Cardiac Cardiac tachyarrhythmias tachyarrhythmias Dr Majid Shojaee Dr Majid Shojaee Assistant professor of Emergency Assistant professor of Emergency Medicine Medicine SBMU SBMU 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cardiac Cardiac tachyarrhythmiastachyarrhythmias
Dr Majid ShojaeeDr Majid ShojaeeAssistant professor of Emergency MedicineAssistant professor of Emergency Medicine
SBMUSBMU
11

22

Case 1Case 1 A 30-year-old woman suddenly has rapid A 30-year-old woman suddenly has rapid
palpitations accompanied by chest palpitations accompanied by chest tightness and dizziness.tightness and dizziness.
Previous similar episodes over last 12 Previous similar episodes over last 12 months –usually 20 -30 minmonths –usually 20 -30 min
PR=190/min ,BP=85/55 mm Hg. PR=190/min ,BP=85/55 mm Hg. Otherwise normalOtherwise normal
cardiovascularcardiovascular examinationexamination
33

Evaluation and managementEvaluation and management
44

Evaluation and managementEvaluation and management signs of increased work of breathing and oxyhemoglobin saturation signs of increased work of breathing and oxyhemoglobin saturation
as determined by pulse oximetryas determined by pulse oximetry.. (O2) (O2) Attach a monitor to the patient, Attach a monitor to the patient, Evaluate blood pressure,Evaluate blood pressure, Establish IV access.Establish IV access. If available, obtain a 12-lead ECG If available, obtain a 12-lead ECG
This(ECG) should This(ECG) should not delay not delay immediate cardioversion if the patient immediate cardioversion if the patient is unstable. While initiating treatment, evaluate the patient’s clinical is unstable. While initiating treatment, evaluate the patient’s clinical status and identify status and identify potential reversible causes potential reversible causes of the tachycardiaof the tachycardia
55

What is the differential diagnosis ?What is the differential diagnosis ?
66

Supraventricular tachycardiaSupraventricular tachycardia Sinus tachycardiaSinus tachycardia PSVTPSVT Atrial tachycardia (multifocal)Atrial tachycardia (multifocal) Atrial fibrillation / flutterAtrial fibrillation / flutter Junctional tachycardiaJunctional tachycardia Ventricular tachycardiaVentricular tachycardia
77

88

First stepFirst step
STABLE or UNSTABLE?STABLE or UNSTABLE?
99

Acute altered mental status, Acute altered mental status, Ischemic chest discomfort, Ischemic chest discomfort, Acute heart failure,Acute heart failure, Hypotension, or Hypotension, or Other signs of shock suspected to be due Other signs of shock suspected to be due
to a tachyarrhythmiato a tachyarrhythmia
1010

Unstability is Primary or secondary?Unstability is Primary or secondary?
With ventricular rates <150/minute in the With ventricular rates <150/minute in the absence of ventricular dysfunction, it is more absence of ventricular dysfunction, it is more likely that the tachycardia is likely that the tachycardia is secondary to the secondary to the underlying condition underlying condition rather than the cause of the rather than the cause of the instabilityinstability
Rate> 220-ageRate> 220-age Acute onset or gradualAcute onset or gradual JVDJVD Fever, hemorrhage, dehydration…Fever, hemorrhage, dehydration…
1111

UANSTABLEUANSTABLE
due to a tachyarrhythmia, proceed to immediate due to a tachyarrhythmia, proceed to immediate synchronized cardioversionsynchronized cardioversion
If possible, If possible,
-establish IV access -establish IV access before cardioversionbefore cardioversion
-administer -administer sedationsedation if the patient is conscious. if the patient is conscious.
Do not delay cardioversion if the patient is Do not delay cardioversion if the patient is extremely unstableextremely unstable
1212

1313

Cardioversion Cardioversion
Synchronized Synchronized
This synchronization avoids shock delivery This synchronization avoids shock delivery during the during the relative refractory period relative refractory period of the of the cardiac cycle when a shock could produce cardiac cycle when a shock could produce VFVF
1414

