Accepted Manuscript Cardiac autonomic responses induced by mental tasks and the influence of musical auditory stimulation Juliana Cristina Barbosa, Heraldo L. Guida, Anne M. G Fontes, Ana M. S Antonio, Luiz Carlos de Abreu, Viviani Barnabé, Renata S. Marcomini, Luiz Carlos M. Vanderlei, Meire L. da Silva, Vitor E. Valenti PII: S1744-3881(14)00034-6 DOI: 10.1016/j.ctcp.2014.04.001 Reference: CTCP 526 To appear in: Complementary Therapies in Clinical Practice Received Date: 28 November 2013 Revised Date: 14 April 2014 Accepted Date: 15 April 2014 Please cite this article as: Barbosa JC, Guida HL, Fontes AMG, Antonio AMS, de Abreu LC, Barnabé V, Marcomini RS, Vanderlei LCM, da Silva ML, Valenti VE, Cardiac autonomic responses induced by mental tasks and the influence of musical auditory stimulation, Complementary Therapies in Clinical Practice (2014), doi: 10.1016/j.ctcp.2014.04.001. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Accepted Manuscript
Cardiac autonomic responses induced by mental tasks and the influence of musicalauditory stimulation
Juliana Cristina Barbosa, Heraldo L. Guida, Anne M. G Fontes, Ana M. S Antonio,Luiz Carlos de Abreu, Viviani Barnabé, Renata S. Marcomini, Luiz Carlos M.Vanderlei, Meire L. da Silva, Vitor E. Valenti
PII: S1744-3881(14)00034-6
DOI: 10.1016/j.ctcp.2014.04.001
Reference: CTCP 526
To appear in: Complementary Therapies in Clinical Practice
Received Date: 28 November 2013
Revised Date: 14 April 2014
Accepted Date: 15 April 2014
Please cite this article as: Barbosa JC, Guida HL, Fontes AMG, Antonio AMS, de Abreu LC, BarnabéV, Marcomini RS, Vanderlei LCM, da Silva ML, Valenti VE, Cardiac autonomic responses induced bymental tasks and the influence of musical auditory stimulation, Complementary Therapies in ClinicalPractice (2014), doi: 10.1016/j.ctcp.2014.04.001.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTCardiac autonomic responses induced by mental tasks and the influence of musical
auditory stimulation
Juliana Cristina Barbosa1, Heraldo L. Guida2, Anne M. G. Fontes1, Ana M. S. Antonio4,
Luiz Carlos de Abreu3, Viviani Barnabé5, Renata S. Marcomini2, Luiz Carlos M.
Vanderlei4, Meire L. da Silva2, Vitor E. Valenti*2
1Centro de Estudos do Sistema Nervoso Autônomo (CESNA), Departamento de
Fonoaudiologia and 2Departamento de Fisioterapia e Terapia Ocupacional, Faculdadede
Filosofia eCiências, UNESP. Av. Hygino Muzzi Filho, 737. 17525-900 Marília, SP,
Brasil.2Departamento de Morfologia e Fisiologia, Faculdade de Medicinado ABC. Av.
Príncipe de Gales, 821. 09060-650 Santo André, SP, Brasil.4Programa de Pós-
Graduação em Fisioterapia, Faculdade de Ciências e Tecnologia, UNESP.Rua Roberto
Simonsen, 305. 19060-900 Presidente Prudente, SP, Brasil. 5Department of
Environmental Health, Harvard Medical School of Public Health.665 Huntington Ave,
II-219 Boston, MA 02115, EUA.
*Corresponding author:
Departamento de Fonoaudiologia
Faculdadede Filosofia eCiências, UNESP.
Av. HyginoMuzzi Filho, 737.
17525-900. Marília, SP, Brasil.
E-mail: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTAcknowledgement
The study was performed at UNESP. We thank Dr. Hani Atrashfor kindly reviewing
English Grammar and Spelling. We also appreciate the Proof-reading-service® for
language editing services.
Conflict of interest
The authors declare no conflict of interest.
Role of the funding source
The study received financial support from FAPESP.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTCardiac autonomic responses induced by mental tasks and the influence of musical
auditory stimulation
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTAbstract
We investigated the acute effects of musical auditory stimulation on cardiac
autonomic responses to a mental task in 28 healthy men (18–22 years old). In the
control protocol (no music), the volunteers remained at seated rest for 10 minutes and
the test was applied for five minutes. After the end of test the subjects remained seated
for five more minutes. In the music protocol, the volunteers remained at seated rest for
10 minutes, then were exposed to music for 10 minutes; the test was then applied over
five minutes, and the subjects remained seated for five more minutes after the test. In
the control and music protocols the time domain and frequency domain indices of heart
rate variability remained unchanged before, during and after the test. We found that
musical auditory stimulation with baroque music did not influence cardiac autonomic
responses to the mental task.
Keywords: Cardiovascular system; Autonomic nervous system; Hearing

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTINTRODUCTION
The possibility that musical auditory stimulation could serve as a form of non-
pharmacological therapy has been proposed in the literature,1–3 and some styles of
music were observed to influence the cardiovascular and autonomic nervous systems.4
Previous studies in music, psychology, and medicine have suggested the anxiolytic
effects of musical auditory stimulation. These effects have been investigated for self-
selected versus experimenter-selected music and for different music styles.1-4 The
physiological responses to specific music are important to comprehend and could
provide further information concerning alternative and complementary therapies.
