .0 .0 2.0 3.0 3,2 2.0 360.0 120.0 1.0 2 5 1 2.0 2.0
ACBG51 26 1 6.0 20.0 2.0 .0 2.0 .0 .0 .0 1.0 25.0 .0 .0 1.0 .0 .0 .0 .0 1 2000.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 1.0 3.0 3 1.0 360.0 120.0 1.0 1 1 3 2.0 2.0
ACBG52 65 1 47.0 18.0 1.0 35.0 1.0 40.0 1.0 35.0 1.0 35.0 .0 .0 1.0 .0 1.0 .0 1.0 2 4000.0 2.0 2.0 0 1.0 EPRESSIO 1.0
DICE , GAS
.0 0 .0 .0 1.0 3.0 3 1.0 540.0 120.0 1.0 1 3,5 1 1.0 2.0
ACBG53 36 1 20.0 16.0 1.0 20.0 1.0 30.0 1.0 20.0 1.0 20.0 .0 .0 1.0 .0 1.0 .0 1.0 2 7000.0 2.0 1.0 1 2.0 0 1.0 RIUM, SEIZ .0 0 .0 .0 1.0 3.0 2,3,4 1.0 720.0 240.0 1.0 2 5 1 2.0 2.0
ACBG54 30 1 12.0 18.0 2.0 .0 2.0 .0 1.0 25.0 1.0 25.0 .0 .0 1.0 .0 1.0 1.0 .0 2 2750.0 2.0 1.0 1 2.0 0 2.0
0
.0 0 .0 .0 3.0 3.0 2,3 3.0 180.0 60.0 1.0 2 3 1 1.0 2.0
ACBG55 42 1 27.0 15.0 1.0 25.0 1.0 30.0 1.0 27.0 1.0 25.0 .0 .0 1.0 .0 .0 1.0 1.0 2 7500.0 3.0 1.0 1 1.0 VIORAL IS 1.0
ES, DT, JA
.0 0 .0 .0 1.0 3.0 1,3 1.0 720.0 120.0 1.0 1 2 1,3 2.0 2.0
ACBG56 55 1 30.0 25.0 1.0 30.0 1.0 40.0 1.0 38.0 1.0 30.0 .0 .0 1.0 .0 .0 .0 1.0 1 3000.0 1.0 1.0 1,9 2.0 0 1.0
OUT,GAS
.0 0 .0 .0 1.0 3.0 2,3 1.0 540.0 60.0 1.0 1 3 1 2.0 1.0
ACBG57 40 1 20.0 20.0 1.0 30.0 2.0 .0 1.0 30.0 1.0 29.0 .0 .0 1.0 .0 .0 1.0 1.0 1 2500.0 1.0 1.0 1 2.0 0 2.0
0
.0 0 .0 .0 2.0 3.0 1,3 2.0 360.0 45.0 1.0 1 3 1 2.0 2.0
ACBG58 29 1 10.0 19.0 1.0 24.0 2.0 .0 1.0 24.0 1.0 23.0 .0 .0 1.0 .0 .0 1.0 .0 1 3000.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 3.0 3 2.0 360.0 120.0 1.0 1 2 1 2.0 2.0
ACBG59 60 1 40.0 20.0 1.0 30.0 1.0 40.0 1.0 39.0 1.0 30.0 .0 .0 1.0 .0 .0 1.0 .0 2 2000.0 1.0 1.0 1 2.0 0 1.0
M, GASTRI .0 0 .0 .0 2.0 3.0 2,3 2.0 540.0 60.0 1.0 1 3 3 2.0 1.0
ACBG60 47 1 29.0 18.0 1.0 35.0 1.0 40.0 1.0 35.0 1.0 34.0 .0 .0 1.0 .0 .0 1.0 .0 1 2000.0 1.0 1.0 1 2.0 0 2.0
0
.0 0 .0 .0 2.0 3.0 2,3,4 2.0 360.0 60.0 1.0 2 3,5 3 2.0 2.0
ACBG61 32 1 12.0 20.0 1.0 25.0 2.0 .0 1.0 25.0 1.0 24.0 .0 .0 .0 .0 1.0 .0 .0 1 2500.0 1.0 2.0 0 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 1.0 1,2,9 2.0 360.0 60.0 1.0 2 3 3 2.0 2.0
ACBG62 58 1 30.0 28.0 1.0 35.0 2.0 .0 1.0 40.0 1.0 35.0 .0 .0 1.0 .0 .0 .0 1.0 1 3000.0 1.0 2.0 0 1.0 EPRESSIO 1.0
PERTENSI .0 0 .0 .0 2.0 3.0 3 2.0 180.0 60.0 1.0 2 3 1,3 2.0 2.0
ACBG63 61 1 31.0 30.0 1.0 35.0 1.0 40.0 1.0 38.0 1.0 35.0 .0 .0 1.0 .0 .0 .0 1.0 2 3000.0 1.0 1.0 1,9 2.0 0 1.0
M,CIRRHO
.0 0 .0 .0 2.0 3.0 2,3 2.0 180.0 120.0 1.0 1 2 3 2.0 1.0
ACBG64 48 1 23.0 25.0 1.0 33.0 1.0 35.0 1.0 33.0 1.0 33.0 .0 .0 .0 .0 1.0 1.0
1 2500.0 1.0 2.0 0 2.0 0 1.0
M,GASTRI
.0 0 .0 .0 1.0 3.0 1,3 1.0 180.0 60.0 1.0 1 2 1 2.0 2.0
ACBG65 30 1 12.0 28.0 2.0 .0 2.0 .0 1.0 25.0 1.0 28.0 .0 .0 1.0 .0 1.0 .0 .0 1 1000.0 1.0 2.0 0 1.0 ANXIETY 2.0
0
.0 0 .0 .0 3.0 1.0 1,2 3.0 180.0 60.0 1.0 2 3 1 1.0 2.0
ACBG66 52 1 27.0 25.0 1.0 36.0 1.0 38.0 1.0 30.0 1.0 30.0 .0 .0 1.0 .0 1.0 1.0 .0 1 2500.0 1.0 1.0 1,9 1.0 EPRESSIO 1.0
PERTENSI .0 0 .0 .0 2.0 1.0 2,3 2.0 360.0 120.0 1.0 1 2 3 2.0 2.0
ACBG67 44 1 20.0 24.0 1.0 30.0 1.0 40.0 1.0 35.0 1.0 30.0 .0 .0 1.0 .0 1.0 1.0 .0 1 1500.0 1.0 1.0 1 2.0 0 1.0
GASTRITIS
.0 0 .0 .0 2.0 3.0 3 2.0 180.0 60.0 1.0 1 3 1 2.0 2.0
ACBG68 39 1 20.0 19.0 2.0 .0 2.0 .0 .0 .0 1.0 25.0 .0 1.0 1.0 .0 .0 1.0 1.0 1 1500.0 1.0 2.0 0 1.0 ANXIETY 1.0
GASTRITIS
.0 0 .0 .0 3.0 2.0 1,2 3.0 180.0 60.0 1.0 2 3 1 2.0 2.0
ACBG69 55 1 30.0 25.0 1.0 30.0 1.0 35.0 1.0 32.0 1.0 29.0 .0 1.0 .0 .0 .0 1.0 1.0 1 3000.0 1.0 1.0 1 1.0 EPRESSIO 1.0
M,GASTRI
.0 0 .0 .0 2.0 3.0 3 2.0 540.0 120.0 1.0 1 3 1 2.0 1.0
ACBG70 34 1 14.0 20.0 2.0 .0 2.0 .0 1.0 30.0 1.0 30.0 .0 1.0 1.0 .0 .0 1.0 .0 1 500.0 1.0 2.0 0 2.0 0 2.0
0
.0 0 .0 .0 3.0 2.0 2 3.0 180.0 60.0 1.0 3 2 1 2.0 2.0

124
ACBG71 46 1 27.0 19.0 1.0 25.0 1.0 30.0 1.0 27.0 1.0 24.0 .0 .0 1.0 .0 .0 1.0 .0 1 4000.0 1.0 1.0 1 1.0 ANXIETY 1.0 GASTRITIS .0 0 .0 .0 2.0 3.0 3 2.0 360.0 60.0 1.0 1 2 1 2.0 2.0
ACBG72 50 1 30.0 20.0 2.0 .0 2.0 .0 1.0 30.0 1.0 30.0 .0 .0 1.0 .0 .0 .0 .0 1 1000.0 1.0 2.0 1 1.0 EPRESSIO 2.0 0 .0 0 .0 .0 2.0 3.0 3 2.0 360.0 120.0 1.0 1 2 1 2.0 2.0
ACBG73 47 1 29.0 18.0 1.0 35.0 1.0 37.0 1.0 35.0 1.0 34.0 .0 .0 1.0 .0 .0 1.0 .0 1 2000.0 1.0 1.0 1 2.0 0 2.0 0 .0 0 .0 .0 2.0 3.0 2,3,4 2.0 360.0 60.0 1.0 2 3,5 3 2.0 2.0
ACBG74 53 1 32.0 21.0 1.0 25.0 1.0 30.0 1.0 28.0 1.0 25.0 .0 .0 1.0 .0 .0 1.0 1.0 2 6000.0 2.0 1.0 1 1.0 RESSION, 1.0 ON,DM,M .0 0 .0 .0 2.0 3.0 3 2.0 540.0 120.0 1.0 2 2 1 2.0 2.0
ACBG75 60 1 40.0 20.0 1.0 35.0 1.0 40.0 1.0 38.0 1.0 35.0 .0 .0 .0 .0 .0 .0 1.0 2 5000.0 2.0 2.0 0 1.0 EPRESSIO 1.0 ENSION,S 1.0 GASTRITIS .0 .0 1.0 3.0 3 1.0 720.0 180.0 1.0 1 3 1 2.0 2.0
ACBG76 42 1 22.0 20.0 1.0 30.0 1.0 40.0 1.0 30.0 1.0 28.0 .0 1.0 1.0 .0 .0 .0 1.0 1 4000.0 1.0 2.0 0 1.0 T,ANXIET 1.0 URE,GAST .0 0 .0 .0 1.0 3.0 2,3,4 1.0 540.0 180.0 1.0 2 3 3 2.0 1.0
ACBG77 30 1 12.0 28.0 2.0 .0 2.0 .0 1.0 25.0 1.0 29.0 .0 .0 1.0 .0 1.0 .0 .0 1 1000.0 1.0 2.0 0 1.0 ANXIETY 2.0 0 .0 0 .0 .0 3.0 1.0 1,2 3.0 180.0 60.0 1.0 2 3 1 1.0 2.0
ACBG78 52 1 27.0 25.0 1.0 36.0 1.0 38.0 1.0 30.0 1.0 36.0 .0 .0 1.0 .0 1.0 1.0 .0 1 2500.0 1.0 1.0 1 1.0 EPRESSIO 1.0 PERTENSI .0 0 .0 .0 2.0 1.0 2,3 2.0 360.0 120.0 1.0 1 2 3 2.0 2.0
ACBG79 34 1 14.0 20.0 2.0 .0 2.0 .0 1.0 30.0 1.0 30.0 .0 1.0 1.0 .0 .0 1.0 .0 1 2000.0 1.0 2.0 0 2.0 0 2.0 0 .0 0 .0 .0 3.0 2.0 2 3.0 180.0 60.0 1.0 3 2 1 2.0 2.0
ACBG80 46 1 27.0 19.0 1.0 25.0 1.0 30.0 1.0 27.0 1.0 25.0 .0 .0 1.0 .0 .0 1.0 .0 1 4000.0 1.0 1.0 1 1.0 ANXIETY 1.0 GASTRITIS .0 0 .0 .0 2.0 3.0 3 2.0 360.0 60.0 1.0 1 2 1 2.0 2.0
ACBG81 20 1 9.0 11.0 1.0 15.0 1.0 17.0 1.0 16.0 1.0 15.0 .0 1.0 1.0 .0 .0 1.0 1.0 2 4000.0 2.0 1.0 1,9 1.0 ANXIETY 1.0 GASTRITIS .0 0 .0 .0 2.0 3.0 2,3 2.0 360.0 60.0 1.0 1,2 2,3,4,5 1,3 2.0 1.0