Synchronized cardioversion is Synchronized cardioversion is recommended to treatrecommended to treat
(1) (1) unstable unstable SVTSVT, , (2) unstable (2) unstable atrial fibrillationatrial fibrillation, , (3) unstable (3) unstable atrial flutteratrial flutter, , (4) unstable monomorphic (regular) (4) unstable monomorphic (regular) VTVT..
1515

Rhythm Biphasic (J) Monophasic (J)
AF 120-200 200
A flutter / SVT 50-100 200
Monomorphic VT 100 100
1616

If a patient has If a patient has polymorphic VTpolymorphic VT, treat the rhythm as VF , treat the rhythm as VF and deliver high-energy and deliver high-energy unsynchronized shocks (ie, unsynchronized shocks (ie, defibrillationdefibrillation doses). doses).
If there is any If there is any doubtdoubt whether monomorphic or whether monomorphic or polymorphic VT is present in the polymorphic VT is present in the unstable patientunstable patient, do not , do not delay shock delivery to perform detailed rhythm analysis: delay shock delivery to perform detailed rhythm analysis: provide provide high-energy unsynchronized high-energy unsynchronized shocks (ie, shocks (ie, defibrillation doses).defibrillation doses).
1717

STABLE STABLE
1818

Narrow OR Wide Complex?Narrow OR Wide Complex?> or < 120 msec.> or < 120 msec.
2020

Regular Narrow QRS Tachycardias therapy
2121

2222

2323

2424

PR=190PR=190BP=85/55BP=85/55
Her ECG Her ECG
2525

Vagotonic ManeuversVagotonic Maneuvers
Valsalva maneuver Valsalva maneuver Facial ice pack (“diving reflex” for kids)Facial ice pack (“diving reflex” for kids) Carotid sinus massageCarotid sinus massage
2626

Valsalva maneuver Valsalva maneuver
The Valsalva maneuver performed in the The Valsalva maneuver performed in the supine position appears to be the most supine position appears to be the most effective vagal maneuver for the effective vagal maneuver for the conversion of reentrant SVT.conversion of reentrant SVT.
For maximal effectiveness the strain For maximal effectiveness the strain phase must be adequate (usually at least phase must be adequate (usually at least l0 seconds), with slowing or conversion l0 seconds), with slowing or conversion seen during the release phaseseen during the release phase
2727

Facial ice pack (“diving reflex”)Facial ice pack (“diving reflex”)
Placing an ice pack on the face or facial Placing an ice pack on the face or facial immersion in cold water is usually immersion in cold water is usually reserved for infants and is done for 6 to 7 reserved for infants and is done for 6 to 7 seconds with the nostrils held closed seconds with the nostrils held closed (diving reflex)(diving reflex)
2828

Carotid Sinus MassageCarotid Sinus Massage
Pressure on the carotid sinus and Pressure on the carotid sinus and Baroreceptors. Carotid massage should be Baroreceptors. Carotid massage should be done for 10 seconds at a time,done for 10 seconds at a time,
first on the side of the nondominant cerebral first on the side of the nondominant cerebral hemisphere, hemisphere,
and never simultaneously on both sides.and never simultaneously on both sides.
2929

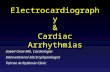
Carotid Sinus Massage
Stimulation of carotid sinus triggers baroreceptorreflex and increased vagaltone, affectingSA and AV nodes
3030

3131

AdenosineAdenosine
6 mg of IV adenosine as a rapid IV push 6 mg of IV adenosine as a rapid IV push through a large (eg, antecubital) vein through a large (eg, antecubital) vein followed by a 20 mL saline flush.followed by a 20 mL saline flush.
If the rhythm does not convert within 1 to 2 If the rhythm does not convert within 1 to 2 minutes, give a 12 mg rapid IV push using minutes, give a 12 mg rapid IV push using the method above.the method above.
3232

As with vagal maneuvers, the effect of As with vagal maneuvers, the effect of adenosine on other SVTs (such as atrial adenosine on other SVTs (such as atrial fibrillation or flutter) is fibrillation or flutter) is to transiently slow to transiently slow ventricular rateventricular rate (which may be useful (which may be useful diagnostically) but not afford their diagnostically) but not afford their termination or meaningful lasting rate termination or meaningful lasting rate control.control.
3333

