CAN DUAL ENERGY CT USING IODINE MAPPING PREDICT THE NUCLEAR GRADE OF CLEAR CELL TYPE OF RENAL CELL CARCINOMA A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT OF MD RADIODIAGNOSIS (BRANCH VIII) EXAMINATION OF THE TAMIL NADU DRM.G.R MEDICAL UNIVERSITY, CHENNAI TO BE HELD IN APRIL 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CAN DUAL ENERGY CT
USING IODINE MAPPING
PREDICT THE NUCLEAR
GRADE OF CLEAR CELL
TYPE OF RENAL CELL
CARCINOMA
A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT
OF MD RADIODIAGNOSIS (BRANCH VIII) EXAMINATION OF
THE TAMIL NADU DRM.G.R MEDICAL UNIVERSITY,
CHENNAI TO BE HELD IN APRIL 2017

CERTIFICATE
This is to certify that the dissertation titled “Can dual energy CT using Iodine mapping
predict the nuclear grade of clear cell type of renal cell carcinoma” is the bonafide
work of Dr. Poulomi Mitra towards the MD Radiology Degree Examination of The
Tamil Nadu Dr. M.G.R Medical University to be conducted in April 2017. This work
has not been submitted to any university in part or full.
Dr. Shyamkumar N.K Dr. Anna Pulimood
Professor and Head Principal
Department of Radiology Christian Medical College
Christian Medical College Vellore 632002
Vellore 632004
CERTIFICATE
This is to certify that the dissertation titled “Can dual energy CT using Iodine mapping
predict the nuclear grade of clear cell type of renal cell carcinoma” is the bonafide
work of Dr. Poulomi Mitra towards the MD Radiology Degree Examination of The
Tamil Nadu Dr. M.G.R Medical University to be conducted in April 2017. This work
has not been submitted to any university in part or full.
Dr. Anu Eapen
Professor
Department of Radiology
Christian Medical College
Vellore - 632002

DECLARATION
I hereby declare that this dissertation titled “Can dual energy CT using Iodine mapping
predict the nuclear grade of clear cell type of renal cell carcinoma” is a bonafide work
done by me under the guidance of Dr. Anu Eapen, Professor of Radiology, Christian
Medical College, Vellore. This work has not been submitted to any university in part
or full.
Dr. Poulomi Mitra
Post Graduate Registrar
Department of Radiology
Christian Medical College Vellore
Vellore-632004

ACKNOWLEDGEMENT
This study would not have been possible without the help and hard work of many
people. It is practically not possible to acknowledge all of them separately by name in
short stretch. I wish to place in my record my sincere appreciation and immense
gratitude to some of them mentioned below.
First of all I would like to thank almighty God for guiding me althrough.
I sincerely thank to Dr Anu Eapen, my guide for guiding me throughout the study
period. I am deeply indebted to Dr Anuradha who was always ready to help and prompt
in response during the protocol development, IRB submission and results and analysis.
I would like to thank Dr. Betty Simon, who helped me setting the protocol. Dr. Ramani,
Associate Professor, Department of pathology patiently went through my proposal and
gave constant support in reading and interpreting pathological reports. Dr. Nitin Kekre
and Dr Antony Devasia and their team from Department of Urology provided all
necessary supports. I cannot forget the help of all the senior and junior radiographers
who worked relentlessly to put my project on the go. All my senior and junior
colleagues in the department helped me and supported me during this project.
I am grateful to Dr Visali Jayaseelan who helped me in analysis of results.
Last but not the least, my family, without their constant support this was not at
all possible.
CONTENTS: Page No
Abstract 09
Introduction 12
Aims 14
Objectives: 14
Review of Literature 14
Methods 46
Results & Analysis 55
Discussion 81
Conclusion 87
Limitation 87
Future Direction 87
Bibliography 88
Annexures 91
ABSTRACT
INTRODUCTION:
Renal cell carcinoma, most common malignancy of kidney is predominantly
disease of elderly. With a steady rise in global incidence of RCC number of
incidentally detected disease and small, localised diseases are also increasing. Other
than tumour stage, nuclear grade is considered an independent prognostic factor of
RCC. Recently introduced dual energy CT which uses two different peak energies
enables us to reconstruct virtual non contrast images, virtual monochromatic images
and two material (commonly iodine and water) decomposition and quantification.
AIMS:
The aim of the study is to see whether iodine concentration in the clear cell renal
cell carcinoma (RCC), obtained using iodine mapping in dual energy CT (DECT) can
predict the nuclear grade of clear cell type of renal cell carcinoma.
OBJECTIVES:
1 To correlate iodine concentration in clear cell type of RCC can predict the
nuclear grade of RCC.
2 To identify cut off values of iodine concentration which can best identify the
nuclear grade of RCC.
MATERIALS & METHODS:
It was a prospective study conducted during the time period of September 2014
to July 2016. Institutional review board approved the study. All patients with suspected

or known renal mass referred for pre-operative CT abdomen was recruited for the
study who underwent dual energy CT in arterial and venous phase in GE Discovery
750 HD CT machine. This is a single source fast kV switching dual energy CT
machine. Water suppressed iodine density images are obtained to draw ROI in three
different levels in RCC in both arterial and venous phases to get maximum, minimum
and mean iodine concentration. ROIs are also drawn in aorta and normal kidney in
arterial and venous phases. Post operatively histological types and nuclear grades were
noted. Finally, patients with clear cell type of RCC are included for analysis
RESULTS & ANALYSIS:
Total 95 lesions were analysed in 95 different patients. For three patients with
multiple RCCs larger lesion was considered for analysis. Predominantly cystic lesions
did not correlate well with nuclear grade. Solid tumours show good correlation with
nuclear grades. The mean iodine concentration in the venous phase showed maximum
correlation to predict nuclear grade. Mean venous phase iodine concentration of 16.74
mg/cc or less was found to predict higher grades of RCC (grade 3 and 4) with 65%
sensitivity and 81% specificity. Other factors which also show significant correlation
with nuclear grades are minimum venous phase iodine concentration, ratio of
minimum venous phase iodine concentration to mean iodine concentration in kidney
and ratio of minimum iodine concentration in arterial phase to arterial phase mean
kidney iodine concentration.
CONCLUSION:
The mean iodine concentration in the venous phase can predict nuclear grade
with moderate accuracy for solid tumours. For predominantly cystic RCCs iodine
concentration did not correlate with the nuclear grade.
INTRODUCTION
Renal cell carcinoma (RCC) is the most common malignancy of kidney accounts
for 3% of adult malignancies and its incidence is steadily increasing throughout the
world at a rate of 2-3%. More than 50% RCCs are now being diagnosed incidentally,
due to sophistication of the imaging tools(1). With increase in incidentally detected
disease the number of localised and small disease are also increasing. Along with the
tumour size, local disease extent, and disease stage, nuclear grade is also considered
as independent prognostic factor for RCC. Fuhrman grading system which is based on
size, shape and margin of nucleus and prominence of nucleoli is now widely used to
grade RCC. Studies have shown that only 9.2% of small tumours are of high grade and
in a metaanalysis of 300 small RCCs 2-3 year follow up showed 2.8 mm growth rate
and only 4 had metastases(2). Because of these observations non- invasive or
minimally invasive treatment options are gaining popularity. Percutaneous renal
biopsies are also being used for planning management. Though renal biopsies are
almost 94% accurate in predicting histological subtypes, prediction of nuclear grade
with core biopsy is not reliable(3)(2). This led the investigators to look for non-
invasive ways to predict nuclear grade. Different CT findings and enhancement
patterns have been studied.
Dual energy CT is different from conventional CT that it uses two different peak
energies and is able to produce reconstructed virtual unenhanced images, virtual
monochromatic images and two basis material (mostly iodine and water)
differentiation and quantification.
In this study we aimed to measure iodine concentration in clear cell RCC and to
find relation with the nuclear grade of RCC.
AIMS
The aim of the study is to see whether iodine concentration in the clear cell renal
cell carcinoma (RCC), obtained using iodine mapping in dual energy CT (DECT) can
predict the nuclear grade of clear cell type of renal cell carcinoma.
OBJECTIVES
3 To correlate iodine concentration in clear cell type of RCC can predict the
nuclear grade of RCC.
4 To identify cut off values of iodine concentration which can best identify the
nuclear grade of RCC.
REVIEW OF LITERATURE
RENAL CELL CARCINOMA:
The most common malignant disease of kidney is renal cell carcinoma (RCC)
comprising of 85% of renal malignancies(1)
GLOBAL EPIDEMIOLOGY:
According to 2013 data, kidney cancer is the 15 th most common cancer in the
world and since 1990 its incidence has increased 107% in both the sexes. (4) This
increase in incidence is attributed by increase in incidence rate as well as increase in
life expectancy, both contributing equally to the overall increase in incidence(4). More
than 50% of RCCs are now being detected incidentally (1). With increase in
incidentally detected RCCs the number of localised disease or small lesions are
increasing. According to SEER (Surveillance Epidemiology and End Results)
statistics number of localised disease is 647% (5). This is predominantly the disease
of elderly, commonly occurring at 6-7th decade. Mortality in RCC is relatively low. In
UK 3% of cancer deaths are caused by kidney cancer in the year 2014. According to
the SEER statistics mortality rate has dropped consistently since year 2000 onwards.
INDIAN SCENARIO:
Incidence of RCC in India is less compared to the western world. Kidney cancers
rank 21st among all the cancers in India.(4). In a large retrospective study in India,
Agnihotri et al found younger age of patient at presentation and larger size of tumour
compared to the western population.(6)
CLINICAL PRESENTATION (1):
The classic triad of flank pain, palpable lump and haematuria are relatively rare
at presentation now a days and almost always indicate locally advanced disease.
Because of sophisticated imaging tools more than 50% of RCCs are now being
detected incidentally while undergoing imaging for other indications. Minority of
patients present with metastatic symptoms like cough and bone pain. An uncommon
but not worthy way of presentation is perirenal hemorrhage. So all patients with
perirenal hematoma with unclear etiology should be investigated to rule out under
lying renal cell carcinoma or angiomyolipoma.
