VOL 20, NO. 1, 1994 Can Estradiol Modulate Schizophrenic Symptomatology? 203 by Anita Rlecher-Rdasler, Heinz HSfner, Michael Stumbaum, Kurt Maurer, and Roland Schmidt Abstract Using epidemiologic data, in an earlier study we formulated the hypothesis that estrogens can de- lay the onset of schizophrenia in females by raising the vulner- ability threshold for this disease. In animal experiments, Hafner and colleagues found evidence that chronic estradiol treatment reduces the sensitivity of dopa- mine (D 2 ) receptors in the brain. In the clinical study presented in this article, as a further step we examined the antipsychotic properties of estradiol in human females by testing whether schiz- ophrenic symptomatology varies with estradiol serum levels throughout the menstrual cycle. We examined 32 acutely admitted female schizophrenia patients (Present State Examination/ CATEGO diagnosis, ICD-9) with a history of regular menstrual cycles, ages 18 to 43 (mean = 30.5), during their hospital stays (3-8 weeks), analyzing hormonal parameters and applying various rating scales for psychopathology every 7 days. In all patients, estradiol serum levels were markedly reduced as compared with the normal population, and fluctuations throughout the cycle were dampened. Nevertheless, a significant association emerged between estradiol levels, on the one hand, and psychopathology scores, on the other—that is, the psychiatric symptomatology as assessed by the clinical psychia- trist (Brief Psychiatric Rating Scale, p =6 0.01), behavior on the ward as assessed by the nursing staff (Nurses' Observa- tion Scale for Inpatient Evalua- tion p as 0.01), paranoid tenden- cies and general well-being as assessed by the patients them- selves (Paranoid-Depressivitats- Skala paranoid score p =£ 0.05; Befindlichkeits-Skala p =s 0.05). Psychopathology seems to im- prove when estradiol levels rise, and vice versa. These findings can be interpreted as further evi- dence for a protective effect of estrogens in schizophrenia, possi- bly due to the known anti- dopaminergic activities of these hormones. Schizophrenia Bulletin, 20(1): 203-214, 1994. The ABC study is an epidemio- logic investigation of schizophrenia with special emphasis on sex dif- ferences in this disease. We ex- amined different populations in the framework of this study and found that females, in comparison with males, not only had a de- layed peak for illness onset, but also exhibited an additional, smaller incidence peak after age 40-45. These peaks are also found using the earliest definition of onset (Hafner et al. 1989, 1991c, 1992). This result was interesting because, when planning our study, Hafner had put forward several psychosocial and biological hypoth- eses for explaining gender dif- ferences in schizophrenia. One hy- pothesis was "that the threshold of vulnerability for schizophrenia is higher in females than in males because of the modulating effect of estrogen on the dopamine activity" (Hafner 1987, p. 69). Assuming that genetically pre- disposed, vulnerable individuals fall ill as soon as (intrinsic or ex- trinsic) stress factors increase or Reprint requests should be sent to Dr. med. A. Riecher-Rossler, Central Institute of Mental Health, P.O. Box 12 21 20, 68072 Mannheim, Germany. by guest on June 1, 2015 http://schizophreniabulletin.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
VOL 20, NO. 1, 1994 Can Estradiol ModulateSchizophrenicSymptomatology?
203
by Anita Rlecher-Rdasler,Heinz HSfner, MichaelStumbaum, Kurt Maurer,and Roland Schmidt
Abstract
Using epidemiologic data, in anearlier study we formulated thehypothesis that estrogens can de-lay the onset of schizophrenia infemales by raising the vulner-ability threshold for this disease.In animal experiments, Hafnerand colleagues found evidencethat chronic estradiol treatmentreduces the sensitivity of dopa-mine (D2) receptors in the brain.
In the clinical study presentedin this article, as a further stepwe examined the antipsychoticproperties of estradiol in humanfemales by testing whether schiz-ophrenic symptomatology varieswith estradiol serum levelsthroughout the menstrual cycle.We examined 32 acutely admittedfemale schizophrenia patients(Present State Examination/CATEGO diagnosis, ICD-9) witha history of regular menstrualcycles, ages 18 to 43 (mean =30.5), during their hospital stays(3-8 weeks), analyzing hormonalparameters and applying variousrating scales for psychopathologyevery 7 days. In all patients,estradiol serum levels weremarkedly reduced as comparedwith the normal population, andfluctuations throughout the cyclewere dampened. Nevertheless, asignificant association emergedbetween estradiol levels, on theone hand, and psychopathologyscores, on the other—that is, thepsychiatric symptomatology asassessed by the clinical psychia-trist (Brief Psychiatric RatingScale, p =6 0.01), behavior onthe ward as assessed by thenursing staff (Nurses' Observa-tion Scale for Inpatient Evalua-tion p as 0.01), paranoid tenden-cies and general well-being asassessed by the patients them-
selves (Paranoid-Depressivitats-Skala paranoid score p =£ 0.05;Befindlichkeits-Skala p =s 0.05).Psychopathology seems to im-prove when estradiol levels rise,and vice versa. These findingscan be interpreted as further evi-dence for a protective effect ofestrogens in schizophrenia, possi-bly due to the known anti-dopaminergic activities of thesehormones.
Schizophrenia Bulletin, 20(1):203-214, 1994.
The ABC study is an epidemio-logic investigation of schizophreniawith special emphasis on sex dif-ferences in this disease. We ex-amined different populations in theframework of this study andfound that females, in comparisonwith males, not only had a de-layed peak for illness onset, butalso exhibited an additional,smaller incidence peak after age40-45. These peaks are also foundusing the earliest definition ofonset (Hafner et al. 1989, 1991c,1992). This result was interestingbecause, when planning our study,Hafner had put forward severalpsychosocial and biological hypoth-eses for explaining gender dif-ferences in schizophrenia. One hy-pothesis was "that the threshold ofvulnerability for schizophrenia ishigher in females than in malesbecause of the modulating effect ofestrogen on the dopamine activity"(Hafner 1987, p. 69).
Assuming that genetically pre-disposed, vulnerable individualsfall ill as soon as (intrinsic or ex-trinsic) stress factors increase or
Reprint requests should be sent toDr. med. A. Riecher-Rossler, CentralInstitute of Mental Health, P.O. Box12 21 20, 68072 Mannheim, Germany.
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
204 SCHIZOPHRENIA BULLETIN
(intrinsic or extrinsic) protectivefactors decrease, estrogens may beone such intrinsic protective factor.In this case, women would, tosome extent, be protected againstschizophrenia between puberty andmenopause by their high estrogenlevels. This difference might ex-plain the delayed and lower first-onset peak in females as comparedwith males. As the physiologicalestrogen production decreases inthe years before and during meno-pause, this protective factor wouldweaken considerably, which mightaccount for females' additionalpeak after age 40-45. Thus, ourepidemiologic data might well beexplained by the sex hormone hy-pothesis, which itself can be situ-ated within a long tradition.