Termination of SVT
3434

Pregnancy? Pregnancy? Drug history?Drug history? Larger doses may be required for patients with Larger doses may be required for patients with
a significant blood level of theophylline, caffeine, or a significant blood level of theophylline, caffeine, or theobromine.theobromine.
The initial dose should be reduced to 3 mg in patients takingThe initial dose should be reduced to 3 mg in patients taking dipyridamole or carbamazepine, those with transplanted dipyridamole or carbamazepine, those with transplanted
hearts, or if given by central venous access.hearts, or if given by central venous access. Childs:Childs: 0.1 mg/kg0.1 mg/kg
3535

Side effects with adenosine are common Side effects with adenosine are common but transient; flushing, dyspnea, and chest but transient; flushing, dyspnea, and chest discomfort are the most frequently discomfort are the most frequently observed.observed.
Adenosine should not be given to patients Adenosine should not be given to patients with asthmawith asthma
3636

Because of the possibility of initiating Because of the possibility of initiating atrial atrial fibrillation fibrillation with rapid ventricular rates in a with rapid ventricular rates in a patient with WPW, patient with WPW, a defibrillatora defibrillator should be should be available when adenosine is administered to any available when adenosine is administered to any patient in whom WPW is a consideration.patient in whom WPW is a consideration.
3737

If adenosine or vagal maneuvers disclose If adenosine or vagal maneuvers disclose another form of SVT (such as atrial another form of SVT (such as atrial fibrillation or flutter), treatment with a fibrillation or flutter), treatment with a longer-acting AV nodal blocking agent longer-acting AV nodal blocking agent should be consideredshould be considered
3838

Calcium Channel Blockers and -Calcium Channel Blockers and -BlockersBlockers
If adenosine and If adenosine and vagal maneuvers fail to vagal maneuvers fail to convert PSVTconvert PSVT
3939

VerapamilVerapamil
2.5 mg to 5 mg2.5 mg to 5 mg IV bolus over 2 minutes IV bolus over 2 minutes (over 3 minutes in older patients). (over 3 minutes in older patients).
If there is no therapeutic response and no If there is no therapeutic response and no drug-induced adverse eventdrug-induced adverse event, repeated , repeated doses of doses of 5 mg to 10 mg5 mg to 10 mg every 15 to 30 min. every 15 to 30 min.
total dose 20 mgtotal dose 20 mg
4040

Verapamil Verapamil should not should not be given to patients be given to patients with:with:
wide-complex tachycardiaswide-complex tachycardias impaired ventricular function impaired ventricular function heart failureheart failure
4141

Diltiazem Diltiazem
give a dose of give a dose of 15 mg to 20 15 mg to 20 mg (0.25 mg (0.25 mg/kg) IV mg/kg) IV over 2 minutesover 2 minutes
if needed, in 15 minutes if needed, in 15 minutes give an additional IV dose of 20 mg to 25 give an additional IV dose of 20 mg to 25
mg (0.35 mg/kg). mg (0.35 mg/kg). The maintenance infusion dose is 5 The maintenance infusion dose is 5
mg/hour to 15 mg/hour, titrated to heart mg/hour to 15 mg/hour, titrated to heart rate.rate.
4242

Beta-blockersBeta-blockers
These agents exert their effect byThese agents exert their effect by
antagonizing sympathetic tone in nodal tissueantagonizing sympathetic tone in nodal tissue,, Side effects Side effects of Beta-blockers can include of Beta-blockers can include
bradycardias, AV conduction delays, and bradycardias, AV conduction delays, and hypotension. hypotension.
beta-blockers should be used with beta-blockers should be used with cautioncaution in in patients with patients with COPDCOPD or or CHFCHF
Esmolol: 500mic/kg stat & 50mic/kg/min infusion..Esmolol: 500mic/kg stat & 50mic/kg/min infusion..
4343

antiarrhythmic medications (eg, antiarrhythmic medications (eg, amiodarone, procainamide, amiodarone, procainamide, or sotalol) can or sotalol) can also be used to treat SVTs,also be used to treat SVTs,
4444

