
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
INSIDE THIS REPORT
1. Chairman’s Message
2. Cancer Registry Report
3. Hospital &Specialty Medical Care
– Oncology Division
4. TumorBoardActivitiesReport
5. GI Cancer Care
6. Urologic Oncology
7. Cancer Care 2018 Cancer
Prevention,CancerScreening
Report
8. DiagnosticImagingServices:
ImplementationofFleischer
Society Guidelines at VAPSHCS
9. RadiationOncology-CancerCare
report
10. Surgical Oncology
11. Telemedicine Cancer Program
12. PalliativeOncologySummary
13. CancerCareNavigation
14. SLP and Cancer Care
15. BeyondCancerCare-Whole
Health care
16. CancerRehabilitationCareService
17. OncologySocialWorkAnnual
Care Report 2018
18. Spiritual Care
Chairman’s MessageChairman’s MessageMichaelPorter,MD(CancerCommitteeChair)
I am excited and privileged to begin my service as the Clinical Cancer Committee Chairperson. I am aUrologistwhohasbeenafull-timestaffphysician at the VA Puget Sound since 2005. I have served as the Chief ofUrologysince2014,andtheAssociateChiefofSurgerysince2015.Myclinicalfocusisonthesurgicalmanagementofgenitourinary cancers, with a specialinterest in bladder cancer. I have served as a physicianmemberof theClinicalCancerCommitteesince2011.I assumed the role of Chairperson inJuly 2018, taking over for Dr. DanielWu,whoservedfrom2017-2018andremains a valuable member of theCancer Committee. I hope everyonecan join me in thanking Dr. Wu forhis service to our community ofcancerprovidersandpatients,andforseeingtheCancerCommitteethroughanothersuccessfulaccreditationcycle.
On that note, it has been an excitingyear. The VA Puget Sound received a glowing report and full 3-yearaccreditation with 5 commendationsafter a site visit from theCommissionon Cancer in June 2018. It is evidence oftheexcellentcarethattheVAPugetSound provides to our Veterans with adiagnosisof cancer, and reflects thehard-work and dedication it takes byour community of cancer providersto meet the rigorous standards set by theCommissiononCancer.Dr.Wuand Sudarshana Das, Cancer Programmanager, deserve special recognitionandthanks for theireffortsduringtheaccreditation process. The year aheadproves to be exciting as well, as wecontinue to improve the world classcancer care we provide Veterans at the VA Puget Sound. Ongoing enrollment in clinical trials, completion of quality
improvement projects, monitoring ofcancerscreeningandpreventionefforts,patient navigation and survivorshipprograms, and efforts to expand ourcollective clinical cancer expertiseto other facilities in the NorthwestNetwork are just a few examples ofareas inwhich the Cancer Committeecontinuestoadvancethismission.
There are challenges ahead. We arecurrently recovering from a cancerdatabasecodingbacklogthatresultedfromacontractedvendorfallingbehindon our timeliness requirements. Wealso face challenges coordinatingthe care we give with community providers who provide cancer care to our Veterans, a growing challenge inan era where community based care ismoreaccessibletoourpatientsthaneverbefore.Iamconfidentthatwewillmeet these challenges, as this is oneofthecorepurposesofmaintaininganaccredited cancer program- to solveproblems that pose threats to the high-qualitycarethatweprovide.
We are one of a small handful ofVA Hospitals in the nation that hasa Commission on Cancer accredited program.Thisaccreditationholdsustothehigheststandards,anddemonstratesour commitment to providing the best care available to the Veterans we serve. Inmy 8 yearsworkingwith theClinicalCancerCommittee,Ihavebeenimpressed by the dedication andtalentoftheindividualswhoprovidecancer care at the VA Puget Sound,and the commitment of hospitalleadership to our program. I lookforward to working with everyonein the year ahead to further ourmission ofmaintaining aworld classmultidisciplinarycancerprogram.

2
Cancer Registry ReportSudarshanaDas,COCCancerProgramManager & Cancer Registry Manager
Chairman’s Message
(Continued on next page)
Recently, the Bureau of Labor Statis-tics announced the establishment ofa special occupation code 29-9021“HealthInformationTechnologistsandMedical Registrars” in the Standard Occupational Classification (SOC) sys-temspecificallyforCancerRegistrars.
So, who are Cancer Registrars, andwhat are Cancer Registries?
According to NCRA1 (National CancerRegistrar Association) “Cancer Regis-trars are data information specialiststhatcaptureacompletehistory,diag-nosis,treatment,andhealthstatusforeverycancerpatientintheU.S.Cancerregistrarsensurethattimely,accurate,and complete data are maintained on all types of cancer diagnosed and/ortreated within a health care institu-tion or within a defined population.The curated data provides essentialinformationtoresearchers,healthcareproviders, and public health officialstobettermonitorandadvancecancertreatments,conductresearch,andim-provecancerpreventionandscreeningprograms.”CertifiedCancerRegistrars(CTRs) must undergo special trainingandachievenationallevelcertificationfromNCRAforthepurpose.
Cancer/ Tumor Registry has beendefined by NCRA as “informationsystem that manage and analyze data on cancer patients and survivors.Cancerregistriescanbeclassifiedintothree general types: hospital regis-triesare thestartingpoint forcancer
surveillance and maintain data on all patients. Cases are reported to thecentral or state cancer registry; central registries that maintain data on all cancer patients within certain geo-graphical areas; and special purpose registriesmaintain data on particulartypeofcancer,suchasbraintumors.”Together,CDC’sNPCR2 and NCI’s SEER3 programscollectcancerdatafor100%oftheUSpopulation.”
CancerRegistrydataareusedforana-lyzingpatterns,effectivenessandqual-ity of care, survival and outcome re-latedstudies,devisingearlydetection/screening cancer programs, and canhelp leadership in making informeddecisions for hospital expansion, re-source allocation and other businesspurposes.
The Department of Veterans Affairs(VA) requireseachVAmedical facilitytomaintainacancerregistrytoidentifyandcollectandreportdataonpatientsdiagnosed and/or treated for canceraccording to current VA Central Cancer Registry’s(VACCR’s)reportablelist.
VA Puget Sound Cancer Registry is staffed by a facility employed cancerprogram manager to oversee the management and operations of thehospitalcancerregistry,whilethebulkoftheregistrytasksarecontractedoutto vendor registry services awarded by Visn-20.
1 NCRA: a not-for-profit association body that represents cancer regis-try professionals, conducts stringent national level certifying exams, and maintains continuing education for its professionals.
2 NPCR: established by The Cancer Registries Amendment Act 1992 (Public Law 102-15) to provide grants to states without central cancer reg-istries, or to enhance existing state population based cancer registries.
3 SEER: a federally funded consortium of population-based cancer regis-tries, established by the National Cancer Act 1971 to collect and pub-lish information on cancer incidence, mortality, survival and trends over time in the US
3
Cancer Registry Report (Continued)
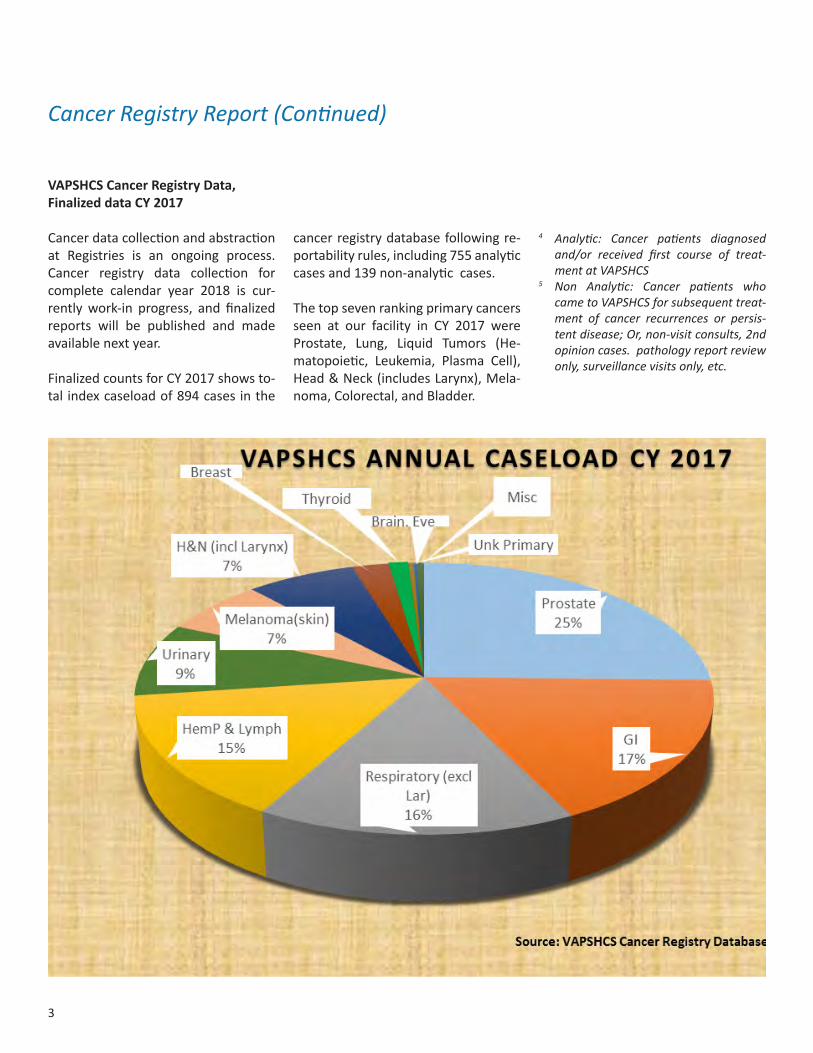
VAPSHCS Cancer Registry Data, Finalized data CY 2017
Cancerdatacollectionandabstractionat Registries is an ongoing process. Cancer registry data collection forcomplete calendar year 2018 is cur-rentlywork-in progress, and finalizedreports will be published and made available next year.
FinalizedcountsforCY2017showsto-tal indexcaseloadof894casesinthe
4 Analytic: Cancer patients diagnosed and/or received first course of treat-ment at VAPSHCS
5 Non Analytic: Cancer patients who came to VAPSHCS for subsequent treat-ment of cancer recurrences or persis-tent disease; Or, non-visit consults, 2nd opinion cases. pathology report review only, surveillance visits only, etc.
cancerregistrydatabasefollowingre-portabilityrules,including755analyticcasesand139non-analyticcases.
Thetopsevenrankingprimarycancersseen at our facility in CY 2017 wereProstate, Lung, Liquid Tumors (He-matopoietic, Leukemia, Plasma Cell),Head&Neck(includesLarynx),Mela-noma,Colorectal,andBladder.