It is widely known that cardiac autonomic regulation can be analysed by
measuring heart rate variability (HRV).5-8 This measurement evaluates the oscillations
of consecutive heart beats (RR intervals), which are affected by the autonomic nervous
system’s influence on the heart or, more specifically, on the sinus node. Increased HRV
is an indicator of good adaptation, and is observed in healthy subjects. Reduced HRV,
on the other hand, is usually a sign of abnormal and inadequate adaptation of the
autonomic nervous system, indicating physiological dysfunction.5 HRV can be analysed
in the time domain (SDNN: standard deviation of normal-to-normal R-R intervals;
pNN50: the percentage of adjacent RR intervals with a difference of duration greater
than 50ms; and, RMSSD: root-mean square of differences between adjacent normal RR
intervals in a time interval) and in the frequency domain (LF: low frequency; HF: high
frequency; and, LF/HF ratio).6 It has been observed that different styles of music can
increase or decrease HRV.7, 8
In this sense, cardiac autonomic regulation may be tested through autonomic tests
such as postural change manoeuvres, pressor cold tests and mental tasks. These tests are
important means of diagnosing autonomic dysfunction.9

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTOne study indicated that music therapy improved HRV indices in the time and
frequency domains in patients with breast cancer treated with an antitumoral cardiotoxic
medications.7 Another study showed that previous exposure to musical auditory
stimulation attenuated cardiac autonomic response induced by postural change
manoeuvre in women.8 However, other studies indicated that music intensifies the
endocrine and stress responses induced by a mental task.10 Therefore, it is currently
unclear whether and how cardiac autonomic response is affected by exposure to music.
Understanding the physiological mechanisms involved in cardiac autonomic responses
under music influence could help to better understand the role of music on
complementary therapies in clinical practice. Therefore, this study aimed to investigate
the effects of a baroque musical auditory stimulation on cardiac autonomic responses
induced by a mental task.
METHOD
Study Population
Subjects were 28 healthy male students, all non-smokers, aged between 18 and 22 years
old. All volunteers were informed about the procedures and the objectives of the study
and gave written informed consent. All study procedures were approved by the Ethics
Committee in Research of the Faculty of Sciences of the Universidade Estadual
Paulista, Campus of Marilia (No. CEP-2011-385), and were in accordance with
Resolution 196/96 National Health 10/10/1996.
Exclusion criteria included body mass index (BMI) >35 kg/m2; systolic blood
pressure (SBP) >140 mmHg or diastolic blood pressure (DBP) >90 mmHg (at rest);
cardiac arrhythmias (atrial flutter or fibrillation, multiple ventricular or atrial ectopy,

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTsecond or third degree atrioventricular block); smoking, left ventricular dysfunction;
reported neurological or respiratory disorders; and, relevant auditory disorders.
Initial Evaluation
Baseline information collected included: age, gender, weight, height and body mass
index (BMI). Weight was determined using a digital scale (W 200/5, Welmy, Brazil)
with a precision of 0.1 kg. Height was determined using a stadiometer (ES 2020, Sanny,
Brazil) with a precision of 0.1 cm and 2.20 m of extension. Body mass index (BMI) was
calculated as weight / height2, with weight in kilograms and height in meters.
HRV analysis
The R-R intervals recorded by the portable HR monitor (with a sampling rate of 1000
Hz) were downloaded to the Polar Precision Performance program (v. 3.0, Polar
Electro, Finland). The software enabled the visualization of HR and the extraction of a
cardiac period (R-R interval) file in “txt” format. Following digital filtering
complemented with manual filtering for the elimination of premature ectopic beats and
artefacts, at least 256 R–R intervals were used for the data analysis. Only series with
sinus rhythm greater than 95% were included in the study.11,12 HRV was analysed
during four time periods: the 10-minute period before the test without exposure to
music, the 10-minute period before the test with exposure to music, the five-minute
period during the test and the five-minute period after the test. The geometric indices of
HRV were evaluated. For calculation of the indices, we used HRV Analysis software
(Kubios HRV v.1.1 for Windows, Biomedical Signal Analysis Group, Department of
Applied Physics, University of Kuopio, Finland).
Linear indices of HRV
To analyze HRV in the frequency domain, the low frequency (LF =0.04–0.15 Hz) and
high frequency (HF = 0.15–0.40 Hz) spectral components were used in ms2 and

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTnormalized units (nu), representing a value relative to each spectral component in
relation to the total power minus the very low frequency (VLF) components, and the
ratio between these components (LF/HF). The spectral analysis was calculated using the
Fast Fourier Transform algorithm.13
The analysis in the time domain was performed in terms of SDNN (standard
deviation of normal-to-normal R-R intervals), pNN50 (percentage of adjacent RR
intervals with a difference of duration greater than 50 ms) and RMSSD (root-mean
square of differences between adjacent normal RR intervals in a time interval).14
The mental arithmetic overload test
The task consisted of mental arithmetic operations involving two- and three-
digit numbers (i.e. 287 + 24 - 43/3 + 28) administered continuously over a period of five
minutes. The test had to be performed without verbal stimulation.15 (Supplemental
files).
Measurement of the auditory stimulation
Measurements of the equivalent sound levels were conducted in a soundproof
room using a SV 102 audiodosimeter (Svantek, Poland). The device was programmed
to take measurements in the "A" weighting circuit with a slow response.
