CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014 MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina 1 ELEMENTS OF CARDIAC FUNCTION I) CARDIAC ACTION POTENTIAL PHASE ACTION POTENTIAL OF THE VENTRICLES, ATRIA AND PURKINJ E FIBERS ACTION POTENTIAL OF THE CONDUCTION SYSTEM FAST RESPONSE (Atria, Ventricles, Purkinje fibers) SLOW RESPONSE (SA node & AV node) 4 Resting membrane potential due to outward diffusion of potassium (via voltage gated channels) - electrolytes are found in areas where they are not originally found Q: What ions do you have inside the cardiac myocyte during resting membrane potential? A: Calcium and Sodium Slow depolarization Responsible for the pacemaker activity or automaticity of the SA node and AV node due to inward movement of sodium (via funny channels) - slow upstroke - Unique characteristic: there is automatic firing of action potential Q: What will happen to the heart rate when phase 4 is suppressed? A: there will be a slower heart rate - Bradycardia Q: What will happen to the heart rate when phase 4 is enhanced? A: there will be a faster heart rate - Tachycardia 0 Depolarization due to influx of sodium via fast sodium channels - rapid upstroke - HYPONATREMIA (low levels of serum sodium) oDecreased depolarization oLesser amplitude at phase 0 (decreased upstroke); cell depolarization is slower leading to diminished action potential and slow conduction velocity. Thus, the patient manifests BRADYCARDIA Upstroke; Depolarization caused by inward movement of calcium (via L-type calcium channels) - CALCIUM CHANNEL BLOCKERS (verapamil and diltiazem) and HYPOCALCEMIA o the upstroke will be reduced, the action will proceed at a slower pace, slower heart rate- BRADYCARDIA 1 Initial repolarization due to transient efflux of potassium None

Cardiac physiology dr. dominguez (oct 21-24, 2014)
Aug 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
1
ELEMENTS OF CARDIAC FUNCTION
I) CARDIAC ACTION POTENTIAL
PHASE ACTION POTENTIAL OF THE VENTRICLES,
ATRIA AND PURKINJE
FIBERS
ACTION POTENTIAL OF THE CONDUCTION SYSTEM
FAST RESPONSE
(Atria, Ventricles, Purkinje fibers)
SLOW RESPONSE
(SA node & AV node)
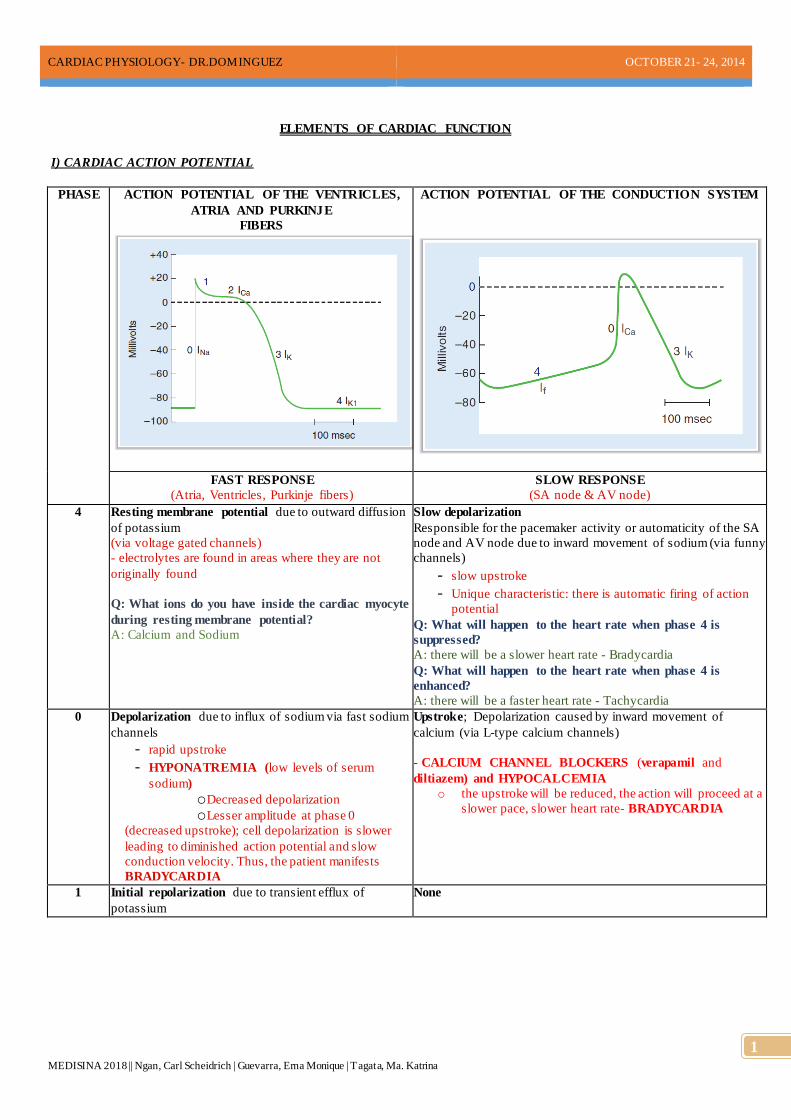
4 Resting membrane potential due to outward diffusion
of potassium
(via voltage gated channels)
- electrolytes are found in areas where they are not
originally found
Q: What ions do you have inside the cardiac myocyte
during resting membrane potential?
A: Calcium and Sodium
Slow depolarization
Responsible for the pacemaker activity or automaticity of the SA
node and AV node due to inward movement of sodium (via funny
channels)
- slow upstroke
- Unique characteristic: there is automatic firing of action
potential
Q: What will happen to the heart rate when phase 4 is
suppressed?
A: there will be a slower heart rate - Bradycardia
Q: What will happen to the heart rate when phase 4 is
enhanced?
A: there will be a faster heart rate - Tachycardia
0 Depolarization due to influx of sodium via fast sodium
channels
- rapid upstroke
- HYPONATREMIA (low levels of serum
sodium)
oDecreased depolarization
oLesser amplitude at phase 0
(decreased upstroke); cell depolarization is slower
leading to diminished action potential and slow
conduction velocity. Thus, the patient manifests
BRADYCARDIA
Upstroke; Depolarization caused by inward movement of
calcium (via L-type calcium channels)
- CALCIUM CHANNEL BLOCKERS (verapamil and
diltiazem) and HYPOCALCEMIA
o the upstroke will be reduced, the action will proceed at a
slower pace, slower heart rate- BRADYCARDIA
1 Initial repolarization due to transient efflux of
potassium
None
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
2
2 Plateau phase due to entry of calcium
(via L-type Calcium channels)
- unique for cardiac action potential
- allow ventricles to fill in with blood
- Beta blockers –prevent the entry of Ca
- efflux of K – but balanced by entry of Na
None
3 Repolarization due to efflux of potassium
- Class III anti arrhythmics- delay repolarization
Repolarization due to efflux of potassium
-Class III anti arrhythmics- delay repolarization
** RESTORATION OF IONIC CONCENTRATIONS**
Q: WHAT WILL ESTABLIS H THE CORRECT IONIC GRADIENT?
A:
1. Na-K-ATPase Pump: allows movement of Sodium out of the cell and Potassium into the cell
2. 3Na-1Ca Antiporter: facilitates calcium efflux
*These are very important because if Calcium and Sodium will stay inside the cell and potassium outside the cell, then no cardiac
action potential will be generated.
*In patients with MYOCARDIAL INFARCTION:
o Na-K-ATPase pump is impaired (it doesn’t work properly)
o Phase 4 is affected
o The resting membrane potential becomes more negative, requiring a longer time to reach threshold. Therefore the
myocardium will not contract properly.