Approximately 20% of patient of RCC have paraneoplastic syndrome which
include polycythemia, hypertension, hypercalcemia and Stauffer’s syndrome ie non
metastatic liver dysfunction.
PROGNOSTIC FACTORS:
Prognosis of RCC depends on the following factors(1)
1. Anatomic- Anatomical extent of disease or disease stage
2. Clinical- Patient’s performance, loss of weight, presence of paraneoplastic
disease
3. Histologic
- Tumour morphotype
- Nuclear grade of tumour
- Histologic necrosis
- Microvascular invasion
- Rhabdoid/ sarcomatoid differentiation
4. Different Molecular markers
1. TUMOUR MORPHOTYPE
RCC is basically adenocarcinoma arising from the tubular epithelial cell.
Recent investigations suggest that clear cell and papillary subtypes of RCC arise from

proximal convoluted tubules of nephrons, whereas all other histologic variants are
distal in origin. Since 1990, histological classifications of RCC underwent several
major modifications. The 2004, WHO classification changed the basic concept of
RCC, as a group of several different tumour subtypes, rather a single entity. Each
different subtypes has distinguished genetic basis and unique clinical features. The
latest classification is ISUP (International Society of Urologic Pathology) Vancouver
modification (2012) of 2004 WHO classification (7).
Table 1: Histological classification of RCC: Adapted from ISUP Vancouver
Modification of WHO (2004) Histologic Classification of Kidney Tumours
1. Clear cell carcinoma
- Multicystic clear cell carcinoma of low malignant potential
2. Papillary RCC
- Type I
- Type II
3. Chromophobe RCC
- Hybrid oncocytic chromophobe tumour
4. Carcinoma of the collecting ducts of Bellini
5. Renal medullary carcinoma
6. MiT family translocation RCC
- Xp11 translocation associated RCC
- t(6-11) translocation RCC
7. Carcinoma associated with Neuroblastoma

8. Mucinous tubular and spindle cell carcinoma
9. Tubulocystic RCC
10. Acquired cystic disease associated RCC
11. Clear cell (tubulo) papillary renal cell carcinoma
12. Hereditary leiomyomatosis and Renal cell carcimoa associated RCC
13. Renal cell carcinoma – unclassified.
Several reports suggests that clear cell RCC has worse prognosis compared to the
papillary and chromophobe subtypes. 5 year survival of clear cell RCC is 44-69%, for
papillary RCC is 82-92% and for chromophobe RCC is 78-87% (8). Presence of
sarcomatoid differentiation, collecting duct/ renal medullary origin and unclassified
RCCs have in general poorer prognosis On the other hand some tumors like
multiloculated cystic clear cell RCC and mucinous tubular and spindle cell RCC have
a documented indolent course.
2. NUCLEAR GRADE:
Grading of RCC is based on nuclear size, outline, presence or absence of nucleoli.
Fuhrman grading system has been widely accepted as a separate prognostic factor of
RCC.
Table 2: Fuhrman grade for clear cell carcinoma (1)
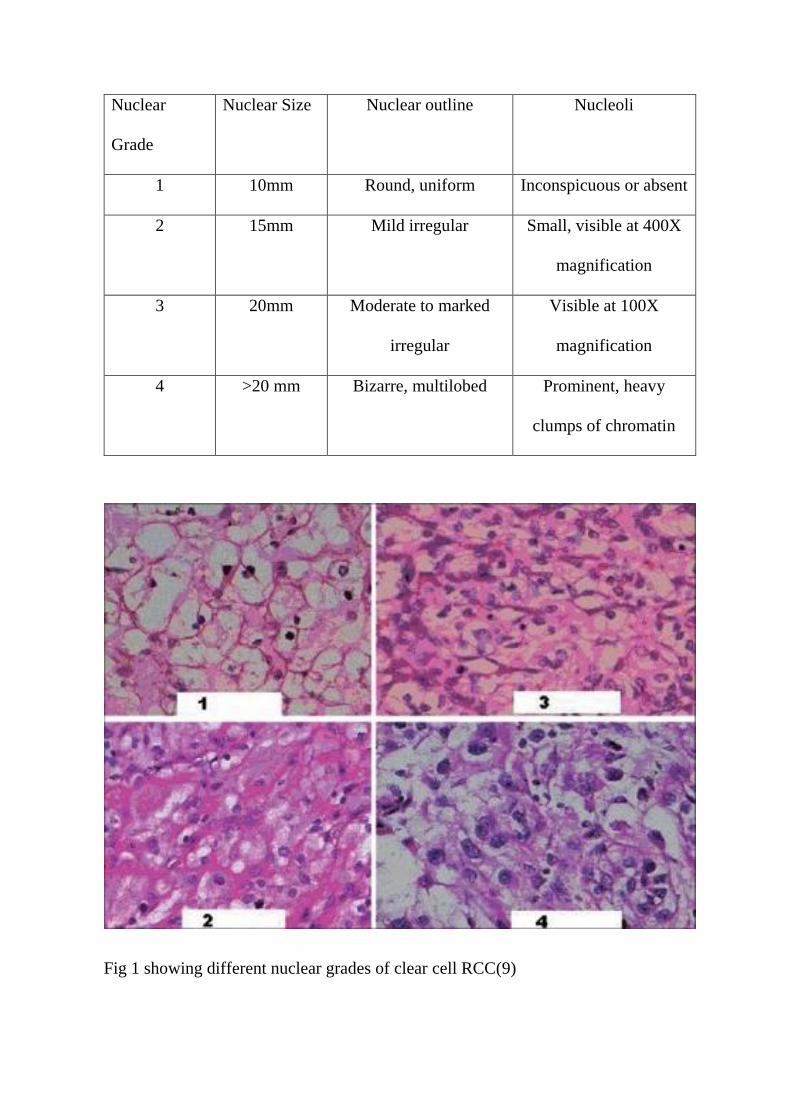
Nuclear
Grade
Nuclear Size Nuclear outline Nucleoli
1 10mm Round, uniform Inconspicuous or absent
2 15mm Mild irregular Small, visible at 400X
magnification
3 20mm Moderate to marked
irregular
Visible at 100X
magnification
4 >20 mm Bizarre, multilobed Prominent, heavy
clumps of chromatin
Fig 1 showing different nuclear grades of clear cell RCC(9)
Nuclear grade has been accepted as independent prognostic factor for RCCs
particularly for clear cell variant. In their original report in 1982, Fuhrman et al
reported 5 year survival of 64%, 34%, 31% and 10% for nuclear grades 1,2,3,4
respectively.
3. DISEASE STAGE & ROLE OF IMAGING:
In a case of renal space occupying lesion, the goal of imaging is to diagnose the
tumour and to assess the stage of the disease. According to the ACR appropriateness
criteria for pre-operative staging of RCC, CT abdomen with and without intravenous
contrast scores maximum with an adult effective radiation dose estimate ranging
between 10-30 mSV. A plain xray chest plays a complimentary role with CT. MRI
abdomen without and with contrast is the second choice in patients with iodinated
contrast allergy. Ultrasound has value in characterising a cystic renal mass and for
image guided biopsy of the renal tumour.
CT Protocol:
CT protocol for suspected or known renal tumour is not absolutely strict. Mild
variations in protocols are seen depending on the institute and author’s preference. But
all authors have recommended a non-contrast scan followed by administration of
iodinated contrast medium (100-150 ml of contrast containing 300mg/ml or 350mg/ml
of iodine) followed by image acquisition at corticomedullary and nephrographic
phases. (10)(11). Corticomedullary phase where contrast enhancement of cortex is
maximum can be acquired at 25-70 s delay and nephrographic phase where there is
homogeneous enhancement of renal parenchyma can be acquired at 100-120 s
delay.(12). A delayed phase or excretory phase (at 5-7 min delay) can be obtained to
complete urologic evaluation if requested by the clinician. Corticomedullary phase can
pick up early enhancing lesions where as some lesions become conspicuous in
nephrographic phase. Staging accuracy of 91% has been reported while using non-
contrast, cortico-medullary and nephrographic phases.
MDCT has an advantage over other CT as it can provide volume rendered data and 3D
reconstruction and maximum intensity projection images can be reconstructed, which
are of help for the clinician for planning surgery.
CT Findings:
In non- contrast images RCC has attenuation of 20HU or higher, difficult to
differentiate from normal renal parenchyma and only identified by focal cortical bulge
in most of the cases. Strong and heterogeneous enhancement is the classical finding in
RCC because of rich vascular supply. However in nephrographic phase RCC appear
hypodense compared to homogeneously enhancing parenchyma. Larger lesions are
usually heterogeneous owing to necrosis and hemorrhage and approximately 30%
RCCs show calcification (8).