ACBG82 61 1 31.0 30.0 1.0 35.0 1.0 45.0 1.0 40.0 1.0 34.0 .0 .0 1.0 .0 .0 .0 1.0 2 3000.0 1.0 1.0 1,9 2.0 0 1.0 M,CIRRHO .0 0 .0 .0 2.0 3.0 2,3 2.0 180.0 120.0 1.0 1 2 3 2.0 1.0
ACBG83 55 1 30.0 25.0 1.0 30.0 1.0 35.0 1.0 30.0 1.0 29.0 .0 1.0 .0 .0 .0 1.0 1.0 1 3000.0 1.0 1.0 1 1.0 EPRESSIO 1.0 M,GASTRI .0 0 .0 .0 2.0 3.0 3 2.0 540.0 120.0 1.0 1 3 1 2.0 1.0
ACBG84 50 1 30.0 20.0 2.0 .0 2.0 .0 1.0 30.0 1.0 30.0 .0 .0 1.0 .0 .0 .0 .0 1 2500.0 1.0 2.0 1 1.0 EPRESSIO 2.0 0 .0 0 .0 .0 2.0 3.0 3 2.0 360.0 120.0 1.0 1 2 1 2.0 2.0
ACBG85 32 1 12.0 20.0 1.0 25.0 2.0 .0 1.0 25.0 1.0 24.0 .0 .0 .0 .0 1.0 .0 .0 1 2500.0 1.0 2.0 0 2.0 0 1.0 GASTRITIS .0 0 .0 .0 2.0 1.0 1,2,9 2.0 360.0 60.0 1.0 2 3 3 2.0 2.0
ACBG86 47 1 29.0 18.0 1.0 35.0 1.0 40.0 1.0 35.0 1.0 35.0 .0 .0 1.0 .0 .0 1.0 .0 1 2000.0 1.0 1.0 1 2.0 0 2.0 0 .0 0 .0 .0 2.0 3.0 2,3,4 2.0 360.0 60.0 1.0 2 3,5 3 2.0 2.0
ACBG87 46 1 27.0 19.0 1.0 25.0 1.0 30.0 1.0 29.0 1.0 25.0 .0 .0 1.0 .0 .0 1.0 .0 1 4000.0 1.0 1.0 1 1.0 ANXIETY 1.0 GASTRITIS .0 0 .0 .0 2.0 3.0 3 2.0 360.0 60.0 1.0 1 2 1 2.0 2.0
ACBG88 48 1 23.0 25.0 1.0 33.0 1.0 35.0 1.0 33.0 1.0 33.0 .0 .0 .0 .0 1.0 1.0
1 2500.0 1.0 2.0 0 2.0 0 1.0 M,GASTRI .0 0 .0 .0 1.0 3.0 1,3 1.0 180.0 60.0 1.0 1 2 1 2.0 2.0
ACBG89 47 1 29.0 18.0 1.0 35.0 1.0 40.0 1.0 35.0 1.0 35.0 .0 .0 1.0 .0 .0 1.0 .0 1 2000.0 1.0 1.0 1 2.0 0 2.0 0 .0 0 .0 .0 2.0 3.0 2,3,4 2.0 360.0 60.0 1.0 2 3,5 3 2.0 2.0
ACBG90 30 1 12.0 28.0 2.0 .0 2.0 .0 1.0 25.0 1.0 28.0 .0 .0 1.0 .0 1.0 .0 .0 1 1500.0 1.0 2.0 0 1.0 ANXIETY 2.0 0 .0 0 .0 .0 3.0 1.0 1,2 3.0 180.0 60.0 1.0 2 3 1 1.0 2.0
ACBG91 44 1 20.0 24.0 1.0 30.0 1.0 40.0 1.0 35.0 1.0 30.0 .0 .0 1.0 .0 1.0 1.0 .0 1 1500.0 1.0 1.0 1 2.0 0 1.0 GASTRITIS .0 0 .0 .0 2.0 3.0 3 2.0 180.0 60.0 1.0 1 3 1 2.0 2.0
ACBG92 32 1 8.0 24.0 1.0 24.0 1.0 30.0 1.0 28.0 1.0 24.0 .0 .0 1.0 .0 .0 .0 .0 1 2000.0 1.0 1.0 1 2.0 0 1.0 RITIS, SEIZ .0 0 .0 .0 1.0 3.0 3 1.0 360.0 45.0 1.0 2 2,6 1 2.0 2.0
ACBG93 55 1 34.0 21.0 1.0 29.0 1.0 31.0 1.0 28.0 1.0 29.0 .0 .0 .0 .0 .0 1.0 1.0 1,2 3000.0 1.0 2.0 0 2.0 0 1.0 RITIS,JAU 1.0 MI .0 .0 2.0 3.0 3 2.0 540.0 120.0 1.0 2 3 1,3 2.0 2.0
ACBG94 57 1 30.0 27.0 1.0 30.0 1.0 40.0 1.0 30.0 1.0 30.0 .0 .0 1.0 .0 1.0 .0 1.0 2 2000.0 1.0 1.0 1 1.0 ANXIETY 1.0 DICE , GAS .0 0 .0 .0 2.0 3.0 3 2.0 360.0 30.0 1.0 2 2 1 2.0 2.0
ACBG95 65 1 40.0 25.0 1.0 25.0 1.0 30.0 1.0 28.0 1.0 24.0 1.0 .0 .0 .0 .0 .0 .0 1 3000.0 1.0 2.0 0 2.0 0 1.0 URE,GAST .0 0 .0 .0 2.0 4.0 3,4 2.0 540.0 60.0 1.0 4 4 1 2.0 2.0
ACBG96 43 1 23.0 20.0 2.0 .0 2.0 .0 2.0 .0 2.0 .0 .0 .0 1.0 .0 .0 .0 1.0 1 1000.0 1.0 2.0 0 2.0 0 2.0 0 .0 0 .0 .0 3.0 4.0 4 3.0 540.0 30.0 1.0 4 1 3 2.0 2.0
ACBG97 57 1 30.0 27.0 1.0 30.0 1.0 41.0 1.0 30.0 1.0 30.0 .0 .0 1.0 .0 1.0 .0 1.0 1 2000.0 1.0 1.0 1 1.0 EPRESSIO 1.0 DICE , GAS .0 0 .0 .0 2.0 3.0 3 2.0 360.0 30.0 1.0 2 2 1 2.0 2.0
ACBG98 26 1 7.0 19.0 2.0 .0 2.0 .0 1.0 24.0 1.0 24.0 1.0 1.0 1.0 .0 .0 1.0 1.0 1 2000.0 1.0 1.0 1 1.0 PHOBIA 1.0 GASTRITIS .0 0 .0 .0 2.0 2.0 1,2,3 3.0 180.0 60.0 1.0 2 1,6,5 1,3,9 2.0 2.0
ACBG99 30 1 12.0 18.0 2.0 .0 2.0 .0 1.0 25.0 1.0 25.0 .0 .0 1.0 .0 1.0 1.0 .0 2 1500.0 1.0 1.0 1 2.0 0 2.0 0 .0 0 .0 .0 3.0 3.0 2,3 3.0 180.0 60.0 1.0 2 3 1 1.0 2.0
ACBG100 32 1 8.0 24.0 1.0 24.0 1.0 30.0 1.0 28.0 1.0 24.0 .0 .0 1.0 .0 .0 .0 .0 1 3000.0 2.0 1.0 1 2.0 0 1.0 RITIS, SEIZ .0 GASTRITIS .0 .0 1.0 3.0 3 1.0 360.0 45.0 1.0 2 2,6 1 2.0 2.0
125
UID
alongwit
hfood
moretha
n1bevera
geinsingl
eoccasio
n
usualtim
eofdrinki
ng
drinkwh
enhappy
drinkwh
enfrustra
ted
drinkwh
enrelaxe
d
drinkwh
entired
drinkwh
enbored
drinkwh
enmeetfr
iends
drinkona
baddayin
work
quarrelw
ith
nopartic
ularsitua
tion
anyfamil
ymembe
rsconsu
mealcoh
ol
knownpe
oplecons
umealco
hol
restrictio
nsagains
tdrinking
drinkingl
eadingto
intoxicati
on
feelafter
drinking
SADQoveralltotal
nameofc
aregivers
age2
sex_A
relationt
opatient
religion_
A
educatio
n_A
residenc
e_A
familyincome
nooffami
lymembe
rs
maritalst
atus_A
occupati
on_A
GHQ1
GHQ2
GHQ3
GHQ4
GHQ5
GHQ6
GHQ7
GHQ8
GHQ9
GHQ10
GHQ11
GHQ12
GHQTOT
AL
FINANCI
AL1
ACGB01 2.0 2.0 3 .0 1.0 1.0 .0 1.0 1.0 .0 1.0 .0 3.0 2,3 1.0 1.0 1.0 19.0 handraka 32.0 2.0 1 1.0 5.0 1.0 7000.0 5.0 1.0 9.0 1.0 2.0 1.0 2.0 2.0 2.0 2.0 1.0 3.0 1.0 1.0 1.0 19.0 1.0
ACGB02 1.0 2.0 3,4 .0 .0 .0 1.0 .0 1.0 .0 1.0 .0 3.0 3 1.0 3.0 3.0 16.0 MALA 35.0 2.0 1 1.0 5.0 1.0 20000.0 6.0 1.0 9.0 1.0 .0 2.0 1.0 2.0 2.0 1.0 1.0 2.0 2.0 1.0 2.0 17.0 .0
ACGB03 2.0 2.0 3 .0 1.0 .0 1.0 .0 .0 .0 .0 .0 2.0 2 1.0 2.0 1.0 14.0 SAROJA 48.0 2.0 2 1.0 3.0 1.0 10000.0 5.0 6.0 6.0 1.0 2.0 1.0 1.0 2.0 1.0 1.0 2.0 2.0 1.0 2.0 1.0 17.0 .0
ACGB04 1.0 1.0 3 .0 .0 1.0 1.0 .0 .0 .0 .0 .0 2.0 3 1.0 1.0 1.0 16.0 MALATHI 39.0 2.0 1 1.0 3.0 1.0 20000.0 4.0 1.0 6.0 1.0 2.0 1.0 1.0 3.0 1.0 3.0 2.0 2.0 1.0 1.0 1.0 19.0 .0
ACGB05 1.0 2.0 3 1.0 1.0 .0 .0 .0 .0 1.0 1.0 .0 2.0 2 1.0 2.0 3.0 11.0 MANJULA 40.0 2.0 1 1.0 3.0 1.0 15000.0 4.0 1.0 9.0 2.0 2.0 1.0 2.0 2.0 1.0 1.0 1.0 1.0 1.0 2.0 2.0 18.0 .0
ACGB06 1.0 2.0 3 .0 1.0 .0 .0 .0 .0 1.0 1.0 .0 2.0 3 1.0 2.0 2.0 15.0 VALLI 45.0 2.0 1 1.0 3.0 1.0 20000.0 5.0 1.0 6.0 1.0 2.0 1.0 1.0 2.0 1.0 1.0 1.0 3.0 2.0 3.0 2.0 20.0 .0
ACGB07 2.0 2.0 3 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 .0 2.0 1,3 1.0 1.0 4.0 12.0 VIJAYA 46.0 2.0 1 1.0 3.0 1.0 25000.0 6.0 1.0 9.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 .0 .0 .0 .0 .0 6.0 .0
ACGB08 1.0 2.0 4 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 .0 3.0 1 1.0 2.0 3.0 20.0 SUDHA 34.0 2.0 1 1.0 3.0 1.0 20000.0 5.0 1.0 9.0 1.0 2.0 2.0 2.0 2.0 1.0 1.0 2.0 2.0 1.0 1.0 2.0 19.0 1.0
ACGB09 2.0 1.0 3 .0 1.0 1.0 1.0 .0 1.0 1.0 0 .0 2.0 3 1.0 2.0 3.0 11.0 SASI 60.0 2.0 1 1.0 3.0 1.0 20000.0 5.0 1.0 9.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 12.0 2.0