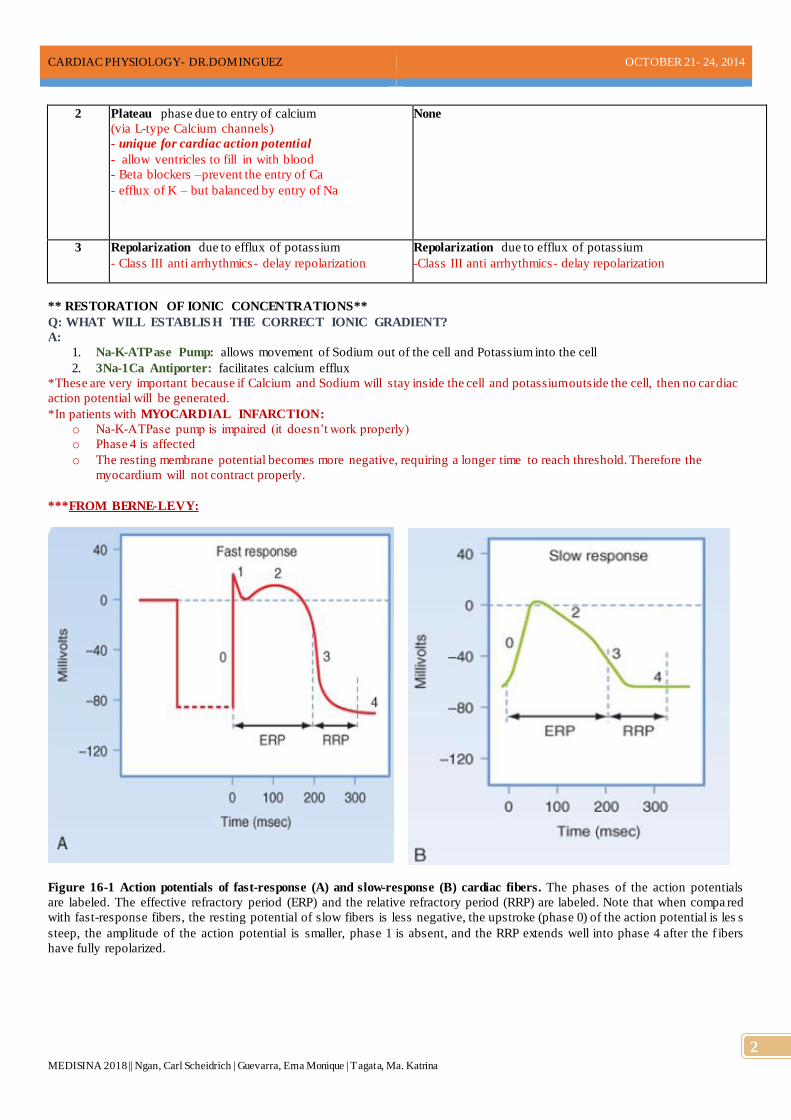
***FROM BERNE-LEVY:
Figure 16-1 Action potentials of fast-response (A) and slow-response (B) cardiac fibers. The phases of the action potentials
are labeled. The effective refractory period (ERP) and the relative refractory period (RRP) are labeled. Note that when compa red
with fast-response fibers, the resting potential of slow fibers is less negative, the upstroke (phase 0) of the action potential is les s
steep, the amplitude of the action potential is smaller, phase 1 is absent, and the RRP extends well into phase 4 after the f ibers
have fully repolarized.
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
3
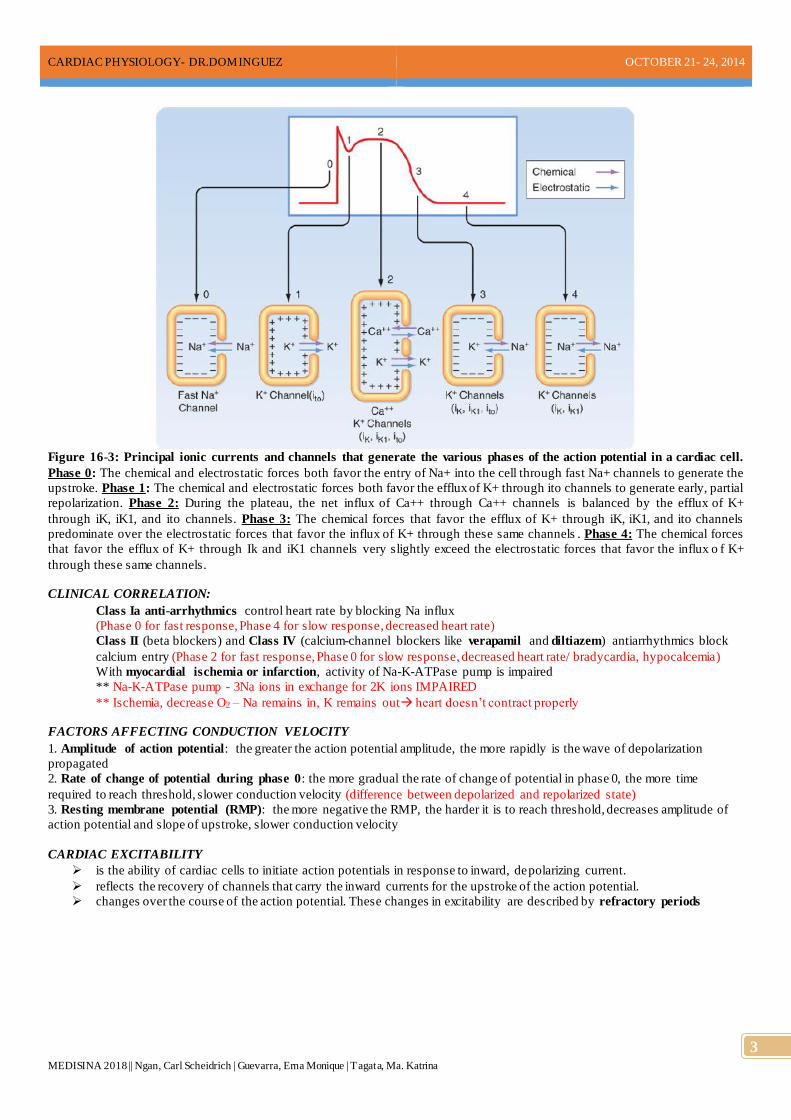
Figure 16-3: Principal ionic currents and channels that generate the various phases of the action potential in a cardiac cell.
Phase 0: The chemical and electrostatic forces both favor the entry of Na+ into the cell through fast Na+ channels to generate the
upstroke. Phase 1: The chemical and electrostatic forces both favor the efflux of K+ through ito channels to generate early, partial
repolarization. Phase 2: During the plateau, the net influx of Ca++ through Ca++ channels is balanced by the efflux of K+
through iK, iK1, and ito channels. Phase 3: The chemical forces that favor the efflux of K+ through iK, iK1, and ito channels
predominate over the electrostatic forces that favor the influx of K+ through these same channels . Phase 4: The chemical forces
that favor the efflux of K+ through Ik and iK1 channels very slightly exceed the electrostatic forces that favor the influx o f K+
through these same channels.
CLINICAL CORRELATION:
Class Ia anti-arrhythmics control heart rate by blocking Na influx
(Phase 0 for fast response, Phase 4 for slow response, decreased heart rate)
Class II (beta blockers) and Class IV (calcium-channel blockers like verapamil and diltiazem) antiarrhythmics block
calcium entry (Phase 2 for fast response, Phase 0 for slow response, decreased heart rate/ bradycardia, hypocalcemia)
With myocardial ischemia or infarction, activity of Na-K-ATPase pump is impaired
** Na-K-ATPase pump - 3Na ions in exchange for 2K ions IMPAIRED
** Ischemia, decrease O2 – Na remains in, K remains out heart doesn’t contract properly
FACTORS AFFECTING CONDUCTION VELOCITY
1. Amplitude of action potential: the greater the action potential amplitude, the more rapidly is the wave of depolarization
propagated
2. Rate of change of potential during phase 0: the more gradual the rate of change of potential in phase 0, the more time
required to reach threshold, slower conduction velocity (difference between depolarized and repolarized state)
3. Resting membrane potential (RMP): the more negative the RMP, the harder it is to reach threshold, decreases amplitude of
action potential and slope of upstroke, slower conduction velocity
CARDIAC EXCITABILITY
is the ability of cardiac cells to initiate action potentials in response to inward, depolarizing current.