Only recently have some authors(e.g., Seeman 1981, 1983; Hafner1987; Lewine 1988; Seeman andLang 1990; Hafner et al. 1991a,1991b, 1991c; Riecher et al. 1991;Riecher-Rossler and Hafner 1993)readdressed the estrogen hypothe-sis in association with schizo-phrenic psychoses, since there isnow increasing evidence for anantipsychotic effect of estrogens.The neuroendocrinologic basis forthis effect seems to be a modulat-ing effect of estrogens on thedopaminergic systems. One canfind the following conclusions inthe literature.
• The presence of estrogen re-ceptors in the limbic system indi-cates that estrogens not only playa part in the modulation of en-docrine functions but also have aneuromodulatory function (Hols-boer 1983; Lobo et al. 1984; Maggiand Perez 1985).
• Estrogens can reduce thedopamine (DA) concentration inthe striatum (Foreman and Porter1980; Dupont et al. 1981) and
modulate the sensitivity as wellas the number of DA receptors(Koller et al. 1980; Gordon andDiamond 1981; Bedard et al. 1984).
• In laboratory animals,estrogens can enhance neuroleptic-induced catalepsy (Gordon et al.1980; DiPaolo et al. 1981; Nicolettiet al. 1983) and reduce ampheta-mine- and apomorphine-inducedbehavior (stereotypies, etc.)(Gordon et al. 1980; Hruska andSilbergeld 1980).
• Qinically, there are case re-ports on women whose psychoticsymptomatology exacerbatesmainly premenstrually—that is,when estrogen levels drop (Endoet al. 1978; Glick and Stewart1980).
• During pregnancy, on theother hand, a time of extremelyhigh estrogen levels, chronic psy-chosis such as schizophrenia seemsto improve (Chang and Renshaw1986).
• After delivery, when estrogenlevels drop dramatically, an in-creased vulnerability for psychosesis observed (Nott 1982; Kendell etal. 1987).
• Female schizophrenia patientsbetween ages 20 and 40 requirelower doses of neuroleptics thanolder females or males of thesame age group (Seeman 1983).
• Estrogens show a positiveclinical effect in neuroleptic-induced dyskinesia, probably be-cause of their antidopaminergicproperties (Bedard et al. 1977;Villeneuve et al. 1980).
• Estrogens may have additionaleffects on other neurotransmittersystems, but these effects are notthe subject of this article.
Thus, the estrogen hypothesisnot only provides an excellent ex-planation for our epidemiologicdata, but is also based on nu-
merous findings of clinical andbasic research. Although there isno conclusive evidence for the in-crease of dopaminergic activity inthe brains of schizophrenia pa-tients (Gattaz et al. 1983; Carlsson1987), schizophrenic symptoms—atleast the productive ones—can besuccessfully treated and suppressedby substances blocking DA trans-mission in the brain. Estrogensmay therefore exert their positiveeffect in schizophrenia by theirantidopaminergic properties.
Hafner et al. (1991a, 1991b) fur-ther examined the neurohormonaleffects of estradiol by means ofanimal experiments. Concerningthe estrogen hypothesis, the resultsonly partly met expectations: Pro-longed estradiol administrationattenuated most of the behaviorinduced by DA agonists and an-tagonists. That this effect wasmore marked in newborn than inadult rats suggests a "structural"effect of physiologic estradiol con-centration on the dopaminergicsystem during brain development(Hafner et al. 1991a, 1991b). How-ever, there was also a "func-tional," though less marked, effectof estrogens in adult brains, indi-cated by a decrease in dopaminereceptor affinity for [3H]sulpiride.Together, those findings lead tothe assumption that estradioldownregulates the D2 receptors inthe brain (Hafner et al. 1991a,1991b; Gattaz et al. 1992).
Thus, starting with our epidemi-ologic findings and encouraged bythe results of the animal study, wetried to test the estrogen hypothe-sis in a clinical study. Since an in-tervention study with estrogenswas not justifiable at such an earlystage of research, we chose thefemale menstrual cycle as a "natu-ral experiment." Throughout the
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 20, NO. 1, 1994 205
menstrual cycle, the ovarian estra-diol production in fertile womenshows strong fluctuations directlymeasurable in the blood. More-over, estradiol has easy access tothe brain, and concentrations ofestradiol in plasma and cerebrospi-nal fluid are highly correlated(Backstrom et al. 1976).
The clinical study starts with thehypothesis that schizophrenicsymptomatology varies with themenstrual cycle—that is, thatsymptoms in women with schizo-phrenia are more likely to occuror be exacerbated at times of lowestrogen blood levels (premenstrualand menstrual phases) than atother phases of the cycle. In par-ticular the following hypothesiswas to be tested: The variation ofthe estradiol level during the men-strual cycle shows a negative cor-relation with the schizophrenicsymptomatology during an acuteepisode; that is, the patients'symptoms decrease when serumestradiol levels increase and viceversa.
Methods
Sample. All females with a clini-cal diagnosis of schizophrenia con-secutively admitted to PfalzklinikLandeck from June 1, 1988, toApril 30, 1989, were screened. In-clusion criteria were age range 18to 45; acute onset or relapse ofpsychosis and acute admission;regular menstrual cycles; no en-docrine disease or suspectedorganic brain syndrome; opera-tionalized diagnosis of schizophre-nia according to the InternationalClassification of Diseases (ICD-9;World Health Organization 1978),based on the Present State Ex-amination and the correspondingcomputer program CATEGO (Winget al. 1974). Of 54 patients who
fulfilled these criteria, 8 refused toparticipate, and another 14 werenot able to give informed consentor to participate because of severeillness; 32 patients could be in-cluded in the study.
The patients examined were onaverage 30.5 years old (standarddeviation [SD] = 6.5; range = 18-43). Nine were being admitted forthe first time. On average, firstpsychiatric hospitalization hadtaken place 2.5 years before thepresent admission. The patients'stated mean cycle length was 27.1days (range 23-32). The observedcycle length varied between 11and 66 days (average: 28.4 days).All but six patients had takenneuroleptics the week before hos-pitalization. Also, during their hos-pital stay they were treated withneuroleptics and other psychophar-macologic drugs by independentclinicians. Medication was docu-mented precisely. Five patients hadtaken hormonal contraceptives,which they had stopped in theweeks preceding admission.
Study Design. Each female wasexamined beginning with hospital-ization over at least one completemenstrual cycle. Psychopathologyand various hormone parameterswere evaluated on the day of ad-mission as well as on the 2nd,7th, 13th, 14th, 21st, and 28th daysof the menstrual cycle (i.e., at leastevery 7 days, with an additionalmidcycle measurement). The cycledays were fixed at first on thebasis of menstrual history but assoon as possible on the basis ofthe observed menstruation, whichvery often occurred with admis-sion. On the defined days, the fol-lowing measurements wereundertaken:
• Psychopathology: General psy-
chiatric symptomatology was as-sessed by the clinician using theBrief Psychiatric Rating Scale(BPRS; Overall and Gorham 1962).Patient's behavior was assessed bythe nursing staff using the Nurses'Observation Scale for InpatientEvaluation (NOSIE; Honigfeld etal. 1976). Paranoid and depressivetendencies as well as general well-being were assessed by the pa-tients themselves using the Para-noid-Depressivitats-Skala (PDS; vonZerssen and Koeller 1976) and theBefindlichkeits-Skala (BFS; vonZerssen and Koeller 1976). Men-strual history and psychopathologywere assessed in the same patientindependently, and the doctor andthe nurse assessing psychopathol-ogy were blind to the patient's cy-cle. The patients were not awarethat their menstrual cycles werebeing correlated to symptoms.