ACGB10 1.0 2.0 4 .0 1.0 .0 1.0 .0 .0 .0 .0 .0 1.0 1,3 1.0 1.0 3.0 21.0 SUMATHI 49.0 2.0 1 1.0 5.0 2.0 10000.0 4.0 1.0 9.0 2.0 3.0 1.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 1.0 1.0 20.0 .0
ACGB11 2.0 2.0 3 .0 1.0 .0 .0 .0 1.0 1.0 1.0 1.0 1.0 1 1.0 2.0 3.0 14.0 LALITHA 30.0 2.0 1 1.0 5.0 2.0 50000.0 4.0 1.0 9.0 2.0 1.0 2.0 1.0 1.0 1.0 1.0 2.0 1.0 2.0 1.0 2.0 17.0 1.0
ACGB12 3.0 2.0 3 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1,3 2.0 2.0 4.0 12.0 RATHNA 57.0 2.0 1 4.0 4.0 1.0 8000.0 6.0 1.0 9.0 1.0 1.0 .0 .0 .0 .0 .0 .0 2.0 2.0 1.0 2.0 9.0 1.0
ACGB13 1.0 1.0 3 .0 1.0 .0 .0 .0 .0 1.0 .0 1.0 1.0 1 1.0 1.0 1.0 5.0 AGALAKSH 38.0 2.0 1 1.0 4.0 1.0 40000.0 4.0 1.0 9.0 .0 .0 .0 .0 .0 .0 1.0 1.0 .0 .0 .0 1.0 3.0 .0
ACGB14 2.0 2.0 3 .0 1.0 .0 .0 1.0 .0 1.0 .0 .0 1.0 1,3 1.0 1.0 3.0 20.0 KALYANI 47.0 2.0 1 1.0 4.0 2.0 40000.0 3.0 1.0 9.0 1.0 3.0 1.0 1.0 3.0 1.0 1.0 1.0 3.0 1.0 1.0 1.0 18.0 .0
ACGB15 1.0 2.0 3 .0 1.0 .0 1.0 1.0 .0 1.0 .0 .0 1.0 1 1.0 1.0 1.0 16.0 ABIRAMI 40.0 2.0 1 1.0 4.0 2.0 30000.0 3.0 1.0 9.0 2.0 2.0 1.0 1.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 2.0 21.0 .0
ACGB16 2.0 2.0 4 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 1.0 1.0 1 1.0 1.0 4.0 13.0 SHANTHI 38.0 2.0 1 1.0 4.0 2.0 10000.0 3.0 1.0 3.0 .0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 1.0 3.0 1.0 9.0 .0
ACGB17 3.0 2.0 3 .0 .0 1.0 .0 1.0 .0 1.0 1.0 .0 1.0 3 1.0 3.0 4.0 21.0 PARVATH 50.0 2.0 1 1.0 4.0 1.0 10000.0 4.0 1.0 6.0 1.0 3.0 2.0 2.0 3.0 2.0 2.0 1.0 2.0 2.0 1.0 1.0 22.0 .0
ACGB18 1.0 1.0 3 .0 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 1.0 1,3 2.0 1.0 1.0 15.0 ROOPA 27.0 2.0 1 4.0 4.0 2.0 70000.0 4.0 1.0 2.0 2.0 2.0 1.0 1.0 2.0 3.0 1.0 1.0 2.0 1.0 1.0 1.0 18.0 1.0
ACGB19 2.0 2.0 1 .0 .0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1 1.0 2.0 1.0 17.0 SAVITHRI 54.0 2.0 1 1.0 3.0 1.0 40000.0 4.0 1.0 9.0 2.0 2.0 1.0 2.0 2.0 1.0 2.0 1.0 2.0 1.0 1.0 1.0 18.0 .0
ACGB20 3.0 2.0 3 .0 .0 1.0 .0 .0 1.0 .0 .0 .0 1.0 1 1.0 2.0 1.0 14.0 RANJITHA 46.0 2.0 1 1.0 4.0 1.0 50000.0 3.0 1.0 9.0 1.0 .0 1.0 .0 1.0 .0 1.0 .0 2.0 2.0 1.0 2.0 11.0 .0
ACGB21 1.0 2.0 3 .0 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 2.0 1 1.0 3.0 1.0 22.0 RANI 49.0 2.0 1 1.0 4.0 1.0 25000.0 4.0 1.0 9.0 2.0 3.0 1.0 1.0 2.0 3.0 1.0 2.0 3.0 1.0 1.0 1.0 21.0 1.0
ACGB22 1.0 2.0 3 .0 1.0 1.0 .0 .0 1.0 1.0 1.0 .0 1.0 1,3 1.0 1.0 3.0 19.0 RAJA 26.0 1.0 5 1.0 6.0 1.0 15000.0 3.0 2.0 5.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 3.0 1.0 14.0 .0
ACGB23 2.0 2.0 3 1.0 .0 .0 .0 .0 1.0 1.0 .0 1.0 1.0 1 1.0 1.0 1.0 17.0 JANAKI 50.0 2.0 1 1.0 3.0 1.0 30000.0 4.0 1.0 6.0 1.0 2.0 1.0 2.0 2.0 1.0 2.0 1.0 2.0 2.0 1.0 2.0 19.0 2.0
ACGB24 2.0 2.0 3 .0 .0 .0 1.0 1.0 1.0 1.0 .0 .0 1.0 1 1.0 1.0 3.0 19.0 PARIMALA 33.0 2.0 3 1.0 5.0 1.0 7000.0 6.0 1.0 9.0 2.0 2.0 1.0 1.0 2.0 1.0 1.0 1.0 2.0 1.0 2.0 2.0 18.0 .0
ACGB25 2.0 2.0 3 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 .0 1.0 1 1.0 2.0 4.0 32.0 PAZHANI 40.0 1.0 5 1.0 5.0 1.0 10000.0 5.0 1.0 5.0 1.0 2.0 1.0 1.0 3.0 2.0 2.0 2.0 3.0 2.0 2.0 3.0 24.0 1.0
ACGB26 4.0 2.0 3 .0 1.0 .0 .0 1.0 .0 1.0 .0 1.0 1.0 1,3 1.0 3.0 1.0 13.0 PONNI 34.0 1.0 3 1.0 5.0 1.0 12000.0 3.0 1.0 9.0 1.0 3.0 .0 1.0 2.0 2.0 2.0 2.0 1.0 3.0 3.0 2.0 22.0 .0
ACGB27 3.0 2.0 3 .0 1.0 1.0 .0 1.0 1.0 1.0 .0 .0 1.0 1 1.0 3.0 1.0 8.0 MYTHILI 31.0 2.0 1 1.0 4.0 1.0 42000.0 3.0 1.0 9.0 .0 .0 .0 .0 .0 .0 .0 .0 .0 1.0 1.0 2.0 4.0 .0
ACGB28 2.0 2.0 3 1.0 1.0 .0 .0 1.0 1.0 1.0 1.0 .0 1.0 1,3 1.0 3.0 1.0 4.0 SARALA 35.0 2.0 1 1.0 5.0 1.0 30000.0 3.0 1.0 9.0 1.0 .0 .0 .0 .0 1.0 .0 .0 1.0 1.0 1.0 2.0 7.0 .0
ACGB29 1.0 2.0 3 .0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 1.0 1,3 1.0 2.0 4.0 19.0 GIRIJA 45.0 2.0 1 1.0 4.0 1.0 10000.0 5.0 1.0 9.0 1.0 3.0 2.0 1.0 3.0 2.0 2.0 2.0 3.0 1.0 1.0 2.0 23.0 .0
ACGB30 1.0 2.0 3 1.0 1.0 .0 1.0 .0 .0 .0 .0 .0 1.0 3 2.0 3.0 3.0 8.0 GOWRI 49.0 2.0 1 1.0 5.0 2.0 20000.0 4.0 1.0 9.0 2.0 1.0 .0 1.0 .0 .0 .0 1.0 1.0 .0 1.0 .0 7.0 .0
ACGB31 2.0 2.0 4 .0 .0 .0 .0 1.0 1.0 1.0 1.0 1.0 1.0 2 2.0 1.0 1.0 32.0 LATHA 26.0 2.0 3 1.0 4.0 2.0 30000.0 3.0 1.0 5.0 3.0 3.0 3.0 3.0 3.0 3.0 3.0 2.0 3.0 3.0 2.0 1.0 32.0 1.0
ACBG32 2.0 2.0 5 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2 2.0 1.0 4.0 36.0 PADMA 46.0 2.0 1 1.0 5.0 1.0 10000.0 4.0 1.0 9.0 2.0 2.0 2.0 1.0 3.0 3.0 3.0 3.0 3.0 1.0 1.0 2.0 26.0 1.0
ACBG33 2.0 2.0 3 1.0 1.0 .0 .0 .0 .0 1.0 1.0 .0 1.0 2 2.0 3.0 1.0 14.0 DHANAM 30.0 2.0 1 1.0 4.0 1.0 30000.0 5.0 1.0 9.0 1.0 1.0 1.0 1.0 1.0 2.0 3.0 1.0 1.0 2.0 1.0 2.0 17.0 1.0
ACBG34 2.0 1.0 4 .0 .0 .0 .0 .0 .0 .0 .0 .0 1.0 3 1.0 2.0 3.0 16.0 VAIDEKI 40.0 2.0 1 1.0 5.0 1.0 50000.0 4.0 1.0 5.0 2.0 2.0 2.0 1.0 2.0 2.0 3.0 2.0 1.0 1.0 1.0 2.0 21.0 1.0
ACBG35 2.0 1.0 5 .0 1.0 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 1 1.0 2.0 1.0 32.0 ANALAKS 42.0 2.0 1 1.0 5.0 1.0 75000.0 4.0 1.0 9.0 2.0 3.0 2.0 3.0 3.0 2.0 3.0 3.0 3.0 2.0 1.0 2.0 29.0 1.0
ACBG36 1.0 1.0 5 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2 1.0 1.0 1.0 11.0 NISHA 30.0 2.0 1 1.0 4.0 1.0 45000.0 6.0 1.0 9.0 2.0 2.0 2.0 1.0 2.0 1.0 1.0 2.0 1.0 2.0 2.0 2.0 20.0 1.0
ACBG37 2.0 1.0 3 1.0 1.0 .0 .0 .0 1.0 .0 .0 .0 1.0 3 1.0 1.0 2.0 20.0 SWARNAM 21.0 2.0 1 1.0 5.0 2.0 50000.0 2.0 1.0 5.0 1.0 1.0 1.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 19.0 1.0
ACBG38 2.0 1.0 5 .0 .0 .0 .0 .0 .0 .0 .0 1.0 1.0 9 2.0 2.0 1.0 18.0 CHITRA 35.0 2.0 3 1.0 5.0 1.0 15000.0 6.0 6.0 5.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 3.0 2.0 1.0 1.0 22.0 1.0