reflects the recovery of channels that carry the inward currents for the upstroke of the action potential.
changes over the course of the action potential. These changes in excitability are described by refractory periods
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
4
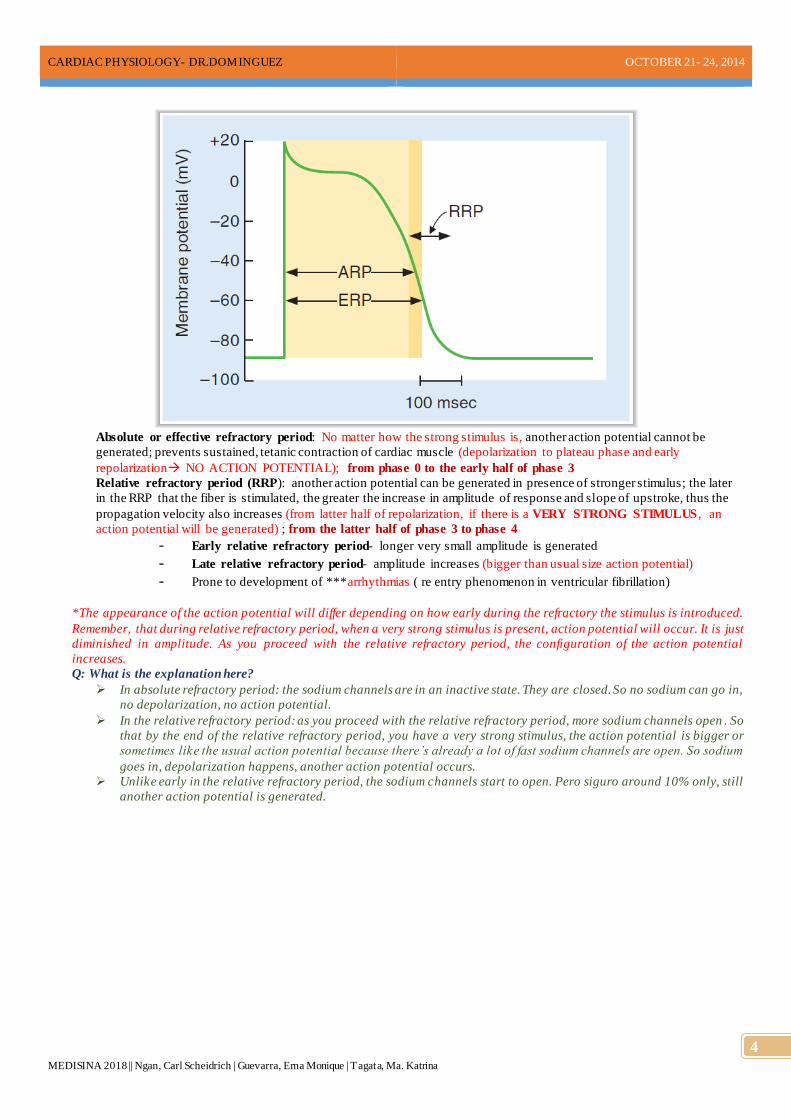
Absolute or effective refractory period: No matter how the strong stimulus is, another action potential cannot be
generated; prevents sustained, tetanic contraction of cardiac muscle (depolarization to plateau phase and early
repolarization NO ACTION POTENTIAL); from phase 0 to the early half of phase 3
Relative refractory period (RRP): another action potential can be generated in presence of stronger stimulus; the later
in the RRP that the fiber is stimulated, the greater the increase in amplitude of response and slope of upstroke, thus the
propagation velocity also increases (from latter half of repolarization, if there is a VERY STRONG STIMULUS , an
action potential will be generated) ; from the latter half of phase 3 to phase 4
- Early relative refractory period- longer very small amplitude is generated
- Late relative refractory period- amplitude increases (bigger than usual size action potential)
- Prone to development of ***arrhythmias ( re entry phenomenon in ventricular fibrillation)
*The appearance of the action potential will differ depending on how early during the refractory the stimulus is introduced.
Remember, that during relative refractory period, when a very strong stimulus is present, action potential will occur. It is just
diminished in amplitude. As you proceed with the relative refractory period, the configuration of the action potential
increases.
Q: What is the explanation here?
In absolute refractory period: the sodium channels are in an inactive state. They are closed. So no sodium can go in,
no depolarization, no action potential.
In the relative refractory period: as you proceed with the relative refractory period, more sodium channels open . So
that by the end of the relative refractory period, you have a very strong stimulus, the action potential is bigger or
sometimes like the usual action potential because there’s already a lot of fast sodium channels are open. So sodium
goes in, depolarization happens, another action potential occurs.
Unlike early in the relative refractory period, the sodium channels start to open. Pero siguro around 10% only, still
another action potential is generated.

CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
5
** FROM BERNE-LEVY:
Figure 16-15 Effects of excitation at various times after the initiation of an action potential in a slow response fiber . In this
fiber, excitation very late in phase 3 (or early in phase 4) induces a small, nonpropagated (local) response (a). Later in phase 4, a
propagated response (b) can be elicited, but its amplitude is small and the upstroke is not very steep; this response is cond ucted
very slowly. Still later in phase 4, full excitability is regained, and the response (c) displays normal characteristics.
Q: Which of these three will have the slowest conduction velocity?
A: The first. So conduction is longer here.
- In arrhythmias, if the conduction is longer, there is a trend in the development of arrhythmias. SO if
any arrhythmia will occur, it will be early here (refer to the figure) because the conduction of this action potential
will take longer.
- If the conduction velocity is slow, that heart is prone to arrhythmias.
****The same thing also happens with your SA node and AV node. Same principle including the generation of action
potentials during relative refractory period.
II) CARDIAC CONDUCTION
one-way conduction: SA node to AV node to AV bundle (bundle of His) to right and left bundle branches to Purkinje
fibers
: the heart is an inverted triangle, base is up and apex is down
Spread of depolarization is from endocardium to epicardium (apex to base)

CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
6
Automaticity – self-excitation; ability to initiate its own beat
Rhythmicity – regularity of pacemaking activity
***Right ventricle contracts first because it is less muscular
** ISCHEMIA/ BYPASS TRACTS: cause retrograde conduction of pathways
** ATRIA and FIBROUS TISSUES: prevent retrograde conduction of pathways
SA node (fires at normal heart rate 60-100 bpm)
Pacemaker of the heart- controls rate of beating of the entire heart
With greatest automaticity and rhythmicity (highest firing rate)
Sympathetic response:
Steeper phase 4
SA node more permeable to sodium and calcium, increased heart rate
Faster conduction velocity
Less negative membrane potential: reach threshold easily
Threshold potential is same with normal
Parasympathetic/ Vagal response:
Reduced slope in phase 4
SA node more permeable to potassium, decreased heart rate
Reach threshold slowly: slower firing rate
***Anti arrythmics – increase threshold – SA node fire slowly
AV node (fires 40 to <60 bpm)
Delay in impulse conduction at the AV node to allow complete emptying of blood from atria to ventricles; with
constant ERP protecting ventricle from excessive firing even in the presence of premature excitations of atria
Ventricular conduction
via bundle branches and Purkinje fibers; rapid transmission of action potential for synchronized and immediate
contraction of thick-walled ventricles
FACTORS AFFECTING THE PACEMAKER ACTIVITY OF THE HEART
Factors Sympathetic Nervous System Parasympathetic Nervous System
Rate of Depolarization (phase 4) SA node is more permeable to Na+ and
Ca2+ (faster)
SA node more permeable to K+ (slower)
*rate of depolarization is directly proportional to the pacemaker potential; if depolarization rapidly occurs, you have a steeper
phase 4 , the threshold will be reached earlier, you’ll have increased heart rate
Maximal Negativity
(phase 4)
Less negative (faster) More negative (slower)
*less negative easier to reach threshold easier to fire action potential
Threshold Potential
*Increased threshold potential difficult to reach threshold longer time to fire AP slower heart rate
Beta agonists (salbutamol) Beta blockers
(-olol’s)
**no P wave- SA node not firing
**if SA node not functioning, AV node takes over (40-59 bpm)
**if AV node not functioning, Purkinje fibers take over (15-30 bpm)
CLINICAL CORRELATION
1. Sympathetic effect: increased permeability to Na and Ca thus increasing slope of slow diastolic depolarization
- More positive RMP of SA node
- Increased rate of SA node discharge
- Increased rate of conduction and excitability of A-V node
- Increased force of contraction
*SA node more permeable to Na and Ca FASTER
2. Parasympathetic effect/ increased vagal activity: increased permeability to potassium thus hyperpolarizing pacemaker cell
membrane and reducing slope of slow diastolic depolarization
*SA node more permeable to K (goes out) MAXIMAL NEGATIVITY
3. Quinidine and procainamide (antiarrhythmics) – raise threshold value to less negative values
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
7
OVERDRIVE SUPPRESSION
-protective mechanism in SA node
e.g.