• Laboratory: On each assess-ment day estradiol and progester-one were measured, and on thesecond day of menstruation pro-lactin and testosterone were alsomeasured. Blood was taken in astandardized manner every morn-ing before medication; serum waskept frozen at -40 °C. Once all ex-aminations in the 32 patients werefinished, all laboratory analyseswere carried out in a single batchto avoid methodologic variation.Immunoassays were used.
Statistical Procedures. To deter-mine the association betweenestradiol blood levels and psycho-pathology scores during the hospi-tal stay, cross-correlations (Jenkinsand Watts 1968) were calculated.The CTOSS-correlation function iswell established in electroen-cephalographic analysis and inengineering as a measure of sim-ilarity between two curves. Foreach individual we calculated
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
206 SCHIZOPHRENIA BULLETIN
cross-correlations between theestradiol curve and the curves ofthe different psychopathologyscores. In this case, the correlationcoefficients are parameters for thesimilarity between the estradiolcurve and the five total scorecurves of the different rating scalesin each individual. Subsequently,Wilcoxon tests were calculatedover the group as a whole to de-termine the significance of theassociations.
Results
Hormonal Status.Normal values. To allow com-
parisons, the normal values of thehormones analyzed will be givenfirst. They were established in the
Institute of Clinical Chemistry ofthe University of Mannheim/Heidelberg, where the analysesfor our study were undertaken aswell, and refer to large samples ofhealthy, fertile women:
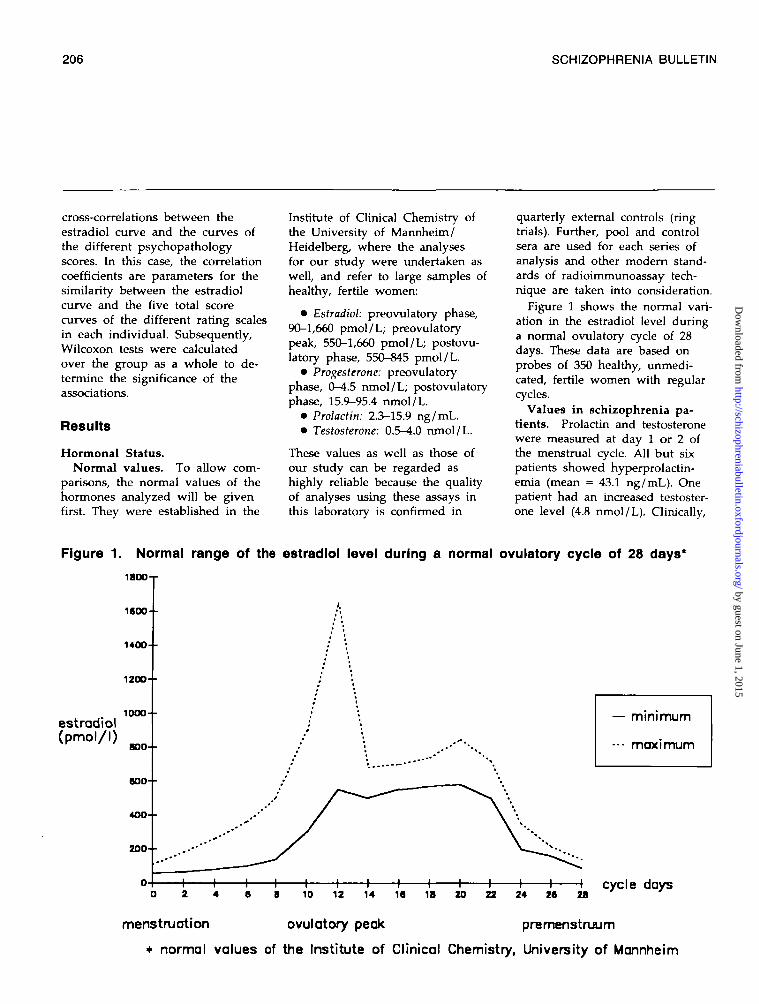
• Estradiol: preovulatory phase,90-1,660 pmol/L; preovulatorypeak, 550-1,660 pmol/L; postovu-latory phase, 550-845 pmol/L.
• Progesterone: preovulatoryphase, 0-4.5 nmol/L; postovulatoryphase, 15.9-95.4 nmol/L.
• Prolactin: 2.3-15.9 ng/mL.• Testosterone: 0.5-4.0 nmol/L.
These values as well as those ofour study can be regarded ashighly reliable because the qualityof analyses using these assays inthis laboratory is confirmed in
quarterly external controls (ringtrials). Further, pool and controlsera are used for each series ofanalysis and other modem stand-ards of radioimmunoassay tech-nique are taken into consideration.
Figure 1 shows the normal vari-ation in the estradiol level duringa normal ovulatory cycle of 28days. These data are based onprobes of 350 healthy, unmedi-cated, fertile women with regularcycles.
Values in schizophrenia pa-tients. Prolactin and testosteronewere measured at day 1 or 2 ofthe menstrual cycle. All but sixpatients showed hyperprolactin-emia (mean = 43.1 ng/mL). Onepatient had an increased testoster-one level (4.8 nmol/L). Clinically,
Figure 1. Normal range of the estradlol level during a normal ovulatory cycle of 28 days*
iBOO-r
1600--
1400- •
1200- •
10OO- -estradiol(pmol/l)
BOO- •
600- •
4OO- •
200- -
— minimum
••• maximum
• + • H h H 1 1 1 1 1 1 h10 12 14 16 IB 20 22 24 26 28
cycle days
menstruation ovulatory peak premenstruum
• normal values of the Institute of Clinical Chemistry, University of Mannheim
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL 20, NO. 1, 1994 207
she showed no signs of viriliza-tion. All the other patients hadnormal testosterone levels (mean =1.8 nmol/L).
In only two patients the pro-gesterone values at admission(mean = 4.3 nmol/L) exceeded15.9 nmol/L, indicating a postovu-latory phase. The estradiol valuesat admission ranged from 45 to502 pmol/L (mean - 176.5 pmol/L), clearly within the lower part ofthe cycle-dependent normal range.No patient showed values over550 pmol/L, which would indicatenormal follicular maturation withovulation.