4545

Narrow Narrow Supraventricular tachycardiaSupraventricular tachycardia Sinus tachycardiaSinus tachycardia ReentryReentry: -Atrial: AT, AF, Af: -Atrial: AT, AF, Af
-AV node: AVNRT, AVRT(PSVT)-AV node: AVNRT, AVRT(PSVT)
Automatic tachycardiaAutomatic tachycardia::
-Junctional tachycardia-Junctional tachycardia
-MAT-MAT
-PAC-PAC
4646

4747

AV Nodal Reentrant Tachycardia Circuit
F = fast AV nodal pathway
S = slow AV nodal pathway
(His Bundle)
During sinus rhythm, impulses conduct preferentiallyvia the fast pathway
5151

Initiation of AV Nodal Reentrant Tachycardia
PAC = premature atrial complex (beat)
PAC
PAC
5252

Sustainment of AV Nodal Reentrant Tachycardia
Rate 150-250beats per min
P waves generatedretrogradely(AV node atria) andfall within orat tail of QRS
5353

P P P P
Sustained AV Nodal Reentrant Tachycardia
Note fixed, short RP interval mimicking r’ deflection of QRS
V1
5454

“pseudo-R’”

Orthodromic AV Reentrant Tachycardia
AP
Anterogadeconduction via normal pathwayRetrograde
conductionvia accessorypathway (AP)
5656

Initiation of Orthodromic AV Reentrant Tachycardia
AVN
Ventricles
Atria
AP
PAC = premature atrial complex (beat)
PAC
5757

Sustainment of Orthodromic AV Reciprocating Tachycardia
Atria
AP
AVN
Ventricles
Retrograde P’s fall in the ST segmentwith fixed, short RP
Rate 150-250beats per min
5858

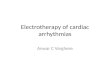
Accessory Pathway with Ventricular Preexcitation(Wolff-Parkinson-White Syndrome)
Fusion activation of the ventricles
“Delta” Wave
APPR < .12 s
QRS .12 s
Sinusbeat
Hybrid QRS shape
5959

Varying Degrees of Ventricular Preexcitation
6060

Orthodromic AV Reentrant Tachycardia
NSR with V Preex
SVT:V Preex gone
Note retrograde P wavesin the ST segment
6161


6363

Type A WPWType A WPW
6464

Type B WPWType B WPW
6565

6666

AF + WPWAF + WPW
6767

Pre-excitation syndromePre-excitation syndrome(W-P-W syndrome)(W-P-W syndrome)
There are several type of accessory There are several type of accessory pathwaypathway
1.1. KentKent: adjacent atrial and ventricular : adjacent atrial and ventricular
2.2. JamesJames: adjacent atrial and his : adjacent atrial and his bundlebundle
3.3. MahaimMahaim: adjacent lower part of the : adjacent lower part of the AVN and ventricularAVN and ventricular
Usually no structure heart disease, Usually no structure heart disease, occur in any age individualoccur in any age individual

6969

7070

7171

7272

A 45 y/o male with chest painA 45 y/o male with chest painRate: 200 Rhythm: non-sinus Axis: normal Rate: 200 Rhythm: non-sinus Axis: normal Dx: PSVT-AVNRT & rate relared ischemia, Dx: PSVT-AVNRT & rate relared ischemia, Management: Adenosin or cardioversion Management: Adenosin or cardioversion
7373

WPW WPW
7474

LGL Lone-Ganong-LevinLGL Lone-Ganong-Levin
7575

WPWWPW
7676

LGL + PVC + RBBBLGL + PVC + RBBB
7777

Sinus TachycardiaSinus Tachycardia
7878

Sinus Tachycardia (100 to 180+ beats/min)
• P waves oriented normally• PR usually shorter than at rest
7979

Causes of Sinus TachycardiaCauses of Sinus Tachycardia
Hypovolemia ( blood loss, dehydration)Hypovolemia ( blood loss, dehydration) FeverFever Respiratory distressRespiratory distress Heart failureHeart failure HyperthyroidismHyperthyroidism Certain drugs (e.g., bronchodilators)Certain drugs (e.g., bronchodilators) Physiologic states (exercise, excitement, Physiologic states (exercise, excitement,
etc)etc)
8080