4
(Continued on next page)
Trendanalysisforpastthreeaccessionyearsshowsshift inanalyticcaseloadversus non-analytic annual caseload
References:1.VACentralOfficeCancerProgram,http://www1.va.gov/cancer/2.VHADirectives2003-034NationalCancerStrategy,VHADirective1072
ReleaseofVAdatatoSateCentralRegistries3.NCRA,https://www.ncra-usa.org/4.NationalInstituteofHealth,http://www.nih.gov/5.VHAHandbook1605.02,http://www.va.gov/vhapublications/
ViewPublication.asp?pub_ID=28586.CommissiononCancer,https://www.facs.org/7.AmericanCancerSociety,http://www.cancer.org/8. Previous VAPSHCS Annual Reports 9.CancerRegistryManagementPrinciples&practice,Hutchison,Menck,Etal.
duetoelectionbyveteranstoreceivecareperVeteran’sAccess,ChoiceandAccountabilityActof2014(CHOICEAct).
5
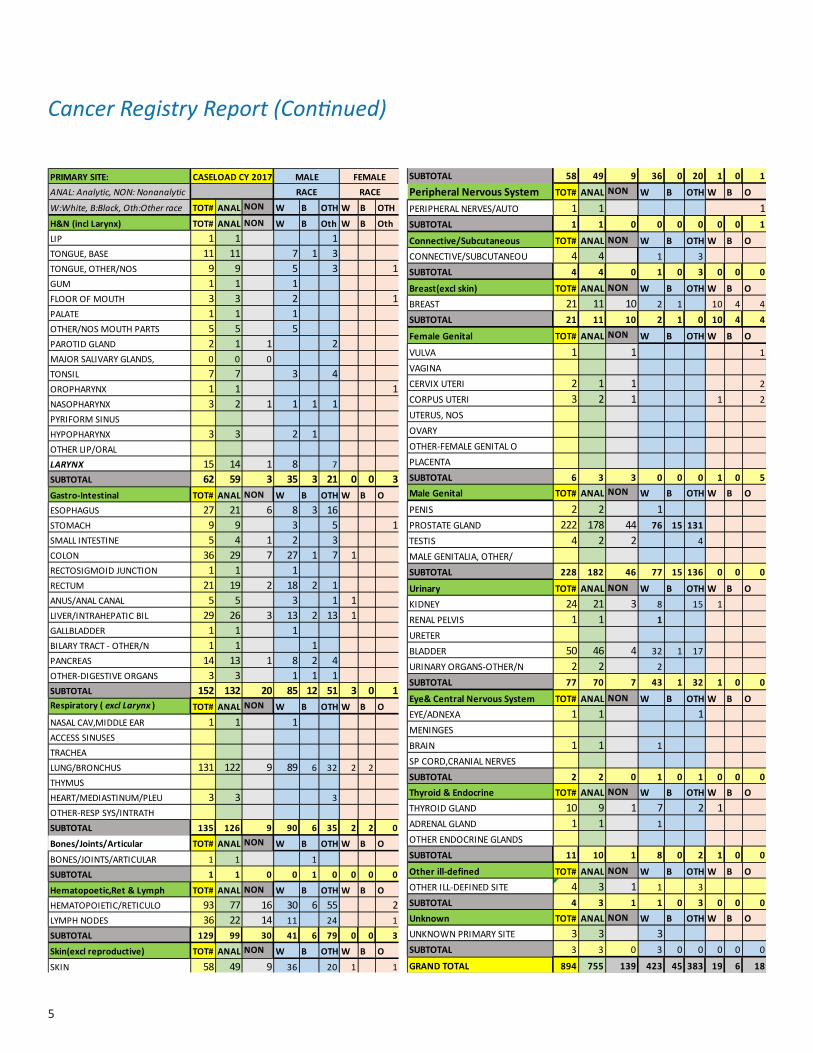
PRIMARY SITE:ANAL: Analytic, NON: Nonanalytic
W:White, B:Black, Oth:Other race TOT# ANAL NON W B OTH W B OTH
H&N (incl Larynx) TOT# ANAL NON W B Oth W B OthLIP 1 1 1TONGUE,BASE 11 11 7 1 3TONGUE,OTHER/NOS 9 9 5 3 1GUM 1 1 1FLOOROFMOUTH 3 3 2 1PALATE 1 1 1OTHER/NOSMOUTHPARTS 5 5 5PAROTID GLAND 2 1 1 2MAJORSALIVARYGLANDS, 0 0 0TONSIL 7 7 3 4OROPHARYNX 1 1 1NASOPHARYNX 3 2 1 1 1 1PYRIFORMSINUSHYPOPHARYNX 3 3 2 1OTHERLIP/ORALLARYNX 15 14 1 8 7SUBTOTAL 62 59 3 35 3 21 0 0 3Gastro-Intestinal TOT# ANAL NON W B OTH W B OESOPHAGUS 27 21 6 8 3 16STOMACH 9 9 3 5 1SMALL INTESTINE 5 4 1 2 3COLON 36 29 7 27 1 7 1RECTOSIGMOID JUNCTION 1 1 1RECTUM 21 19 2 18 2 1ANUS/ANALCANAL 5 5 3 1 1LIVER/INTRAHEPATICBIL 29 26 3 13 2 13 1GALLBLADDER 1 1 1BILARYTRACT-OTHER/N 1 1 1PANCREAS 14 13 1 8 2 4OTHER-DIGESTIVEORGANS 3 3 1 1 1SUBTOTAL 152 132 20 85 12 51 3 0 1Respiratory ( excl Larynx ) TOT# ANAL NON W B OTH W B O
NASALCAV,MIDDLEEAR 1 1 1ACCESS SINUSESTRACHEALUNG/BRONCHUS 131 122 9 89 6 32 2 2THYMUSHEART/MEDIASTINUM/PLEU 3 3 3OTHER-RESPSYS/INTRATHSUBTOTAL 135 126 9 90 6 35 2 2 0
Bones/Joints/Articular TOT# ANAL NON W B OTH W B O
BONES/JOINTS/ARTICULAR 1 1 1SUBTOTAL 1 1 0 0 1 0 0 0 0
Hematopoetic,Ret & Lymph TOT# ANAL NON W B OTH W B OHEMATOPOIETIC/RETICULO 93 77 16 30 6 55 2LYMPHNODES 36 22 14 11 24 1SUBTOTAL 129 99 30 41 6 79 0 0 3
Skin(excl reproductive) TOT# ANAL NON W B OTH W B O
SKIN 58 49 9 36 20 1 1SUBTOTAL 58 49 9 36 0 20 1 0 1
Peripheral Nervous System TOT# ANAL NON W B OTH W B O
PERIPHERALNERVES/AUTO 1 1 1SUBTOTAL 1 1 0 0 0 0 0 0 1
Connective/Subcutaneous TOT# ANAL NON W B OTH W B OCONNECTIVE/SUBCUTANEOU 4 4 1 3SUBTOTAL 4 4 0 1 0 3 0 0 0
Breast(excl skin) TOT# ANAL NON W B OTH W B OBREAST 21 11 10 2 1 10 4 4SUBTOTAL 21 11 10 2 1 0 10 4 4
Female Genital TOT# ANAL NON W B OTH W B O
VULVA 1 1 1VAGINACERVIXUTERI 2 1 1 2CORPUS UTERI 3 2 1 1 2UTERUS,NOSOVARYOTHER-FEMALEGENITALOPLACENTASUBTOTAL 6 3 3 0 0 0 1 0 5Male Genital TOT# ANAL NON W B OTH W B O
PENIS 2 2 1PROSTATE GLAND 222 178 44 76 15 131TESTIS 4 2 2 4MALEGENITALIA,OTHER/SUBTOTAL 228 182 46 77 15 136 0 0 0
Urinary TOT# ANAL NON W B OTH W B OKIDNEY 24 21 3 8 15 1RENAL PELVIS 1 1 1URETERBLADDER 50 46 4 32 1 17URINARYORGANS-OTHER/N 2 2 2SUBTOTAL 77 70 7 43 1 32 1 0 0
Eye& Central Nervous System TOT# ANAL NON W B OTH W B OEYE/ADNEXA 1 1 1MENINGESBRAIN 1 1 1SPCORD,CRANIALNERVESSUBTOTAL 2 2 0 1 0 1 0 0 0Thyroid & Endocrine TOT# ANAL NON W B OTH W B OTHYROIDGLAND 10 9 1 7 2 1ADRENAL GLAND 1 1 1OTHER ENDOCRINE GLANDSSUBTOTAL 11 10 1 8 0 2 1 0 0
Other ill-defined TOT# ANAL NON W B OTH W B OOTHERILL-DEFINEDSITE 4 3 1 1 3SUBTOTAL 4 3 1 1 0 3 0 0 0Unknown TOT# ANAL NON W B OTH W B OUNKNOWNPRIMARYSITE 3 3 3SUBTOTAL 3 3 0 3 0 0 0 0 0
GRAND TOTAL 894 755 139 423 45 383 19 6 18
CASELOAD CY 2017 MALE FEMALERACE RACE
PRIMARY SITE:ANAL: Analytic, NON: Nonanalytic
W:White, B:Black, Oth:Other race TOT# ANAL NON W B OTH W B OTH
H&N (incl Larynx) TOT# ANAL NON W B Oth W B OthLIP 1 1 1TONGUE,BASE 11 11 7 1 3TONGUE,OTHER/NOS 9 9 5 3 1GUM 1 1 1FLOOROFMOUTH 3 3 2 1PALATE 1 1 1OTHER/NOSMOUTHPARTS 5 5 5PAROTID GLAND 2 1 1 2MAJORSALIVARYGLANDS, 0 0 0TONSIL 7 7 3 4OROPHARYNX 1 1 1NASOPHARYNX 3 2 1 1 1 1PYRIFORMSINUSHYPOPHARYNX 3 3 2 1OTHERLIP/ORALLARYNX 15 14 1 8 7SUBTOTAL 62 59 3 35 3 21 0 0 3Gastro-Intestinal TOT# ANAL NON W B OTH W B OESOPHAGUS 27 21 6 8 3 16STOMACH 9 9 3 5 1SMALL INTESTINE 5 4 1 2 3COLON 36 29 7 27 1 7 1RECTOSIGMOID JUNCTION 1 1 1RECTUM 21 19 2 18 2 1ANUS/ANALCANAL 5 5 3 1 1LIVER/INTRAHEPATICBIL 29 26 3 13 2 13 1GALLBLADDER 1 1 1BILARYTRACT-OTHER/N 1 1 1PANCREAS 14 13 1 8 2 4OTHER-DIGESTIVEORGANS 3 3 1 1 1SUBTOTAL 152 132 20 85 12 51 3 0 1Respiratory ( excl Larynx ) TOT# ANAL NON W B OTH W B O
NASALCAV,MIDDLEEAR 1 1 1ACCESS SINUSESTRACHEALUNG/BRONCHUS 131 122 9 89 6 32 2 2THYMUSHEART/MEDIASTINUM/PLEU 3 3 3OTHER-RESPSYS/INTRATHSUBTOTAL 135 126 9 90 6 35 2 2 0
Bones/Joints/Articular TOT# ANAL NON W B OTH W B O
BONES/JOINTS/ARTICULAR 1 1 1SUBTOTAL 1 1 0 0 1 0 0 0 0
Hematopoetic,Ret & Lymph TOT# ANAL NON W B OTH W B OHEMATOPOIETIC/RETICULO 93 77 16 30 6 55 2LYMPHNODES 36 22 14 11 24 1SUBTOTAL 129 99 30 41 6 79 0 0 3
Skin(excl reproductive) TOT# ANAL NON W B OTH W B O
SKIN 58 49 9 36 20 1 1SUBTOTAL 58 49 9 36 0 20 1 0 1
Peripheral Nervous System TOT# ANAL NON W B OTH W B O
PERIPHERALNERVES/AUTO 1 1 1SUBTOTAL 1 1 0 0 0 0 0 0 1
Connective/Subcutaneous TOT# ANAL NON W B OTH W B OCONNECTIVE/SUBCUTANEOU 4 4 1 3SUBTOTAL 4 4 0 1 0 3 0 0 0
Breast(excl skin) TOT# ANAL NON W B OTH W B OBREAST 21 11 10 2 1 10 4 4SUBTOTAL 21 11 10 2 1 0 10 4 4
Female Genital TOT# ANAL NON W B OTH W B O
VULVA 1 1 1VAGINACERVIXUTERI 2 1 1 2CORPUS UTERI 3 2 1 1 2UTERUS,NOSOVARYOTHER-FEMALEGENITALOPLACENTASUBTOTAL 6 3 3 0 0 0 1 0 5Male Genital TOT# ANAL NON W B OTH W B O
PENIS 2 2 1PROSTATE GLAND 222 178 44 76 15 131TESTIS 4 2 2 4MALEGENITALIA,OTHER/SUBTOTAL 228 182 46 77 15 136 0 0 0
Urinary TOT# ANAL NON W B OTH W B OKIDNEY 24 21 3 8 15 1RENAL PELVIS 1 1 1URETERBLADDER 50 46 4 32 1 17URINARYORGANS-OTHER/N 2 2 2SUBTOTAL 77 70 7 43 1 32 1 0 0
Eye& Central Nervous System TOT# ANAL NON W B OTH W B OEYE/ADNEXA 1 1 1MENINGESBRAIN 1 1 1SPCORD,CRANIALNERVESSUBTOTAL 2 2 0 1 0 1 0 0 0Thyroid & Endocrine TOT# ANAL NON W B OTH W B OTHYROIDGLAND 10 9 1 7 2 1ADRENAL GLAND 1 1 1OTHER ENDOCRINE GLANDSSUBTOTAL 11 10 1 8 0 2 1 0 0
Other ill-defined TOT# ANAL NON W B OTH W B OOTHERILL-DEFINEDSITE 4 3 1 1 3SUBTOTAL 4 3 1 1 0 3 0 0 0Unknown TOT# ANAL NON W B OTH W B OUNKNOWNPRIMARYSITE 3 3 3SUBTOTAL 3 3 0 3 0 0 0 0 0
GRAND TOTAL 894 755 139 423 45 383 19 6 18
CASELOAD CY 2017 MALE FEMALERACE RACE
Cancer Registry Report (Continued)