CT plays an important role in differentiating RCC from other benign tumours
like angiomyolipoma (AML) and oncocytoma to avoid radical nephrectomy in benign
diseases. AML can be diagnosed with confidence by presence of intra-tumoral fat
content, However in approximately 4.5% cases fat content may be minimal and is

undetectable by CT. In those cases, homogeneous enhancement, prolonged
enhancement and hyperdense nature of the tumour in non-enhanced images can act as
a reliable guiding tool to diagnose AML. (8) Lee-Felker et al reported that absolute
HU value in unenhanced scan of more than 40 has 100% negative predictive value for
AML (13). The hallmark findings of oncocytoma are absence of necrosis, hemorrhage,
calcification; homogeneous contrast enhancement, central stellate scar and spoke
wheel appearance in a well marginated renal lesion. However it is difficult to diagnose
oncocytoma confidently on imaging. (8) Compared to oncocytoma clear cell RCC
shows absolute contrast wash out from corticomedullary to nephrographic phase and
significantly greater relative attenuation in the corticomedullary phase (13)
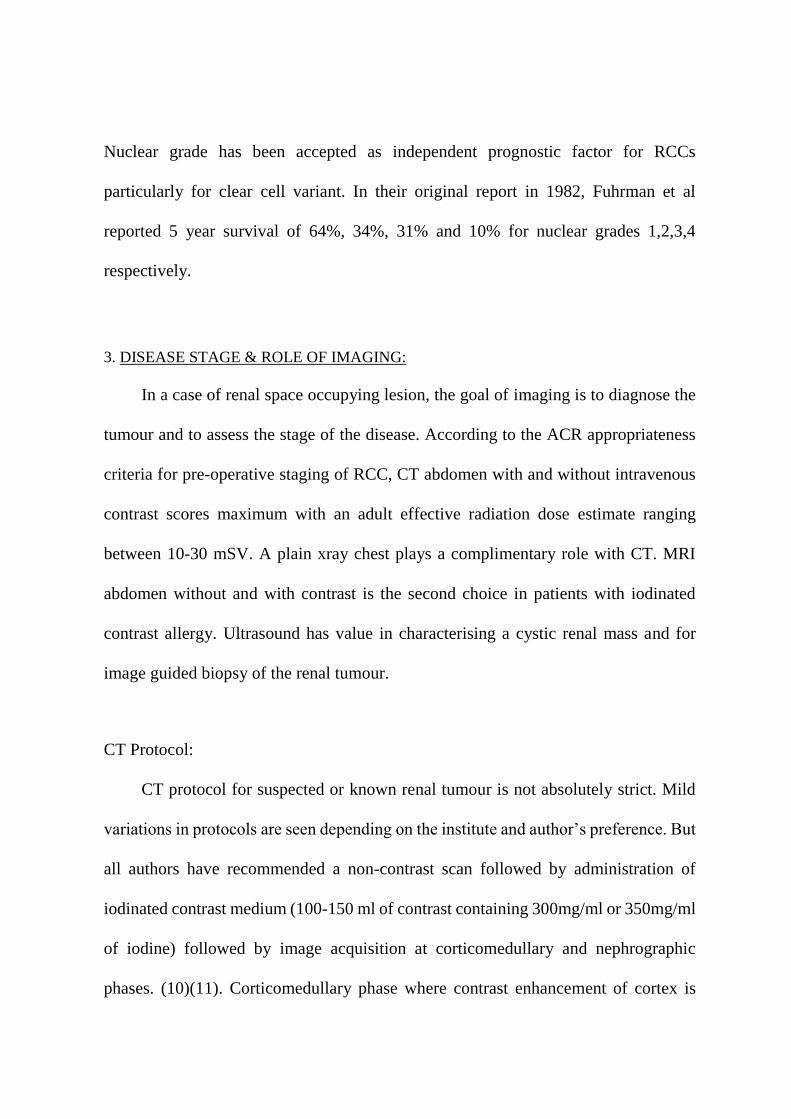
Bosniak et al classified cystic renal masses on CT.
Table 3: Bosniak classification system of characterising cystic renal masses(14)
Category CT Features and Proposed Management
I Simple cyst with thin wall, no septae or wall calcification or solid
component. It has attenuation of water with no enhancement
Intervention is not needed.
II Benign cystic lesion which may contain a few thin septae, fine
calcifications, or small segment of thick calcification in the wall
or septa
Or a uniformly high attenuated lesion (<3 cm), which show sharp
well defined margin and no enhancement in post contrast study
Intervention is not needed.
IIF Cysts showing thin septae, perceived but not measurable
enhancement of septae, focal wall or septal thickening or
calcification (which can be thick and nodular); no nodular
component present
Totally intrarenal, non enhancing, high attenuation lesions are
included
They are probably benign; however follow up is required
III Cystic mass with thick irregular or smooth wall or septae which
show measurable enhancement. Complicated, infected or
hemorrhagic cysts, multilocular cystic nephroma or cystic
neoplasms can be included in this group.
Usually requires surgery
IV Undoubtedly malignant features which include enhancing soft
tissue nodule within the cyst independent of the wall & septae
along with all other features described in type III
These lesions warrant surgical removal
CT scan plays a pivotal role in preoperative disease staging and guiding
management. Assessment of disease stage includes evaluation of the following (12)
i) Tumour size
ii) Tumour renal parenchyma interface
iii) Perinephric extension- involvement of Gerota’s fascia
iv) Involvement of pelvicalyceal system
v) Involvement of contiguous organs and adrenal gland
vi) Presence of venous involvement and extension
vii) Local and regional lymphadenopathy
viii) Local and distal metastases
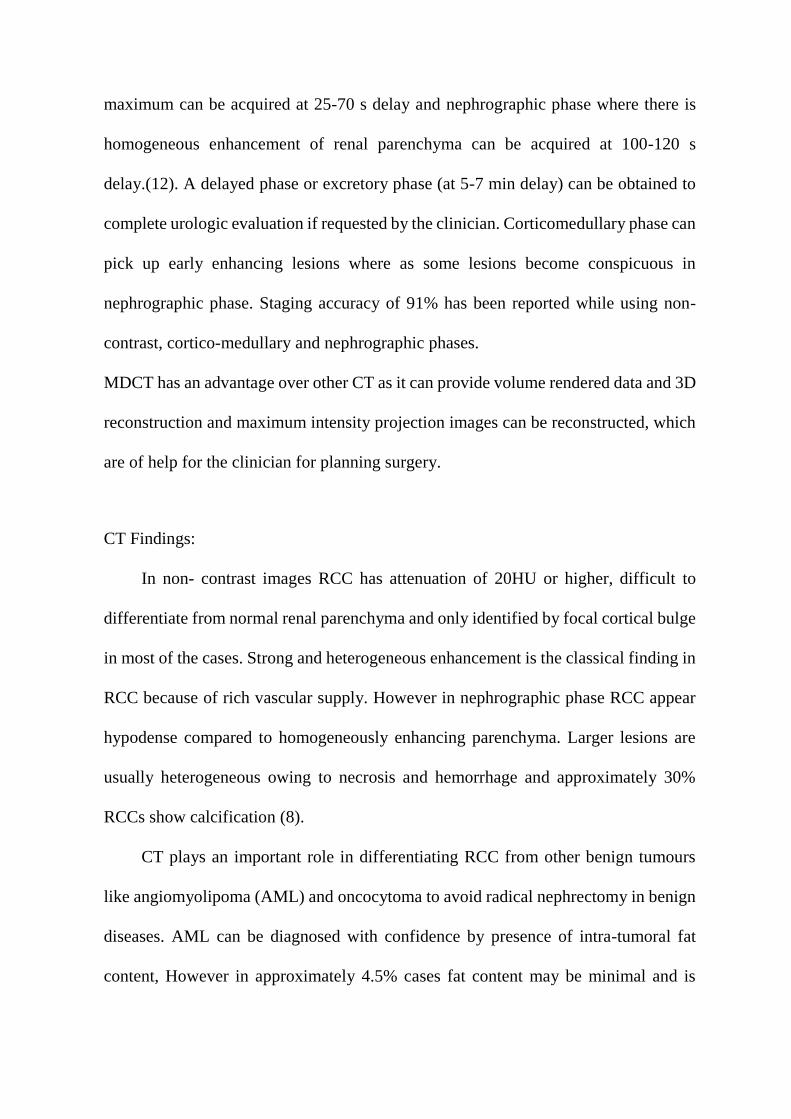
Table 4: Modified AJCC staging of Kidney cancer (2010)
Primary Tumour
Tx Primary tumour cannot be assessed
T0 No evidence of primary tumour
T1 Tumour _< 7 cm, confined to kidney
T1a Tumour _< 4 cm, confined to kidney
T1b Tumour > 4cm and _< 7 cm, confined to kidney
T2 Tumour > 7 cm, confined to kidney
T2a Tumour > 7 cm and _< 10 cm, confined to kidney
T2b Tumour >10 cm, confined to kidney
T3 Tumour extends into major veins, perinephric spread, but no
extension beyond Gerota’s fascia and no involvement of adrenal
glands
T3a Tumour in renal vein or its segmental branches, perinephric or
renal sinus fat involvement, however no involvement beyond
Gerota’s fascia
T3b Tumour extending into the inferior vena cava (IVC) below the
diaphragm
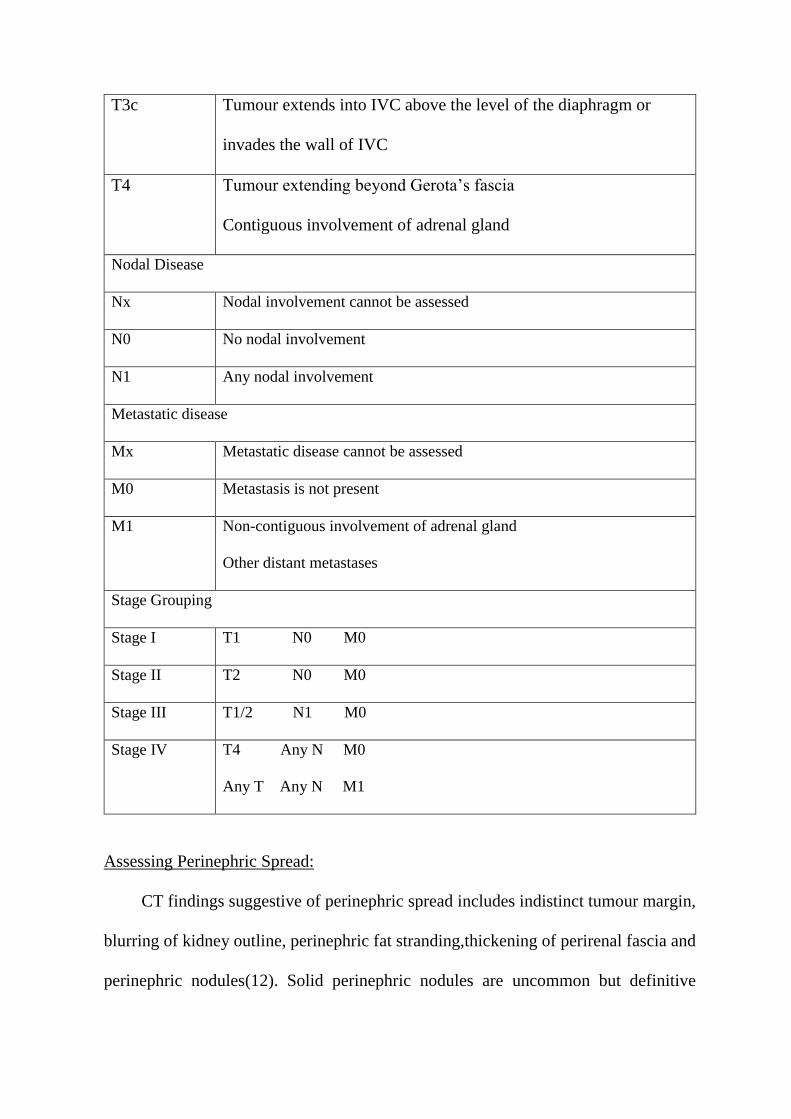
T3c Tumour extends into IVC above the level of the diaphragm or
invades the wall of IVC
T4 Tumour extending beyond Gerota’s fascia
Contiguous involvement of adrenal gland
Nodal Disease
Nx Nodal involvement cannot be assessed
N0 No nodal involvement
N1 Any nodal involvement
Metastatic disease
Mx Metastatic disease cannot be assessed
M0 Metastasis is not present
M1 Non-contiguous involvement of adrenal gland
Other distant metastases
Stage Grouping
Stage I T1 N0 M0
Stage II T2 N0 M0
Stage III T1/2 N1 M0
Stage IV T4 Any N M0
Any T Any N M1
Assessing Perinephric Spread:
CT findings suggestive of perinephric spread includes indistinct tumour margin,
blurring of kidney outline, perinephric fat stranding,thickening of perirenal fascia and
perinephric nodules(12). Solid perinephric nodules are uncommon but definitive
feature of perinephric spread. Perinephric fat stranding is non-specific findings as it
can be associated with other inflammatory edema, fat necrosis, hemorrhage.
