Cardiac Transplantation in Infants and Children Mark W. Turrentine, MD, Kenneth A. Kesler, MD, Randall Caldwell, MD, Robert Darragh, MD, Lynda Means, MD, Yousuf Mahomed, MD, and John W. Brown, MD Departments of Surgery, Pediatrics, and Anesthesia, Riley Hospital for Children, Indiana University Medical Center, Indianapolis, Indiana Cardiac transplantation has become a more frequently used therapeutic modality for select cardiac pathology in infants and children. Since June 1986, 30 pediatric pa- tients (19 male and ll female) ranging in age from 4 days to 15 years (11 5 1 month old) have undergone orthotopic cardiac transplantation at our institution. Indications included idiopathic cardiomyopathy (n = 8), hypoplastic left heart syndrome (n = 13), and other forms of complex congenital heart disease (n = 9). There have been four operative and three late deaths only in the groups with hypoplastic left heart syndrome and other forms of complex congenital heart disease. Cumulative survival is 77% after a mean follow-up of 30 months (range, 6 to 77 months). Three operative deaths were attributable to he introduction of cyclosporin A as an adjunctive T immunosuppressive agent a decade ago has resulted in 1-year survival rates approaching 90% after cardiac transplantation in the adult population [l]. More recently, cardiac transplantation procedures have been extended to the pediatric age group. Because of generally discourag- ing results with open repair techniques for hypoplastic left heart syndrome (HLHS) in neonates, Bailey in 1985 pioneered cardiac transplantation as an alternative treat- ment [2, 31. Early and medium-term survival has been superior to that of the staged open technique as described by Norwood. Cardiac transplantation in the pediatric age group now constitutes a frequently used therapeutic modality for both HLHS and idiopathic cardiomyopathy (IDC) as well as a variety of complex congenital heart diseases (CCHD) resulting in end-stage cardiac dysfunction [4,5]. Concerns regarding cardiac transplantation in this young age group have focused not only on operative morbidity and mor- tality but also on the long-term effects of immunosuppres- sion with respect to growth retardation, infection, and the potential to develop neoplastic diseases. Moreover, as with other forms of cardiac surgery, the unique physiol- ogy of the pediatric age group poses challenges in post- operative care compared with the adult population. This study reviews our 6%-year cardiac transplant experience in infants and children and compares outcomes between three distinct indications for transplantation. Presented at the Twenty-ninth Annual Meeting of The Society of Thoracic Surgeons, San Antonio, TX, Jan 2527, 1993. Address reprint requests to Dr Turrentine, Indiana University Medical Center, 545 Barnhill Dr, EM #212, Indianapolis, IN 46202-5125. pulmonary hypertension, and the other was due to pul- monary hemorrhage. Two late deaths were secondary to allograft rejection, and the third was due to infection. There has been uniform survival in the group with idiopathic cardiomyopathy, and intermediate-term sur- vival rates are 78% and 62% in the groups with complex congenital heart diseases and hypoplastic left heart syn- drome, respectively (p = 0.15). Although longer-term results are necessary, orthotopic cardiac transplantation appears to be an acceptable mode of therapy for end- stage heart disease in the pediatric age group and tech- nically can be performed despite complex malformations of the great arteries or atria. (Ann Thorac Surg 1994;57:546-54) Material and Methods From June 1986 through December 1992, 46 infants and children were placed on the national computer recipient waiting list (United Network for Organ Sharing) for cardiac transplantation by the Multidisciplinary Cardiac Transplantation Committee at Riley Hospital for Chil- dren. Thirteen of these patients (8 with HLHS) died while awaiting a donor organ, and 30 underwent orthotopic cardiac transplantation. Time on the transplant waiting list ranged from 0 to 179 days (mean time, 19.7 days). Of the patients who had transplantation, 19 were male and 11, female. They ranged in age from 4 days to 16 years; 11 patients were 1 month old or younger at the time of operation (Fig 1). Twenty-three patients (77%) were considered to be “status 1” priority by virtue of dependence on inotropic agents (n = 16, 53%), a ventilator (n = 15, 50%), or both at the time of donor organ availability. Eight patients (27%)had an end-stage IDC; the indication for transplan- tation in the remaining 22 patients (73%) was complex congenital heart malformations not amenable or poorly amenable to repair. In this latter group, 13 patients (43% of those having transplantation) exhibited either type 1 (n = 12, 92%)or type 2 (n = 1, 8%)HLHS [6]. One patient with HLHS had previously undergone the first stage of the Norwood procedure but was not considered a candi- date for the second stage because of right ventricular failure. The other 9 patients (30%) had various forms of CCHD, and all but 2 of them had undergone prior attempts at surgical palliation, open repair, or both (Table 1). 0 1994 by The Society of Thoracic Surgeons 0003-4975/94/$7.00

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cardiac Transplantation in Infants and Children Mark W. Turrentine, MD, Kenneth A. Kesler, MD, Randall Caldwell, MD, Robert Darragh, MD, Lynda Means, MD, Yousuf Mahomed, MD, and John W. Brown, MD Departments of Surgery, Pediatrics, and Anesthesia, Riley Hospital for Children, Indiana University Medical Center, Indianapolis, Indiana
Cardiac transplantation has become a more frequently used therapeutic modality for select cardiac pathology in infants and children. Since June 1986, 30 pediatric pa- tients (19 male and ll female) ranging in age from 4 days to 15 years (11 5 1 month old) have undergone orthotopic cardiac transplantation at our institution. Indications included idiopathic cardiomyopathy (n = 8), hypoplastic left heart syndrome (n = 13), and other forms of complex congenital heart disease (n = 9). There have been four operative and three late deaths only in the groups with hypoplastic left heart syndrome and other forms of complex congenital heart disease. Cumulative survival is 77% after a mean follow-up of 30 months (range, 6 to 77 months). Three operative deaths were attributable to
he introduction of cyclosporin A as an adjunctive T immunosuppressive agent a decade ago has resulted in 1-year survival rates approaching 90% after cardiac transplantation in the adult population [l]. More recently, cardiac transplantation procedures have been extended to the pediatric age group. Because of generally discourag- ing results with open repair techniques for hypoplastic left heart syndrome (HLHS) in neonates, Bailey in 1985 pioneered cardiac transplantation as an alternative treat- ment [2, 31. Early and medium-term survival has been superior to that of the staged open technique as described by Norwood.
Cardiac transplantation in the pediatric age group now constitutes a frequently used therapeutic modality for both HLHS and idiopathic cardiomyopathy (IDC) as well as a variety of complex congenital heart diseases (CCHD) resulting in end-stage cardiac dysfunction [4,5]. Concerns regarding cardiac transplantation in this young age group have focused not only on operative morbidity and mor- tality but also on the long-term effects of immunosuppres- sion with respect to growth retardation, infection, and the potential to develop neoplastic diseases. Moreover, as with other forms of cardiac surgery, the unique physiol- ogy of the pediatric age group poses challenges in post- operative care compared with the adult population. This study reviews our 6%-year cardiac transplant experience in infants and children and compares outcomes between three distinct indications for transplantation.
Presented at the Twenty-ninth Annual Meeting of The Society of Thoracic Surgeons, San Antonio, TX, Jan 2 5 2 7 , 1993.
