Cardiovascular characterization of Pkd2 +/LacZ mice, an animal model for the autosomal dominant polycystic kidney disease type 2 (ADPKD2) Jörg Stypmann a,b,1 , Markus A. Engelen a,c,1 , Stefan Orwat a , Konstantinos Bilbilis d , Markus Rothenburger e , Lars Eckardt a , Wilhelm Haverkamp a,b , Jürgen Horst d , Bernd Dworniczak d , Petra Pennekamp d, ⁎ a Department of Cardiology and Angiology, Hospital of the University of Münster, Germany b Interdisciplinary Center for Clinical Research (IZKF), Central Project Group 4 (ZPG4a), Münster, Germany c Department of Medical Physiology, University Medical Center Utrecht, The Netherlands d Institut für Humangenetik, Universitätsklinikum Münster, Vesaliusweg 12, D - 48149 Münster, Germany e Department for Thoracic and Cardiovascular Surgery, Hospital of the University of Münster, Germany Received 21 February 2006; received in revised form 27 August 2006; accepted 20 September 2006 Available online 19 December 2006 Abstract Background: Autosomal dominant polycystic kidney disease (ADPKD) is caused by mutations in PKD1 or PKD2. Patients with ADPKD have an increased incidence of cardiac valve abnormalities and left ventricular hypertrophy. Systematic analyses of cardiovascular involvement have so far been performed only on genetically unclassified patients or on ADPKD1 patients, but not on genetically defined ADPKD2 patients. Even existing Pkd1 or Pkd2 mouse models were not thoroughly analyzed in this respect. Therefore, the aim of this project was the noninvasive functional cardiovascular characterization of a mouse model for ADPKD2. Methods: Pkd2 +/LacZ mice and wildtype controls were classified into 8 groups with respect to gender, age and genotype. In addition, two subgroups of female mice were analyzed for cardiac function before and during advanced pregnancy. Doppler-echocardiographic as well as histological studies were performed. Results: Doppler-echocardiography did not reveal significant cardiovascular changes. Heart rate and left ventricular (LV) length, LV mass, LV enddiastolic and LVendsystolic diameters did not differ significantly among the various groups when comparing wildtype and knockout mice. There were no significant differences except for a tendency towards higher maximal early and late flow velocities over the mitral valve in old wildtype mice. Conclusions: Non-invasive phenotyping using ultrasound did not reveal significant cardiovascular difference between adult Pkd2 +/LacZ and WT mice. Due to the lack of an obvious renal phenotype in heterozygous mice, it is likely that in conventional ADPKD knock out mouse models severe cardiac problems appear too late to be identified during the reduced lifespan of the animals. © 2006 Elsevier Ireland Ltd. All rights reserved. Keywords: Polycystin-2; Pkd2; APKD; Cystic kidney disease; Ultrasound; Echocardiography 1. Introduction Autosomal dominant polycystic kidney disease (ADPKD) is a frequent hereditary renal disorder with an overall incidence of 1 to 2.5 in 1000 [1]. It is characterized by the formation of multiple, fluid-filled cysts not only in both kidneys but also in other organs [2]. About 50% of PKD patients develop end-stage renal failure (ESRF) by late middle age [3], accounting for 5–10% of patients requiring haemodialysis world wide [4]. However, the course of the disease frequently is complicated by a multiplicity of extra renal manifestations: even in patients with normal renal function, nearly 70% suffer from hypertension; many patients develop left ventricular hypertrophy and 20% suffer from International Journal of Cardiology 120 (2007) 158 – 166 www.elsevier.com/locate/ijcard ⁎ Corresponding author. Tel.: +49 251 8355405; fax: +49 251 8356995. E-mail address: [email protected] (P. Pennekamp). 1 The first two authors contributed equally to this work. 0167-5273/$ - see front matter © 2006 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ijcard.2006.09.013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

logy 120 (2007) 158–166www.elsevier.com/locate/ijcard
International Journal of Cardio
Cardiovascular characterization of Pkd2+/LacZ mice, an animal model forthe autosomal dominant polycystic kidney disease type 2 (ADPKD2)
Jörg Stypmann a,b,1, Markus A. Engelen a,c,1, Stefan Orwat a, Konstantinos Bilbilis d,Markus Rothenburger e, Lars Eckardt a, Wilhelm Haverkamp a,b, Jürgen Horst d,
Bernd Dworniczak d, Petra Pennekamp d,⁎
a Department of Cardiology and Angiology, Hospital of the University of Münster, Germanyb Interdisciplinary Center for Clinical Research (IZKF), Central Project Group 4 (ZPG4a), Münster, Germany
c Department of Medical Physiology, University Medical Center Utrecht, The Netherlandsd Institut für Humangenetik, Universitätsklinikum Münster, Vesaliusweg 12, D - 48149 Münster, Germanye Department for Thoracic and Cardiovascular Surgery, Hospital of the University of Münster, Germany
Received 21 February 2006; received in revised form 27 August 2006; accepted 20 September 2006Available online 19 December 2006
Abstract
Background: Autosomal dominant polycystic kidney disease (ADPKD) is caused by mutations in PKD1 or PKD2. Patients with ADPKDhave an increased incidence of cardiac valve abnormalities and left ventricular hypertrophy. Systematic analyses of cardiovascularinvolvement have so far been performed only on genetically unclassified patients or on ADPKD1 patients, but not on genetically definedADPKD2 patients. Even existing Pkd1 or Pkd2 mouse models were not thoroughly analyzed in this respect. Therefore, the aim of this projectwas the noninvasive functional cardiovascular characterization of a mouse model for ADPKD2.Methods: Pkd2+/LacZ mice and wildtype controls were classified into 8 groups with respect to gender, age and genotype. In addition, twosubgroups of female mice were analyzed for cardiac function before and during advanced pregnancy. Doppler-echocardiographic as well ashistological studies were performed.Results: Doppler-echocardiography did not reveal significant cardiovascular changes. Heart rate and left ventricular (LV) length, LV mass,LV enddiastolic and LV endsystolic diameters did not differ significantly among the various groups when comparing wildtype and knockoutmice. There were no significant differences except for a tendency towards higher maximal early and late flow velocities over the mitral valvein old wildtype mice.Conclusions: Non-invasive phenotyping using ultrasound did not reveal significant cardiovascular difference between adult Pkd2+/LacZ andWT mice. Due to the lack of an obvious renal phenotype in heterozygous mice, it is likely that in conventional ADPKD knock out mousemodels severe cardiac problems appear too late to be identified during the reduced lifespan of the animals.© 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: Polycystin-2; Pkd2; APKD; Cystic kidney disease; Ultrasound; Echocardiography
1. Introduction
Autosomal dominant polycystic kidney disease (ADPKD)is a frequent hereditary renal disorder with an overallincidence of 1 to 2.5 in 1000 [1]. It is characterized by the
⁎ Corresponding author. Tel.: +49 251 8355405; fax: +49 251 8356995.E-mail address: [email protected] (P. Pennekamp).
