Dr. A López-Beltrán Córdoba ¿CUÁNDO NUNCA HARÉ EL DIAGNÓSTICO DE...? CARCINOMA UROTELIAL DE VÍAS URINARIAS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dr. A López-Beltrán
Córdoba
¿CUÁNDO NUNCA HARÉ EL DIAGNÓSTICO DE...?
CARCINOMA UROTELIAL DE VÍAS URINARIAS
Tumor-like Lesions of the Urinary
Bladder
A Lopez-Beltran
Cordoba
Tumor-like Lesions of the Urinary Bladder
• Malakoplakia• Polyps• - Fibroepithelial– - Other
• Amyloidosis• Endometriosis• Endocervicosis• Mullerianosis• Postoperative spindle cell nodule
• Inflammatory pseudotumor• Paraganglionic tissue
• Epithelial abnormalities:
• - Von Brunn’s nests
• - Cystitis glandularis
• - Cystitis cystica
• - Squamous metaplasia
• - Nephrogenic adenoma
• - Papillary hyperplasia
• Non-specific cystitis:
• - Papillary-polypoid cystitis
• Specific cystitis:
• - Radiation cystitis
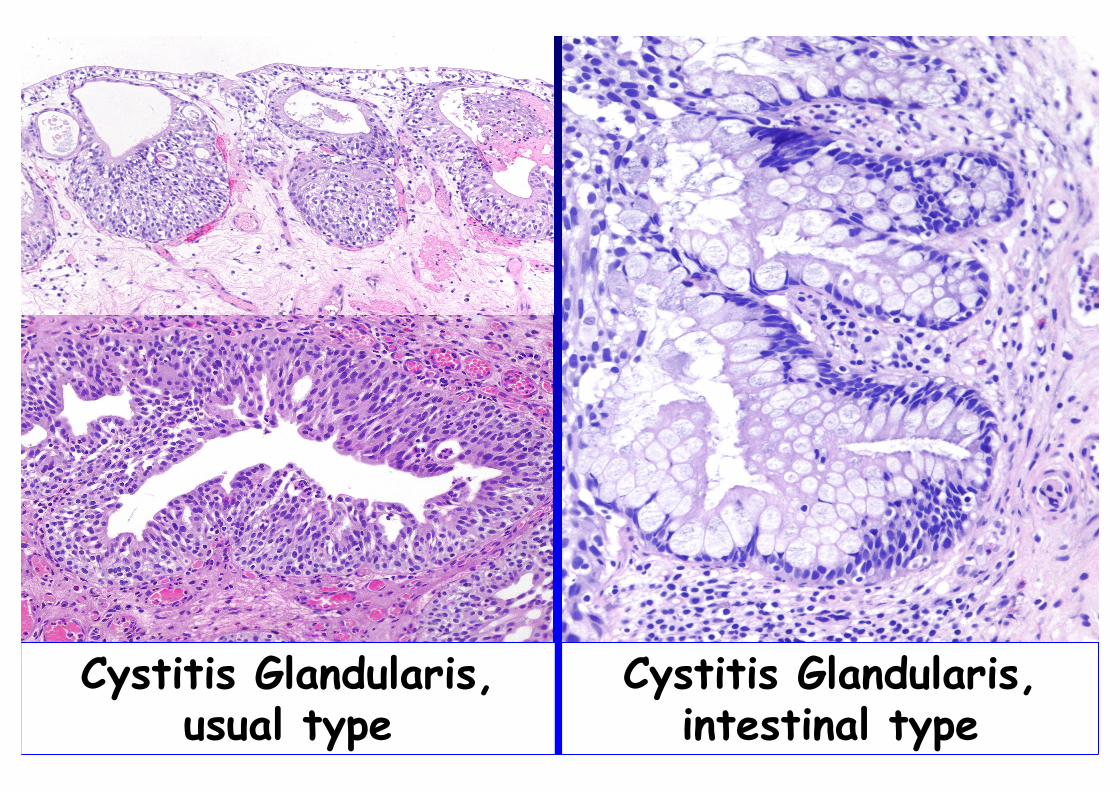
Cystitis Glandularis, usual type
Cystitis Glandularis, intestinal type
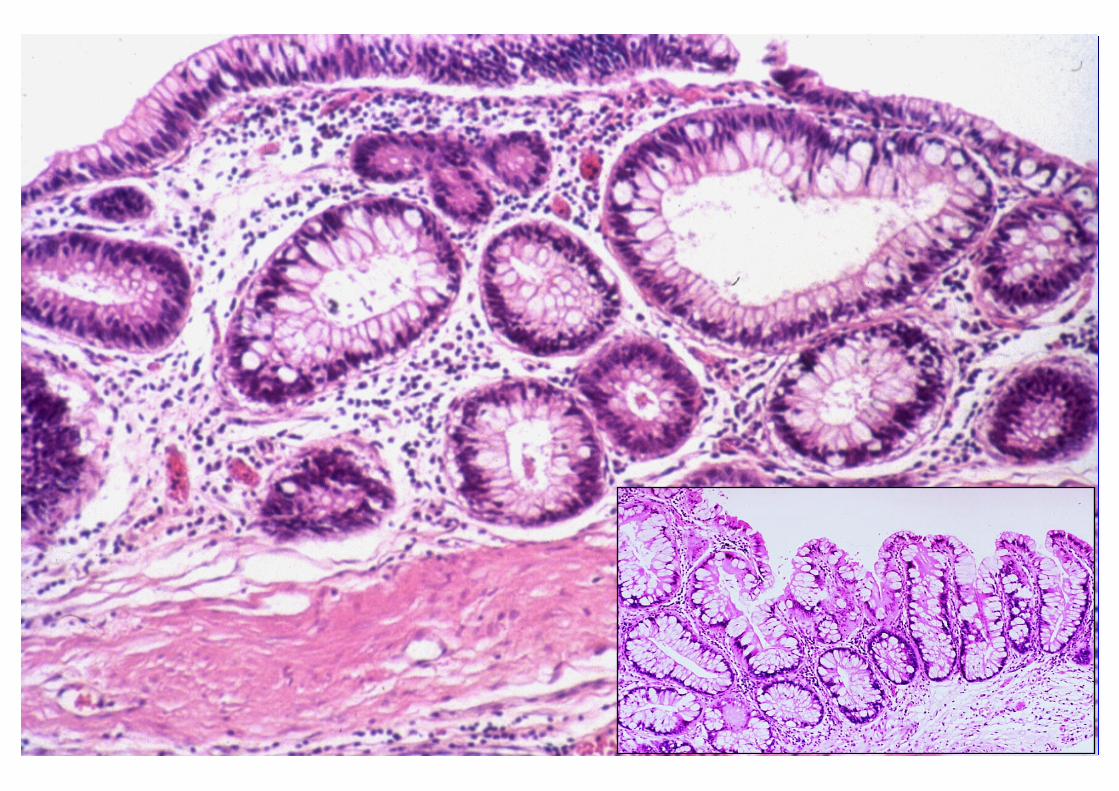
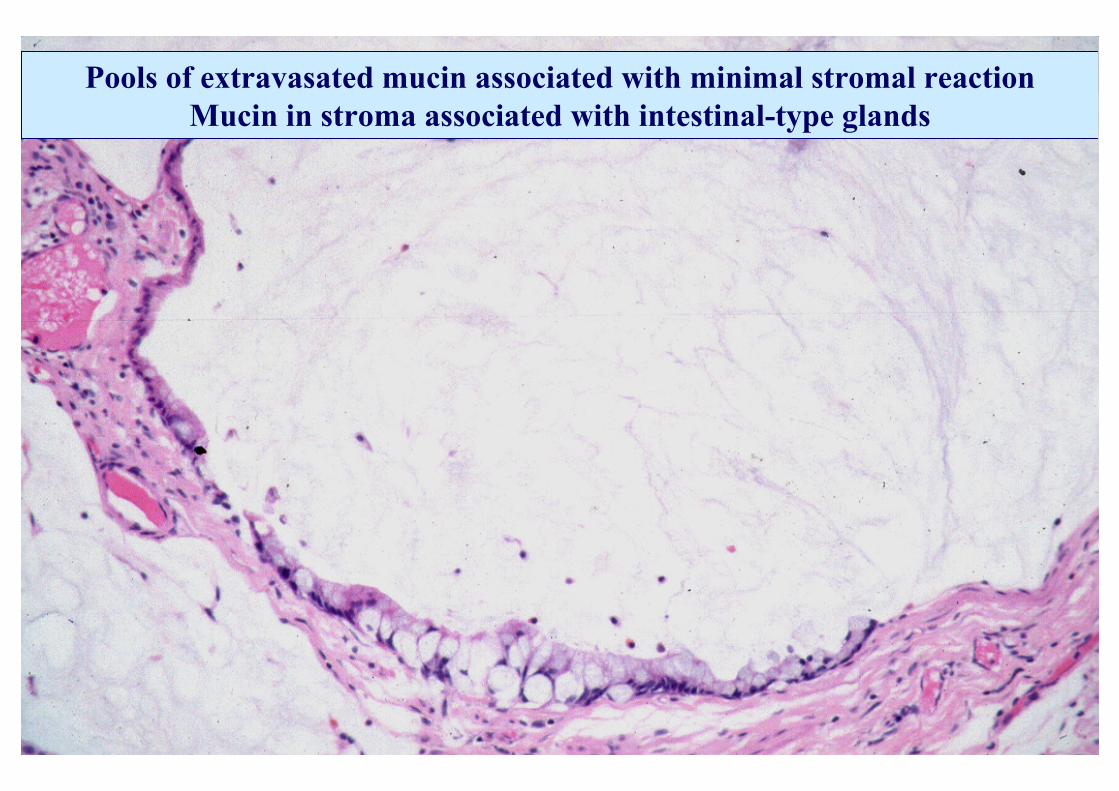
Pools of extravasated mucin associated with minimal stromal reaction Mucin in stroma associated with intestinal-type glands
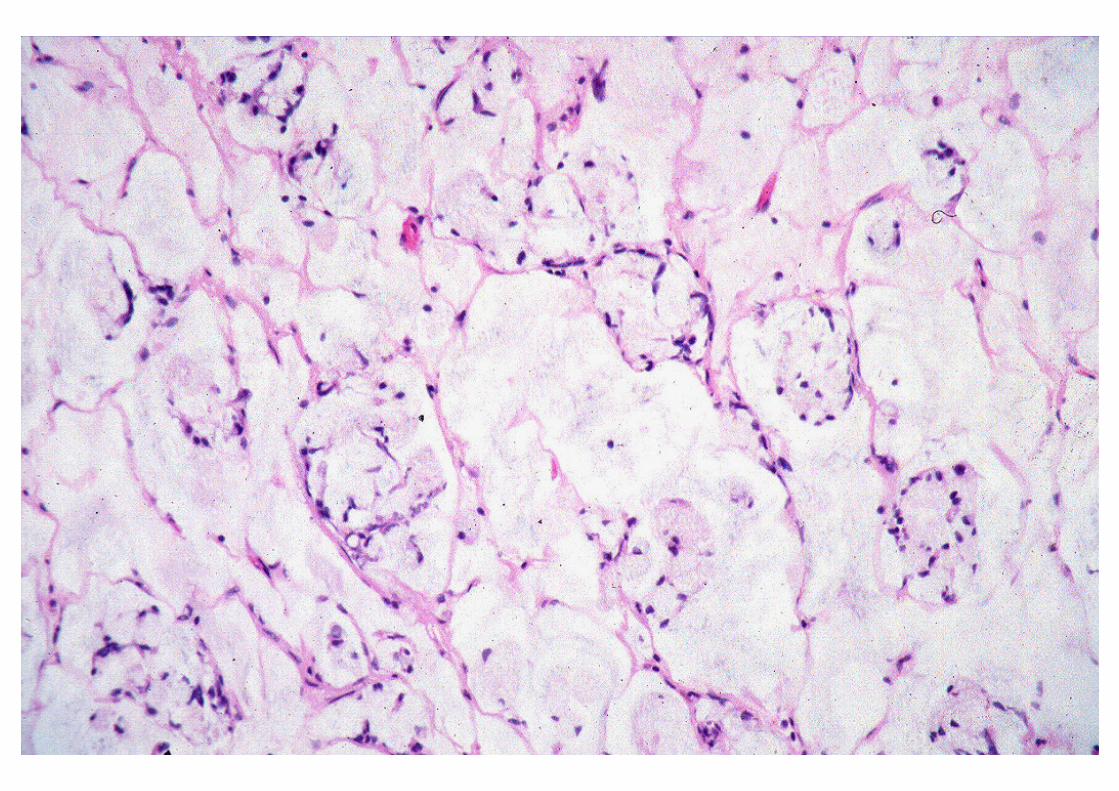
Cystitis Glandularis with Mucin Extravasation:
• Orderly distribution