Address reprint requests to Dr Turrentine, Indiana University Medical Center, 545 Barnhill Dr, EM #212, Indianapolis, IN 46202-5125.
pulmonary hypertension, and the other was due to pul- monary hemorrhage. Two late deaths were secondary to allograft rejection, and the third was due to infection. There has been uniform survival in the group with idiopathic cardiomyopathy, and intermediate-term sur- vival rates are 78% and 62% in the groups with complex congenital heart diseases and hypoplastic left heart syn- drome, respectively ( p = 0.15). Although longer-term results are necessary, orthotopic cardiac transplantation appears to be an acceptable mode of therapy for end- stage heart disease in the pediatric age group and tech- nically can be performed despite complex malformations of the great arteries or atria.
(Ann Thorac Surg 1994;57:546-54)
Material a n d Methods
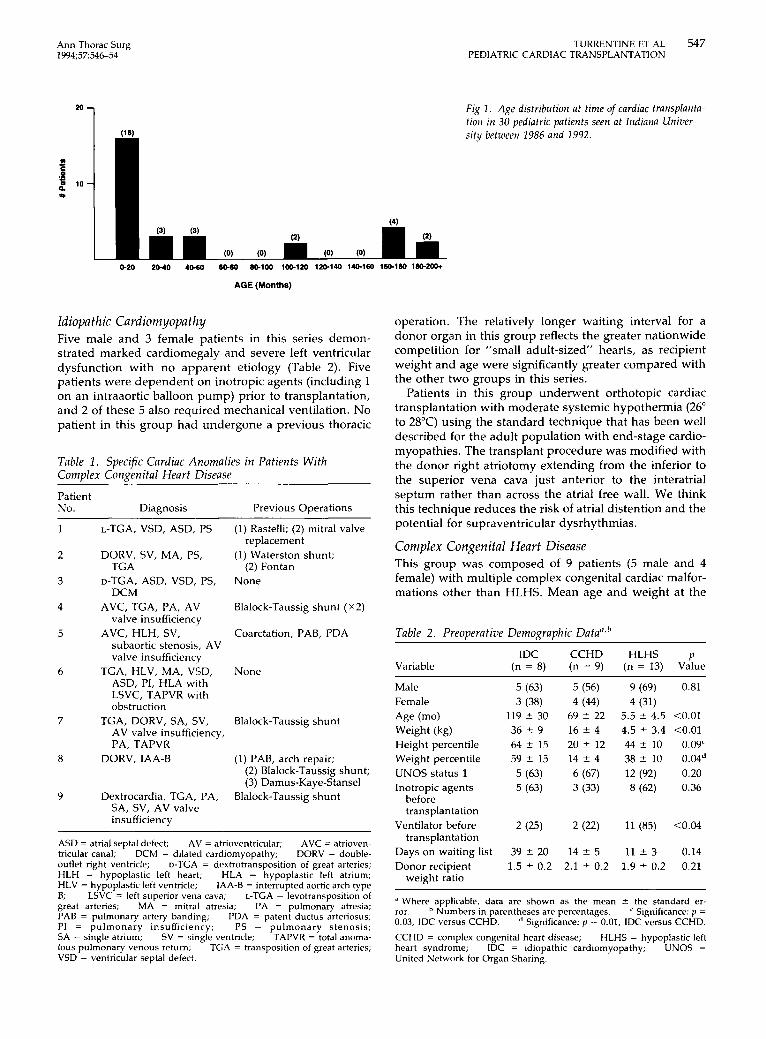
From June 1986 through December 1992, 46 infants and children were placed on the national computer recipient waiting list (United Network for Organ Sharing) for cardiac transplantation by the Multidisciplinary Cardiac Transplantation Committee at Riley Hospital for Chil- dren. Thirteen of these patients (8 with HLHS) died while awaiting a donor organ, and 30 underwent orthotopic cardiac transplantation. Time on the transplant waiting list ranged from 0 to 179 days (mean time, 19.7 days). Of the patients who had transplantation, 19 were male and 11, female. They ranged in age from 4 days to 16 years; 11 patients were 1 month old or younger at the time of operation (Fig 1).
Twenty-three patients (77%) were considered to be “status 1” priority by virtue of dependence on inotropic agents (n = 16, 53%), a ventilator (n = 15, 50%), or both at the time of donor organ availability. Eight patients (27%) had an end-stage IDC; the indication for transplan- tation in the remaining 22 patients (73%) was complex congenital heart malformations not amenable or poorly amenable to repair. In this latter group, 13 patients (43% of those having transplantation) exhibited either type 1 (n = 12, 92%) or type 2 (n = 1, 8%) HLHS [6]. One patient with HLHS had previously undergone the first stage of the Norwood procedure but was not considered a candi- date for the second stage because of right ventricular failure. The other 9 patients (30%) had various forms of CCHD, and all but 2 of them had undergone prior attempts at surgical palliation, open repair, or both (Table 1).
0 1994 by The Society of Thoracic Surgeons 0003-4975/94/$7.00
Ann Thorac Surg 1994;57546-54
TURRENTINE ET AL 547 PEDIATRIC CARDIAC TRANSPLANTATION
"1
AGE (Months)
Idiopathic Card iom yopath y Five male and 3 female patients in this series demon- strated marked cardiomegaly and severe left ventricular dysfunction with no apparent etiology (Table 2). Five patients were dependent on inotropic agents (including 1 on an intraaortic balloon pump) prior to transplantation, and 2 of these 5 also required mechanical ventilation. No patient in this group had undergone a previous thoracic
Table 1. Specific Cardiac Anomalies in Patients With Corntllex Conpenital Heart Disease
Patient No. Diagnosis Previous Operations
6
7
8
9
L-TGA, VSD, ASD, PS
DORV, SV, MA, PS, TGA
D-TGA, ASD, VSD, PS, DCM
AVC, TGA, PA, AV valve insufficiency
AVC, HLH, SV, subaortic stenosis, AV valve insufficiency
TGA, HLV, MA, VSD, ASD, PI, HLA with LSVC, TAPVR with obstruction
TGA, DORV, SA, SV, AV valve insufficiency, PA, TAPVR
DORV, IAA-B
Dextrocardia, TGA, PA, SA, SV, AV valve insufficiency
(1) Rastelli; (2) mitral valve
(1) Waterston shunt;
None
replacement
(2) Fontan
Blalock-Taussig shunt ( ~ 2 )
Coarctation, PAB, PDA
Fig 2 . Age distribution a t time of cardiac fransplanta- tion in 30 pediatric patients seen a t Indiana Univer- sity between 1986 and 2992.
operation. The relatively longer waiting interval for a donor organ in this group reflects the greater nationwide competition for "small adult-sized' hearts, as recipient weight and age were significantly greater compared with the other two groups in this series.
Patients in this group underwent orthotopic cardiac transplantation with moderate systemic hypothermia (26" to 28°C) using the standard technique that has been well described for the adult population with end-stage cardio- myopathies. The transplant procedure was modified with the donor right atriotomy extending from the inferior to the superior vena cava just anterior to the interatrial septum rather than across the atrial free wall. We think this technique reduces the risk of atrial distention and the potential for supraventricular dysrhythmias.
