Maysah Al-Mulla OHCM, Passmedicine Cardiology OBJECTIVES - Chest pain ACS MI Angina - Heart murmurs - HTN - Arrhythmia - DVLA - Cardiovascular diseases in pregnancy - Heart failure - Pericardial disease - Valvular disease - Rheumatic heart diseases Causes of Chest pain Condition Characteristic exam feature Myocardial infarction Cardiac-sounding pain heavy, central chest pain they may radiate to the neck and left arm nausea, sweating elderly patients and diabetics may experience no pain Risk factors for cardiovascular disease Pneumothorax History of asthma, Marfan's etc Sudden dyspnea and pleuritic chest pain Pulmonary embolism Sudden dyspnea and pleuritic chest pain Calf pain/swelling Current combined pill user, malignancy Pericarditis Sharp pain relieved by sitting forwards May be pleuritic in nature Dissecting aortic aneurysm 'Tearing' chest pain radiating through to the back Unequal upper limb blood pressure Gastro-oesophageal Burning retrosternal pain

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Maysah Al-Mulla OHCM, Passmedicine
Cardiology
OBJECTIVES
- Chest pain
ACS
MI
Angina
- Heart murmurs
- HTN
- Arrhythmia
- DVLA
- Cardiovascular diseases in pregnancy
- Heart failure
- Pericardial disease
- Valvular disease
- Rheumatic heart diseases
Causes of Chest pain
Condition Characteristic exam feature Myocardial infarction Cardiac-sounding pain
heavy, central chest pain they may radiate to the neck and left arm
nausea, sweating elderly patients and diabetics may experience no pain
Risk factors for cardiovascular disease
Pneumothorax History of asthma, Marfan's etc Sudden dyspnea and pleuritic chest pain
Pulmonary embolism Sudden dyspnea and pleuritic chest pain Calf pain/swelling Current combined pill user, malignancy
Pericarditis Sharp pain relieved by sitting forwards May be pleuritic in nature
Dissecting aortic aneurysm
'Tearing' chest pain radiating through to the back Unequal upper limb blood pressure
Gastro-oesophageal Burning retrosternal pain

Maysah Al-Mulla OHCM, Passmedicine
reflux disease Other possible symptoms include regurgitation and dysphagia
Musculoskeletal chest pain
One of the most common diagnoses made in the Emergency Department. The pain is often worse on movement or palpation.
May be precipitated by trauma or coughing
Shingles
Pain often precedes the rash
NICE guidelines on assessing a patient you suspect having a cardiac chest pain
Patients presenting with acute chest pain
Immediate management
GTN ASA 300mg. NICE do not recommend giving other antiplatelet
agents (i.e. Clopidogrel) outside of hospital Do not routinely give oxygen, only give if sats < 94%*
- People with oxygen saturation (SpO2) of less than 94% who
are not at risk of hypercapnic respiratory failure, aiming for SpO2 of 94-98%.
- People with chronic obstructive pulmonary disease who are at risk of hypercapnic respiratory failure, to achieve a target SpO2 of 88-92% until blood gas analysis is available
Perform an ECG as soon as possible but do not delay transfer to hospital. A normal ECG does not exclude ACS
Referral Current chest pain or chest pain in the last 12 hours with an abnormal ECG:
- Emergency admission Chest pain 12-72 hours ago:
- Refer to hospital the same-day for assessment Chest pain > 72 hours ago
- Perform full assessment with ECG and troponin measurement before deciding upon further action
Patients presenting with stable chest pain
Anginal Pain Constricting discomfort in the front of the chest, neck,
shoulders, jaw or arms Precipitated by physical exertion
Relieved by rest or GTN in about 5 minutes
Patients with all 3 typical angina Patients with 2/3atypical angina
Patients with 0/3Non angina chest pain

Maysah Al-Mulla OHCM, Passmedicine
Cardiovascular risk factors
Smoking hx DM
HTN Dyslipidemia
Family hx of premature CKD
Other cardiovascular diseases Estimation of risks Typical angina + risk of CAD>90%
Men older than 70 Women older than 70 with high risk and typical symptoms
No diagnostic tests Treat as known CAD
Risk of CAD 61-90% Women older than 70
Coronary angiography
Risk of CAD 30-60% Functional imaging
SPECT Stress echo MR perfusion MR for stress induced wall
motion abnormalities
Risk of CAD 10-29% CT calcium scoring
Angina pectoris
Types Causes Management (NICE 2011)
Stable with activity relieved by rest
Can be induced by cold, heavy meals or emotions
Atheroma AS, HOCM, anemia
Modify risk factors ASA+statins GTN for attacks BB or CCB CCB if alone should
be rate limiting (verapamil or diltiazin)
CCB+BB (use long
acting dihydroperidine CCB)
SEQUENCE: Increase doses of monotherapy
Add combination If can’t tolerate a combination therapy:
- Long acting nitrate
Unstable with no activity or with Decubitus
when lying flat
Variant coronary artery spasm