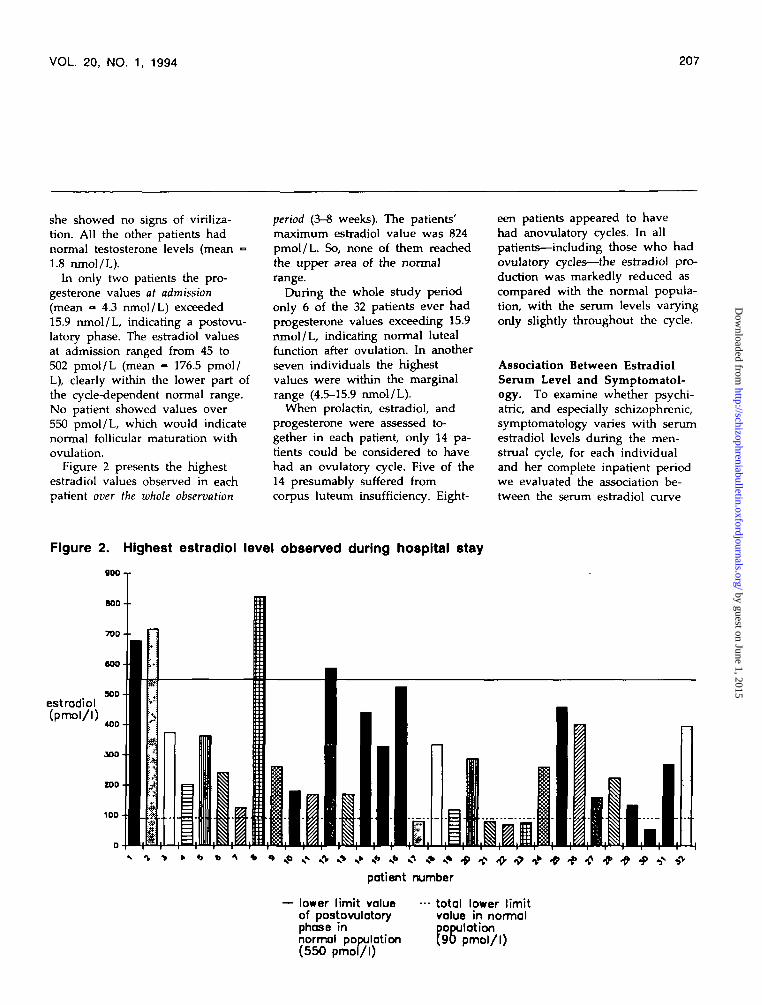
Figure 2 presents the highestestradiol values observed in eachpatient over the whole observation
period (3-8 weeks). The patients'maximum estradiol value was 824pmol/L. So, none of them reachedthe upper area of the normalrange.
During the whole study periodonly 6 of the 32 patients ever hadprogesterone values exceeding 15.9nmol/L, indicating normal lutealfunction after ovulation. In anotherseven individuals the highestvalues were within the marginalrange (4.5-15.9 nmol/L).
When prolactin, estradiol, andprogesterone were assessed to-gether in each patient, only 14 pa-tients could be considered to havehad an ovulatory cycle. Five of the14 presumably suffered fromcorpus luteum insufficiency. Eight-
een patients appeared to havehad anovulatory cycles. In allpatients—including those who hadovulatory cycles—the estradiol pro-duction was markedly reduced ascompared with the normal popula-tion, with the serum levels varyingonly slightly throughout the cycle.
Association Between EstradiolSerum Level and Symptomatol-ogy. To examine whether psychi-atric, and especially schizophrenic,symptomatology varies with serumestradiol levels during the men-strual cycle, for each individualand her complete inpatient periodwe evaluated the association be-tween the serum estradiol curve
Figure 2. Highest estradiol level observed during hospital stay
goo- -
BOO- -
700- •
estradiol(pmol/l)
900
40D
ZOO
100
patient number
lower limit valueof postovulatoryphase innormal population(550 pmol/l)
total lower limitvalue in normalpopulation(90 pmol/l)
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
208 SCHIZOPHRENIA BULLETIN
and the different curves of specificand unspecific psychopathology.As was outlined in the methodssection, we calculated cross-correlations between the individualcurves of each woman separately.We thus got five association pa-rameters per woman: estradiol cor-related with each of BPRS, NOSIE,BFS, PDS paranoid score, and PDSdepression score. The associationparameters vary between women.Table 1 shows for each associationparameter the mean value and SDfor the 32 women. The meanvalues are all negative, except forNOSIE, whose higher value, incontrast to the other scales, meansless pathology. And all meanvalues (except that for depression)deviate significantly from zero(one-sided Wilcoxon test).
Thus, symptomatology seems toimprove when estradiol levels rise,and vice versa. This is true forpsychiatric symptomatology (BPRS)as assessed by the clinical psychia-trist, for the general behavior onward as assessed by the nursingstaff (NOSIE), and for the areas"paranoid tendencies" (PDS para-noid score) and "general well-
being" (BFS), both of which areassessed by the patientsthemselves.
An analysis of the BPRS sub-scores pointed in the same direc-tion. There was an inverse asso-ciation for all subscores except"anxiety/depression": thoughtdisturbance, p =» 0.01; activation,p =£ 0.01; anergia, p < 0.10; andhostile-suspiciousness, p < 0.10.As "thought disturbance" is a sub-score with mainly psychotic items,this result indicates that estradiollevels are inversely associated notonly with general psychiatricsymptomatology, but also, espe-cially strongly, with psychoticsymptoms.
As we have shown, our patients'estradiol levels were very low andshowed only slight cyclical varia-tions. And when a parametervaries only a little, it is difficult toidentify associations with other pa-rameters. Nevertheless, these in-verse associations could be seen.Only for the patients' self-assessedchange in depressiveness was theassociation with estradiol not sig-nificant, a finding that agrees withthe hypothetic neuroleptic-like
Table 1. Means of individual correlation coefficients betweenestradiol curves and psychopathology (n = 32)
BPRS, total scoreNOSIE, total score1
BFS, total scorePDS, paranoid scorePDS, depression score
Mean (SD)
-0.25 (0.41)0.25 (0.49)
-0.20 (0.43)-0.17 (0.42)-0.10 (0.52)
P0.0020.0040.0320.0290.277 (NS)
Note.—SD = standard deviation; BPRS = Brief Psychiatric Rating Scale (Overall and Gorham1962), NOSIE = Nurses' Observation Scale lor Inpatienl Evaluation (Honigfeld et al 1976);BFS = Befindlichkeits-Skala and PDS = ParanokJ-Depresslvttats-Skala (von Zerssen andKoeller 1976); NS = not significant.
'Unlike the other scores, In the total NOSIE score a higher value means lesspsychopathology.