• No cells floating in mucin
• Lack of atypia of lining cells
• No muscularis propria invasion
Florid Cystitis Glandularis of Intestinal Florid Cystitis Glandularis of Intestinal Type with Mucin ExtravasationType with Mucin Extravasation
Differential Diagnosis
Endocervicosis
Bladder Adenocarcinoma
Urachal Adenocarcinoma
Metastatic Rectal Adenocarcinoma

BLADDER ADENOCARCINOMABLADDER ADENOCARCINOMA
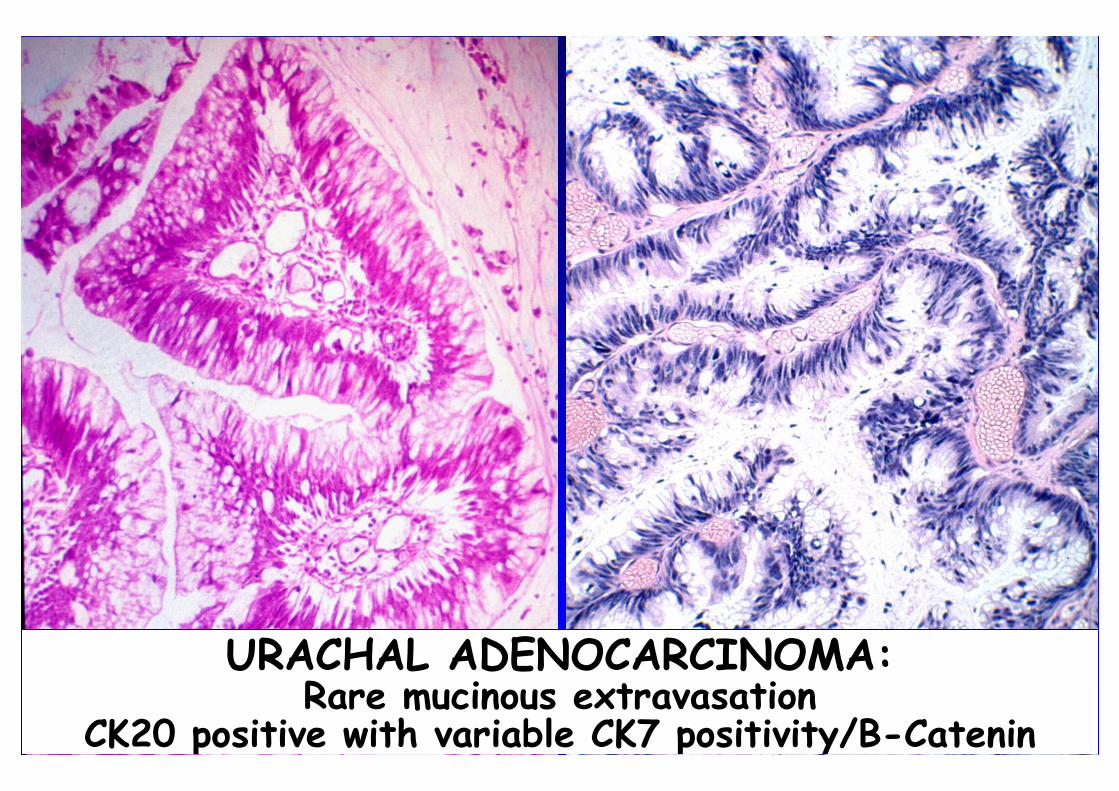
URACHAL ADENOCARCINOMA: Rare mucinous extravasation
CK20 positive with variable CK7 positivity/B-Catenin nuclear
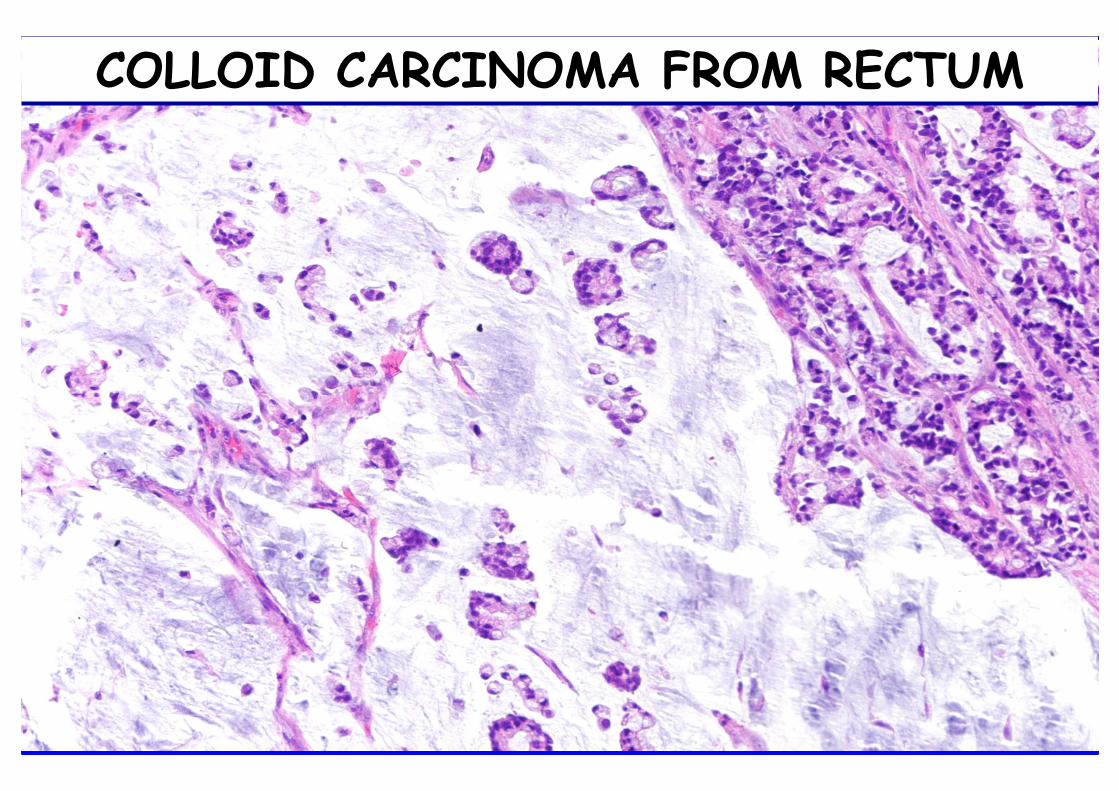
COLLOID CARCINOMA FROM RECTUM
COLLOID CARCINOMA FROM RECTUM
Bladder Adenocarcinoma
• Immunohistochemical profile intermediate between urothelial and colorectal carcinoma . Nuclear B-Catenin
•More frequently CK7 and thrombomodulin while colon carcinoma expresses more frequently CK20 and β-catenin nuclear-cytoplasmic
• CDX2 and villin positivity favor colorectal carcinoma
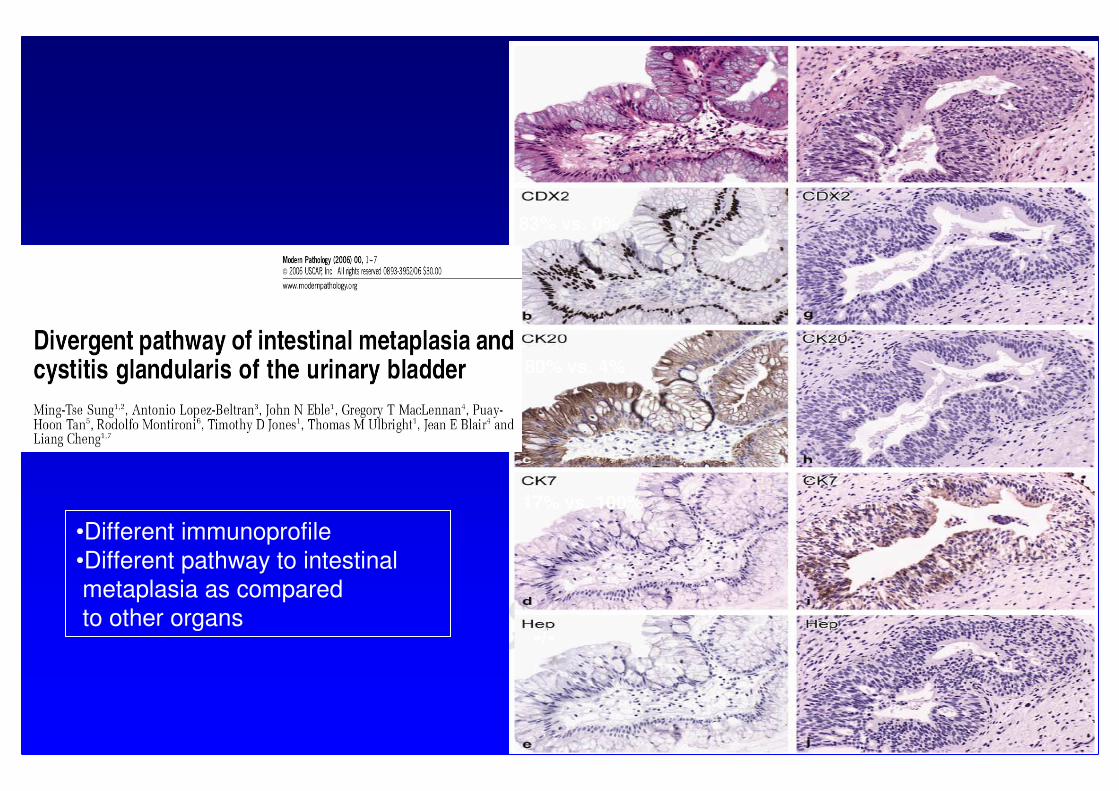
83% vs. 0%
80% vs. 4%
17% vs. 100%
-/-
•Different immunoprofile
•Different pathway to intestinal
metaplasia as compared
to other organs


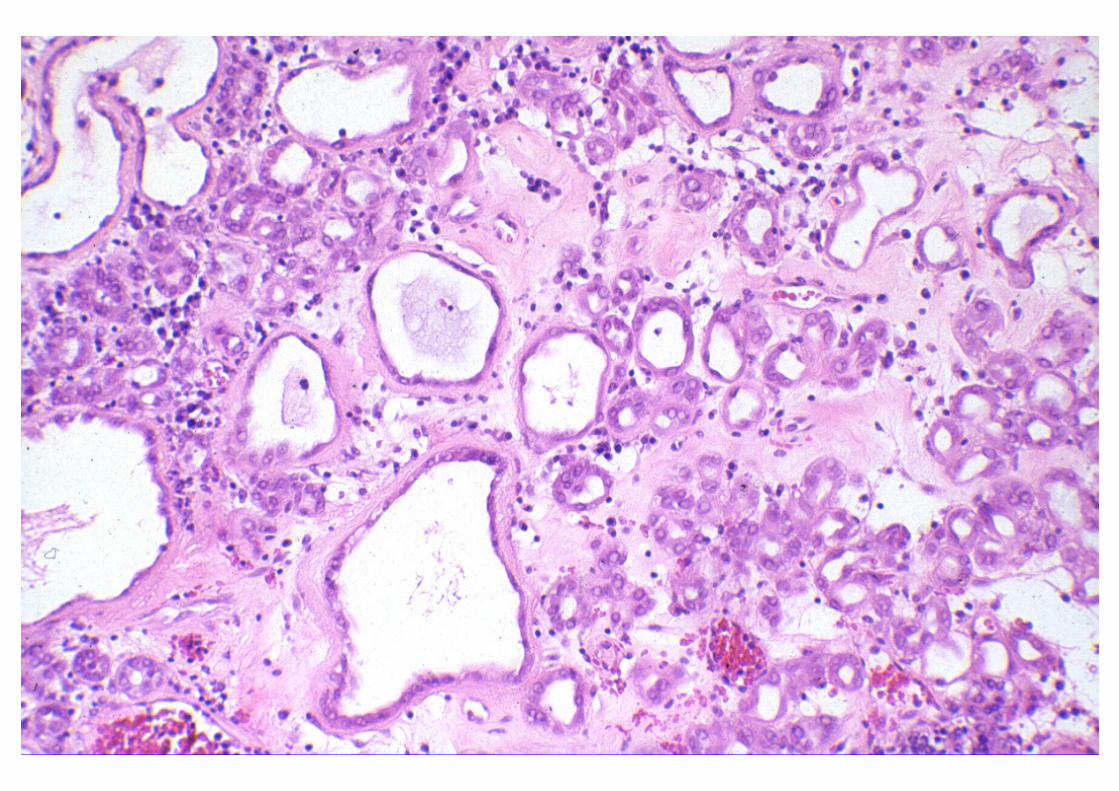
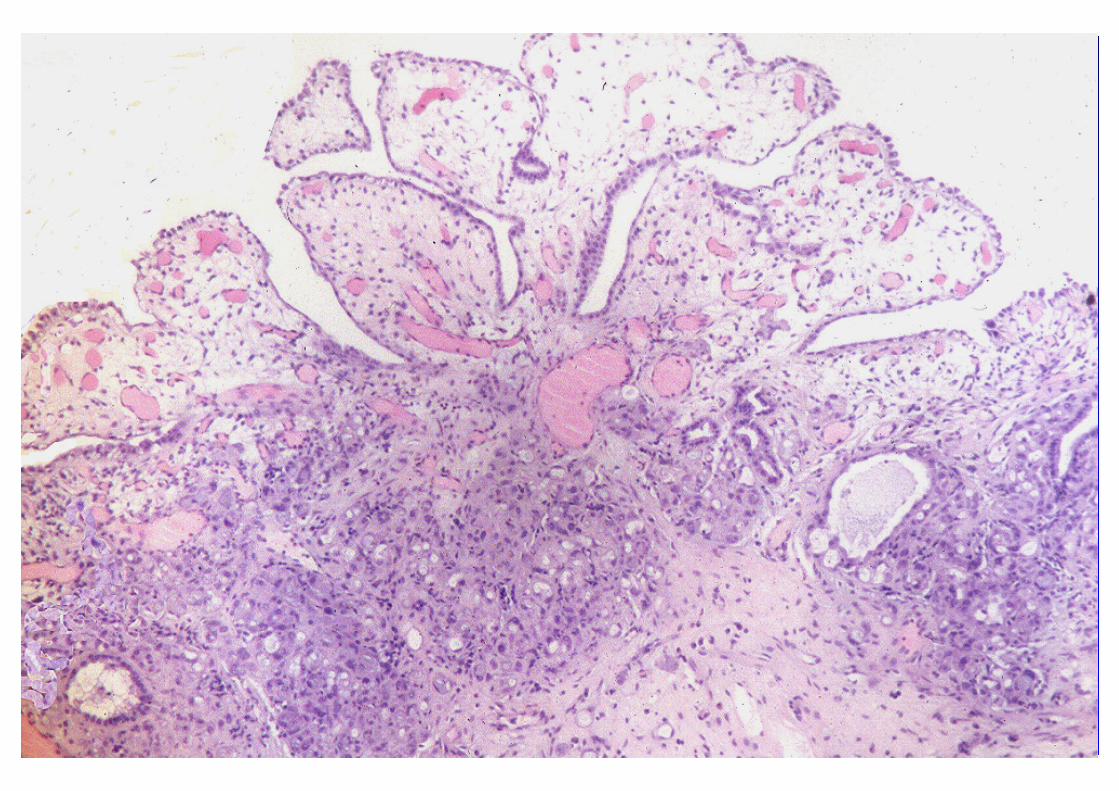
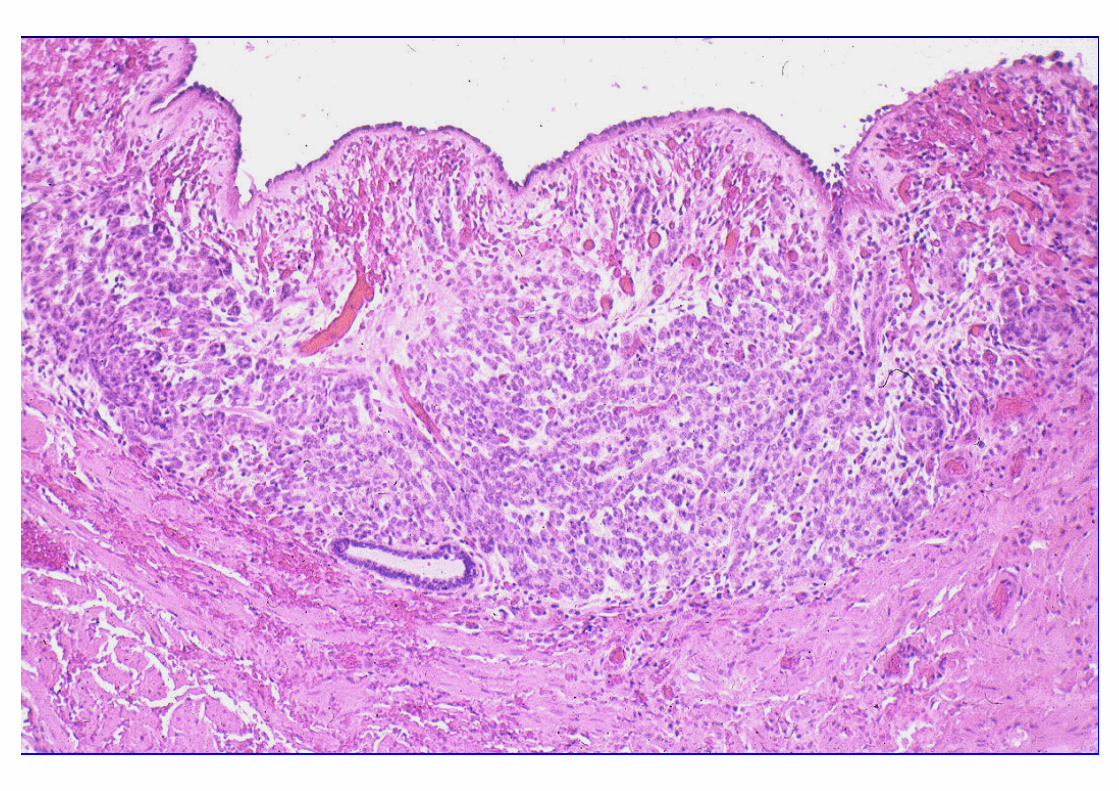