Maysah Al-Mulla OHCM, Passmedicine
- Ivabradine - Nicorandil - Ranolazine
If on combination, add third only if before CABG or
PCI NO BB+CCB heart
block if nitrate
tolerancetake second dose after 8 hrs
Ivabradine Act on *funny* channelsreduce HR Referral Diagnostic uncertainty
New angina of sudden onset
Recurrent angina if past MI or CABG Angina uncontrolled by drugs Unstable angina
Heart Sounds
S1 S2 S3 S4 Closure of mitral and
tricuspid valve
Closure of aortic and
pulmonary valves
Diastolic filling of the
left ventricle
Atrial contraction
against stiff ventricle
Normal is <30 yrs Causes of a loud
S1 - mitral stenosis
- left to right shunts
- short PR interval, atrial premature
beats - hyperdynamic
states
Causes of a quiet
S1 - mitral
regurgitation
Maysah Al-Mulla OHCM, Passmedicine
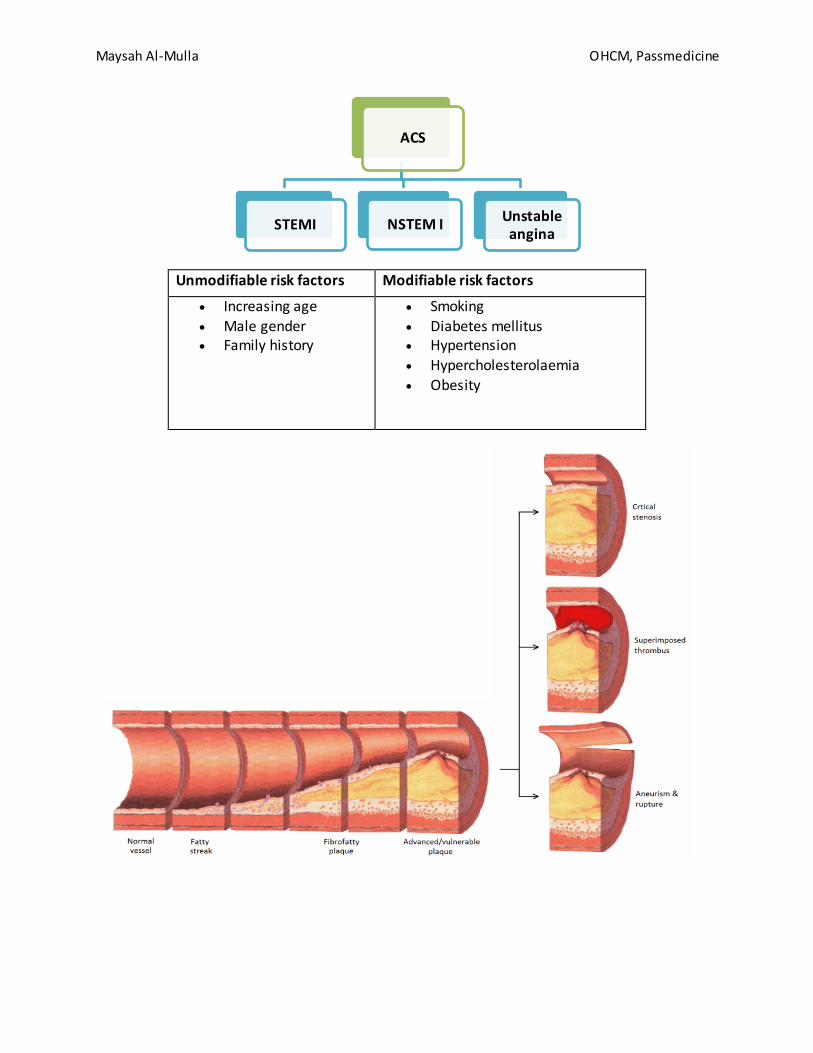
Unmodifiable risk factors Modifiable risk factors
Increasing age Male gender Family history
Smoking Diabetes mellitus Hypertension
Hypercholesterolaemia Obesity
ACS
STEMI NSTEM I Unstable angina
Maysah Al-Mulla OHCM, Passmedicine
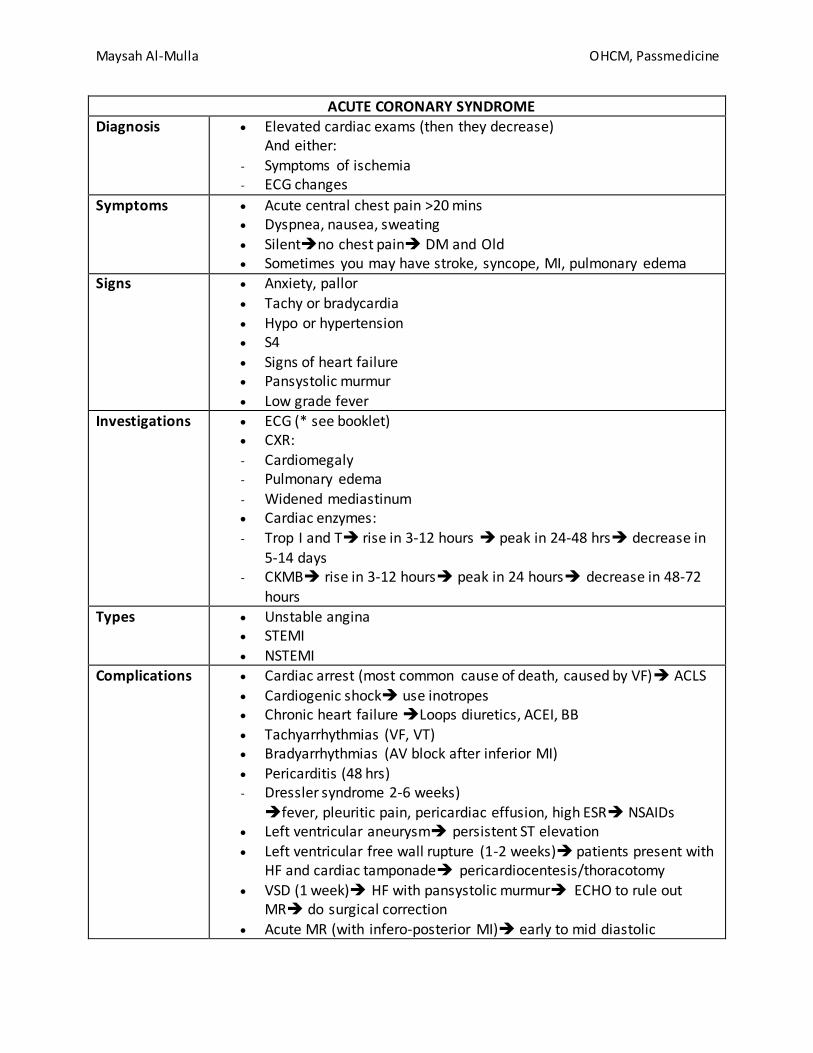
ACUTE CORONARY SYNDROME
Diagnosis Elevated cardiac exams (then they decrease) And either:
- Symptoms of ischemia - ECG changes
Symptoms Acute central chest pain >20 mins Dyspnea, nausea, sweating Silentno chest pain DM and Old Sometimes you may have stroke, syncope, MI, pulmonary edema
Signs Anxiety, pallor
Tachy or bradycardia Hypo or hypertension S4 Signs of heart failure Pansystolic murmur
Low grade fever Investigations ECG (* see booklet)
CXR: - Cardiomegaly - Pulmonary edema - Widened mediastinum Cardiac enzymes: - Trop I and T rise in 3-12 hours peak in 24-48 hrs decrease in
5-14 days - CKMB rise in 3-12 hours peak in 24 hours decrease in 48-72
hours
Types Unstable angina STEMI
NSTEMI Complications Cardiac arrest (most common cause of death, caused by VF) ACLS
Cardiogenic shock use inotropes Chronic heart failure Loops diuretics, ACEI, BB Tachyarrhythmias (VF, VT) Bradyarrhythmias (AV block after inferior MI) Pericarditis (48 hrs) - Dressler syndrome 2-6 weeks) fever, pleuritic pain, pericardiac effusion, high ESR NSAIDs
Left ventricular aneurysm persistent ST elevation Left ventricular free wall rupture (1-2 weeks) patients present with
HF and cardiac tamponade pericardiocentesis/thoracotomy
VSD (1 week) HF with pansystolic murmur ECHO to rule out MR do surgical correction
Acute MR (with infero-posterior MI) early to mid diastolic
Maysah Al-Mulla OHCM, Passmedicine
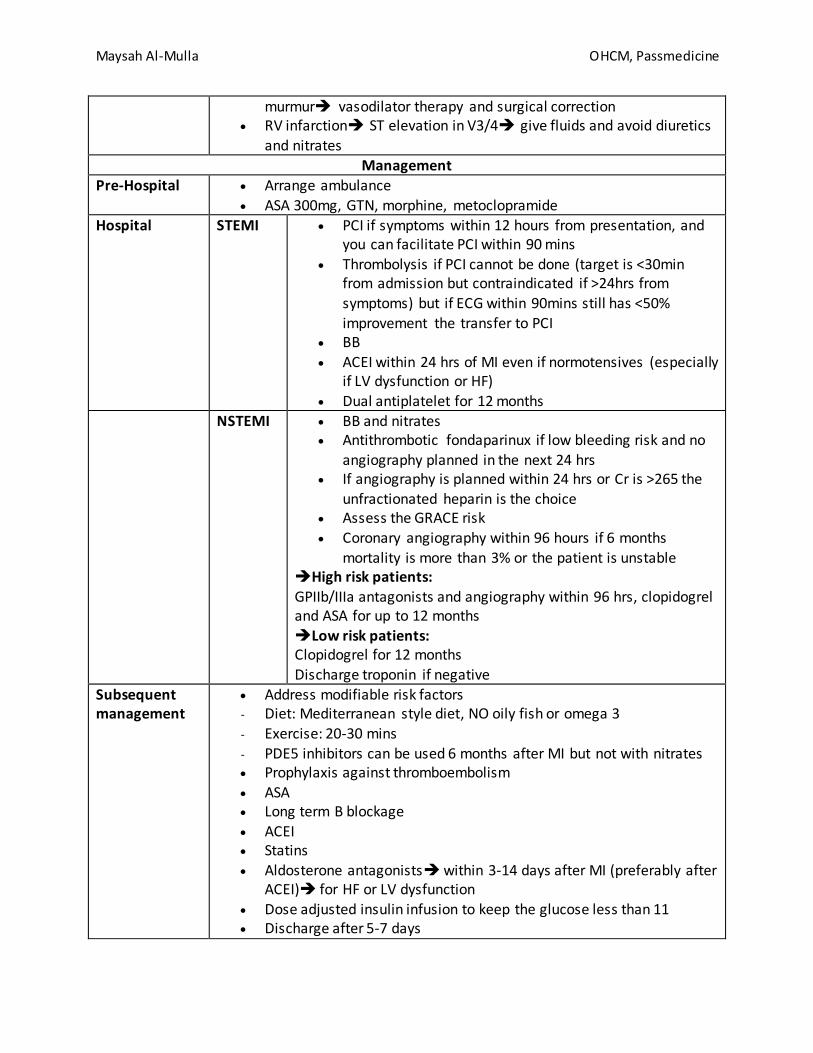
murmur vasodilator therapy and surgical correction RV infarction ST elevation in V3/4 give fluids and avoid diuretics
and nitrates
Management Pre-Hospital Arrange ambulance
ASA 300mg, GTN, morphine, metoclopramide
Hospital STEMI PCI if symptoms within 12 hours from presentation, and you can facilitate PCI within 90 mins
Thrombolysis if PCI cannot be done (target is <30min from admission but contraindicated if >24hrs from
symptoms) but if ECG within 90mins still has <50% improvement the transfer to PCI
BB ACEI within 24 hrs of MI even if normotensives (especially
if LV dysfunction or HF)
Dual antiplatelet for 12 months NSTEMI BB and nitrates
Antithrombotic fondaparinux if low bleeding risk and no angiography planned in the next 24 hrs
If angiography is planned within 24 hrs or Cr is >265 the unfractionated heparin is the choice
Assess the GRACE risk Coronary angiography within 96 hours if 6 months
mortality is more than 3% or the patient is unstable High risk patients: GPIIb/IIIa antagonists and angiography within 96 hrs, clopidogrel and ASA for up to 12 months Low risk patients: Clopidogrel for 12 months Discharge troponin if negative
Subsequent management
Address modifiable risk factors - Diet: Mediterranean style diet, NO oily fish or omega 3
- Exercise: 20-30 mins
- PDE5 inhibitors can be used 6 months after MI but not with nitrates Prophylaxis against thromboembolism
ASA Long term B blockage
ACEI Statins
Aldosterone antagonists within 3-14 days after MI (preferably after ACEI) for HF or LV dysfunction
Dose adjusted insulin infusion to keep the glucose less than 11 Discharge after 5-7 days