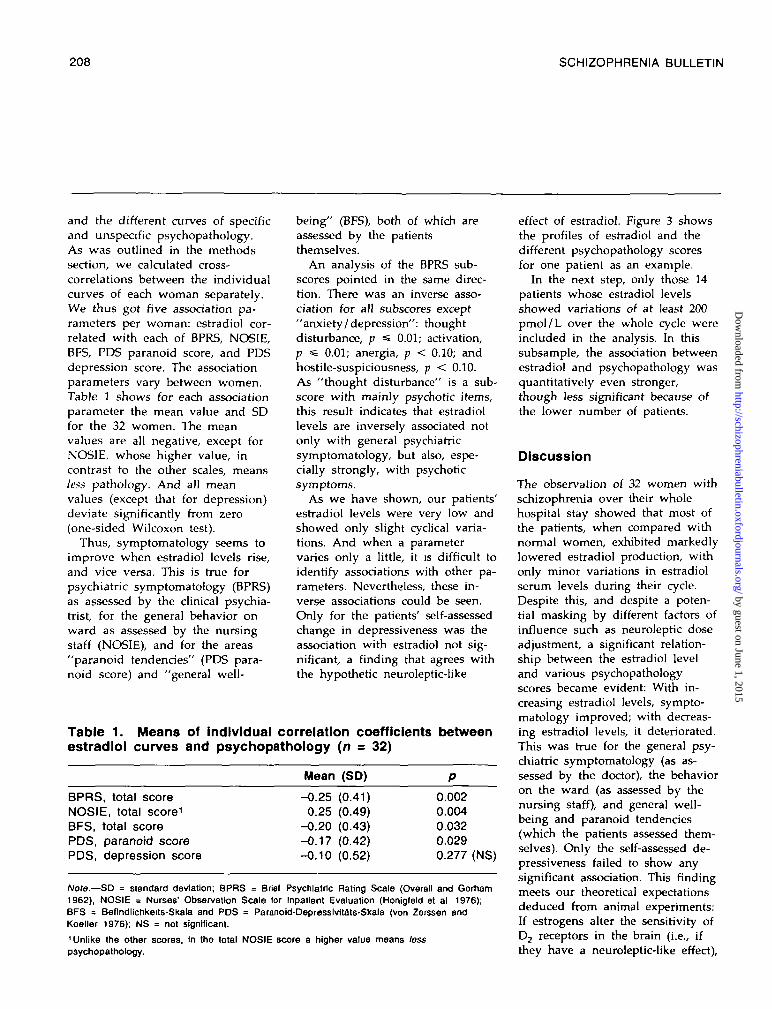
effect of estradiol. Figure 3 showsthe profiles of estradiol and thedifferent psychopathology scoresfor one patient as an example.
In the next step, only those 14patients whose estradiol levelsshowed variations of at least 200pmol/L over the whole cycle wereincluded in the analysis. In thissubsample, the association betweenestradiol and psychopathology wasquantitatively even stronger,though less significant because ofthe lower number of patients.
Discussion
The observation of 32 women withschizophrenia over their wholehospital stay showed that most ofthe patients, when compared withnormal women, exhibited markedlylowered estradiol production, withonly minor variations in estradiolserum levels during their cycle.Despite this, and despite a poten-tial masking by different factors ofinfluence such as neuroleptic doseadjustment, a significant relation-ship between the estradiol leveland various psychopathologyscores became evident: With in-creasing estradiol levels, sympto-matology improved; with decreas-ing estradiol levels, it deteriorated.This was true for the general psy-chiatric symptomatology (as as-sessed by the doctor), the behavioron the ward (as assessed by thenursing staff), and general well-being and paranoid tendencies(which the patients assessed them-selves). Only the self-assessed de-pressiveness failed to show anysignificant association. This findingmeets our theoretical expectationsdeduced from animal experiments:If estrogens alter the sensitivity ofD2 receptors in the brain (i.e., ifthey have a neuroleptic-like effect),
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL. 20, NO. 1, 1994 209
Figure 3. Course of estradiol serum level and different psychopathology scores duringhospital stay—Example of one patient
ESTBEFIND700
600 -
500
BPRSNOSIEPARAN
60
admission
EST = estradiol serum level [pmol /1]BEFIND = Beflndllchkeits-Skala - total score x 10
BPRS = BPRS-total score x 0,5 ^NOSIE = NOSIE total score x 0,2 1),2)
- - - PARAN = Paranoidscore of PDS
1) The higher the different psychopathology scores, the more severely disturbedis the patient. The NOSIE - Index curve had to be mirrored for this purpose.
2) Some scores had to be multiplied by a factor in order to fit them Into one diagram.
Note.—Some scores had to be multiplied by a factor to fit them into one diagram. The higher the different psychopathology scores, the moreseverely disturbed Is the patient. The NOSIE curve had to be mirrored for this purpose.
an antidepressive effect is not nec-essarily to be expected.
Our findings raise various ques-tions. First, it is of interest toknow the strength of the effect.The correlation coefficients used asa measure of association betweenthe estradiol and the psychopathol-ogy profiles are on average notvery high, but they deviate signifi-cantly from zero. Here, one has tobear in mind that our patients'
estradiol levels showed only minorvariations. And if despite onlyminor variations of one parameter,there is a significant relationshipto other parameters, this relation-ship must be a clear one. Also,the effects were quantitativelystronger in the subgroup ofwomen whose estradiol variationswere more marked; that the effectswere not more significant in thissubgroup is probably because of
the small number of patients. Ourresults therefore seem to indicatethat the influence of estrogens isnot negligible. A larger group ofpatients should be studied, though.
Further questions concern thespecificity of our results:
• The specificity of estradiol as aninfluencing factor: Is it reallyestradiol that accounts for the vari-ations of symptomatology, and notother factors?
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

210 SCHIZOPHRENIA BULLETIN
• The specificity of the dependentfactor (i.e., psychopathology): (1) Is itonly the symptomatology of schiz-ophrenia that is subject toestradiol-dependent variations, oris it also the mental state in otherdiseases and in the healthy? (2) Inschizophrenia patients, is it onlythe nonspecific symptoms, or alsothe specific, psychotic symptomsthat are influenced by estradiol?
Regarding the first question, itcannot be ruled out that the asso-ciation between estradiol level andsymptomatology is due to other,covarying factors. Among thosefactors the most important may beneuroleptics, the dosage of whichdepends in part on the sympto-matology. Neuroleptics couldtheoretically suppress the ovarianestradiol production through hy-perprolactinemia. The fact, how-ever, that long-term hyperprolac-tinemia can suppress ovarianestradiol production is known onlyfrom inquiries into hyperprolac-tinemia of other etiology (Diedrichand Wildt 1990). As to a potentialinfluence of neuroleptics on estro-gens, most studies have been per-formed before the advent of radio-immunoassays. Findings were ofteninconsistent and contradictory (forreviews see Shader and Di Mascio1970; Beumont and Bergen 1982).Beumont et al. (1974a, 19746) usingradioimmunoassay in a longitudi-nal study of psychiatric inpatientsreceiving neuroleptics foundestrogen levels to be in the normalrange in premenopausal womenwithout amenorrhea as well as inposrmenopausal women. Even inpremenopausal women with amen-orrhea, estrogen values were inthe normal range for the follicularphase of the cycle. For schizophre-nia, Prentice and Deakin (1992) re-cently showed that there is no dif-
ference between patients with andwithout menstrual irregularities intotal neuroleptic dosage or serumprolactin concentration. These find-ings speak against neurolepticsbeing the major determining influ-ence on menstrual irregularitiesand on estradiol production. In acomprehensive review on long-term effects of neuroleptic drugs,Meltzer (1985) stated: "[similar]difficulty in attributing sexual dys-function such as amenorrhea, orabnormalities in sex hormoneserum levels in female schizo-phrenics to neuroleptic treatmentrather than to the illness per se[also exists]" (p. 60).