Hemorrhage is common in renal cancer and can mask or over-estimate perinephric
spread. Reports suggest that accuracy of detecting perinephric spread is low for both
CT and MRI. So all potentially locally advanced diseases are managed with radical
nephrectomy.
Assessment of Adrenal Gland:
Adrenal gland involvement cab be diagnosed with reasonable accuracy (100%
sensitivity and 76% specificity) with preoperative CT and per-operative findings.
Enlarged adrenal gland with indistinct margin and large renal tumour suggests adrenal
involvement.
Assessment of Nodal Disease:
Predominantly paraortic and renal hilar nodes are involved in nodal disease.
Though rare involvement of mediastinal and pulmonary hilar nodes are also reported,
more on right side because of direct communication with the thoracic duct (24).
Enlarged hilar or retroperitoneal lymph nodes more than 2 cm are almost always
metastatic. 43% false positive results are noted when 1 cm size criteria is used for
nodal enlargement. Incidence of reactive lymphadenopathy is higher in primary
tumour necrosis and IVC thrombosis. However CT has been reported to be 83-89%
accurate in predicting nodal disease.(12)

Assessment of Vascular Invasion:
The CT findings suggestive of venous involvement are distension of the vein,
abrupt change in venous calibre, intraluminal low density areas or filling defects.
Presence of collateral veins also support the diagnosis. Previously MRI was considered
to be superior in evaluating venous involvement. But recent data suggest multiplaner
CT can be equally helpful.
Assessment of Contiguous organ involvement & Distal metastases:
Direct involvement of the diaphragm, psoas, erector spinae, quadratous
lumborum by tumor are well seen in CT. Mere loss of fat plane with adjacent organs
such as liver and colon cannot be taken as contiguous organ involvement. The involved
organ should show definite change in attenuation and enlargement.(12). CT can show
lung, liver and bone metastases. Liver metastases are hypervascular and show arterial
phase enhancement. Bone lesions are expansile, lytic, can be seen in vertebrae, ribs
and pelvic bones. MDP Tc99 Bone scintigraphy is not sensitive for lytic bone
metastases and should be reserved for selected cases with bone pain, raised alkaline
phosphatase. Xray chest play complimentary role with CT abdomen to rule out
pulmonary metastases. CT thorax can be done with extensive intra- abdominal disease,
IVC thrombosis to rule out lung metastases. Resection of solitary pulmonary
metastases can improve 5 year survival from 26 to 56 %.( 24)
Table 5: TNM staging and 5 year survival of RCC
TNM (2009) 5 year survival (%)

T1aN0M0 90-100
T1bN0M0 80-90
T2aN0M0 65-80
T2bN0M0 50-70
T3aN0M0 50-70
T3bN0M0 40-60
T3cN0M0 20-40
T4N0M0 0-30
AnyTN1M0 0-20
AnyTN0M1 0-10
RECENT ADVANCES IN CT FURTHER CHARACTERISING RCC:
1. Predicting RCC subtypes in CT
Because of the known prognostic value of tumour morphotypes and nuclear
grades, different imaging parameters have been tested by several investigators to
predict the different subtypes of RCC. Various authors have suggested increased
enhancement and more heterogeneity in clear cell RCC compared to other subtypes
(15)(16)(17). Kim et.al reported significantly more attenuation value and degree of
enhancement in clear cell RCC compared to papillary and chromophobe variety in
both corticomedullary and excretory phases.(15) Same study mentioned a cut off value
for increase in attenuation by 84HU has 74% sensitivity and 100% specificity for clear
cell carcinoma. Clear cell RCCs are hypervascular and heterogeneous whereas
papillary and chromophobe RCCs are relatively hypovascular and more homogeneous.
In a recent retrospective study conducted in clear cell and papillary RCC who
underwent dual energy CT as part of pre-operative assessment, Mileto et al measured
iodine concentration in RCC. They concluded that iodine concentration of 0.9mg/ml
has 98.2% sensitivity and 86.3% specificity in differentiating clear cell from papillary
RCC. They also noted a significant correlation between the iodine concentration in
tumour and nuclear grade for both clear cell RCC (τ = 0.85; P < .001) and
papillary RCC (τ = 0.53; P < .001).
2. Predicting Nuclear Grade of RCC in CT
In 1994, after studying 100 renal cell carcinoma, Birnbaum reported that
tumour with higher nuclear grade are more likely to show larger size, more
heterogeneous appearance, indistinct margin and higher tumour stage; of which
tumour margin is more closely related to nuclear grade of tumour. In a recent
retrospective study on 48 patients Villalobos-Gollas et al concluded that lower
enhancing areas are negatively related with nuclear grade.(18) In another retrospective
study of 255 patients with clear cell carcinoma Zhu et al found that low enhancement
in corticomedullary phase has high association with high grade tumour. They also
concluded that relative enhancement in cortico-medullary phase in multiphasic CT
scan is the best predictor of grade tumour and it has 84% sensitivity and 93%
specificity when cut of value of 0.65 relative corticomedullary enhancement is
used.(19)
RECENT ADVANCES IN CT TECHNOLOGY:
With advent of multi detector row CT (MDCT) image acquisition has become
faster with acquisition of volume data, better multiplaner and 3D reconstruction, which
dramatically changed the radiologic imaging. Additional application of dual energy
CT technology enables further imaging analysis and advantage of material
differentiation and quantification
What is Dual Energy CT?
In contrast to conventional CT which uses polychromatic xray beam with single
peak energy (chosen between 80-140 kV), dual energy CT uses two peak energies.(20)
Two most frequently used energies in dual energy CT are 80 kV and 140 kV.
In dual energy CT, two different data sets are obtained from single anatomic
location, one with high energy and one with low energy. Because each material
behaves in specific way when exposed to different energy of xray photon their change
in attenuation is specific. Two materials which have similar appearance in one energy
can show significant attenuation difference at other energy. Like iodine and calcium
can have similar appearance in conventional CT, but at lower energies attenuation of
iodine is much more compared to the calcium.(21)
Dual energy CT principle is mainly based on the photoelectric effect of matter
when exposed to xray. At energies just above the k-shell binding energy (which is
specific for each material) of the element the element shows spike in the attenuation,
known as k-edge. Human body is mainly made of organic substances containing
hydrogen, oxygen, nitrogen, carbon and some inorganic substances like calcium,
phosphorus. Iodine, injected during post contrast studies show causes varying
enhancement of the structures depending on the vascularity because of its high
attenuation values compared to soft tissue. The k-edge values of carbon, nitrogen,
hydrogen and oxygen ranges from 0.01 to 0.53keV which are far below the xary
energies used in diagnostic imaging. K-shell energies of calcium (4.0keV) and iodine
(33.2 keV) are quite high compared to soft tissues in body and forms the basis of
material differentiation in dual energy CT scan.