ACBG39 2.0 2.0 3 .0 1.0 .0 .0 .0 .0 .0 1.0 .0 1.0 3 2.0 3.0 2.0 21.0 LAKSHMI 34.0 2.0 1 1.0 4.0 1.0 20000.0 3.0 1.0 5.0 2.0 2.0 2.0 1.0 2.0 2.0 3.0 2.0 1.0 1.0 1.0 2.0 21.0 1.0
ACBG40 2.0 2.0 3 .0 1.0 .0 1.0 .0 .0 1.0 1.0 .0 1.0 2 1.0 3.0 2.0 23.0 VAIJENTH 51.0 2.0 1 1.0 4.0 2.0 40000.0 5.0 1.0 9.0 2.0 2.0 1.0 2.0 2.0 1.0 2.0 3.0 3.0 3.0 2.0 1.0 24.0 2.0
ACBG41 3.0 1.0 5 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1 2.0 2.0 1.0 24.0 PANDIYAN 68.0 1.0 4 1.0 3.0 1.0 8000.0 3.0 2.0 9.0 1.0 3.0 1.0 1.0 3.0 2.0 1.0 2.0 3.0 1.0 1.0 1.0 20.0 .0
ACBG42 2.0 2.0 3 .0 1.0 .0 .0 .0 1.0 .0 .0 .0 1.0 1,3 1.0 2.0 4.0 32.0 ANURADH 41.0 2.0 1 1.0 4.0 2.0 30000.0 4.0 1.0 5.0 2.0 3.0 2.0 3.0 3.0 2.0 2.0 3.0 3.0 3.0 2.0 1.0 29.0 1.0
ACBG43 1.0 2.0 3 1.0 1.0 1.0 .0 1.0 1.0 .0 .0 .0 1.0 3 2.0 3.0 4.0 16.0 ARAGATH 50.0 2.0 1 4.0 5.0 1.0 52000.0 4.0 1.0 9.0 2.0 3.0 2.0 1.0 3.0 2.0 3.0 2.0 3.0 1.0 1.0 2.0 25.0 1.0
ACBG44 2.0 2.0 4 .0 1.0 .0 .0 1.0 .0 .0 1.0 .0 1.0 2 1.0 2.0 3.0 11.0 ALAVATH 34.0 2.0 1 1.0 5.0 2.0 15000.0 3.0 1.0 9.0 1.0 2.0 1.0 1.0 2.0 1.0 1.0 3.0 3.0 1.0 3.0 1.0 19.0 .0
ACBG45 1.0 2.0 3 .0 1.0 1.0 .0 .0 1.0 1.0 1.0 .0 1.0 3 1.0 1.0 4.0 14.0 JAMUNA 29.0 2.0 3 1.0 4.0 1.0 20000.0 5.0 6.0 9.0 1.0 2.0 .0 1.0 2.0 1.0 2.0 3.0 1.0 3.0 3.0 1.0 20.0 .0
ACBG46 2.0 2.0 4 .0 .0 1.0 1.0 1.0 .0 .0 .0 .0 3.0 1,3 1.0 2.0 3.0 17.0 BALU 31.0 1.0 5 1.0 5.0 1.0 20000.0 6.0 6.0 5.0 2.0 2.0 1.0 2.0 2.0 1.0 2.0 2.0 3.0 1.0 1.0 1.0 20.0 .0
ACBG47 2.0 2.0 3 1.0 .0 .0 1.0 .0 1.0 .0 .0 .0 1.0 1 1.0 1.0 4.0 12.0 VIVEK 28.0 1.0 5 1.0 4.0 1.0 30000.0 2.0 5.0 5.0 1.0 2.0 1.0 2.0 3.0 2.0 3.0 2.0 2.0 1.0 3.0 2.0 24.0 1.0
ACBG48 2.0 2.0 3 .0 1.0 .0 1.0 .0 .0 1.0 .0 .0 3.0 1,3 1.0 3.0 3.0 18.0 ARCHANA 31.0 2.0 1 1.0 4.0 1.0 25000.0 4.0 1.0 5.0 2.0 2.0 1.0 1.0 3.0 2.0 2.0 2.0 3.0 1.0 1.0 1.0 21.0 .0
ACBG49 1.0 2.0 3 1.0 1.0 1.0 .0 .0 1.0 1.0 .0 .0 3.0 1,3 1.0 2.0 4.0 19.0 SEETHA 48.0 2.0 1 1.0 5.0 1.0 15000.0 3.0 1.0 9.0 1.0 3.0 1.0 2.0 3.0 1.0 1.0 2.0 3.0 1.0 1.0 2.0 21.0 .0
ACBG50 2.0 2.0 3 .0 1.0 .0 .0 .0 .0 .0 .0 .0 2.0 3 1.0 2.0 3.0 23.0 JAYASREE 43.0 2.0 1 1.0 4.0 1.0 10000.0 5.0 1.0 9.0 1.0 2.0 1.0 2.0 3.0 1.0 3.0 1.0 2.0 2.0 2.0 1.0 21.0 .0
ACBG51 1.0 2.0 4 1.0 1.0 1.0 .0 .0 .0 .0 .0 .0 1.0 1 1.0 2.0 1.0 12.0 SURESH 54.0 2.0 4 1.0 4.0 1.0 30000.0 4.0 1.0 5.0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 2.0 2.0 2.0 2.0 12.0 1.0
ACBG52 2.0 2.0 4 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 3 1.0 2.0 3.0 32.0 ANNAMM 58.0 2.0 1 1.0 2.0 1.0 10000.0 6.0 1.0 9.0 2.0 3.0 3.0 3.0 2.0 2.0 3.0 3.0 3.0 3.0 2.0 2.0 31.0 1.0
ACBG53 1.0 2.0 3 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 3.0 1,3 1.0 3.0 4.0 36.0 PADMA 65.0 2.0 2 1.0 3.0 2.0 25000.0 3.0 6.0 6.0 2.0 3.0 3.0 3.0 3.0 3.0 2.0 3.0 3.0 2.0 3.0 1.0 31.0 1.0
ACBG54 1.0 1.0 3 .0 1.0 1.0 .0 .0 1.0 1.0 .0 .0 3.0 3 1.0 2.0 3.0 9.0 KOKILA 50.0 2.0 2 1.0 3.0 1.0 9000.0 4.0 1.0 9.0 1.0 .0 .0 1.0 1.0 .0 .0 .0 1.0 .0 .0 .0 4.0 .0
ACBG55 2.0 1.0 3 .0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 3.0 1 2.0 2.0 4.0 34.0 MARIYA 54.0 2.0 2 4.0 4.0 1.0 10000.0 2.0 6.0 6.0 2.0 3.0 2.0 2.0 3.0 3.0 2.0 3.0 3.0 3.0 2.0 2.0 30.0 1.0
ACBG56 2.0 1.0 3 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 3.0 1 1.0 1.0 1.0 17.0 RENUGA 47.0 2.0 1 1.0 3.0 1.0 25000.0 5.0 1.0 9.0 1.0 2.0 2.0 1.0 2.0 2.0 1.0 2.0 2.0 1.0 2.0 1.0 19.0 1.0
ACBG57 2.0 1.0 4 1.0 1.0 1.0 .0 .0 1.0 1.0 .0 .0 2.0 1 1.0 1.0 3.0 16.0 BHARATH 33.0 2.0 1 1.0 4.0 2.0 35000.0 4.0 1.0 9.0 2.0 2.0 1.0 2.0 2.0 1.0 3.0 3.0 3.0 1.0 1.0 1.0 22.0 .0
ACBG58 1.0 2.0 3 .0 1.0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 0 2.0 1.0 3.0 11.0 KOMATHI 49.0 2.0 2 1.0 4.0 1.0 15000.0 4.0 1.0 9.0 1.0 3.0 1.0 .0 2.0 1.0 1.0 1.0 3.0 1.0 2.0 .0 16.0 .0
ACBG59 1.0 1.0 3 .0 1.0 1.0 .0 .0 .0 .0 .0 1.0 3.0 3 1.0 2.0 1.0 16.0 KALA 52.0 2.0 1 1.0 3.0 1.0 20000.0 6.0 1.0 9.0 1.0 2.0 1.0 1.0 3.0 2.0 2.0 2.0 2.0 1.0 1.0 1.0 19.0 1.0
ACBG60 2.0 2.0 3 .0 .0 .0 1.0 .0 .0 1.0 1.0 .0 3.0 3 1.0 2.0 3.0 12.0 MALIGA 44.0 2.0 1 1.0 4.0 1.0 16000.0 4.0 1.0 7.0 1.0 3.0 1.0 1.0 2.0 1.0 2.0 2.0 1.0 2.0 1.0 1.0 17.0 1.0
ACBG61 1.0 1.0 4 .0 1.0 .0 1.0 .0 .0 .0 1.0 .0 3.0 3 2.0 2.0 3.0 11.0 MERRY 25.0 2.0 1 4.0 6.0 1.0 25000.0 6.0 1.0 6.0 2.0 2.0 1.0 1.0 3.0 2.0 3.0 2.0 1.0 2.0 3.0 2.0 24.0 1.0
ACBG62 1.0 2.0 3 .0 .0 1.0 .0 .0 1.0 1.0 .0 .0 1.0 3 2.0 2.0 1.0 13.0 DULRAHE 51.0 1.0 7 2.0 5.0 2.0 40000.0 5.0 1.0 9.0 1.0 2.0 1.0 1.0 1.0 2.0 2.0 1.0 3.0 2.0 1.0 1.0 18.0 .0
ACBG63 2.0 1.0 3 .0 .0 1.0 1.0 .0 .0 1.0 .0 .0 2.0 3 1.0 1.0 3.0 15.0 AJESHWA 55.0 2.0 1 1.0 3.0 1.0 13000.0 5.0 1.0 7.0 1.0 2.0 1.0 2.0 2.0 2.0 1.0 1.0 2.0 2.0 2.0 1.0 19.0 .0
ACBG64 2.0 1.0 1 1.0 .0 .0 1.0 .0 1.0 1.0 .0 .0 1.0 3 1.0 2.0 3.0 17.0 AMUDHA 44.0 2.0 1 1.0 5.0 1.0 30000.0 4.0 1.0 9.0 2.0 2.0 1.0 2.0 3.0 2.0 1.0 2.0 2.0 1.0 1.0 1.0 20.0 .0
ACBG65 1.0 2.0 4 1.0 .0 .0 1.0 .0 1.0 .0 1.0 1.0 1.0 3 1.0 2.0 3.0 11.0 PRIYA 25.0 2.0 1 1.0 6.0 2.0 30000.0 4.0 1.0 5.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 .0 .0 8.0 19.0 1.0
ACBG66 2.0 1.0 3 .0 1.0 .0 1.0 .0 .0 1.0 1.0 .0 1.0 0 1.0 1.0 1.0 14.0 ANGAMM 46.0 2.0 1 1.0 3.0 1.0 20000.0 5.0 1.0 9.0 .0 1.0 .0 2.0 2.0 2.0 2.0 3.0 3.0 3.0 2.0 1.0 21.0 .0
ACBG67 1.0 1.0 3 .0 1.0 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 2 1.0 1.0 3.0 13.0 RADHA 40.0 2.0 1 1.0 4.0 1.0 8000.0 4.0 1.0 9.0 2.0 1.0 1.0 3.0 3.0 2.0 2.0 1.0 3.0 3.0 3.0 2.0 26.0 1.0
ACBG68 1.0 1.0 3 1.0 1.0 1.0 1.0 1.0 .0 .0 .0 .0 1.0 1 2.0 1.0 3.0 12.0 MARY 37.0 2.0 1 4.0 5.0 2.0 50000.0 4.0 1.0 9.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 12.0 .0
ACBG69 1.0 2.0 3 .0 .0 .0 .0 1.0 1.0 1.0 .0 1.0 1.0 3 1.0 1.0 3.0 17.0 KAVERY 49.0 2.0 1 1.0 4.0 1.0 15000.0 4.0 1.0 9.0 1.0 2.0 2.0 2.0 3.0 2.0 2.0 1.0 2.0 1.0 1.0 1.0 19.0 1.0