Atrial Tachyarrhythmias
8181

V5
P P P P’ P
Timing of Expected P
Premature Atrial Complex (PAC)
Non-Compensatory Pause
8282

• RP intervals can be variable • RP often > PR• (Example slower than more common rate 150-250 beats per min)
Multifocal Atrial Tachycardia (MAT)
V1
Differs fromAV nodal or AV reentrantSVT
8383

Atrial Flutter (“Typical,” Counterclockwise)
Reentrant mechanism
8585

II
V1
Atrial Flutter
4:1 2:1
Classicinverted “sawtooth”flutter wavesat 300/min (best seen inII, III and AVF)
Note variableventricularresponse
8686

Atrial Flutter
2:1Conduction(common)
2:1 & 3:2Conduction
1:1Conduction(rare but dangerous)
V. rate 140-160beats/min
8787

Atrial FibrillationAtrial Fibrillation
8888

Atrial Fibrillation
Focal firingormultiplewavelets
Chaotic, rapidatrial rate at400-600beats per min
8989

V5
Atrial Fibrillation
• Rapid, undulating baseline (best seen in V1)• Most impulses block in AV node Erratic conduction
V1
9090

Atrial Fibrillation: Characteristic “Irregularly Irregular” Ventricular Response
II
9191

PR=190PR=190BP=85/55BP=85/55
Her ECG Her ECG
9292

Typical AVNRTTypical AVNRT
9393

After 6 mg AdenosineAfter 6 mg Adenosine
9494

Responses of narrow complex Responses of narrow complex tachycardias to adenosinetachycardias to adenosine
9595

Next Next
9696

Case 2Case 2
33 year old female presents with intense 33 year old female presents with intense palpitations and chest tightnesspalpitations and chest tightness
Similar episodes several times a year for Similar episodes several times a year for the last 5 yearsthe last 5 years
Episode of syncope 3 months agoEpisode of syncope 3 months ago She is confuse, BP=85/55 PR=190,She is confuse, BP=85/55 PR=190, Has cold sweeting,Has cold sweeting,
9797

9898

Dx ?Dx ? PSVT (AVRT)PSVT (AVRT)
Therapy?Therapy?
50J synch. shock50J synch. shock
9999

Next Next
100100

Case 3Case 3
72 year old presents with pneumonia72 year old presents with pneumonia Long history of smoking / COPDLong history of smoking / COPD
101101

102102

What would you do next ?What would you do next ?
103103

104104

Next Next
105105

Atrial FibrillationAtrial Fibrillation
106106

Atrial Fibrillation
The most common sustained arrhythmia in clinical practice
5% of people over age 70 years of age and 15% of those over age 80 years 107107

Atrial Fibrillation: Triggers
• Initiation of atrial fibrillation with a single PAC• Most of these triggers originate in the PVs
108108

Atrial fibrillation –Atrial fibrillation –initial assessmentinitial assessment
Onset (paroxysmal vs persistent/chronic) Onset (paroxysmal vs persistent/chronic)
SymptomsSymptoms
Haemodynamic stabilityHaemodynamic stability
Co-existing conditions ( AS ,HOCM ,CAD , CHF)Co-existing conditions ( AS ,HOCM ,CAD , CHF)
TriggersTriggers
109109

AF Management?AF Management?
110110

111111

Rhythm controlRhythm control Synchronised DC cardioversionSynchronised DC cardioversion
Chemical cardioversionChemical cardioversion Amiodarone ( iv / po )Amiodarone ( iv / po )
112112

Atrial Fibrillation with Rapid Conduction Via Accessory Pathway
113113

Next Next
114114

Premature Ventricular Complex Premature Ventricular Complex (PVC):(PVC):
Alternative Terminology Alternative Terminology
Premature ventricular Premature ventricular contractioncontraction
Ventricular Ventricular extrasystoleextrasystole
Ventricular Ventricular premature beatpremature beat
Ventricular Ventricular ectopic beatectopic beat
Ventricular Ventricular premature depolarizationpremature depolarization
115115