6
The VA Puget Sound Oncology Divi-sionprovides initialmedicaldiagnosis,medicaltreatment,andfollow-upcarefor Veterans diagnosed with cancer.ThedivisionworkscloselywithsurgicalsubspecialtiesandRadiationOncologytooffermultidisciplinarycare;andwithsocialwork,nursing,dietary,chaplain-cy,andotheralliedhealthcareservicestoprovideholisticcare.Careandtreat-ment for cancerpatients is frequentlycoordinatedthroughamultidisciplinaryTumorBoard. In this forum, individualcases and therapeutic options are re-viewed by representatives from allservices and a consensus recommen-dationisrendered.Oncologynurseco-ordinators fromtheOncologyDivisionensurefollow-up,coordinatesdiagnos-ticand therapeuticrecommendations,andmaintainscontactwiththepatient.Inaddition,awell-staffedCancerCareClinic provides ongoing chemothera-peutic,transfusion,andsupportiveser-vicesforpatientsundergoingtreatment.
The Oncology Division provides care in bothinpatientandoutpatientsettings.Patientsareevaluatedandfollowedatfour weekly subspecialty outpatientclinics staffedbyattendingphysicianswho are also faculties of the Univer-sity of Washington and fellow physi-ciansfromtheFredHutchinsonCancerCenter. Chemotherapy and treatment related care is provided in the newly remodeled Cancer Care Clinic that op-eratesfivedaysperweekandstaffedbytwophysicianassistants,twonursepractitioners, three to four RNs, andone clerk. This unit provides all ofthe outpatient chemotherapy for VAPuget Sound Health Care System pa-tientsandalsooffersaconvenientlo-
cationforoutpatientprocedures,suchas bone marrow aspirates and physi-calexaminations,outsideoftheregularoutpatientclinichours.Afull-timeclini-cal pharmacist manages chemotherapy forbothinpatientsandoutpatients,andensuressafetyofdrugadministration.
Recently,theDivisionhasaddedafourmembercancernavigationteamtosup-portpatientswhomusttravelgreatdis-tances or are challenged with difficultpersonal issues. This navigation team,consistsofanursepractitioner,anursecoordinator,asocialworkerandaclerk,maintainscontactwiththepatientandprovidesthroughouthis/hercancercarejourney. Thenavigation teamalsoen-suresseamlesstransitionofthepatientbacktothereferralfacilityandprovider.Additionally, the teamwillprovide sur-vivorship counseling to patients, whohave completed treatment.
The Marrow Transplant Service re-mains a marquee program of the VAPuget Sound Oncology Division. The MarrowTransplantUnit (MTU) isoneofonlythreesuchunitsnationwideun-derthenationalVAprogram.TheMTUperforms approximately 50-60 trans-plants per year on patients referredfrom both remote and regional sites.TheMTUworks inclosecollaborationwith the Fred Hutchinson Cancer Re-searchCenter,andthetreatmentandexperimental protocols for transplan-tation are shared between the twoinstitutions.Aftertheacutetransplantphase, the MTU performs outpatientfollow-up on transplanted patients aswell as annual long-term follow-up.TheMTUisadiscretephysicalpatientcare unit with integrated outpatient
and inpatient care, and a dedicatednursingandclericalsupportstaff.Theunitoperatesfull-timeandmanagestransplantpatients24/7.
Asalways,theOncologyDivisionsup-ports the overall direction of the VAPuget Sound Cancer Committee, amultidisciplinarycommitteethatmain-tainsaccreditationsandpromotescan-cercareactivitiesoftheinstitution.AsapartofthemissiontoprovideVeter-answithcuttingedgecancercare,theOncologyDivision also activelymain-tainsaclinicalresearchprogram.Weprovide clinical trial participation op-portunities so that patients can haveaccess to novel drugs and advanced oncological concepts. Our clinical re-searchprogramparticipatesinanum-berofstudiesthroughnationalcoop-erativeprogramsandpharmaceuticalsponsors; and is staffed with threeclinical research coordinators. The On-cologyDivisionadditionallymaintainsalocalcancerregistryunderacertifiedCancer Registrar; and undergoes regu-lar clinical and system improvement evaluations under a full-timequalityimprovement coordinator.
The Oncology Division is a central partoftheVACancerProgram,whichhas received continuous distinctionas a comprehensive cancer center designated by the Commission on Cancer. The marrow transplant unit hasbeenawardedmultipleachieve-mentsandcertificatesofexcellenceby the National Marrow Donors’Program.TheentireOncology teamstrives daily to provide superior care to our Veterans whom have served this country with honor.
Hospital & Specialty Medical Care-OncologyDivisionDanielWu,MD,PhD

7
TumorBoardActivitiesfor2018VictoriaCampa(Compileddataisfrom1/3/18through12/5/18)
The VA Puget Sound Health Care System Tumor Board is held every Wednesday from 1:00 p.m. to 2:00p.m. in Building 100, Room BD-152.Tumor Boards provide clinical infor-mation,pathologicstaging,andtreat-ment recommendations for the pa-tient'sdisease.
TheTumorBoardiscomposedofamul-tidisciplinarygroupofattendingphysi-cians,fellows,residents,physicianas-sistants,nurses,medicalstudents,andother health care professionals. Staffrepresentatives from Medical, Surgi-cal,andRadiationOncologyactasdis-cussants.Allsurgicalsubspecialtiesarerepresented. Images and micrographs
arepresentedbystaffphysiciansfromDiagnostic Radiology and Pathology.The conference provides a forum todisseminate the most current infor-mation on cancer management. Thediscussants review data from currentpublications and determine eligibilityofpatientsforcooperativegrouptrialssponsored by the Southwest Oncol-ogyGroup(SWOG)aswellasin-houseclinicaltrials.Theconferencesprovidecontinuingmedicaleducationandpro-vide a convenient forum for expedi-tiousmanagement decisions of com-plexpatients.
In 2018, there were 47 conferencesfor the year. All the major cancer
sites were represented in the cases discussed.Theaverageattendanceateach conference was 22. Attendeescanreceiveonecredithourcontinuingmedical education category 1 persession, which can be appliedtoward re-licensure requirements inWashingtonState.
AllrequestsforTumorBoardsubmis-sion shall be ordered online in CPRS ontheordertab.Therequestingser-vice must complete the consult tem-plate and include a reason for therequest. All consult requests will becoordinatedthroughVictoriaCampa,Tumor Board Coordinator, OncologySection(6-4757).
HEADandNECK[90],[26.3%]
MUSCULOSKELETAL (6),1.8%
SKIN(6),1.8%BREAST(1),0.3%
GENITOURINARY(23),6.7%
OPHTHALMIC(2),0.6%
LYMPHOIDNEOPLASM(3),0.9%
CENTRAL NERVOUS SYSTEM(5),1.5%
NON-CANCEROUS(0),0.0%
OTHER(0),0.0%
UNKNOWN(20),5.8%
DIGESTIVE(63),18.4%
THORAX(123),[36.0%]
Tumor Board Annual Report- 01/3 thru 12/5, 2018Tumor Board 2018 - Distribution of 342 Total Cases (1/3/18 – 12/5/18)
HEAD&NECK 90 26.3%MUSCULOSKELETAL 6 1.8%SKIN 6 1.8%BREAST 1 0.3%GENITOURINARY 23 6.7%OPHTHALMIC 2 0.6%LYMPHOIDNEOPLASMS 3 0.9%CENTRALNERVOUSSYSTEM 5 1.5%NON-CANCEROUS 0 0.0%OTHER 0 0.0%UNKNOWN 20 5.8%DIGESTIVE 63 18.4%THORAX 123 36.0%

8
Cancers of the digestive system con-stituteasignificantportionofthecan-cers diagnosed and treated at the VA PugetSoundHealthCareSystem(VAP-SHCS).Increasedawarenessandcom-pliance with colorectal cancer screen-ing, aswell as the rising incidenceofhepatocellularcarcinoma,esophagealandpancreaticadenocarcinoma,haveresultedinever-increasingnumbersofproceduresperformedforthescreen-ing,surveillance,diagnosis,andtreat-mentofthesecancersatourfacility.
Procedures offered at the VAPSHCSinclude liver biopsy, esophagogastro-duodenoscopy (EGD), sigmoidoscopy,colonoscopy, capsule endoscopy, andendoscopic retrograde cholangio-pancreatography (ERCP). Endoscopicultrasound (EUS) is also available toVeterans needing tissue acquisitionforthediagnosisofcancer,aswellasfor cancer staging. Other proceduresinclude endoscopic palliation of ma-lignant obstruction (e.g. esophageal,duodenal, biliary or colonic obstruc-tion),inadditiontopercutaneousen-doscopic gastrostomy for nutritional
support. There are now eleven full-timestaffgastroenterologists/hepatol-ogists,threenursepractitioners,andasuperbteamofnursesonstaffattheSeattleandAmericanLakecampuses.Gastroenterology and Hepatology providersparticipate inweeklymulti-disciplinary conferences for theman-agement ofmalignancies (e.g. TumorBoardandLiverTumorConference).
AllstaffphysiciansattheVAPSHCSholdfaculty positions at the University ofWashingtonandtheGastroenterologyteam also includes fellows, residentsandmedicalstudentsfromtheUniver-sity.MembersofourGastronterologySection are also actively involved inresearch relevant to cancer, includingbasic (e.g. DNA methylation & carci-nogenesis), translational (e.g. screen-ingtools),andclinical(e.g.screening,diagnostic and treatment strategies)research. They also collaborate with theresearchprogramsofmanyotherdepartmentswithintheVAPSHCS,theFredHutchinsonCancerResearchCen-terandtheUniversityofWashington.
Gastroenterology and HepatologyJasonDominitz,MD,MHS,HarithaAvula,MBBS, GeorgeIoannou,MD,MS
9
Urologic Oncology ProgramBruceMontgomery,MDandMichaelPorter,MD
Tobacco:HowtheVA Can Help Veterans QuitMicheleMeconi,ARNP,CDE
The multidisciplinary Urologic Oncol-ogy program is designed to help pa-tientswithgenitourinarycancersofalltypes and give them the opportunity to discuss their therapeutic optionswith a broad range of care providerswho treat patients with this disease,includingurologists, radiationoncolo-gists, medical oncologists endocri-nologists, advanced registered nursepractitioners,specialtytrainednurses,and physical therapists. By providing this type of integrated patient care,doctors hope to help patients makeinformed decisions and receive thebestpossibletreatment.Themultidis-ciplinaryteamofferssomeofthemostadvancedtreatmentoptionsavailablefor prostate cancer, including nervesparingprostatesurgery,brachythera-
py(radiation implants),adjuvantche-motherapy, the latest options in hor-monaltherapy,andadvanceddiseasechemotherapy studies. The center is oneofaselect fewVAcenters in thecountry utilizing the DaVinci roboticsystem to perform prostatectomies.Wealsooffer cuttingedge treatmentoptionsforkidneyandbladdercancer,includingroboticpartialnephrectomy,laparoscopic nephrectomy, energybased ablative techniques for smallrenaltumors,radicalcystectomywithurinary diversion for muscle invasivebladder cancer, and adjuvant thera-pies for non-muscle invasive bladdercancer including chemotherapy placed intothebladder.Finally,weoffercon-tinuing care of urologic cancer survi-vors which includes management of
long termsideeffectsofcancer ther-apyincludingerectiledysfunctionandurinarysymptoms.Weareacancerre-ferralcenterforallofVISN20andalsoprovide comprehensive care for can-cers that are more uncommon in the Veteran population, including testisandpeniscancer.TheProgramactivelyparticipates in cutting edge research,and offers ongoing trials in bladdercancer treatment and active surveil-lanceoflocalizedprostatecancerandprecisiononcologystudiesofgermlineand somatic sequencing paired withrelevant clinical trials for advancedprostatecancer.Forinformation,con-tacttheOncologyDepartmentat(206)764-2709or theUrologyDepartmentat(206)764-2265
Tobacco Use Rates among VeteransVeterans have much higher rates oftobacco use compared to nonveter-ans. Currentuseof tobaccoproductswashigheramongpersonsaged18-25years. A 2017 survey of Veterans en-rolled in VAhealth care found 15.9%of those who responded are currentsmokers.ThatIsanincreasefrom2016(14.9%), but still far lower thanwhatwas seen just 12 years ago in 2005 (22.2%).[i]Thesurveyalsofoundthatcurrent smokers were more likely tobe female (16.9%) thanmale (15.5%)andmorelikelytohaveOEF/OIF/ONDstatus. Because Veterans have higher rates of smoking than nonveterans
and smoking is the leading cause ofpreventabledeath,theimportanceofVA’s tobacco cessation efforts is vitaltotheoverallhealthofmanyVeteransin our care.
Negative Health Effects of Tobacco UseThe U.S. Surgeon General advises that smokingcanharmalmosteveryorganin the body. Using tobacco exposes youtoharmfulchemicalsthatcan:• Increaseyourriskformanytypesof
cancer, including lung, pancreatic,kidney,stomach,bladder,aswellascancersoftheblood,throat,mouth,colon,andrectum.
• Lead to problemswith your teeth,gums,andmouth.
• Decreasetheeffectivenessofmedi-cationsfordepression,anxiety,andpsychoticdisorders.
Ifyousmokecigarettes,youareabout25 timesmore likely to develop lungcancer than a person who doesn'tsmoke,andnineoutof10lungcancerdeathsareduetosmoking. It isesti-mated that more than 1.5 million peo-ple in the United States are living with cancer other than lung cancer that is duetocigarettesmoking.