Complex Congenital Heart Disease This group was composed of 9 patients (5 male and 4 female) with multiple complex congenital cardiac malfor- mations other than HLHS. Mean age and weight at the
Table 2. Preoaeratiue Demowaahic Data","
None IDC CCHD HLHS p
Variable (n = 8) (n = 9) (n = 13) Value
Blalock-Taussig shunt
(1) PAB, arch repair; (2) Blalock-Taussig shunt; (3) Damus-Kaye-Stansel
Blalock-Taussig shunt
ASD = atrial septal defect; AVC = atrioven- tricular canal; DCM = dilated cardiomyopathy; DORV = double- outlet right ventricle; D-TGA = dextrotransposition of great arteries; HLH = hypoplastic left heart; HLA = hypoplastic left atrium; HLV = hypoplastic left ventricle; IAA-B = interrupted aortic arch type B; L-TGA = levotransposition of great arteries; MA = mitral atresia; PA = pulmonary atresia; PAB = pulmonary artery banding; FDA = patent ductus arteriosus; PI = pulmonary insufficiency; PS = pulmonary stenosis; SA = single atrium; TAPVR = total anoma- lous pulmonary venous return; TGA = transposition of great arteries; VSD = ventricular septal defect.
AV = atrioventricular;
LSVC = left superior vena cava;
SV = single ventricle;
Male Female Age (mo) Weight (kg) Height percentile Weight percentile UNOS status 1 Inotropic agents
before transplantation
Ventilator before transplantation
Days on waiting list Donor recipient
weight ratio
5 (63) 3 (38)
119 2 30 36 t 9 64 t 15 59 t 15 5 (63) 5 (63)
2 (25)
39 t 20 1.5 t 0.2
5 (56) 9 (69) 0.81 4 (44) 4 (31)
69 t 22 5.5 t 4.5 <0.01 16 t 4 4.5 t 3.4 <0.01 20 t 12 44 t 10 0.09' 14 t 4 38 t 10 0.04d 6 (67) 12 (92) 0.20 3 (33) 8 (62) 0.36
2 (22) 11 (85) <0.04
14 t 5 11 t 3 0.14 2.1 5 0.2 1.9 t 0.2 0.21
a Where applicable, data are shown as the mean 2 the standard er- ror. Numbers in parentheses are percentages. Significance: p = 0.03, IDC versus CCHD. Significance: p = 0.01, IDC versus CCHD. CCHD = complex congenital heart disease; HLHS = hypoplastic left heart syndrome; IDC = idiopathic cardiomyopathy; UNOS = United Network for Organ Sharing.
548 TURRENTINE ET AL PEDIATRIC CARDIAC TRANSPLANTATION
Ann Thorac Surg 19945754654
time of transplantation were intermediate in this group compared with the IDC or HLHS group (see Table 2 ) . As a result of severe lifelong cardiac disease, these patients had the lowest average height and weight percentiles of the three groups, which was significant compared with the IDC category. Three patients with CCHD were depen- dent on infusions of inotropic agents, and 2 patients required mechanical ventilation prior to operation.
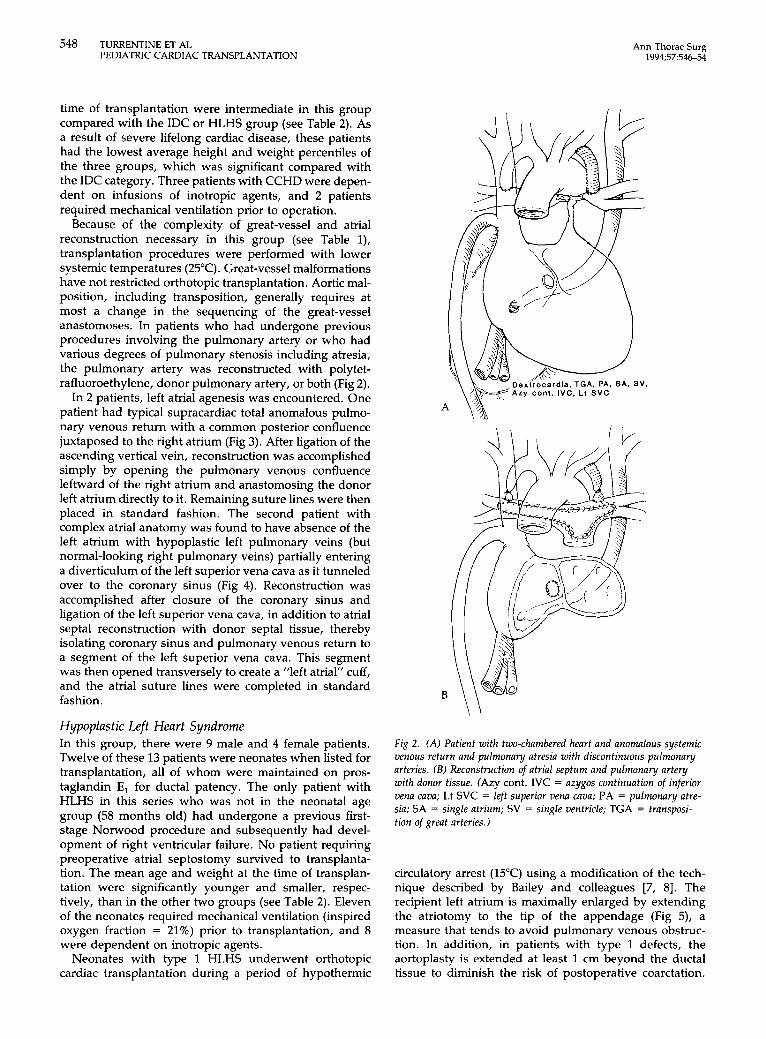
Because of the complexity of great-vessel and atrial reconstruction necessary in this group (see Table l), transplantation procedures were performed with lower systemic temperatures (25°C). Great-vessel malformations have not restricted orthotopic transplantation. Aortic mal- position, including transposition, generally requires at most a change in the sequencing of the great-vessel anastomoses. In patients who had undergone previous procedures involving the pulmonary artery or who had various degrees of pulmonary stenosis including atresia, the pulmonary artery was reconstructed with polytet- rafluoroethylene, donor pulmonary artery, or both (Fig 2) .