1 The first two authors contributed equally to this work.
0167-5273/$ - see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijcard.2006.09.013
formation of multiple, fluid-filled cysts not only in bothkidneys but also in other organs [2]. About 50% of PKDpatients develop end-stage renal failure (ESRF) by latemiddle age [3], accounting for 5–10% of patients requiringhaemodialysis world wide [4]. However, the course of thedisease frequently is complicated by a multiplicity of extrarenal manifestations: even in patients with normal renalfunction, nearly 70% suffer from hypertension; many patientsdevelop left ventricular hypertrophy and 20% suffer from

159J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166
intracranial aneurysm. Furthermore, patients can be affectedby cardiac valvular abnormalities, colonic diverticuli, andinguinal hernia. In the meantime, ADPKD is regarded as amultisystemic disorder [5].
So far, two genes have been identified which are mutatedin the majority (99%) of ADPKD cases: PKD1, encodingpolycystin-1 (PC1), an integral membrane-spanning glyco-protein suggested to function as epithelial cell membranemechanoreceptor, sensing morphogenetic cues in the extra-cellular environment, and PKD2, encoding polycystin-2(PC2), a membrane-spanning protein as well functioning as aCa2+ permeable cation channel [6–8].
Both polycystins are likely to function in a commonpathway because mutations in either gene cause strikinglysimilar phenotypes. Although the disease displays inter- andintrafamilial phenotypic heterogeneity [9], detailed studiesrevealed that in the long run ADPKD has a milder course infamilies linked to PKD2. These patients suffer later fromsymptoms, exhibit a smaller number of cysts at the time ofdiagnosis, and chronic renal failure threaten PKD2 patientslater in life as compared to PKD1 patients [10].
Orthologues of the human PKD1 and PKD2 genes existin the mouse genome, and several different knockout micehave been created. Heterozygous mice appear normal butdevelop single cysts in the kidney or liver late in life andhave a reduced overall lifespan [11]. Homozygous nullmutant mice die in utero with massively enlarged cystickidneys, pancreatic ductal cysts and pulmonary hypoplasiaand often exhibit edema, vascular leaks, and rupture of bloodvessels suggesting that the polycystins are required for thestructural integrity of blood vessels [12,13]. In addition mostof the homozygous embryos display multiple cardiacabnormalities including cardiac septation defects, doubleoutlet right ventricle and pericardial effusions [11,14,15].Severe cardiovascular abnormalities in homozygous mutantPKD1 or PKD2 knockout mouse embryos might be due toloss of polycystin function in the heart tissue which normallyshows a high expression of both genes (Figs. 2 and 3; [14]).Moreover, patients frequently develop left ventricularhypertrophy before developing hypertension [16]. Therefore,the cardiovascular complications in ADPKD patients begunto be recognized as a primary defect due to the loss of PC1and/or PC2 function in cardiovascular organs and not solelyas a secondary defect due to decreasing renal function.
However, owing to the similarity of the overall clinicalphenotypes of ADPKD1 and 2 patients, it is assumed thatthe cardiovascular phenotypes in ADPKD1 and ADPKD 2patients are virtually identical [17]. But, systematic analysesof the cardiovascular involvement have so far beenperformed only on genetically unclassified patients or onADPKD1 patients, but not on genetically well defined panelsof ADPKD2 patients. Even existing Pkd1 or Pkd2 mousemodels were not thoroughly analyzed in that respect. There-fore, in the present study the cardiovascular performance ofthe Pkd2+/LacZ mouse as a mouse model for the ADPKD2was investigated in more detail using noninvasive Doppler-
echocardiography of heterozygous and wildtype mice ofdifferent gender and age. In addition, two subgroups of micebefore and during advanced pregnancy were examined toclarify whether pregnancy deteriorates the heart performancein this mouse model of ADPKD2.
2. Methods
2.1. Generation and maintenance of Pkd2-deficient mice
Pkd2-deficient mice have been generated by gene targetinginmouse embryonic stem cells as described previously [15]. Inthis mouse line, we replaced Pkd2 exon 1 and part of intron 1by LacZ as a reporter gene. LacZ was fused to the originalPkd2 ATG start codon enabling to monitor LacZ expressionunder the control of the Pkd2 promotor (Mouse GenomeInformatics: allele Pkd2tm1Dwo (http://www.informatics.jax.org). In this report, heterozygous Pkd2 mutated mice arenamed Pkd2+/LacZ and homozygous Pkd2 mutated mice arenamed Pkd2LacZ/LacZ). For the present study, Pkd2+/LacZ miceon a mixed C57/BL6 and 129/Sv genetic background wereused. Mice were conventionally housed in a controlled envi-ronment at a temperature of 21 °C±1 and a 12 h day/nightcycle. Mice were kept in macrolon cages and had access tostandard food pellets and tap water ad libidum. All experi-mental procedures had been approved by the local governmentauthorities and confirm to the NIH Guide for the Care and Useof Laboratory Animals.