In our own study we could findno association between neurolepticsand estradiol serum levels, eitherinterindividual or intraindividual.Among individuals, there was nocorrelation between mean neuro-leptic dosage (in chlorpromazineequivalents) and mean estradiollevel during hospital stay (r =-0.14; p - NS). The average neuro-leptic dose during hospital staywas about the same for patientswith and without ovulation (815.3and 757.5 chlorpromazine equiva-lents; p = NS, t test). Nor did test-ing intraindividuaUy by calculatingcross-correlations between neuro-leptic dosage and estradiol curvesreveal any significant association.These facts speak against a directinfluence of neuroleptics on theestradiol serum level.
Apart from that, it is not to beexpected that a complex chain ofreactions like symptom deteriora-tion leading to increase of neuro-leptic dose leading to increase ofprolactin blood levels leading todecrease of estrogen blood levelswould go on without a time lag.Therefore, the direct temporal asso-ciation between estradiol level and
symptomatology shown in table 1also speaks against causation bysuch an intermediate factor. Thus,it seems unlikely that the inverseassociation between estradiol andsymptomatology is mediatedthrough neuroleptics.
As to the specificity of estra-diol's effects for schizophrenia,there is also evidence for cycle-dependent variations of well-beingin many healthy women, knownas premenstrual syndrome. The re-lationship between this syndromeand the estradiol level has beendiscussed but not yet proved. Re-sults from the large number ofstudies are very inconsistent interms of etiology (Rubinow andRoy-Byrne 1984). We do not knowof any corresponding studies forthe mentally ill that include directmeasurement of estradiol levels.
Finally, we could show in ourschizophrenia patients that notonly are unspecific symptoms andgeneral behavior associated withcyclical variations of estradiol, butpsychotic symptoms and paranoidtendencies are also related. Inschizophrenia patients, estradiolseems to have clear antipsychoticproperties in addition to a generalstabilizing effect.
Another important point to dis-cuss is that we observed a markedexcess of admissions during thelow-estrogen phase of the cycle. Infact, 16 of 28 patients in whomwe could exactly determine the cy-cle phases were admitted in thelow-estrogen third of their cycle,defined as the third of the cyclestarting 3 days before menstruationonset (p =s 0.01). Therefore thequestion arose whether this over-representation could account forthe correlations found. However,this would only be a problem ifall patients had the same cycle
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 20, NO. 1, 1994 211
length and the same duration oftreatment until symptom improve-ment, which was not the case:Symptom improvement took 3 to8 weeks (observation period), andthe cycle lengths of the 32 patientsincluded in the analysis varied be-tween 11 and 66 days. Thus, withmaximum symptom improvementat the end of their hospital staythe patients were in different cyclephases and had different estradiollevels.
A secondary finding of ourstudy also requires some explana-tion. Many female schizophreniapatients exhibited considerablecyclical disturbances; for that rea-son several patients acutely admit-ted during the study period failedto qualify for our study. Most ofthe examined patients appeared tohave reduced estradiol levels com-pared with normal females, and insome of them these low levelswere obviously linked withanovulatory cycles. As we havediscussed above, this might not bedue to neuroleptic treatment only.Furthermore, the fact that "hypo-estrogenism" in women with schiz-ophrenia was observed before thediscovery of neuroleptics (e.g.,Kretschmer 1921/1967; Bleuler1943) implies that those disturb-ances may be a primary part ofthe schizophrenia process. Ourstudy was not designed to testthis question, and we may havemissed higher hormone values be-cause of infrequent measurements.But in our opinion there areenough indications of hypoesrro-genism in schizophrenia patients tojustify further investigations (forreview see Riecher-Rossler andHafner 1993).
Provided our results are con-firmed by replication, they may berelevant to research as well as tothe clinic. First, our findings fur-
ther confirm the hypothesis pro-posed by Hafner (1987) to explaingender differences in age at onsetin schizophrenia: Women pre-disposed to schizophrenia wouldbe particularly protected from theonset between puberty and(pre-)menopause, when their phys-iological ovarian estrogen produc-tion is high. In some women theillness onset would be delayedeven until menopause, when pro-tection by estrogens disappears.
Moreover, our results show thatthe protective effect of estradiol infertile women varies not only overthe female life cycle, but also overthe menstrual cycle; that is, if thedisease occurs, it occurs mostly inthe phase when estradiol levels arelow. And during an episode, psy-chopathology varies with serumestradiol levels throughout themenstrual cycle.
The mechanism of this effectseems to be similar to that of ma-jor tranquilizers, since apart froma general stabilization, an antipsy-chotic effect can also be observed.Thus, our clinical study can be re-garded as a confirmation of thefindings from our animal experi-ments, which indicated that estra-diol can have a neuroleptic-likeeffect by altering the sensitivityof D2 receptors in the brain. Thestudy goes beyond the animal ex-periments in that it also suggestseffects of estradiol in humans. Andit goes beyond our epidemiologicresults, which only indicated aninfluence of estrogens on age atonset and thus on the vulnerabilitythreshold for the outbreak of thedisease: The study on the men-strual cycle also demonstrates a di-rect influence of estradiol on theintensity of the symptomatology.
Last but not least, our resultsmay have clinical relevance fortherapy and relapse prevention.
First, in treating young womenwith schizophrenia, one could ad-just the neuroleptic dose to themenstrual cycle to give higherdoses during perimenstruum andlower doses intennenstruaJly. Thus,perimenstrual exacerbations mightbe avoided; at least, the overallneuroleptic dose could be lowerand yet have the same therapeuticand relapse-preventing effect,which would have the advantageof fewer side effects. This ap-proach could be especially worth-while in the subgroup of womenwith a perimenstrual excess ofrelapses.
Second, menopausal and post-menopausal women could undergoa hormonal substitution treatment,similar to the one used againstosteoporosis. Here, one has to bearin mind that estrogen levels beginto fall years before the last men-struation. Corresponding interven-tion studies should be carried outin the next step. In the long run,such a "cycle-modulated" neuro-leptic dosage in fertile women onthe one hand, and "adjuvant" es-trogen therapy in women beforeand after menopause, on the other,could—at least in women—have apositive influence on the course ofschizophrenic disorders.