SA node fires too much (must be controlled) SA node overdrive Na-K-ATPase activity enhanced Na goes out, K gets
in membrane potential: more negative (hyperpolarization) maximal negativity slow diastolic depolarization suppressed
automaticity
***Na-K-ATPase in SA node and AV node re-establish Ionic gradient. When established, Na goes into the cell via “FUNNY
CHANNELS” AUTOMATIC FIRING
** “AV node” traffic light: regulates impulses from atria to ventricles
***Refractory period in Purkinje fibers longer than other system problem with arrythmias
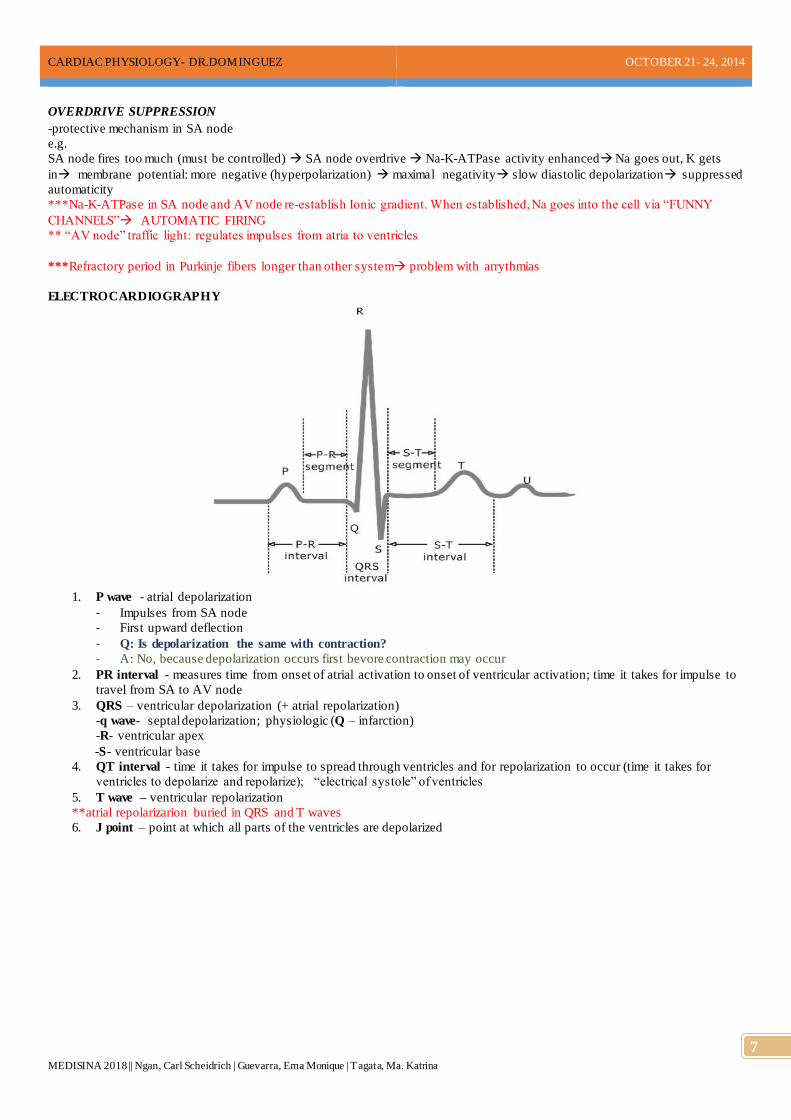
ELECTROCARDIOGRAPHY
1. P wave - atrial depolarization
- Impulses from SA node
- First upward deflection
- Q: Is depolarization the same with contraction?
- A: No, because depolarization occurs first bevore contraction may occur
2. PR interval - measures time from onset of atrial activation to onset of ventricular activation; time it takes for impulse to
travel from SA to AV node
3. QRS – ventricular depolarization (+ atrial repolarization)
-q wave- septal depolarization; physiologic (Q – infarction)
-R- ventricular apex
-S- ventricular base
4. QT interval - time it takes for impulse to spread through ventricles and for repolarization to occur (time it takes for
ventricles to depolarize and repolarize); “electrical systole” of ventricles
5. T wave – ventricular repolarization
**atrial repolarizarion buried in QRS and T waves
6. J point – point at which all parts of the ventricles are depolarized
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
8
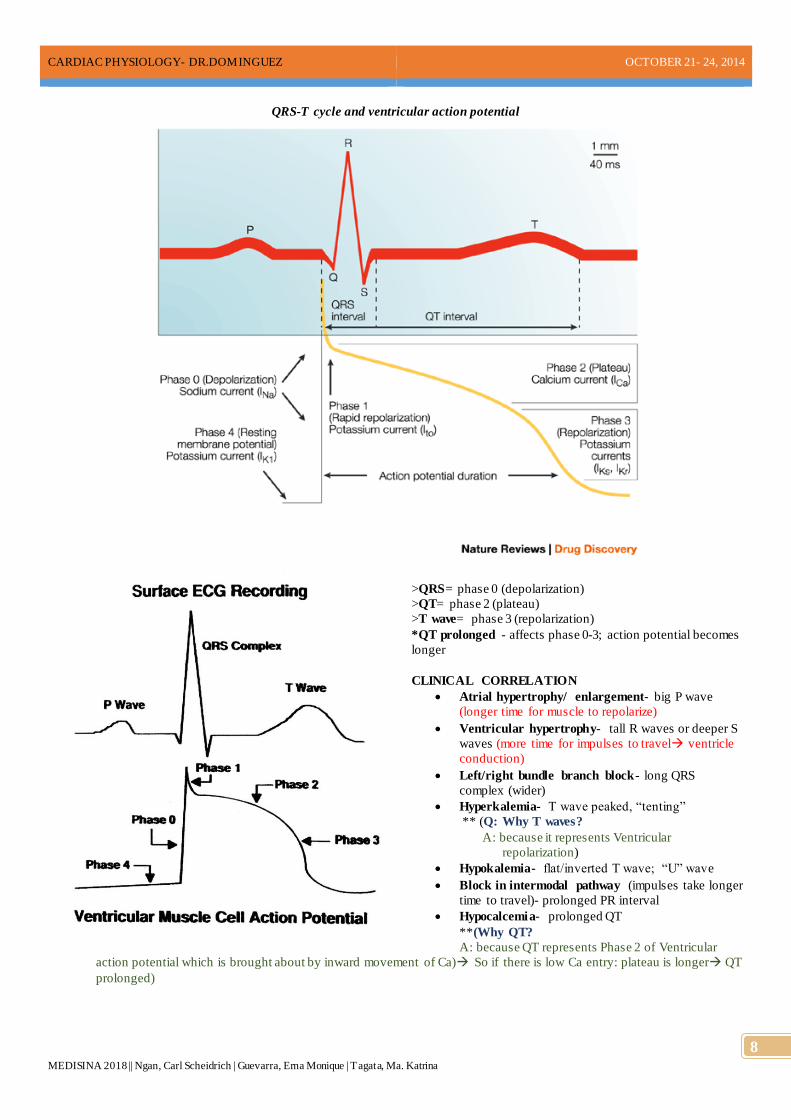
QRS-T cycle and ventricular action potential
>QRS= phase 0 (depolarization)
>QT= phase 2 (plateau)
>T wave= phase 3 (repolarization)
*QT prolonged - affects phase 0-3; action potential becomes
longer
CLINICAL CORRELATION
Atrial hypertrophy/ enlargement- big P wave
(longer time for muscle to repolarize)
Ventricular hypertrophy- tall R waves or deeper S
waves (more time for impulses to travel ventricle
conduction)
Left/right bundle branch block- long QRS
complex (wider)
Hyperkalemia- T wave peaked, “tenting”