NEPHROGENIC ADENOMANEPHROGENIC ADENOMA4-81 Yrs (Av 41 yrs)
M:F = 2:1GU Surgery: 61%GU Stones: 14%GU Trauma: 9%
Renal Transplant: 8%
Bladder 80%Urethra 12% (1/4 TIC)Ureter 8%
Location:
NEPHROGENIC ADENOMANEPHROGENIC ADENOMA
Papillary 56%Polypoid 10%Sessile 34%
At least 17% multiple
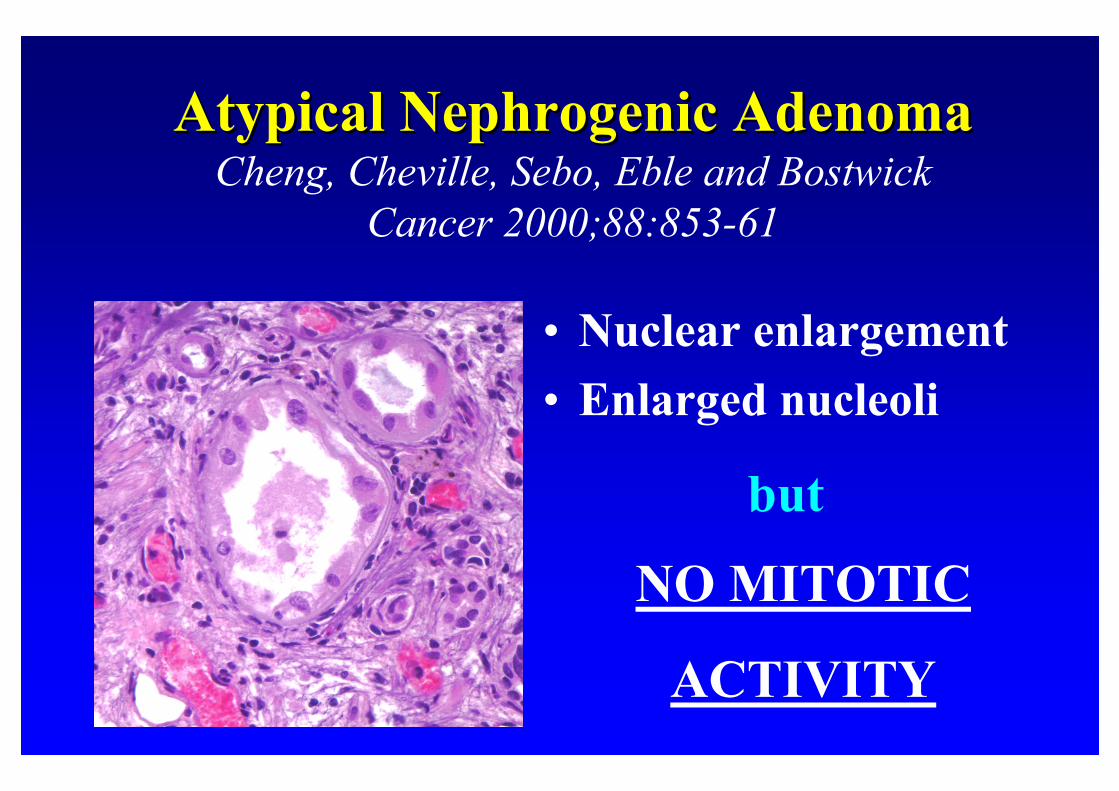
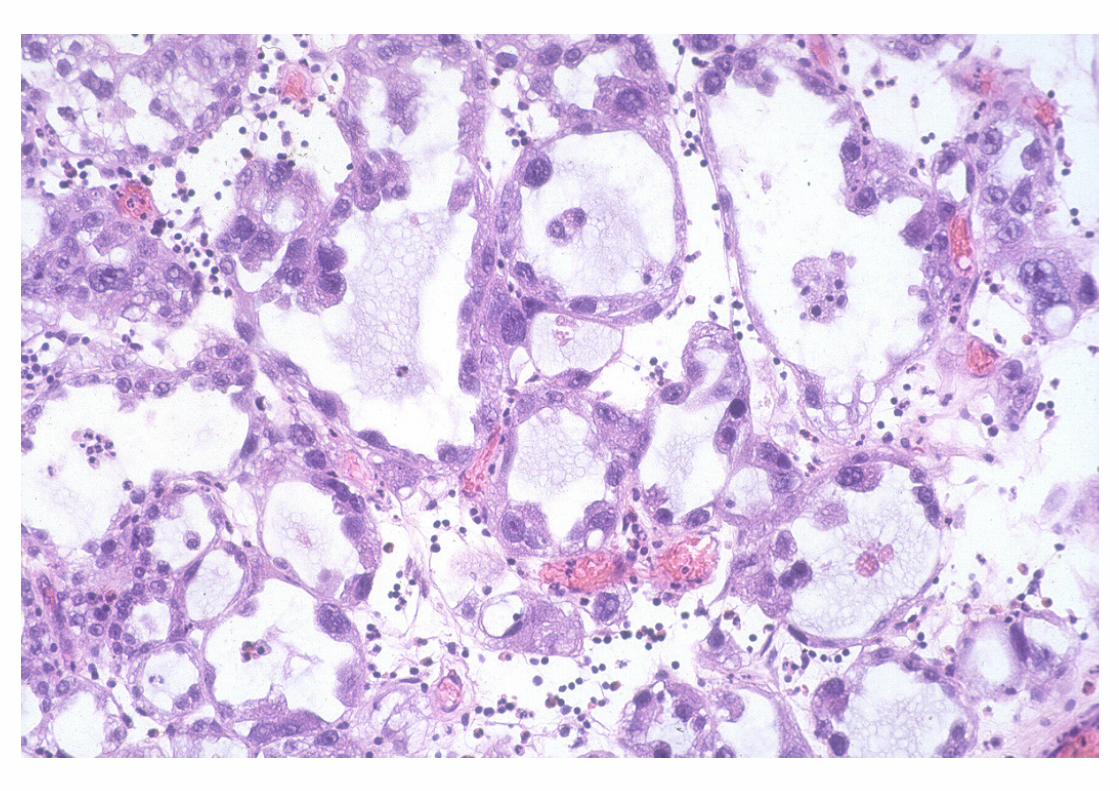
Atypical Nephrogenic AdenomaAtypical Nephrogenic AdenomaCheng, Cheville, Sebo, Eble and Bostwick
Cancer 2000;88:853-61
• Nuclear enlargement
• Enlarged nucleoli
NO MITOTIC
ACTIVITY
but

WORRISOME FEATURES:
HOBNAILING CELLS
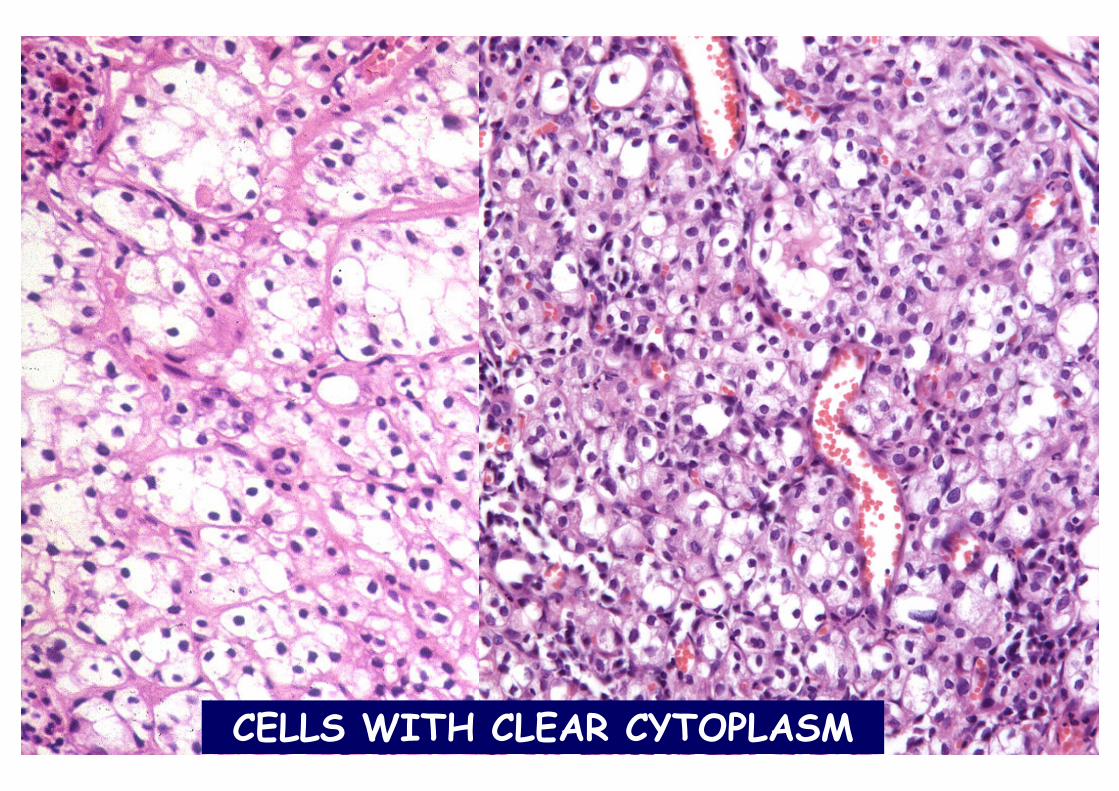
CELLS WITH CLEAR CYTOPLASM
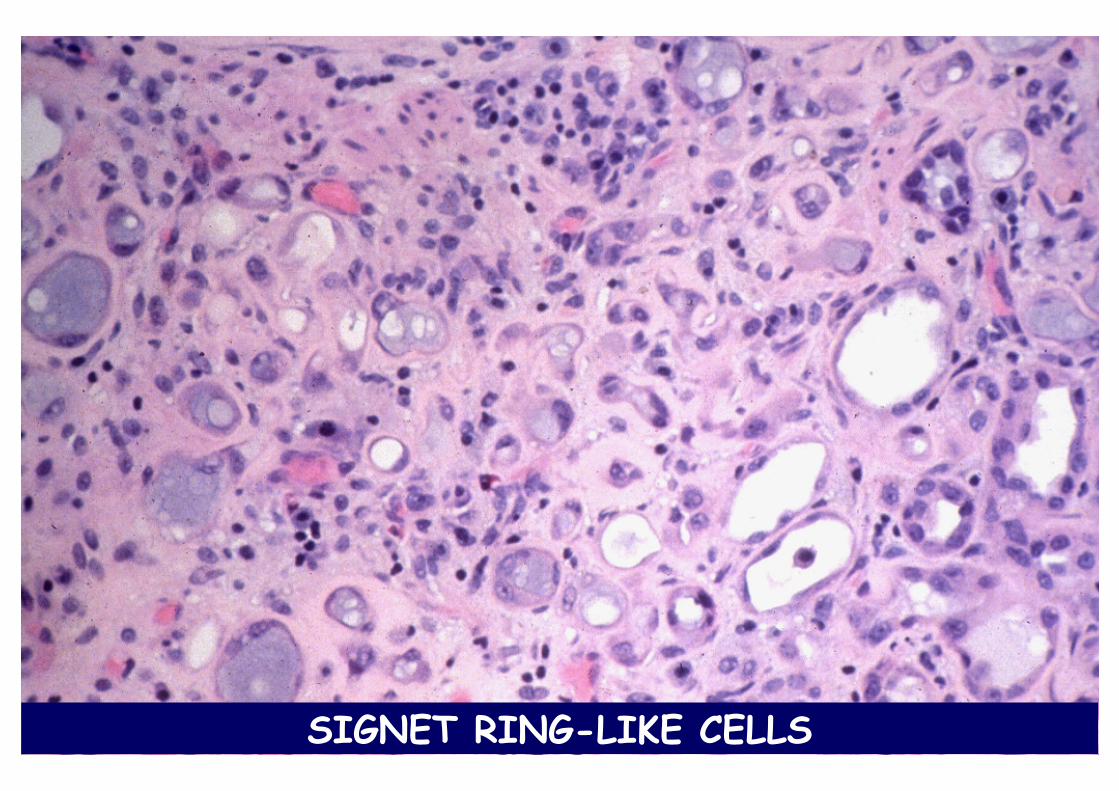
SIGNET RING-LIKE CELLS
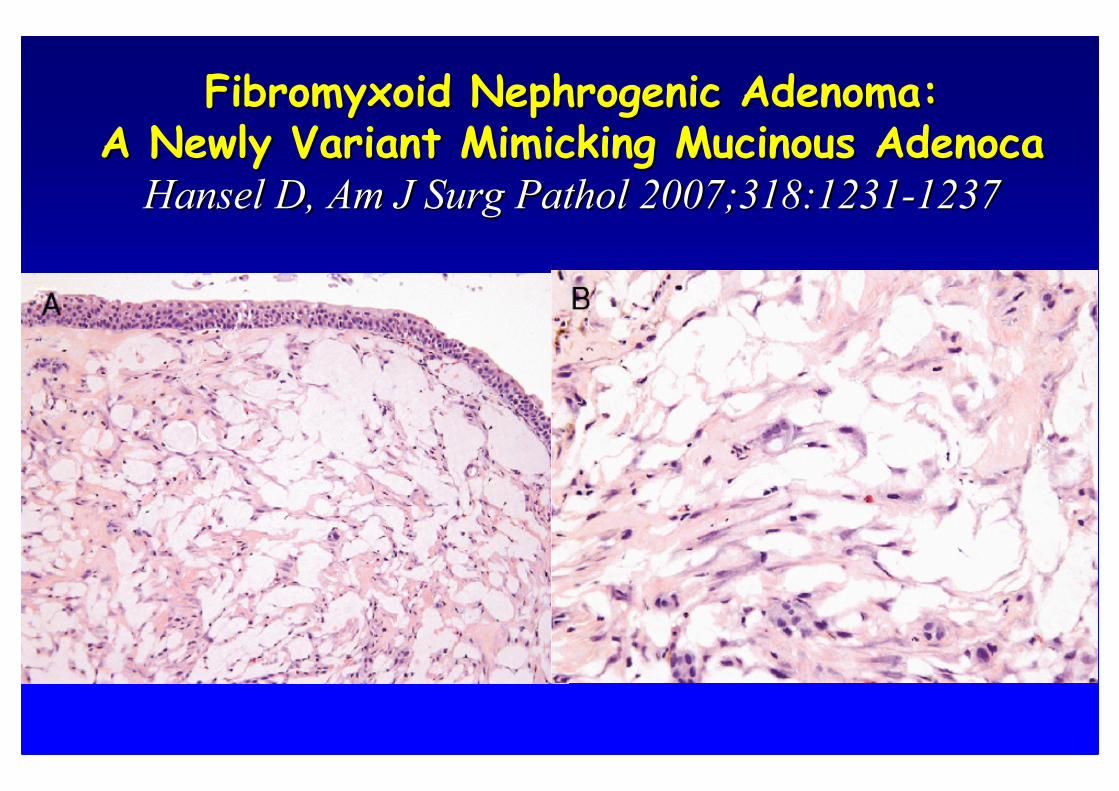
Fibromyxoid Nephrogenic Adenoma: Fibromyxoid Nephrogenic Adenoma: A Newly Variant Mimicking Mucinous A Newly Variant Mimicking Mucinous AdenocaAdenoca
Hansel D, Am J Hansel D, Am J SurgSurg PatholPathol 2007;318:12312007;318:1231--12371237
NEPHROGENIC ADENOMANEPHROGENIC ADENOMADifferential Diagnosis
• Clear cell carcinoma• Nested variant of transitional cell carcinoma• Prostatic carcinoma (urethra)• Signet ring cell carcinoma, primary or metastatic
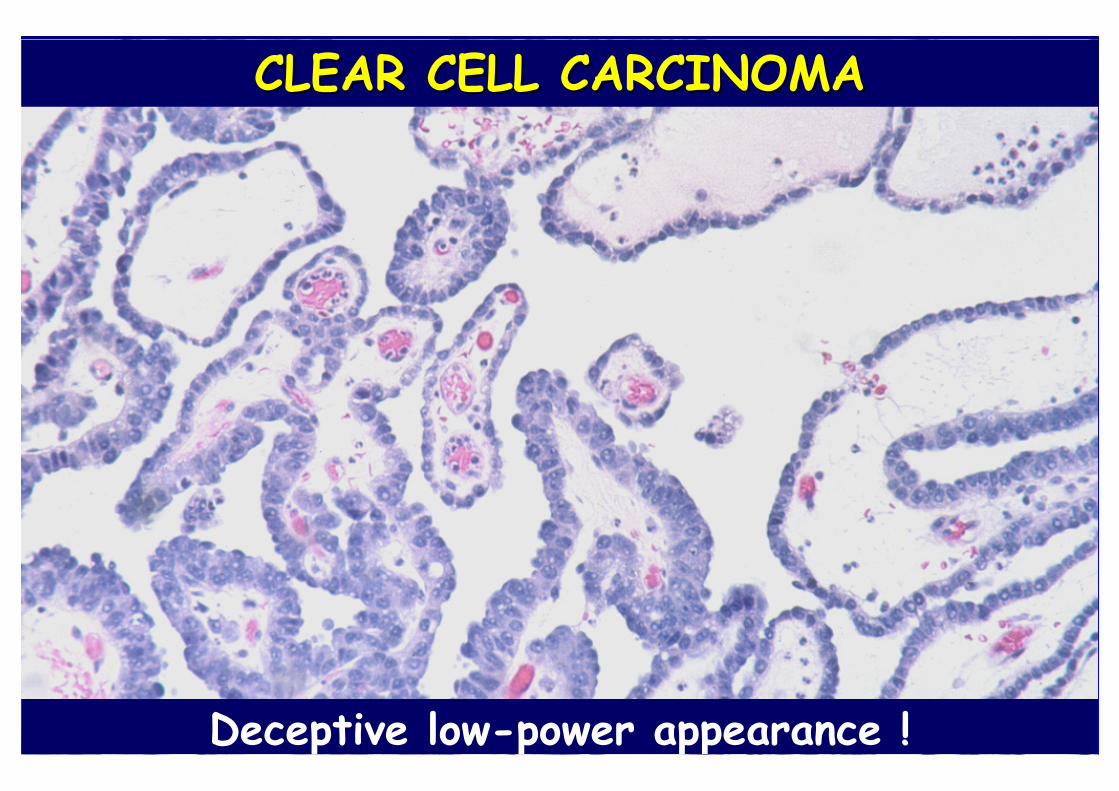
CLEAR CELL CARCINOMACLEAR CELL CARCINOMA