Maysah Al-Mulla OHCM, Passmedicine
Return to work after 2 months Avoid intercourse for 1 month Avoid travels for 2 months Don’t return to work if airtravel pilot, air traffic control, divers If heavy manual labor advise light work 5 weeks FU for symptoms
3 months FU for lipid profile Thrombolysis ECG criteria:
- ST elevation >1mm in 2 or more limb leads or >2mm in 2 or more chest leads
- LBBB - Posterior changes (deep ST depression and tall R waves in leads V1-
V3) Examples:
- Alteplase (should be followed by unfractionated heparin), Tenecteplase (preferred in out of hospital setting) (both less death but more stroke)
- Streptokinase Contraindications: - GI bleed <1 month - Non compressible punctures <24 hrs - Recent hemorrhage, trauma or surgery (including dental extraction)
<3 weeks
- coagulation and bleeding disorders - intracranial neoplasm - stroke < 3 months - aortic dissection - recent head injury - pregnancy or <1 week postpartum - severe hypertension >180/110
PCI Poor response or intolerance to medical rx Refractory angina in patients not suitable for CABG
Previous CABG Post thrombolysis in patients with severe stenosis, symptoms or
+stress test Complications:
- Restenosis - Emergency CABG
- MI - Death
CABG Indications: - Left main disease - Triple disease involving the proximal part of the LAD

Maysah Al-Mulla OHCM, Passmedicine

Maysah Al-Mulla OHCM, Passmedicine

Maysah Al-Mulla OHCM, Passmedicine
Arrhythmias (look at the 2015 UK resuscitation guidelines)
Causes Cardiac: MI
CAD LV aneurysm
Mitral valve disease
Cardiomyopathy Myocarditis, pericarditis
Non cardiac: Caffeine
Smoking/alcohol Drugs (B2 agonist, L dopa, digoxin)
Metabolic imbalance Pheochromocytoma
Presentation Palpitations, chest pain
Syncope/presyncope Hypotension Pulmonary edema
Investigations CBC, FBS
Electrolytes TFTs
ECG, 24 hrs ECHO MS, HCM
Bradycardia HR >40 with no symptoms drugs, sick sinus, hypoth - No treatment, avoid the drugs HR<40 with symptoms - 0.6-1.2mg atropine IV (up to 3) - Temporary pacing wire - Isoprenaline infusion - External cardiac pacing
Narrow complex
tachycardia (no
adenosine in asthma, give
Verapamil)
Sinus tachycardia rate control if necessary Atrial tachyarrhythmia
- AF no P waves
- Atrial flutter atrial rate 260-340, ventricular rate 150 (2;1 block) - Atrial tachycardia give digoxin specific antibody, keep K 4-5
- Multifactorial atrial tachycardia in COPD, correct the hypoxia and hypercapnia, consider verapamil or BB if HR >110
- Junctional P wave is either buried in the QRS complex or right after the QRS vagal maneuvers, adenosine, and ablation. If recurrence
give BB or amiodarone - WPW:
ablation, flecanide, satolol (DON’T GIVE IN AFIB), amiodarone

Maysah Al-Mulla OHCM, Passmedicine
Wide complex tachycardia
VT/VF Torsade de pointe (VT)
Holiday heart
syndrome
Binge drinking conduction disturbances
Ventricular tachycardia
Types Monomorphic - Caused by MI Polymorphic - Torsade de pointe (long QT) MgSO4 over 10 min 2g (can lead to VF
and death)
Long QT Causes Congenital
Jervel-Lange-Neilsen (deafness with abnormal K channel)
Romano-Ward (no deafness) Drugs
TCA Chloroquine
Amiodarone, satolol, class 1a anti arrhythmic Erythromycin, anti-histamines
Others: Electrolytes hypo Ca, hypo K, hypo Mg
MI, myocarditis Hypothermia SAH
Types Long QT 1
Exertional syncope (swimming) Long QT 1
Syncope after emotional stress, exercise or auditory stimuli Long QT3
Events occur at night or rest
Management Avoid precipitating factors
BB (NOT SATOLOL) Implantable defibrillator
Management See 2015 UK resuscitation guidelines Drugs - Amiodarone (thru central line)
- Lidocaine (careful if LV dysfunction )
- Procainamide If fails use EPS or ICD
NO VERAPAMIL IN VT

Maysah Al-Mulla OHCM, Passmedicine
Atrial fibrillation
Rate Atrial rate is 300-600 Causes Cardiac
MI HF Cardiomyopathy
Mitral valve disease Extra-Cardiac
Thyroid disease Pneumonia Caffeine Alcohol Post-op K/Mg imbalance
Symptoms Chest pain Palpitations SOB Fainting
Investigations ECG Blood tests (CBC, electro, TFTs) Echo
Classifications First detected episode Recurrent episodes if 2 or more - If the episode terminates spontaneously less than 7 days
Paroxysmal - Non limiting more than 7 days Persistent
- Permanent cant cardiovert do rate control and anticoagulation Rate control and maintenance of sinus rhythm
Rate control (Risk of bradycardia if BB+CCB (like verapamil and diltiazem)
- BB - CCB (diltiazem)
- Digoxin (not first line, only in HF) Rhythm control (<65 yrs, new onset, correctable, symptomatic, CHF)
- Satolol - Amiodarone - Flecainide
Cardioversion Acute (<48 hrs)
- Ill, unstable electrical cardioversion - Stablepharmacological or elective electrical cardioversion
- Start LMWH >48 hrs - At least 3 weeks of anticoagulation before cardioversion

Maysah Al-Mulla OHCM, Passmedicine
- TEE to exclude left atrial thrombus if excluded then heparinize and cardiovert immediately (electrical)
- If high risk of cardioversion failure, give at least 4 weeks of amiodarone or satolol prior to cardioversion
- Post cardioversion anticoagulation for at least 4 weeks
Anticoagulation CHA2DS2-VASc score (see below)
Apixaban - Prior stroke or TIA
- 75 yrs or more - HTN
- DM - Symptomatic HF
Dabigatran - Previous stroke, TIA or embolus
- LV EF <40% - NYHA class 2 or more - Age 75 or more - Age 65 or more if DM, HTN or CAD Rivaroxaban - Prior stroke or TIA - CHF - DM, HTN - 75 yr or more
Warfarin (INR 2-3)
Post-stroke Following a stroke, Warfarin is the choice of anticoagulation In acute stroke and absence of hemorrhage commence
anticoagulation after 2 weeks (unless large cerebral infarction) Atrial flutter
Manage same as Afib (it is more sensitive to cardioversion, also ablation of tricuspid isthmus is curative)
CHA2DS2-VASc SCORE for need of anticoagulation
Risk factor Points C Congestive heart failure 1
H Hypertension (or treated hypertension) 1 A2 Age >= 75 years 2
Age 65-74 years 1
D Diabetes 1
S2 Prior Stroke or TIA 2
V Vascular disease (including ischemic heart disease and peripheral arterial disease)
1
S Sex (female) 1