The measurement was made during the 10-minute session of relaxing classical
baroque music. An insert-type microphone (MIRE - Microphone In Real Ear) was
placed inside the auditory canal of the subject, just below the speaker, which was
connected to a personal stereo.
Before each measurement, the microphone was calibrated with an acoustic CR:
514 model calibrator (Cirrus Research plc).
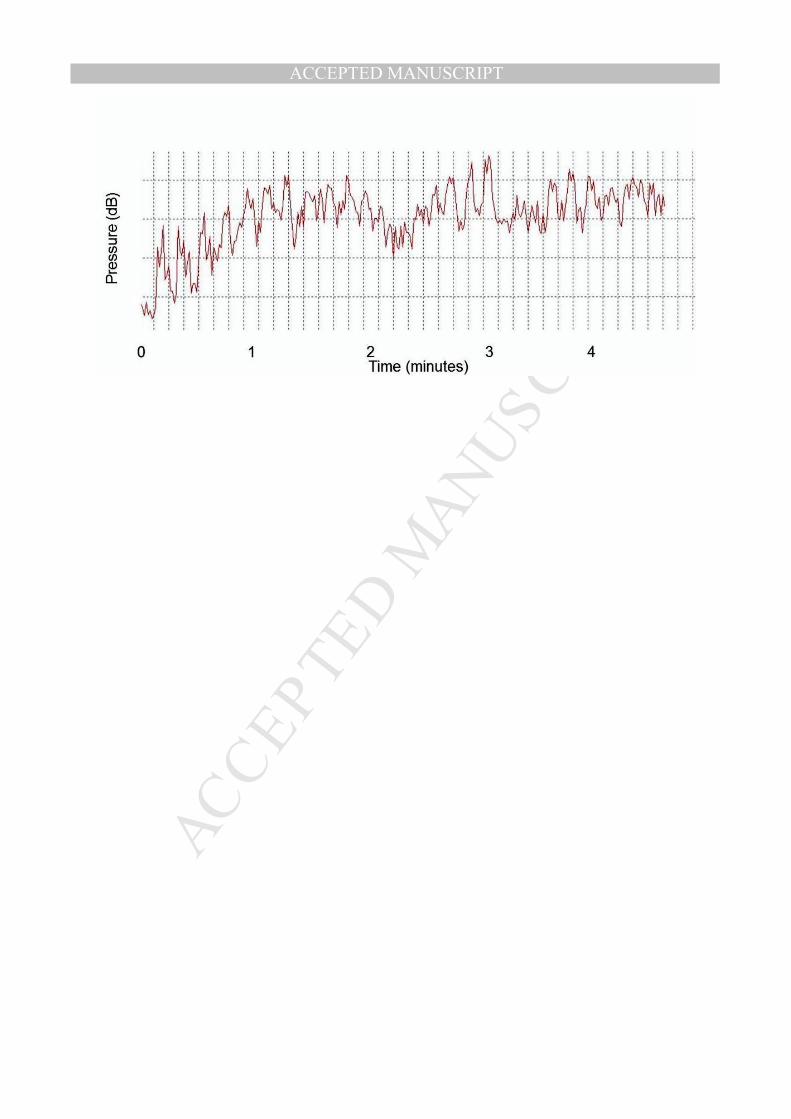
For the analysis, we used Leq (A), which is defined as the equivalent sound
pressure level and which corresponds to the constant sound level in the same time

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTinterval. It contains the same total energy as the sound. We also analyzed the frequency
spectrum of the sound stimulation (octave band). The music ranged from 63-84 dB.
(Figure 1).16,17
Protocol
Data collection was carried out in the same soundproof room for all volunteers;
the temperature was between 21°C and 25°C and the relative humidity was between 50
and 60%. Volunteers were instructed not to drink alcohol or caffeine for 24 hours before
the evaluation. Data were collected on an individual basis, always between 6 and 9 PM
to standardize the protocol. All procedures necessary for the data collection were
explained to each subject separately, and the subjects were instructed to remain at rest
and avoid talking during the collection.
After the initial evaluation, a heart monitor belt was placed over the thorax,
aligned with the distal third of the sternum, and the Polar RS800CX heart rate receiver
(Polar Electro) was placed on the wrist. The equipment had previously been validated
for monitoring heart rate beat-by-beat, as had the use of these data for HRV analysis.
In the control protocol (n=28), after placement of the strap and the monitor,
subjects were seated and remained at rest with spontaneous breathing for 10 minutes
with the earphones turned off. Subsequently, the subjects performed the mental
arithmetic overload test. In the music protocol (n=28), the volunteers were seated and
remained at rest with spontaneous breathing for 10 minutes with the earphones turned
off; then the earphones were turned on and the volunteers were exposed to musical
auditory stimulation before the mental arithmetic test. The sequence of exposition was
randomized for each individual and the mental arithmetic test was based on different
calculations for each protocol.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTHRV was analyzed in the following periods: control protocol – the 10-minutes
period before the test without exposure to music, the five-minutes period during the test
and the five-minutes period after the test; music protocol – the 10-minutes period before
the test without exposure to music, the 10-minutes period before the test with exposure
to music, the five-minutes period during the test and the five-minutes period after the
test. The subjects were exposed to classical music in the baroque style (Pachelbel:
Canon in D). This music was selected because a recent study from our laboratory
observed that this style influenced HRV responses to orthostatic change maneuver.8
Statistical Analysis
Standard statistical methods were used to calculate the means and standard
deviations. The Shapiro-Wilk test was performed to evaluate the distributions. For
parametric distributions we applied ANOVA for repeated measures followed by the
Bonferroni posttest. For non-parametric distributions we used the Friedman test
followed by Dunn’s posttest. Differences were considered significant when the
probability of a Type I error was less than 5% (p < 0.05). We used GraphPadStatMate
software version 2.00 for Windows (GraphPad Software, San Diego, CA, USA).