Deceptive low-power appearance !
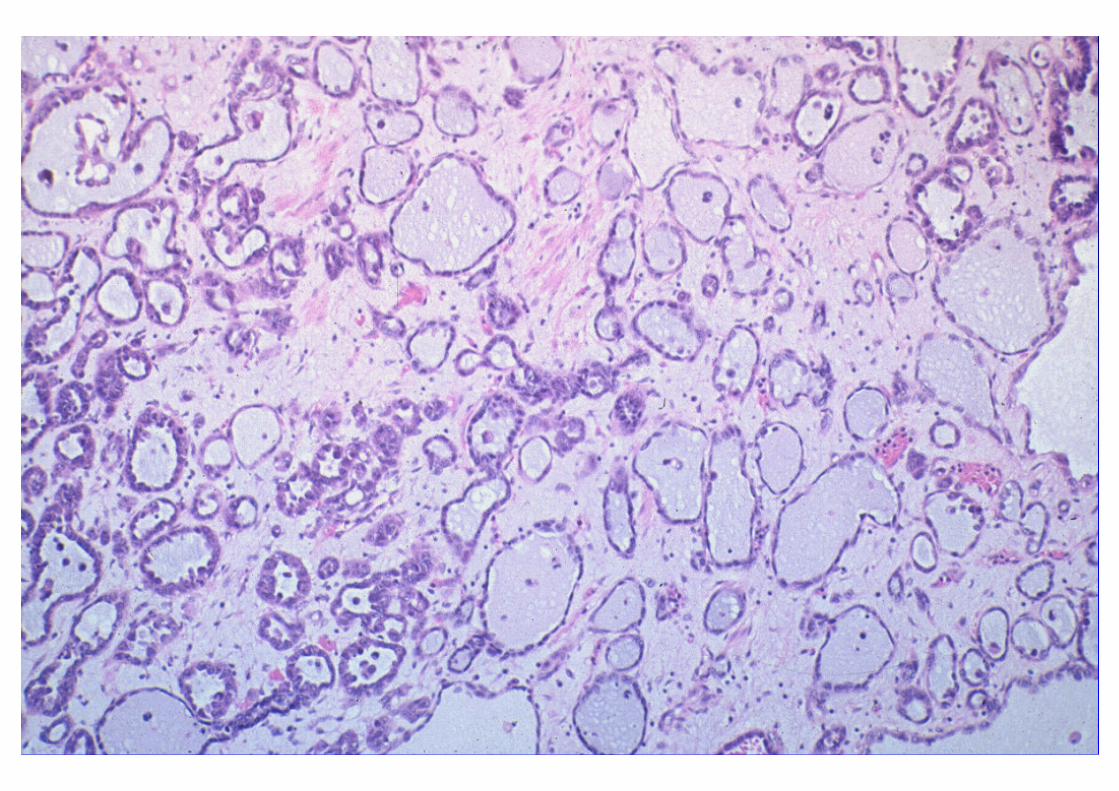
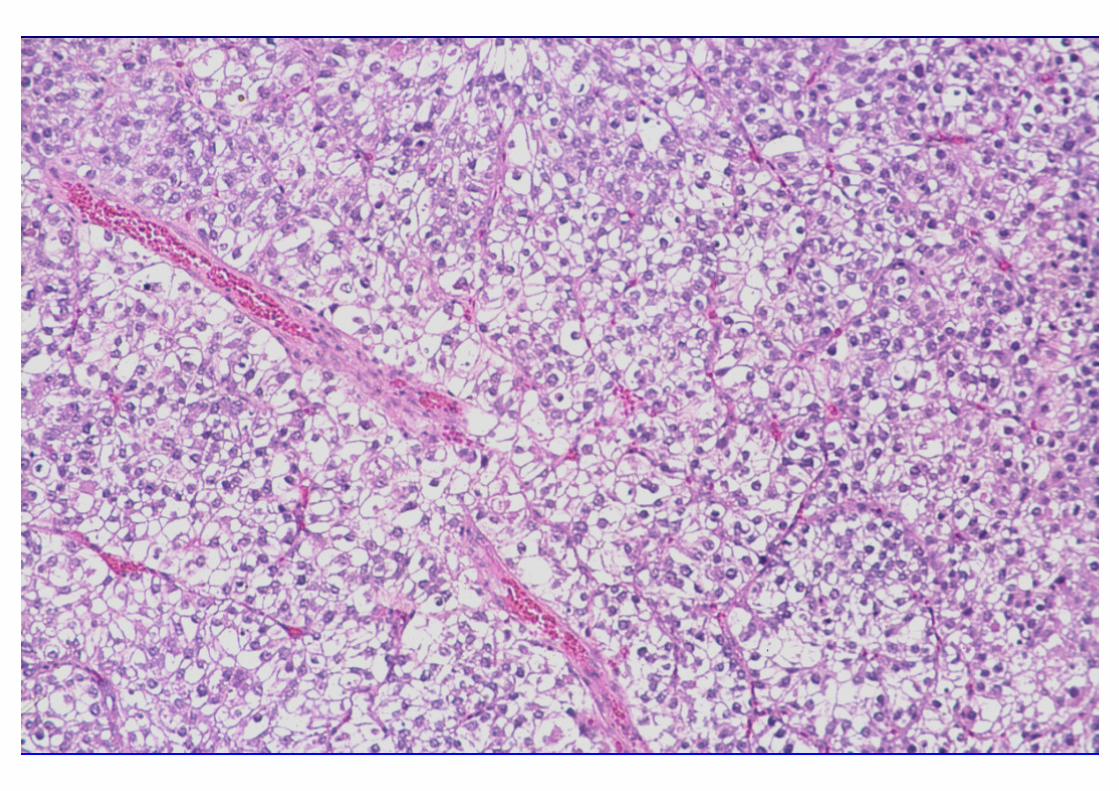
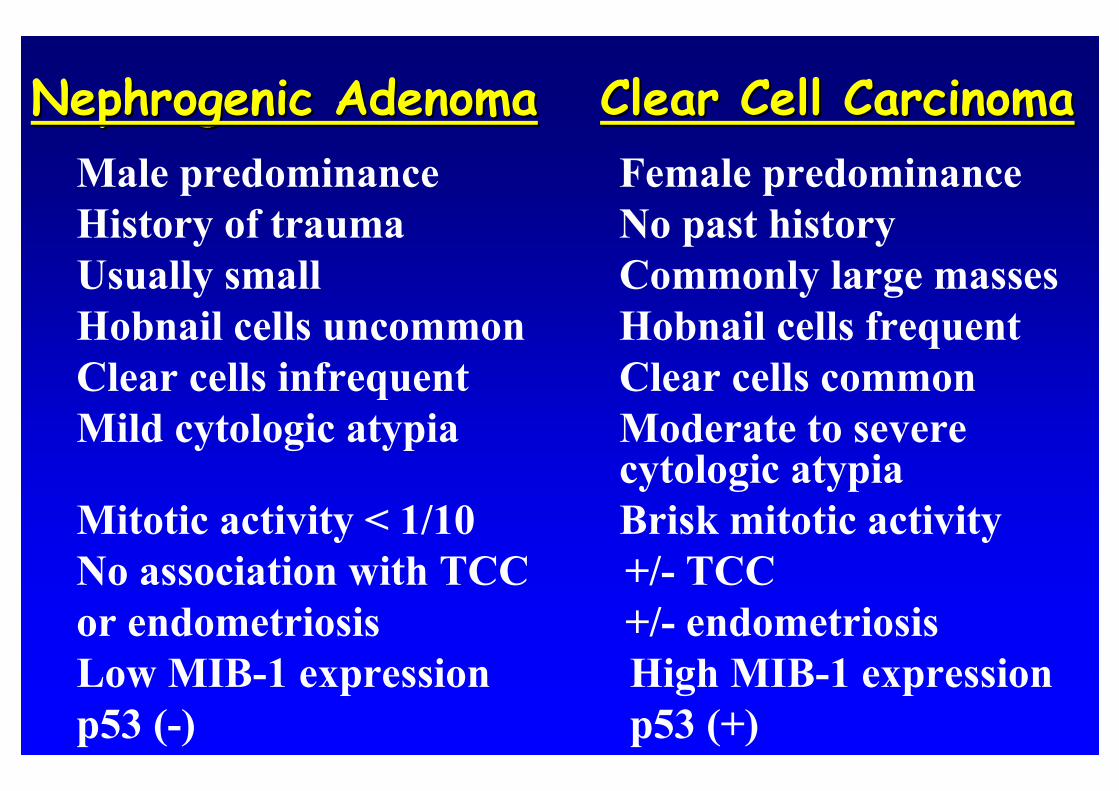
Nephrogenic AdenomaNephrogenic Adenoma Clear Cell CarcinomaClear Cell Carcinoma
Male predominance Female predominanceHistory of trauma No past historyUsually small Commonly large massesHobnail cells uncommon Hobnail cells frequentClear cells infrequent Clear cells commonMild cytologic atypia Moderate to severe
cytologic atypiaMitotic activity < 1/10 Brisk mitotic activityNo association with TCC +/- TCCor endometriosis +/- endometriosisLow MIB-1 expression High MIB-1 expressionp53 (-) p53 (+)
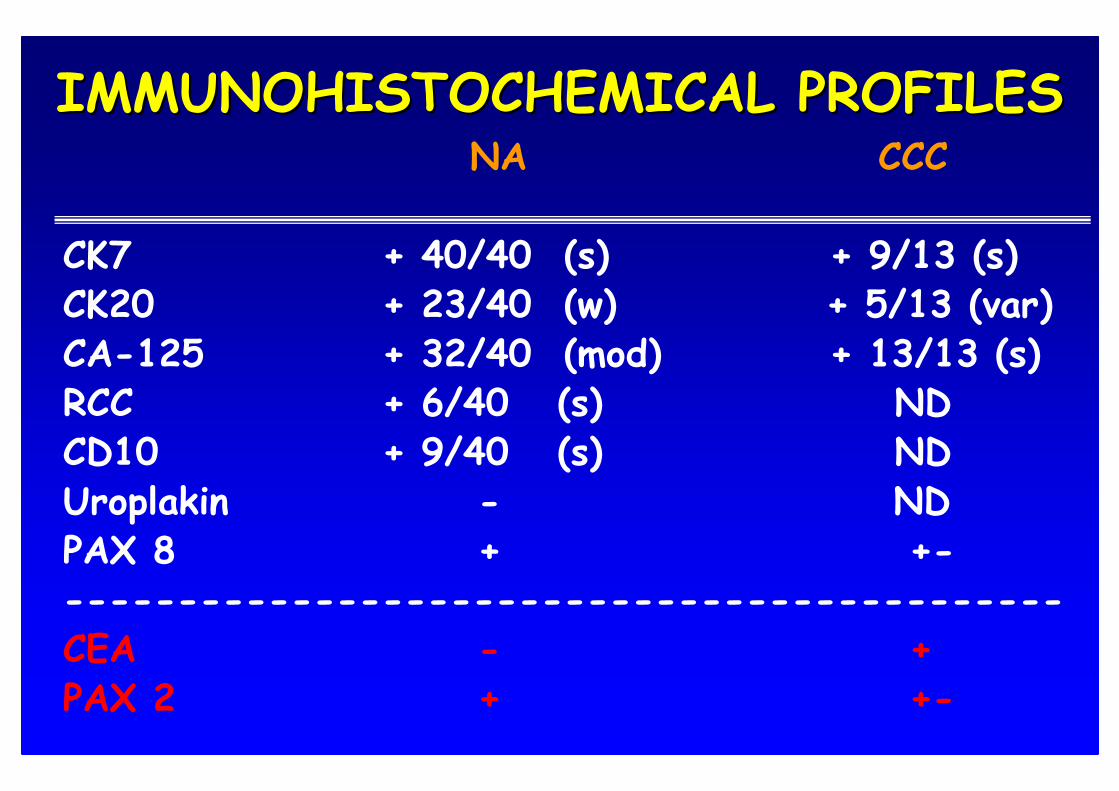
IMMUNOHISTOCHEMICAL PROFILESIMMUNOHISTOCHEMICAL PROFILESNA CCC
CK7 + 40/40 (s) + 9/13 (s)CK20 + 23/40 (w) + 5/13 (var)CA-125 + 32/40 (mod) + 13/13 (s)RCC + 6/40 (s) NDCD10 + 9/40 (s) NDUroplakin - NDPAX 8 + +---------------------------------------------CEA - +PAX 2 + +-
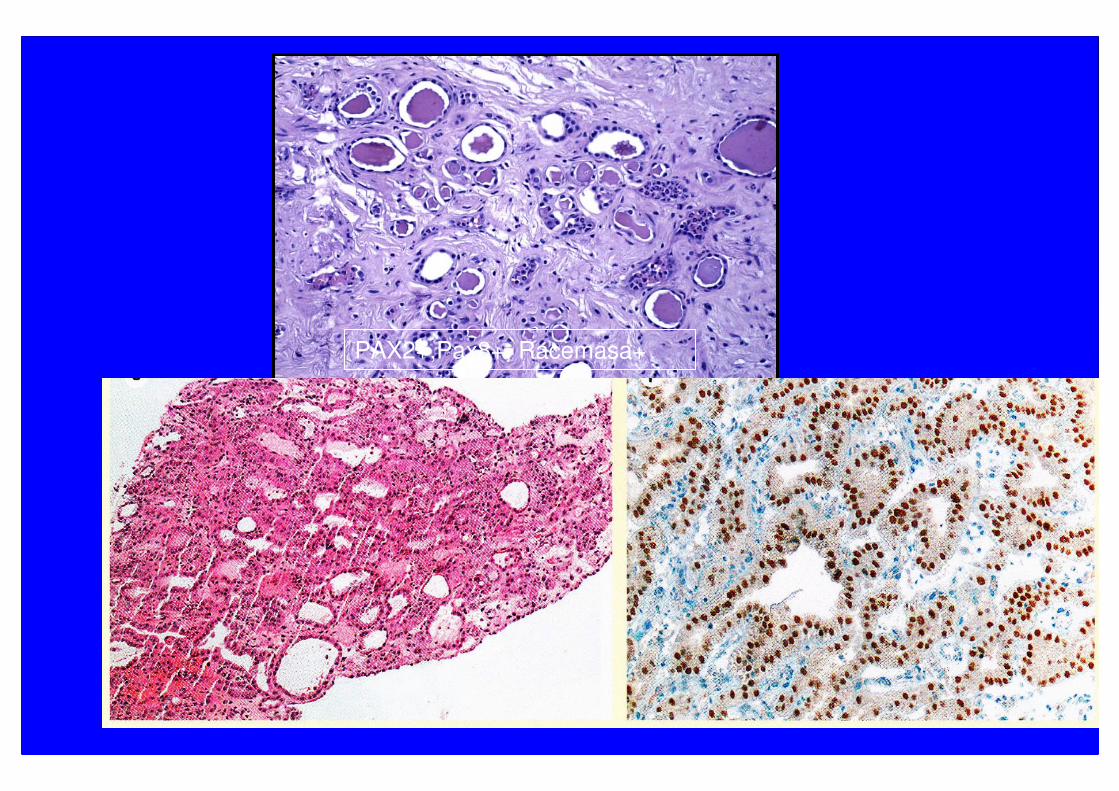
PAX2+,Pax8+, Racemasa+
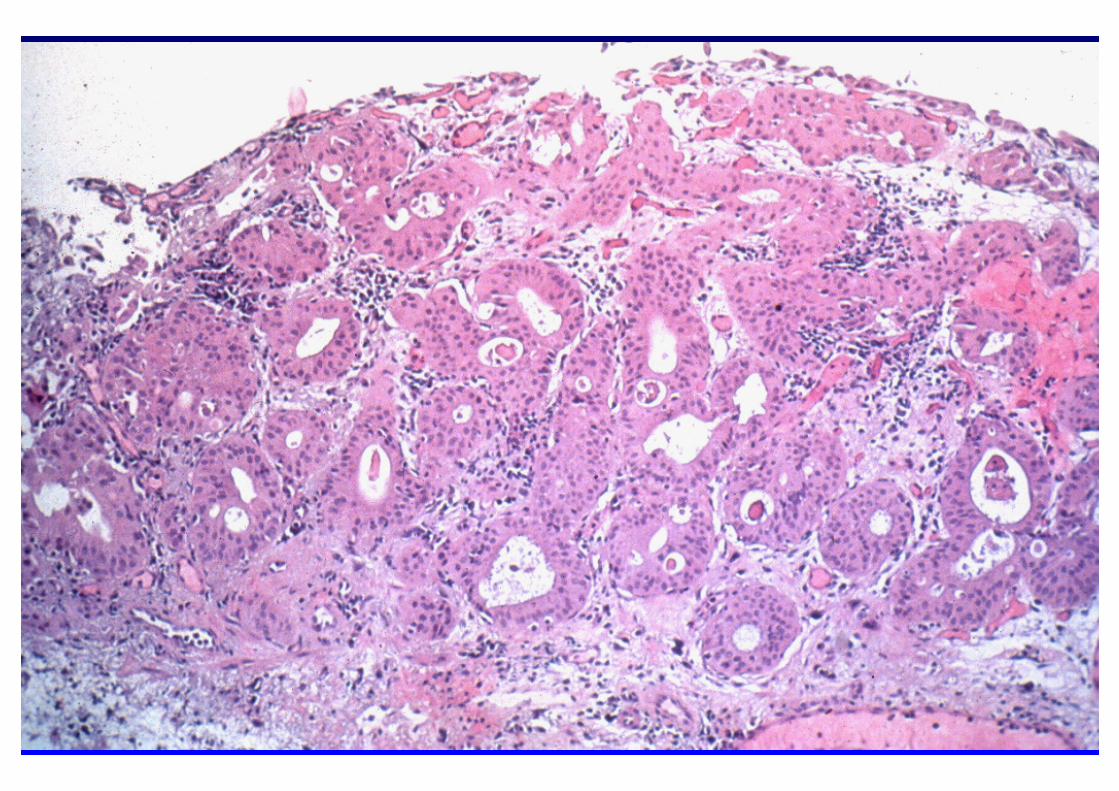
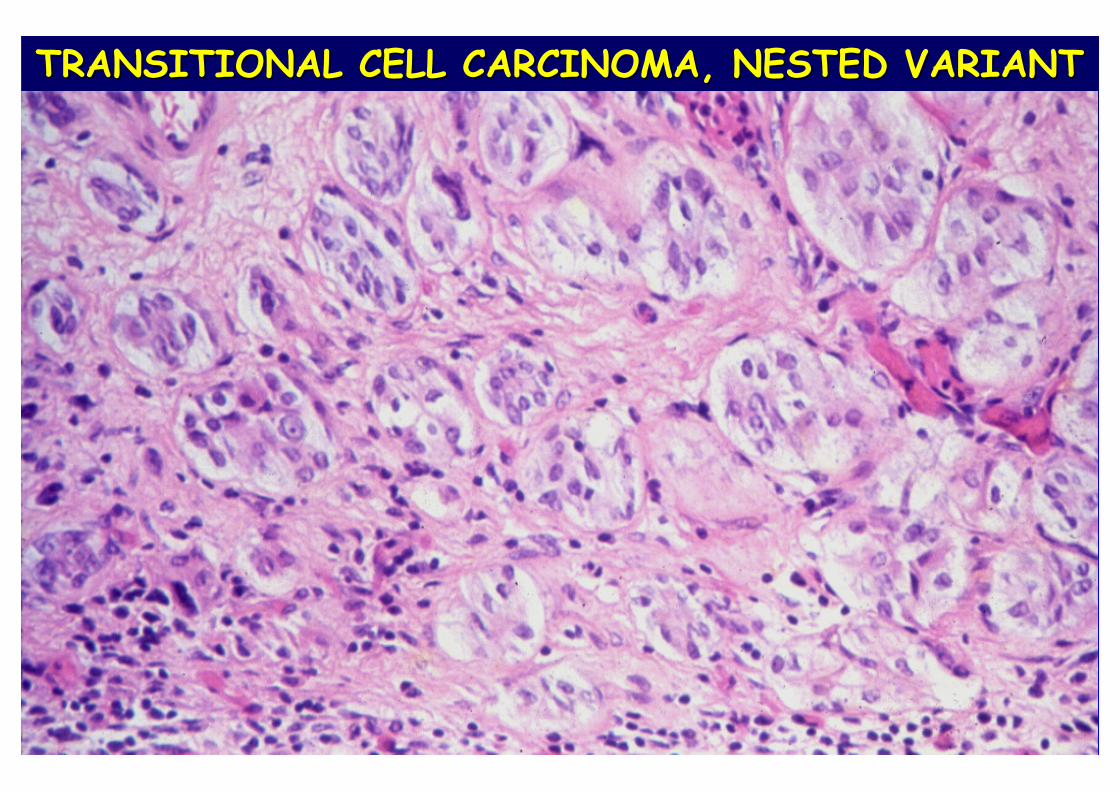
TRANSITIONAL CELL CARCINOMA, NESTED VARIANTTRANSITIONAL CELL CARCINOMA, NESTED VARIANT
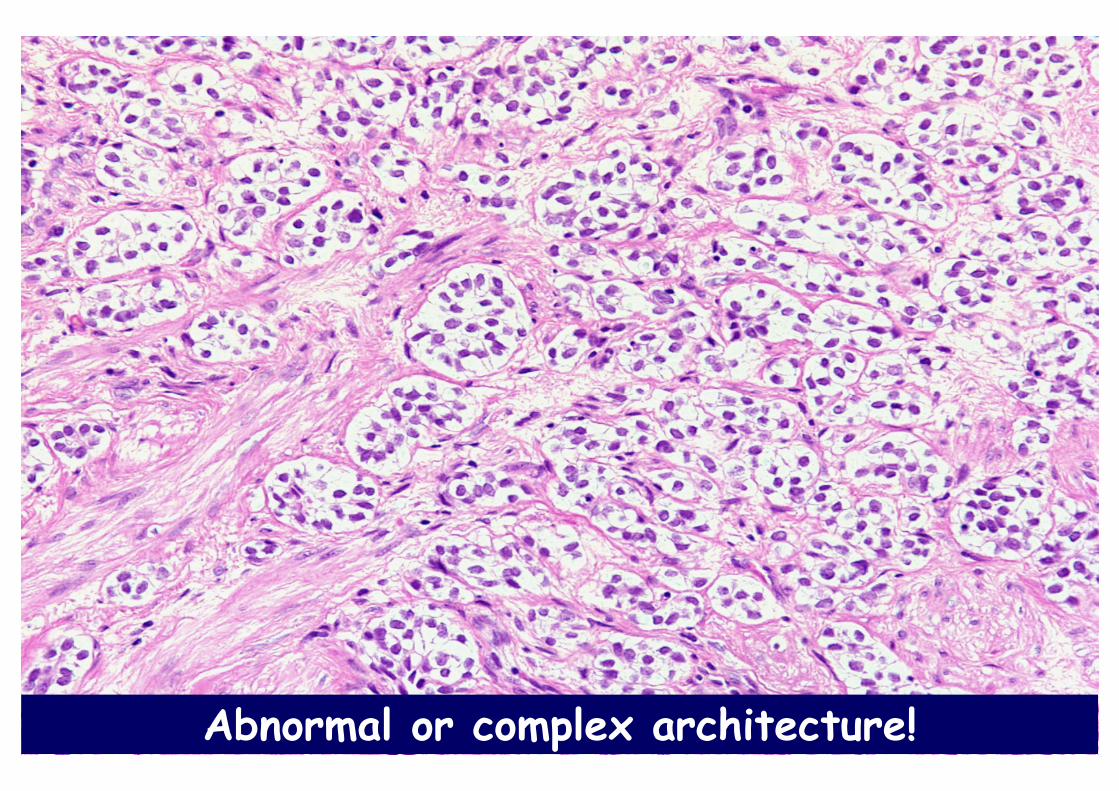
Abnormal or complex architecture!