Maysah Al-Mulla OHCM, Passmedicine
Scoring
0 No treatment 1 Males: consider anticoagulation
Females: No treatment 2 or more
Offer anticoagulation
HASBLED SCORE (for risk of bleeding with anticoagulation)
Risk factors Score
H Hypertension, uncontrolled, systolic BP > 160 mmHg 1
A Abnormal renal function (dialysis or creatinine > 200) Or
Abnormal liver function (cirrhosis, bilirubin > 2 times normal, ALT/AST/ALP > 3 times normal
1 for any renal abnormalities
1 for any liver
abnormalities
S Stroke, history of 1 B Bleeding, history of bleeding or tendency to bleed 1
L Labile INRs (unstable/high INRs, time in therapeutic range < 60%) 1 E Elderly (> 65 years) 1
D Drugs Predisposing to Bleeding (Antiplatelet agents, NSAIDs) Or Alcohol Use (>8 drinks/week)
1 for drugs 1 for alcohol
3 or more means high risk of bleeding
General cardiac investigations and management
Pacing Indications for temporary pacing Symptomatic bradycardia Anterior MI with AV block Inferior MI if AV block Drug resistant SVT and VT
Indications for permanent pacing Complete AV block
Mobitz II Persistent AV block after anterior MI
HF Drug resistant tachyarrhythmias
CRT HF with EF <35% and QRS >120ms
ECG Look at the booklet
Exercise ECG Indication IHD
Exercise induced arrhythmias
Maysah Al-Mulla OHCM, Passmedicine
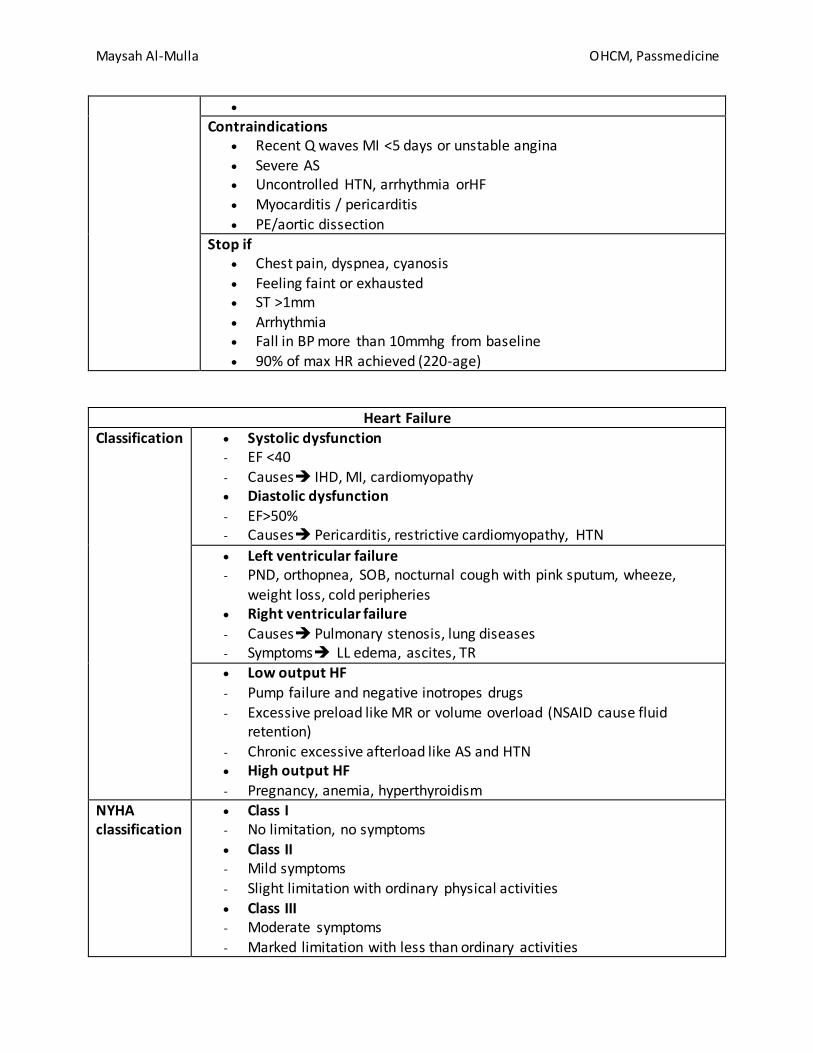
Contraindications Recent Q waves MI <5 days or unstable angina
Severe AS Uncontrolled HTN, arrhythmia orHF
Myocarditis / pericarditis
PE/aortic dissection Stop if
Chest pain, dyspnea, cyanosis Feeling faint or exhausted ST >1mm Arrhythmia Fall in BP more than 10mmhg from baseline 90% of max HR achieved (220-age)
Heart Failure
Classification Systolic dysfunction - EF <40
- Causes IHD, MI, cardiomyopathy Diastolic dysfunction
- EF>50% - Causes Pericarditis, restrictive cardiomyopathy, HTN
Left ventricular failure - PND, orthopnea, SOB, nocturnal cough with pink sputum, wheeze,
weight loss, cold peripheries Right ventricular failure - Causes Pulmonary stenosis, lung diseases - Symptoms LL edema, ascites, TR Low output HF
- Pump failure and negative inotropes drugs - Excessive preload like MR or volume overload (NSAID cause fluid
retention)
- Chronic excessive afterload like AS and HTN High output HF
- Pregnancy, anemia, hyperthyroidism NYHA classification
Class I - No limitation, no symptoms Class II - Mild symptoms
- Slight limitation with ordinary physical activities
Class III - Moderate symptoms - Marked limitation with less than ordinary activities

Maysah Al-Mulla OHCM, Passmedicine
Class IV - Severe symptoms - Unable to carry out any activities without symptoms, even at rest
Diagnosis With previous MI - ECHO in 2 weeks
With no previous MI - Measure BNP If high echo in 2 weeks if raised echo in 6 weeks
BNP levels - High >400pg/ml - Raised 100-400 - Normal <100
High BNP - LVH - Ischemia - Tachycardia - HYpoexemia - GFR<60, liver cirrhosis - COPD - Diabetes - Sepsis
Low BNP - Obesity
- Diuretics - ACEI, BB, ARBs, aldosterone antagonists
Management Acute management Sit up O2 Diamorphine 1.25-5mg IV slowly (careful in liver disease or
COPD) Furosemide 40-80mg IV slowly (more in renal failure) GTN (NOT if SBP<90) If SBP ≥100 start nitrate infusion 2-10mg/hr
If still no improvement
Further dose of furosemide 40-80mg CPAP Increase nitrate infusion If SBP< 90 treat as cardiogenic shock
Chronic management Mortality improvement (no improvements with furosemide or digoxin)
- ACEI - Spironolactone 25mg/day (risk of hyperkalemia)
- BB - Hydralazine with nitrates

Maysah Al-Mulla OHCM, Passmedicine
NICE guidelines
First line ACEI+BB Second line aldosterone antagonists OR angiotensin II receptor
blocker OR hydralazine+nitrite If no symptomatic relief CRT or Digoxin
Influenza and pneumococcal vaccine Diuretics (you can give bumetanide 1-2mg/day or metolazone 5-
20mg/day) be careful of low K caused by any conditions in combination with digoxin as
toxicity increases
Murmurs
Innocent murmurs
Soft blowing in pulmonary area or buzzing in aortic area No radiation
Vary with posture No thrills or added sounds No diastolic component Asymptomatic
Type of Murmur Conditions
Ejection systolic Aortic stenosis
Pulmonary stenosis, HOCM ASD, Fallot's
Pan-systolic Mitral regurgitation (blowing) Tricuspid regurgitation (blowing)
VSD
Late systolic Mitral valve prolapse Coarctation of aorta
Early diastolic Aortic regurgitation (blowing) Graham-Steel murmur (pulmonary regurgitation)
Mid-late diastolic Mitral stenosis (rumbling)
Austin-Flint murmur (severe aortic regurgitation) Rumbling
Continuous PDA (machinery)

Maysah Al-Mulla OHCM, Passmedicine
Hypertension
BP ranges NICE definitions Clinical BP readings persistently ≥140/90
24 BP monitoring ≥135/85 Causes Essential HTN 90%
Secondary HTN
- Renal disease GN Pyelonephritis APKD Renal artery stenosis
- Endocrine Primary hyperaldosteronism Pheochromocytoma Cushing, acromegaly
Primary adrenal hyperplasia (11 betahydroxylase def) - Others
Coarctation of the aorta Glucocorticoids, NSAIDs, OCPs
Pregnancy Classifications Stage I
- Clinic BP ≥140/90, AMBP or HBPM ≥135/85 Stage II
- Clinic BP ≥160/100, AMBP or HBPM ≥ 150/95 Severe - Systolic ≥180 or diastolic BP ≥110
Symptoms Headaches, visual disturbances, seizures Investigations U&E, urinary proteins renal disease
HbA1C coexisting DM Lipids hyperlipidemia
ECG LVH Funduscopy hypertensive retinopathy
Diagnosis Clinic measurement in both arms, repeat of >20mmhg difference, if still
repeat measurement in arm with higher BP Take 2nd reading at clinic (if >140/90), with the lowest to determine
further plan
AMBP or HBPM if BP ≥140/90
AMBP - 2 readings per hour, average of 14 readings
HBPM - For each BP recording, two consecutive measurements need to be

Maysah Al-Mulla OHCM, Passmedicine
taken, at least 1 minute apart and with the person seated - BP should be recorded twice daily, ideally in the morning and evening - BP should be recorded for at least 4 days, ideally for 7 days - Discard the measurements taken on the first day and use the average
value of all the remaining measurements
Management Lifestyle modification
Drugs (see below)
When to treat AMBP/HBPM ≥ 135/85
- <80 years, with one of the following: Target organ damage
Cardiovascular diseases Renal disease
DM 10 cardio risk is ≥20%
AMPB/HBPM ≥ 150/95 - Drug treatment regardless of age BP ≥180/110 - Immediate treatment should be considered - If there are signs of papilledema or retinal hemorrhages same day
assessment by a specialist - Referral if a pheochromocytoma is suspected
Trials in HTN
STOP-2 The 1999 Swedish Trial in Old Patients with Hypertension-2 study looked at whether older drugs (beta-blockers or thiazides) or newer drugs (ACE inhibitors or calcium channel blockers) were better at preventing fatal cardiovascular disease. Main results
old and new antihypertensive drugs were similar in prevention of cardiovascular mortality or major events
decrease in blood pressure was the most important factor in the prevention of cardiovascular events in this age group
ALLHAT The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial was
a large randomized controlled trial that was started in 1994 and reported in 2002. ALLHAT compared amlodipine, chlorthalidone (a thiazide), lisinopril and doxazosin.
Over 40,000 patients aged 55 years or older who had hypertension with one other risk factor (for example diabetes) were included in the trial.