2.2. Expression analysis by LacZ staining
Whole embryos were fixed in 4% PFA/PBS+2 mMMgCl2 for 5–30 min at room temperature and washed 3times in 1×PBS, 0.01% sodium deoxycholate, and 0.02%Nonidet P-40. LacZ staining was performed by incubation ofsamples with 5 mM K3Fe(CN)6, 5 mM K4Fe(CN)6 3H2O,2 mM MgCl2, 0.01% sodium deoxycholate, 0.02% NonidetP-40, and 1 mg/ml X-Gal (4-chloro-5-bromo-3-indolyl-β-D-galactopyranoside) in 1×PBS (pH 7.4–8.0) at 30 °C. Afterstaining, samples were washed in 1×PBS, postfixed in 4%PFA, dehydrated in methanol, and embedded in Historesin(Leica Microsystems, Bensheim, Germany). Stained embry-os were sectioned at 4 μm on a MICROM HM 355 micro-tome (MICROM, Walldorf, Germany) and staining wasvisualized under darkfield illumination by use of a ZeissAxioskop microscope. Adjacent sections were counter-stained with methylen blue/azur II and visualized underbright field illumination. Adult organs were frozen andsectioned on a MICROM HM 500 O microtome (MICROM,Walldorf, Germany) at 20 μm for X-Gal staining asdescribed above and counterstained with eosin.
2.3. Grouping of mice for analysis
Pkd2+/LacZ mice and their wildtype littermates were classi-fied into 10 groups with respect to gender, age and genotype as

Table 1Basic characteristics of all Doppler-echocardiographically examined mice
Group I II Ib IIb III IV V VI VII VIII
Age 102±33 days 483±69 days
Gender Female Female/pregnant Male Female Male
Genotype Pkd2+/LacZ WT Pkd2+/LacZ WT Pkd2+/LacZ WT Pkd2+/LacZ WT Pkd2+/LacZ WTNumber of animals 21 23 7 5 6 11 6 6 6 6Body weight [g] 22.1 22.3 33.79 33.04 28.6 30.0 38.3 38.6 40.9 41.0Heart rate [bpm] 335±58 322±70 387±145 356±38 333±74 353±70 346±33 312±95 357±48 323±46
160 J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166
shown in Tables 1 and 2. In addition, after the first examinationseveral female mice out of groups I and II were mated toanalyze cardiac performance during pregnancy betweenembryonic day (E) 15 and E17 (subgroups Ib and IIb). Theage of the young animals (groups I–IV) varied between 2 and5 months (mean age 102±33 days), the age of the old animals(groups V–VIII) varied between 14 and 16 months (mean age483±69 days).
2.4. Doppler-echocardiography
Doppler-echocardiographic examination was performedas previously described in detail [18–20]. The investigator
Table 2Doppler-echocardigraphic data of left ventricular performance with subgroup anal
Group I II Ib IIb II
Age 102±33 days
Gender Female Female/pregnant M
Genotype Pkd2+/LacZ WT Pkd2+/LacZ WT PkLA [mm] 1.99±0.31 1.96±0.38 2.14±0.33 2.02±0.37 1.LVAWd [mm] 0.82±0.07 0.85±0.11 0.88±0.04 0.82±0.06 0.LVEDd [mm] 4.29±0.91 4.28±1.13 4.00±0.83 3.75±0.63 3.LVESd [mm] 2.76±0.71 2.68±0.68 2.35±0.65 2.20±0.31 1.LVPWd [mm] 0.88±0.09 0.94±0.10 0.66±0.05 0.64±0.07 0.LV-length [mm] 5.97±0.45 6.00±0.76 6.67±0.66 6.53±0.48 6.LV-FS [%] 35.08±6.80 37.04±5.96 42.05±
4.5640.67±5.97
456.
LV-EF [%] 57±9 60±8 66±6 64±7 69Mass of LV [mg] 92±25 100±33 100±19 91±9 74LV mass index [mg/g] 4.28±1.32 4.50±1.63 2.98±0.51 2.77±0.31 2.LV-CO [ml/min] 10±2 11±3 18±4 17±1 14Cardiac index [ml/min/g] 0.47±0.13 0.50±0.16 0.53±0.13 0.53±0.03 0.Ao Vmax [cm/s] 59.7±6.6 60.8±6.0 68.30±7.2 68.94±7.2 77Ao PGmax [mmHg] 1.46±0.33 1.49±0.30 1.89±0.40 1.93±0.40 2.Ao MPG [mmHg] 0.779±
0.1840.793±0.176
0.96±0.750
0.75±0.340
1.0.
MV E-wave [cm/s] 42.7±8.8 47.2±10.3 48.14±6.8 55.94±6.5 58MVA-wave [cm/s] 21.3±5.2 23.6±8.0 30.46±
16.629.04±7.76
25
Ratio of E/A-Wave 2.08±0.53 2.12±0.57 1.93±0.68 2.01±0.33 2.MV PGmean [mmHg] 0.271±
0.0930.300±0.146
0.33±0.080
0.40±0.140
0.0.
