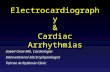
Cardiac Arrhythmias Atria Contract P P P Q P Q R P wave PQ Segment Q wave R wave P Q R S T P Q R S P Q R S P Q R S T Ventricles Contract S wave ST Segment T wave The end Arrhythmia Substrate Normal Reentry Stimulus + = Unidirectional conduction Stimulus point Dividing impulses Blocked impulse A Diseased tissue Ventricular Arrhythmias Life Saving Devices Deadly Arrhythmias Leads Right Atrium Right Ventricle Pacemaker Pacemaker Treatment for Ventricular Tachycardia VF Defibrillation pulse Normal rhythm Implantable Cardioveter Defibrillator (ICD) Automatic External Defibrillator (ICD) Treatment for Ventricular Fibrillation Atrial Arrhythmias Increasing Prevalence Greater Risk with Age Cause 20% of All Strokes Triggering Foci Atrial Septum Superior Vena Cava Inferior Vena Cava Left Atrium Pulmonary Veins Right Ventricle Left Ventricle Right Atrium Mapping Catheter Ablation Catheter RF Ablation of AF Termination of AF - Atrial Dilation - Fibrosis Triggers AF Begets AF Structural Remodeling Electrical Remodeling - Ectopic Foci - Hypertension - Aging - Heart Valve Disease - Heart Failure - Slowed Conduction - Increased Excitability ECG ECG Atrial EGM Atrial EGM Atrial Fibrillation Sinus Rhythm www.sci.utah.edu S C I I N S T I T U T E ● E X H I B I T ● EX P L O R E ● E X C I T E EX P E R I E N C E ● EX C H A N G E ● SCI Ventricular Fibrillation (VF) Ventricular Tachycardia (VT) VT Anti-tachycardia pacing Normal rhythm Normal Conduction

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cardiac Arrhythmias
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence and ECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
Oriented from active to inactive tissueChanges location and magnitudeGross simplification
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence and ECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
• Oriented from active to inactive tissue
• Changes location and magnitude
• Gross simplification
Bioengineering 6000 CV PhysiologyECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
• Oriented from active to inactive tissue
• Changes location and magnitude
• Gross simplification
Bioengineering 6000 CV PhysiologyECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
• Oriented from active to inactive tissue
• Changes location and magnitude
• Gross simplification
P wave
Atria Contract
P P PQ
PQ
RP wave PQ Segment Q wave R wave
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence and ECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
• Oriented from active to inactive tissue
• Changes location and magnitude
• Gross simplification
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence and ECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
• Oriented from active to inactive tissue
• Changes location and magnitude
• Gross simplification
Bioengineering 6000 CV PhysiologyECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
• Oriented from active to inactive tissue
• Changes location and magnitude
• Gross simplification
Bioengineering 6000 CV PhysiologyECG
Bioengineering 6000 CV PhysiologyECG
Cardiac Activation Sequence: Moving Dipole
• Oriented from active to inactive tissue
• Changes location and magnitude
• Gross simplification
PQ
R
STP
Q
R
SP
Q
R
SP
Q
R
ST
Ventricles Contract
S wave ST Segment T wave The end
Arrhythmia Substrate
Normal Reentry
Stimulus
+=
Unidirectional conduction
Chapter 13 Cardiac Arrhythmias and Their Electrocardiographic Interpretation 153
Phenomenon of Re-entry—“CircusMovements” as the Basis forVentricular Fibrillation
When the normal cardiac impulse in the normal hearthas traveled through the extent of the ventricles, it hasno place to go because all the ventricular muscle isrefractory and cannot conduct the impulse farther.Therefore, that impulse dies, and the heart awaits a newaction potential to begin in the atrial sinus node.
Under some circumstances, however, this normalsequence of events does not occur. Therefore, let usexplain more fully the background conditions that caninitiate re-entry and lead to “circus movements,” whichin turn cause ventricular �brillation.
Figure 13–14 shows several small cardiac musclestrips cut in the form of circles. If such a strip is stimu-lated at the 12 o’clock position so that the impulse travelsin only one direction, the impulse spreads progressivelyaround the circle until it returns to the 12 o’clock posi-tion. If the originally stimulated muscle �bers are still ina refractory state, the impulse then dies out becauserefractory muscle cannot transmit a second impulse. Butthere are three di�erent conditions that can cause thisimpulse to continue to travel around the circle, that is,to cause “re-entry” of the impulse into muscle that has already been excited. This is called a “circus movement.”