Maysah Al-Mulla OHCM, Passmedicine
Main results
chlorthalidone outperformed lisinopril in preventing cardiovascular disease, a surprising finding which has been debated since (particularly in relation to the large number of black patients in the trial (ACE inhibitors are known to be less effective in this group)
the doxazosin arm was stopped prematurely due to a higher incidence of
heart failure 60% of patients reached the target blood pressure of 140/90 mmHg (it was
generally thought prior to the trial that blood pressure targets were more difficult to achieve)
ASCOT The 2003 Anglo-Scandinavian Cardiac Outcomes Trial - Blood Pressure Lowering Arm was a double-blinded, randomized controlled trial of around 20,000 patients with hypertension and other risk factors. Patients were randomized to either atenolol (with the addition of bendroflumethiazide if needed) or amlodipine (with the addition perindopril if needed). The primary outcome was non-fatal myocardial infarction (MI)
and fatal ischemic heart disease (IHD).
Main results
the study was stopped prematurely because of a higher death rate in the atenolol assigned group
the group receiving amlodipine-based regimes had a non-significant 10% reduction in primary outcomes (non-fatal MI plus fatal IHD) and significant
reductions in nearly all secondary cardiovascular endpoints and new-onset
diabetes

Maysah Al-Mulla OHCM, Passmedicine
Drug Mechanism of action Common side-effects
Notes
ACEI Inhibit the conversion angiotensin I to angiotensin II
Cough Angioedema Hyperkalaemia
First-line treatment in younger patients (< 55 years old)
Less effective in Afro-Caribbean patients
Must be avoided in pregnant women
Renal function must be check 2-3 weeks after starting due to the risk
of worsening renal function in patients with renovascular disease
Drug names end in '-pril' CCB Block voltage-gated
calcium channels relaxing vascular
smooth muscle and force of myocardial
Flushing
Ankle swelling Headache
First line in older patients (>= 55
years old)
Maysah Al-Mulla OHCM, Passmedicine
contraction
Thiazides Inhibit sodium absorption at the
beginning of the distal convoluted tubule
Hyponatraemia Hypokalaemia
Dehydration
Have a very weak diuretic action
ARBS Block effects of angiotensin II at the AT1 receptor
Hyperkalaemia In patients who cant tolerate ACEI (cough)
Drug names end in '-sartan'
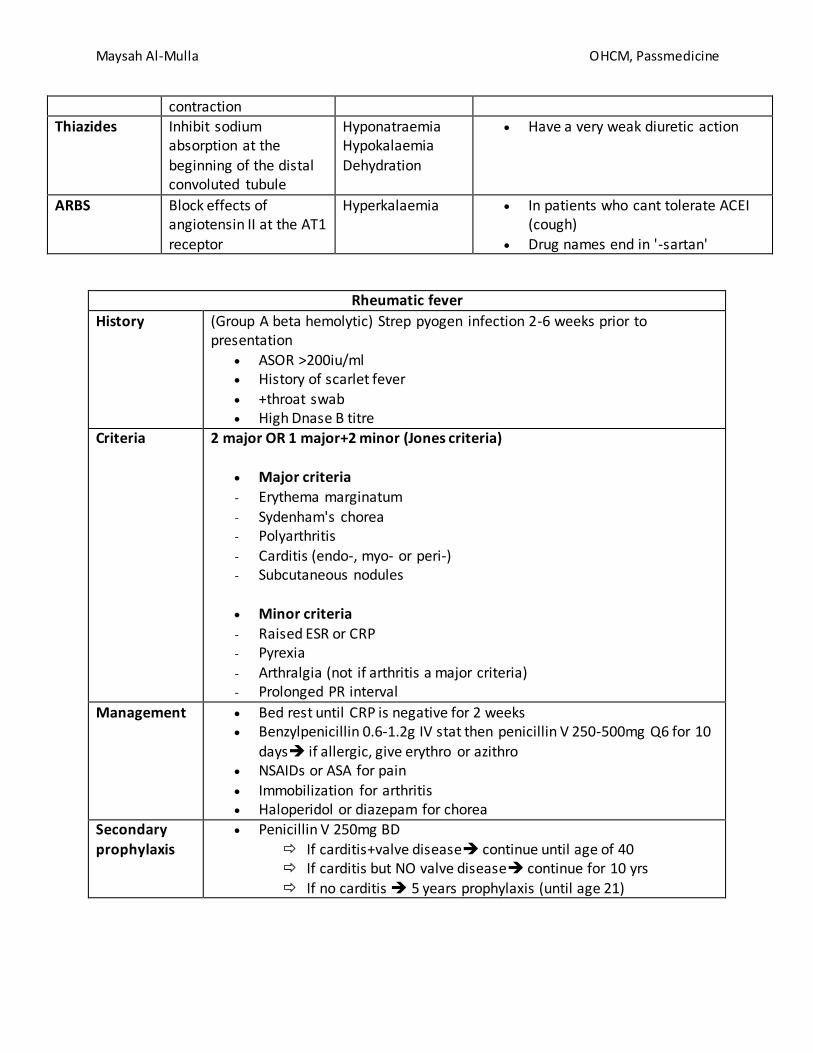
Rheumatic fever
History (Group A beta hemolytic) Strep pyogen infection 2-6 weeks prior to presentation
ASOR >200iu/ml History of scarlet fever
+throat swab High Dnase B titre
Criteria 2 major OR 1 major+2 minor (Jones criteria)
Major criteria - Erythema marginatum
- Sydenham's chorea - Polyarthritis
- Carditis (endo-, myo- or peri-) - Subcutaneous nodules
Minor criteria - Raised ESR or CRP - Pyrexia - Arthralgia (not if arthritis a major criteria) - Prolonged PR interval
Management Bed rest until CRP is negative for 2 weeks Benzylpenicillin 0.6-1.2g IV stat then penicillin V 250-500mg Q6 for 10
days if allergic, give erythro or azithro NSAIDs or ASA for pain
Immobilization for arthritis Haloperidol or diazepam for chorea
Secondary prophylaxis
Penicillin V 250mg BD If carditis+valve disease continue until age of 40 If carditis but NO valve disease continue for 10 yrs
If no carditis 5 years prophylaxis (until age 21)

Maysah Al-Mulla OHCM, Passmedicine
Valvular disease
Mitral stenosis Causes Rheumatic fever
Mucopolycassaridosis Fibroelastosis
Carcinoid
Presentation When valve area is <2cm sq Dyspnea
Fatigue Palpitations
Chest pain Hemoptysis and a picture of bronchitis
Signs Features - mid-late diastolic murmur (best heard in expiration)
- loud S1, opening snap - low volume pulse - malar flush - atrial fibrillation
Features of severe MS - length of murmur increases - opening snap becomes closer to S2
Investigations ECG - P mitrale
- RVH - RAD
Chest x-ray
- left atrial enlargement may be seen
Echocardiography - The normal cross sectional area of the mitral valve is 4-6 sq cm. A 'tight'
mitral stenosis implies a cross sectional area of < 1 sq cm
Management If in AF rate control and anticoagulation Diuretics Balloon vulvoplasty, open valvotomy, valve replacement
Mitral regurgitation
Causes Functional (LV dilatation) Annular calcification (elderly)
Rheumatic fever Infection endocarditis Mitral valve prolapse, ruptured chordea, papillary muscle dysfunction Connective tissue, cardiomyopathy
Maysah Al-Mulla OHCM, Passmedicine
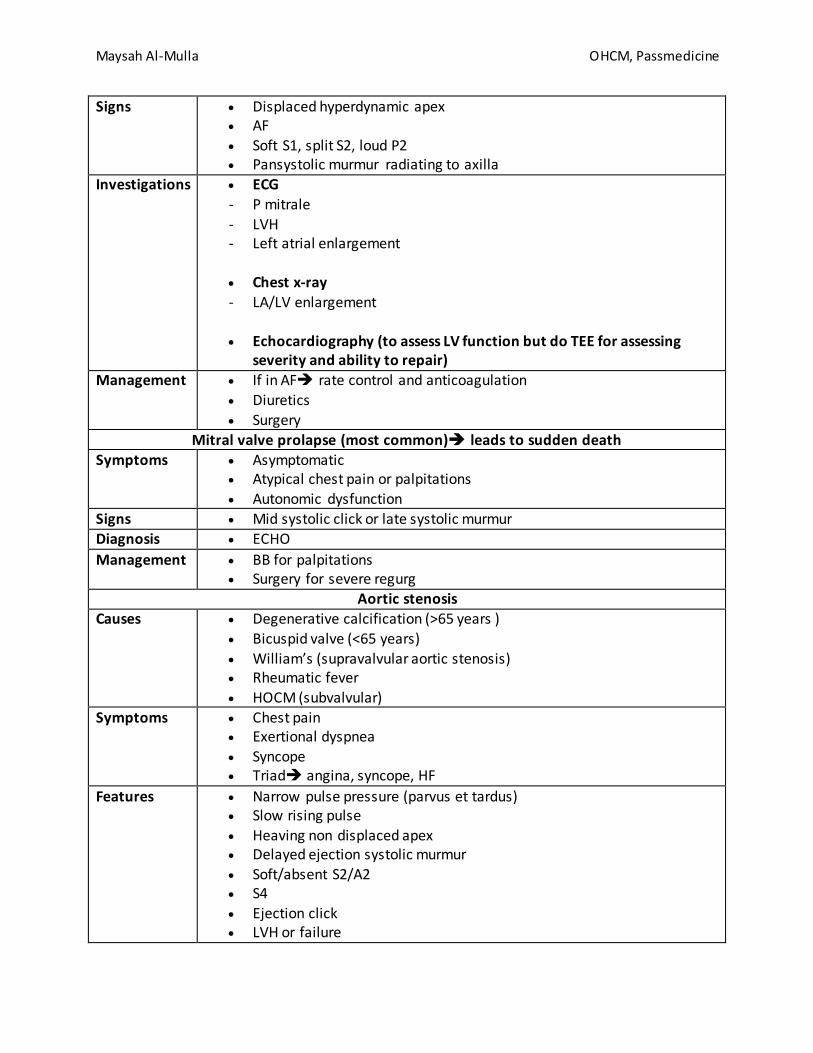
Signs Displaced hyperdynamic apex AF Soft S1, split S2, loud P2 Pansystolic murmur radiating to axilla
Investigations ECG
- P mitrale
- LVH - Left atrial enlargement
Chest x-ray
- LA/LV enlargement
Echocardiography (to assess LV function but do TEE for assessing severity and ability to repair)
Management If in AF rate control and anticoagulation
Diuretics Surgery
Mitral valve prolapse (most common) leads to sudden death Symptoms Asymptomatic
Atypical chest pain or palpitations Autonomic dysfunction
Signs Mid systolic click or late systolic murmur
Diagnosis ECHO
Management BB for palpitations Surgery for severe regurg
Aortic stenosis
Causes Degenerative calcification (>65 years ) Bicuspid valve (<65 years)
William’s (supravalvular aortic stenosis) Rheumatic fever
HOCM (subvalvular)
Symptoms Chest pain Exertional dyspnea
Syncope Triad angina, syncope, HF
Features Narrow pulse pressure (parvus et tardus) Slow rising pulse
Heaving non displaced apex Delayed ejection systolic murmur Soft/absent S2/A2 S4 Ejection click LVH or failure