RESULTS
Data on baseline systolic (SAP) and diastolic arterial pressure (DAP), heart rate
(HR) and mean RR interval, age, height, body weight and body mass index (BMI) are
presented in Table 1.
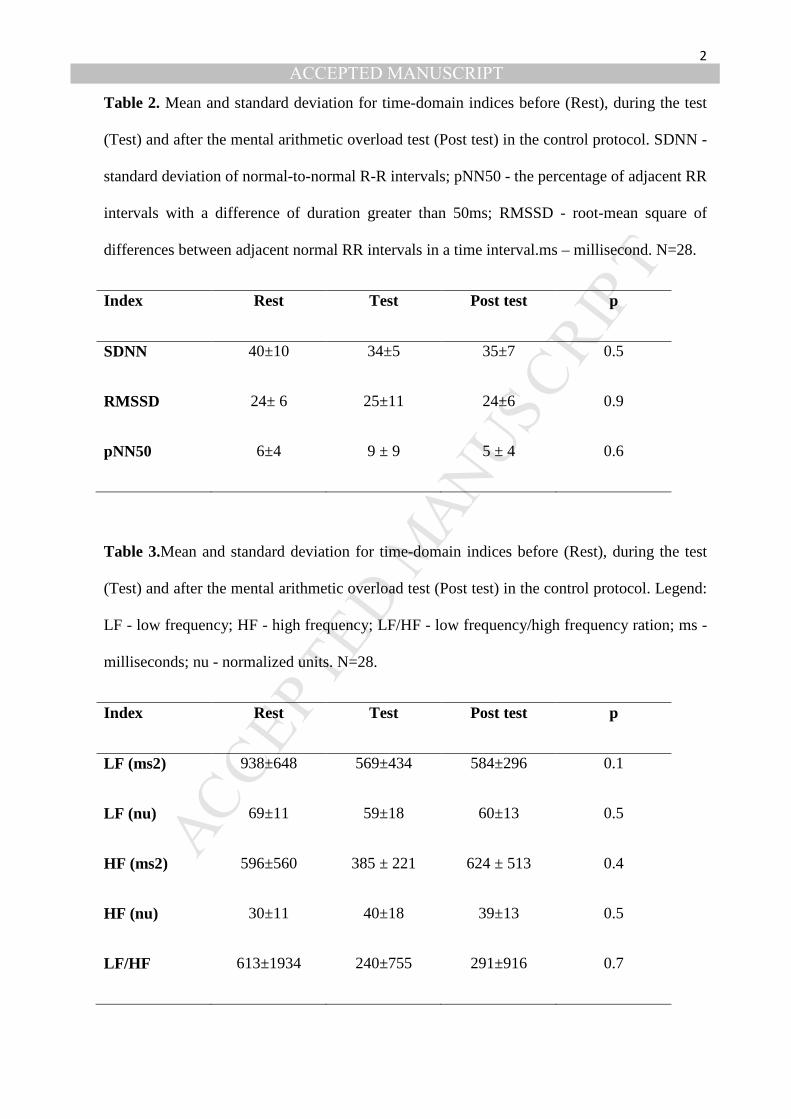
Results related to the rest period before the test (Rest), the mental arithmetic
overload test itself (Test) and the period after the test (Post-test) in the control protocol
are presented in Table 2. The SDNN, RMSSD and pNN50 indices were not changed. In
addition, neither the LF and HF in absolute (ms2) and normalized (nu) units nor the

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTLF/HF ratio exhibited significant responses induced during or after the mental test
(Table 3).
Table 4 displays data on the time domain indices in the Rest, Test and Post-test
periods in the music protocol. As in the control group, the SDNN, pNN50 and RMSSD
indices were not different before, during or after the test compared to the values
obtained for the control group during the Rest period.
In relation to the frequency domain indices (LF and HF in absolute (ms2) and
normalized (nu) units as well as LF/HF ratio), no significant responses were induced by
musical auditory stimulation in the music protocol either during or after the mental test
(Table 5).
DISCUSSION
Based on the use of self-selected and experimenter-selected music for alternative
and complementary therapies,1-4 this investigation was undertaken to evaluate changes
in cardiac autonomic modulation induced by a mental task through the well-known
mental arithmetic overload test15 and to determine whether auditory stimulation with the
experimenter-selected baroque music influences this response. The hypothesized effect
of the music on the cardiac autonomic regulation induced by the test was a late increase
in sympathetic modulation on the heart and a parasympathetic decrease.15 In actual fact,
no significant HRV responses were induced by the mental arithmetic overload test in
either the control or the music protocol. Our findings do not provide evidence to
indicate Pachelbel music for musical therapy, since it did not induce significant changes
in cardiac autonomic regulation.