First, if the pathway around the circle is too long, bythe time the impulse returns to the 12 o’clock position,the originally stimulated muscle will no longer berefractory and the impulse will continue around thecircle again and again.
Second, if the length of the pathway remains constantbut the velocity of conduction becomes decreasedenough, an increased interval of time will elapse beforethe impulse returns to the 12 o’clock position. By thistime, the originally stimulated muscle might be out of
the refractory state, and the impulse can continuearound the circle again and again.
Third, the refractory period of the muscle mightbecome greatly shortened. In this case, the impulse couldalso continue around and around the circle.
All these conditions occur in di�erent pathologicalstates of the human heart, as follows: (1) A long pathwaytypically occurs in dilated hearts. (2) Decreased rate ofconduction frequently results from (a) blockage of thePurkinje system, (b) ischemia of the muscle, (c) highblood potassium levels, or (d) many other factors. (3) A shortened refractory period commonly occurs inresponse to various drugs, such as epinephrine, or afterrepetitive electrical stimulation. Thus, in many cardiacdisturbances, re-entry can cause abnormal patterns ofcardiac contraction or abnormal cardiac rhythms thatignore the pace-setting e�ects of the sinus node.
Chain Reaction Mechanism of Fibrillation
In ventricular �brillation, one sees many separate andsmall contractile waves spreading at the same time indi�erent directions over the cardiac muscle. The re-entrant impulses in �brillation are not simply a singleimpulse moving in a circle, as shown in Figure 13–14.Instead, they have degenerated into a series of multiplewave fronts that have the appearance of a “chain reac-tion.” One of the best ways to explain this process in �brillation is to describe the initiation of �brillation byelectric shock caused by 60-cycle alternating electriccurrent.
Fibrillation Caused by 60-Cycle Alternating Current. At acentral point in the ventricles of heart A in Figure 13–15,a 60-cycle electrical stimulus is applied through a stimulating electrode. The �rst cycle of the electricalstimulus causes a depolarization wave to spread in alldirections, leaving all the muscle beneath the electrodein a refractory state.After about 0.25 second, part of thismuscle begins to come out of the refractory state. Someportions come out of refractoriness before other
Absolutelyrefractory
Absolutelyrefractory
Relativelyrefractory
LONG PATHWAY
NORMAL PATHWAY
Figure 13–14
Circus movement, showing annihilation of the impulse in the shortpathway and continued propagation of the impulse in the longpathway.
Stimuluspoint Dividing
impulses
Blockedimpulse
BA
Figure 13–15
A, Initiation of �brillation in a heart when patches of refractory mus-culature are present. B, Continued propagation of �brillatoryimpulses in the �brillating ventricle.
Diseasedtissue
Ventricular Arrhythmias
Life Saving Devices
Deadly Arrhythmias
Leads
Right Atrium
Right Ventricle
Pacemaker
Pacemaker
Treatment for Ventricular Tachycardia
VF Defibrillation pulse Normal rhythm
Implantable Cardioveter Defibrillator (ICD)
Automatic External Defibrillator (ICD)
Treatment for Ventricular Fibrillation
Atrial Arrhythmias
Increasing PrevalenceGreater Risk with Age
Cause 20% of All Strokes
TriggeringFoci
Atrial Septum
SuperiorVena Cava
InferiorVena Cava
LeftAtrium
PulmonaryVeins
RightVentricle
LeftVentricle
RightAtrium
MappingCatheter
AblationCatheter
RF Ablation of AF Termination of AF
- Atrial Dilation- Fibrosis
Triggers
AF Begets AF
StructuralRemodeling
ElectricalRemodeling
- Ectopic Foci- Hypertension- Aging- Heart Valve Disease- Heart Failure
- Slowed Conduction- Increased Excitability
ECG
ECG
Atr
ial E
GM
Atr
ial E
GM
Atrial Fibrillation
Sinus Rhythm
www.sci.utah.edu
SCI
INSTITUTE ● EXHIBIT ● EXPLO
RE ● EXCITE EXPERIENCE ● E
XCHAN
GE ●
SCI
Ventricular Fibrillation (VF)Ventricular Tachycardia (VT)
VT Anti-tachycardia pacing Normal rhythm
Normal Conduction
Related Documents