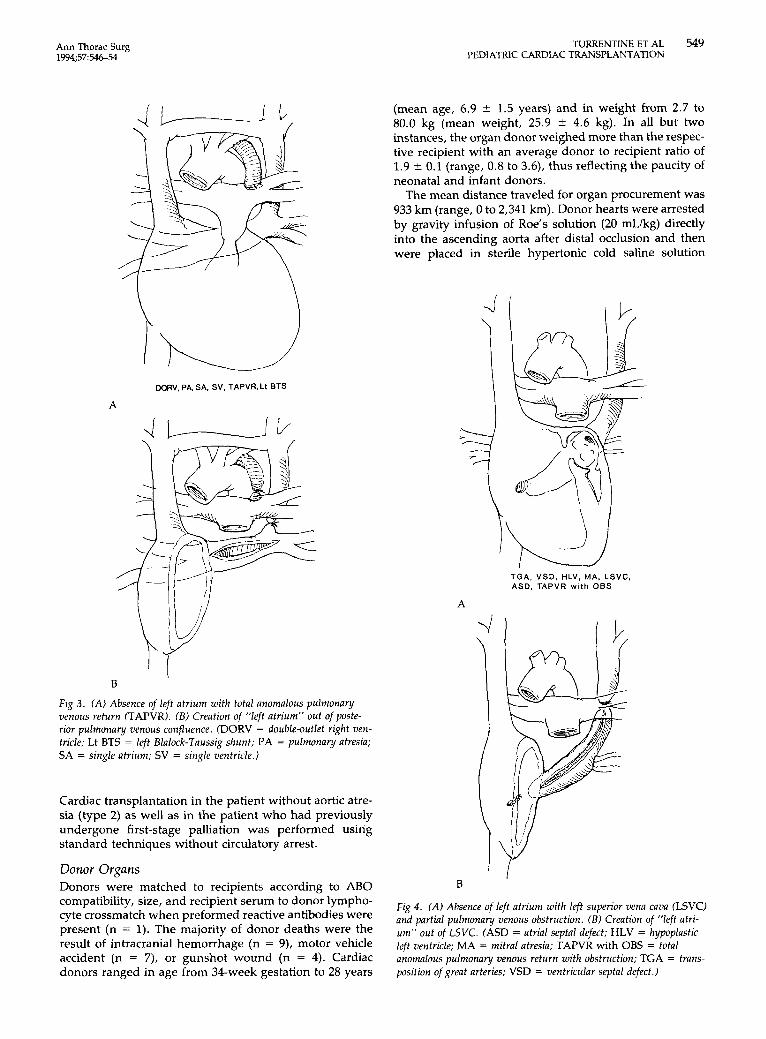
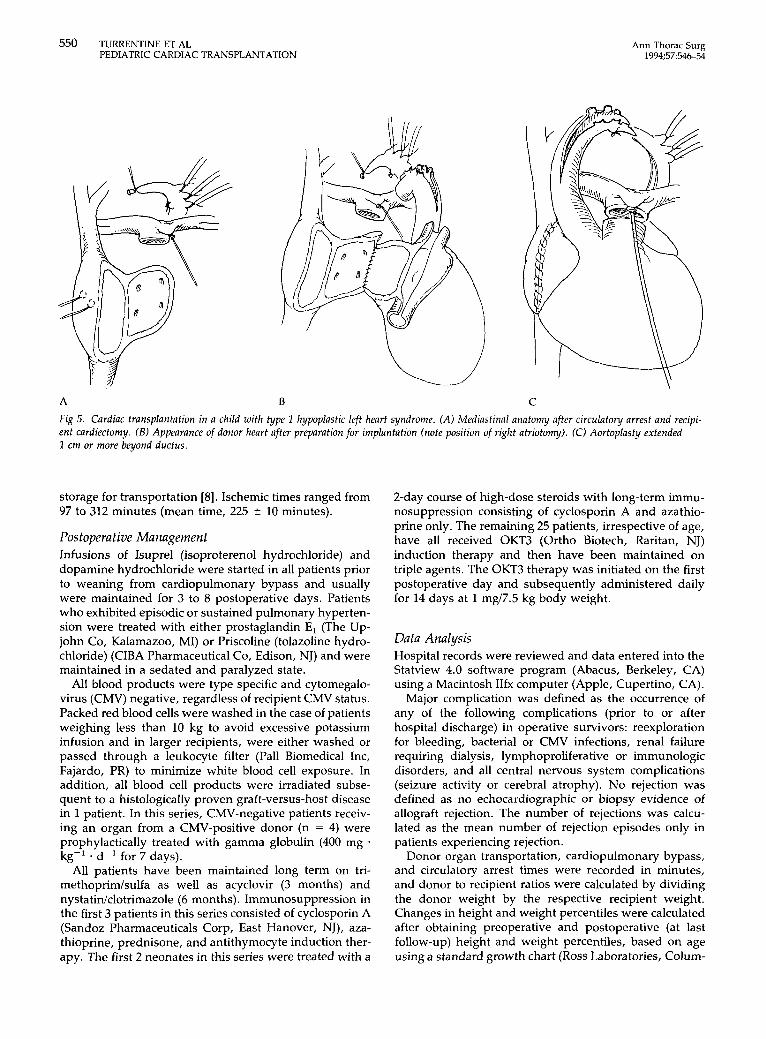
In 2 patients, left atrial agenesis was encountered. One patient had typical supracardiac total anomalous pulmo- nary venous return with a common posterior confluence juxtaposed to the right atrium (Fig 3). After ligation of the ascending vertical vein, reconstruction was accomplished simply by opening the pulmonary venous confluence leftward of the right atrium and anastomosing the donor left atrium directly to it. Remaining suture lines were then placed in standard fashion. The second patient with complex atrial anatomy was found to have absence of the left atrium with hypoplastic left pulmonary veins (but normal-looking right pulmonary veins) partially entering a diverticulum of the left superior vena cava as it tunneled over to the coronary sinus (Fig 4). Reconstruction was accomplished after closure of the coronary sinus and ligation of the left superior vena cava, in addition to atrial septal reconstruction with donor septal tissue, thereby isolating coronary sinus and pulmonary venous return to a segment of the left superior vena cava. This segment was then opened transversely to create a "left atrial" cuff, and the atrial suture lines were completed in standard fashion.
Hypoplastic Left Heart Syndrome In this group, there were 9 male and 4 female patients. Twelve of these 13 patients were neonates when listed for transplantation, all of whom were maintained on pros- taglandin E, for ductal patency. The only patient with HLHS in this series who was not in the neonatal age group (58 months old) had undergone a previous first- stage Norwood procedure and subsequently had devel- opment of right ventricular failure. No patient requiring preoperative atrial septostomy survived to transplanta- tion. The mean age and weight at the time of transplan- tation were significantly younger and smaller, respec- tively, than in the other two groups (see Table 2) . Eleven of the neonates required mechanical ventilation (inspired oxygen fraction = 21%) prior to transplantation, and 8 were dependent on inotropic agents.
Neonates with type 1 HLHS underwent orthotopic cardiac transplantation during a period of hypothermic
A
Fig 2. (A) Patient with two-chambered heart and anomalous systemic venous return and pulmona y atresia with discontinuous pulmona y arteries. ( B ) Reconstruction of atrial septum and pulmonary artey with donor tissue. (Azy cont. IVC = azygos continuation of inferior vena cava; Lt SVC = left superior vena cava; PA = pulmona y atre- sin; SA = single atrium; SV = single ventricle; TGA = transposi- tion of great arteries.)
circulatory arrest (15°C) using a modification of the tech- nique described by Bailey and colleagues [7, 81. The recipient left atrium is maximally enlarged by extending the atriotomy to the tip of the appendage (Fig 5), a measure that tends to avoid pulmonary venous obstruc- tion. In addition, in patients with type 1 defects, the aortoplasty is extended at least 1 cm beyond the ductal tissue to diminish the risk of postoperative coarctation.
Ann Thorac Surg 1994;57546-54
DORV, PA, SA. SV, TAPVR. Lt BTS
A
B
Fig 3. (A) Absence of left atrium with total anomalous pulmonary venous return (TAPVR). ( B ) Creation of "left atrium" out of poste- rior pulmonary venous confluence. (DORV = double-outlet right ven- tricle; Lt BTS = left Blalock-Taussig shunt; PA = pulmonary atresia; SA = single atrium; SV = single ventricle.)
Cardiac transplantation in the patient without aortic atre- sia (type 2) as well as in the patient who had previously undergone first-stage palliation was performed using standard techniques without circulatory arrest.
Donor Organs Donors were matched to recipients according to ABO compatibility, size, and recipient serum to donor lympho- cyte crossmatch when preformed reactive antibodies were present (n = 1). The majority of donor deaths were the result of intracranial hemorrhage (n = 9), motor vehicle accident (n = 7), or gunshot wound (n = 4). Cardiac donors ranged in age from 34-week gestation to 28 years
TURRENTINE ET AL 549 PEDIATRIC CARDIAC TRANSPLANTATION
(mean age, 6.9 2 1.5 years) and in weight from 2.7 to 80.0 kg (mean weight, 25.9 L 4.6 kg). In all but two instances, the organ donor weighed more than the respec- tive recipient with an average donor to recipient ratio of 1.9 2 0.1 (range, 0.8 to 3.6), thus reflecting the paucity of neonatal and infant donors.