DUAL ENERGY CT ACQUISITION:
The most commonly used energies are 80 and 140 kV because they allow
maximum spectral differentiation and minimum overlap. Five different ways of dual
energy image acquisition are possible
i) Sequential acquisition at two different energies in available CT machines
ii) Fast kV switching in a single tube DECT scanner – Prototype GE Discovery
750 HD
iii) Dual source dual energy CT- Prototype Siemens Somatom
iv) Layer detectors with single xray tube Protype Philips
v) Quantum counting or energy resolving detectors- not available
Each machine has unique way of acquiring and processing images and has their own
advantages and disadvantages
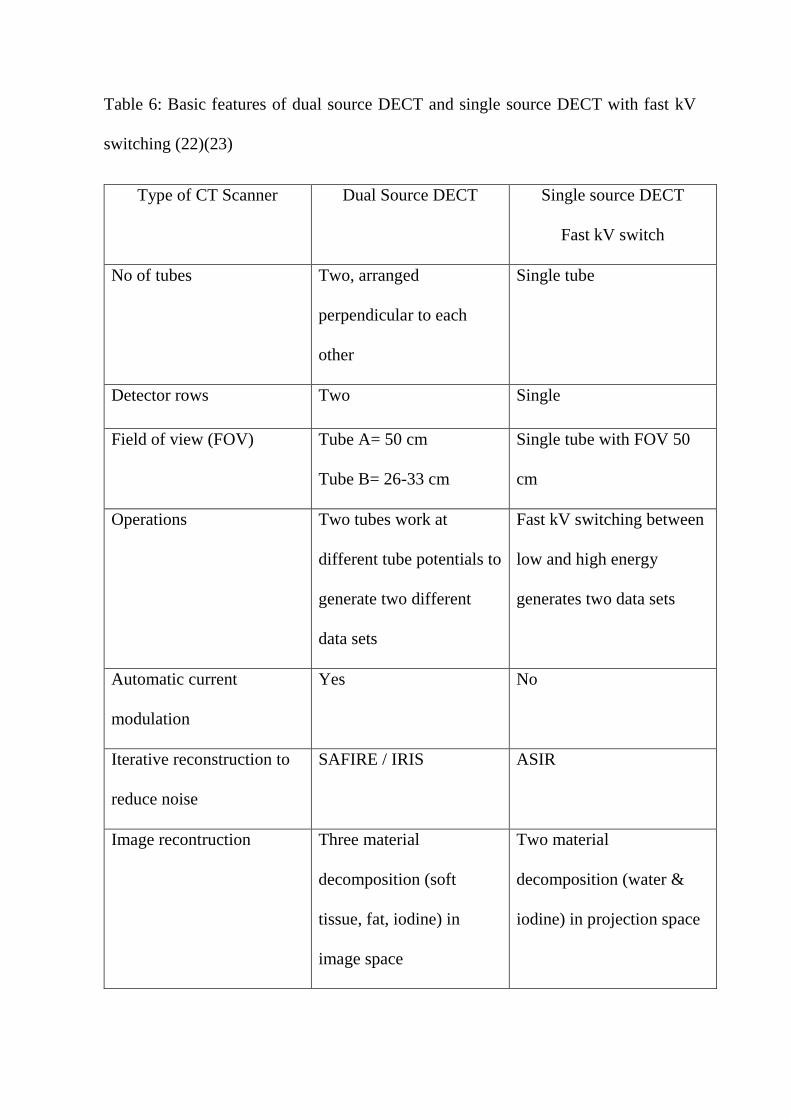
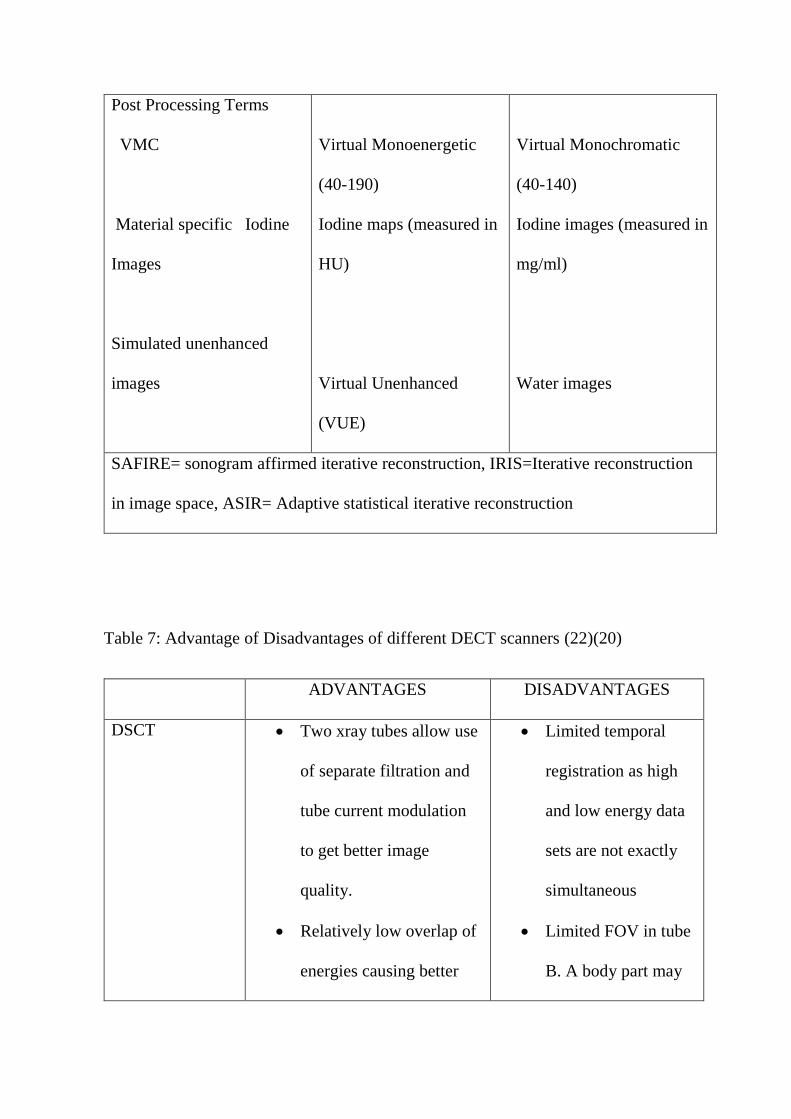
Table 6: Basic features of dual source DECT and single source DECT with fast kV
switching (22)(23)
Type of CT Scanner Dual Source DECT Single source DECT
Fast kV switch
No of tubes Two, arranged
perpendicular to each
other
Single tube
Detector rows Two Single
Field of view (FOV) Tube A= 50 cm
Tube B= 26-33 cm
Single tube with FOV 50
cm
Operations Two tubes work at
different tube potentials to
generate two different
data sets
Fast kV switching between
low and high energy
generates two data sets
Automatic current
modulation
Yes No
Iterative reconstruction to
reduce noise
SAFIRE / IRIS ASIR
Image recontruction Three material
decomposition (soft
tissue, fat, iodine) in
image space
Two material
decomposition (water &
iodine) in projection space
Post Processing Terms
VMC
Material specific Iodine
Images
Simulated unenhanced
images
Virtual Monoenergetic
(40-190)
Iodine maps (measured in
HU)
Virtual Unenhanced
(VUE)
Virtual Monochromatic
(40-140)
Iodine images (measured in
mg/ml)
Water images
SAFIRE= sonogram affirmed iterative reconstruction, IRIS=Iterative reconstruction
in image space, ASIR= Adaptive statistical iterative reconstruction
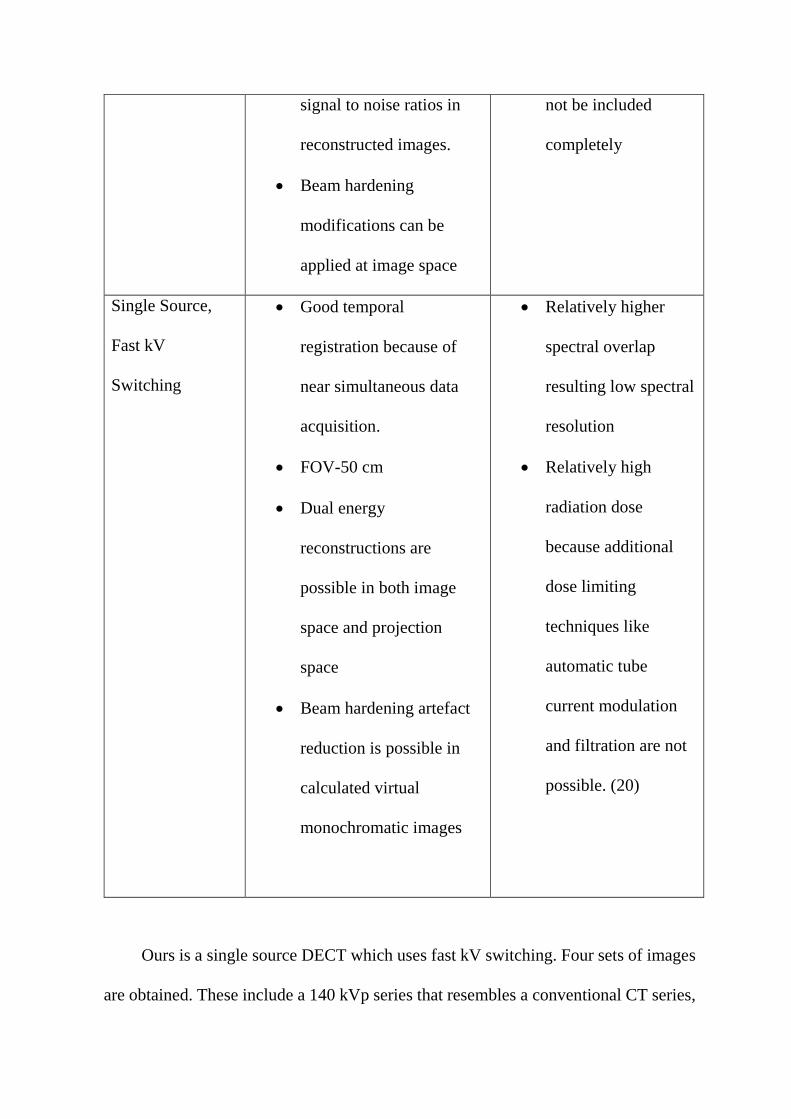
Table 7: Advantage of Disadvantages of different DECT scanners (22)(20)
ADVANTAGES DISADVANTAGES
DSCT Two xray tubes allow use
of separate filtration and
tube current modulation
to get better image
quality.
Relatively low overlap of
energies causing better
Limited temporal
registration as high
and low energy data
sets are not exactly
simultaneous
Limited FOV in tube
B. A body part may
signal to noise ratios in
reconstructed images.
Beam hardening
modifications can be
applied at image space
not be included
completely
Single Source,
Fast kV
Switching
Good temporal
registration because of
near simultaneous data
acquisition.
FOV-50 cm
Dual energy
reconstructions are
possible in both image
space and projection
space
Beam hardening artefact
reduction is possible in
calculated virtual
monochromatic images
Relatively higher
spectral overlap
resulting low spectral
resolution
Relatively high
radiation dose
because additional
dose limiting
techniques like
automatic tube
current modulation
and filtration are not
possible. (20)
Ours is a single source DECT which uses fast kV switching. Four sets of images
are obtained. These include a 140 kVp series that resembles a conventional CT series,
also known as the quality series; a virtual mono-chromatic images obtained with single
photon energy between 40 and 140 keV; a material-specific base pair series showing
low (ie, water) and high (ie, iodine) attenuating material(24).