Maysah Al-Mulla OHCM, Passmedicine
Investigations ECG - P mitrale - LVH - LAD - Poor R wave progression, LBBB, complete AV block
CXR - LVH
- Calcific aortic valve
ECHO (Diagnostic) - Severe stenosis if gradient ≥50 mmhg and valve area <1cm sq - Aortic jet velocity >4 or increasing by >0.3/yr more complications
Management Asymptomatic
Observe Asymptomatic with valve gradiet >50 + features of left systolic
dysfunction Surgery
Symptomatic Valve replacement
Prognosis Symptomatic with no surgery Angina and syncope 2-3 yrs Cardiac failure 1-2 yrs Moderate to severe with medical intervention 50% mortality
at 2 yrs Aortic regurgitation
Causes Valve disease - Rheumatic fever - IE - CTD - Bicuspid aortic valve Aortic root disease - Aortic dissection
- Spondylarthropathies - HTN
- Syphilis - Marfan’s, Ehler Danlos
Symptoms Exertional dyspnea Orthopnea
PND Palpitations, angina, syncope
Features Early diastolic murmur
Collapsing pulse

Maysah Al-Mulla OHCM, Passmedicine
Displaced hyperdynamic apex Wide pulse pressure Mid diastolic Austin Flint murmur (in severe AR) Corrigon sign
Carotid pulsation De Musset sign
Head nodding with each heart beat Quincke’s sign
Capillary pulsation in nail beds Duroziez’s sign
In the groin, if you press on the femoral pulse, put your stethoscope 2 cm proximal you’ll get a systolic murmur, distal you’ll get diastolic murmur
Traube’s sign Pistol shot sound over the femoral arteries
Diagnosis ECHO
Management ACEI (reduce the HTN) ECHO every 6-12 months to monitor Surgery
Increasing symptoms Enlarging heart T wave inversion on lateral leads Failure of medical treatment
Prognosis Poor post-operative survival EF <50% NYHA class III, IV Duration of CCF >12months
Tricuspid Regurgitation
Causes Functional (RV dilatation) Rheumatic fever
IE (IV drug abusers) Carcinoid
Symptoms Fatigue Hepatic pain Ascites Edema Dyspnea and orthopnea (if LV dysfunction)
Signs Giant V wave and Y descent in JVP Pulsatile hepatomegaly Pansystolic murmur head best at lower sternal boarder on inspiration
Management Digoxin, ACEI, diuretics Surgery

Maysah Al-Mulla OHCM, Passmedicine
Tricuspid stenosis
Causes Rheumatic fever IE
Congenital Signs Giant a wave and slow y descent in JVP
Opening snap Early diastolic murmur heard at left sternal edge on inspiration
Diagnosis ECHO
Management Diuretics Surgery
Pulmonary stenosis
Causes Congenital (Turner’s, william’s, Noonan’s) Acquired (rheumatic fever, carcinoid)
Dyspnea Fatigue Edema Ascites
Dysmorphic facies Prominent a wave on JVP Ejection systolic murmur radiating to the shoulder Widely split S2 In severe stenosis longer murmur, obscured A2, soft P2
ECG - P pulmonale - RVH - RBBB
Diagnosis Cardiac catheterization Management Vuloplasty/ vulvotomy
Pulmonary regurgitation
Graham steel murmur if associated with MS and Pulmonary HTN Valve replacement
Biological valves Mechanical valves Origin Bovine or porcine Bileaflet valve
Disadvantages Structural deterioration or calcification over time
High risk of thrombosis
Anticoagulation No long term anticoagulation
Warfarin for the first 3 months
ASA long term
Long term anticoagulation
ASA is added
INR target Aortic 2-3
Mitral 2.5-3.5

Maysah Al-Mulla OHCM, Passmedicine
Infective endocarditis
Affected patients Previously normal valve (50%) Rheumatic valve disease
Prosthetic valve Congenital heart defects
IV drug users
Causes Streptococcus viridans (most common cause - 40-50%). Streptococcus mitis and Streptococcus sanguinis
Staphylococcus epidermidis prosthetic valves
Staphylococcus aureus acute presentation IVDUs
Streptococcus bovis colorectal cancer
Non-infective Systemic lupus erythematosus (Libman-Sacks) Malignancy: marantic endocarditis
Culture negative causes
prior antibiotic therapy Coxiella burnetii Bartonella Brucella
HACEK: Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, Kingella)
Diagnosis Dukes criteria (one of these) - Pathological criteria +
- 2 major - 1 major + 3 minor
- 5 minor
Pathological criteria Positive histology or microbiology of pathological material
obtained at autopsy or cardiac surgery (valve tissue, vegetations, embolic fragments or intracardiac abscess content)
Major criterial - Positive blood cultures
2 positive blood cultures showing typical organisms
consistent with infective endocarditis, such as Streptococcus viridans and the HACEK group
persistent bacteremia from two blood cultures taken > 12 hours apart or three or more positive blood cultures where

Maysah Al-Mulla OHCM, Passmedicine
the pathogen is less specific such as Staph aureus and Staph epidermidis
positive serology for Coxiella burnetii, Bartonella species or Chlamydia psittaci
positive molecular assays for specific gene targets - Evidence of endocardial involvement
positive echocardiogram (oscillating structures, abscess formation, new valvular regurgitation or dehiscence of
prosthetic valves), or new valvular regurgitation
Minor criteria - predisposing heart condition or intravenous drug use - microbiological evidence does not meet major criteria - fever > 38ºC
- vascular phenomena: major emboli, splenomegaly, clubbing, splinter haemorrhages, Janeway lesions, petechiae or purpura
- immunological phenomena: glomerulonephritis, Osler's nodes, Roth spots
Management Antibiotics - Bling therapy for native valve
Amoxicillin 2g Q4 IV ± gentamicin 1mg/kg Q12 IV Penicillin allergy Vanco 1g Q12 IV + gentamicin 1mg/kg
Q12 IV If negative organism meropenem 2g Q8 IV+ vanco
(trough 15-20) - Blind therapy for prosthetic valve
Vanco + genta + rifampicin 300-600 BD - Staph with native valve
Flucloxacillin >4 weeks (vanco + rifamp if allergic) - Staph with prosthetic valve
Fluclo + genta + rifamp >6 weeks - Strep
1.2g Q4 IV for 4-6 weeks - Entercoccus & HACEK
Amoxi 4 weeks + genta 2 weeks Surgery
HF Valvular obstruction Repeated emboli
Fungal endocarditis Persistent bacteremia
Myocardial abscess
Maysah Al-Mulla OHCM, Passmedicine
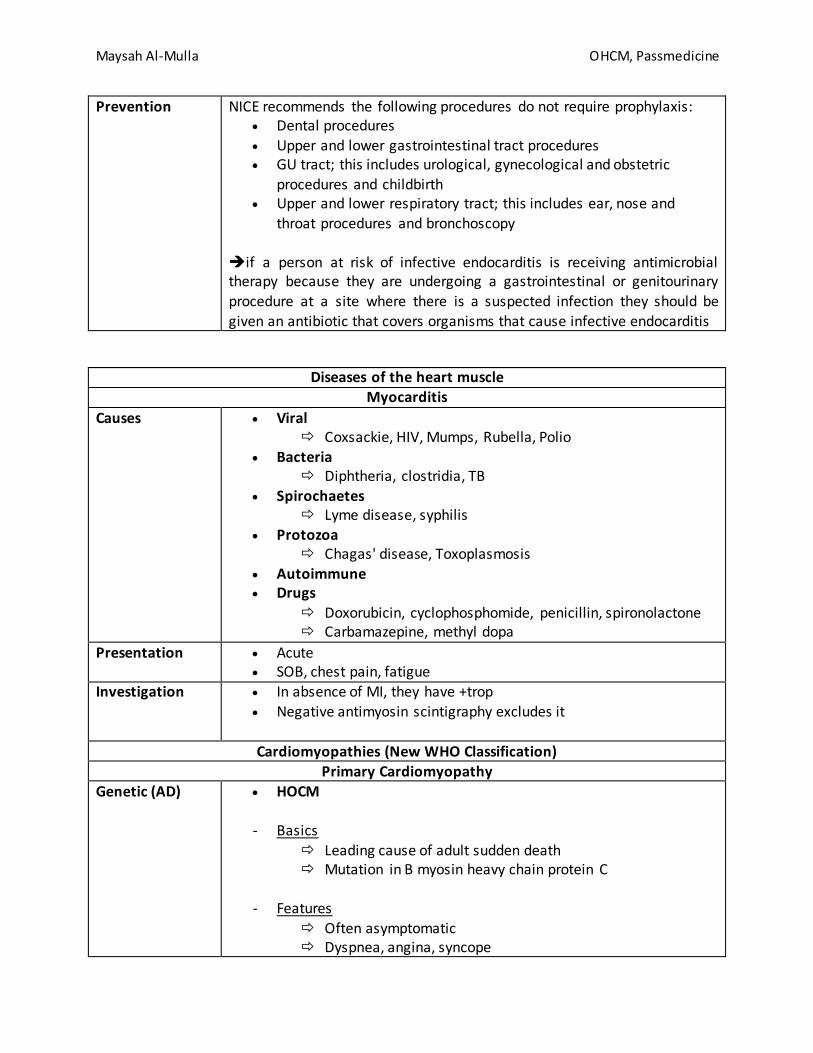
Prevention NICE recommends the following procedures do not require prophylaxis: Dental procedures Upper and lower gastrointestinal tract procedures GU tract; this includes urological, gynecological and obstetric
procedures and childbirth Upper and lower respiratory tract; this includes ear, nose and
throat procedures and bronchoscopy
if a person at risk of infective endocarditis is receiving antimicrobial therapy because they are undergoing a gastrointestinal or genitourinary
procedure at a site where there is a suspected infection they should be given an antibiotic that covers organisms that cause infective endocarditis
Diseases of the heart muscle Myocarditis
Causes Viral Coxsackie, HIV, Mumps, Rubella, Polio
Bacteria Diphtheria, clostridia, TB
Spirochaetes Lyme disease, syphilis
Protozoa Chagas' disease, Toxoplasmosis
Autoimmune Drugs
Doxorubicin, cyclophosphomide, penicillin, spironolactone Carbamazepine, methyl dopa
Presentation Acute SOB, chest pain, fatigue
Investigation In absence of MI, they have +trop Negative antimyosin scintigraphy excludes it
Cardiomyopathies (New WHO Classification) Primary Cardiomyopathy
Genetic (AD) HOCM
- Basics Leading cause of adult sudden death Mutation in B myosin heavy chain protein C
- Features
Often asymptomatic Dyspnea, angina, syncope