** (Q: Why T waves?
A: because it represents Ventricular
repolarization)
Hypokalemia- flat/inverted T wave; “U” wave
Block in intermodal pathway (impulses take longer
time to travel)- prolonged PR interval
Hypocalcemia- prolonged QT
**(Why QT?
A: because QT represents Phase 2 of Ventricular
action potential which is brought about by inward movement of Ca) So if there is low Ca entry: plateau is longer QT
prolonged)
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
9
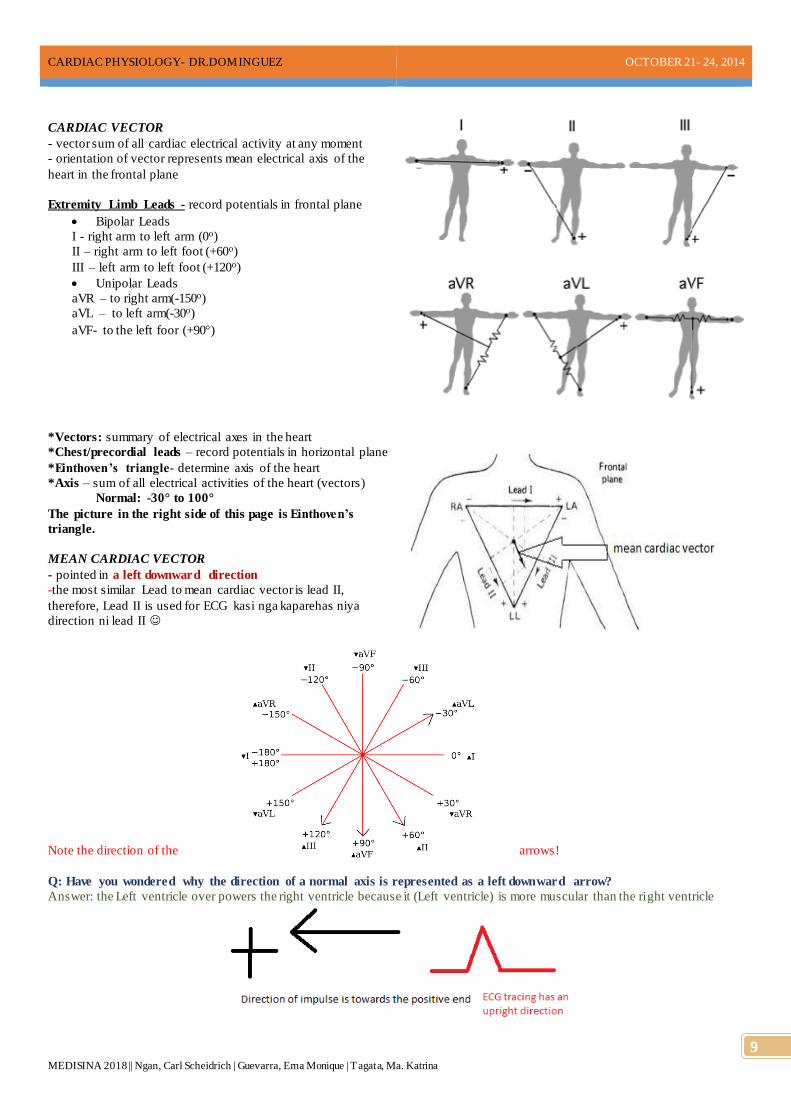
CARDIAC VECTOR
- vector sum of all cardiac electrical activity at any moment
- orientation of vector represents mean electrical axis of the
heart in the frontal plane
Extremity Limb Leads - record potentials in frontal plane
Bipolar Leads
I - right arm to left arm (0o)
II – right arm to left foot (+60o)
III – left arm to left foot (+120o)
Unipolar Leads
aVR – to right arm(-150o)
aVL – to left arm(-30o)
aVF- to the left foor (+90)
*Vectors: summary of electrical axes in the heart
*Chest/precordial leads – record potentials in horizontal plane
*Einthoven’s triangle- determine axis of the heart
*Axis – sum of all electrical activities of the heart (vectors)
Normal: -30° to 100°
The picture in the right side of this page is Einthoven’s
triangle.
MEAN CARDIAC VECTOR
- pointed in a left downward direction
-the most similar Lead to mean cardiac vector is lead II,
therefore, Lead II is used for ECG kasi nga kaparehas niya
direction ni lead II
Note the direction of the arrows!
Q: Have you wondered why the direction of a normal axis is represented as a left downward arrow?
Answer: the Left ventricle over powers the right ventricle because it (Left ventricle) is more muscular than the right ventricle
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
10
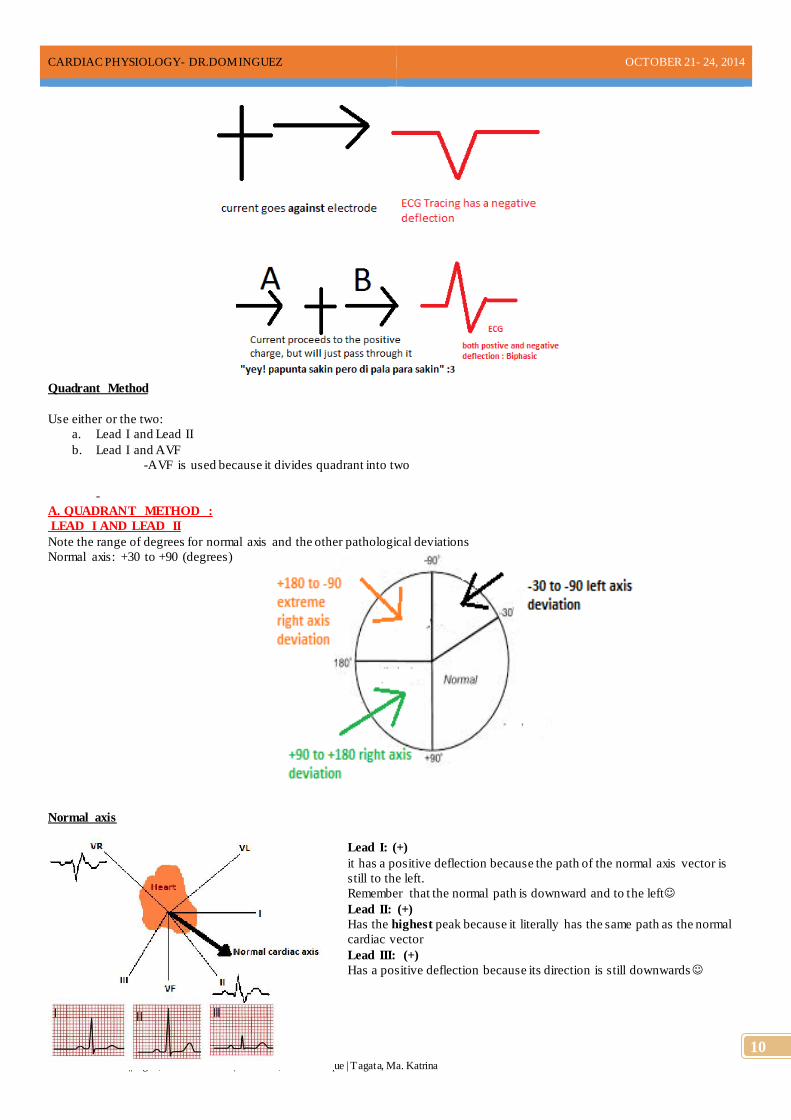
Quadrant Method
Use either or the two:
a. Lead I and Lead II
b. Lead I and AVF
-AVF is used because it divides quadrant into two
-
A. QUADRANT METHOD :
LEAD I AND LEAD II
Note the range of degrees for normal axis and the other pathological deviations
Normal axis: +30 to +90 (degrees)
Normal axis
Lead I: (+)
it has a positive deflection because the path of the normal axis vector is
still to the left.