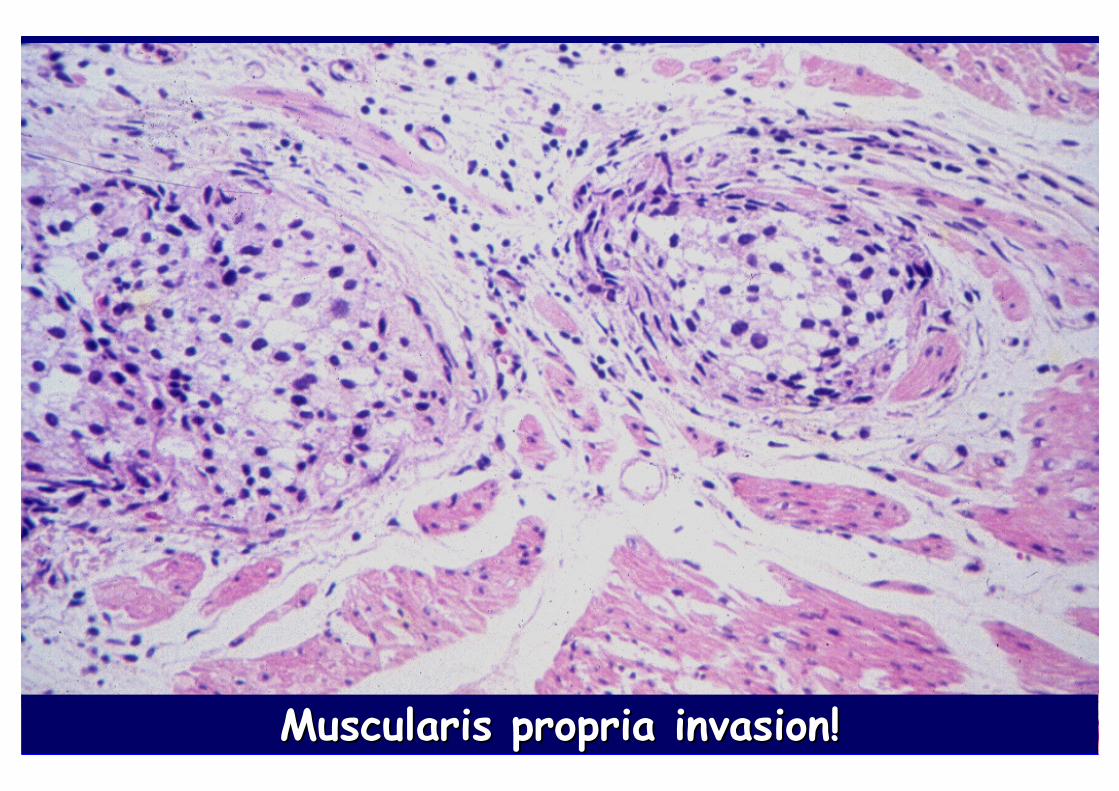
Muscularis propria invasion!Muscularis propria invasion!

• Benign lesion with no definitive premalignant potential
• NAs may recur, however, any recurrent tubulocystic or papillary lesion, especially with any degree of atypia in a woman, should raise the possibility of a CCC with deceptive benign features
• NA should be considered in the DDx of acinar proliferations in prostatic biopsies and TURPs
• There is no specific immunohistochemical profile to distinguish NA from its malignant mimics
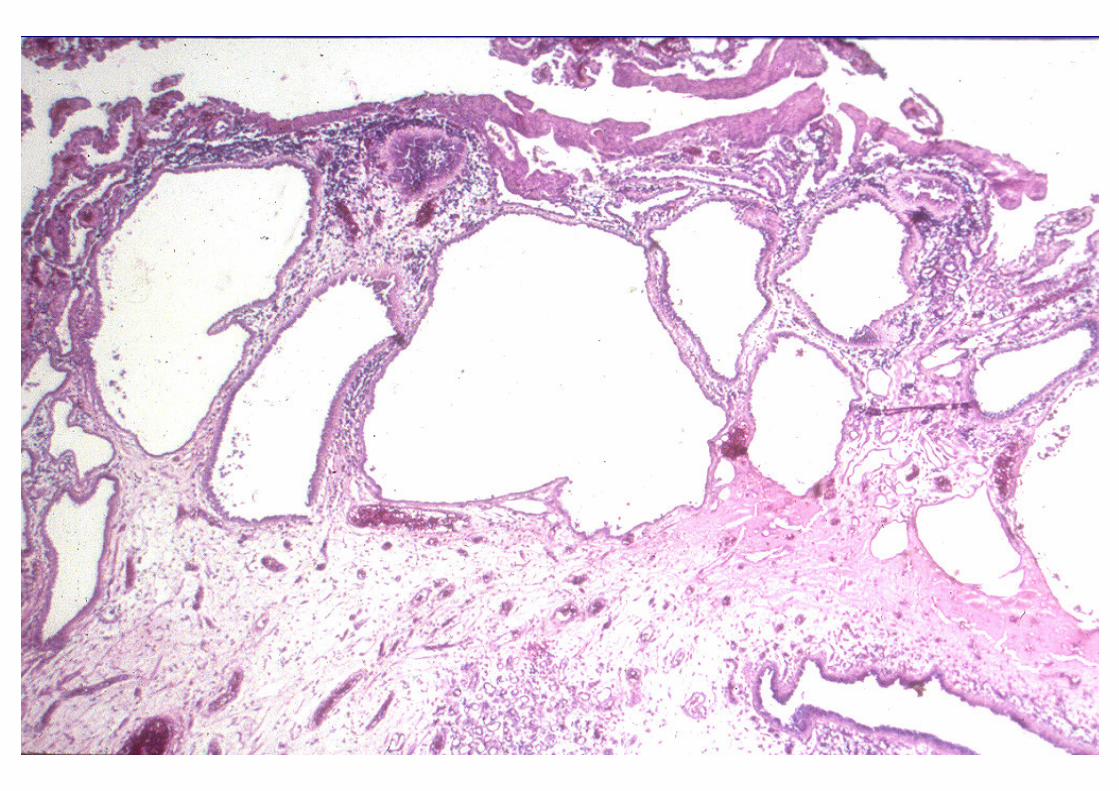
NEPHROGENIC ADENOMANEPHROGENIC ADENOMA
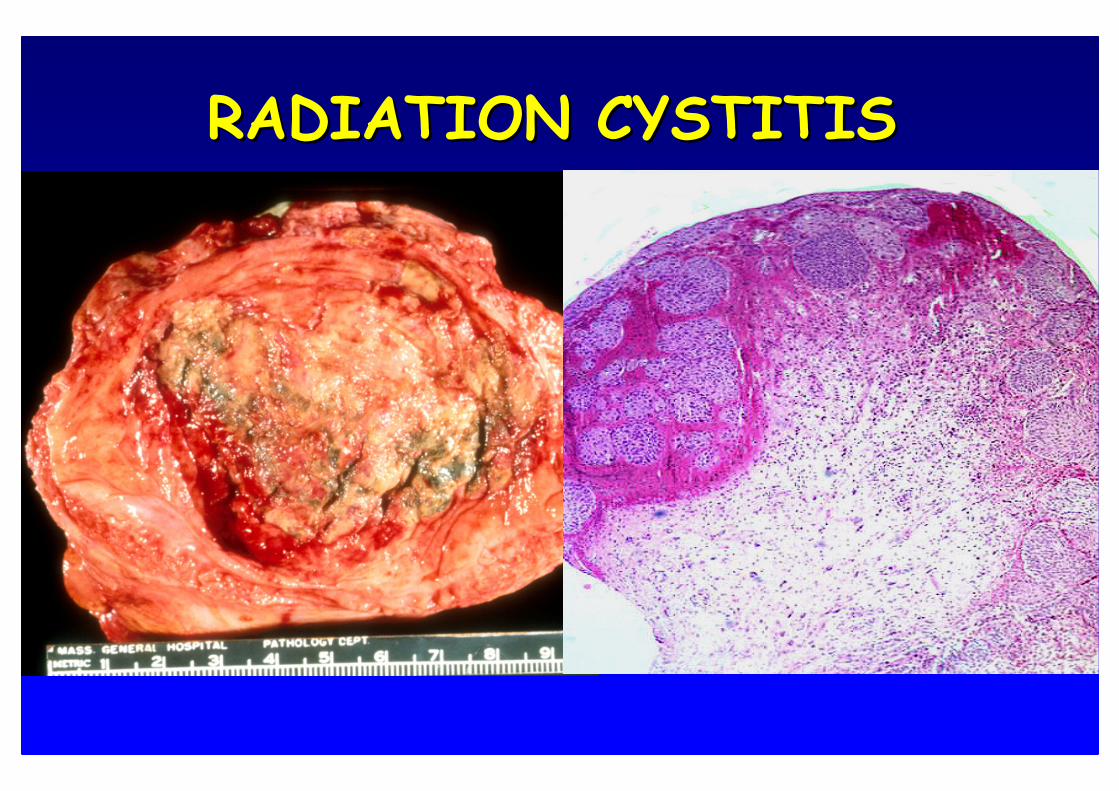
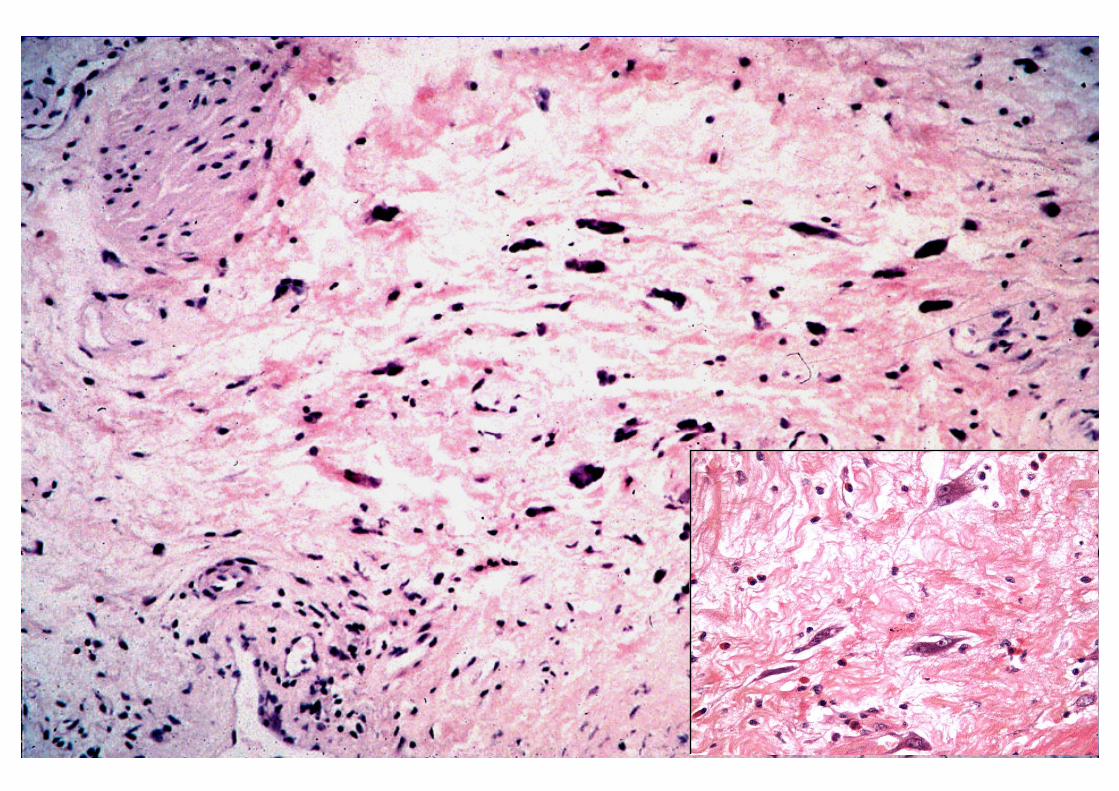
RADIATION CYSTITISRADIATION CYSTITIS

PSEUDOEPITHELIOMATOUS HYPERPLASIA

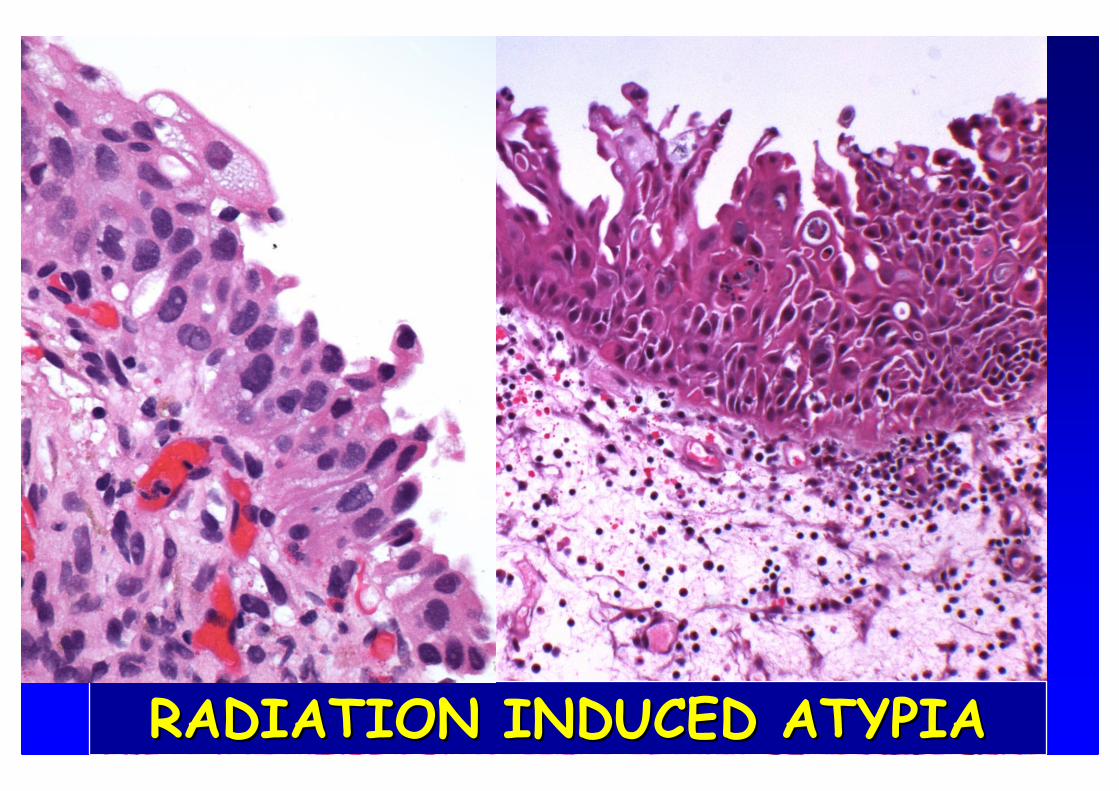
RADIATION INDUCED ATYPIARADIATION INDUCED ATYPIA

CIS
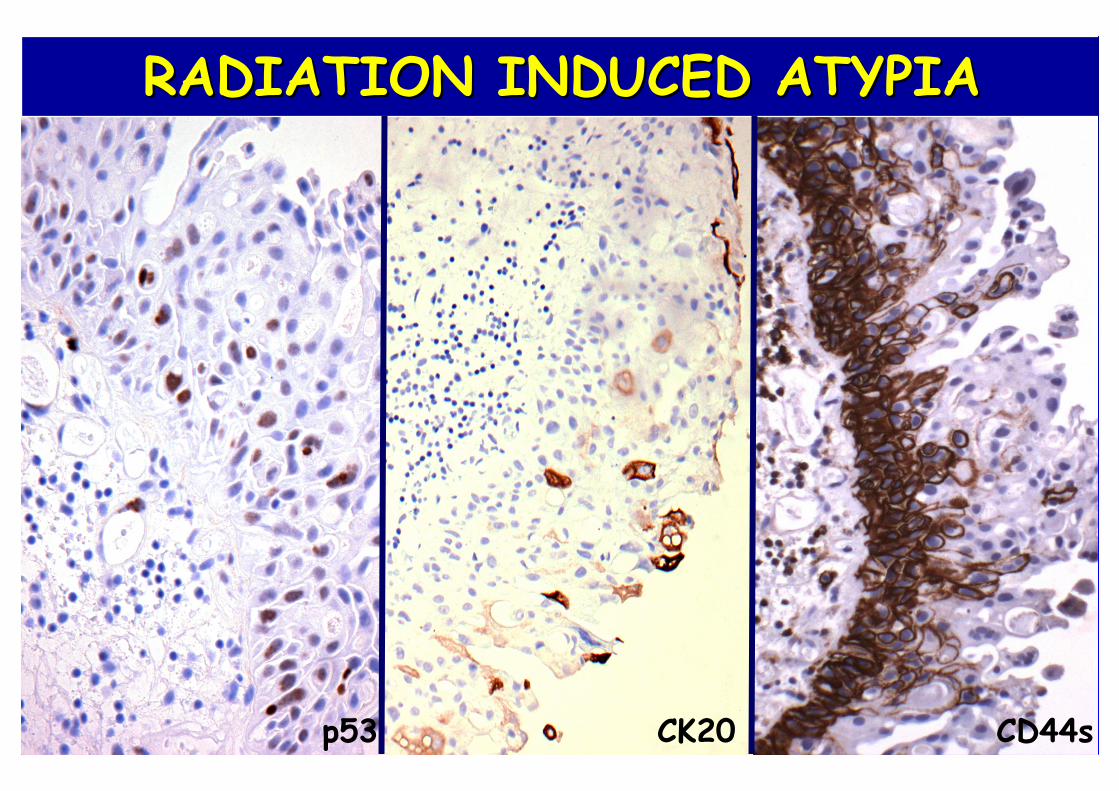
RADIATION INDUCED ATYPIARADIATION INDUCED ATYPIA
CD44sp53 CK20
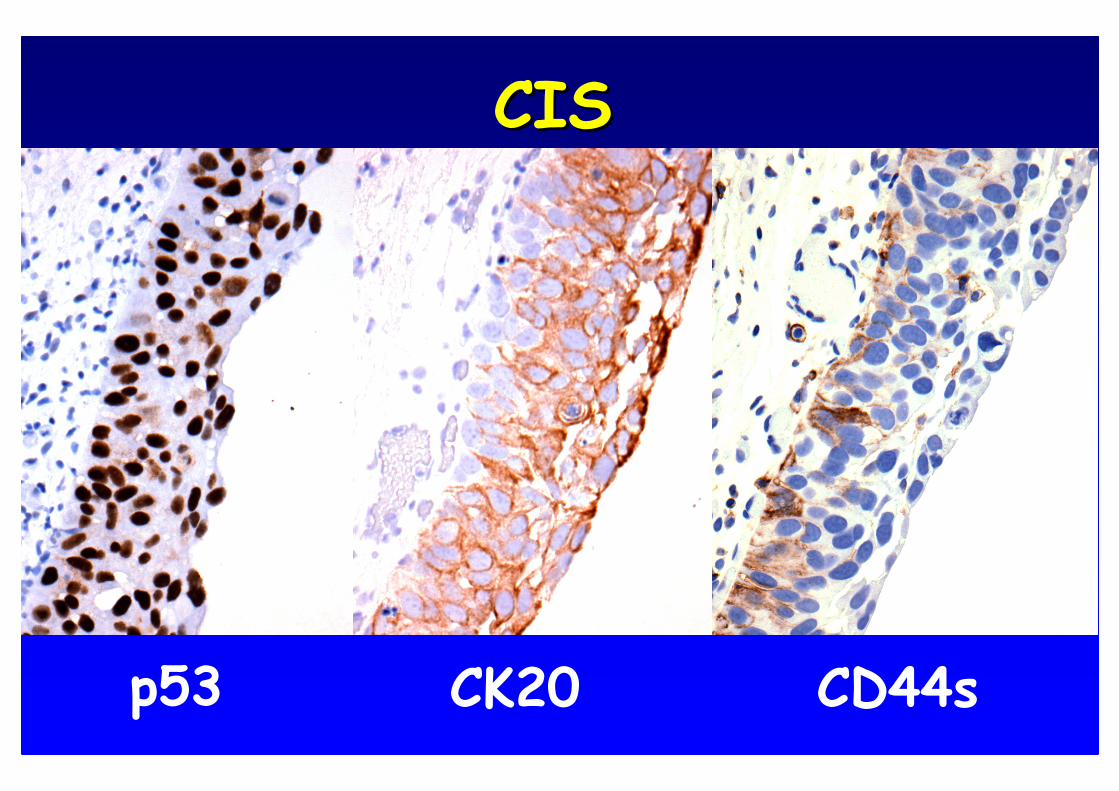
p53 CD44sCK20
CISCIS
ENDOMETRIOSIS OF THE ENDOMETRIOSIS OF THE URINARY BLADDERURINARY BLADDER
• Most common organ involved in the urinary tract• Typically affects women of reproductive age• It has been described in men with prostate cancer treated with estrogen therapy