ACBG70 1.0 2.0 3 1.0 1.0 .0 .0 .0 .0 1.0 .0 1.0 1.0 3 1.0 2.0 1.0 7.0 ANANDHI 30.0 2.0 1 1.0 6.0 2.0 25000.0 3.0 1.0 9.0 2.0 2.0 1.0 1.0 1.0 1.0 .0 .0 .0 .0 .0 .0 8.0 .0
126
ACBG71 1.0 2.0 3 .0 .0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 3 1.0 1.0 3.0 18.0 SAROJINI 40.0 2.0 1 1.0 3.0 1.0 30000.0 5.0 1.0 9.0 2.0 2.0 1.0 1.0 2.0 2.0 2.0 1.0 2.0 2.0 1.0 2.0 20.0 1.0
ACBG72 1.0 1.0 3 .0 1.0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 0 2.0 2.0 3.0 11.0 PREETHI 45.0 2.0 1 1.0 4.0 1.0 15000.0 4.0 1.0 7.0 1.0 2.0 1.0 2.0 1.0 .0 .0 1.0 1 2.0 3.0 2.0 16.0 1.0
ACBG73 2.0 2.0 3 .0 .0 .0 .0 .0 .0 1.0 1.0 .0 3.0 3 1.0 2.0 3.0 12.0 MALINI 40.0 2.0 1 1.0 4.0 1.0 16000.0 4.0 1.0 7.0 1.0 3.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 1.0 1.0 1.0 20.0 1.0
ACBG74 2.0 2.0 3 .0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 2.0 1 1.0 1.0 4.0 19.0 USHA 49.0 2.0 1 1.0 4.0 1.0 20000.0 4.0 1.0 9.0 1.0 2.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 20.0 .0
ACBG75 2.0 2.0 3 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1 2.0 2.0 4.0 21.0 JANSI 27.0 2.0 3 4.0 6.0 1.0 20000.0 4.0 2.0 2.0 1.0 2.0 1.0 2.0 2.0 1.0 2.0 2.0 3.0 1.0 1.0 1.0 19.0 1.0
ACBG76 2.0 1.0 3 .0 1.0 .0 .0 .0 1.0 1.0 1.0 1.0 2.0 1 1.0 2.0 3.0 18.0 VASANTH 36.0 2.0 1 1.0 5.0 1.0 30000.0 4.0 1.0 9.0 2.0 2.0 1.0 1.0 2.0 1.0 2.0 1.0 2.0 2.0 1.0 2.0 19.0 .0
ACBG77 1.0 2.0 4 1.0 .0 .0 1.0 .0 1.0 .0 1.0 1.0 1.0 3 1.0 2.0 3.0 10.0 SUBHA 25.0 2.0 1 1.0 6.0 2.0 30000.0 4.0 1.0 5.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 12.0 .0
ACBG78 2.0 1.0 3 .0 1.0 .0 1.0 .0 .0 1.0 1.0 .0 1.0 0 1.0 1.0 1.0 14.0 DEVIKA 46.0 2.0 1 1.0 3.0 1.0 20000.0 5.0 1.0 9.0 1.0 2.0 1.0 2.0 2.0 1.0 2.0 3.0 3.0 3.0 2.0 1.0 23.0 .0
ACBG79 1.0 2.0 3 1.0 1.0 .0 .0 .0 .0 1.0 .0 1.0 1.0 3 1.0 1.0 1.0 3.0 NANDHIN 30.0 2.0 1 1.0 6.0 2.0 25000.0 3.0 1.0 9.0 .0 1.0 1.0 1.0 .0 .0 1.0 1.0 .0 .0 .0 1.0 6.0 .0
ACBG80 1.0 2.0 3 .0 .0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 3 1.0 1.0 3.0 18.0 AKILA 40.0 2.0 1 1.0 4.0 1.0 30000.0 5.0 1.0 9.0 2.0 3.0 2.0 2.0 2.0 3.0 2.0 1.0 2.0 1.0 1.0 2.0 23.0 .0
ACBG81 1.0 1.0 3,4 .0 1.0 .0 .0 .0 1.0 1.0 1.0 .0 3.0 3 1.0 1.0 3.0 19.0 ONAMMA 60.0 2.0 6 1.0 3.0 1.0 15000.0 3.0 6.0 6.0 1.0 3.0 1.0 1.0 3.0 2.0 2.0 1.0 3.0 1.0 2.0 1.0 21.0 .0
ACBG82 2.0 1.0 3 .0 .0 1.0 1.0 .0 .0 1.0 .0 .0 2.0 3 1.0 1.0 3.0 15.0 ARASWAT 55.0 2.0 1 1.0 3.0 1.0 13000.0 5.0 1.0 7.0 1.0 2.0 1.0 1.0 2.0 2.0 1.0 1.0 1.0 2.0 2.0 .0 16.0 1.0
ACBG83 1.0 2.0 3 .0 .0 .0 .0 1.0 1.0 1.0 .0 1.0 1.0 3 1.0 1.0 3.0 17.0 AMILARA 49.0 2.0 1 1.0 4.0 1.0 15000.0 4.0 1.0 9.0 1.0 2.0 1.0 1.0 3.0 1.0 2.0 2.0 3.0 2.0 1.0 1.0 20.0 .0
ACBG84 1.0 1.0 3 .0 1.0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 0 2.0 2.0 3.0 9.0 JANAKI 47.0 2.0 1 1.0 4.0 1.0 15000.0 4.0 1.0 7.0 2.0 1.0 1.0 1.0 .0 .0 .0 1.0 1 .0 .0 .0 5.0 1.0
ACBG85 1.0 1.0 4 .0 1.0 .0 1.0 .0 .0 .0 1.0 .0 3.0 3 2.0 2.0 3.0 11.0 SHEEBA 25.0 2.0 1 4.0 6.0 1.0 25000.0 6.0 1.0 6.0 2.0 3.0 1.0 2.0 3.0 1.0 2.0 2.0 1.0 2.0 3.0 2.0 24.0 1.0
ACBG86 2.0 2.0 3 .0 .0 .0 .0 .0 .0 1.0 1.0 .0 3.0 3 1.0 2.0 3.0 12.0 UMA 42.0 2.0 1 1.0 4.0 1.0 16000.0 4.0 1.0 7.0 2.0 3.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 24.0 1.0
ACBG87 1.0 2.0 3 .0 .0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 3 2.0 1.0 3.0 18.0 REENI 40.0 2.0 1 4.0 5.0 1.0 30000.0 5.0 1.0 9.0 1.0 2.0 1.0 1.0 2.0 1.0 2.0 1.0 3.0 1.0 2.0 2.0 19.0 .0
ACBG88 2.0 1.0 1 1.0 .0 .0 1.0 .0 1.0 1.0 .0 .0 1.0 3 1.0 2.0 3.0 17.0 KUMUDH 44.0 2.0 1 1.0 5.0 1.0 30000.0 4.0 1.0 9.0 1.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 3.0 1.0 1.0 21.0 .0
ACBG89 2.0 2.0 3 .0 .0 .0 1.0 .0 .0 1.0 1.0 .0 3.0 3 1.0 2.0 3.0 12.0 SUGANTH 42.0 2.0 1 1.0 4.0 1.0 16000.0 4.0 1.0 7.0 1.0 2.0 1.0 1.0 3.0 1.0 2.0 1.0 2.0 2.0 .0 1.0 17.0 .0
ACBG90 1.0 2.0 4 1.0 .0 .0 1.0 .0 1.0 .0 1.0 1.0 1.0 3 1.0 1.0 3.0 7.0 RILOCHA 27.0 2.0 1 1.0 6.0 2.0 30000.0 4.0 1.0 5.0 1.0 3.0 1.0 1.0 .0 .0 .0 .0 .0 .0 2.0 1.0 9.0 .0
ACBG91 1.0 1.0 3 .0 1.0 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 2 1.0 1.0 3.0 13.0 SUGANYA 41.0 2.0 1 1.0 4.0 1.0 8000.0 4.0 1.0 9.0 2.0 1.0 1.0 3.0 1.0 2.0 2.0 1.0 3.0 3.0 3.0 2.0 24.0 1.0
ACBG92 2.0 2.0 3 .0 1.0 .0 1.0 .0 .0 .0 .0 .0 2.0 2 1.0 2.0 1.0 14.0 MEENAKSH 50.0 2.0 2 1.0 3.0 1.0 10000.0 5.0 6.0 6.0 1.0 3.0 1.0 1.0 2.0 3.0 1.0 1.0 3.0 1.0 2.0 2.0 21.0 .0
ACBG93 1.0 2.0 3 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1 1.0 2.0 4.0 17.0 ANDAL 49.0 2.0 1 1.0 4.0 1.0 15000.0 4.0 1.0 9.0 1.0 3.0 1.0 1.0 3.0 2.0 1.0 2.0 2.0 1.0 1.0 1.0 19.0 1.0
ACBG94 2.0 2.0 4 .0 .0 1.0 1.0 1.0 .0 .0 .0 .0 3.0 2 1.0 2.0 4.0 19.0 KAMALA 51.0 2.0 1 1.0 4.0 1.0 20000.0 6.0 1.0 9.0 2.0 3.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 22.0 1.0
ACBG95 1.0 2.0 3 .0 1.0 1.0 .0 .0 1.0 1.0 1.0 .0 1.0 1 1.0 2.0 3.0 18.0 THALAKS 59.0 2.0 1 1.0 3.0 1.0 20000.0 5.0 1.0 9.0 1.0 2.0 1.0 1.0 2.0 3.0 1.0 1.0 3.0 1.0 1.0 1.0 18.0 .0
ACBG96 2.0 1.0 4 .0 .0 .0 .0 .0 .0 .0 .0 .0 1.0 3 1.0 2.0 3.0 11.0 REVATHI 37.0 2.0 1 1.0 5.0 1.0 50000.0 4.0 1.0 9.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 2.0 14.0 1.0
ACBG97 2.0 2.0 4 .0 .0 1.0 1.0 1.0 .0 .0 .0 .0 3.0 2 1.0 1.0 4.0 17.0 AJALAKSH 50.0 2.0 1 1.0 5.0 1.0 20000.0 5.0 1.0 9.0 1.0 3.0 1.0 1.0 3.0 1.0 2.0 2.0 2.0 2.0 1.0 2.0 21.0 .0
ACBG98 1.0 1.0 3 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 .0 3.0 2 1.0 1.0 4.0 7.0 ULOCHAN 46.0 2.0 2 1.0 4.0 1.0 15000.0 4.0 1.0 9.0 1.0 2.0 2.0 .0 .0 .0 .0 1.0 1.0 1.0 1.0 1.0 10.0 1.0
ACBG99 1.0 1.0 3 .0 1.0 1.0 .0 .0 1.0 1.0 .0 .0 3.0 3 1.0 2.0 3.0 5.0 THAMARA 50.0 2.0 2 1.0 3.0 1.0 9000.0 4.0 1.0 9.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 11.0 1.0