DECT RECONSTRUCTION:
CT image reconstruction in a fast kV switching scanner occurs in projection
space. Two basic types of reconstruction can be done.
a) Material density images which gives material specific information.
b) Monochromatic images which give images at selected energy between 80-120k
Material Differentiation:
Generation of material density images is based on the theory that attenuation
coefficient of any material can be obtained by weighted sum of attenuation coefficients
of two basis materials as long as the k-edge of the material is not within the evaluated
energy range. The material pair should have significant difference in their effective
atomic number and their mass attenuation coefficients.
Depending on the clinical setting base material pairs can be chosen(25). The most
common material pairs used for material decomposition images are iodine-water and
iodine-calcium. The water density images in iodine-water material specific
reconstructed images can represent virtual non contrast images as it removes iodine
from reconstructed images. On the other hand in iodine density images in material
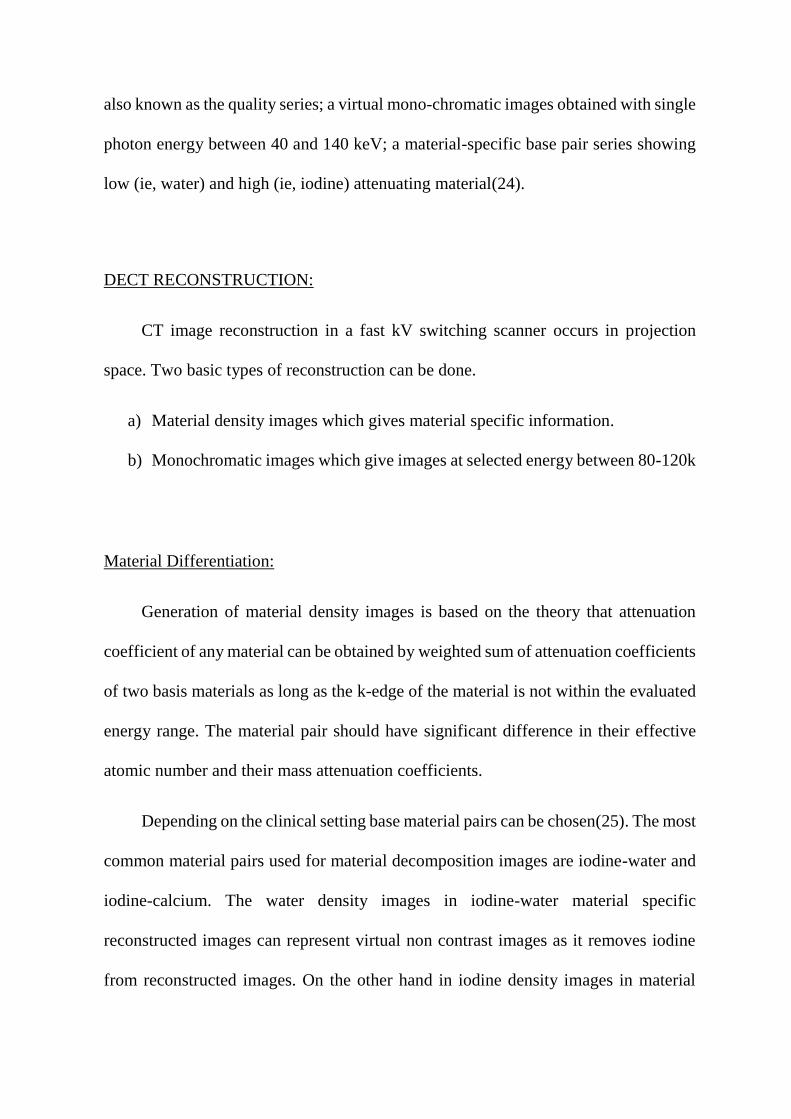
specific image sets show only iodine containing areas as high density areas and iodine
concentration is represented as mg/ml. Another important material is calcium which is
widely present in bones and plaques. Bone and calcium removal can play a significant
role in neurologic, cardiac and vascular imaging.
Fig 2 showing Colour coded iodine images (A) and Spectral HU curve (B)
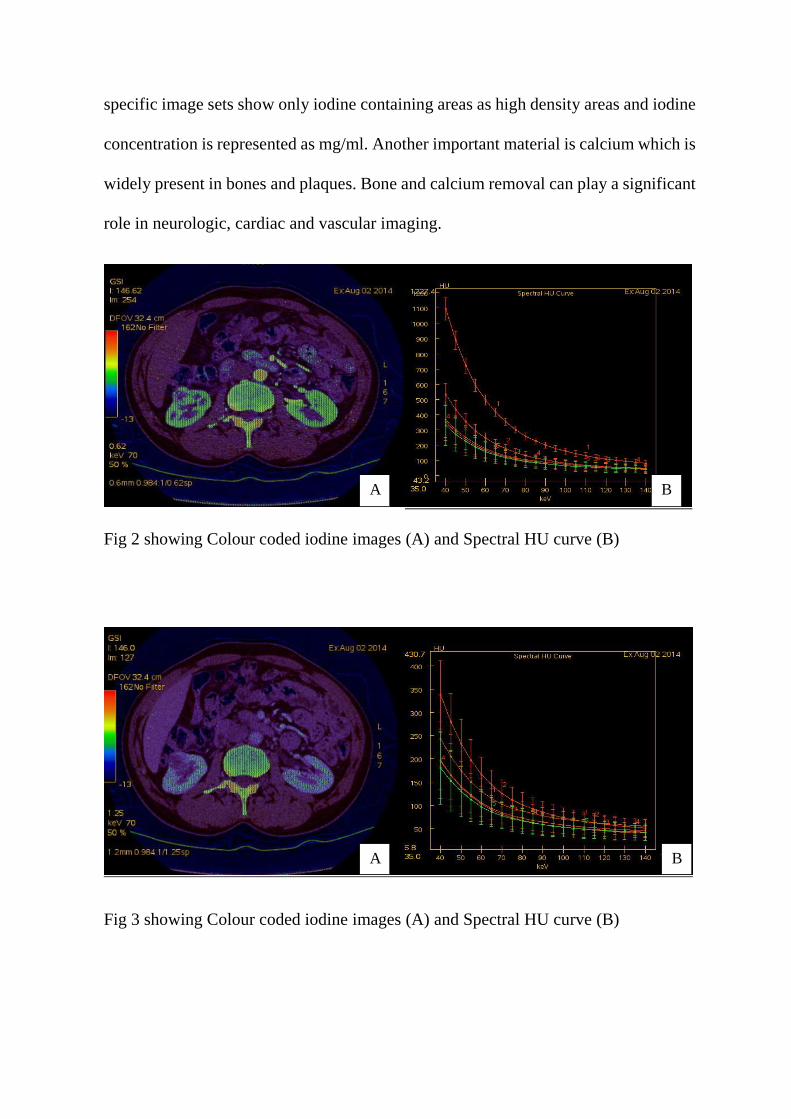
Fig 3 showing Colour coded iodine images (A) and Spectral HU curve (B)
A B
A B

Fig 4A shows iodine suppressed water images (virtual unenhanced images) and 4B
shows water suppressed iodine images
Virtual Monochromatic Images:
Dual-energy CT scanners are able to generate virtual monochromatic (VMC)
images at any given kVp using complex algorithm resulting in images as if they were
imaged with a theoretical monochromatic beam. The appearance of images changes
with change in keV even if window width and levels are unchanged. The lower energy
images have higher contrast as well as more noise, and high energy images have less
contrast and less noise. So monoenergetic reconstruction should be done depending on
the clinical requirement. Matsumoto et al reported lowest image noise and improved
contrast to noise ratio in virtual monochromatic images obtained close to 70keV(26).
Reconstruction at 50-55keV has been reported to be better for evaluation of vessels
and slow flow or subtle endoleaks. High energy reconstruction at 95-150 keV can be
done to reduce metal artefacts depending upon the implant composition. It can be done
either is projection space or image space. Projection space reconstruction has
A B
additional advantage of reduced beam hardening artefacts and it provides curve
showing CT numbers (HU) of different materials against energy range of 40-
140keV.(25) Because of high attenuation of iodine at lower signal and improved
contrast to noise ratio lower dose of contrast dose can be used. These virtual single
photon–energy images provide more reliable attenuation values than conventional
polychromatic CT images.(27).However a single-energy CT scan using low tube
potential is superior to a dual energy scan with virtual monochromatic reconstruction
if material differentiation is not required(25)
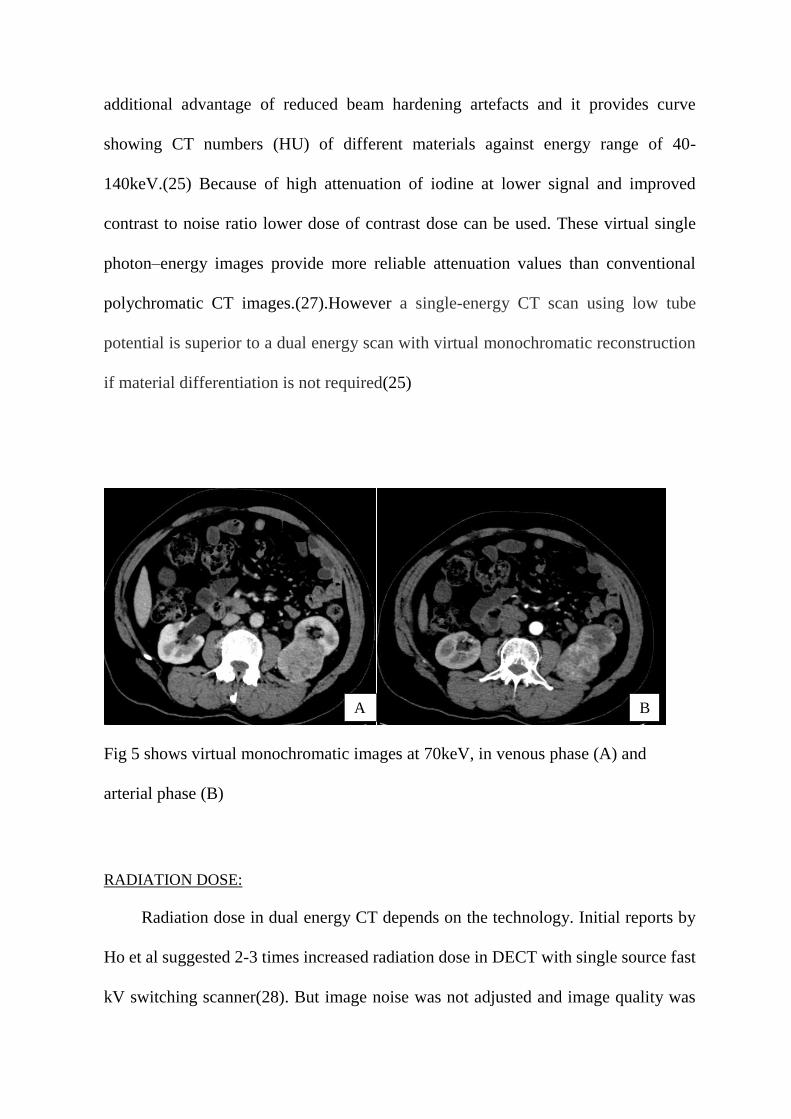
Fig 5 shows virtual monochromatic images at 70keV, in venous phase (A) and
arterial phase (B)
RADIATION DOSE:
Radiation dose in dual energy CT depends on the technology. Initial reports by
Ho et al suggested 2-3 times increased radiation dose in DECT with single source fast
kV switching scanner(28). But image noise was not adjusted and image quality was
A B
not taken into account. Thomas et al conducted a phantom study using Alderson model
to characterise renal calculi using DECT showed comparable radiation dose with
SECT(29). Advantage of dual source system is, adjustment of the tube current and use
of separate filters can be done which will further reduce radiation dose to the patient.