• Catamenial exacerbations of symptoms• Secondary and significant complications• On cystoscopy: abnormalities present in 90% of women • Posterior wall and trigone more frequently involved• Rarely malignant transformation
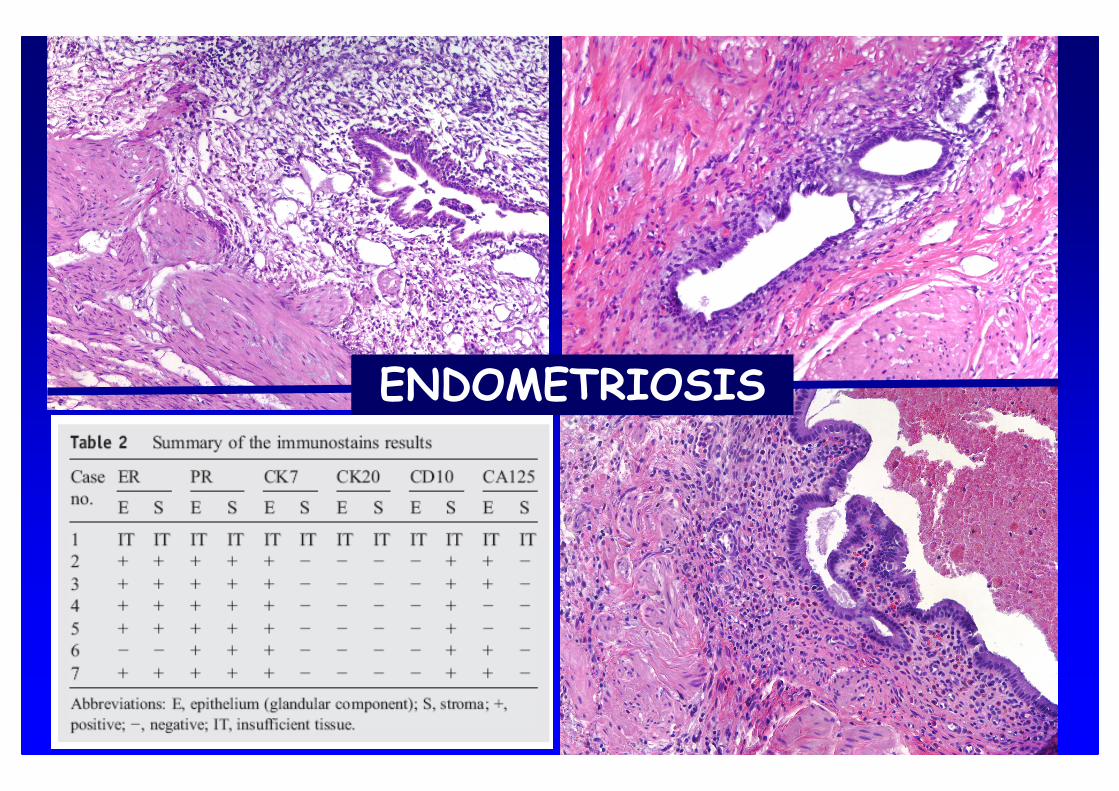
ENDOMETRIOSIS

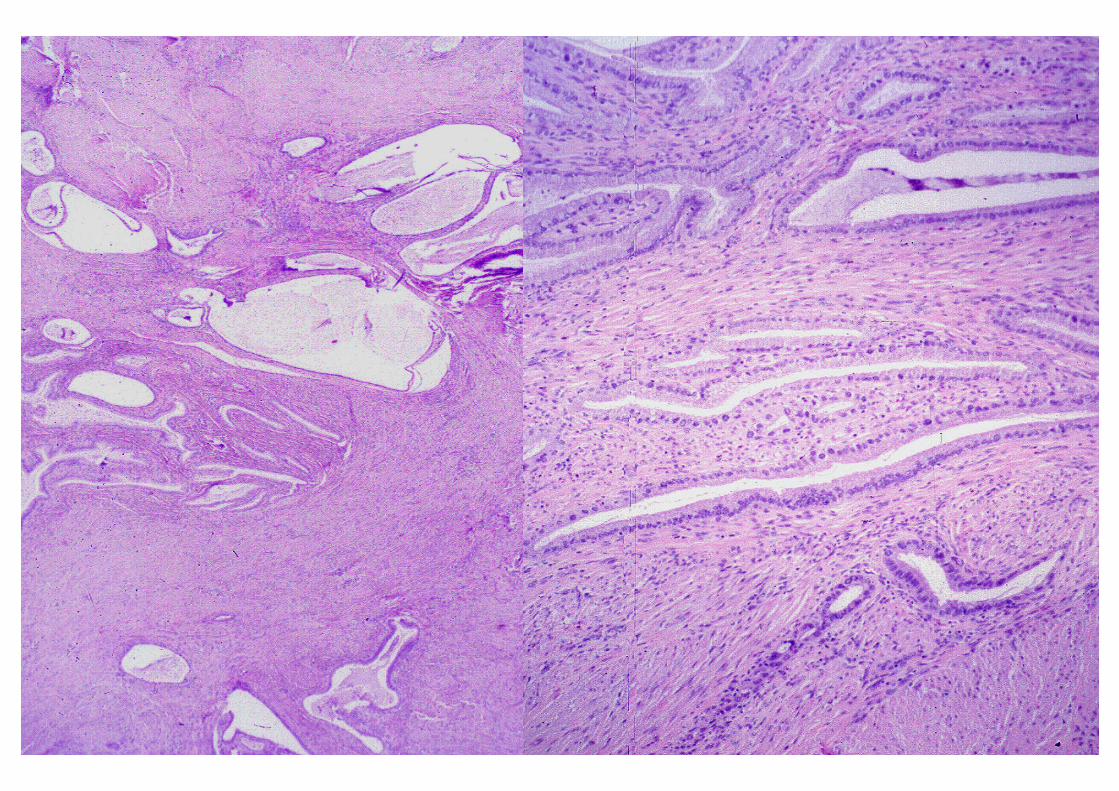
Endocervicosis Endocervicosis ofof the Urinary Bladderthe Urinary BladderClement PB, Young RH. Am J Surg Pathol 1992
• Women of reproductive age
• Common bladder symptoms including dysuria, frequency, hematuria, and pain
• Typically located in posterior wall or dome and forming a mass
• Involvement of muscularis propria by irregularly disposed benign endocervical glands
• 3/6 initially diagnosed as adenocarcinoma
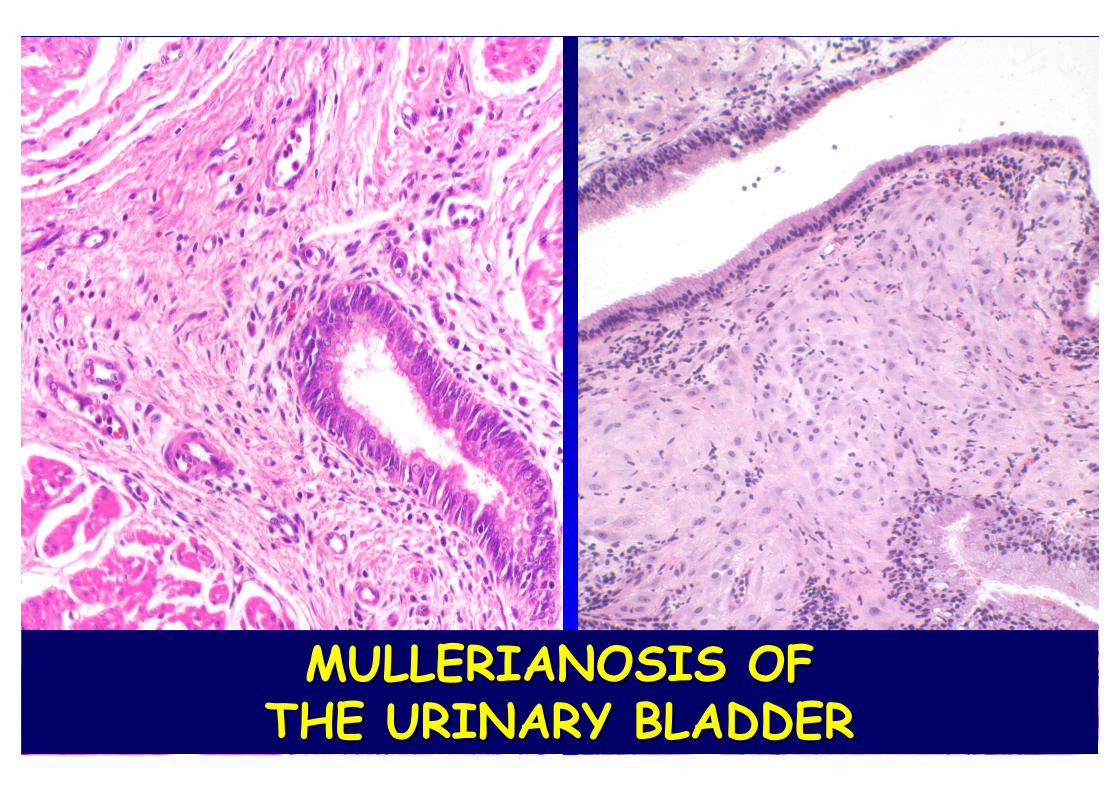
MULLERIANOSIS OF MULLERIANOSIS OF THE URINARY BLADDERTHE URINARY BLADDER
ENDOCERVICOSIS ENDOCERVICOSIS OFOF THE THE URINARY BLADDERURINARY BLADDERDifferential Diagnosis
• Cystitis glandularis, intestinal type
• Urachal remnants
• Primary bladder adenocarcinoma
• Metastatic adenocarcinoma
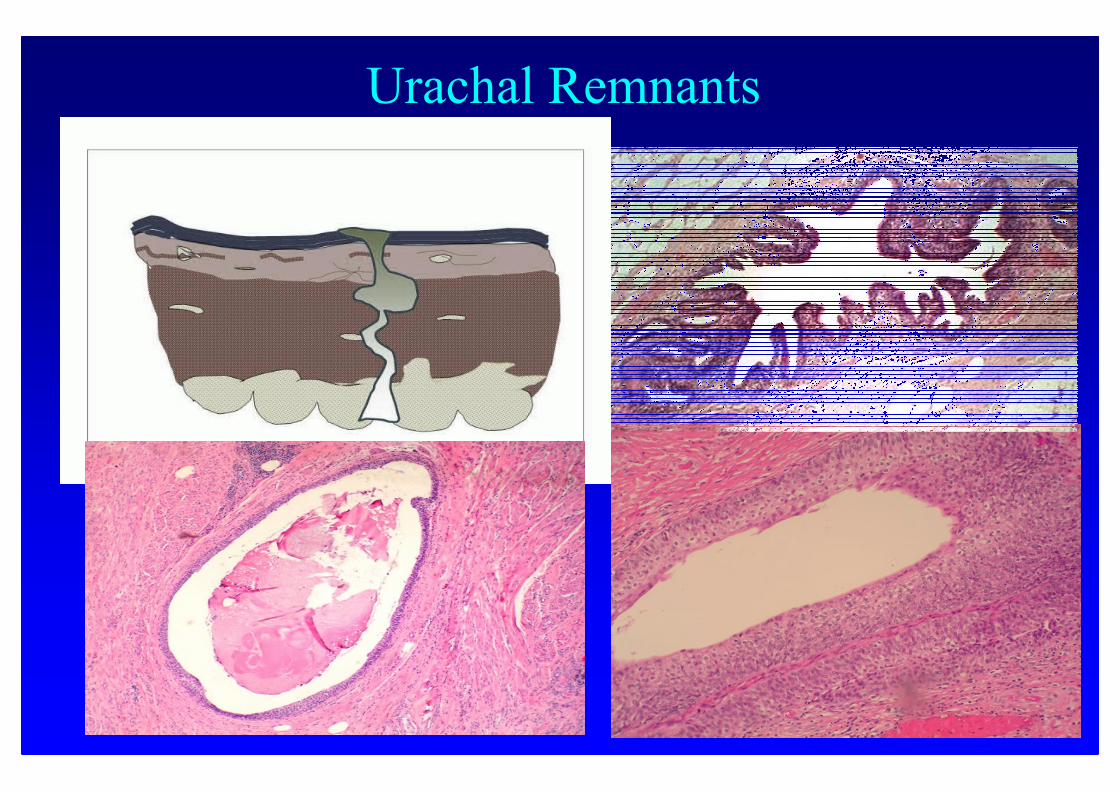
Urachal Remnants
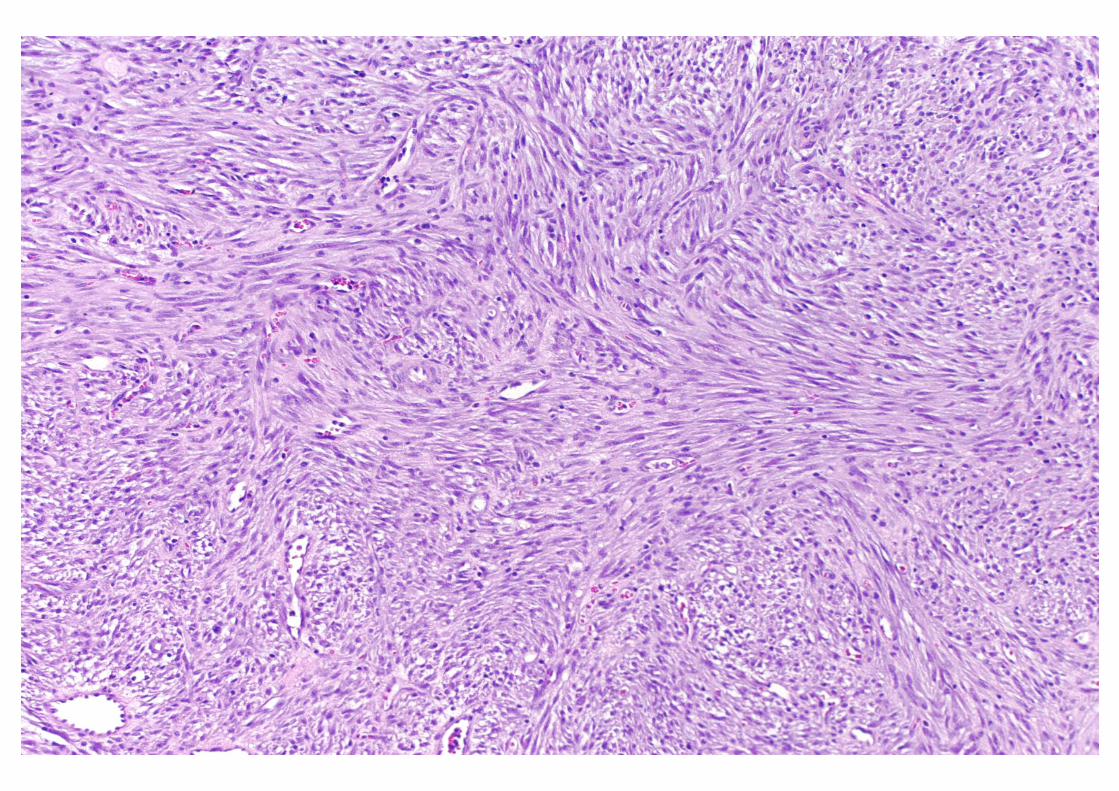
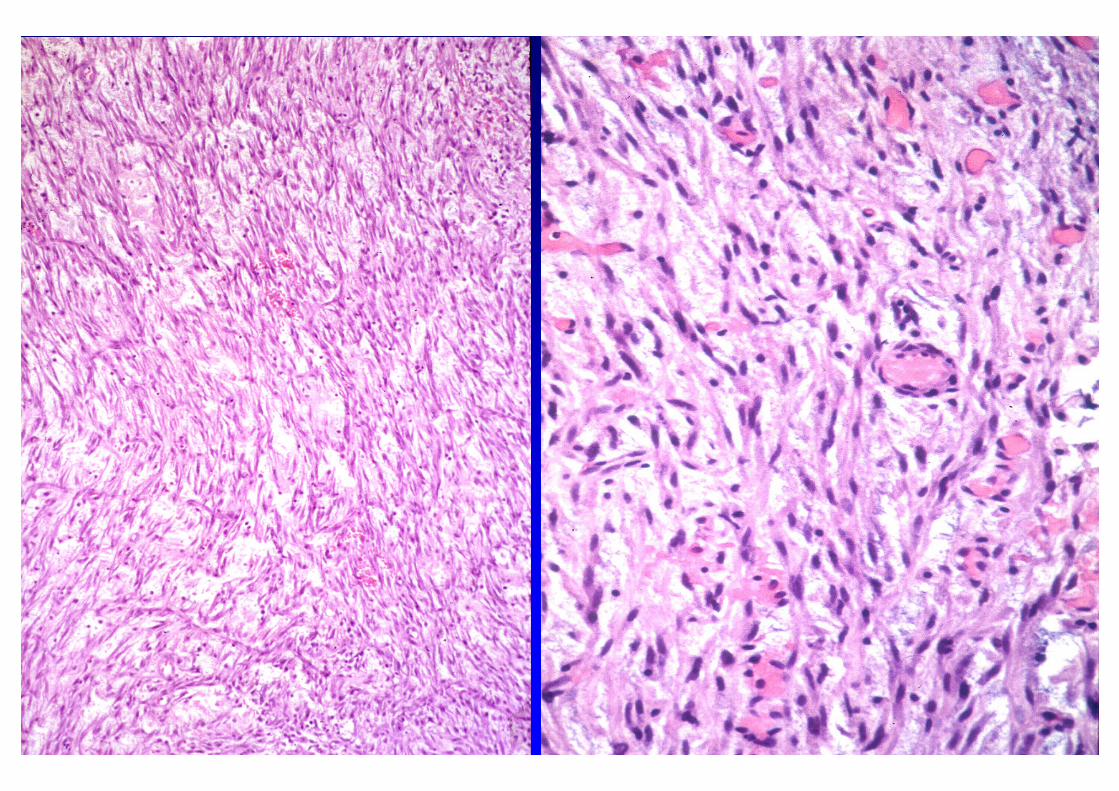
POSTOPERATIVE SPINDLE POSTOPERATIVE SPINDLE CELL NODULECELL NODULE