Although some indices almost reached statistical significance in the music
protocol, tending toward a reduction in the parasympathetic modulation of the heart
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTduring the mental task, we failed to observe a significant effect on the cardiac
autonomic response to the mental arithmetic overload test. Among the previous studies
in this area, most have emphasized either mental load or physical load, while only a few
have considered both. In this context, HRV has been widely used to investigate
reactions to mental demands on the autonomic nervous system.18 In this study, HRV
values in the time and frequency domains were compared before, during and after a
mental task, because HRV is sensitive to alterations in mental state.6 The mental task
was expected to reduce the HF power of the heartbeat interval time series and to affect
other indices that correspond to the parasympathetic modulation of the heart, such as
pNN50 and RMSSD, as mentioned above.19 Nevertheless, no significant changes were
observed in those indices during or after the mental task used in this study compared to
the values before the task. It may be surmised that the mental arithmetic overload test
used in this study does not cause significant stimulation of HRV. A previous study
indicated that the addition of mental tasks to a physical computer task did not cause an
additional effect on the HRV parameters related to autonomic modulation. This may
mean that while physical demands have a major influence on HRV responses, the effect
of this type of mental task is not significant.18
In the music protocol, there was no change in the HRV indices during the music
or during or after the mental task. A recent study found that music had a significant
effect on the cardiac autonomic response to a postural change maneuver.9 It was
observed that auditory stimulation with the same music used in this investigation
(Pachelbel’s Canon in D) attenuated the reaction induced by the postural change
manoeuvre in women: in the music protocol, the HRV indices were not different from
those in the seated position, while in the control protocol this manoeuvre caused
significant changes in HRV, i.e. reduction of pNN50, RMSSD, LF and HF indices in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTnormalized units. It was hypothesized that, due to the rhythmic and harmonic features of
the music, the parasympathetic withdrawal that was seen in the control protocol was
absent in the same subjects when they were exposed to music before the application of
the postural change test.20 Nevertheless, the present study found no significant effects of
music on the cardiac autonomic response to the mental arithmetic load test.
According to our findings, the changes in the music protocol almost reached
statistical significance, tending toward a parasympathetic reduction during the mental
arithmetic load test as compared to the period of musical auditory stimulation; this
phenomenon was not observed when the same volunteers were subjected to the control
protocol, suggesting that music may slightly intensify the cardiac autonomic responses
induced by this mental task. The effect of relaxing acoustic stimulation and relaxing
music on changes in physiological parameters induced by a laboratory test in healthy
volunteers was recently evaluated.10 The authors reported higher plasma cortisol levels
in women who were exposed to music before the mental task and lower plasma cortisol
levels in those who were exposed to the sound of rippling water. In that study,
autonomic function was analyzed through salivary alpha-amylase responses, and similar
responses were observed in both groups. In the mental task used in that study,10 the
subjects had to calculate backwards in steps of 17 from the number 2043. After each
calculation error the participants were asked to start over from 2043. Some issues
regarding that study and the present investigation are worth mentioning; for example,
that study evaluated women whereas the present study evaluated men. It is also possible
that the mental arithmetic load test used in the present study causes less intense
physiological responses.
Our findings indicate the selected baroque music (Pachelbel: Canon in D) does
not significantly influence cardiac autonomic responses to a mental task. The music

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTstyle is an important factor that influences HRV.2,3 It lacks in the literature the
physiological effects of the Canon in D music from Pachelbel. In this circumstance, this
music was chosen because our group has recently investigated the effects of this
specific stimulation on cardiac autonomic regulation.9,16,17,21 It was observed that this
music significantly influenced HRV indices in the time and frequency domain in
women,16 though it did not cause significant responses in the geometric indices of
HRV.17 The literature indicates that the inconsistency of the published results on heart
rate alterations in response to music are due to individual response specificity in the
autonomic nervous system.22,23 Another issue that may be involved in the inconsistent
data is the period of exposure to musical auditory stimulation. While in some studies
women were exposed to five minutes and it was found significant influence of music on
HRV, 16,17 other investigations reported no significant difference when women were
exposed during 10 minutes to music.8 Based on Iwanaga et al,24 the repetitive exposure
to music may have influenced cardiac autonomic responses to music.
According to this investigation, musical auditory stimulation with Pachelbel’s
Canon in D did not acutely influence cardiac autonomic responses to a mental task. The
sound intensity investigated in this study ranged from 63 to 84 dB. Auditory stimulation
at an equivalent level has elsewhere been reported to induce changes in cardiac
autonomic regulation.25 HRV was evaluated in healthy volunteers during five minutes
of binaural exposure to white noise at a low-to-moderate intensity, i.e. between 50 and
90 dB. The authors observed a significant association between the LF/HF ratio and the
equivalent sound level of the white noise. No changes in arterial blood pressure or basal
heart rate were found. Regardless, subjects who are exposed to noise intensities above
50 dB reportedly exhibit increased sympathetic regulation of the heart as shown through
frequency domain indices analysis, as the LF/HF ratio increases. However, there are
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTsome differences between white noise and musical auditory stimulation. White noise is
characterized by a small range of intensity,26 while the intensity of music fluctuates.
Musical auditory stimulation influences the cognitive system,27 but it has not yet been
established whether white noise induces a positive or negative response in the cognitive
system. In this context, it may be postulated that the effects of auditory stimulation on
the cardiac autonomic regulation depend on the type of auditory stimulation.