10
current smokers—andVAhasmoretreatmentoptionsavailablethaneverbefore. Every day, Veterans just likeyoumakeoneof themost importantchoicesthattheycanfortheirhealth.Theydecidetoquitusingtobacco.
Important Benefits of Quitting TobaccoTherearemanyreasonstoquittobac-co.Withinfiveyearsofquittingsmok-ing, your chance of getting cancer ofthe mouth, throat, esophagus, andbladder is cut in half. Ten years afterquittingsmokingyourriskofdyingfromlungcancerdropsbyhalf.Whenaper-son living with cancer quits smoking,they can improve the course of theircancerandtheirchanceofsurvival.
Thebenefitsofquittingtobacco—foryourphysicalandmentalhealth—canbeginalmost immediately.Yourheartrateandbloodpressurewillbothdrop,andwithindaysyouwillnoticeabet-tersenseoftasteandsmell,aswellasbreathing.
Quittingcanalso:• Reduce stress and improve your
mental health.• Help you save money.• Boost the effectiveness of some
anxietyanddepressionmedications.• Make it easier to stop using drugs
and alcohol.• Increase your energy.• Reduceyourriskforcancer.• Lower your blood pressure and cho-
lesterol.• Improve your lung function, skin,
and night vision.• Strengthen your immune system,
muscles,andbones.• Limit the exposure of loved ones
andpetstosecondhandsmoke.
VA Tobacco Cessation EffortsIt is important to note that tobacco use rates among Veterans in VA care have greatly decreased in the past de-cade, and there is stillmuchwork tobedone.Inaddition,theVHAhasde-veloped tobacco cessationpolicy andprograms as well as clinical resources for providers. We believe these re-sources can support efforts to bringthe tobacco use rate down among Vet-erans in our care.
Quittingtobaccoisaprocessthatoftentakes many attempts. With tobaccousedisorderbeingachronicconditionthatoftenrequiresrepeatedinterven-tions,allVAhealthcareprovidersareencouraged to address tobacco use withtheirpatients.Withinthelasttwoyears, close to 60% of VA enrolleeswho smoked cigarettes made a quitattempt,yetwereunsuccessful.Morethananything, this shows thatVeter-answant toquit smoking,and thatahuge percentage of current smokershasbeeninthe“action”stageofquit-tingtobacco,but likelyneedthesup-portofcounselingandmedicationof-feredthroughVA.VAknowsthatwithits supportand resources,alongwithyourdesireandstrength,youcanquitandstayquit.
For VA health care providers, thisrepresents a great opportunity to talk to our patients about theirtobacco use and help them with this behavioral change through counseling, medication, and comingupwithaquitplan.Ifyou’rereadytoquittobacco,yourVAhealthcareteamisreadytoworkwithyoutocreateaquitplanthat’srightforyou.Quittingisn’t easy, but you can do it. Therearemore former smokers today than
• Help you manage chronic health conditions.
Tobacco Cessation Resources
Research shows that a person has thebestchanceofquittingtobaccofor good when they use tobaccocessationmedicationandtakepartintobaccocessationcounseling.Tobaccocontainsnicotine,ahighlyaddictive chemical. Using smokingcessation medications for the firstfew months while you’re quittingcanhelpyoumanagenicotinewith-drawal symptoms and cope with the urgetosmoke.
MedicationsThereareseveraldifferenttypesofmedication,including:• Nicotine Replacement Therapy
(NRT): The nicotine patch, nico-tine gum, and nicotine lozengesgive your body medicinal nico-tine to reduce your withdrawalsymptoms.
• Bupropion (Zyban®): This pillhelpsreduceyoururgetosmoke.It can be combined with a single typeofNRT.
(Continued on next page)
How the VA Can Help Veterans Quit (Continued)

11
• Varenicline (CHANTIX®): This pillblocks the effects of nicotine onyour brain, making smoking lessenjoyable and reducing your with-drawal symptoms. It should not be combinedwith any other smokingcessationmedication.
Counseling Tobaccocessationcounseling iswhenyoutalkwithahealthcareproviderora counselor about your tobacco use andworkonwaystogettobaccooutofyourlife.Thistypeofcounselingcanhelpyoubreakyourtobaccohabitandthedailypatternsyouhavedevelopedover the years.
Counseling is available in person or overthephone.Youcantalkwithyourhealth care provider or a counselor one-on-one, or participate in groupcounseling sessions. An important part ofcounselingisfiguringoutwhattrig-gers your tobacco use; common trig-gersincludedrinkingcoffeeoralcohol,andfeelingbored.Yourcounselorwillhelp you find ways to avoid or copewith your triggers so that you don’t start using tobacco again.
Contact your VA health care provider andletthemknowyouarequittingto-bacco. They can offer you counselingandtherightsmokingcessationmedi-cationforyou.
Learn more at www.publichealth.va.gov/smoking/quit.
Other VA Tobacco Cessation supportoptionsincludethefollowing:
A Self-Management Workbook to Help You on Your Journey to Quitting
This workbook is intended to be uti-lizedbyVeteransparticipatingincessa-
tionprograms.Itprovidesinformationabouttheharmfuleffectsof tobacco,preparing to quit tobacco, tips andstrategiesforsuccess,aswellasotherVA resources that can be accessed to accompanythismini-workbook.
QuitlineTobacco quitlines can double yourchance of quitting, compared to get-ting no support at all. And they’regreatforVeteranswithbusyschedulesor Veterans who can’t attend coun-seling in person. Call VA’s smokingquitline toll free at 1-855-QUIT-VET(1-855-784-8838). A counselor willanswer your call in less than a minute and begin helping you create your own personalquitplan.Yourcounselorwillaskyouaboutyourtobaccouse,quit-ting history, andmotivations to quit.Anyinformationyoushareduringthecallwillbekeptprivate.
A recent Veteran caller said, “Youknowwhat? This is actually going towork!” Let it work for you too, andcall1-855-QUIT-VET(1-855-784-8838)Monday throughFriday from6AMto6PMPacificTime.Counseling isavail-able in English and Spanish.
Visit www.publichealth.va.gov smoking/quitline.asptolearnmore.
Smokefreevet Text ServiceSmokefreeVET is a free text messag-ing service that sends daily support,advice, and encouragement directlytoyourmobilephone.Youwillreceive1-5messagesperdayandcanreceiveadditional quit support by textingkeywords such as URGE, STRESS, orSMOKED.
SignupfortheprograminEnglishbytexting the word VET to 47848 fromyourmobilephoneorbyvisitingwww.smokefree.gov/VET. For Spanish,text VETesp to 47848 or visit www.smokefree.gov/VETespanol.
Formore informationandtowatchashortvideoabouttheprogram,gotowww.publichealth.va.gov/smoking/smokefreevet.asp.
Stay Quit Coach App TheStayQuitCoachappwas specifi-cally designed to help Veterans with Post-TraumaticStressDisorder (PTSD)quit smoking. It has been shown todouble quit rates for Veterans withPTSD.
UsetheStayQuitCoachmobileappto:• Createacustomquitplanthattakes
into account your personal reasons for quitting, such as coping withsymptomsofPTSD;
• Learnmoreabouttherisksofsmok-ing, the benefits of quitting smok-ing,andhowtocopewithurgestosmoke;
• Access support contacts and hot-linesthatcanhelpyoustaysmoke-free;
• Receivemotivationalmessagesandreminderstotakeanymedications;and more.
How the VA Can Help Veterans Quit (Continued)

12
• StayQuitCoachisavailableforfreeone the Apple iTunes store. Learn more at mobile.va.gov/app/stay-quit-coach.
You're Not Alone: Join an Online Sup-port CommunityOntheSmokefreeVETFacebookpage[www.facebook.com/smokefreevet]Veterans can share stories, offer andreceivetipsandencouragement,findresources to help them as they quit,andgetthelatestnewsonthebenefitsoflivingatobacco-freelife.
Tobacco Cessation Counseling at your VA Puget Sound ClinicTherearemanylocaltobaccocessationresources, including group options atthemainfacilitiesaswellastheCBOCsorthroughtelehealthoptions.
Tobacco Cessation Events You have likely seen many of thesetobaccocessationresourcesathealthfairs, stroke fairs, diabetes fairs, andpatienteducationfairswhereyouhavetheopportunitytospeaktoourdedi-
cated doctors and nurses. Our Healthy LivingTeamreachesouttohelpmoti-vate and encourage Veterans to quittobacco. We asked Veterans visitingourTobaccoCessationboothwhetheroureffortswereeffective.Asaresultofvisitingourtobaccocessationboothpatientreportedthefollowing:1)94%reportedtheyweremorelikely
toreviewinformationandresourc-esaboutquittingtobacco.
2)88%reportedtheywouldbemorelikely to think aboutwhat quittingtobaccomightbelike.
3)81% reported theywould considermovingtowardquittingtobacco.
4)87%reportedtheywouldbemorelikelytotalkaboutquittingtobaccowith their health care team.
5)67%reportedtheywouldbemorelikelytomakeaplanforquittingto-bacco.
6)64% reported they would be morelikelytosetadateforquittingtobacco.
Not everyone is ready to quit rightnow and that’s okay. Our goal is toprovide those who use tobacco with information to at least think aboutquitting.That’sthefirststep.WewillsupportVeterans’effortstoquitusingtobacco in any way we can at VA Puget Sound.Yourhealthcareteamwillaskyou about tobacco use at least once a year.Ifyoudousetobacco,ourclinicalstaffare trained toguideyou towardresources to help you quitwheneveryou are ready.
[i] Department of Veterans Affairs (2006). 2005 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Com-parisons to the 1999-2003 Surveys. Re-trieved from https://www.va.gov/health-policyplanning/reports/FinalSOE_05.pdf
13
TheImplementationof2017FleischnerSocietyGuidelines-DiagnosticImagingService(DIS) JulieTakasugiMD,StevenZeliadt,PhD,LawrenceSwanson,ChristianHelfrich,PhD,LauraFeemster,MD
Quality Improvement Study: Imple-mentation of 2017 version of Fleis-chner Society Guidelines for Man-agement of Small Lung NodulesDiscovered on CT Scans at VA Puget Sound Health Care System.
History: In 2005 (1), the FleischnerSociety, an international society ofindividuals interested in lungdisease,published a set of guidelines for themanagement of small lung nodulesdetected on computed tomographic (CT) examinations. The goal of theguidelines was to provide a sensible and homogeneous pathway forman-agement of the numerous small pul-monary nodules identifiedbyCT andtoreducepatientanxiety,unnecessarypatient radiation exposure, health-carecostandtimeexpenditure.Priortothis,follow-upmanagementwaser-raticandatthediscretionoftheradi-ologist/pulmonologist/clinician caringforthepatient.Theinitialsetofguide-lines were applied to indeterminate,smalllungnodules,thosewithoutbe-nigncharacteristicsandofcompletelysolid nature.
VA Puget Sound Health Care System (VAPSHCS): 2011 (6 years afterpubli-cationoforiginal2005FSG)–Ourfa-cilityevaluatedtheCTreportsof153cancer-freepatientswithlungnodulestoseeiftheyrecommendedmanage-ment inaccordancewithFSG.To iso-late reports containing lung nodules only, not nodules in other organs, or“nodular opacities” of infection/in-flammation, the reports underwentscreening by a natural language pro-cessingprogram(WEKAtool)–apro-
gram that was being developed by Dr. Steven Zeliadt’s research group(VAPSHCS/UWMC).Resultswerethenmanually reviewed and if lung nod-ules were not present, reports wereexcluded. The 153 reports indicated above were the end results.
Nodules were categorized as 1) verysmall(≤4mm);2)stableorbenign;and3) indeterminate requiring additionalsurveillance. A radiologist specializing in thoracic imaging reviewed recom-mendationsandclinicalindicationsin-cludedinthetextreportandclassifiedfollow-uprecommendationsasappro-priate,inappropriateorincomplete.
Focusing on 139 patients with smalland/or stable nodules, our reviewfoundthat43%ofverysmallnodulesor clearly benign or stable nodules (categories 1 and 2) received appro-priaterecommendationfromtheradi-ologistintheCTreport.9%hadinap-propriate follow-up recommendation.Theremaining47%hadincompleteorvaguefollow-uprecommendations.
Amongthe14(9%)ofpatientswithinde-terminatenodules(category3),43%hadappropriate follow-up recommendationincluded in report, 43% had incorrectrecommendationwithfollow-upintervalnotappropriatelyspecifiedand14%hadincompleterecommendations.
2013 – The 2nd version of FSG waspublished and included management suggestionsforlungnodulesthatwerenotcompletelysolid,butpart-solidorfullyground-glass.
Implementation: In March of 2017,thelatest(3rd)versionoftheFSGwaspublished (3). Revisions were basedon experience with prior versions ofFSG, as well as lessons learned fromNational Lung Screen Programs. Theguidelines were not to be applied to individuals younger than35 years, topatients with knownmalignancies orimmunocompromisedstates,orinthepresence of active infections; whichareallvariablesthatsignificantlyaffectthelikelihoodofmalignancy.Therec-ommended surveillance was more so-phisticatedthantheoriginalFSG.Man-agementstrategiesdiffereddependingonwhetherthepatientwasathighorlowriskforlungcancer;whethernod-ules were solid, part-solid, or purelyground-glass,andwhether theyweresolitaryormultiple.Additionally,flex-ibility in the recommendedperiodoftimeuntilthenextCTscanwasaddedallowing the radiologist, clinician andpatient some input based on his/herconcernformalignancy.
To educate our radiologists on apply-ingthelatestFSG,2power-pointpre-sentationsweremadeavailabletotheattendingradiologists intheVAPSHCSBody Imaging section. The first pre-sentationexplainedCTtechnique,de-scribednoduletypes,CTfindingssus-picious for malignancy, how nodulesaremeasured,whatnodulesshouldbereported, and the new FSG. The 2ndpower-point was a self- assessmentthat included 35 test cases with imag-esandpossiblefollow-upapproaches.The test cases were selected to rep-resent both common presentation ofnodules as well as to highlight instanc-