References
Backstrom, T.; Carstensen, H.; andSodergard, R. Concentration ofestradiol, testosterone and pro-gesterone in cerebrospinal fluidcompared to plasma unbound andtotal concentrations, journal ofSteroid Biochemistry, 7:469-472,1976.Beumont, P.J.V., and Bergen, J.Neuroendocrine effects of neuro-leptics. In: Beumont, P.J.V., andBurrows, G., eds. Handbook of Psy-
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
212 SCHIZOPHRENIA BULLETIN
chiatry and Endocrinology. Amster-dam, The Netherlands: Elsevier,1982. pp. 157-181.Beumont, P.J.V.; Corker, C.S.;Friesen, H.G.; Kolakowska, T.;Mandelbrote, B.M.; Marshall, J.;Murray, M.A.F.; and Wiles, D.H.The effects of phenothiazines onendocrine function: II. Effects inmen and postmenopausal women.British Journal of Psychiatry,124:420-430, 1974a.Beumont, P.J.V.; Gelder, M.G.;Friesen, H.G.; Harris, G.W.; Mac-Kinnon, P.C.B.; Mandelbrote, B.M.;and Wiles, D.H. The effects ofphenothiazines on endocrine func-tion: I. Patients with inappropriatelactation and amenorrhoea. BritishJournal of Psychiatry, 124:413-419,1974i>.
Bedard, P.; Boucher, R.; Daigle, M.;and DiPaolo, T. Similar effect ofestradiol and haloperidol on ex-perimental tardive dyskinesia inmonkeys. Psychoneuroendocrinology,9:375-379, 1984.
Bedard, P.; Langelier, P.; andVilleneuve, A. Estrogens and theextrapyramidal system. Lancet,11:1367-1368, 1977.
Bleuler, M. Die spatschizophrenenKrankheitsbilder. Fortschritte derNeurologie und Psychiatric, 9:259-290, 1943.Carlsson, A. The dopamine hy-pothesis of schizophrenia 20 yearslater. In: Hafner, H.; Gattaz, W.F.;and Janzarik, W., eds. Search forthe Causes of Schizophrenia. Vol. I.Berlin, West Germany: SpringerVerlag, 1987. pp. 223-235.
Chang, S.S., and Renshaw, D.C.Psychosis and pregnancy. Com-prehensive Therapy, 12:36-^1, 1986.
Diedrich, K., and Wildt, L. NeueWege in Diagnostic und Therapieder Sterilitdt. Stuttgart, West Ger-many: Enke Verlag, 1990.
DiPaolo, T.; Payet, P.; and Labrie,F. Effect of chronic estradiol andhaloperidol treatment on striataldopamine receptors. European Jour-nal of Pharmacology, 73:105-106,1981.
Dupont, A.; DiPaolo, T.; Gagne, B.;and Barden, N. Effects of chronicestrogen treatment on dopamineconcentrations and turnover in dis-crete brain nuclei of ovariec-tomized rats. Neuroscience Letters,22:69-74, 1981.
Endo, M.; Daiguji, M.; Asano, Y.;Yamashita, I.; and Takahashi, S.Periodic psychosis recurring in as-sociation with menstrual cycle.Journal of Clinical Psychiatry,39:456-466, 1978.
Foreman, M.M., and Porter, J.C.Effects of catechol estrogens andcatecholamines on hypothalamicand corpus striatal tyrosine hy-droxylase activity. Journal of Neuro-chemistry, 34:1175-1183, 1980.
Gattaz, W.F.; Behrens, S.; de Vry,J.; and Hafner, H. Ostradiolhemmt Dopaminvermittelte Ver-haltensweisen bei Ratten: Ein Tier-modell zur Untersuchung dergeschlechtsspezifischen Unter-schiede bei der Schizophrenie.Fortschritte der Neurologie und Psy-chiatrie, 60:1-44, 1992.
Gattaz, W.F.; Riederer, P.; Rey-nolds, D.; and Beckmann, H.Dopamine and noradrenalin in thecerebrospinal fluid of schizophrenicpatients. Psychiatry Research, 8:243-250, 1983.
Glide, J., and Stewart, D. A newdrug treatment for premenstrualexacerbation of schizophrenia.Comprehensive Psychiatry, 21:281-287, 1980.
Gordon, J.H.; Borison, R.L.; andDiamond, B.I. Modulation ofdopamine receptor sensitivity by
estrogen. Biological Psychiatry,15:389-396, 1980.
Gordon, J.H., and Diamond, B.I.Antagonism of dopamine supersen-sitivity by estrogen: Neurochemicalstudies in an animal model of tar-dive dyskinesia. Biological Psychia-try, 16:365-371, 1981.
Hafner, H. Epidemiology of schizo-phrenia. In: Hafner, H.; Gattaz,W.F.; and Janzarik, W., eds. Searchfor the Causes of Schizophrenia. Vol.I. Berlin, West Germany: SpringerVerlag, 1987. pp. 47-74.
Hafner, H.; Behrens, S.; de Vry, J.;and Gattaz, W.F. An animal modelfor the effects of estradiol ondopamine-mediated behavior: Im-plications for sex differences inschizophrenia. Psychiatry Research,38:125-134, 1991a.
Hafner, H.; Behrens, S.; de Vry, J.;Gattaz, W.F.; Loffler, W.; Maurer,K.; and Riecher-Rossler, A. Warumerkranken Frauen spater anSchizophrenie? Erhohung der Vul-nerabilitatsschwelle durch Ostro-gen. Nervenheilkunde, 10:154-163,1991b.
Hafner, H.; Riecher-Rossler, A.;Maurer, K.; Fatkenheuer, B.; andLoffler, W. First onset and earlysymptomatology of schizophrenia.European Archives of Psychiatry andClinical Neuroscience, 242:109-118,1992.
Hafner, H.; Riecher-Rossler, A.;Hambrecht, M.; Maurer, K.;Meissner, S.; Schmidtke, A.;Fatkenheuer, B.; Loffler, W.; andan der Heiden, W. Geschlechts-unterschiede bei schizophrenenErkrankungen. Fortschritte derNeurologie und Psychiatrie, 59:343-360, 1991c.
Hafner, H.; Riecher, A.; Maurer,K.; Loffler, W.; Munk-Jorgensen, P.;and Stromgren, E. How does gen-
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
VOL. 20, NO. 1, 1994 213
der influence age at first hospital-ization for schizophrenia? Psycho-logical Medicine, 19:903-918, 1989.
Holsboer, F. Hormones. In: Hip-pius, H., and Winokur, G., eds.Psychopharmacology. Amsterdam,The Netherlands: Elsevier, 1983.pp. 144-161.
Honigfeld, G.; Gillis, R.D.; andKlett, C.J. NOSIE: Nurses' Obser-vation Scale for Inpatient Evalua-Hon. In: Guy, W., ed. ECDEUAssessment Manual for Psychophar-macology. Rockville, MD: NationalInstitute of Mental Health, 1976.pp. 265-273.
Hruska, R.E., and Silbergeld, E.K.Estrogen treatment enhances dopa-mine receptor sensitivity in the ratstriarum. European Journal ofPharmacology, 61:397-100, 1980.
Jenkins, G.M., and Watts, D.G.Spectral Analysis and Its Applica-tions. Oakland, CA: Holden Day,1968.