• First described by Proppe, Scully and Rosai (1984) in the genitourinary tract
• Typically associated with a previous history of surgery
• Clinical symptoms and cystoscopic findings often mimic a malignant neoplasm
• Myofibroblastic derivation• Benign clinical course, conservative treatment advised

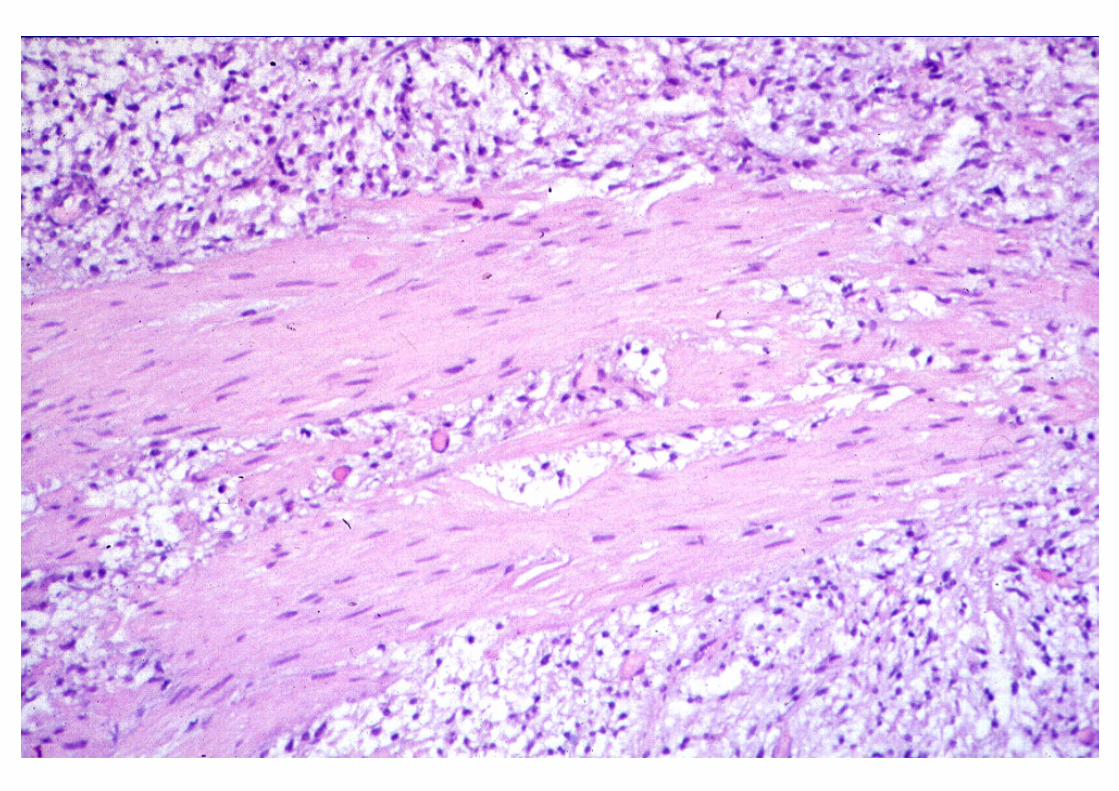
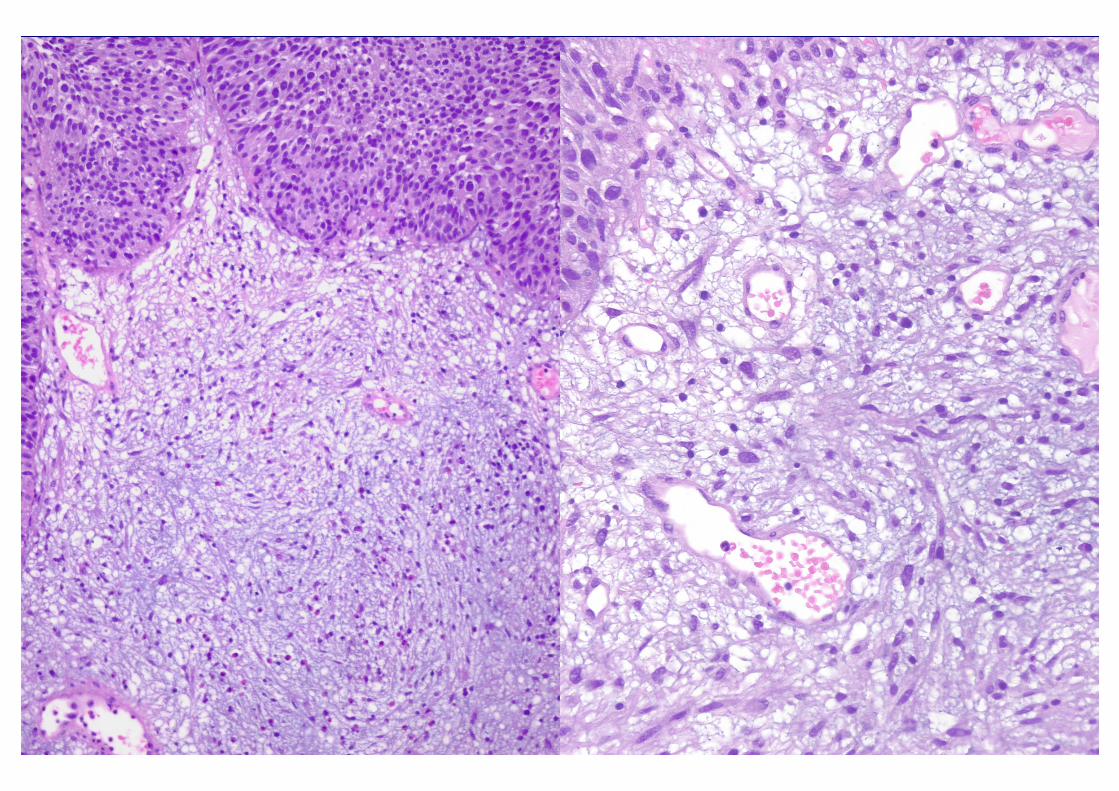
INFLAMMATORY PSEUDOTUMORINFLAMMATORY PSEUDOTUMOR
• M > F: 3-60 (average 40) years• No previous history of surgery• Immunochemistry: Vimentin and cytokeratin + • EM: Myofibroblasts • DNA: Diploid • May recur but typically do not metastasize• Reactive vs neoplastic process (benign) but different from the so-called inflammatory myofibroblastic tumor of childhood

INFLAMMATORY PSEUDOTUMOR INFLAMMATORY PSEUDOTUMOR Worrisome features:
• Large polypoid intraluminal or intramural tumor
• Frequently gelatinous cut-surface
•Myxoid or edematous background with delicate
vasculature
• +/- infiltration into muscular wall/perivesical fat
• Variable cellularity and mitotic activity
• Necrosis deep in the muscularis propria (rare)
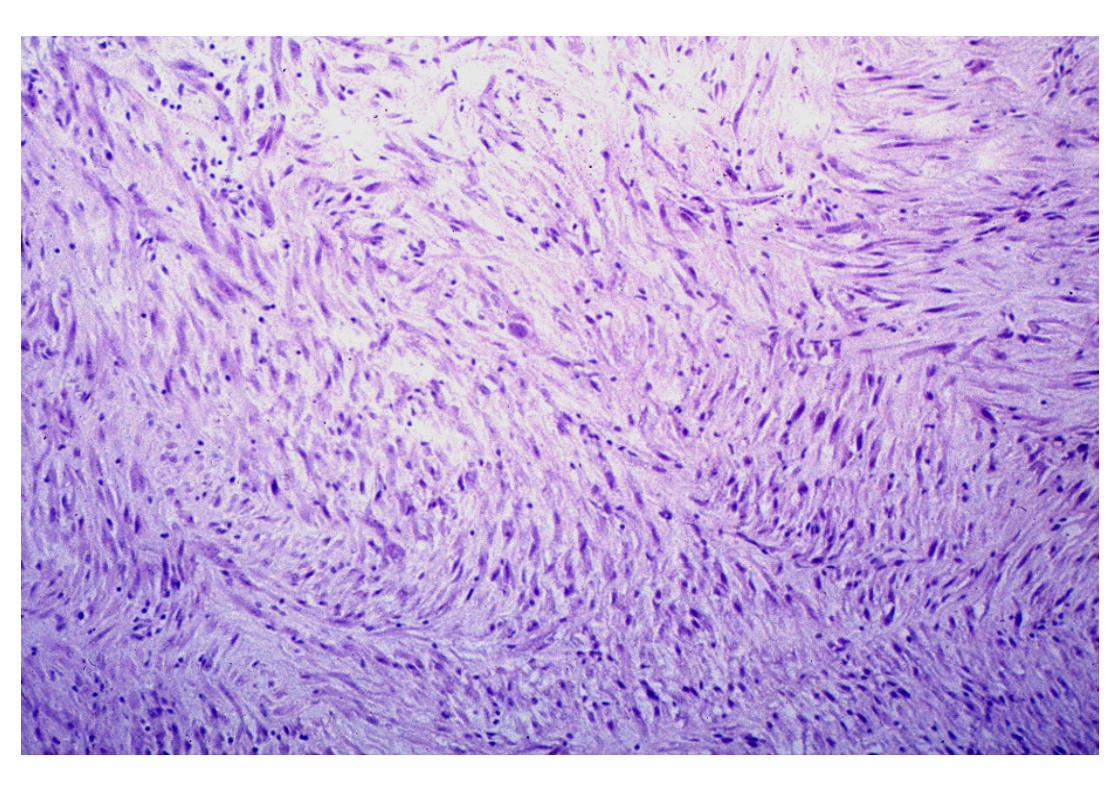
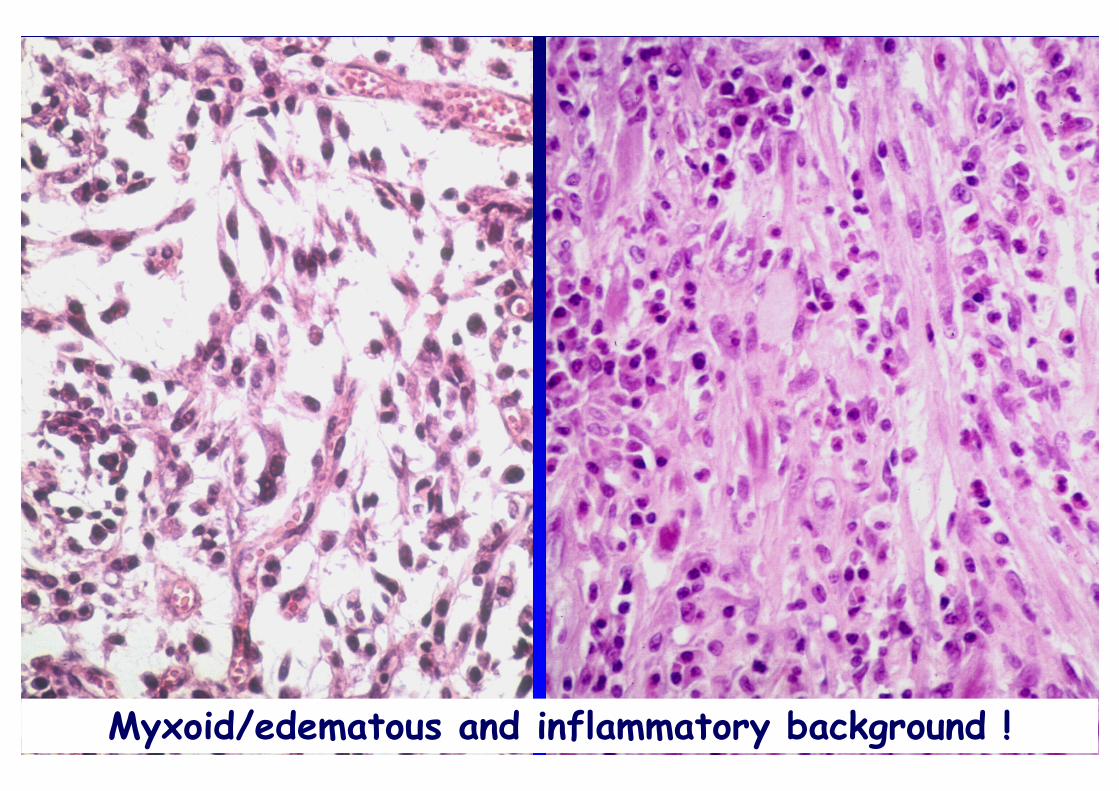
Myxoid/edematous and inflammatory background !
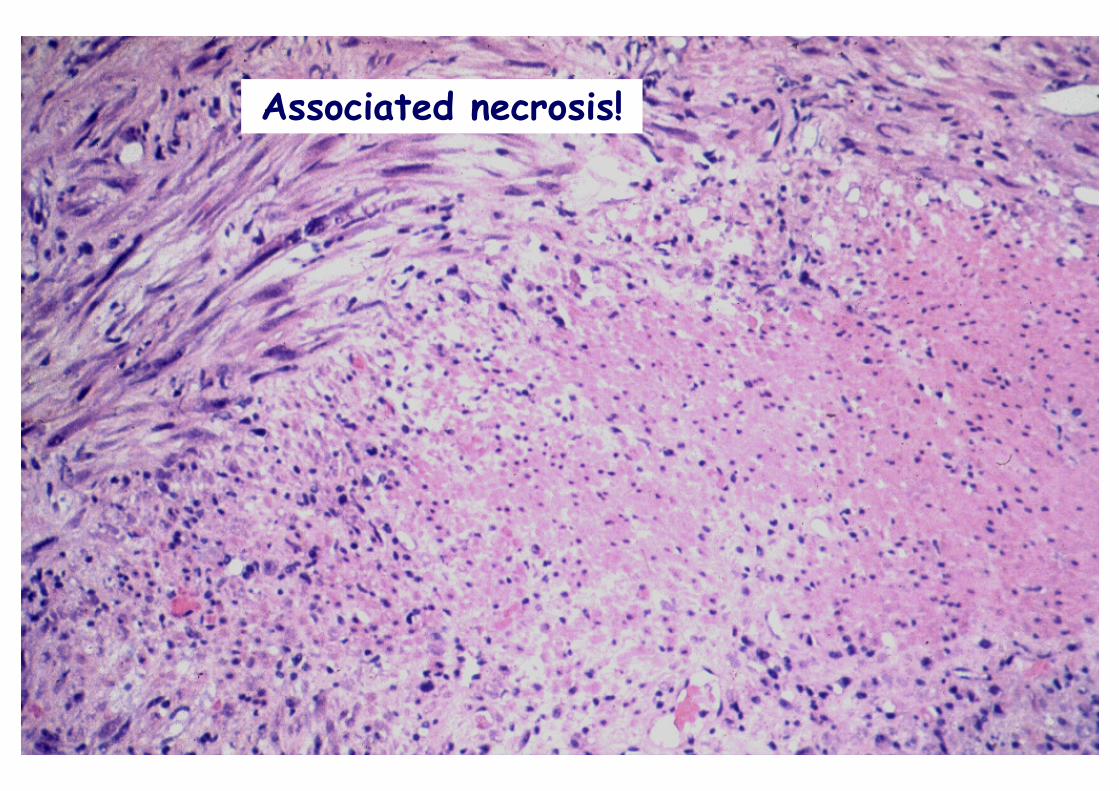
Associated necrosis!