14
eswhenFSGwouldindicateadditionalfollow-up is not necessary. AnswerswithassociatedwithFSGrecommend-edfollow-upandclinicalreasoningforfollow-upwereimmediatelyavailable.Body Imaging attendings were askedto review the power-point presenta-tions.Scoresfromtheself-assessmentwerenotcollected.The2017FSGwasposted on the wall in the reading room above the workstations of the BodyImagingsection.
Results: To learn whether our radi-ologists were compliant with the new FSG,anothergroupofCTreportswassampled. InDecemberof2017,chestCT reports (with lung nodules identi-fied by WEKA tool) were pulled forthe months of April, May, and Juneof 2017. These reports were not ashighly selected as the original 2011 set,sosomedifferencesinthereportpools between the 2 groups would be expected. 285 reports were selected from 377. Excluded reports (92) in-cluded those that were dictated by non-PSVAradiologistswhodidnotun-dergo training, reports from patientswithaknownmalignancyorimmuno-compromisedstateifidentifiedinthebody of the dictated report (not FSGcandidates). The nodules were notsub-categorizedintoverysmall,stable
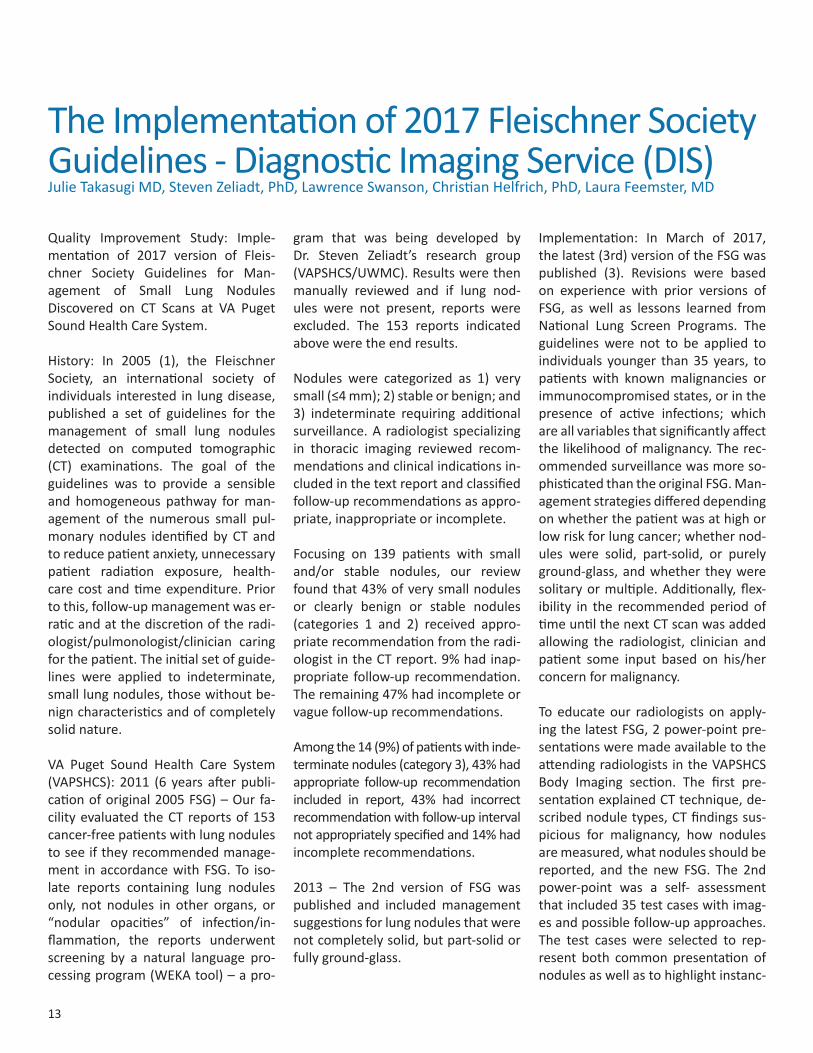
orbenign,orindeterminatesincethatstatus was not always available to the radiologist or to us. Individuals who may have had a malignancy or immu-nocompromised state, but could notbeidentifiedassuchbyreviewoftheradiology report (clinical history wasnot made available) were included.The same chest radiologist reviewed these 285 reports and classified fol-low-up recommendations made bythe interpreting radiologists as ap-propriate, inappropriate, or missing/vague.43%(123/285)wereappropri-ate,23%(66/285)wereinappropriate,34%(96/285)werevagueormissing.
Following the FSG training, one radi-ologist expressed concern with recom-mending specific follow-up manage-mentinaccordancewithFSGbecauseof a lack of radiologist knowledge ofpatient risk-factors (smoking status,pack-years of smoking, carcinogenicexposures, etc.) for lung cancer. Re-sults above show the percentages ofappropriate, inappropriateandvagueormissingrecommendationsmadebyallradiologistsin2017(2017all),with-outtheoneradiologist in2017(2017[-1rad]) and all radiologists in 2011(2011all).
(Continued on next page)
15
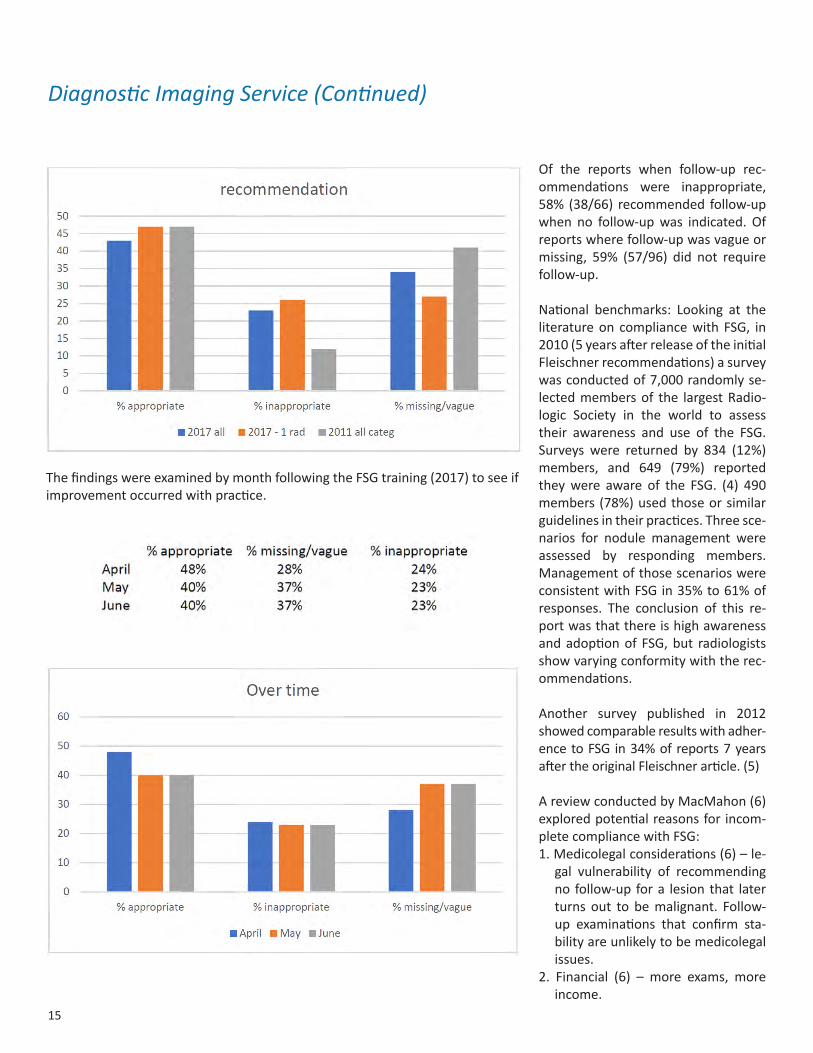
ThefindingswereexaminedbymonthfollowingtheFSGtraining(2017)toseeifimprovementoccurredwithpractice.
Of the reports when follow-up rec-ommendations were inappropriate,58% (38/66) recommended follow-upwhen no follow-upwas indicated. Ofreportswherefollow-upwasvagueormissing, 59% (57/96) did not requirefollow-up.
National benchmarks: Looking at theliteratureon compliancewith FSG, in2010(5yearsafterreleaseoftheinitialFleischnerrecommendations)asurveywasconductedof7,000randomlyse-lectedmembersof the largestRadio-logic Society in the world to assess their awareness and use of the FSG.Surveys were returned by 834 (12%)members, and 649 (79%) reportedtheywere aware of the FSG. (4) 490members(78%)usedthoseorsimilarguidelinesintheirpractices.Threesce-narios for nodule management wereassessed by responding members. ManagementofthosescenarioswereconsistentwithFSGin35%to61%ofresponses. The conclusion of this re-port was that there is high awareness andadoptionofFSG,but radiologistsshowvaryingconformitywiththerec-ommendations.
Another survey published in 2012 showed comparable results with adher-encetoFSG in34%ofreports7yearsaftertheoriginalFleischnerarticle.(5)
AreviewconductedbyMacMahon(6)exploredpotentialreasonsforincom-pletecompliancewithFSG:1.Medicolegalconsiderations(6)–le-
gal vulnerability of recommendingno follow-up fora lesion that laterturns out to bemalignant. Follow-up examinations that confirm sta-bilityareunlikelytobemedicolegalissues.
2. Financial (6) – more exams, moreincome.
Diagnostic Imaging Service (Continued)

16
3. Pressure by patient or clinician tofollowmorecloselythannecessary(6).
4. Remembering to use FSG, remem-bering to remind residents/fellowto use.
5.Difficulty remembering specificguidelinerecommendations(5)
Inadditiontothesereasons,ourstudyidentifiedadditionalpotentialreasonsstatedbyradiologiststhatareuniquetotheupdatedFSG.6.PracticeneededtounlearnoldFSG
recommendation,makecorrectfol-low-uprecommendationsbasedonchangesmade in2017FSGregard-ingnodulesizeandtimingofsubse-quentCTscans.
7. Patient risk factors, highlighted byupdatedFSG,areoftennotprovid-edbyorderingclinician/patients
Anotherstudy(7)thatfocusedonim-provingFSGcomplianceshowednear-ly twice the level of FSG adherence(82%).Thatachievementwascreditedto the radiology department stressing useofFSGtoreducepatientradiationexposure and health care costs. Small laminated cardshaving theFSGwereattachedtoeveryworkstationat thatfacility.
In addition, the increase in complex-ityinthe3rditerationoftheFSGitselfmay have contributed to the greater proportion of inappropriate recom-mendationobserved in the follow-upperiod. Research in behavioral eco-nomics has demonstrated that as de-cision-makingbecomesmorecomplex(e.g., more options are available ormorevariablesneedtobeevaluated)individuals are more likely to experi-ence choice overload. One way they deal with choice overload is to revert
to prior habits or defaults. (https://www.behavioraleconomics.com/mini-encyclopedia-of-be/choice-over-load/).Facedwithflexibilityintherec-ommendedfollow-uptimeperiodanduncertaintyaboutpatientriskfactors,it might be expected that radiologists reverting to decision defaults wouldrecommendmore frequent follow-upthan appropriate.
Summary: Following educationalsteps, a self-assessment tool, andposting FSG on-site above the workareafortheBodyImagingsection,wewereabletoimplementtheuseofthe2017FleischnerSocietyGuidelinesformanagement of small lung noduleswith adherence in accordance with reportedbenchmarksforpreviousedi-tionsofFSG.
CorrectiveActionPlan:Although we achieved adherence at about 45%, there is significant roomforimprovement.1. Our department should make fur-
thereffortstohighlightFSG,includ-ing promoting their use throughposting and discussion at facultymeetings,educatingandremindingstudents to use FSG, and sendingreminders to each Body Imaging at-tending,residentandfellowatthebeginningofeachrotation(every4weeks).
2.Our department shouldworkwithPrimaryCare,Pulmonaryandotherordering providers to ensure pa-tient risk-factors for cancer are in-cluded in CT orders. This issue can beaddressedforFSGcandidatesaswellaspotentialLungScreencandi-datesthroughseveralpaths:a.Patientquestionnaireb. CPRS pulled datac.Referringclinicianquestionnaire (Continued on next page)
17
RadiationOncologyTonyQuang,MD,JD,AdamTazi,PhD,andKentWallner,MD
3.Recurringreview:Ourfacultyismo-tivatedtoimproveadherencetothenewFSGandwillprioritizerecurringreviews.WhentheDiagnosticImag-ing Service is fully staffed, we willroutinelysamplesetsofCTreportsfrom all Body Imaging attendingphysicians forreviewofadherencetoFSGandfeedbackwillbeprovid-ed to the radiologist.
4. Although financial incentives havebeen highlighted as a concern in other settings, this likely does notaffectourdepartmentbecausetheattending physicians are salariedand there are not financial incen-tives to recommended additionalimagingat thetimeofexam inter-pretationandreporting.
References:1. Guidelines for Management of
Small Pulmonary Nodules Detected onCTScans:AStatementfromtheFleischner Society. MacMahon H,AustinJHM,GamsuG,etal.Radiol-ogy2005;237:395-400.
2.RecommendationsfortheManage-ment of Subsolid Pulmonary Nod-ules Detected at CT: A StatementfromtheFleischnerSociety.NaidichDP,BankierAA,MacMahonH,etal.Radiology2013;266(1):304-17.
3.GuidelinesforManagementofInci-dental Pulmonary Nodules Detect-ed on CT Images: From the Fleis-chner Society2017.MacMahonH,NaidichDP,GooJM,etal.Radiology2017;284:1:228-43.
4. Eisenberg RL, Bankier AA, BoisellePM. Compliance with FleischnerSociety Guidelines for Manage-mentofSmallLungNodules:Asur-vey of 834 radiologists. Radiology2010;255(1):218-224
5. Lacson R, Prevedello LM, AndrioleKPetal.FactorsAssociatedwithRa-diologists’AdherencetoFleischnerSocietyGuidelinesforManagementof Pulmonary Nodules. J Am CollRadiol2012;9:468-73
6.MacMahonH.CompliancewithFSGforManagement of LungNodules:LessonsandOpportunities.Radiol-ogy2010;255:14-15
7.EisenbergRL.WaystoImproveRadi-ologists’AdherencetoFSGforMan-agement of Pulmonary Nodules. JAmCollRadiol2013;10:439-441.
Diagnostic Imaging Service (Continued)
The VA Puget Sound Health Care Sys-tem is a radiation oncology referralcenter in theVeteransAffairssystem,which is the first radiation oncologyfacilityintheStateofWashingtonac-credited by the American College ofRadiology. It provides cancer care for patients from the VA NorthwestHealthNetwork20whichservesAlas-ka, Idaho, Oregon and Washington.Wedeliverstateoftheartclinicalcaretopatients.
Weseizeeveryopportunity to imple-menttechnologicaladvances.Wearecurrently preparing to upgrade our linear accelerators and standard op-erating procedures in anticipation ofoffering SBRT (stereotactic body ra-diotherapy) and SRS (stereotactic ra-diosurgery) treatments. Thiseffort is
spear-headed by our interdisciplinaryteam of radiation oncologists—TonyS.Quang,MD,JDandKentE.Wallner,MD, physicists Adam Tazi, PhD andCarlBergsagel,MS,dosimetristsDavidCain,CMD,ARRT(T),andBlakeWebb,CMD, ARRT(T). Moreover, MelissaMitchell,CMD,ARRT(T)hasservedasliaison between dosimetry and treat-mentdelivery;KarinaDean,ARRT(T)isdevelopingstandardoperatingproce-dures to improveworkflowbetweenCTsimulationandtreatmentdelivery;andJanyceShort,ARRT(T)hasfocusedoninformaticstobetternavigateMO-SAIQ.
While IMRT (intensity-modulated ra-diotherapy) continues to be used totreat head and neck, prostate, lung,andrectalcancers,VMAT(volumetric-
modulated arc therapy), a faster andbetter techniqueof radiation therapydelivery,hasbeencommissionedandadded to the treatment planning tool box.Infact,VMAThasbeeninclinicaluseformorethan1.5years.
As part of external peer review forquality assurancemeasurements anddosimetry review of our radiationtreatment machines and planning sys-tem,werecentlyhadanonsitevisitonOctober24–26,2018,byIROC(Imaging and Radiation OncologyCore)fromMDAndersonCancerCen-ter in Houston, Texas. IROC providedtheserviceunderagrantfromtheNa-tionalCancer Instituteandacontractwith the Department of Veterans Af-fairs. Because of this affiliation IROCobtained confirmatory machine data