ACBG100 2.0 2.0 3 .0 1.0 .0 1.0 .0 .0 .0 .0 .0 2.0 2 1.0 2.0 1.0 14.0 SAROJA 48.0 2.0 2 1.0 3.0 1.0 10000.0 5.0 6.0 6.0 2.0 2.0 3.0 2.0 2.0 1.0 2.0 1.0 1.0 1.0 .0 1.0 18.0 .0

127
UID
FINANCI
AL2
FINANCI
AL3
FINANCI
AL4
FINANCI
AL5
FINANCI
AL6
ROUTINE
ACT1
ROUTINE
ACT2
ROUTINE
ACT3
ROUTINE
ACT4
ROUTINE
ACT5
FAMILYL
EISUR1
FAMILYL
EISURE2
FAMILYL
EISURE3
FAMILY
LEISUR 4
FAMILY
INTERAC
FAMILY
INTERAC
T 2
FAMILY
INTERAC
T 3
FAMILY
INTERAC
T 4
FAMILY
INTERAC
T 5
PHYSICA
L
HEALTH
1
PHYSICA
LHEALTH
2
MENTAL
HEALTH1
MENTAL
HEALTH2
FBS total
score
subjectiv
e burden
FBSCAT
FBSDUAL
CAT
ghqcat
GHQDUA
LCAT
SADQ
CAT
Financial
Routine
family
leisure
family
interacti
on
physical
health
mental
health
Financial
avg
routinea
vg
leisure
avg
interacti
onavg
physicala
vg
mental
avg
ACGB01 1.0 2.0 .0 2.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 1.0 .0 1.0 1.0 .0 1.0 .0 2.0 1.0 .0 2.0 1.0 24.0 2 2 1 3 1 2.0 7.0 6.0 3.0 4.0 1.0 3.0 1.166667 1.2 0.75 0.8 0.5 1.5
ACGB02 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 2.0 2.0 23.0 1 1 1 3 1 2.0 3.0 5.0 5.0 5.0 1.0 4.0 0.5 1 1.25 1 0.5 2
ACGB03 .0 1.0 .0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 .0 1.0 .0 .0 1.0 2.0 1.0 1.0 .0 18.0 1 1 1 3 1 1.0 4.0 5.0 3.0 2.0 3.0 1.0 0.666667 1 0.75 0.4 1.5 0.5
ACGB04 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 1.0 2.0 1.0 1.0 .0 18.0 1 1 1 3 1 2.0 3.0 5.0 4.0 2.0 3.0 1.0 0.5 1 1 0.4 1.5 0.5
ACGB05 .0 1.0 .0 1.0 1.0 1.0 .0 .0 1.0 .0 .0 1.0 1.0 1.0 .0 2.0 .0 .0 1.0 2.0 2.0 .0 1.0 16.0 1 1 1 3 1 1.0 3.0 2.0 3.0 3.0 4.0 1.0 0.5 0.4 0.75 0.6 2 0.5
ACGB06 .0 1.0 .0 1.0 1.0 2.0 1.0 .0 1.0 .0 1.0 1.0 1.0 1.0 .0 .0 .0 1.0 1.0 2.0 1.0 1.0 1.0 18.0 1 1 1 4 1 1.0 3.0 4.0 4.0 2.0 3.0 2.0 0.5 0.8 1 0.4 1.5 1
ACGB07 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 1.0 .0 1.0 .0 .0 1.0 1.0 .0 4 1.0 .0 2.0 1 2 1.0 0.0 0.0 0.0 2.0 1.0 1.0 0 0 0 0.4 0.5 0.5
ACGB08 .0 1.0 1.0 1.0 2.0 1.0 1.0 1.0 1.0 2.0 .0 1.0 1.0 1.0 .0 1.0 1.0 .0 1.0 .0 1.0 1.0 2.0 22.0 2 1 1 3 1 2.0 6.0 6.0 3.0 3.0 1.0 3.0 1 1.2 0.75 0.6 0.5 1.5
ACGB09 1.0 1.0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 1.0 1.0 .0 .0 .0 .0 1.0 7 1.0 .0 2.0 3 1 1.0 4.0 0.0 0.0 2.0 0.0 1.0 0.666667 0 0 0.4 0 0.5
ACGB10 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 2.0 .0 .0 2.0 2.0 2.0 .0 1.0 23.0 2 1 1 4 1 2.0 3.0 6.0 4.0 5.0 4.0 1.0 0.5 1.2 1 1 2 0.5
ACGB11 .0 1.0 .0 .0 1.0 1.0 1.0 .0 .0 .0 1.0 .0 .0 .0 .0 2.0 .0 1.0 .0 1.0 1.0 2.0 2.0 15 1.0 1.0 1.0 3 1 1.0 3.0 2.0 1.0 3.0 2.0 4.0 0.5 0.4 0.25 0.6 1 2
ACGB12 .0 1.0 .0 .0 .0 2.0 .0 1.0 .0 .0 .0 .0 1.0 .0 .0 .0 .0 1.0 1.0 .0 .0 .0 .0 8 1.0 1.0 1.0 1 2 1.0 2.0 3.0 1.0 2.0 0.0 0.0 0.333333 0.6 0.25 0.4 0 0
ACGB13 .0 1.0 .0 .0 .0 .0 1.0 .0 .0 .0 .0 1.0 1.0 .0 1.0 1.0 .0 .0 .0 .0 .0 .0 .0 6 1.0 .0 2.0 1 2 1.0 1.0 1.0 2.0 2.0 0.0 0.0 0.166667 0.2 0.5 0.4 0 0
ACGB14 .0 1.0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 .0 1.0 .0 .0 1.0 2.0 1.0 1.0 1.0 16.0 1 1 1 3 1 2.0 3.0 4.0 2.0 2.0 3.0 2.0 0.5 0.8 0.5 0.4 1.5 1
ACGB15 .0 1.0 .0 1.0 1.0 2.0 1.0 1.0 1.0 2.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 .0 1.0 21.0 1 1 1 4 1 2.0 3.0 7.0 4.0 2.0 4.0 1.0 0.5 1.4 1 0.4 2 0.5
ACGB16 1.0 1.0 .0 .0 .0 1.0 1.0 .0 .0 .0 .0 .0 1.0 .0 1.0 .0 1.0 .0 1.0 .0 1.0 .0 1.0 10 1.0 1.0 1.0 1 2 1.0 2.0 2.0 1.0 3.0 1.0 1.0 0.333333 0.4 0.25 0.6 0.5 0.5
ACGB17 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 2.0 .0 .0 2.0 1.0 2.0 1.0 .0 19.0 1 1 1 4 1 2.0 3.0 5.0 3.0 4.0 3.0 1.0 0.5 1 0.75 0.8 1.5 0.5
ACGB18 1.0 .0 .0 1.0 1.0 1.0 1.0 1.0 1.0 .0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 .0 .0 1.0 2.0 18 1.0 1.0 1.0 3 1 1.0 4.0 4.0 2.0 5.0 0.0 3.0 0.666667 0.8 0.5 1 0 1.5
ACGB19 .0 2.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 1.0 1.0 21.0 1 1 1 3 1 2.0 4.0 5.0 4.0 2.0 4.0 2.0 0.666667 1 1 0.4 2 1
ACGB20 1.0 .0 .0 .0 .0 .0 1.0 .0 .0 1.0 .0 .0 .0 .0 .0 .0 .0 .0 .0 1.0 .0 1.0 .0 5 1.0 .0 2.0 2 1 1.0 1.0 2.0 0.0 0.0 1.0 1.0 0.166667 0.4 0 0 0.5 0.5
ACGB21 1.0 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 1.0 .0 20.0 1 1 1 4 1 2.0 4.0 5.0 4.0 2.0 4.0 1.0 0.666667 1 1 0.4 2 0.5
ACGB22 2.0 1.0 .0 1.0 .0 2.0 1.0 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 20 2.0 1.0 1.0 3 1 2.0 4.0 4.0 3.0 5.0 2.0 2.0 0.666667 0.8 0.75 1 1 1
ACGB23 1.0 1.0 .0 1.0 .0 2.0 1.0 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 .0 .0 .0 1.0 17 2.0 1.0 1.0 3 1 2.0 5.0 4.0 3.0 4.0 0.0 1.0 0.833333 0.8 0.75 0.8 0 0.5
ACGB24 .0 2.0 1.0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 1.0 1.0 2.0 24.0 2 2 1 3 1 2.0 6.0 5.0 5.0 4.0 1.0 3.0 1 1 1.25 0.8 0.5 1.5
ACGB25 1.0 2.0 .0 2.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 2.0 .0 .0 2.0 2.0 2.0 1.0 2.0 30.0 2 2 1 4 1 3.0 8.0 5.0 5.0 5.0 4.0 3.0 1.333333 1 1.25 1 2 1.5
ACGB26 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 2.0 1.0 1.0 1.0 .0 .0 1.0 2.0 2.0 23.0 1 1 1 4 1 1.0 3.0 5.0 5.0 5.0 1.0 4.0 0.5 1 1.25 1 0.5 2
ACGB27 .0 .0 .0 1.0 .0 .0 .0 .0 1.0 .0 1.0 .0 .0 .0 .0 1.0 .0 1.0 .0 .0 .0 1.0 1.0 7 1.0 1.0 1.0 1 2 1.0 1.0 1.0 1.0 2.0 0.0 2.0 0.166667 0.2 0.25 0.4 0 1
ACGB28 .0 1.0 .0 .0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 1.0 .0 1.0 .0 10 1.0 1.0 1.0 1 2 1.0 2.0 2.0 2.0 2.0 1.0 1.0 0.333333 0.4 0.5 0.4 0.5 0.5
ACGB29 1.0 1.0 .0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 2.0 1.0 2.0 1.0 1.0 24.0 2 2 1 4 1 2.0 5.0 5.0 4.0 5.0 3.0 2.0 0.833333 1 1 1 1.5 1
ACGB30 .0 1.0 .0 .0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 .0 1.0 .0 .0 .0 .0 .0 .0 .0 1.0 .0 7 1.0 1.0 1.0 1 2 1.0 2.0 2.0 2.0 0.0 0.0 1.0 0.333333 0.4 0.5 0 0 0.5