The intensity of musical auditory stimulation is a relevant point to be discussed.
As mentioned above, noise intensity has been indicated to influence the effect of
auditory stimulation on cardiac autonomic regulation.28 The cardiovascular responses to
auditory stimulation are conducted through several proposed mechanisms, including the
startle reflex, a response mediated by a brainstem circuit. The acoustic startle reflex is a
well-known effect of loud auditory stimulation on heart rate. This reflex is an abrupt
response of the heart rate and blood pressure to a sudden loud auditory stimulation. The
usual intensity used to elicit a startle reflex is 110 dB, and this intensity is much louder
than environmental noise. Nonetheless, subjects repeatedly exposed to 60 dB and 110
dB white-noise stimuli were seen to become habituated over time with regard to their
cardiac response.29 These heart rate and arterial blood pressure responses are regarded
as startle and defence responses in humans and a fight-or-flight response in animals.
The rise in blood pressure and heart rate in response to auditory stimulation indicates an
autonomic function responding to the acoustic stimuli.30
However, after a careful search on Medline/Pubmed database we did not find any
study that investigated the relevance of music intensity on HRV. In this circumstance,
there are some differences between white noise and musical auditory stimulation. White
noise is characterized by a small range in its intensity26 and music presents oscillation of
its intensity. Musical auditory stimulation influences the cognitive system,27 however, it

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTwas not proved yet if white noise induces positive or negative responses in the cognitive
system. It may be postulated that the effects of auditory stimulation on the cardiac
autonomic regulation depend on its style.
In this sense, one previous study has indicated a consistent trend towards
increased cardiovascular risk among individuals with a daytime noise exposure level
higher than 65 dBA.30 Another study by Lee et al,25 however, has reported that noises
equal to or greater than 50 dBA induce an immediate and intense sympathetic activation
without inducing a feeling of anxiety. Thus sound or noise stimulation may produce
significant and prompt cardiac stress responses even at relatively low levels such as 50–
60 dBA.25
Although no significant effects of music on cardiac autonomic responses during
and after a mental test were found in the present study, other studies have indicated a
relationship between music and the central nervous system based on physiological
mechanisms. Neurochemical evidence has revealed that strong emotional reactions
induced by music involve reward circuitry and function based on dopamine release in
the nucleus accubens.31 It has also been reported that musical auditory stimulation in
rats increases calcium/calmodulin-dependent dopamine synthesis in the brain, inducing
a blood pressure decrease32. Another study in rats has indicated the importance of the
hypothalamus in the physiological responses induced by music (“Träumerei” from
Kinderszenen Op.15-7).33 Even in rats under anaesthesia, musical auditory stimulation
decreases arterial blood pressure and sympathetic activity. Yet that investigation also
shows that not all music decreases blood pressure and sympathetic activity, as shown
through an analysis of renal sympathetic nerve activity, and that this mechanism is
dependent on an intact cochlea and auditory cortex and is regulated by histaminergic H3
receptors in the suprachiasmatic nucleus of the hypothalamus.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMoreover, subcortical and cortical centres have been shown to be involved in the
hormonal and cardiovascular responses to long-term stress activation induced by
environmental auditory stimulation, even at a fairly low noise intensity of 53 dB.34 The
locus coeruleus is indicated to be a central control centre for autonomic function
regulation in response to acoustic stimuli, suggesting its involvement in the acoustic
startle reflex.29
CONCLUSION
Auditory stimulation with music did not significantly influence the cardiac autonomic
responses induced by a mental task consisting of the mental arithmetic overload test in
men, as shown through analysis of the linear indices of HRV. The findings of this study
indicate that this particular choice of music accompanied with a mental task does not
affect heart rate
REFERENCES
1. Phipps MA, Carroll DL, Tsiantoulas A. Music as a therapeutic intervention on
an inpatient neuroscience unit. Complement Ther Clin Pract 2010;16:138–42.
2. Valenti VE, Guida HL, Frizzo AC, Cardoso AC, Vanderlei LC, Abreu LC.
Auditory stimulation and cardiac autonomic regulation. Clinics 2012;67:955–8.
3. Valenti VE, Guida HL, Vanderlei LCM, Roque AL, Ferreira LL, Ferreira C,
Silva TD, Manhabusque KV, Fujimori M, Abreu LC. Relationship between
cardiac autonomic regulation and auditory mechanisms: importance for growth
and development. Journal of Human Growth and Development 2013;23:94–98.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT4. Bernardi L, Porta C, Casucci G, Balsamo R, Bernardi NF, Fogari R, Sleight P.
Dynamic interactions between musical, cardiovascular, and cerebral rhythms in
humans. Circulation 2009;119:3171–80.
5. Vanderlei LC, Pastre CM, Hoshi RA, Carvalho TD, Godoy MF. Basic notions of
heart rate variability and its clinical applicability. Rev Bras Cir Cardiovasc
2009;24(2):205–17.
6. Abreu LC. Heart rate variability as a functional marker of development. Journal
of Human Growth and Development 2012;22:279–281.
7. Chuang CY, Han WR, Li PC, Song MY, Young ST. Effect of long-term music
therapy intervention on autonomic function in anthracycline-treated breast
cancer patients. Integr Cancer Ther 2011;10(4):312–6.