Maysah Al-Mulla OHCM, Passmedicine
Sudden death (most commonly due to ventricular arrhythmias), arrhythmias, heart failure
Jerky pulse, large 'a' waves, double apex beat Ejection systolic murmur: increases with Valsalva maneuver
and decreases on squatting
- Associations Friedreich's ataxia
Wolff-Parkinson White
- Echo - mnemonic - MR SAM ASH Mitral regurgitation (MR) Systolic anterior motion (SAM) of the anterior mitral valve
leaflet Asymmetric hypertrophy (ASH)
- ECG
Left ventricular hypertrophy Progressive T wave inversion
Deep Q waves Atrial fibrillation may occasionally be seen
Arrhythmogenic right ventricular dysplasia
- Basics 2nd most leading cause of sudden death Mutations in desmosomes genes
- Presentation
Syncope, palpitations, sudden death
- Investigations Epsillon notch/terminal notch in QRS Echo hypokinetic RV
MRI fibrofatty tissue
- Management Drugs satolol
Ablation ICD
Naxos disease is AR variant (ARVC+ palmoplantar keratosis + woolly hair)

Maysah Al-Mulla OHCM, Passmedicine
Mixed Dilated cardiomyopathy
- Features Dilated heart leading to systolic (+/- diastolic) dysfunction All 4 chambers affected but LV more so than RV Features include arrhythmias, emboli, mitral regurgitation
Absence of congenital, valvular or ischemic heart disease
- Causes Alcohol: may improve with thiamine
Postpartum HTN Inherited Infections e.g. Coxsackie B, HIV, diphtheria, parasitic Endocrine e.g. Hyperthyroidism
Infiltrative* e.g. Haemochromatosis, sarcoidosis Neuromuscular e.g. Duchenne muscular dystrophy
Nutritional e.g. Kwashiorkor, pellagra, thiamine/selenium deficiency Drugs e.g. Doxorubicin
- Investigations
Low NA indicates poor prognosis ECHO global hypokinetic heart and low EF
- Treatment Digoxin, diuretics, ACEI, anticoagulation, biventricular pacing, ICD
Restrictive cardiomyopathy
- Causes Idiopathic Amyloidosis
Hemochromatosis Sarcoidosis
Scleroderma
- Diagnosis Cardiac cath
Acquired Peripartum
- Between last month of pregnancy and 5 months post partum
Takotsubo - Stress induced, transient

Maysah Al-Mulla OHCM, Passmedicine
Secondary cardiomyopathies
Infective Coxacki
Chagas Infiltrative
Amyolidosis
Storage Hemochromatosis
Toxicity Doxorubicin
Alcohol Inflammatory
Sarcoidosis Endocrine
DM Thyrotoxicosis Acromegaly
Neuromuscular Friedreich’s ataxia Duchenne muscular dystrophy
Nutritional Beriberi (thiamine)
Autoimmune
SLE
Pericardial diseases Acute pericarditis
Features Chest pain: may be pleuritic. Is often relieved by sitting forwards Other symptoms include non-productive cough, dyspnea and flu-
like symptoms Pericardial rub
Tachypnea Tachycardia
Causes viral infections (Coxsackie)
tuberculosis uremia (causes 'fibrinous' pericarditis) trauma post-myocardial infarction, Dressler's syndrome connective tissue disease
hypothyroidism
Investigations ECG - widespread 'saddle-shaped' ST elevation - PR depression: most specific ECG marker for pericarditis

Maysah Al-Mulla OHCM, Passmedicine
Treatment Analgesics Colchicine if relapse Steroids if relapse
Constrictive pericarditis Causes Any cause of pericarditis (particularly TB)
Features Dyspnea
right heart failure: elevated JVP, ascites, oedema, hepatomegaly JVP shows prominent x and y descent
pericardial knock - loud S3 Kussmaul's sign is positive
Investigations CXR Pericardial calcification
Both Y and X present in JVP (compared to tamponade where you have absent Y)
Pericardia effusion
Causes infectious pericarditis: viral, tuberculosis, pyogenic spread from septicemia and pneumonia
uremia idiopathic
post myocardial infarction (including Dressler's syndrome) malignancy
heart failure nephrotic syndrome hypothyroidism trauma
Features Dyspnea Raised JVP Bronchial breathing at left base
Diagnosis CXR Enlarged and globular heart
ECG Low voltage QRS
ECHO
Echo free area surrounding the heart Management Pericardiocentesis
Cardiac Tamponade Causes Any pericarditis
Aortic dissection Hemodialysis
Features Dyspnea
Raised JVP, with an absent Y descent - this is due to the limited right ventricular filling
Tachycardia
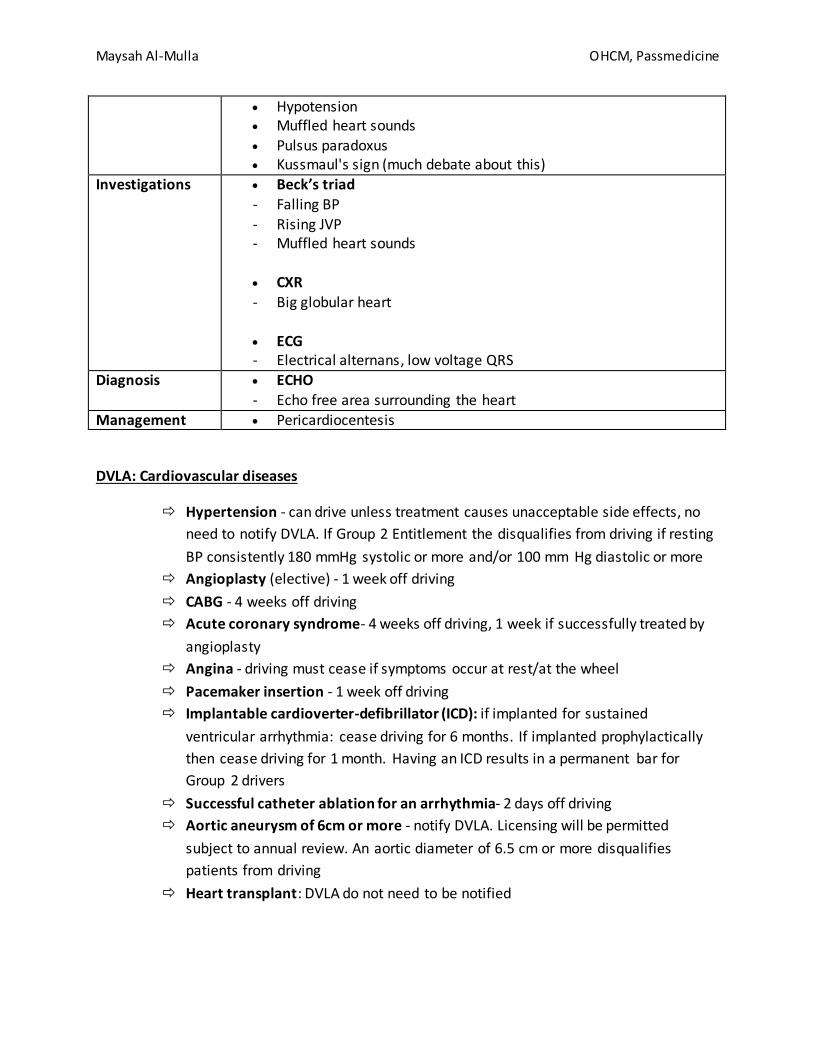
Maysah Al-Mulla OHCM, Passmedicine
Hypotension Muffled heart sounds Pulsus paradoxus Kussmaul's sign (much debate about this)
Investigations Beck’s triad
- Falling BP
- Rising JVP - Muffled heart sounds
CXR
- Big globular heart
ECG - Electrical alternans, low voltage QRS
Diagnosis ECHO
- Echo free area surrounding the heart Management Pericardiocentesis
DVLA: Cardiovascular diseases
Hypertension - can drive unless treatment causes unacceptable side effects, no
need to notify DVLA. If Group 2 Entitlement the disqualifies from driving if resting
BP consistently 180 mmHg systolic or more and/or 100 mm Hg diastolic or more
Angioplasty (elective) - 1 week off driving
CABG - 4 weeks off driving
Acute coronary syndrome- 4 weeks off driving, 1 week if successfully treated by
angioplasty
Angina - driving must cease if symptoms occur at rest/at the wheel
Pacemaker insertion - 1 week off driving
Implantable cardioverter-defibrillator (ICD): if implanted for sustained
ventricular arrhythmia: cease driving for 6 months. If implanted prophylactically
then cease driving for 1 month. Having an ICD results in a permanent bar for
Group 2 drivers
Successful catheter ablation for an arrhythmia- 2 days off driving
Aortic aneurysm of 6cm or more - notify DVLA. Licensing will be permitted
subject to annual review. An aortic diameter of 6.5 cm or more disqualifies
patients from driving
Heart transplant: DVLA do not need to be notified