The mean distance traveled for organ procurement was 933 km (range, 0 to 2,341 km). Donor hearts were arrested by gravity infusion of Roe's solution (20 mLkg) directly into the ascending aorta after distal occlusion and then were placed in sterile hypertonic cold saline solution
TGA. VSD. HLV, MA, LSVC. ASD. TAPVR w i t h OBS
A
I B
Fig 4. (A) Absence of left atrium with left superior vena cava (LSVC) and partial pulmonary venous obstruction. ( B ) Creation of "left atri- um" out of LSVC. (ASD = atrial septal defect; HLV = hypoplastic left ventricle; MA = mitral atresia; TAPVR with OBS = total anomalous pulmona y venous return with obstruction; TGA = trans- position of great arteries; VSD = ventricular septal defect.)
550 TURRENTINE ET AL PEDIATRIC CARDIAC TRANSPLANTATION
Ann Thorac Surg 1994;57:546-54
A €3 C Fig 5 . Cardiac transplantation in a child with type I hypoplastic left heart syndrome. (A) Mediastinal anatomy after circulatory arrest and recipi- ent cardiectomy. ( B ) Appearance of donor heart after preparation for implantation (note position of right atriotomy). (C) Aortoplasty extended 1 cm or more beyond ductus.
storage for transportation [8]. Ischemic times ranged from 97 to 312 minutes (mean time, 225 ? 10 minutes).
Postoperative Management Infusions of Isuprel (isoproterenol hydrochloride) and dopamine hydrochloride were started in all patients prior to weaning from cardiopulmonary bypass and usually were maintained for 3 to 8 postoperative days. Patients who exhibited episodic or sustained pulmonary hyperten- sion were treated with either prostaglandin E, (The Up- john Co, Kalamazoo, MI) or Priscoline (tolazoline hydro- chloride) (CIBA Pharmaceutical Co, Edison, NJ) and were maintained in a sedated and paralyzed state.
All blood products were type specific and cytomegalo- virus (CMV) negative, regardless of recipient CMV status. Packed red blood cells were washed in the case of patients weighing less than 10 kg to avoid excessive potassium infusion and in larger recipients, were either washed or passed through a leukocyte filter (Pall Biomedical Inc, Fajardo, PR) to minimize white blood cell exposure. In addition, all blood cell products were irradiated subse- quent to a histologically proven graft-versus-host disease in 1 patient. In this series, CMV-negative patients receiv- ing an organ from a CMV-positive donor (n = 4) were prophylactically treated with gamma globulin (400 mg *
kg-’ * d-I for 7 days). All patients have been maintained long term on tri-
methoprim/sulfa as well as acyclovir (3 months) and nystatinklotrimazole (6 months). Immunosuppression in the first 3 patients in this series consisted of cyclosporin A (Sandoz Pharmaceuticals Corp, East Hanover, NJ), aza- thioprine, prednisone, and antithymocyte induction ther- apy. The first 2 neonates in this series were treated with a
2-day course of high-dose steroids with long-term immu- nosuppression consisting of cyclosporin A and azathio- prine only. The remaining 25 patients, irrespective of age, have all received OKT3 (Ortho Biotech, Raritan, NJ) induction therapy and then have been maintained on triple agents. The OKT3 therapy was initiated on the first postoperative day and subsequently administered daily for 14 days at 1 mg/7.5 kg body weight.
Data Analysis Hospital records were reviewed and data entered into the Statview 4.0 software program (Abacus, Berkeley, CA) using a Macintosh IIfx computer (Apple, Cupertino, CA).
Major complication was defined as the occurrence of any of the following complications (prior to or after hospital discharge) in operative survivors: reexploration for bleeding, bacterial or CMV infections, renal failure requiring dialysis, lymphoproliferative or immunologic disorders, and all central nervous system complications (seizure activity or cerebral atrophy). No rejection was defined as no echocardiographic or biopsy evidence of allograft rejection. The number of rejections was calcu- lated as the mean number of rejection episodes only in patients experiencing rejection.
Donor organ transportation, cardiopulmonary bypass, and circulatory arrest times were recorded in minutes, and donor to recipient ratios were calculated by dividing the donor weight by the respective recipient weight. Changes in height and weight percentiles were calculated after obtaining preoperative and postoperative (at last follow-up) height and weight percentiles, based on age using a standard growth chart (ROSS Laboratories, Colum-
Ann Thorac Surg 1994;5754&54
TURRENTINE ET AL 551 PEDIATRIC CARDIAC TRANSPLANTATION
bus, OH), by the following formula: [(postop% - preop%)/preop%] x 100.
Creatinine increase was expressed as the difference between the postoperative (at last follow-up) and preop- erative creatinine values (mg/dL). Hypertension was de- fined as the need of calcium-channel blockers or angio- tensin-converting enzyme inhibitors to control systolic blood pressure at the time of hospital discharge and at last
All continuous variables were expressed as the mean * the standard error and were compared between patient groups with one-way analysis of variance and Fisher's PLSD post hoc analysis when significant differences were found. Paired t testing was used for intragroup compari- sons of continuous data. Discrete variables between groups were analyzed using ,$ statistics with continuity correction where appropriate. Cumulative survival was calculated for all three patient groups, and differences were compared employing Mantel-Cox analysis.
follow-up.
Results Overall there were 26 operative survivors (87%) and only three late deaths after an average of 30 months' follow-up (range, 6 to 77 months). Major postoperative complica- tions occurred in about one third (n = 8) of the survivors: 3 patients (12%; 2 with HLHS and 1, CCHD) had bacterial pneumonia; 1 patient (4%; CCHD) had a CMV infection; 1 patient (4%) required reexploration for bleeding and 1 (4%), temporary dialysis, both in the HLHS category; and 2 (8%) had neurologic sequelae (seizure disorder and cerebral atrophy) (Table 3). These 2 patients were both in the CCHD category, hence, the sequelae were unrelated to total circulatory arrest. In 1 patient (4%, CCHD) in this series, a late lymphoproliferative disorder developed.
Patients in all three indication categories have demon- strated postoperative increases in both height and weight percentiles (60 * 47 and 172 * 73, respectively). In addition, all surviving patients demonstrate excellent donor organ function and have an essentially unrestricted life-style.
Of the four operative deaths, three occurred secondary to pulmonary hypertension (2 patients with HLHS and 1 with CCHD), and one was due to pulmonary hemorrhage (HLHS). Postmortem examination in this 1 patient failed to identify the definitive cause of death, although a bland necrotizing process after thromboembolism was suspected. One of the 2 HLHS patients who died secondary to pulmo- nary hypertension demonstrated Heath-Edwards grade 4 pulmonary vascular changes on postmortem examination. Two of the three late deaths were attributed to allograft rejection (both HLHS patients), and the third was due to bacterial pneumonia with sepsis in a patient with unrec- ognized asplenia (CCHD).