8. de Castro BC, Guida HL, Roque AL, de Abreu LC, Ferreira LL, Raimundo RD,
Monteiro CB, Goulart FC, Ferreira C, Marcomini RS, Ribeiro VF, Ré AH,
Vanderlei LC, Valenti VE. Previous exposure to musical auditory stimulation
immediately influences the cardiac autonomic responses to the postural change
manoeuvre in women. Int Arch Med. 2013;14;6(1):32.
9. Ziegler D. Diabetic cardiovascular autonomic neuropathy: prognosis, diagnosis
and treatment. Diabetes Metab Rev 1994;6:339–383.
10. Thoma MV, La Marca R, Brönnimann R, Finkel L, Ehlert U, Nater UM. The
effect of music on the human stress response. PLoS One 2013;5;8(8):e70156.
11. Pivatelli FC, Dos Santos MA, Fernandes GB, Gatti M, de Abreu LC, Valenti
VE, Vanderlei LC, Ferreira C, Adami F, de Carvalho TD, Monteiro CB, de
Godoy MF. Sensitivity, specificity and predictive values of linear and nonlinear
indices of heart rate variability in stable angina patients. Int Arch Med
2012;30;5(1):31.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT12. Moreno IL, Pastre CM, Ferreira C, de Abreu LC, Valenti VE, Vanderlei LC.
Effects of an isotonic beverage on autonomic regulation during and after
exercise. J Int Soc Sports Nutr 2013;4;10(1):2.
13. Carvalho TD, Pastre CM, de Godoy MF, Fereira C, Pitta FO, de Abreu LC,
Ramos EM, Valenti VE, Vanderlei LC. Fractal correlation property of heart rate
variability in chronic obstructive pulmonary disease. Int J Chron Obstruct
Pulmon Dis 2011;6;6:23–8.
14. Dias de Carvalho T, Marcelo Pastre C, Claudino Rossi R, de Abreu LC, Valenti
VE, Marques Vanderlei LC. [Geometric index of heart rate variability in chronic
obstructive pulmonary disease]. Rev Port Pneumol 2011;17(6):260–5.
15. Taelman J, Vandeput S, Gligorijević I, Spaepen A, Van Huffel S. Time-
frequency heart rate variability characteristics of young adults during physical,
mental and combined stress in laboratory environment. Conf Proc IEEE Eng
Med Biol Soc 2011;2011:1973–6.
16. Roque AL, Guida HL, Abreu LC, Vanderlei LC, Ferreira C, Valenti VE, et al.
The effects of different styles of musical auditory stimulation on cardiac
autonomic regulation in healthy women. Noise & Health 2013;15:281–287.
17. Roque AL, Guida HL, Campos MF, Ferreira LL, Knap A, Abreu LC, et al. The
effects of auditory stimulation with music on heart rate variability in healthy
women. Clinics 2013;68(7):960–7.
18. Garde AH, Laursen B, Jørgensen AH, Jensen BR. Effects of mental and physical
demands on heart rate variability during computer work. Eur J Appl Physiol
2002;87:456–461.
19. Zhong X, Hilton HJ, Gates GJ, Jelic S, Stern Y, Bartels Y et al. Increased
sympathetic and decreased parasympathetic cardiovascular modulation in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTnormal humans with acute sleep deprivation. J Appl Physiol 2005;98:2024–
2032.
20. Hatem TP, Lira PI, Mattos SS. The therapeutic effects of music in children
following cardiac surgery. J Pediatr 2006;82:86–92.
21. daSilva AG, Guida HL, Antônio AMS, Marcomini RS, Fontes AMG, de Abreu
LC, Roque AL, Silva SB, Raimundo RD, Ferreira C, Valenti VE. Acute
responses of the heart period to musical auditory stimulation in different periods.
Complement Ther Clin Pract 2013. In press.
22. Fiske DW, Rice L. Intra-individual response variability. Psychol Bull
1955;52:217–250.
23. Lacey JI, Lacey BC. Some autonomic-central nervous system interrelationships.
In: Black, P. (Ed.), Physiological Correlates of Emotion. Academic Press, New
York. 1970:205–227.
24. Iwanaga M, Kobayashi A, Kawasaki C. Heart rate variability with repetitive
exposure to music. Biol Psychol 2005;70:61-6.
25. Lee OK, Chung YF, Chan MF, Chan MW. Music and its effect on the
physiological responses and anxiety levels of patients receiving mechanical
ventilation: a pilot study. J Clin Nurs 2005;14:609–20.
26. Daee S, Wilding JM. Effects of high intensity white noise on short-term memory
for position in a list and sequence. Br J Psychol 1977;68:335–49.
27. Burns JL, Labbe E, Arke B, Capeless K, Cooksey B, Steadman A. The effects of
different types of music on perceived and physiological measures of stress. J
Music Ther 2002;39:101–116.
28. Turpin G, Siddle DA. Cardiac and forearm plethysmographic responses to high
intensity auditory stimulation. Biol Psychol 1978;6:257–81.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT29. Samuels ER, Hou RH, Langley RW, Szabadi E, Bradshaw CM. Modulation of
the acoustic startle response by the level of arousal: comparison of clonidine and
modafinil in healthy volunteers. Neuropsychopharmacol 2007;32:2405–21.
30. Spreng M. Noise induced nocturnal cortisol secretion and tolerable overhead
flights. Noise Health 2004;6:35–4.