Graser et al showed single phase acquisition using DECT can characterise renal mass
as benign or malignant accurately with colour coded images reducing the image
interpretation time and finally it reduced radiation exposure to patient.(30)
APPLICATIONS OF DECT IN GENITOURINARY DISEASES:
Song et al showed iodine overlay technique and using virtual non contrast images
can characterise renal masses as simple cysts, haemorrhagic cysts, angiomyolipoma
and RCC accurately. (31)
Graser et al showed single phase acquisition using DECT can characterise renal
mass as benign or malignant accurately with colour coded images reducing the image
interpretation time and finally it reduced radiation exposure to patient. (30)
Ascenti et al showed the value of virtual non contrast image and colour coded
iodine images in diagnosis of complex renal cysts. The use of virtual non contrast
images can obviate the need of the true noncontrast images and thus reduce radiation
dose. Color coded iodine images can pick up intra cystic enhancement effectively.(32)
Since DECT scanners are commercially available it has been used to characterise
renal stones into uric acid and non- uric acid stones. Recent in vitro studies could
successfully separate five different types of kidney stones ie struvite, cysteine, uric
acid, calcium- oxalate mono or dihydrate and hydroxyapatite/carbonate apatite using
DECT.
Brown et al reported the feasibility of using dual energy CT iodine overlay images to
differentiate a renal cyst from a solid enhancing lesion in a phantom model.(33)
Graser et al reported virtual unenhanced images can provide a reasonable
approximation of true unenhanced images and accordingly can lower radiation
exposure in patients with suspected renal disease.(24)
Ascenti G et al showed enhancement of renal lesions is important when
differentiating benign from malignant tumours. Dual energy CT offers measurement
of iodine uptake rather than mere enhancement values. Whole-tumour iodine
quantification seems more accurate than standard CT enhancement measurements.(32)
MANAGEMENT OF RCC:
Surgery is the mainstay of treatment in cases of renal cell carcinoma. Open/
laparoscopic partial nephrectomy, and open/ laparoscopic radical nephrectomy are the
available surgical techniques and can be selected according to the tumour size, renal
function. Those who are not good surgical candidates can be offered with other
ablation procedures and Active surveillance.
Partial nephrectomy:
Partial nephrectomy is the standard of care for all T1a diseases and it should
be offered to T1b patients also where technically feasible or where renal function is of

concern. If done in properly selected patients there is no significant change in outcome
compared to the radical nephrectomy.
Radical Nephrectomy:
Radical nephrectomy is the standard of care for T2 and higher stage diseases. In T1b
diseases also radical nephrectomy can be offered to patients after discussing the increase in
chances of CKD. Laparoscopic approach is preferred wherever feasible as it facilitates faster
recovery. Advanced stage like IVC involvement of disease doesn’t preclude surgical
management. Routine adrenalectomy and extensive lymph node dissection is not
recommended when there is no evidence of involvement in imaging or during surgery.
Ablative procedures:
Different ablative procedures like cryoablation, radiofrequency ablation can be
offered in patients with tumour size <3 cm. Compared to partial nephrectomy
recurrence rate is higher in this group and later on surgical management is more
difficult. However in elderly patients and patients with major surgical risks or
comorbidities, this offers an alternative treatment as it is minimally invasive.
Active Surveillance:
Several studies have suggested very no or minimal interval growth over the
period of 1-2 years in majority of localised RCC.(34). So this is a valid option in
sporadic, small incidentally detected RCC, particularly in patients who have limited
life expectancy or have other major comorbidities. Wehle et al have shown that if
surgery cannot be done due to comorbid illness or due to patient’s wish, incidentally
detected RCC <3.5 cm and with well differentiated histopathology can do well with
watchful waiting and regular CT scan without any surgery.(35)
Cytoreductive surgery & Metastectomy: Can be done to reduce tumour burden
Systemic Therapy:
Different systemic chemotherapy protocols can be offered to patients with
metastatic disease after prognosis stratification and depending on the response.
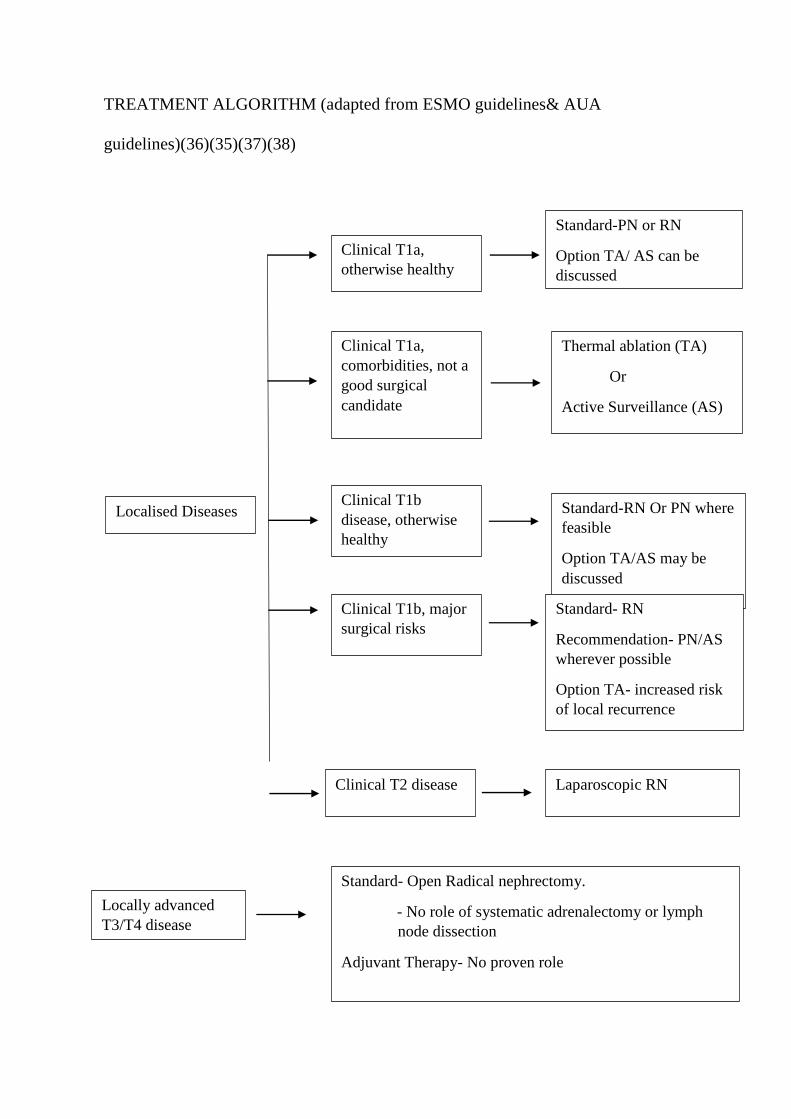
TREATMENT ALGORITHM (adapted from ESMO guidelines& AUA
guidelines)(36)(35)(37)(38)
Localised Diseases
Clinical T1a,
otherwise healthy
Standard-PN or RN
Option TA/ AS can be
discussed
Clinical T1a,
comorbidities, not a
good surgical
candidate
Thermal ablation (TA)
Or
Active Surveillance (AS)
Clinical T1b
disease, otherwise
healthy
Standard-RN Or PN where
feasible
Option TA/AS may be
discussed
Clinical T1b, major
surgical risks
Standard- RN
Recommendation- PN/AS
wherever possible
Option TA- increased risk
of local recurrence
Clinical T2 disease Laparoscopic RN
Locally advanced
T3/T4 disease
Standard- Open Radical nephrectomy.
- No role of systematic adrenalectomy or lymph
node dissection
Adjuvant Therapy- No proven role
*PN- Partial Nephrectomy, RN- Radical Nephrectomy, TA- Thermal Ablation, AS-
Active Surveillance
.