Premature Ventricular Complex (PVC)
Compensatory Pause
116116

PVCs: Bigeminal Pattern
“Regularly Irregular” Rhythm
117117

118118

119119

Next Next
120120

Case 4Case 4
70 year-old-man presents to the ER with a 70 year-old-man presents to the ER with a 3 hour history of palpitations that started 3 hour history of palpitations that started suddenly while gardeningsuddenly while gardening
Similar shorter episodes for last 3 yearsSimilar shorter episodes for last 3 years 2-3 episodes /month , usually 1-2 hours2-3 episodes /month , usually 1-2 hours Associated SOB and fatigueAssociated SOB and fatigue
121121

What else do you want to know from the What else do you want to know from the history?history?
Differential diagnosis ?Differential diagnosis ?
122122

Wide-Complex TachycardiaWide-Complex Tachycardia
The first step :The first step :
stable or unstable?stable or unstable? An An unstableunstable patient with a wide-complex patient with a wide-complex
tachycardia should be presumed to have tachycardia should be presumed to have VT and VT and immediate cardioversion immediate cardioversion should be should be performedperformed
123123

Precordial thump Precordial thump may be considered for may be considered for patients with patients with witnessedwitnessed, monitored, , monitored, unstableunstable ventricular tachycardia if a ventricular tachycardia if a defibrillator is defibrillator is not immediately not immediately ready for ready for useuse
124124

If stable If stable
the second step:the second step: obtain a 12-lead ECGobtain a 12-lead ECG
125125

DDxDDx
● ● VT or VFVT or VF
● ● SVT with aberrancySVT with aberrancy
● ● Pre-excited tachycardias (associated with Pre-excited tachycardias (associated with or mediated by an accessory pathway)or mediated by an accessory pathway)
● ● Ventricular paced rhythmsVentricular paced rhythms
126126

The The third step:third step: regular or irregularregular or irregular
127127

Ladder Diagram of AV Dissociation During Ventricular Tachycardia
Slower atrial rate
Faster ventricular rate
Impulses invade the AV node retrogradely and anterogradely,creating physiologic “interference” and block. Under the right conditions, some anterograde impulses may slip through.
This phenomenon is not equivalent to third degree AV block
128128

129129

Monomorphic VT
130130

V1
Polymorphic VT
131131

“Torsade de Pointes”(Polymorphic VT Associated with Prolonged Repolarization)
132132

Regular Wide QRS Tachycardia: VT or SVT with Aberrant Conduction?
V1
133133

Clinical Clues to Basis Clinical Clues to Basis for Regular Wide QRS Tachycardiafor Regular Wide QRS Tachycardia
REMEMBER: VT does REMEMBER: VT does notnot invariably cause invariably cause hemodynamic collapse; patients may be hemodynamic collapse; patients may be conscious and stableconscious and stable
History of heart disease, History of heart disease, especially priorespecially prior myocardial infarctionmyocardial infarction, suggests VT, suggests VT
Occurrence in a young patient with no Occurrence in a young patient with no known heart disease suggests SVTknown heart disease suggests SVT
12-lead EKG (if patient stable) should be 12-lead EKG (if patient stable) should be obtainedobtained
135135

136136

Regular Wide QRS Tachycardia: VT or SVT with Aberrant Conduction?
137137

138138

139139

Artifact Mimicking “VT”
Artifact precedes“VT”
QRS complexes “march through”the pseudo-tachyarrhythmia
140140

141141

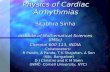
Ectopic ventricular activation
Normal ventricular activation
Fusionbeat
Accelerated Idioventricular Rhythm ( Ventricular Escape Rate, but 100 bpm)
Sinus acceleration
142142

Case 5Case 5
68-year-old man presents with an 8-hour 68-year-old man presents with an 8-hour history of palpitations and chest tightness- history of palpitations and chest tightness- no lightheadednessno lightheadedness
Previous history of myocardial infarction 5 Previous history of myocardial infarction 5 years ago treated with angioplasty and years ago treated with angioplasty and stent – no recurrent angina sincestent – no recurrent angina since
What is the differential diagnosis?What is the differential diagnosis?
143143