31. Salimpoor VN, Benovoy M, Larcher K, Dagher A, Zatorre RJ. Anatomically
distinct dopamine release during anticipation and experience of peak emotion to
music. Nat Neurosci 2011;14(2):257–62.
32. Sutoo D, Akiyama K. Music improves dopaminergic neurotransmission:
demonstration based on the effect of music on blood pressure regulation. Brain
Res 2004;1016(2):255–62.
33. Nakamura T, Tanida M, Niijima A, Hibino H, Shen J, Nagai K. Auditory
stimulation affects renal sympathetic nerve activity and blood pressure in rats.
Neurosci Lett 2007;416(2):107–12.
34. Ising H, Kruppa B. Health effects caused by noise: evidence in the literature
from the past 25 years. Noise Health 2004;6:5–13.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
FIGURE LEGENDS
Figure 1.Equivalent sound level of auditory musical stimulation of classical style.dB:
Decibel; Hz: hertz. Edited by Roque et al, 2013.
Figure 2.Frequency sound level of auditory musical stimulation of classical style.dB:
Decibel. Edited by Roque et al, 2013.
Table 1. Baseline diastolic (DAP) and systolic arterial pressure (SAP), heart rate (HR), mean
RR interval, weight, height and body mass index (BMI) of the volunteers. Mean+standard
deviation. Legend: m: meters; ms: millisecond; kg: kilograms; bpm: beats per minute; mmHg:
millimeters of mercury. N=28
Variables Value
Age (years) 19.1+ 1
Height (m) 1.74+0.11
Weight (kg) 77.4+15.6
BMI (kg/m2) 25.4+ 2.8
HR (bpm) 83.3+10
Mean RR (ms) 738.7+113.3
SAP (mmHg) 115.6+11.1
DAP (mmHg) 81+9.05
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 2
Table 2. Mean and standard deviation for time-domain indices before (Rest), during the test
(Test) and after the mental arithmetic overload test (Post test) in the control protocol. SDNN -
standard deviation of normal-to-normal R-R intervals; pNN50 - the percentage of adjacent RR
intervals with a difference of duration greater than 50ms; RMSSD - root-mean square of
differences between adjacent normal RR intervals in a time interval.ms – millisecond. N=28.
Index Rest Test Post test p
SDNN 40±10 34±5 35±7 0.5
RMSSD 24± 6 25±11 24±6 0.9
pNN50 6±4 9 ± 9 5 ± 4 0.6
Table 3.Mean and standard deviation for time-domain indices before (Rest), during the test
(Test) and after the mental arithmetic overload test (Post test) in the control protocol. Legend:
LF - low frequency; HF - high frequency; LF/HF - low frequency/high frequency ration; ms -
milliseconds; nu - normalized units. N=28.
Index Rest Test Post test p
LF (ms2) 938±648 569±434 584±296 0.1
LF (nu) 69±11 59±18 60±13 0.5
HF (ms2) 596±560 385 ± 221 624 ± 513 0.4
HF (nu) 30±11 40±18 39±13 0.5
LF/HF 613±1934 240±755 291±916 0.7

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 3
Table 4.Mean and standard deviation for time-domain indices before (Rest), during the test
(Test), during musical auditory stimulation (Music) and after the mental arithmetic overload
test (Post test) in the music protocol. SDNN - standard deviation of normal-to-normal R-R
intervals; pNN50 - the percentage of adjacent RR intervals with a difference of duration
greater than 50ms; RMSSD - root-mean square of differences between adjacent normal RR
intervals in a time interval.ms – millisecond. N=28.
Index Rest Music Test Post test p
SDNN 43.2±8 46±3 31±11 36±12 0.1
RMSSD 25±7 27±5 24±14 25±10 0.9
pNN50 6.85±6.3 7.65±5.05 7 ± 13 7 ± 8 0.9

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 4
Table 5.Mean and standard deviation for time-domain indices before (Rest), during the test
(Test), during musical auditory stimulation (Music) and after the mental arithmetic overload
test (Post test) in the music protocol. Legend: LF - low frequency; HF - high frequency;
LF/HF - low frequency/high frequency ration; ms - milliseconds; nu - normalized units.
N=28.
Index Rest Music Test Post test p
LF (ms2) 1213±674 1345±964 827±751 1258±961 0.1
LF (nu) 60±21 72±5 54±18 68±7 0.3
HF (ms2) 574±383 471±317 392±286 531±382 0.6
HF (nu) 30±8 27±5 45±18 31±7 0.1
LF/HF 2±1 658±2072 110±341 2±1 0.5

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTHighlights
• Musical auditory stimulation with some styles was shown to influence cardiac
autonomic regulation.
• It is not clear in the literature whether music attenuates or intensifies cardiac
autonomic responses induced by autonomic tests.
• We reported that auditory stimulation with Pachelbel (Canon in D) music does
not influence cardiac responses elicited by a mental task.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7+5= 9+6= 14+3= 18+15=
9-7= 26-14= 35-6= 45-18=
26+12= 24+11= 54+24= 79+48=
36-16= 57-14= 72-26= 80-11=
3+7-6= 9+7-10= 25+28-18= 44+36-27=
21+14-18= 35+50-25= 46+45-60= 94+76-64=
63-17+26= 62-18+28= 78-32+64= 96-36+80=
7-11+5= 18-20+24= 39-55+40= 41-54+63=
Teste Matemático
Related Documents