Kendell, R.E.; Chalmers, J.C.; andPlatz, C. Epidemiology of puer-peral psychoses. British Journal ofPsychiatry, 150:662-673, 1987.
Koller, W.C.; Weiner, W.J.;Klawans, H.L.; and Nausieda, P.A.Influence of female sex hormoneson neuroleptic-induced behavioralsupersensitivity. Neuropharmacology,19:387-391, 1980.
Kretschmer, E. Korperbau undCharakter. Untersuchungen zumKonstitutionsproblem und zur Lehrevon den Temperamenten. 25th ed.(1921) Berlin, West Germany:Springer Verlag, 1967.
Lewine, R.R.J. Gender and schizo-phrenia. In: Nasrallah, H.A., ed.Handbook of Schizophrenia. Vol. III.New York, NY: Elsevier, 1988.pp. 121-136.
Lobo, R.A.; Shoupe, D.; Roy, S.;and Paul, W. Central and periph-
eral metabolites of norepinephrineand dopamine in postmenopausalwomen. American Journal of Obstet-rics and Gynecology, 5:548-552,1984.
Maggi, A., and Perez, J. Mini-review: Role of female gonadalhormones in the CNS; Clinical andexperimental aspects. Life Sciences,37:893-906, 1985.Meltzer, H.Y. Long-term effects ofneuroleptic drugs on the neuroen-docrine system. In: Kemali, D., andRacagni, G., eds. Chronic Treat-ments in Neuropsychiatry: Advancesin Biochemical Psychopharmacology.New York, NY: Raven Press, 1985.pp. 59-68.
Nicoletti, F.; Ferrara, N.; Parti, F.;Viglianesi, M.; Rampello, L.;Bianchi, A.; Reggio, A.; andScapagnini, U. Influence of sexsteroids and prolactin on halo-peridol-induced catalepsy. BrainResearch, 279:352-358, 1983.
Nott, P.N. Psychiatric illness fol-lowing childbirth in Southampton:A case register study. PsychologicalMedicine, 12:557-561, 1982.
Overall, J.E., and Gorham, D.R.The Brief Psychiatric Rating Scale.Psychological Reports, 10:799-812,1962.
Prentice, D.S., and Deakin, J.F.W.Role of neuroleptic drugs andorganic mechanism in the aetiologyof menstrual irregularities inwomen. [Abstract] SchizophreniaResearch, 6:114, 1992.
Riecher, A.; Maurer, K.; Loffler,W.; Fatkenheuer, B.; an derHeiden, W.; Munk-Jergensen, P.;Stromgren, E.; and Hafner, H. Sexdifferences in age at onset andcourse of schizophrenic disorders—A contribution to the understand-ing of the disease? In: Hafner, H.,and Gartaz, W.F., eds. Search forthe Causes of Schizophrenia. Vol. II.
Berlin, Germany: Springer Verlag,1991. pp. 14-33.
Riecher-Rossler, A., and Hafner, H.Schizophrenia and oestrogens—Isthere an association? European Ar-chives of Psychiatry and ClinicalNeuroscience, 242:323-328, 1993.
Rubinow, D.R., and Roy-Byrne, P.Premenstrual syndromes: Overviewfrom a methodologic perspective.American Journal of Psychiatry,141:163-172, 1984.
Seeman, M.V. Gender and theonset of schizophrenia: Neuro-humoral influences. PsychiatricJournal of the University of Ottawa,6:136-138, 1981.
Seeman, M.V. Interaction of sex,age, and neuroleptic dose. Com-prehensive Psychiatry, 24:125-128,1983.
Seeman, M.V., and Lang, M. Therole of estrogens in schizophreniagender differences. SchizophreniaBulletin, 16:185-194, 1990.
Shader, R.I., and Di Mascio, A.Psychotropic Drug Side Effects. Bal-timore, MD: Williams & WilkinsCompany, 1970.
Villeneuve, A.; Cazejust, T.; andCote, M. Estrogens in tardive dys-kinesia in male psychiatric pa-tients. Neuropsychobiology, 6:145-151, 1980.
von Zerssen, D., and Koeller, D.M.Klinische Selbstbeurteilungs-Skalen(KSb-Si) aus dem Munchener Psy-chiatrischen Informations-System(PSYCHIS Munchen) (Manual).Weinheim, West Germany: Beltz,1976.
Wing, J.K.; Cooper, J.E.; and Sar-torius, N. The Description and Clas-sification of Psychiatric Symptoms:An Instructional Manual for PSEand CATEGO. London, England:Cambridge University Press, 1974.
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
214 SCHIZOPHRENIA BULLETIN
World Health Organization. MentalDisorders: Glossary and Guide toTheir Classification in AccordanceWith the Ninth Revision of the In-ternational Classification of Diseases.Geneva, Switzerland: The Organi-zation, 1978.
Acknowledgments
This study was funded by theFederal Ministry for Research andTechnology under No. 07-016370.The authors are grateful to Prof.Dr. Steinberg, Director of the StateMental Hospital, Landeck, for hissupport of the study; Dr. Eggert-
Kruse, Unit of Gynecologic En-docrinology of the University ofHeidelberg, for her advice in theevaluation of the patients' cycles;and Prof. Dr. Gasser, Head of theDepartment of Biostatistics, In-stitute for Social and PreventiveMedicine, University of Zurich,and Dr. Jennen and Mr. Wolf,Unit of Biostatistics at the CentralInstitute of Mental Health, Mann-heim, for their statistical adviceand help.
The Authors
Anita Riecher-Rossler, M.D., is
Senior Scientist, and Heinz Hafner,M.D., Ph.D., is Director, Schizo-phrenia Research Unit, CentralInstitute of Mental Health, Mann-heim, Germany. Michael Stum-baum, M.D., is Psychiatrist, StateMental Hospital Klingenmunster,Landeck, Germany. Kurt Maurer,Ph.D., is Psychologist and SeniorScientist, Schizophrenia ResearchUnit, Central Institute of MentalHealth, Mannheim, Germany.Roland Schmidt, Dr. rer. nat., isDirector, Unit of Endocrinology,Institute of Clinical Chemistry,University of Heidelberg, Mann-heim, Germany.
Announcement The International Health Society andthe World Association for SocialPsychiatry will sponsor a conferenceentitled Medicine and Psychologyin a Holistic Approach to Healthand Illness. The conference will beheld October 25-29, 1994, in St.Petersburg, Russia. Topics to becovered include: theory andmethodology of the systems ap-proach to health and illness; holisticapproach to understanding andtreatment of the patient in dynamicpsychiatry; psychosocial aspects of
prevention, treatment, and rehabilita-tion; psychosomatic problems ofmodem medicine; psychotherapy:theory and practice; psychotherapyand psychopharmacology; and legaland ethical aspects of psychiatry.
For further information, pleasecontact
Gunter Ammon, M.D.Geothestrape 548000 Munchen 2, GermanyTelephone: 0049 89/53 96 75Fax: 0049 98/53 28 837
by guest on June 1, 2015http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from
Related Documents