144144

VA dissociation on ECGVA dissociation on ECG proves VT but proves VT but is clearly discernible in only 30% - is clearly discernible in only 30% - evidence of VA dissociation on physical evidence of VA dissociation on physical examination may be usefulexamination may be useful Irregular cannon A waves in the JVPIrregular cannon A waves in the JVP Variability in loudness of S1Variability in loudness of S1
Fusion complexes / capture beatsFusion complexes / capture beats
145145

146146

Differential diagnosis of wide Differential diagnosis of wide complex tachycardiacomplex tachycardia
RegularRegular SVT with bundle branch block aberrancySVT with bundle branch block aberrancy
• Pre-existingPre-existing• Rate-relatedRate-related
Antidromic AVRTAntidromic AVRT Atrial flutter / tachycardia with aberrancy or conduction over Atrial flutter / tachycardia with aberrancy or conduction over
acc.pathway (bystander)acc.pathway (bystander) VTVT
IrregularIrregular AFAF Atrial flutter / atrial tachycardia with variable conduction andAtrial flutter / atrial tachycardia with variable conduction and
• Bundle branch blockBundle branch block• Antegrade conduction via accessory pathwayAntegrade conduction via accessory pathway
147147

Wide complex tachycardiaWide complex tachycardia
Stable vital signs during WCT are not Stable vital signs during WCT are not useful for distinguishing SVT from VTuseful for distinguishing SVT from VT
In the event of previous MI or LV In the event of previous MI or LV dysfunction VT is dysfunction VT is by farby far more likely more likely
If in doubt , avoid iv verapamil / If in doubt , avoid iv verapamil / diltiazem - can be catastrophic in VTdiltiazem - can be catastrophic in VT
Response to adenosine is not proof Response to adenosine is not proof that the WCT was SVTthat the WCT was SVT
148148

CautionCaution
DO NOT use verapamil , digoxin or DO NOT use verapamil , digoxin or
b-blockers in patients with WPWb-blockers in patients with WPW
may lead to rapid ventricular response and may lead to rapid ventricular response and cause VF in case of AFcause VF in case of AF
149149

Irregular wide QRS tachycardia-Irregular wide QRS tachycardia-preexcited AFpreexcited AF
Approximately 30% of patients with WPW Approximately 30% of patients with WPW also have AFalso have AF
DCCV is preferredDCCV is preferred
DO NOT use AV node blocking drugsDO NOT use AV node blocking drugs
150150

Management of wide QRS complex Management of wide QRS complex tachycardiatachycardia
Haemodynamically unstableHaemodynamically unstable DC cardioversionDC cardioversion
Haemodynamically stableHaemodynamically stable IV amiodaroneIV amiodarone
152152

Case 6ECG faxed – 70-year admitted with pre-syncope
153153

ECG artifact mimicking VTECG artifact mimicking VT
154154

Artifact or VT ?Artifact or VT ?
Absence of symptoms or haemodynamic Absence of symptoms or haemodynamic deterioration during the event deterioration during the event (but can not rely on this criterion)(but can not rely on this criterion)
Normal QRS complexes within the artifactNormal QRS complexes within the artifact Unstable baseline before, after the event Unstable baseline before, after the event
or bothor both Association with body movement or Association with body movement or
intermittent skin-electrode contactintermittent skin-electrode contact
155155

What is the rhythm ?What is the rhythm ?
156156

What is the rhythm?What is the rhythm?
157157

Pacemaker mediated tachycardiaPacemaker mediated tachycardia
Abnormal consequence of normal pacemaker Abnormal consequence of normal pacemaker functionfunction
Retrograde conduction ->sensed and trackedRetrograde conduction ->sensed and tracked Can only happen in dual chamber devicesCan only happen in dual chamber devices
WHAT TO DO :WHAT TO DO : Application of magnetApplication of magnet to inhibit atrial sensing, to inhibit atrial sensing,
thereby breaking tachycardia loopthereby breaking tachycardia loop
158158

80 year old woman with recurrent 80 year old woman with recurrent syncope and pre-syncopesyncope and pre-syncope
159159
Related Documents