Ao PGmax: aortic maximum pressure gradient [mmHg]; Ao MPG: mean aortic presLV anterior wall enddiastolic diameter; LVPWd: LV posterior wall enddiastolic dienddiastolic diameter; LV-EF: LV-ejection fraction; LVESD: left ventricular endechocardiographic cardiac output via left ventricular outflow tract; MVA-Wave: aPGmean: Mean pressure gradient of mitral valve. Significances pb0.05: a=V/VI,
was blinded with regard to the genotype of the mice. Afterinduction of light anesthesia with a combination of 50 mg/kgketamin (Ketavet®, Pfizer Pharma GmbH, Karlsruhe,Germany) and 5 mg/kg xylazine (Rompun®, BayerVital,Leverkusen, Germany), the chests of the mice were pre-cordially shaved. The mice were secured in a supine positionto a warm waterbed heated to 38 °C and angled 45° to theleft. One lead ECG was used to monitor heart rate. Trans-thoracic echocardiography was performed using a commer-cially available digital cardiac ultrasound platform equippedwith either a 6- to 12-MHz short focal length-phased arraytransducer equipped with an acoustic stand-off or a 15-MHzlinear-array transducer (Sonos 5500, B1-software package,
yses
I IV V VI VII VIII
483±69 days
ale Female Male
d2+/LacZ WT Pkd2+/LacZ WT Pkd2+/LacZ WT90±0.14 2.02±0.30 1.84±0.29 1.80±0.09 2.00±0.39 2.12±0.2277±0.08 0.79±0.09 0.91±0.10 0.94±0.11 0.94±0.06d 1.01±0.13e
43±0.29 4.00±0.85 2.85±0.25b 3.05±0.14 3.10±0.26 3.26±0.3489±0.31 2.36±0.63 1.92±0.18b 2.08±0.04 1.90±0.15 1.84±0.2184±0.10 0.86±0.11 1.05±0.14b 1.02±0.08a 1.02±0.07 0.97±0.1146±0.79 6.57±0.28 6.01±0.45 5.90±0.63 6.27±0.61 6.09±0.61.04±75
41.50±6.79
32.39±5.88
31.72±2.03
38.38±4.57
43.38±4.39
±8 65±8 54±8 53±3 62±6 68±5±13 90±19 78±17 81±14 86±8 91±2260±0.34 2.99±0.55 1.97±0.38b 2.12±0.39c 2.14±0.37 2.42±0.78±3 15±4 17±6b 14±3 16±2 16±349±0.12 0.50±0.14 0.42±0.10 0.35±0.08 0.41±0.13 0.43±0.14.1±13.5 75.0±8.9 58.6±5.8 62.0±3.8 63.6±1.6 75.8±9.144±0.82 2.28±0.57 1.39±0.28 1.54±0.19 1.62±0.09 2.33±0.53239±390
1.230±0.315
0.736±0.180
0.837±0.097
0.841±0.076
1.123±0.285
.7±11.8 62.8±14.1 41.1±4.4 39.7±7.6 54.5±13.3 57.3±4.5
.8±5.5 30.7±8.9 20.6±3.5 20.8±4.9 18.1±6.3 24.0±3.8
33±0.51 2.09±0.35 2.05±0.47 1.95±0.28 3.21±1.09 2.43±0.35372±078
0.472±0.147
0.295±0.123
0.215±0.070
0.375±0.214
0.364±0.088
sure gradient [mmHg]; Ao Vmax: aorta velocity maximum [cm/s]; LVAWD:ameter; LA: left atrial diameter; LV: left ventricle; LVEDD: left ventricularsystolic diameter; LV-FS: LV-fractional shortening; LVOT-CO: Doppler-trial inflow of mitral valve; MV E-Wave: early inflow of mitral valve; MVb=I/V, c= II/VI, d= III/VII, e= IV/VIII.

Fig. 1. Representative echocardiographic images. Parasternal long axis view (A), M-mode (B), Doppler flow signals of the mitral inflow with E- and A-wave (C)and Doppler flow over the aortic valve (D). Velocity of the Doppler flow signals shown on the right side of the images are given in m/s. Exemplary image of anaortic insufficiency (E). LV=left ventricle, LA=left atrium, Ao=aorta.
161J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166
Philips, The Netherlands). A smooth layer of 1.5–2 cm thickcentrifuged ultrasound gel was placed on the chest of themice and the probe was gently dipped into this layer of gelavoiding any pressure on the thorax to prevent thorax defor-mation or reflex bradycardia. Parasternal long-axis andshort-axis views were obtained at a frame rate of 300 persecond. The variable depth of the zoom box was set at 2–4 cm. M-mode and Doppler recordings were performed at asweep speed of 150 mm/s. M-Mode data of the LV anterior(LVAWd) and posterior wall thickness (LVPWd) at end-diastole as well as end-diastolic and end-systolic dimensionsof the left ventricle were acquired in the parasternal long axisview following the leading edge to leading edge method [20]of three consecutive cycles. Percentage of fractional shorten-ing (FS) as an index of LV systolic function was calculatedusing the equation [18,20–22]
FSð%Þ ¼ LVEDD−LVESDLVEDD
� �� �d100:
Echocardiographic LVmass was calculated using the area-length method as previously described [22–24] and correctedfor bodyweight by calculating the LV mass index [18].
Pulsed wave Doppler signals were obtained in a modifiedapical view by placing the sample volume parallel to the flowinto LVoutflow tract (LVOT) for systolic outflow of the leftventricle as well as apical to the mitral valve within leftventricle for diastolic inflow. The left atrium was checked formitral regurgitation by pulsed wave Doppler. In addition,mitral and aortic valves were examined for regurgitation bycolor flow Doppler. Cardiac output was calculated using
heart rate, velocity time integral of the Doppler-signals in theLVoutflow tract and the end-diastolic diameter of the LVOT[21].
3. Histological analyses
For light microscopy, organs were fixed in 4% parafor-maldehyde dissolved in 1×PBS (4% PFA/PBS) solution andembedded in paraffin. Sections of 6 μm were stained withmethylen blue/azur II and analyzed by light microscopy(Axioskop, Zeiss, Germany).
4. Statistical analyses
Values were calculated with SPSS 11 statistical softwareand expressed as means and their respective standard errorsor standard deviations. Groups I/II, I/Ib, II/IIb, Ib/IIb, III/IV,V/VI, VII/VIII, I/V, II/VI, III/VII and IV/VIII were com-pared using the two-tailed Student's t test and the Wilcoxonrank sum test. A pb0.05 was considered to indicate statisti-cally significant differences between the groups investigated.