Multiple variables including sex, preoperative require- ment for inotropic agents, preoperative ventilator depen- dence, allograft ischemic time, and cardiopulmonary by- pass time were not predictive of operative death for the entire series. There was a trend toward lower operative weight being a risk factor for perioperative mortality with survivors weighing 18.0 * 4.1 kg and nonsurvivors
Table 3 . Operative and Late Results"."
P Variable IDC CCHD HLHS Value ~
Ischemic time (min) 205 2 20 229 2 22 234 2 13 0.54 Pump time (min) 110 2 7 152 2 23 140 2 11 0.24 TCA time (min) NA NA 6 2 C 3 NA Operative deaths 0 (0) l(11) 3 (23) 0.12 Late deathsc 0 (0) 1 (13) 2 (20) 0.31 Significant 0 (0) 5 (63) 3 (30) 0.18
Hypertension complications'
Discharge' 4 (50) 6 (75) 6 (60) 0.62 Last follow-up' 5 (63) 4 (50) 2 (20) 0.08
No rejection' 1 (13) 1 (13) 4 (40) 0.27 No. of rejection 2.0 2 0.3 2.0 2 0.3 1.8 2 0.4 0.35
% Height change' 25 2 52 3 2 23 129 2 112 0.51 % Weight change' 94 2 62 117 2 67 273 2 170 0.55 Creatinine increase' 0.4 2 0.1 0.3 2 0.1 0.1 2 0.1 0.28
a Where applicable, data are shown as the mean 2 the standard er- ror. Numbers in parentheses are percentages. Data are based on operative survivors. CCHD = complex congenital heart disease; HLHS = hypoplastic left heart syndrome; IDC = idiopathic cardiomyopathy; NA = not applicable;
episodes'
TCA = total circulatory arrest.
weighing 3.4 5 0.6 kg ( p = 0.16). Similarly, age at time of transplantation was higher in operative survivors com- pared with patients who did not survive (63.4 * 15.1 months versus 2.6 * 0.1 months) but did not reach significance ( p = 0.13). Both of these trends, lower recip- ient weight and younger age in nonsurvivors, were re- flective of the increased risks associated with cardiac transplantation for HLHS and were not independent risk factors. Two variables, donor to recipient weight ratio and postoperative pulmonary hypertension, appeared to be predictive of perioperative mortality by univariate analy- sis. Donor to recipient weight ratios were found to be higher in nonsurvivors than in survivors: 2.4 * 0.4 versus 1.8 * 0.1 ( p = 0.06). There were three operative deaths (38%) among the 8 patients (7 HLHS patients and 1 CCHD patient) requiring postoperative pulmonary vasodilator therapy ( p = 0.02).
There were a total of 39 rejections episodes requiring therapy in 20 operative survivors (mean number, 1.95 * 0.2 per patient). To date, 6 patients have not experienced a rejection episode, all of whom were immunosuppressed with our current three-drug protocol with monoclonal antibody induction therapy. Further, in the subgroup of neonates undergoing transplantation at or less than 1 month, 4 of the 10 survivors have not experienced a rejection episode, and the other 6 have sustained a mean of 2.0 t 0.4 episodes. In contrast, only 2 (13%) of 16 patients greater than 1 month of age have been rejection free ( p = 0.10 versus neonates <1 month old). There was an average of 1.9 * 0.2 rejection episodes per patient in patients greater than 1 month of age.
Only 5 patients in this series were immunosuppressed using protocols other than the protocol currently em-
552 TURRENTINE ET AL PEDIATRIC CARDIAC TRANSPLANTATION
Ann Thorac Surg 1994;57:54&54
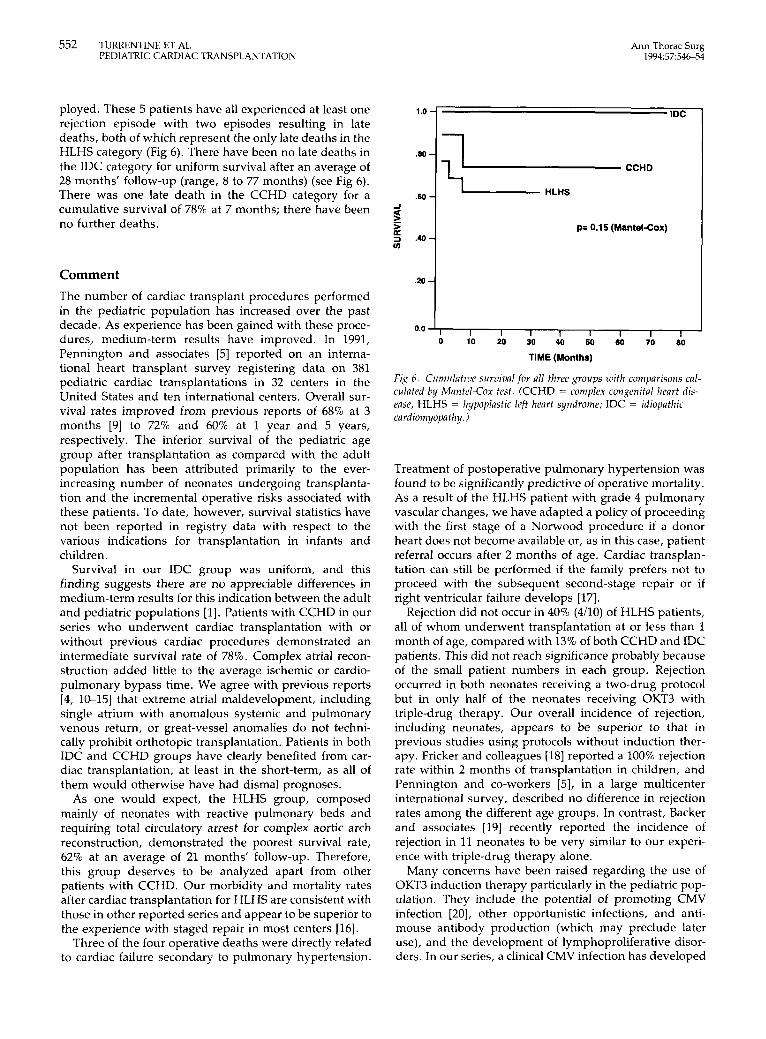
ployed. These 5 patients have all experienced at least one rejection episode with two episodes resulting in late deaths, both of which represent the only late deaths in the HLHS category (Fig 6). There have been no late deaths in the IDC category for uniform survival after an average of 28 months’ follow-up (range, 8 to 77 months) (see Fig 6). There was one late death in the CCHD category for a cumulative survival of 78% at 7 months; there have been no further deaths.
Comment The number of cardiac transplant procedures performed in the pediatric population has increased over the past decade. As experience has been gained with these proce- dures, medium-term results have improved. In 1991, Pennington and associates [5] reported on an interna- tional heart transplant survey registering data on 381 pediatric cardiac transplantations in 32 centers in the United States and ten international centers. Overall sur- vival rates improved from previous reports of 68% at 3 months [9] to 72% and 60% at 1 year and 5 years, respectively. The inferior survival of the pediatric age group after transplantation as compared with the adult population has been attributed primarily to the ever- increasing number of neonates undergoing transplanta- tion and the incremental operative risks associated with these patients. To date, however, survival statistics have not been reported in registry data with respect to the various indications for transplantation in infants and children.