18
andreviewedourcalculationalproce-dures to ensure accuracy. The outcome ofthereviewincludedafewexcellentrecommendationsandthefindingthatthere were no items missing in our current quality assurance program.BecauseofDr.AdamTazi’sleadership,our physics program is second to none.
Wecontinuetoperformrigorouscon-tinuous quality improvement includ-ing interdisciplinary chart rounds,morbidity andmortality conferences,outcomes studies, focus studies, andpeer review. Drs. Quang and Wall-ner are active participants at weeklyTumor Board meetings. Dr. Wallnerruns monthly journal clubs teaching residentsatUniversityofWashingtonMedicalCenter.Drs.QuangandWall-ner continue to be Visiting OncologyLecturers at Bellevue College teaching clinical oncology to radiation therapystudents. Students from this trainingprogram have consistently over the years scored in the90th to95th-per-centileontheirboardexaminations.
Asaninternationalauthorityonpros-tate brachytherapy, Dr. Wallner haspioneered a specialty clinic, whichcontinues to offer seed implant toprostate cancer patients in the coun-try.Wehaveintegratedbrachytherapywith an interdisciplinary prostate can-cerprogramthatincludesIMRT/VMATwithplacementofgoldseedfiducialsforIGRT(image-guidedradiotherapy).Moreover, using a shorter course—hypofractionated radiation therapytreatment has allowed patients tocomplete their treatment quicker sotheycangobackhome.Patientshavetolerated this regimen exceptionallywellandhaveexpressedhighsatisfac-tionwiththeconvenience.
Furthermore,Dr.Quang remainsasaBoardMember to the Association ofVA Hematology/Oncology, an organi-zation with members who are inter-ested in advocating and promotingcancer care of Veterans. At the lastannualmeeting in Chicago, Illinois inSeptember 2018, he served as oneof the moderators for the scientificposter session. He continues topro-videourVAwithup-to-datescientificand best clinical practice expertise inhis respective roles as Surveyor fortheAmericanCollegeofRadiology.Dr.Quang also serves on the American So-ciety for RadiationOncology (ASTRO)Bylaws Committee. Dr. Quang servesasaBoardmembertotheWashingtonState Medical Associations and joinedtheCommitteeonUniversalHealthcare.
The VA Puget Sound Radiation Ther-apy Department has maintained its position as anationally visible centerdrawingreferralsfromotherVAfacili-tiesthroughouttheUnitedStates.Ourdepartment continues to successfullyimplement technological advances andupgradestoofferstateoftheartcancercare.Ourexpansionofcuttingedge technology, continued innova-tion efforts, and our commitment toquality assurance through the imple-mentation of a robust continuousquality improvement has positionedour department to offer our patientsthebestofcarefornowandwellintothe future. With costs continuing toincrease inhealth care,which affectsaccess tocare, it isnowmore impor-tantthanevertoreaffirmourcommit-ment to our Veterans.
Radiation Oncology (Continued)

19
Palliative Care Service Growth Summary:The SeattleVAPalliativeCare consul-tation service continues to expandat a rapid pace. Themajority of newgrowth is in theoutpatientclinicandwehaveenjoyedgettingtoknowandworkwithVeteransoutsideofthehos-pital setting. Consults and follow-uprequests from Oncology services, in-cludingRadiationOncology,continuestobeourtopsourceofreferrals,andweoftenseeVeteransduringtheirap-pointments with other specialty pro-viders. Our local Cancer Navigationteamcontinues tobe instrumental inidentifying and facilitating additionalsupport for Veterans with a cancerdiagnosis who may benefit from en-hanced palliative specialty care. Thiscare includes complex symptom man-agement, helping patients to identifyandaddresstheirgoalsofcare,aswellasfindingadditionalservicesandpro-grams to help individuals maintain as much independence and functioningas possible while they receive impor-tant treatments.
Thefollowingservicescontinuetobeoffered:Acutecareconsultation,out-patient consultation, non-visit con-sults, andhospice in theVACommu-nity Living Center. We also continue
AnnualPalliativeCareReport2018AliceFoy,ARNP,CHPN
to partner with community based pal-liativeandhospiceagenciestoensurethat care is being provided for Vet-erans with advanced illness. We areabletoseenewclinicpatientswithinamonthandcanoftenaccommodateurgentvisitswithindays.Wehavealsobeenabletoutilizenon-VAcommunitybasedpalliativecareservicestomeetgrowing needs and distance challenges forourVeteransoutsideofKingCoun-ty.AmericanLakehasrecentlyaddedanewMDandARNPfortheirPalliativeCareconsultationserviceandarenowable to see Veterans in clinic on Mon-dayandWednesdayatthatlocation.
Education: Our teaching program continues togrowandwelookforwardtoarobustpalliative fellowship program againnextyear.WenowalsohaveanactiveCLChospicerotationfor4thyearMed-ical Students as well.
Advanced planning initiative:We continue to implement The Life-SustainingTreatmentDecisions Initia-tive (LSTDI,) aVAnationwidequalityimprovement project to improve pa-tient-centered care for Veteranswithserious illness. The project promotes proactive goals of care conversations
with patientswho are at high risk ofa life-threatening clinical event.Mostof theOncologists andPalliativePhy-sicians have already completed this trainingwhichisanimportantpartofensuringthatVeteranandfamilygoalsare understood and honored at all stagesofanillness.
Special Projects:Thepalliativecareteamiscollaborat-ing on a very important project to de-velopabettersymptommanagementpathway for Veterans experiencingHead and Neck cancer. Tamarind Ke-ating,ARNPof theCancerNavigationTeam,isleadingoureffortstoidentifythe best and most effective ways toaddress the very complex symptoms,particularly pain, that these individu-als experience during and after thetreatment process. Because we feelthat this project has valuable and im-portantimplicationsforboththelocalandnational level in ensuringqualitycare for Veterans, the Palliative CareteamhasmadethefocalpointoftheirFY 2019 “Smart Goal” to support allcancerteameffortsincreatingacom-prehensive plan to deliver effectivesymptom management.
20
The surgical oncology program pro-vides comprehensive evaluation andtreatment for tumors of the upperand lower gastrointestinal tract, hep-atobiliary system, pancreas, breast,melanoma, soft tissue sarcoma, andendocrine system. Together with Drs. Lorrie Langdale, Roger Tatum, DanaLynge,EdgarFigueredo,andDeborahMarquardt;oursectionprovidessurgi-calexpertisecoveringabroadrangeofprocedures, including sentinel lymphnodemapping,minimallyinvasiveandroboticsurgery,andcomplexoncologicresections including esophagectomy,hepatic resection, pancreaticoduode-nectomy and total mesorectal exci-sionwithanalsphincterpreservation.We work in tandem with colleaguesinMedicalandRadiationOncologytooffer personalized combined modal-ity protocols. Our goals are to provide state-of-the-artsolidtumortreatmentin a multidisciplinary environment,enrollpatientsincancerclinicaltrials,conduct innovative cancer research,and provide education and mentor-ship to our students, residents, andfellowsaffiliatedwiththeUniversityofWashingtonandFredHutchinsonCan-cer Research Center.
Surgical OncologyPeterWu,MD
The Cancer Telemedicine Program based at the VA Puget Sound is broad-cast twice monthly and serves to ad-vise and coordinate multidisciplinaryoncology care throughout the Veterans IntegratedServiceNetwork(VISN)20.Originally conceived as the Northern AllianceCancerCenterandfundedbytheVANewClinicalInitiativesProgramandVACOTransformational InitiativesProgram,theVACancerTelemedicineProgram has matured into a vital clini-cal program for the region. ProvidersatregionalVAfacilitiesthroughouttheVISN 20 present cases in a live interac-tiveformattothemultidisciplinarytu-morboardinSeattlestaffedbysurgicalandmedicaloncologists.Participationin this program facilitates patient re-ferral, minimizes consultation delays,avoidsunnecessarypatienttravel,co-ordinatesoutpatientstudies,andpro-videsmultidisciplinaryevaluationofallcancerpatients.Theprogram’ssuccessensures that all veterans within the VISN20haveaccesstostate-of-the-artmultidisciplinarycancercare.
For further information, please con-tactourCancerTelehealthCoodinator,Lisa Mandell, R.N., J.D. e-mail: [email protected]
Cancer Telemedicine ProgramPeterWu,MD