5. Results
85 mice were included in this study including 12 femalemice which were examined before and during pregnancy. Asexpected, the body weight of female non-pregnant mice(25.9±8.4 g) was significant lower than the body weight ofmale mice (33.8±6.8 g) (pb0.0001) and body weight in-creased with age in both genders. No significant differencesof body weight or heart rate have been observed between

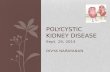
Fig. 3. Pkd2 expression and abnormal cardiovascular development in Pkd2LacZ/LacZ embryos and a representative kidney section of a male Pkd2+/LacZ mouseat the age of 16 month. In this mouse line, LacZ is fused to the Pkd2 ATG start codon enabling to monitor LacZ expression under the control of the Pkd2 promotorusing whole mount X-Gal staining. Viewed under darkfield illumination, blue X-Gal precipitates appear pink. Expression to different extend was detectable inall structures of the heart with the highest expression in the outflow tracts, especially the endocardial cushions and valve leaflets, and lower levels inthe myocardium. Mutant embryos showed cardiovascular abnormalities to different extend including disorganization of the myocardial wall and ventricularseptum, dysplastic endocardial cushions, double outlet right ventricle (DORV) and single chambered ventricle. Frontal (A–F) and sagital sections of WT (A),Pkd2+/LacZ (B, G) and Pkd2LacZ/LacZ (C–F, H) embryonic hearts and kidney section of a male Pkd2+/LacZ mouse at the age of 16 month (I). A, B: newborn; C, E–H: E16.5; D: E17.5; I: E15.5; A–F: X-Gal staining viewed under dark field illumination; G–I: bright field illumination; G, H, I: methylen blue/azur II staining.
Fig. 2. Pkd2 expression in the heart of adult Pkd2+/LacZ mice. Pkd2 expression is reduced in the cardiac region of adult mice, but still can be detected in the cardiacvalves and the septum membranaceum as demonstrated by X-Gal histochemistry (blue dots in A I, A II, B I and B II). Frontal sections of a heart isolated from aPkd2+/LacZ mouse (A and B) and higher magnifications of the aortic valve (A I), tricuspid valve (A II), mitral valve (B I) and septum membranaceum (B II)viewed under bright field illumination.
162 J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166

163J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166
Pkd2+/LacZ and wildtype mice of the same age and gender(Table 1). Heart rate did not differ significantly between allgroups. The anesthetic regimen did not produce significant,prolonged or temporally variable changes in heart rate duringthe examination.
Adequate Doppler-echocardigraphic measurements couldbe obtained in all mice without any problems within less than20 min (mean less than 15 min).
Representative images are shown in Fig. 1. Doppler-echocardiographic measurements and calculated values areshown in Table 2.
Overall, there were not much striking significant differ-ences between the compared groups. Color flow Dopplerrevealed insufficiencies of the aortic valve in one young femalePkd2+/LacZ mouse (group I) and in one young male wildtypemouse (group IV). LVEDD and LVEDS were significantlydecreased in the old female Pkd2+/LacZ mice as compared withyoung heterozygous knockout mice. LVPWd and COincreased significantly with age in the female Pkd2+/LacZ
mice. LVAWd was significantly increased as well in the oldmale Pkd2+/LacZ mice as in the old wildtypes as comparedwithyoungermice of the respective genotype and gender. AoVmaxdecreased significantly with age in the Pkd2+/LacZ mice. FS, E-wave andA-wavewere higher inmalemice independent of thegenotype when compared to females of the same age. Bothgender and genotypes showed a tendency to an increase incardiac output at older ages, but this trend cleared out aftercorrection for body-weight. The observed time pattern of sono-morphometric indices during pregnancy and changes infunctional Doppler-echocardiographic measurements in theexamined mice did not show significant differences betweenPkd2+/LacZ and wildtype mice.
In summary, there were no significant differences be-tween age-matched Pkd2 heterozygous mice and wildtypecontrols.
As previously shown, embryos lacking polycystin-2(Pkd2LacZ/LacZ) exhibited severe defects in cardiac morpho-genesis including ventricular septal defects (VSD), abnormalformation of cardiac valves and transposition of the greatvessels (TGA) [15,11]. During mouse embryogenesis, poly-cystin-2 is, similar to polycystin-1 [14], highly expressed in theconotruncus, especially in the endocardial cushion, structuresthat give rise to the affected heart valves and the membranousventricular septum. In adult animals, expression of polycystin-2 is decreased in the cardiac region but still can be detected inthe cardiac valves and the septum membranaceum (Fig. 2). Inthe kidney, only few cysts can be detected in adult hetero-zygous knockout mice older than one year (Fig. 3). Asexpected, renal function in these mice is not affected ([11] andunpublished own data).
6. Discussion
In recent years, autosomal dominant polycystic kidneydisease (ADPKD) became increasingly recognized as asystemic disorder and on the cellular level this seems to
be reasonable due to the wide spread expression of bothgenes. Although ADPKD patients suffer from manyextrarenal manifestations [2], cardiovascular problems arethe most severe side effects and several studies have beenconducted to characterize the cardiac involvement inADPKD patients. Cardiovascular problems seem to be acontinuous process starting early during the course of thedisease and it has to be pointed out that they are still amajor cause of morbidity and mortality in patients withADPKD [25,26].
Hypertension and left ventricular hypertrophy is commonand associated with faster progression to end stage renaldisease [16,25,27]. Especially hypertension develops in themajority of patients before any decrease in renal function canbe determined [27]. It has been proposed that formation andexpansion of renal cysts activate the renin–angiotensin–aldosterone system (RAAS) by which development ofhypertension is triggered [28]; consistent with this hypoth-esis activation of RAAS can be verified well before onset ofhypertension or any other clinical finding in ADPKDpatients [29,30]. Recent studies showed that patients benefitfrom lowering the mean arterial pressure and by use ofangiotensin-converting enzyme inhibitors which significant-ly slow down the decrease of renal function [31].
Beside hypertension and left ventricular hypertrophy, theprevalence of mitral-valve prolapse, mitral regurgitation,aortic insufficiency, tricuspid incompetence, and tricuspid-valve prolapse is increased [32]. The same holds true for theleft ventricular mass (LVM) index and it was clearly shownthat left ventricular dysfunction increases if ADPKD patientsbecome hypertensive [33]. The same study revealed that themajority of valvular abnormalities occurred in dialysispatients which were generally related to annular calcificationof the mitral or aortic valve.