Survival in our IDC group was uniform, and this finding suggests there are no appreciable differences in medium-term results for this indication between the adult and pediatric populations [l]. Patients with CCHD in our series who underwent cardiac transplantation with or without previous cardiac procedures demonstrated an intermediate survival rate of 78%. Complex atrial recon- struction added little to the average ischemic or cardio- pulmonary bypass time. We agree with previous reports [4, 10-151 that extreme atrial maldevelopment, including single atrium with anomalous systemic and pulmonary venous return, or great-vessel anomalies do not techni- cally prohibit orthotopic transplantation. Patients in both IDC and CCHD groups have clearly benefited from car- diac transplantation, at least in the short-term, as all of them would otherwise have had dismal prognoses.
As one would expect, the HLHS group, composed mainly of neonates with reactive pulmonary beds and requiring total circulatory arrest for complex aortic arch reconstruction, demonstrated the poorest survival rate, 62% at an average of 21 months’ follow-up. Therefore, this group deserves to be analyzed apart from other patients with CCHD. Our morbidity and mortality rates after cardiac transplantation for HLHS are consistent with those in other reported series and appear to be superior to the experience with staged repair in most centers [16].
Three of the four operative deaths were directly related to cardiac failure secondary to pulmonary hypertension.
.20
p= 0.15 (Mantel-Cox)
0.0 ‘ I I I I 1 I I I I 0 10 20 30 40 50 60 70 80
TIME (Months)
Fix 6 . Cumulative surriival for all three groups with comparisons cal- culated by Mantel-Cox test. (CCHD = complex congenital lieart dis- ease; HLHS = hypoplastic left heart syndrome; IDC = idiopathic cardiomyopa thy.)
Treatment of postoperative pulmonary hypertension was found to be significantly predictive of operative mortality. As a result of the HLHS patient with grade 4 pulmonary vascular changes, we have adapted a policy of proceeding with the first stage of a Norwood procedure if a donor heart does not become available or, as in this case, patient referral occurs after 2 months of age. Cardiac transplan- tation can still be performed if the family prefers not to proceed with the subsequent second-stage repair or if right ventricular failure develops [17].
Rejection did not occur in 40% (400) of HLHS patients, all of whom underwent transplantation at or less than 1 month of age, compared with 13% of both CCHD and IDC patients. This did not reach significance probably because of the small patient numbers in each group. Rejection occurred in both neonates receiving a two-drug protocol but in only half of the neonates receiving OKT3 with triple-drug therapy. Our overall incidence of rejection, including neonates, appears to be superior to that in previous studies using protocols without induction ther- apy. Fricker and colleagues [18] reported a 100% rejection rate within 2 months of transplantation in children, and Pennington and co-workers [5], in a large multicenter international survey, described no difference in rejection rates among the different age groups. In contrast, Backer and associates [19] recently reported the incidence of rejection in 11 neonates to be very similar to our experi- ence with triple-drug therapy alone.
Many concerns have been raised regarding the use of OKT3 induction therapy particularly in the pediatric pop- ulation. They include the potential of promoting CMV infection [20], other opportunistic infections, and anti- mouse antibody production (which may preclude later use), and the development of lymphoproliferative disor- ders. In our series, a clinical CMV infection has developed

Ann Thorac Surg 1994;57:54&54
TURRENTINE ET AL 553 PEDIATRIC CARDIAC TRANSPLANTATION
in only 1 patient to date. Moreover, none of the 25 patients receiving OKT3 induction therapy have had clinical CMV infections. We believe the greater risk factor for CMV infection after transplantation is exposure to CMV by either the donor organ or blood products, regard- less of recipient serology, as opposed to induction ther- apy. To date, we have not treated a pediatric cardiac transplant recipient for CMV since administering CMV- negative blood products to all patients [XI. A lymphopro- liferative disorder associated with an Epstein-Barr virus infection developed in 1 patient and was successfully treated by reduction in immunosuppression. Our data suggest that induction therapy with monoclonal antibod- ies is safe and efficacious in the pediatric age group and in the neonatal age group in particular. However, the degree of immunocompetence and the level of immunosuppres- sion needed in these patients are issues that cannot be answered at present and await further study.
All but 2 donors weighed more than the respective recipient. Univariate analysis demonstrated a donor to recipient weight ratio of greater than 1.9 adversely affects survival, as has been similarly suggested by Costanzo- Nordin and associates (221. In our four operative deaths, the weight ratio exceeded 2.5, although three of these oversized hearts were easily accommodated in the recip- ient mediastinum. In the fourth case, the sternum could not be closed in part because of myocardial edema. One can speculate that excessive cardiac output, as seen with relatively larger donor hearts [23], may paradoxically contribute to severe pulmonary vasospasm in patients with reactive pulmonary vasculature. Other consider- ations may relate to volume displacement of the lungs or left ventricular compression leading to dysfunction and an increase in the transpulmonary gradient. We have not made intentional efforts to ”oversize” donor hearts, as our high donor to recipient weight ratio is merely a function of the lack of neonatal organ donors. We have previously accepted any heart from a donor up to 350% greater than the recipient weight; however, in light of these data, we have more recently refused hearts from donors with ratios greater than 2.5.
In conclusion, orthotopic cardiac transplantation has become a frequently used therapeutic option in infants and children with CCHD not amenable or poorly amena- ble to palliative or corrective procedures currently avail- able and those with end-stage cardiomyopathies. Infants and children appear to tolerate intense immunosuppres- sion without substantial detriment, and in our series, triple-drug therapy appears advantageous for allograft survival even in the neonatal age group. With the excep- tion of a few children in this series, all patients have demonstrated improvement on the growth scales.
Although the long-term results have yet to be deter- mined, we believe that cardiac transplantation for select congenital pediatric cardiac pathology results in lower operative mortality and improved medium-term survival than occur with current techniques of surgical repair. Pediatric patients with idiopathic cardiomyopathies can
expect the same excellent results as the adult patient population.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Kriett JM, Kaye MP. The Registry of the International Society for Heart and Lung Transplantation: eighth official report- 1991. J Heart Lung Transplant 1991;10:491-8. Bailey LL, Nelson-Cannarella SL, Doroshow RW. Cardiac allotransplantation in newborns as therapy for hypoplastic left heart syndrome. N Engl J Med 1986;315:949-51. Bailey LL, Assaad AN, Trimm RF, et al. Orthotopic trans- plantation during infancy as therapy for incurable congenital heart disease. Ann Surg 1988;208:279-86. Mayer JE, Perry S, OBrien P, et al. Orthotopic heart trans- plantation for complex congenital heart disease. ] Thorac Cardiovasc Surg 1990;99:484-92. Pennington DG, Noedel N, McBride LR, Naunheim KS, Ring WS. Heart transplantation in children: an international sur- vey. Ann Thorac Surg 1991;52:710-5. Mavroudis C, Harrison HL. Perspectives in infant orthotopic cardiac transplantation. Cardiac Surg: State Art Rev 1989;3: 331-54. Bailey L, Concepcion W, Shattuck H, Huang L. Method of heart transplantation for treatment of hypoplastic left heart syndrome. J Thorac Cardiovasc Surg 1986;92:1-5. Allard M, Assaad A, Bailey L, et al. Session IV: Surgical techniques in pediatric heart transplantation. J Heart Lung Transplant 1991;10(Suppl 2):80%27. Pennington DG, Sarafian J, Swartz M. Heart transplantation in children. J Heart Transplant 1985;4:441-5. Reitz BA, Jamieson SW, Gaudiani VA, Oyer PE, Stinson EB. Method for cardiac transplantation in corrected transposition of the great arteries. J Cardiovasc Surg (Torino) 1982;23: 2 9 s . Macoviak JA, Baldwin JC, Ginsburg R, et al. Orthotopic cardiac transplantation for univentricular heart. Ann Thorac Surg 1988;45:85-6. Harjula ALJ, Heikkila LJ, Nieminen MS, Kupari M, Keto P, Mattila SP. Heart transplantation in repaired transposition of the great arteries. Ann Thorac Surg 1988;46:6114. Doty DB, Renlund DG, Caputo GR, Burton NA, Jones KW. Cardiac transplantation in situs inversus. J Thorac Cardio- vasc Surg 1990;99:493-9. Chartrand C. Pediatric cardiac transplantation despite atrial and venous anomalies. Ann Thorac Surg 1991;52:716-21. Menkis AH, McKenzie FN, Novick RJ, et al. Expanding applicability of transplantation after multiple prior palliative procedures. Ann Thorac Surg 1991;52:7224. Meliones JN, Snider R, Bove EL, Rosenthal A, Rosen DA. Longitudinal results after first-stage palliation for hypoplastic left heart syndrome. Circulation 1990;82(Suppl 4):1514. Bove EL. Transplantation after first-stage reconstruction for hypoplastic left heart syndrome. Ann Thorac Surg 1991;52: 701-7. Fricker FJ, Griffith BP, Hardesty RL, et al. Experience with heart transplantation in children. Pediatrics 1987;79:138-46. Backer CL, Zales VR, ldriss FS, et al. Heart transplantation in neonates and children. J Heart Lung Transplant 1992;ll:
Costanzo-Nordin MR, Swinnen LJ, Fisher SG, et al. Cyto- megalovirus infections in heart transplant recipients: rela-
31 1-9.