POSTOPERATIVE SPINDLE CELL POSTOPERATIVE SPINDLE CELL NODULE VS INFLAMMATORY NODULE VS INFLAMMATORY
PSEUDOTUMORPSEUDOTUMOR
Only difference:
HISTORY OF INSTRUMENTATION
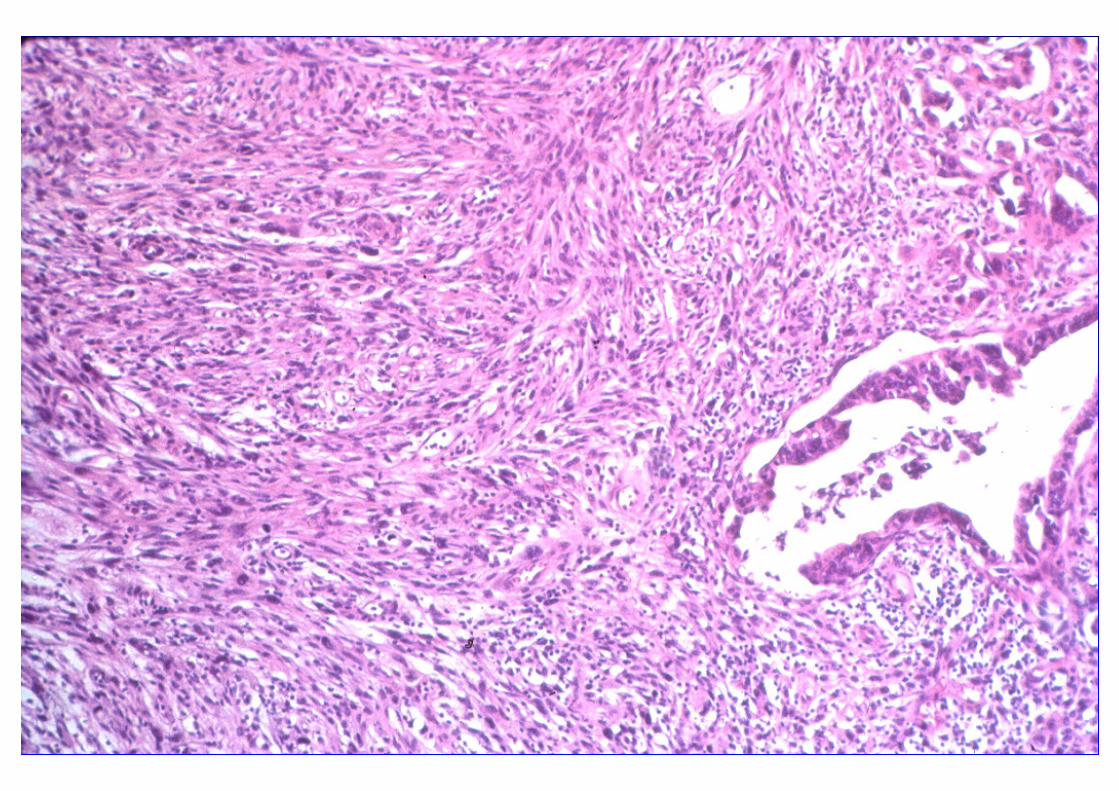
PSEUDOSARCOMATOUS MYOFIBROBLASTIC PROLIFERATIONS
Lara H, Am J Surg Pathol 2006,30:787-794
PSEUDOSARCOMATOUS PSEUDOSARCOMATOUS MYOFIBROBLASTIC PROLIFERATIONSMYOFIBROBLASTIC PROLIFERATIONS
Differential Diagnosis:
• Sarcomatoid carcinoma
• Carcinoma with pseudosarcomatous change
• Leiomyosarcoma
• Kaposis’s sarcoma
• Low-grade myofibroblastic sarcoma

Sarcomatoid Ca Leiomyosarcoma Infl Pseudotumor
SARCOMATOID CARCINOMASARCOMATOID CARCINOMA
• Controversy regarding nomenclature
• WHO definition: Biphasic malignant neoplasm exhibiting morphologic evidence of epithelial and mesenchymal differentiation (+/- heterologous elements)
• Previous history of carcinoma treated by radiation or chemotherapy is common
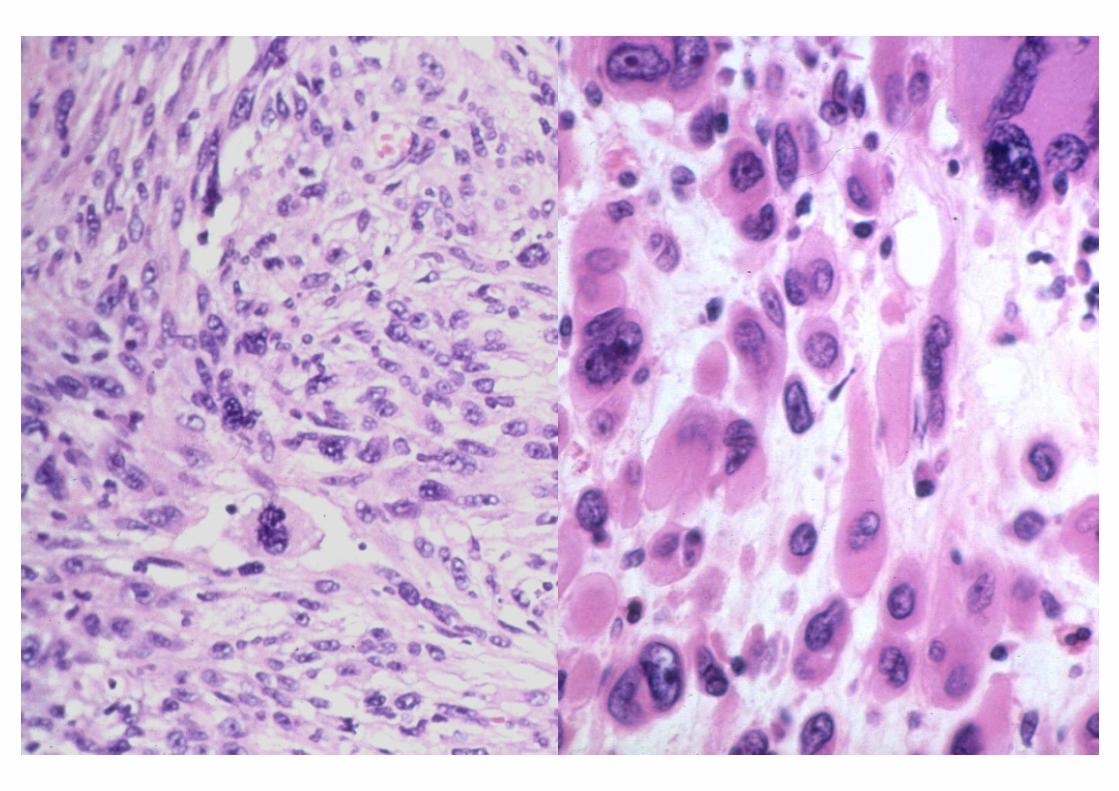
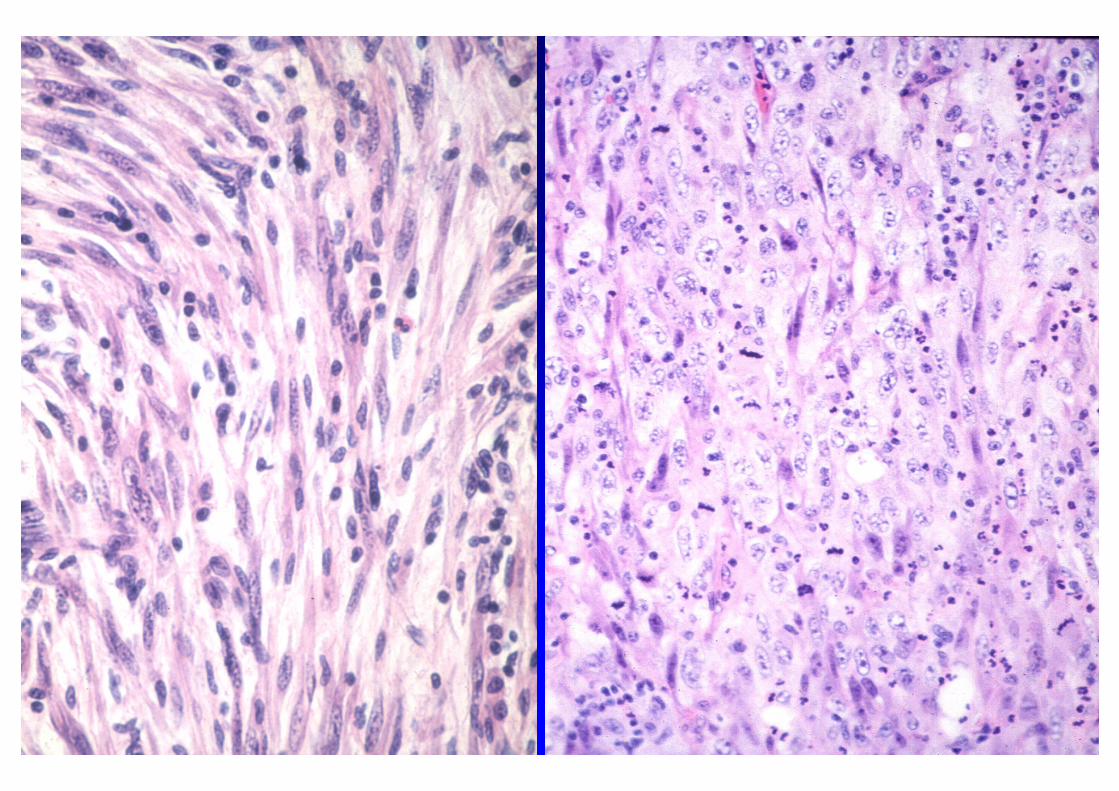
LEIOMYOSARCOMA OF THE LEIOMYOSARCOMA OF THE URINARY BLADDERURINARY BLADDER
• M>F (Average 50 yrs)
• Frequent myxoid degeneration
• Tumor cell necrosis at tumor-bladder wall interface
• No prominent microvasculature
• Only mild acute inflammatory infiltrate
• Frequently brisk mitotic activity
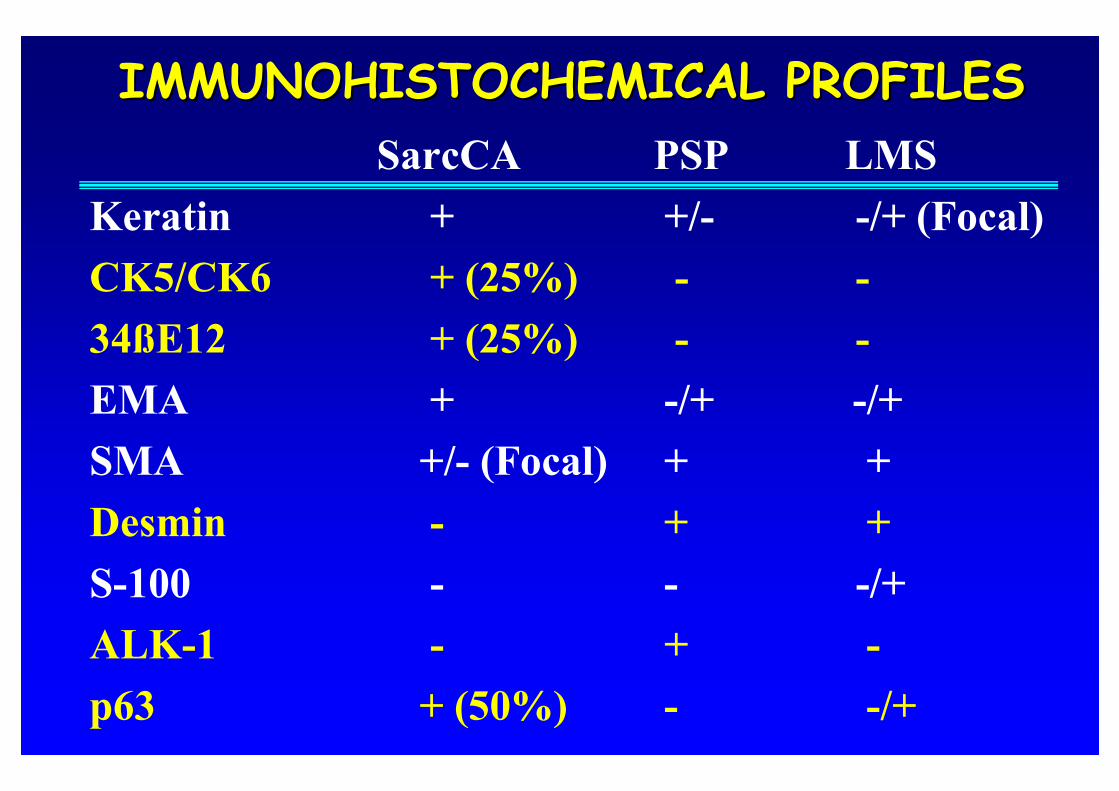
IMMUNOHISTOCHEMICAL PROFILESIMMUNOHISTOCHEMICAL PROFILES
SarcCA PSP LMS
Keratin + +/- -/+ (Focal)
CK5/CK6 + (25%) - -
34ßE12 + (25%) - -
EMA + -/+ -/+
SMA +/- (Focal) + +
Desmin - + +
S-100 - - -/+
ALK-1 - + -
p63 + (50%) - -/+
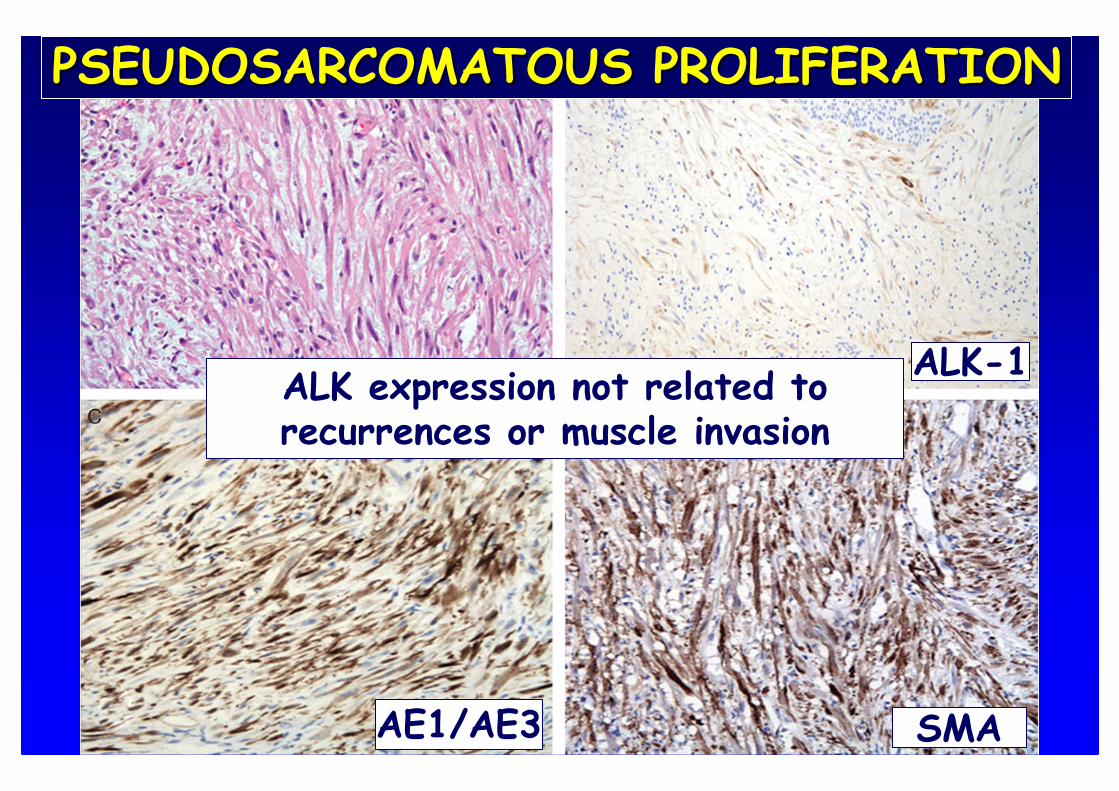
ALK-1
AE1/AE3 SMA
ALK expression not related to recurrences or muscle invasion
PSEUDOSARCOMATOUS PROLIFERATIONPSEUDOSARCOMATOUS PROLIFERATION
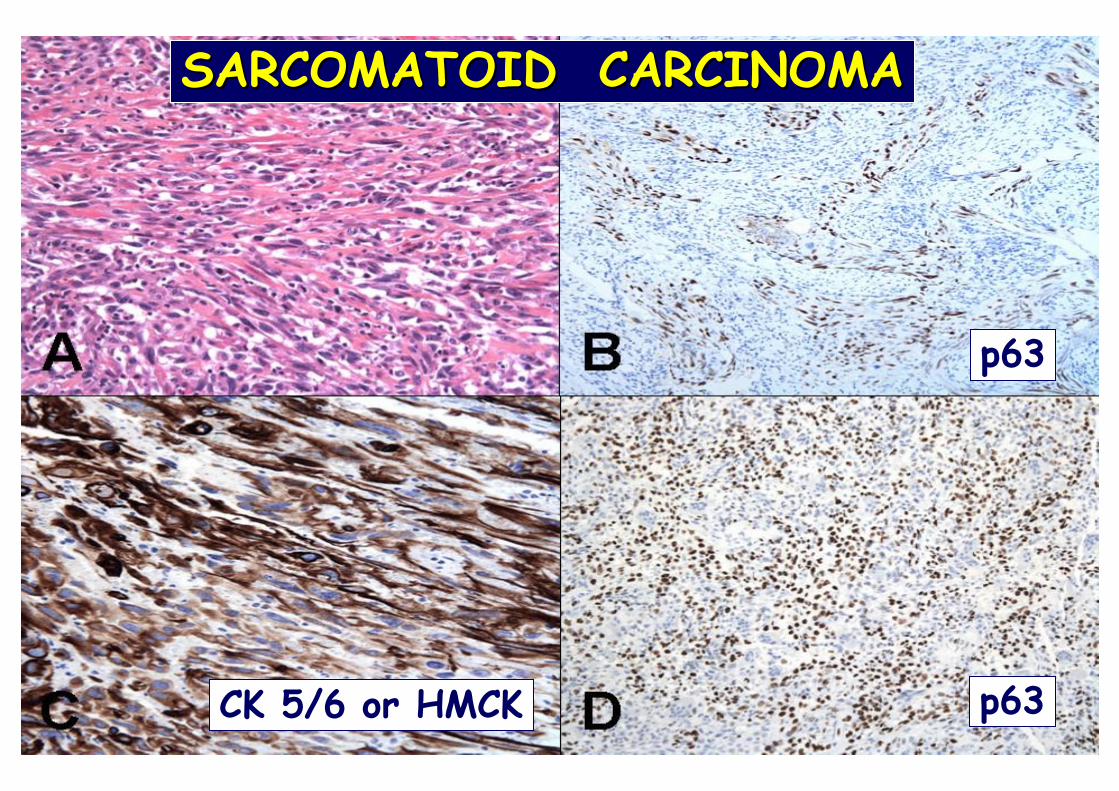
SARCOMATOID CARCINOMASARCOMATOID CARCINOMA
p63
CK 5/6 or HMCK p63
• UNUSUAL BENIGN LESIONS OF THE BLADDER MAY SUGGEST MALIGNACY
• CLINICAL HISTORY MAY BE OF HELP
• IHC MAY BE OF VALUE IN SOME CASES
CONCLUSIONS:

¡¡¡Gracias¡¡¡
Related Documents