However, despite the feasibility of subdividing ADPKDpatients into genetically defined groups (ADPKD type Icaused by mutations in PKD1 versus ADPKD type 2 causedby mutation in PKD2) up to now only a single study has beenpublished comparing a genetically classified cohort ofADPKD type 1 patients to unaffected family members andhealthy controls [34]. In addition, although Pkd1 and Pkd2mouse models are available, there are to the best of ourknowledge no published data concerning the questionwhether cardiac performance is impacted in these animals.But, embryos lacking polycystin-2 and some of the mousemutants for polycystin-1 [11,14,15] exhibit severe defects incardiac morphogenesis including ventricular septal defects(VSD), abnormal formation of cardiac valves and transpo-sition of the great vessels (TGA). Furthermore, during mouseembryogenesis, polycystin-2 is highly expressed in theconotruncus, especially the endocardial cushions, structuresthat give rise to the affected heart valves and the mem-branous ventricular septum. Later in development, expres-sion of the polycystins can still be detected in the cardiacvalves and great vessels. The prominent cardiac expressionpatterns for both polycystins suggest a relevant function of

164 J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166
both proteins not only during development but in additionfor maintenance of cardiac valves during adulthood.
These findings let us assume that Pkd knockout mice canserve as model to analyze cardiac involvement in ADPKD inmore detail. As initial step we therefore performed a non-invasive analysis of the cardiac performance of heterozygousmice of different gender and age using Doppler-echocardiog-raphy. In addition, two subgroups of femalemicewere analyzedfor cardiac function before and during advanced pregnancy.
Our echocardiographic data correspond very well withpreviously published values obtained in similar analysesusing C57/Bl6 mice [24,35]. Despite the assumed functionof the polycystins during development of cardiac structureand during adulthood, we did not detect significantpathological cardiovascular changes neither in young norin older Pkd2+/LacZ mice of either gender or during preg-nancy. Particularly, there were hardly any differences inrespect to wall thickness, LV mass and occurrence ofvalvular insufficiencies. The significant change in LV massindex of the young versus the old female mice is due tochanges of the body-weight during aging. If Pkd2+/LacZ micehad developed arterial hypertension, we would expectsignificant differences in left ventricular mass due todifferent load, which was not the case.
These surprising findings might be due to a couple ofdifferent reasons: The course of the disease of ADPKD1 orADPKD2 patients is in general clinically hardly to distinguish,but long term investigations uncovered that disease progres-sion is milder in ADPKD2. Exemplary, onset of end-stagerenal disease is later and ADPKD2-patients are less likely tohave hypertension, urinary-tract infection or hematuria [10]and the same might be true for cardiovascular problems.
However, following the course of the disease in humanpatients, independent whether it is caused by PKD1 or PKD2mutations, severity of most symptoms clearly progress withincreasing age of affected patients. Assumed that progressionof disease is comparable fast in humans and mice, this ageingeffect is only mimicked partially in mice. Cyst formation inkidney should serve as an example: Even though the muta-tional mechanism underlying initiation of cyst formation inADPKD remains controversial the most widely acceptedhypothesis proposes a two-hit mechanism of cyst formationto explain the focal nature of cyst development.
However, frequency of the second hit clearly depends ontime and total number of renal cells susceptible for the loss[36–38]. Indeed, cyst formation in conventionally targetedPkd1 and Pkd2 mice is only detected rarely and their numberand relative size is reduced as compared to humans [11] andresulting reduction of the renal function in these mice isobviously too low to impact cardiac function.
Nevertheless, approaching the age of 15–18 months,many Pkd2+/LacZ mice suddenly die ([11] and unpublishedown observations). Macroscopic investigations of deceasedanimals – if possible – suggest that death was either causedby ruptures of blood vessels or of large liver cysts similar towhat is described for humans [39,40,25,41,42].
However, we could not identify the reason for suddendeath in all animals investigated. Nevertheless, data formus and other groups show that haploinsufficiency of eitherPkd1 or Pkd2 is sufficient to reduce survival of mutant mice[11,43,44]. Interestingly, it has been shown that loss ofPolycystin 1 or 2 function and haploinsufficiency of eitherPkd1 or Pkd2 deteriorates the structural integrity of theblood vessel walls [13,43,44] suggesting that sudden rup-tures of these vessels might be a major cause of sudden deathin these animals.
But, if decreased survival of mice for which we could notidentify the cause of death would be caused by cardiacfailure, cardiovascular abnormalities have to develop veryrapid because in part of this study we examined a rather oldmouse population (14–16 months old) short before animalsreached the end of the average life span and did not findgross structural or functional changes explaining forthcom-ing sudden death.
If cardiac involvement in ADPKD is not only secondarybut due to loss of polycystin function in the heart tissueitself – as we hypothesize – again average life span ofPkd2+/LacZ mice seems to be too short to emerge. Thus,these changes are hardly to detect in commonly sizedcohorts of mice. Even triggering the development of car-diovascular problems by additional stress – in our case wemeasured heart performance before and during pregnancy –did not uncover pathological findings.
It is known that in human disease progression isinfluenced by the type of the germ line and somatic muta-tions and so far unknown modifier genes. Especially inanimal models it could be shown that environmental factorse.g. diet and housing conditions, could also affect diseaseprogression [45]. To exclude an influence of the environ-mental factors on disease progression, especially housing anddiet were kept constant during the complete study. Data fromthe literature and own observations suggest that in micemodifier genes play an important role in disease progression.In case of Pkd2 this indeed results in a more severe phenotypein homozygous mutant embryos on a 129/Sv genetic back-ground compared to a pure C57/BL6 genetic background(unpublished own observation) leading to an earlier prenataldeath in 129/Sv embryos. In this study, we examined F1 andN2 mice derived from backcrosses between 129/Sv (donorstrain) and C57/BL6 (recipient strain) with the F1 generationproviding especially the mice of the 14–16 month old mousepopulation. Though we cannot exclude the influence ofmodifier genes on the cardiac performance of heterozygousPkd2 mutant mice, at least in the genetically homogenous F1generation, the influence of these modifier genes should havebeen minimized if not excluded.
During the complete study environmental factors, espe-cially housing and diet, were kept constant to eliminate anypossible influence of these factors. This tightly controlledstudy enabled us to evaluate solely the influence of haplo-insufficiency of the Pkd2 mutation on to cardiac performanceand resulting data can be used as base line for future studies.