tionship to immunosuppression. J Heart Lung Transplant 1992;11:83746. O’Donnell JA, Turrentine MW, Kesler KA, et al. Modification of cytomegalovirus risk in cardiac transplantation. Circula- tion 1992;86(Suppl 1):1-38. Costanzo-Nordin MR, Liao Y, Grusk BB, et al. Oversizing of donor hearts: beneficial or detrimental? J Heart Lung Trans- plant 1991;10:777-30. Reichart B. Size matching in heart transplantation. J Heart Lung Transplant 1992;11:5199-202.

554 TURRENTINE ET AL PEDIATRIC CARDIAC TRANSPLANTATION
Ann Thorac Surg 1994;57:54&54
DISCUSSION
DR STEVEN R. GUNDRY (Loma Linda, CA): I extend the congratulations of the Loma Linda group to Dr Turrentine and his co-authors. It has been said that we must have some secret ingredient either in our water or in our smog in Loma Linda to produce our superb results. It is very gratifying to see that another fine center can produce equally good results with these difficult children. I think Dr Turrentine has very nicely shown that this is exceptional therapy, particularly for failed complex palliative operations, and the degree of detail in the manuscript is excellent. I will review briefly our most recent experience.
We recently examined the first 111 patients having transplan- tation for hypoplastic left heart syndrome and compared them with patients who died waiting at the Loma Linda University Medical Center or elsewhere on our transplant list. Almost all of these children do die while waiting if a heart transplant cannot be found. Recently, however, and this is a tribute to our neonatol- ogists, we have performed transplantation in infants at 5 and 6 months of age who had hypoplastic left heart syndrome and were on the waiting list for a donor heart. In our overall 5-year experience to date, the 5-year survival rate for patients who have had transplantation is 81%. There have been no late deaths, and when the 27 children who died while waiting are added, the 5-year survival is 61%, which I think is better than that with most palliative operations.
As you know, one of the highlights of the Loma Linda program has been the avoidance of steroids, and I believe this is reflected in the growth and development of these children. My first question to Dr Turrentine and associates concerns their experi- ence with steroids as a triple-drug immunosuppression therapy. Dr Turrentine, what have the growth and development in your patients been in terms of normal pediatric growth charts? Our patient population reveals normal growth and development over a 30-month period for both boys and girls. There is always some concern about circulatory arrest for repair of these complex lesions, but head growth has been 94% normal in this group, and 89% of the surviving infants remain neurologically normal.
I have three other questions. Doctor Turrentine mentioned the use of prophylactic OKT3 for 14 days. We have studied an earlier cohort of patients in whom we compared antithymocyte serum and OKT3. We found an increased incidence of late rejection in the OKT3 group and a problem with pulmonary hypertension early in the postoperative period. Could OKT3 have contributed to any of the episodes of pulmonary hypertension in the present series?
The manuscript stated that Dr Turrentine and associates had some difficulty using hearts more than 350% larger than the recipient. We have been able to place hearts up to 440% larger and have not noticed a problem with big hearts in terms of rejection or mortality. I wonder if Dr Turrentine has a comment on this.
Finally, how long can you wait? According to the manuscript, the Indiana group has now started doing a Norwood procedure at 2 months because of pulmonary hypertension.
DR TURRENTINE: I thank Drs Cooley and Gundry for review- ing our manuscript and Dr Gundry for his generous remarks. The
first two questions he asked are the subject of a discussion currently being prepared for the Loma Linda Conference on Pediatric Heart Transplantation to be held in March 1993. For that presentation, we will demonstrate the growth patterns of our children based on preoperative and most recent postoperative growth indices. With few exceptions, the patients in each cate- gory have demonstrated stable or improved growth on standard growth charts in both the height and weight categories. Higher gains were made in the weight category, presumably because of steroids, and a large number of these children do not otherwise exhibit the other external stigmata of steroid use.
The type and the incidence of OKT3 reactions in children have mimicked those in the adult experience of most centers. Approx- imately one third of patients exhibit a “shake and bake” reaction or a change in hemodynamics early after the first and second doses, whereas another third have a flulike syndrome, which lasts between 2 and 4 days. Several of our children in whom pulmonary artery catheters were placed at the time of transplan- tation did demonstrate an approximate 50% elevation of the systolic pulmonary pressure from baseline after administration of OKT3, a rise that was transient.
The patients who died early postoperatively of pulmonary hypertension had more significant risk factors for hypertensive crisis than OKT3 administration. These factors included trans- plantation within the first 2 weeks of life and unrestricted left-to-right shunting for a period of greater than 2 months. Doctor Gundry has stated that they have been able to wait as long as 4 to 5 months before doing transplantation in some of their babies with hypoplastic left heart syndrome; our experience suggests that major irreversible pulmonary vasculopathy may occur within 2 to 4 months in patients with unrestricted left-to- right pulmonary blood flow. Therefore, we elect to proceed with a first-stage Norwood procedure in infants who have not been offered a suitable heart within the first 1 to 2 months of life and then either proceed with the second-stage Norwood or relist the patient for transplantation.
We experienced several problems with the use of oversized donor hearts, particularly in children who had undergone a previous mediastinal operation. We found these chests were not nearly as compliant and able to accommodate larger hearts compared with the chests of patients who had not had previous mediastinal procedures. We have been able to transplant hearts from donors at least 350% larger by weight than the recipient with techniques such as division of the posterior pericardium and opening of the left pleura. Occasionally, the sternum cannot be closed immediately after transplantation, and this must be ac- complished a few days later. Although technically possible, we have found that there is a significant increase in mortality in patients who receive hearts from donors with a greater than 250% increase in body weight. Consequently, we have tended to use hearts from donors less than 2.5 times the body weight of the recipient.
Related Documents