Maysah Al-Mulla OHCM, Passmedicine
Surgical Chest pain
Dissection of thoracic aorta
Tearing interscapular pain Discrepancy in arterial blood pressures taken in both arms
May show mediastinal widening on chest x-ray
Diffuse oesophageal spasm
Spectrum of oesophageal motility disorders Caused by uncoordinated contractions of oesphageal muscles May show "nutcracker oesophagus" on barium swallow Symptoms include dysphagia, retrosternal discomfort and dyspepsia
Gastro-oesphageal reflux
Common cause of retrosternal discomfort Usually associated with symptoms of regurgitation, odynophagia and
dyspepsia Symptoms usually well controlled with PPI therapy Risk factors include obesity, smoking and excess alcohol
consumption
Boerhaaves syndrome
Spontaneous rupture of the oesophagus Caused by episodes of repeated vomiting often in association with
alcohol excess Typically there is an episode of repetitive vomiting followed by
severe chest and epigastric pain Diagnosis is by CT and contrast studies
Treatment is surgical; during first 12 hours primary repair, beyond this usually creation of controlled fistula with a T Tube, delay beyond 24 hours is associated with fulminent mediastinitis and is usually fatal.
Achalasia Difficulty swallowing, dysphagia to both liquids and solids and sometimes chest pain
Usually caused by failure of distal oesphageal inhibitory neurones Diagnosis is by pH and manometry studies together with contrast
swallow and endoscopy
Treatment is with either botulinum toxin, pneumatic dilatation or cardiomyotomy

Maysah Al-Mulla OHCM, Passmedicine
Cardiovascular diseases in pregnancy
Chest pain in pregnancy Aortic dissection • Predisposing factors in pregnancy are
hypertension, congenital heart disease and Marfan's syndrome
• Mainly Stanford type A dissections • Sudden tearing chest pain, transient
syncope • Patient may be cold and clammy,
hypertensive and have an aortic regurgitation murmur
• Involvement of the right coronary artery may cause inferior myocardial infarction
Surgical correction
- <24 weeks
Aortic repair with fetus kept in utero
- 28-32 weeks
Dependent on fetal condition
- >32 weeks Primary cesarean section
followed by primary aortic repair at the same operation
Mitral stenosis • Leading cause of mortality in pregnancy • Half dose scintigraphy; CT chest if
underlying lung disease should aid diagnosis
• Treatment with low molecular weight heparin throughout pregnancy and 4-6
weeks after childbirth • Warfarin is contra indicated in
pregnancy Hypertension in Pregnancy
High risk of hypertensive diseases take ASA 75mg OD from 12 weeks until the birth of the baby Hypertensive disease during previous pregnancies
Chronic kidney disease Autoimmune disorders such as SLE or antiphospholipid syndrome
Type 1 or 2 diabetes mellitus
Maysah Al-Mulla OHCM, Passmedicine
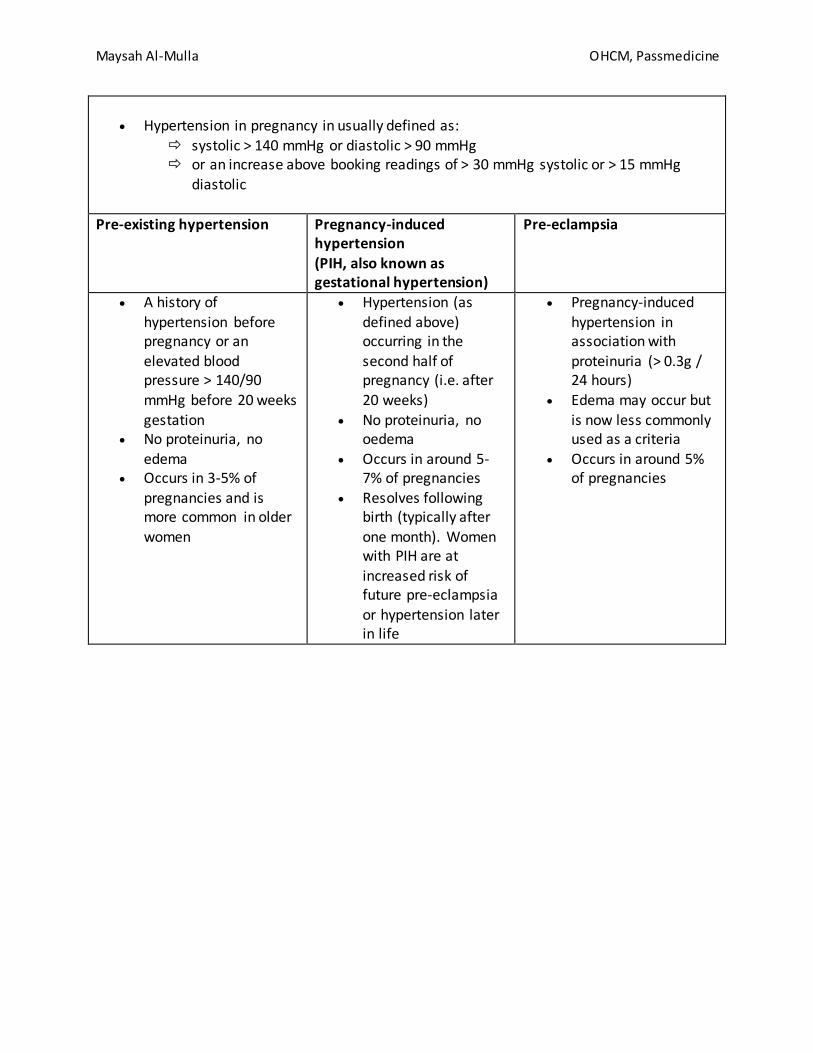
Hypertension in pregnancy in usually defined as:
systolic > 140 mmHg or diastolic > 90 mmHg or an increase above booking readings of > 30 mmHg systolic or > 15 mmHg
diastolic
Pre-existing hypertension Pregnancy-induced hypertension
(PIH, also known as gestational hypertension)
Pre-eclampsia
A history of hypertension before pregnancy or an elevated blood pressure > 140/90
mmHg before 20 weeks gestation
No proteinuria, no edema
Occurs in 3-5% of pregnancies and is more common in older women
Hypertension (as defined above) occurring in the second half of pregnancy (i.e. after
20 weeks) No proteinuria, no
oedema Occurs in around 5-
7% of pregnancies Resolves following
birth (typically after one month). Women with PIH are at
increased risk of future pre-eclampsia
or hypertension later in life
Pregnancy-induced hypertension in association with proteinuria (> 0.3g / 24 hours)
Edema may occur but is now less commonly used as a criteria
Occurs in around 5% of pregnancies
Related Documents