165J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166
7. Limitations
One limitation of this study is the low medium heart ratedue to the use of ketamin–xylazine–narcosis. Most availablenarcotics have an impact on cardiac function of the mouse[46,47], partly by their influence on autonomic tone, partlydue to a direct cardiodepressive effect. The normal heart rateof mice lies around 475–540 bpm [48] but heart rate isclearly depressed by most anesthetic drugs. Anesthesia byinhalation of volatile anesthetics like isoflurane or sevo-flurane has less impact on cardiac function and heart rate.Some groups have performed echo in awake mice[47,49,50], but this technique requires a lot of training ofthe animals, a second researcher and much more time.Furthermore, this technique causes a high level of stress forthe mice which again changes cardiac function and espe-cially will increase heart rate. Finally, a change of cardiacmorphology by fixing the mouse in a supine position cannotbe excluded.
8. Conclusion
In conclusion, the cardiac performance of our mousemodel for Pkd2 seems to be not affected by partial loss ofpolycystin 2 function. This diagnostic finding is likely due tothe fact that the life span of mice is too short to developcardiovascular problems. Although it could be of someinterest to analyze the cardiovascular phenotype of thedifferent Pkd1 knockout mouse models we do not expecttremendous differences compared to our result.
Acknowledgement
Parts of these data are part of the doctoral thesis of StefanOrwat. We thank Axel Bohring for helpful discussions. Thiswork was partly supported by the Interdisciplinary Center forClinical Research (IZKF) Münster, project numbers ZPG4aand BD IKF 2B 4 and by grants from the DeutscheForschungsgemeinschaft (DFG), Sonderforschungsbereich656 MoBil Münster, Germany (project C3).
Recent address of Wilhem Haverkamp: MedizinischeKlinik mit Schwerpunkt Kardiologie, Campus Virchow-Klinikum Charité – Universitätsmedizin Berlin, Augusten-burger Platz 1, D – 13353 Berlin, Germany.
References
[1] Gabow PA. Autosomal dominant polycystic kidney disease. N EnglJ Med 1993;329:332–42.
[2] Gabow PA. Autosomal dominant polycystic kidney disease—morethan a renal disease. Am J Kidney Dis 1990;16:403–13.
[3] Gabow PA, Johnson AM, Kaehny WD, et al. Factors affecting theprogression of renal disease in autosomal-dominant polycystic kidneydisease. Kidney Int 1992;41:1311–9.
[4] Wilson PD. Polycystic kidney disease. N Engl J Med 2004;350:151–64.
[5] Perrone RD. Extrarenal manifestations of ADPKD. Kidney Int1997;51:2022–36.
[6] Polycystic kidney disease: the complete structure of the PKD1 geneand its protein. The international polycystic kidney disease consortium,vol. 81. Cell; 1995. p. 289–98.
[7] Gonzalez-Perrett S, Kim K, Ibarra C, et al. Polycystin-2, the proteinmutated in autosomal dominant polycystic kidney disease (ADPKD),is a Ca2+-permeable nonselective cation channel. Proc Natl Acad SciU S A 2001;98:1182–7.
[8] Koulen P, Cai Y, Geng L, et al. Polycystin-2 is an intracellular calciumrelease channel. Nat Cell Biol 2002;4:191–7.
[9] Torra R, Darnell A, Estivill X, Botey A, Revert L. Interfamilial andintrafamilial variability of clinical expression in ADPKD. ContribNephrol 1995;115:97–101.
[10] Hateboer N, v Dijk MA, Bogdanova N, et al. Comparison ofphenotypes of polycystic kidney disease types 1 and 2. EuropeanPKD1-PKD2 Study Group. Lancet 1999;353:103–7.
[11] Wu G, Markowitz GS, Li L, et al. Cardiac defects and renal failure inmice with targeted mutations in Pkd2. Nat Genet 2000;24:75–8.
[12] Lu W, Peissel B, Babakhanlou H, et al. Perinatal lethality with kidneyand pancreas defects in mice with a targetted Pkd1 mutation. Nat Genet1997;17:179–81.
[13] Kim K, Drummond I, Ibraghimov-Beskrovnaya O, Klinger K, ArnaoutMA. Polycystin 1 is required for the structural integrity of bloodvessels. Proc Natl Acad Sci U S A 2000;97:1731–6.
[14] Boulter C, Mulroy S, Webb S, Fleming S, Brindle K, Sandford R.Cardiovascular, skeletal, and renal defects in mice with a targeteddisruption of the Pkd1 gene. Proc Natl Acad Sci U S A 2001;98:12174–9.
[15] Pennekamp P, Karcher C, Fischer A, et al. The ion channel polycystin-2 is required for left–right axis determination in mice. Curr Biol2002;12:938–43.
[16] Chapman AB, Johnson AM, Rainguet S, Hossack K, Gabow P, SchrierRW. Left ventricular hypertrophy in autosomal dominant polycystickidney disease. J Am Soc Nephrol 1997;8:1292–7.
[17] Kimberling WJ, Fain PR, Kenyon JB, Goldgar D, Sujansky E, GabowPA. Linkage heterogeneity of autosomal dominant polycystic kidneydisease. N Engl J Med 1988;319:913–8.
[18] Stypmann J, Engelen MA, Epping C, et al. Age and gender relatedreference values for transthoracic Doppler-echocardiography in theanesthetized CD1 mouse. Int J Card Imaging 2006.
[19] Petermann I, Mayer C, Stypmann J, et al. Lysosomal, cytoskeletal, andmetabolic alterations in cardiomyopathy of cathepsin L knockout mice.FASEB J 2006;20:1266–8.
[20] Stypmann J, Janssen PM, Prestle J, et al. LAMP-2 deficient mice showdepressed cardiac contractile function without significant changes incalcium handling. Basic Res Cardiol 2006;101:281–91.
[21] Strauch OF, Stypmann J, Reinheckel T. Cardiac and ocular pathologiesin a mouse model of mucopolysaccharidosis type VI. Pediatr Res2003;54:701–8.
[22] Collins KA, Korcarz CE, Shroff SG, et al. Accuracy of echocardio-graphic estimates of left ventricular mass in mice. Am J Physiol HeartCirc Physiol 2001;280:H1954–62.