ACGB31 1.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 2.0 2.0 1.0 1.0 2.0 2.0 41.0 2 2 1 4 1 3.0 9.0 10.0 8.0 8.0 2.0 4.0 1.5 2 2 1.6 1 2
ACBG32 1.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 2.0 2.0 1.0 1.0 2.0 1.0 1.0 2.0 2.0 2.0 1.0 1.0 38.0 2 2 1 4 1 3.0 9.0 9.0 7.0 7.0 4.0 2.0 1.5 1.8 1.75 1.4 2 1
ACBG33 1.0 .0 1.0 .0 1.0 1.0 .0 .0 1.0 .0 1.0 1.0 .0 1.0 .0 .0 1.0 1.0 1.0 .0 1.0 1.0 1.0 15 1.0 1.0 1.0 3 1 1.0 4.0 2.0 3.0 3.0 1.0 2.0 0.666667 0.4 0.75 0.6 0.5 1
ACBG34 1.0 .0 .0 .0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 1.0 2.0 1.0 .0 2.0 1.0 18 1.0 1.0 1.0 4 1 2.0 3.0 4.0 3.0 4.0 1.0 3.0 0.5 0.8 0.75 0.8 0.5 1.5
ACBG35 1.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 1.0 2.0 2.0 2.0 1.0 1.0 40.0 2 2 1 4 1 3.0 9.0 10.0 8.0 7.0 4.0 2.0 1.5 2 2 1.4 2 1
ACBG36 .0 2.0 .0 1.0 1.0 1.0 2.0 1.0 2.0 1.0 1.0 .0 1.0 2.0 .0 2.0 .0 1.0 2.0 1.0 .0 2.0 2.0 26.0 1 2 1 4 1 1.0 5.0 7.0 4.0 5.0 1.0 4.0 0.833333 1.4 1 1 0.5 2
ACBG37 .0 .0 .0 .0 1.0 .0 1.0 .0 .0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 1.0 1.0 1.0 .0 1.0 1.0 13 1.0 1.0 1.0 3 1 2.0 2.0 2.0 3.0 3.0 1.0 2.0 0.333333 0.4 0.75 0.6 0.5 1
ACBG38 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 2.0 2.0 23.0 1 1 1 4 1 2.0 5.0 5.0 4.0 4.0 1.0 4.0 0.833333 1 1 0.8 0.5 2
ACBG39 1.0 .0 .0 1.0 1.0 1.0 .0 .0 1.0 1.0 1.0 1.0 .0 .0 .0 2.0 .0 1.0 .0 2.0 .0 2.0 2.0 18 2.0 1.0 1.0 4 1 2.0 4.0 3.0 2.0 3.0 2.0 4.0 0.666667 0.6 0.5 0.6 1 2
ACBG40 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 .0 .0 2.0 2.0 2.0 1.0 1.0 1.0 1.0 1.0 23 2.0 1.0 1.0 4 1 2.0 6.0 4.0 2.0 7.0 2.0 2.0 1 0.8 0.5 1.4 1 1
ACBG41 .0 1.0 .0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 2.0 .0 .0 1.0 2.0 2.0 1.0 1.0 22.0 1 1 1 4 1 2.0 4.0 5.0 4.0 3.0 4.0 2.0 0.666667 1 1 0.6 2 1
ACBG42 1.0 2.0 1.0 2.0 2.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 1.0 2.0 2.0 2.0 1.0 1.0 39.0 2 2 1 4 1 3.0 9.0 9.0 8.0 7.0 4.0 2.0 1.5 1.8 2 1.4 2 1
ACBG43 .0 2.0 .0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 2.0 .0 1.0 .0 1.0 .0 1.0 1.0 2.0 1.0 1.0 .0 22.0 2 1 1 4 1 2.0 5.0 6.0 4.0 3.0 3.0 1.0 0.833333 1.2 1 0.6 1.5 0.5
ACBG44 1.0 1.0 .0 1.0 2.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 1.0 .0 2.0 1.0 .0 1.0 .0 1.0 2.0 2.0 21.0 1 1 1 3 1 1.0 5.0 4.0 3.0 4.0 1.0 4.0 0.833333 0.8 0.75 0.8 0.5 2
ACBG45 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 .0 1.0 .0 1.0 .0 1.0 .0 1.0 2.0 2.0 17.0 1 1 1 4 1 1.0 3.0 4.0 2.0 3.0 1.0 4.0 0.5 0.8 0.5 0.6 0.5 2
ACBG46 .0 2.0 .0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 2.0 2.0 24.0 1 2 1 4 1 2.0 5.0 5.0 5.0 4.0 1.0 4.0 0.833333 1 1.25 0.8 0.5 2
ACBG47 1.0 2.0 .0 2.0 1.0 1.0 1.0 .0 1.0 2.0 1.0 2.0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 2.0 1.0 24.0 1 2 1 4 1 1.0 7.0 5.0 4.0 4.0 1.0 3.0 1.166667 1 1 0.8 0.5 1.5
ACBG48 .0 2.0 .0 1.0 2.0 1.0 1.0 1.0 .0 2.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 2.0 .0 1.0 2.0 1.0 21.0 1 1 1 4 1 2.0 5.0 5.0 4.0 3.0 1.0 3.0 0.833333 1 1 0.6 0.5 1.5
ACBG49 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 1.0 1.0 2.0 1.0 1.0 20.0 1 1 1 4 1 2.0 3.0 5.0 4.0 3.0 3.0 2.0 0.5 1 1 0.6 1.5 1
ACBG50 1.0 2.0 .0 2.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 2.0 .0 .0 2.0 2.0 1.0 1.0 1.0 26.0 2 2 1 4 1 2.0 6.0 6.0 4.0 5.0 3.0 2.0 1 1.2 1 1 1.5 1
ACBG51 .0 .0 .0 .0 .0 .0 1.0 .0 .0 1.0 .0 .0 .0 1.0 .0 .0 .0 1.0 1.0 1.0 .0 .0 .0 7 1.0 1.0 1.0 2 1 1.0 1.0 2.0 1.0 2.0 1.0 0.0 0.166667 0.4 0.25 0.4 0.5 0
ACBG52 1.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 2.0 2.0 2.0 2.0 1.0 2.0 42.0 2 2 1 4 1 3.0 9.0 10.0 8.0 8.0 4.0 3.0 1.5 2 2 1.6 2 1.5
ACBG53 2.0 2.0 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.0 1.0 2.0 2.0 2.0 2.0 1.0 42.0 2 2 1 4 1 3.0 10.0 10.0 8.0 7.0 4.0 3.0 1.666667 2 2 1.4 2 1.5
ACBG54 .0 1.0 .0 1.0 .0 .0 1.0 .0 .0 1.0 1.0 .0 .0 .0 .0 .0 .0 .0 1.0 .0 .0 1.0 .0 7 1.0 1.0 1.0 1 2 1.0 2.0 2.0 1.0 1.0 0.0 1.0 0.333333 0.4 0.25 0.2 0 0.5
ACBG55 1.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 2.0 1.0 1.0 44.0 2 2 1 4 1 3.0 10.0 10.0 8.0 10.0 4.0 2.0 1.666667 2 2 2 2 1
ACBG56 .0 1.0 .0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 1.0 1.0 22.0 1 1 1 3 1 2.0 5.0 5.0 4.0 2.0 4.0 2.0 0.833333 1 1 0.4 2 1
ACBG57 1.0 1.0 .0 1.0 2.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 .0 .0 .0 1.0 .0 1.0 .0 1.0 2.0 2.0 18.0 1 1 1 4 1 2.0 5.0 4.0 2.0 2.0 1.0 4.0 0.833333 0.8 0.5 0.4 0.5 2
ACBG58 1.0 2.0 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 1.0 1.0 2.0 .0 1.0 19.0 1 1 1 3 1 1.0 4.0 5.0 4.0 2.0 3.0 1.0 0.666667 1 1 0.4 1.5 0.5
ACBG59 1.0 2.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 2.0 .0 .0 2.0 2.0 2.0 1.0 1.0 25.0 2 2 1 3 1 2.0 6.0 5.0 4.0 4.0 4.0 2.0 1 1 1 0.8 2 1
ACBG60 .0 1.0 .0 1.0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 1.0 1.0 2.0 2.0 1.0 1.0 19.0 1 1 1 3 1 1.0 3.0 4.0 3.0 3.0 4.0 2.0 0.5 0.8 0.75 0.6 2 1
ACBG61 .0 2.0 .0 1.0 1.0 1.0 2.0 1.0 2.0 1.0 1.0 .0 1.0 2.0 .0 2.0 .0 1.0 2.0 1.0 .0 2.0 2.0 26.0 2 2 1 4 1 1.0 5.0 7.0 4.0 5.0 1.0 4.0 0.833333 1.4 1 1 0.5 2
ACBG62 .0 1.0 .0 .0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 1.0 1.0 .0 .0 1.0 1.0 1.0 2.0 2.0 1.0 1.0 18.0 1 1 1 3 1 1.0 2.0 4.0 3.0 3.0 4.0 2.0 0.333333 0.8 0.75 0.6 2 1
ACBG63 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 1.0 1.0 18.0 1 1 1 3 1 1.0 3.0 4.0 3.0 2.0 4.0 2.0 0.5 0.8 0.75 0.4 2 1
ACBG64 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 1.0 2.0 2.0 1.0 1.0 21.0 2 1 1 4 1 2.0 3.0 5.0 4.0 3.0 4.0 2.0 0.5 1 1 0.6 2 1
ACBG65 .0 1.0 .0 2.0 .0 .0 1.0 1.0 .0 .0 .0 2.0 1.0 1.0 2.0 1.0 .0 2.0 .0 1.0 1.0 1.0 2.0 20 2.0 1.0 1.0 3 1 1.0 4.0 2.0 4.0 5.0 2.0 3.0 0.666667 0.4 1 1 1 1.5