Remember that the normal path is downward and to the left
Lead II: (+)
Has the highest peak because it literally has the same path as the normal
cardiac vector
Lead III: (+)
Has a positive deflection because its direction is still downwards

CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
11
Left axis deviation
Lead I: (+)
the ECG has a s positive deflection because the Left axis deviation (LAD)
vector still travels to the left, but the height is short because the LAD vector
travels upward(opposite to the normal axis, which is downard)
Lead II: (-)
Still has a short positive deflection because the LAD vector is still towards the
left, but it also has a tall negative deflection because the LAD vector is
upwards. (total opposite of normal axis)
Characterized as biphasic: has both positive and negative deflection
Lead III: (-)
Biphasic wave, but has a taller negative deflection because the LAD vector
travels opposite the normal axis vector
Right Axis Deviation
Lead I:
vector of the right axis deviation(RAD) is entirely opposite to the normal
axis vector, that is why It has a tall negative peak
Lead II:
Biphasic or positive
RAD Vector goes to the right , that is why it has a short negative
deflection, but at the same time the RAD vector travels downwards, that
is why it has a positive deflection
Lead III:
Has a positive deflection because the RAD vector is downwards
But also has a negative deflection because the vector is towards the right
Note: positive deflection> negative deflection
Extreme right axis deviation
Lead I, Lead II, and Lead III:
All negative because the extreme right axis deviation is the
total opposite of the normal axis.
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
12
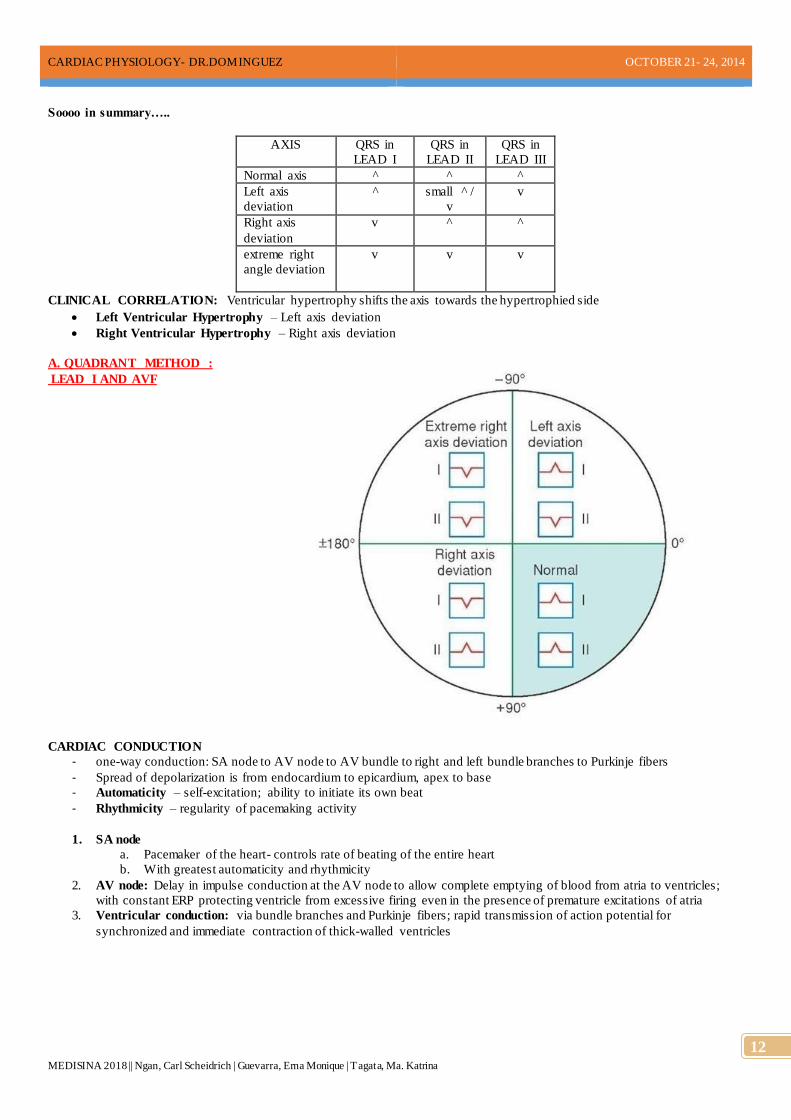
Soooo in summary…..
AXIS QRS in
LEAD I
QRS in
LEAD II
QRS in
LEAD III
Normal axis ^ ^ ^
Left axis
deviation
^ small ^ /
v
v
Right axis
deviation
v ^ ^
extreme right
angle deviation
v v v
CLINICAL CORRELATION: Ventricular hypertrophy shifts the axis towards the hypertrophied side
Left Ventricular Hypertrophy – Left axis deviation
Right Ventricular Hypertrophy – Right axis deviation
A. QUADRANT METHOD :
LEAD I AND AVF
CARDIAC CONDUCTION
- one-way conduction: SA node to AV node to AV bundle to right and left bundle branches to Purkinje fibers
- Spread of depolarization is from endocardium to epicardium, apex to base
- Automaticity – self-excitation; ability to initiate its own beat
- Rhythmicity – regularity of pacemaking activity
1. SA node
a. Pacemaker of the heart- controls rate of beating of the entire heart
b. With greatest automaticity and rhythmicity
2. AV node: Delay in impulse conduction at the AV node to allow complete emptying of blood from atria to ventricles;
with constant ERP protecting ventricle from excessive firing even in the presence of premature excitations of atria
3. Ventricular conduction: via bundle branches and Purkinje fibers; rapid transmission of action potential for
synchronized and immediate contraction of thick-walled ventricles

CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
13
Mechanism of Arrhythmia
I: alterations in impulse initiation
A.Ectopic pacemakers- regions in the heart other than SA node initiating beats
-Mechanisms:
1. Enhanced own rhythmicity
-e.g sinus tachycardia (automaticity of the Sa node, P waves are present)
2. Depressed rhythmicity of higher-order pacemakers
-In the event that the SA node(60-100beats/min) will not function here are the elements of conduction that will take over
*1st to take over: AV node (40-59 beats/min)
*2nd : purkinje fibers: (15-39 beats/min)
*3rd: ventricles: <15 beats/min
-If there is a P wave, the SA node is still functional and is the pace maker of the heart
-Absent P wave: AV node is the one that takes over, or presence of other pacemakers
3. Block in pathways between ectopic focus and pacemaker
e.g. 3rd degree AV block, complete AV block. There is a P wave, but the QRS do not follow. The QRS is fired by the purkinje
fibers, so there are more P waves than QRS’s.