[23] Ghanem A, Röll W, et al. Echocardiographic assessment of leftventricular mass in neonatal and adult mice — Accuracy of differentechocardiographic methods. Echocardiography 2006;23(10):900–7.
[24] Tiemann K, Weyer D, Djoufack PC, et al. Increasing myocardialcontraction and blood pressure in C57BL/6 mice during early postnataldevelopment. Am J Physiol Heart Circ Physiol 2003;284:H464–74.
[25] Fick GM, Johnson AM, HammondWS, Gabow PA. Causes of death inautosomal dominant polycystic kidney disease. J Am Soc Nephrol1995;5:2048–56.
[26] Perrone RD, Ruthazer R, Terrin NC. Survival after end-stage renaldisease in autosomal dominant polycystic kidney disease: contributionof extrarenal complications to mortality. Am J Kidney Dis 2001;38:777–84.
[27] Ecder T, Schrier RW. Hypertension in autosomal-dominant polycystickidney disease: early occurrence and unique aspects. J Am SocNephrol 2001;12:194–200.

166 J. Stypmann et al. / International Journal of Cardiology 120 (2007) 158–166
[28] Chapman AB, Johnson A, Gabow PA, Schrier RW. The renin–angiotensin–aldosterone system and autosomal dominant polycystickidney disease. N Engl J Med 1990;323:1091–6.
[29] Harrap SB, Davies DL, Macnicol AM, et al. Renal, cardiovascular andhormonal characteristics of young adults with autosomal dominantpolycystic kidney disease. Kidney Int 1991;40:501–8.
[30] Barrett BJ, Foley R, Morgan J, Hefferton D, Parfrey P. Differences inhormonal and renal vascular responses between normotensive patientswith autosomal dominant polycystic kidney disease and unaffectedfamily members. Kidney Int 1994;46:1118–23.
[31] Schrier RW, McFann KK, Johnson AM. Epidemiological study ofkidney survival in autosomal dominant polycystic kidney disease.Kidney Int 2003;63:678–85.
[32] Hossack KF, Leddy CL, Johnson AM, Schrier RW, Gabow PA.Echocardiographic findings in autosomal dominant polycystic kidneydisease. N Engl J Med 1988;319:907–12.
[33] Bardaji A, Martinez-Vea A, Valero A, et al. Cardiac involvement inautosomal-dominant polycystic kidney disease: a hypertensive heartdisease. Clin Nephrol 2001;56:211–20.
[34] Lumiaho A, Ikaheimo R, Miettinen R, et al. Mitral valve prolapse andmitral regurgitation are common in patients with polycystic kidneydisease type 1. Am J Kidney Dis 2001;38:1208–16.
[35] Kemi OJ, Loennechen JP, Wisloff U, Ellingsen O. Intensity-controlledtreadmill running in mice: cardiac and skeletal muscle hypertrophy.J Appl Physiol 2002;93:1301–9.
[36] Wu G, D'Agati V, Cai Y, et al. Somatic inactivation of Pkd2 results inpolycystic kidney disease. Cell 1998;93:177–88.
[37] Kondrashov AS. Direct estimates of human per nucleotide mutationrates at 20 loci causing Mendelian diseases. Human Mutat2003;21:12–27.
[38] Nachman MW, Crowell SL. Estimate of the mutation rate pernucleotide in humans. Genetics 2000;156:297–304.
[39] Carels RA, van Bommel EF. Ruptured giant liver cyst: a rare cause ofacute abdomen in a haemodialysis patient with autosomal dominantpolycystic kidney disease. Neth J Med 2002;60:363–5.
[40] Chung TK, Chen KS, Yen CL, Chen HY, Cherng WJ, Fang KM. Acuteabdomen in a haemodialysed patient with polycystic kidney disease-rupture of a massive liver cyst. Nephrol Dial Transplant 1998;13:1840–2.
[41] Adeola T, Adeleye O, Potts JL, Faulkner M, Oso A. Thoracic aorticdissection in a patient with autosomal dominant polycystic kidneydisease. J Natl Med Assoc 2001;93:282–7.
[42] Belz MM, Hughes RL, Kaehny WD, et al. Familial clustering ofruptured intracranial aneurysms in autosomal dominant polycystickidney disease. Am J Kidney Dis 2001;38:770–6.
[43] Lantinga-van Leeuwen IS, Dauwerse JG, Baelde HJ, et al. Lowering ofPkd1 expression is sufficient to cause polycystic kidney disease. HumMol Genet 2004;13:3069–77.
[44] Qian Q, Hunter LW, Li M, et al. Pkd2 haploinsufficiency altersintracellular calcium regulation in vascular smooth muscle cells. HumMol Genet 2003;12:1875–80.
[45] Peters DJ, Breuning MH. Autosomal dominant polycystic kidneydisease: modification of disease progression. Lancet 2001;358:1439–44.
[46] Roth DM, Swaney JS, Dalton ND, Gilpin EA, Ross Jr J. Impact ofanesthesia on cardiac function during echocardiography in mice. Am JPhysiol Heart Circ Physiol 2002;282:H2134–40.
[47] Yang XP, Liu YH, Rhaleb NE, Kurihara N, Kim HE, Carretero OA.Echocardiographic assessment of cardiac function in conscious andanesthetized mice. Am J Physiol 1999;277:H1967–74.
[48] Desai KH, Sato R, Schauble E, Barsh GS, Kobilka BK, Bernstein D.Cardiovascular indexes in the mouse at rest and with exercise: newtools to study models of cardiac disease. Am J Physiol 1997;272:H1053–61.
[49] Esposito G, Santana LF, Dilly K, et al. Cellular and functional defectsin a mouse model of heart failure. Am J Physiol Heart Circ Physiol2000;279:H3101–12.
[50] Semeniuk LM, Kryski AJ, Severson DL. Echocardiographic assess-ment of cardiac function in diabetic db/db and transgenic db/db-hGLUT4 mice. Am J Physiol Heart Circ Physiol 2002;283:H976–82.
Related Documents