ACBG66 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 .0 .0 .0 1.0 .0 1.0 2.0 1.0 1.0 1.0 17.0 1 1 1 4 1 1.0 4.0 4.0 2.0 2.0 3.0 2.0 0.666667 0.8 0.5 0.4 1.5 1
ACBG67 1.0 .0 .0 1.0 1.0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 19.0 1 1 1 4 1 1.0 4.0 3.0 4.0 4.0 2.0 2.0 0.666667 0.6 1 0.8 1 1
ACBG68 .0 .0 .0 1.0 1.0 .0 1.0 .0 .0 1.0 .0 1.0 .0 .0 .0 .0 1.0 1.0 .0 .0 .0 .0 .0 7 1.0 1.0 1.0 3 1 1.0 2.0 2.0 1.0 2.0 0.0 0.0 0.333333 0.4 0.25 0.4 0 0
ACBG69 .0 1.0 .0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 .0 1.0 1.0 2.0 1.0 1.0 22.0 1 1 1 3 1 2.0 5.0 5.0 4.0 3.0 3.0 2.0 0.833333 1 1 0.6 1.5 1
ACBG70 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 1.0 .0 1.0 1.0 1.0 .0 .0 .0 1.0 .0 14 1.0 1.0 1.0 1 2 1.0 3.0 4.0 3.0 3.0 0.0 1.0 0.5 0.8 0.75 0.6 0 0.5
128
ACBG71 1.0 2.0 .0 2.0 2.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 2.0 1.0 28.0 2 2 1 4 1 2.0 8.0 6.0 3.0 5.0 3.0 3.0 1.333333 1.2 0.75 1 1.5 1.5
ACBG72 .0 1.0 .0 1.0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 1.0 1.0 1.0 .0 1.0 1.0 16 2.0 1.0 1.0 4 1 1.0 3.0 4.0 3.0 3.0 1.0 2.0 0.5 0.8 0.75 0.6 0.5 1
ACBG73 .0 1.0 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 .0 1.0 .0 1.0 1 1.0 2.0 1.0 .0 20.0 1 1 1 4 1 1.0 3.0 5.0 5.0 3.0 3.0 1.0 0.5 1 1.25 0.6 1.5 0.5
ACBG74 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 2.0 .0 1.0 2.0 2.0 2.0 1.0 1.0 23.0 1 1 1 4 1 2.0 3.0 5.0 4.0 5.0 4.0 2.0 0.5 1 1 1 2 1
ACBG75 .0 2.0 .0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 .0 1.0 2.0 2.0 18.0 1 1 1 3 1 2.0 5.0 4.0 2.0 2.0 1.0 4.0 0.833333 0.8 0.5 0.4 0.5 2
ACBG76 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 2.0 1.0 1.0 2.0 2.0 2.0 1.0 1.0 25.0 1 2 1 3 1 2.0 4.0 5.0 4.0 6.0 4.0 2.0 0.666667 1 1 1.2 2 1
ACBG77 .0 2.0 .0 1.0 .0 .0 .0 .0 1.0 1.0 .0 .0 .0 1.0 .0 1.0 .0 .0 1.0 .0 1.0 1.0 1.0 11 1.0 1.0 1.0 3 1 1.0 3.0 2.0 1.0 2.0 1.0 2.0 0.5 0.4 0.25 0.4 0.5 1
ACBG78 1.0 1.0 .0 2.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 .0 2.0 .0 1.0 2.0 2.0 .0 1.0 21.0 1 1 1 4 1 1.0 5.0 4.0 3.0 4.0 4.0 1.0 0.833333 0.8 0.75 0.8 2 0.5
ACBG79 .0 1.0 .0 .0 1.0 1.0 .0 1.0 1.0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 .0 1.0 .0 6 1.0 .0 2.0 1 2 1.0 2.0 3.0 0.0 0.0 0.0 1.0 0.333333 0.6 0 0 0 0.5
ACBG80 .0 1.0 .0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 1.0 1.0 2.0 1.0 1.0 2.0 2.0 2.0 1.0 1.0 27.0 2 2 1 4 1 2.0 4.0 5.0 5.0 7.0 4.0 2.0 0.666667 1 1.25 1.4 2 1
ACBG81 1.0 2.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 2.0 2.0 1.0 1.0 1.0 22.0 1 1 1 4 1 2.0 5.0 5.0 4.0 3.0 3.0 2.0 0.833333 1 1 0.6 1.5 1
ACBG82 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 1.0 1.0 18.0 1 1 1 3 1 1.0 3.0 4.0 3.0 2.0 4.0 2.0 0.5 0.8 0.75 0.4 2 1
ACBG83 1.0 2.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 2.0 1.0 1.0 24.0 1 2 1 4 1 2.0 5.0 5.0 3.0 5.0 4.0 2.0 0.833333 1 0.75 1 2 1
ACBG84 .0 .0 .0 1.0 .0 .0 .0 .0 .0 1.0 1.0 .0 .0 .0 .0 1.0 .0 1.0 .0 .0 .0 1.0 .0 7 1.0 1.0 1.0 1 2 1.0 2.0 1.0 1.0 2.0 0.0 1.0 0.333333 0.2 0.25 0.4 0 0.5
ACBG85 1.0 2.0 .0 2.0 1.0 1.0 2.0 2.0 1.0 2.0 1.0 2.0 1.0 1.0 .0 2.0 .0 1.0 2.0 1.0 .0 2.0 2.0 30.0 2 2 1 4 1 1.0 7.0 8.0 5.0 5.0 1.0 4.0 1.166667 1.6 1.25 1 0.5 2
ACBG86 .0 1.0 .0 1.0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 1 1.0 1.0 .0 1.0 18.0 1 1 1 4 1 1.0 3.0 4.0 4.0 4.0 2.0 1.0 0.5 0.8 1 0.8 1 0.5
ACBG87 1.0 2.0 .0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 2.0 2.0 1.0 1.0 26.0 2 2 1 3 1 2.0 6.0 5.0 4.0 5.0 4.0 2.0 1 1 1 1 2 1
ACBG88 .0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 .0 2.0 1.0 2.0 1.0 .0 19.0 1 1 1 4 1 2.0 3.0 5.0 4.0 3.0 3.0 1.0 0.5 1 1 0.6 1.5 0.5
ACBG89 .0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 1.0 1.0 18.0 1 1 1 3 1 1.0 3.0 4.0 3.0 2.0 4.0 2.0 0.5 0.8 0.75 0.4 2 1
ACBG90 .0 1.0 .0 1.0 .0 .0 .0 1.0 .0 .0 .0 1.0 .0 .0 .0 .0 .0 1.0 .0 .0 1.0 .0 .0 6 1.0 .0 2.0 1 2 1.0 2.0 1.0 1.0 1.0 1.0 0.0 0.333333 0.2 0.25 0.2 0.5 0
ACBG91 1.0 1.0 .0 1.0 1.0 1.0 2.0 2.0 .0 1.0 2.0 1.0 2.0 1.0 1.0 1.0 .0 1.0 2.0 2.0 2.0 1.0 1.0 28.0 1 2 1 4 1 1.0 5.0 6.0 6.0 5.0 4.0 2.0 0.833333 1.2 1.5 1 2 1
ACBG92 .0 2.0 .0 .0 2.0 1.0 1.0 1.0 .0 .0 .0 1.0 1.0 1.0 1.0 2.0 1.0 .0 2.0 1.0 2.0 .0 .0 19.0 1 1 1 4 1 1.0 4.0 3.0 3.0 6.0 3.0 0.0 0.666667 0.6 0.75 1.2 1.5 0
ACBG93 .0 2.0 .0 2.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 2.0 .0 .0 1.0 2.0 2.0 .0 1.0 24.0 2 2 1 3 1 2.0 7.0 5.0 4.0 3.0 4.0 1.0 1.166667 1 1 0.6 2 0.5
ACBG94 .0 2.0 .0 1.0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 2.0 .0 .0 1.0 2.0 2.0 1.0 1.0 24.0 1 2 1 4 1 2.0 6.0 5.0 4.0 3.0 4.0 2.0 1 1 1 0.6 2 1
ACBG95 .0 2.0 .0 .0 2.0 1.0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 .0 .0 1.0 2.0 2.0 2.0 1.0 21.0 1 1 1 3 1 2.0 4.0 5.0 3.0 2.0 4.0 3.0 0.666667 1 0.75 0.4 2 1.5
ACBG96 .0 1.0 .0 1.0 .0 .0 1.0 .0 .0 .0 .0 .0 .0 1.0 .0 1.0 .0 1.0 1.0 1.0 .0 1.0 1.0 11 1.0 1.0 1.0 2 1 1.0 3.0 1.0 1.0 3.0 1.0 2.0 0.5 0.2 0.25 0.6 0.5 1
ACBG97 .0 1.0 .0 1.0 2.0 1.0 1.0 .0 1.0 1.0 1.0 1.0 1.0 1.0 .0 1.0 .0 1.0 1.0 1.0 2.0 1.0 1.0 20.0 1 1 1 4 1 2.0 4.0 4.0 4.0 3.0 3.0 2.0 0.666667 0.8 1 0.6 1.5 1
ACBG98 .0 1.0 .0 1.0 .0 1.0 1.0 .0 1.0 1.0 .0 .0 1.0 1.0 .0 1.0 1.0 1.0 1.0 .0 .0 1.0 .0 14 1.0 1.0 1.0 1 2 1.0 3.0 4.0 2.0 4.0 0.0 1.0 0.5 0.8 0.5 0.8 0 0.5
ACBG99 .0 1.0 .0 1.0 .0 .0 1.0 .0 1.0 .0 .0 .0 .0 1.0 .0 2.0 .0 .0 2.0 .0 .0 1.0 2.0 13 1.0 1.0 1.0 2 1 1.0 3.0 2.0 1.0 4.0 0.0 3.0 0.5 0.4 0.25 0.8 0 1.5
ACBG100 .0 2.0 1.0 2.0 1.0 1.0 1.0 1.0 2.0 2.0 2.0 1.0 .0 2.0 .0 1.0 .0 .0 1.0 1.0 1.0 1.0 1.0 24.0 2 2 1 3 1 2.0 6.0 7.0 5.0 2.0 2.0 2.0 1 1.4 1.25 0.4 1 1
Related Documents