Triggered automaticity:
-dependent on AP
2 mechanisms:
a. Early After Depolarization (EAD):
-Occurs when heart rate is low
-Main mechanism:
Reactivation of L type Ca2+ channels
(even at late phase (2 or 3))
More Ca2+ goes into the cell
Prolonged phase 3 OR
Trigger another AP early in phase 3
Late repolarization of the cell
Therefore: depolarize at a later time
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
14
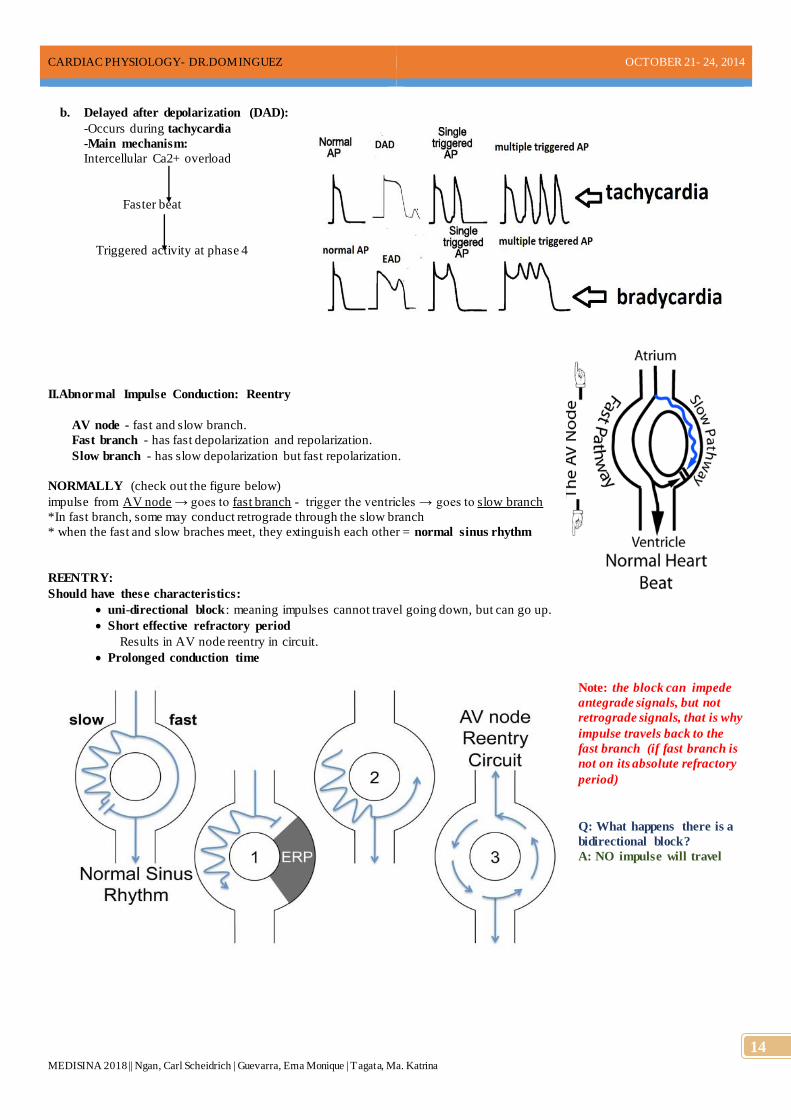
b. Delayed after depolarization (DAD):
-Occurs during tachycardia
-Main mechanism:
Intercellular Ca2+ overload
Faster beat
Triggered activity at phase 4
II.Abnormal Impulse Conduction: Reentry
AV node - fast and slow branch.
Fast branch - has fast depolarization and repolarization.
Slow branch - has slow depolarization but fast repolarization.
NORMALLY (check out the figure below)
impulse from AV node → goes to fast branch - trigger the ventricles → goes to slow branch
*In fast branch, some may conduct retrograde through the slow branch
* when the fast and slow braches meet, they extinguish each other = normal sinus rhythm
REENTRY:
Should have these characteristics:
uni-directional block: meaning impulses cannot travel going down, but can go up.
Short effective refractory period
Results in AV node reentry in circuit.
Prolonged conduction time
Note: the block can impede
antegrade signals, but not
retrograde signals, that is why
impulse travels back to the
fast branch (if fast branch is
not on its absolute refractory
period)
Q: What happens there is a
bidirectional block?
A: NO impulse will travel
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
15
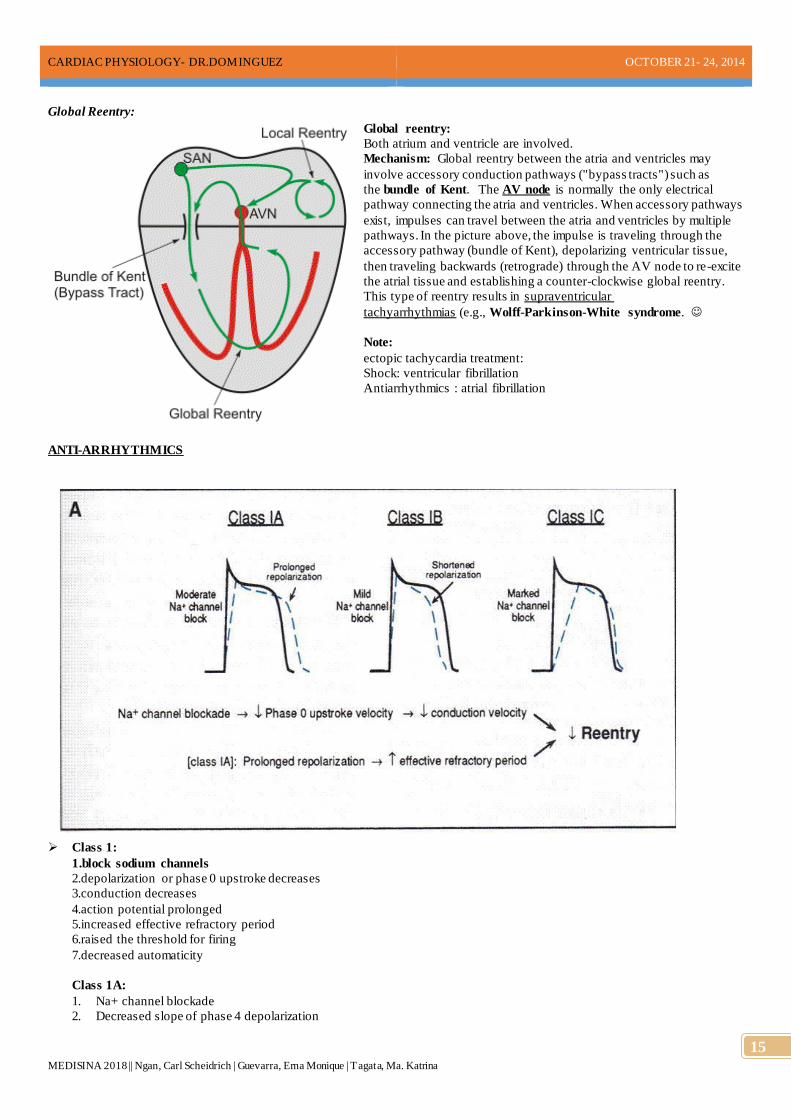
Global Reentry:
Global reentry:
Both atrium and ventricle are involved.
Mechanism: Global reentry between the atria and ventricles may
involve accessory conduction pathways ("bypass tracts") such as
the bundle of Kent. The AV node is normally the only electrical
pathway connecting the atria and ventricles. When accessory pathways
exist, impulses can travel between the atria and ventricles by multiple
pathways. In the picture above, the impulse is traveling through the
accessory pathway (bundle of Kent), depolarizing ventricular tissue,
then traveling backwards (retrograde) through the AV node to re-excite
the atrial tissue and establishing a counter-clockwise global reentry.
This type of reentry results in supraventricular
tachyarrhythmias (e.g., Wolff-Parkinson-White syndrome.