21
A multidisciplinary team partneringwithVeteranswith cancer to identifyand eliminate barriers to care and im-prove patient outcomes. Cancer pa-tientnavigationwasdevelopedinthe1990s as a method to address health disparitiesthatimpactcancerpreven-tion, detection, diagnosis, treatmentand survival. Poverty, lack of insur-ance,distancefromatreatmentfacil-ity andother factorsmaybebarriersthatpreventpatientsfromgettingnec-essaryandtimelycare.Bypartneringwith vulnerable patient populationstoidentifyandaddressthesebarriers,navigationprogramshavebeenabletoimprovescreeningrates,timelinessofcare, compliance, patient satisfactionand survival rates. These programs have been implemented in cancer centersacrossthecountryandpatientnavigation is now a standard of carefor programs accreditedby theCom-mission on Cancer.
The VA Puget Sound Cancer Care Navi-gationTeam(CCNT)wasestablishedaspartofanetworkofCancerCareNavi-gation Teams across VISN20with ad-ditionalsitesinIdaho(Boise),Oregon(Portland, White City and Roseburg),and Washington (Spokane, and WallaWalla).InSeattle,CCNTincludesanursepractitioner, registered nurse, socialworkerandprogramsupportassistant.
Veterans with cancer may experience anumberofbarriers to receiving thecaretheyneed,includingalackofso-cialsupportorcaregiver,difficultywithtransportation or travel, coordinatingappointments with multiple services,distress,poornutrition,andlowhealth
literacy.WhenaVeteranisreferredtoCCNT,ourstaffconductacomprehen-sive assessment for distress and bar-riers to care and individualize a plan of care foreachVeteran.Weprovidepatient education regarding their di-agnosis and treatment and resources available fromtheVA.Weassistwithschedulecoordinationtoreduceaddi-tionaltripstoourfacilityandcounselVeterans regarding the costs of theircare with referrals to eligibility andcommunity sources of financial sup-port when available.
ForVeteransreferredfromanotherVAfacility, CCNT conducts a history andphysical exam to document and ad-dressotherhealthconditionsthatmaybe relevant during an extended stay awayfromhome.Veteransreceiveon-going support through their treatment and a written treatment summary attheend,detailingtheircancerdiagnosis,treatment,complicationsandfollow-upplan.Thisinformationissenttohomeprovidersviainterfacilityconsult.
For Veterans who are within the VAPuget Sound catchment that report significant barriers in traveling to Se-attleforcancer-relatedtreatmentthatcannotberesolvedbyCCNT,aformalreview process is in place to review named barriers or “geoburden” forconsideration of the Veteran receiv-ing their cancer care locally. CCNT completes a thorough geoburden as-sessment and presents this informa-tiontoVISN20CancerInterdisciplinaryPurchaseCareTeamforreviewbasedon established care routing businessrules. Upon approval of local cancer
care,CCNTcontinuestoassisttheVet-eraninsettingupcareinthecommu-nitytoassureitistimely.
The Cancer Survivorship Clinic coun-sels Veterans regarding their diagno-sis and treatment and related poten-tial latehealtheffects.A survivorshipcare plan is detailed for the Veteranand their health care providers and resources are provided to assist Vet-eransinmanagingsomeoftheuniqueaspects of physical and psychosocialhealth following cancer treatment.The Cancer Survivorship Clinic is meet-ingthegoalsetforthbytheCommis-siononCancerthatourfacilityprovidethis care tomore than50%ofall eli-giblecancerpatientseachyear.
To date, the VA Puget Sound CancerCare Navigation Team has enrolledover2000Veterans innavigationser-vices.Approximately50%ofthesepa-tients are referred from VA facilitiesacross VISN 20 while the other 50%comefromtheVAPugetSoundcatch-ment area. We have received over1700consultsfrom320VAproviders,including specialty and primary care providers,nurses,dieticians,andcoor-dinators. Over 400 Veterans have been seen in the Cancer Survivorship Clinic.
To refer a Veteran to CCNT: Submita consult to Cancer Care NavigationTeamintheCPRSconsultmenuorcall:206-277-4593
CancerCareNavigationTeam and Survivorship ClinicLynsiSlind,RN,MN,TamarindKeating,ARNP, AnaFisher,LICSWOSW-C,WerkuDemisse,MSA
22
Speech Language Pathologists (alsoknown as Speech Therapists) are ac-tively involved in thecareofpatientsifspeech/communication,swallowing,and/orcognitionareeffectedbycan-cer.Weworkwithpatientsattheon-setofcancerdiagnosis,throughoutthecourse of their treatment, and yearsafterthecompletionoftheirtreatmentfor ongoing therapy or managementof any difficulties that may continue.We primarily work with patients whoare diagnosedwith head and/or neckcancers,butwecanworkwithpatientswithothertypesofcancertoo.
Speech Language Pathologists are specialists that help educate you and your family about ways to minimizethesideeffectsofheadandneckcan-cer,bothfromthetumoritself,orthesideeffectsoftreatment.SpeechLan-guage Pathologists can help manage the symptoms that you are experienc-ingwhetheryouundergosurgery, ra-diation, chemotherapy, or even if notreatment course is pursued.
Because the cancer and/or its treat-mentoftenaffecttheabilitytotalkandeat, theSpeechLanguagePathologistevaluatesforanychewing,swallowing,speech/communication, language, orcognitivedifficultiesandprovidesedu-cationandtherapyasneeded.
Someexamplesoftheareas inwhichSpeech Language Pathologists help cancerpatientsandtheirfamilies:- Difficulty eating or drinking (dys-
phagia),suchasdifficultychewing,difficultyswallowing,orothercom-plicationsarisingfromthetumororsurgery.
- Preventionofswallowingproblems
mentioned above that may occurfrom the treatment (radiation orchemotherapy).
- Changes in your voice or speechproduction.
- Evaluating andmanaging cognitive(memory,attention)changes.
- Managementofyourstomaandal-ternative communication options/methods following Total Laryngec-tomy Surgery.
When you meet with a Speech Lan-guagePathologist,theymayhelpyouwiththefollowing:- Understand themuscles, anatomy,
and sequence involved in eating,drinking,andtalking.
- Understand more about your sur-gery or treatment and how it may affect your ability to eat, drink, orcommunicate.
- Learn the short and long term ef-fectsofchemotherapyandradiationon speech and swallowing and ways tominimizeanyadverseeffects.
- Evaluateforanydifficultiesyoumayalready havewith talking and eat-ing,aswellasmonitoryouforanychangesintheseabilitiesasyouprog-resswiththerapy.Wecandothisbothclinically and instrumentally with a varietyofevaluationmethods.
- Teach youways tominimize effectsofsurgeryortreatmentonyourswal-lowfunction,suchascompensatorystrategiesordietmodifications.
- Teach you exercises to maximizeshortand longtermrangeofmotion,strength,andoverallfunctiontocom-bateffectsofsurgeryand/ortreatment.
- Teachyouways tocompensate forany speech or voice changes, in-cludinguseof compensatory strat-egies,compensatorytools,orother
alternative methods of commu-nicationthatmaybeusedintheshort and long term. Tools and devices include simple “low tech” options, such as writing padsor picture boards, as well more“hightech”optionssuchasalter-native communication devices,voice amplifiers, tablet applica-tions,etc.
Ideally, patients should expect tosee a Speech Language Pathologist whenever they are experiencing changes in their swallowing, com-munication,orcognition–andthismay occur even prior to their diag-nosis. However, once diagnosed,SpeechLanguagePathologistsliketoseepatientsatthefollowingtimes:- Priortosurgerytodiscusschanges
inswallowing,speech/communica-tion,or cognitionandways to im-mediatelycompensateforchanges.
- Followingsurgerytohelpmanageany changes (whether in acutecareorintheoutpatientsetting).
- Priortoinitiatingradiationtherapyand throughout your treatment.
- Intensivetreatmentoroccasionalfollow-up after treatment, de-pending on your needs.
Swallowing and communicationareextremely importantaspectsofthehumanconditionthatweoftentake for granted until changes oc-cur; our goals as Speech Language Pathologists are to help you under-stand how your cancer diagnosis and treatment can impact talking,eating, and thinking, butmore im-portantly to maximize your qualityoflifeduringyourtreatmentandfortheremainderofyourlife.
Speech Language Pathology (RehabilitationCareServices)EmilyJohnson,MS,CCC-SLP

23
BeyondCancerCare:WholeHealthCareDr.LeilaKozak
Anewlyexpandedparadigmforhealthcare called Whole Health is beingtestedattheU.S.DepartmentofVet-eransAffairs(VA).WholeHealthgoesbeyondyourillnesses,injuries,ordis-abilities. The Whole Health conceptincludesconventionaltreatment,self-empowerment, apersonalizedhealthplan, self-healing, self-care, and non-drug complementary and integrativetherapies.
InWholeHealthcare,theVeteranisanactivepartnerwithhis/herhealthcareteam.WhyistheVAchangingthewayhealth care is provided? The core mis-sionofVeteransHealthAdministrationis to “Honor America’s Veterans by providingexceptionalhealthcarethatimprovestheirhealthandwell-being.”OnThursday,November29,Dr. TracyGaudet, director of the Office of Pa-tientCenteredCareandCulturalTrans-formation–OPCC&CTC–atVACentralOffice, spoke at the National Insti-tutes of Health about the VA’s jour-neythroughthisnewmodelofhealthcare.This innovativemodelofcare isbecoming an example to other health caresystems,showingexcitingpoten-tialforapplicationtootherhealthcaresystems.Dr.Gaudet’spresentationwillbestreamedliveontheNationalCen-terforComplementaryandIntegrativeHealthFacebookpage(https://bit.ly/2ArAoEi?fbclid=IwAR08xFU940TMmCn8amGgVwqCtgv_rt-L8YOf40CMlKxMgvAQPCZm301-XqM).
Join the conversation on Twitter us-ing #ChatVets #Straus18 http://bit.ly/2ArAn3c
Whole Health Approach to Engage Transitioning Service Members According to the guidance on the Exec-utiveOrdersignedbyPresidentTrumpon January 9, 2018, the VHA WholeHealth approach will be the corner-stone to engage transitioning Servicemembersindiscoveringtheirmission,aspiration, purpose and learning ac-tivitiestopromotewell-being.
The Whole Health Pathway compo-nent of the Whole Health approachconsistsoftwokeyaspects:
1. Introduction toWhole Health ses-sions,thatprovidesthecontextfortheWholeHealthapproachonboththeNationalandlocallevels.
2.TakingChargeofMy Life&Healthpeer group sessions
AllVeteranswhoparticipateintheIn-troductiontoWholeHealthsessionarepreparedtojointheTakingChargeofMyLifeandHealthpeer-ledgroupses-sions. These sessions provide a more in-depth immersion into self-explora-tion,self-careandgoal-creationaroundwhatreallymatterstotheVeteran.
Informationandresourcestosupportour facility’s Whole Health Pathwaymaybefoundhttps://vaww.infoshare.va.gov/sites/OPCC/2018ExecutiveOrderGuidanceTraining/Forms/AllItems.aspx.
ForWholeHealtheducationresources,visit https://vaww.infoshare.va.gov/sites/OPCC/Education/SitePages/Home.aspx
VA Puget Sound expanding Whole Health CareAs of today, every VA facility aroundthecountryisrequiredtoofferthefol-lowingintegrativetherapies:• Acupuncture• Biofeedback• Clinical Hypnosis • Guided Imagery • Meditation:Mindfulness,Mantram
Repetition,IRest• Massage• TaiChi/QiGong• Yoga
HerearesomeexamplesofhowWholeHealth is actively being implementedatVAPugetSound:o Lastyear,VAPugetSoundheldaTai
Chitrainingforstaffwhere20healthcare providers completed the train-ing, including one of our radiationoncologists,Dr. TonyQuang.Manyof these providers are offering TaiChiclassesthroughoutthefacility.
o Wealsocontinuetohaveanexten-sive Mindfulness program led byDr.DavidKearney,whoseprogramshave reached out to Veterans and staff for many years. In addition,various staff members have re-cently received training in and are currently offering classes on IRestmeditation.
o WithinPrimaryCareMentalHealthIntegration, Dr. Kelly Caver will beoffering clinical hypnosis to Veter-ans living with Chronic Pain.
o Bothofourfacilitieshadveryactiveacupunctureclinicsformanyyears,led by our two nurse acupuncturists LaurieanneNabingerRN,L.AC.andMary Muth RN L.Ac. During the last year, two other staff members atAmericanLake(BernardCanlasMD

24
and StevenHedt PA) also receivedfundingtoattendmedicalacupunc-ture training.
o During the next 4 years, VA PugetSoundwillalsobeoneof3nationalresearchsitesforMissionReconnect(https://missionreconnect.com).Mission Reconnect is an evidence-based on-demand program thatteachesWholeHealthinterventionsvia a mobile app. Veterans and their partners/spouses participating inthis project will have free accessto the mobile app where they will learnmeditationtechniques, relax-ation exercises and instruction insimplemassagetechniquestopro-motestressreductionandinterper-sonal connection. To participate inthisopportunity,[email protected].
o In addition, Veterans at VA PugetSound HCS have access to OPCC&CT onlineresourcescompletelyfreeofcharge such as a library of guidedmeditations available on demand(https://www.healthjourneys.com/partneraccess/index/). Guided im-agery and meditation have beenshown to reduce stress, improvesleep, reduce pain, and clear the
way for finding your owndeep in-ner peace. This page streams a va-rietyofbriefmeditationsbyleadingpractitionersinthemind-bodyfield.Findyourfavorites,listenregularly,andenjoy thebenefits. Inviteyourfamily to use the page, too. It’savailable24/7
o Another meditation resourcefree of charge is the MeditationOasis® Podcast (https://www.meditationoasis.com/podcast)that features guided meditations,instructions for meditation, andmusicformeditation.Youcanlistento it at iTunes or Google Play or by clickingontheplaybuttons.
o Youwill find otherweb-based andmobile tools to support your whole health journey from patient cen-tered care at va.gov.
Recently,our facilityhas takenanewstepbycreatingtheWholeHealthCo-alition,agroupthathasbeenmeetingto develop a charter and organiza-tionalplanforWholeHealthatPugetSound.ThiswilltakeWholeHealthtoanew levelof integrationand imple-mentationatbothofourfacilitiesandcommunity clinics.
Why is Whole Health such an im-portant addition to Cancer Care?Integrative therapies are abig partofwholehealthcare.Someofthesetherapies have been shown to de-creaseanxietyandpain,toimprovemood and to help manage chemo-therapy-inducednauseaandvomit-ing. For example, acupuncture andaromatherapy are widely used to decrease chemotherapy-inducednauseaandvomitingatcancercareservices around the world. Mas-sage, acupuncture and music arecurrently used to help manage pain andanxiety.Yoga,taichiandmedi-tationareofferedwithincancercareto help manage pain and anxiety andenhancequalityoflife.
Anestimated50%ofcancerpatientsin the United States already use in-tegrative therapies to deal withside effects from cancer treatmentincluding massage, acupuncture,aromatherapy, hypnosis, guidedimagery,meditation, art andmusictherapy,yogaandtaichi.
To learn more about WholeHealth and how whole health can benefit you, visit the Office ofPatient Centered Care and CulturalTransformation’s site (https://www.va.gov/patientcenteredcare/)
You can also explore a variety ofWholeHealthvideoresources,readmoreaboutVA’sWholeHealthPeerto Peer programandfindmore in-formation about Whole HealthPeertoPeertrainingprogramfromabovelink.