Note:
ectopic tachycardia treatment:
Shock: ventricular fibrillation
Antiarrhythmics : atrial fibrillation
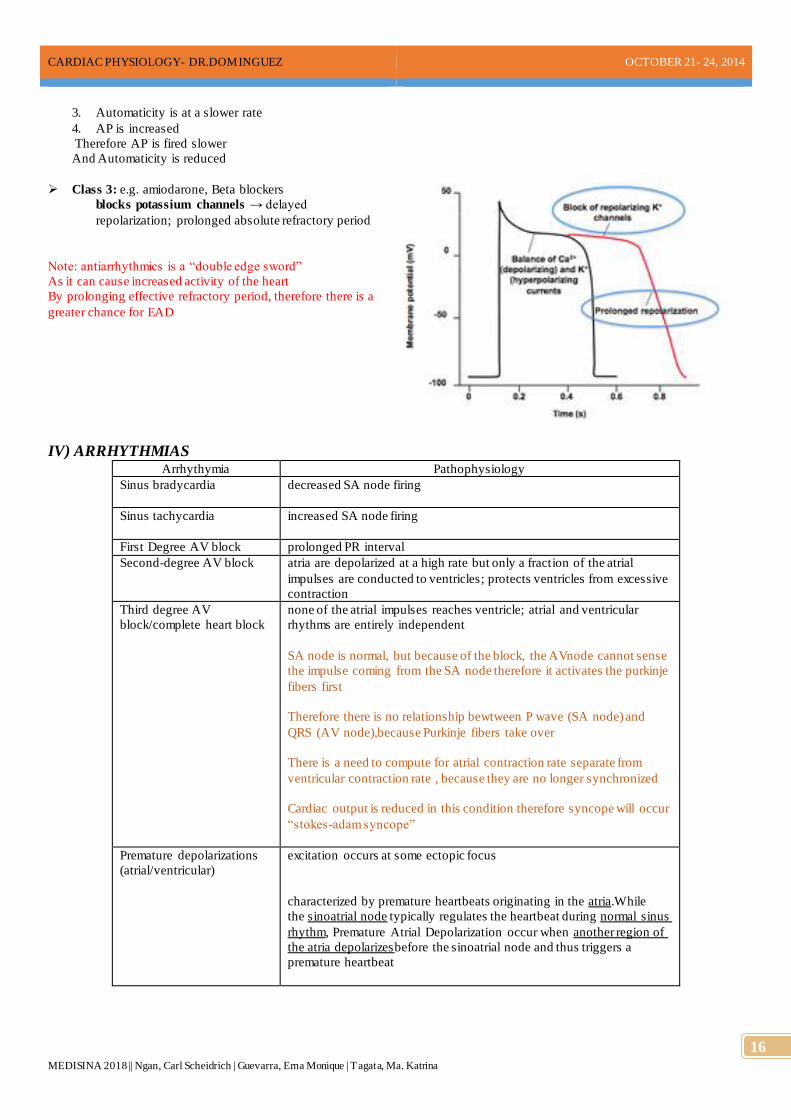
ANTI-ARRHYTHMICS
Class 1:
1.block sodium channels
2.depolarization or phase 0 upstroke decreases
3.conduction decreases
4.action potential prolonged
5.increased effective refractory period
6.raised the threshold for firing
7.decreased automaticity
Class 1A:
1. Na+ channel blockade
2. Decreased slope of phase 4 depolarization
CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
16
3. Automaticity is at a slower rate
4. AP is increased
Therefore AP is fired slower
And Automaticity is reduced
Class 3: e.g. amiodarone, Beta blockers
blocks potassium channels → delayed
repolarization; prolonged absolute refractory period
Note: antiarrhythmics is a “double edge sword”
As it can cause increased activity of the heart
By prolonging effective refractory period, therefore there is a
greater chance for EAD
IV) ARRHYTHMIAS Arrhythymia Pathophysiology
Sinus bradycardia decreased SA node firing
Sinus tachycardia increased SA node firing
First Degree AV block prolonged PR interval
Second-degree AV block atria are depolarized at a high rate but only a fraction of the atrial
impulses are conducted to ventricles; protects ventricles from excessive
contraction
Third degree AV
block/complete heart block
none of the atrial impulses reaches ventricle; atrial and ventricular
rhythms are entirely independent
SA node is normal, but because of the block, the AVnode cannot sense
the impulse coming from the SA node therefore it activates the purkinje
fibers first
Therefore there is no relationship bewtween P wave (SA node) and
QRS (AV node),because Purkinje fibers take over
There is a need to compute for atrial contraction rate separate from
ventricular contraction rate , because they are no longer synchronized
Cardiac output is reduced in this condition therefore syncope will occur
“stokes-adam syncope”
Premature depolarizations
(atrial/ventricular)
excitation occurs at some ectopic focus
characterized by premature heartbeats originating in the atria.While
the sinoatrial node typically regulates the heartbeat during normal sinus
rhythm, Premature Atrial Depolarization occur when another region of
the atria depolarizesbefore the sinoatrial node and thus triggers a
premature heartbeat

CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
17
abnormally shaped P wave. Since the premature beat initiates outside
the sinoatrial node, the associated P wave appears different from those
seen in normal sinus rhythm. Typically, the atrial impulse propagates
normally through the atrioventricular node and into the cardiac
ventricles, resulting in a normal, narrow QRS complex.
Premature Ventricular Contraction
heartbeat is initiated by Purkinje fibres in the ventricles rather than by
the sinoatrial node
QRS Looks bizaare
Fibrillation (Atrial or
ventricular)
reentry phenomenon; premature impulse arrives during vulnerable
period of cardiac cycle ( downslope of T wave); during this period,
excitability of cardiac cells varies ( some in ERP, others fully
recovered, others able to conduct impulses). As region of cardiac cells
becomes excitable again, it is ultimately reentered by one of the wave
fronts travelling around chamber, hence process is self-sustaining

CARDIAC PHYSIOLOGY- DR.DOMINGUEZ OCTOBER 21- 24, 2014
MEDISINA 2018 || Ngan, Carl Scheidrich | Guevarra, Erna Monique | Tagata, Ma. Katrina
18
V) CARDIAC CYCLE
Ventricular Filling
1. Rapid ventricular filling: AV valves open due to higher pressures in atria; ventricular volumes start to increase rapidly
2. Diastasis or reduced ventricular filling: reduced ventricular filling since increasing volume in ventricles results to equ ilibrating
pressures in atria and ventricles
3. Atrial systole: ventricular pressures start to increase greater than atrial pressures, thus atria have to contract to empty remaining
blood in atria into ventricles
Isovolumic Contraction
-AV valve and semilunar valve is close
-no change in volume in the ventricles
-because there is a lot of blood in the ventricles, there is increased pressure, blood has no way out, the ventricles are “tensed”
>>>>The phase between the start of ventricular systole and opening of the semilunar valves (when ventricular pressure rises
abruptly)is called the isovolumic (literally, “same volume”) contraction period. This term is appropriate because ventricular
volume remains constant during this brief period The onset of isovolumic contraction also coincides with the peak of the R wa ve
on an ECG, initiation of the first heart sound, and the earliest rise in ventricular pressure on the ventricular pressure curve after
atrial contraction.
Period of Ejection
- LV pressure is at its maximum
- Semilunar valves open
- Blood pours out of ventricles via great arteries
- left ventricle has to exceed pressure in aorta so that the ventricle can pump blood out of the aorta
Isovolumic Relaxation
- The period between closure of the semilunar valves and opening of the AV valves is termed isovolumic relaxation. It is
characterized by a precipitous fall in ventricular pressure without a change in ventricular volume.
-semilunar valves close (2nd heart sound)
- AV valves are still closed
-atria fills up with blood
Arterial pressure is higher than ventricles
-at the end of isovolumic relaxations, valves open and blood goes to the ventricles, ventricle filling occurs
-atria starts to fill with blood
Clinical correlation:
In patients with heart failure, the ventricles do not contract normally, therefore blood in the ventricles is increased by the blood
given to it by the atria and atria contracts more because it still wants to give blood to the ventricles, this is seen as the a wave.
Atrial contraction for patients with heart failure accounts for 30% of cardiac output.... This is beneficial for the patient
Left atrial pressure curve
1. a wave – rise in pressure caused by atrial contraction
2. c wave - caused by impact of common carotid artery with adjacent jugular vein and to some extent by abrupt closure of
the tricuspid valve in early ventricular systole
3. v wave – rise in pressure associated with atrial filling
A Video has been posted regarding the Cardiac Cycle.
DETERMINANTS OF MYOCARDIAL CONTRACTILITY
1. Preload – force that stretches relaxed muscle fibers
- Also refers to the blood that enters the heart
2. Afterload – force against which contracting muscle must overcome
If arterial pressure is increase, the myocardial muscles will initially increase its contraction to overcome the increased pressure
from the arteries, but as time goes by, the heart will suffer and enlarge(hypertrophy), leading to decreased myocardial contraction
*Stroke volume = amount of blood pumped per beat
*Cardiac output = stroke volume/minute (multiply with heart rate)
*INDEX OF CONTRACTILITY: Ejection fraction
Measured through 2D echo
↓ ejection fraction: failure
Related Documents