25
For patients undergoing cancer treat-ment,qualityoflifemattersasmuch—ifnotmore—thanthequantityof life.Withanincreasingfocusonrehabilita-tion,patientsareabletohaveimprovedquality of life during and after theircancertreatment.Patientsundergoingcancer treatment may experience one ormore of the following side effects:decreasedmuscle strength,decreasedbone density, peripheral neuropathyrelated to chemotherapy, fatigue, de-creasedrangeofmotion,pain, lymph-edema,and scaradhesion.Rehabilita-tion Care Services can assist patientswho have been diagnosed with cancer withavarietyoftheirrehabneedsonaninpatientoroutpatientbasis.Theseneeds include pain control, weaknessanddeconditioning,mobility includingassessmentandprovisionofequipmentformobilitysafety,activitiesofdailyliv-ingsuchasdressing/grooming/bathing,cognition,communication,swallowing,nutrition, bowel/bladder functions,skinintegrityandwoundmanagement,lymphedema management, depres-sion/adjustment/anxiety, social sup-port,andvocationalguidance.Goalsforcancer rehabilitation often include ef-fectivepaincontrol,maximalfunctionalindependence, restorationofmaximalstrength and mobility, prevention offurtherimpairment,care-givertrainingto assist functionally-dependent pa-tients,homemanagement,communityreintegration, and behavioral adapta-tion topain and illness. In addition, aspecialized service that RehabilitationCareServicesoffersisCompleteDecon-gestiveTherapy(CDT),atreatmentforlymphedema. Lymphedema is swelling ofabodypart,mostcommonlyinvolv-
CancerRehabilitation/ RehabilitationCareServiceMegSablinsky,PT,DPT,CLT–LANA
ingtheextremities,faceandneckbutitmayalsooccurinthetrunk,abdomenor genital area. It is most commonly theresultofdamagetothe lymphaticsystem due to surgery or radiationtreatmenttherapy,surgicalproceduresperformed in combination with theremovalof lymphnodessuchasmas-tectomies, lumpectomies, prostatec-tomies,orneckdissectionprocedures,trauma or infection of the lymphaticsystem,aswellasseverevenousinsuf-ficiency.Thereisnocureforlymphede-ma.However,CDTcanhelpreducetheswelling and maintain reduction, andsignificantlyimproveapatient’squalityof life. This comprehensive treatmentinvolvesthefollowingfoursteps:• manual lymph drainage• compressiontherapy(bandaging)• decongestiveexercises• skincare
Once the treated extremity/area isback to close to normal size or is nolonger reducing in size, the patient isfittedwithacompressiongarment.Pa-
tientsarealsotaughthowtoselfman-agetheirconditionaftertreatmenthasended.Attheendof6-8weeksofses-sions, we can expect a 60% decreasein the swelling,which facilitates func-tional activities for these patients. Inaddition, the lymphedema treatmentprogramforheadandneckpatientswillhelp them recover their ability to swal-lowandproducesaliva,voice,andROMoftheneck.Thesepatientsreceiveedu-cationregardingwarningsigns,decon-gestiveexercises,activitiesofdailylife,manual lymphaticdrainagewhenindi-cated, and education on donning anddoffing the appropriate compressiongarment. The overall goal is to improve apatient’squalityoflife.
Duringthis2018year,ourLymphede-ma Clinic has a total of six certifiedtherapists: Brian Reaksecker, PT CLT,Mary Matthews-Brownell, OTR-L CLT,MaureenMclain,PTCLTatALVA,andin SeattlewehaveMeg Sablinsky, PTCLT-LANA,MelissaSmith,PTACLT,andJenniferBoyce,OTR-L,CLT.

26
Whenpatients receivea cancerdiag-nosis they have many concerns about whatthediagnosismeans,whattoex-pect,detailsonmedicalcare,concernsfrom loved ones, finances, and sur-vival. Comprehending and organizing theprovidedinformationcanprovokeanxiety and be overwhelming while one is making important health caredecisions.TheroleoftheOncologySo-cialWorker(OSW)iscentraltohelpingpatients, caregivers and communitieswith detection, prevention, naviga-tionandsurvivalinarapidly-changingtreatment environment. OSWs areuniquelytrainedinaccessingresourc-es, recognizing disparities in care,communication,stressreduction,fam-ilysystems,advocacy,andcommunityresources,allowingtheOSWtoaffectpositivechangeinthelivesofVeteransandtheirfamilies.
Specifically,OSWsstrive toobtainac-curate and up-to-date educationalinformation and other resources forpatients.Thehopeisthatbycontact-ing patients early in the process andproviding them with verbal and writ-tenmaterial, thepatientswill have abetter understanding of what to ex-pect during their treatment and will alsobebetterprepared tocope. So-cialworkershavebeenactiveinpubliceducation campaigns including work-shops for veterans, conducting train-ingforstaffandcommunitypartners,andpublicmessageboards to informVeteransaboutcancerprevention,de-tectionandcare;aswellasVeterans’benefits and VA resources. The OSWparticipated on a panel to help edu-cateclinicalsocialworkersandhospi-
OncologySocialWorkAnaFisher,LICSW,OSW-C,MelindaWalker,LICSW, KimmyVanHayes,LICSW
talstaffonpalliativecareandhospiceservicesofferedthroughtheVAandtodiscussAdvanceCarePlanning.OSWswere involved in participated in ahospital wide event in March 2018 to help Veterans complete Advance Di-rectives. InSeptember2018,OSWfa-cilitatedthePsychosocial(socialwork-ers /psychologists) breakout sessionat theannualAssociationofVeteransAffairs Oncology/Hematology confer-enceinChicago,Illinoisandpresentedon Cancer Care Navigation: Address-ing Psychosocial Distress at the Asso-ciationofOncologySocialWorkersAn-nualconferenceinAtlanta,GeorgiainMay 2018.OSW andOSW Intern/Pa-tientAdvocateparticipatedinthePa-tientCenteredResearchCollaborativeGroupforPsychosocialOncologyfromMay2017toMay2018andattendedthe PCRC/Association of OncologySocial Workers Conference, Atlanta,GeorgiainMay2018.OSWwasnamedasaCo-Chairof theCommunicationsCommittee:PCRC.Additionally,OSWsprovide ongoing education to socialworkstudents through theUniversityofWashington School of SocialWork(UWSSW) practicum program, whichprovideshands-onexperience to stu-dents and to provide the University with input regarding Social Work inhealth care.
Support groups and educational of-ferings can be beneficial at all stagesofthecancerexperience.AtVAPugetSound, Social Workers co-facilitate asupport group for patient caregiverswho receive stem cell transplants as well as a general diagnosis support group for caregivers. OSW facilitate (Continued on next page)

27
the weekly Veteran cancer supportgrouponFridaysatnoonatSeattleVA.
Cancertreatmentmovespatientsintoa new awareness and self-image. Pa-tients and their loved ones may feelincapableofmanaging independentlyathome.OSWsarehighlyskilledatas-sessingpatients’andfamilies’resourc-esandreferringpatientstothelevelofcareappropriatefortheircurrentsitu-ationandneeds,includingcommunityoutpatient programs, home healthcare, skilled nursing or assisted livingfacilities, or hospice/palliative care.OSW assisted in the implementationoftheNCCNDistressThermometerforPatientsandisaddressingthepsycho-social needs of the Veterans at theirinitial radiation oncology and cancercare clinic visits.
OSWs participate asmembers of theinpatient consultation team in thepalliative and hospice care program.Socialworkers,alongwithother staffmembers,focusonthepatient’squal-ityof lifebyassistingwithend-of-lifeplanning,careresourcesandemotion-alsupport.Additionally,OSWsprovidethepatientand lovedoneswithgriefandbereavementsupportandreferraltoresourcesduringthistransition.So-cial workers participate in end-of-lifeeducationforstaffmembersandedu-cation for community partners aboutthe VA hospice and palliative careprogram,survivorbenefits,andburialbenefits.
OSWsareessentialinAdvanceCareDi-rective(ACD)planning,educationandcompletion. The Cancer Care Naviga-tionTeamOSWisparticipatinginedu-catinghospitalnurses,socialworkers,
psychologists and chaplains on how to improve goals of care conversationsanddocumentationregardinglifesus-taining treatment initiative. Socialworkersparticipateinahospital-wideinitiative to improve Veterans’ andstaffmembers’understandingoflivingwills, durable power of attorney, andtheroleofsurrogatedecisionmakers.Veterans are encouraged to complete health caredirectives to ensure theirongoing participation in their ownhealth care and to relieve stress forloved ones who are named as surro-gatedecisionmakers.
During the next year, OSWs at VAPugetSoundwillcontinuetoadvocateforVeteransinourcare,reducingbar-riers to care and increasing access to treatment whether through locatingappropriate transportation resourcesor finding financial resources to al-lowthemtokeeptheirappointments.
Social workers conduct quality train-ing forveterans,caregivers,staff,andcommunitymembersandwill contin-ue to train student interns at VA Puget Sound. Social Work will continue tohold trainings at community hospitals and institutions of higher educationto increase awareness of Veterans’benefits,programsanduniquehealthcare needs. With renewed emphasison survivorship, there are is now acancer survivorship clinic at VA Puget Sound.OSWswillcontinuetoworkonthecommitteeto improvethecancersurvivorship resources and pass that information to Veterans and medicalprofessionals at the hospital.WewillcontinuetoprovidecaregiverandVet-eran education and support groups.Theseeffortssupporttheoverallgoaltohelppatientsmaintaintheirqualityoflifewhiletheycopewithvariousis-sues that arise during cancer care.
Oncology Social Work (Continued)

28
TheChaplainServiceof theVAPugetSound Health Care System has been given the overall spiritual care of allVApatients.AmongourVeteransarethose that experience the diagnosis andtreatmentofcancer. Atthetimeofapatient’sdiagnosisandtreatmentprojection, Chaplaincy endeavors tosupport the patient and their familyas they progress through the various treatments,whetheritissurgery,che-motherapy, radiation, or a stem celltransplant. Spiritual support covers boththenegativeandpositiveaspectsofcancercaresuchastimesofwellnessandtimesofpalliativeintervention.
Chaplains are available with the treat-ment teams as various spiritual needs surfaceinthetreatmentprocess.Of-ten,alongwiththeconcernsoftreat-ment symptoms, comes uncertainty,anxiety, fear of treatment outcomes,guilt, and spiritual distress. Throughconsultsandvariouspatientcontacts,chaplainsgivespiritualsupportaffect-ingpatientandfamilymorale. Chap-lains have also been involved in the Tele-healthprogramwhichbringscareto patients in their home. Chaplainsare trained to work with patients ofanyfaith,ornone,withoutprejudice;chaplainsneverproselytize.
Spiritual CareChaplainGaryCowden,BCC
One aspect of care involves timeswhentreatmentoptionsbecome lim-ited.PalliativeCarechaplaincyaffordsopportunity to bring meaning and pur-pose to these times to help patientsand their families transition to a dif-ferentperspectiveontheir treatmentgoals. Chaplains have given consistent andpositivesupportthroughthispro-cess.Whenthelimitationsofscienceleadapatienttowardanotherdestiny,Chaplains are prepared to give spiri-tualsupportthroughtheseun-chartedexperiences to both the patient andthefamiliessurroundingthem.
Finally, Chaplains bring bereavementcare to patients and families in thejourneyoffinishing theirtimeof life.Memorial services are held annually forallpatientswhohavebeen in thehospitalattheirendoflife.Theirfami-lies are invited to attend as awayofcelebrating theirmemory. Each fam-ily is invited to attend and to bringpictures and memorabilia that helps share their memory with others. The Hospital Director and various staffmembers are invited to share the ex-perience.Familymembersareinvitedto share their loved ones experience. ManyofthestoriesofsupportbytheVA Hospital give overwhelming cred-ibility to the Cancer program .

1660S.ColumbianWaySeattle,WA98108Phone:206.764.2934Fax:206.764.2851
CREDITS
EditingConsultantsSudarshana Das
Graphic DesignAlisa Engeland
ArticleContributorsHarithaAvula,MBBSVictoriaCampa,MSAGaryK.Cowden,BCC,ChaplainSudarshanaDas,B.Com,RHIT,CTRWerkuDemisse,MSAJasonDominitz,MD,MHSAnaFisher,LICSWOSW-CAliceFoy,ARNP,CHPNGeorgeIoannou,MD,MSEmilyJohnson,MS,CCC-SLPTamarindKeating,ARNPLeilaKozak,PhDMicheleMeconi,ARNP,CDEBruceMontgomery,MDMichaelPorter,MD(CancerCommitteeChair)TonyQuang,MD,JDMargaretSablinsky,PT,DPT,CLT-LANALynsiSlind,RN,MNJulieTakasugiMDAdamTazi,PhDKimmyVanHayes,LICSWMelindaWalker,LICSWKentWallner,MDDanielWu,MD,PhDPeterWu,MD
Related Documents