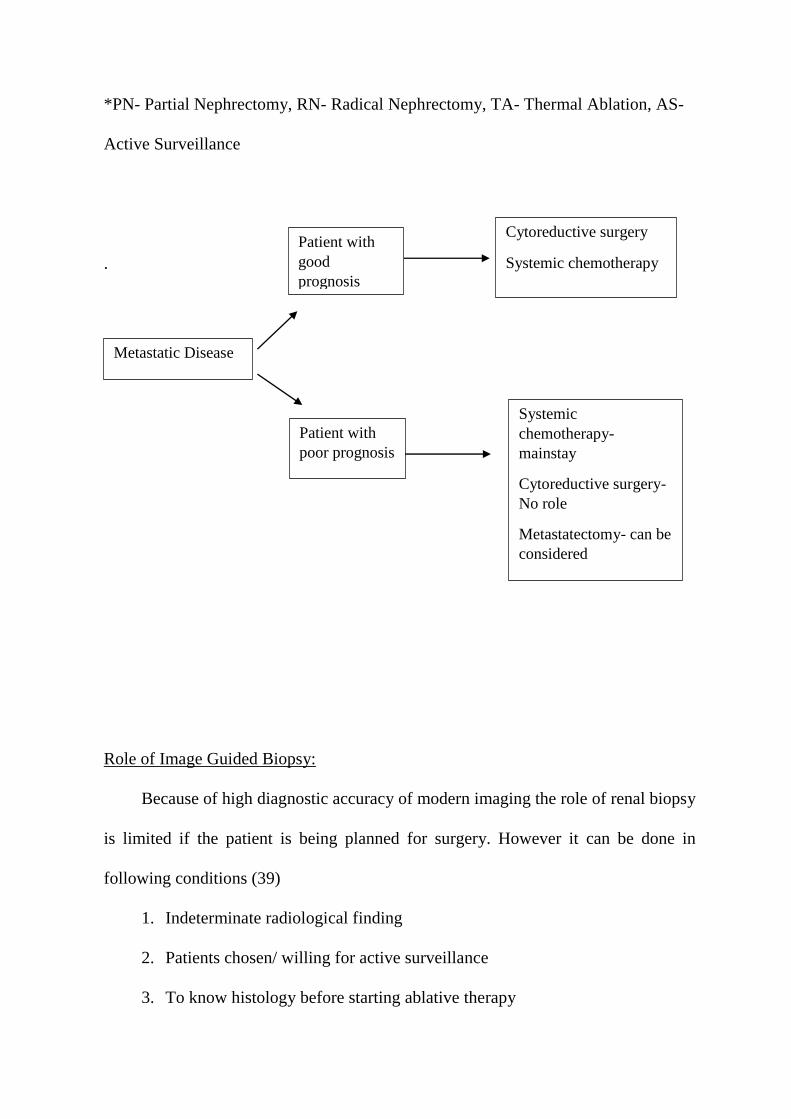
Role of Image Guided Biopsy:
Because of high diagnostic accuracy of modern imaging the role of renal biopsy
is limited if the patient is being planned for surgery. However it can be done in
following conditions (39)
1. Indeterminate radiological finding
2. Patients chosen/ willing for active surveillance
3. To know histology before starting ablative therapy
Metastatic Disease
Patient with
good
prognosis
Patient with
poor prognosis
Cytoreductive surgery
Systemic chemotherapy
Systemic
chemotherapy-
mainstay
Cytoreductive surgery-
No role
Metastatectomy- can be
considered
4. To select appropriate targeted therapeutic agent in patients with metastatic
disease
Core biopsies from solid renal tumours have very high diagnostic yield with
specificity 98-100% and sensitivity 86-100%. However very nuclear grading remains
challenging in core biopsy. Wang et al reported diagnostic accuracy as low as 46%.(3)
Overall, renal cell carcinoma can be considered as a heterogeneous group of
clinic-radio-pathologically different tumours. Each one is unique in clinical course and
prognosis. Fuhrman nuclear grade is another independent prognostic factor for the
renal cell carcinoma particularly of clear cell type. Different imaging findings has been
tested for assessing the type and grade of RCC. With the increase in number of
incidentally detected RCC, non-invasive/ minimally invasive way of typing and
grading appears to be the need of hour particularly in patients not a candidate for
surgery. Per cutaneous core biopsy can diagnose histologic type of RCC but core
biopsies cannot reliably depict nuclear grade. There are very few studies which had
attempted to correlate imaging findings with the nuclear grade.
With the above knowledge in mind we planned to correlate iodine concentration
in clear cell RCC using dual energy technique, with the Fuhrman nuclear grade of
RCC.
METHODS
STUDY DESIGN: Prospective
STUDY TYPE: Observational study.
This study was conducted in the department of radiology with collaboration with
departments of urology and pathology in Christian Medical College, Vellore.
STUDY PERIOD:
Patients were prospectively recruited from September 2014 to July 2016.
STUDY SETTING:
This study was conducted in the department of radiology with collaboration with
departments of urology and pathology in Christian Medical College, Vellore, which is
a tertiary care centre in south India with patients coming from all over India and also
from neighbouring countries like Bangladesh & Nepal. It has almost 2million annual
outpatient visits and in patient admission close to 130000.
STUDY POPULATION:
Inclusion Criteria:
All consecutive patients with known or suspected renal mass, referred for
preoperative CT scan and gave consent were initially recruited. However those who
underwent surgery in our institution during the study period and with histologically
proven clear cell subtype were finally included in analysis.
Exclusion Criteria:
Patients with known major contrast reaction and renal failure were excluded in
the study. Patients who were operated elsewhere or patients with renal tumour other
than clear cell RCC were also excluded from the study.
CT EXAMINATION:
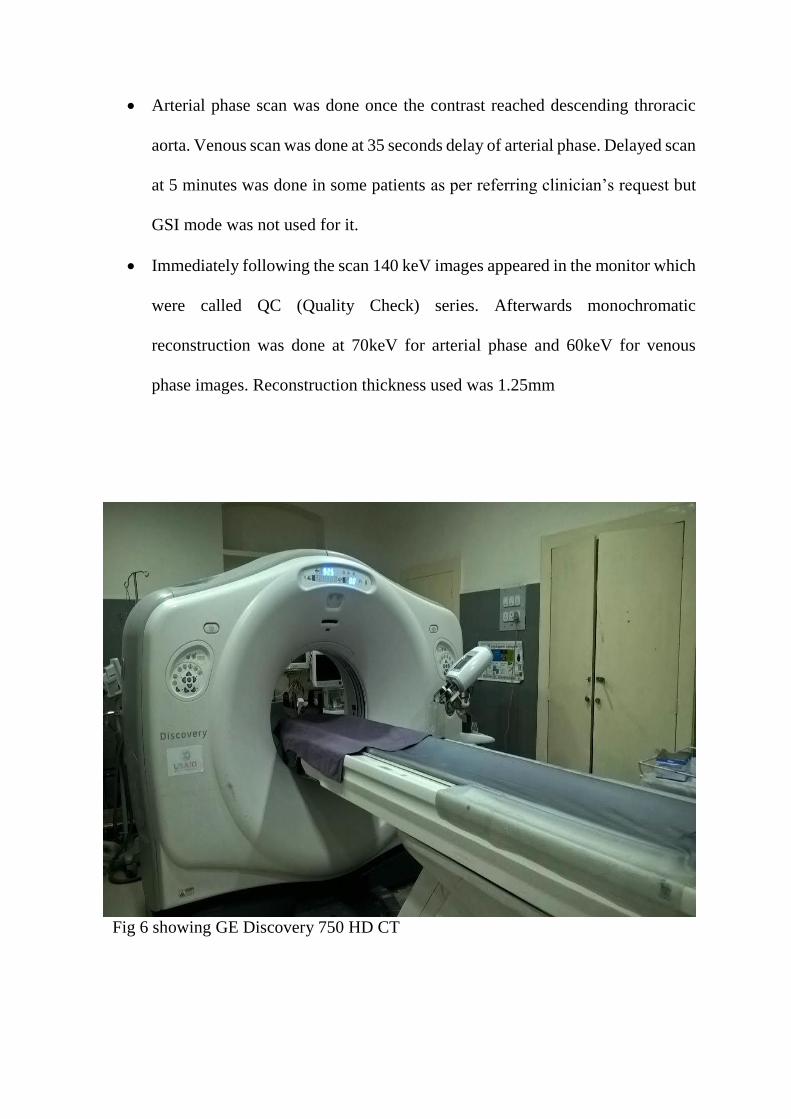
CT Machine: GE Discovery 750 HD
CT Protocol:
Post contrast enhanced multiphasic CT was done using GSI (Gemstone Spectral
Imaging) mode.
Parameters used are fixed pitch of 0.9, mAs of 275-400 depending on the
patient’s thickness.
80 ml of non-ionic iodinated contrast was administered at a rate of 3ml/s using
dual chamber power injector followed by 10 ml saline flush.
Contrast tracker was used to trigger the post contrast scan.
Arterial phase scan was done once the contrast reached descending throracic
aorta. Venous scan was done at 35 seconds delay of arterial phase. Delayed scan
at 5 minutes was done in some patients as per referring clinician’s request but
GSI mode was not used for it.
Immediately following the scan 140 keV images appeared in the monitor which
were called QC (Quality Check) series. Afterwards monochromatic
reconstruction was done at 70keV for arterial phase and 60keV for venous
phase images. Reconstruction thickness used was 1.25mm
Fig 6 showing GE Discovery 750 HD CT

Fig 7 showing nonionic contrast agents used for intravenous contrast in CT
CT Evaluation:
Evaluation of CT images were done in PACS using coded proforma.
DECT Post Processing:
Dual energy post processing was done in GE AWHD workstation using ‘GSI
Volume Viewer’ software.
It generated paired sets of water and iodine images. Iodine concentration was
measured in the iodine images in mg/ml.
Regions of interest (ROIs) in the RCC at three different levels in both arterial
and venous phases. Out of the three ROIs drawn in RCC one was drawn at the
level of maximum tumour dimension. Areas showing calcific densities were
excluded. Maximum, minimum, mean iodine concentrations and the area of
ROI at each level noted down.
ROIs are also drawn in aorta at the level of kidney and in normal kidney. Only
the mean iodine concentration in aorta and normal kidney were noted down in
arterial and venous phases.
While processing the iodine-images spectral HU curve was also obtained which
shows attenuation values (HU) of aorta, normal kidney and RCCs at different
keVs. The HU value at the 40keV where the separation between the curves were
maximum, were noted down.
Fig 8 showing GE AWHD workstation
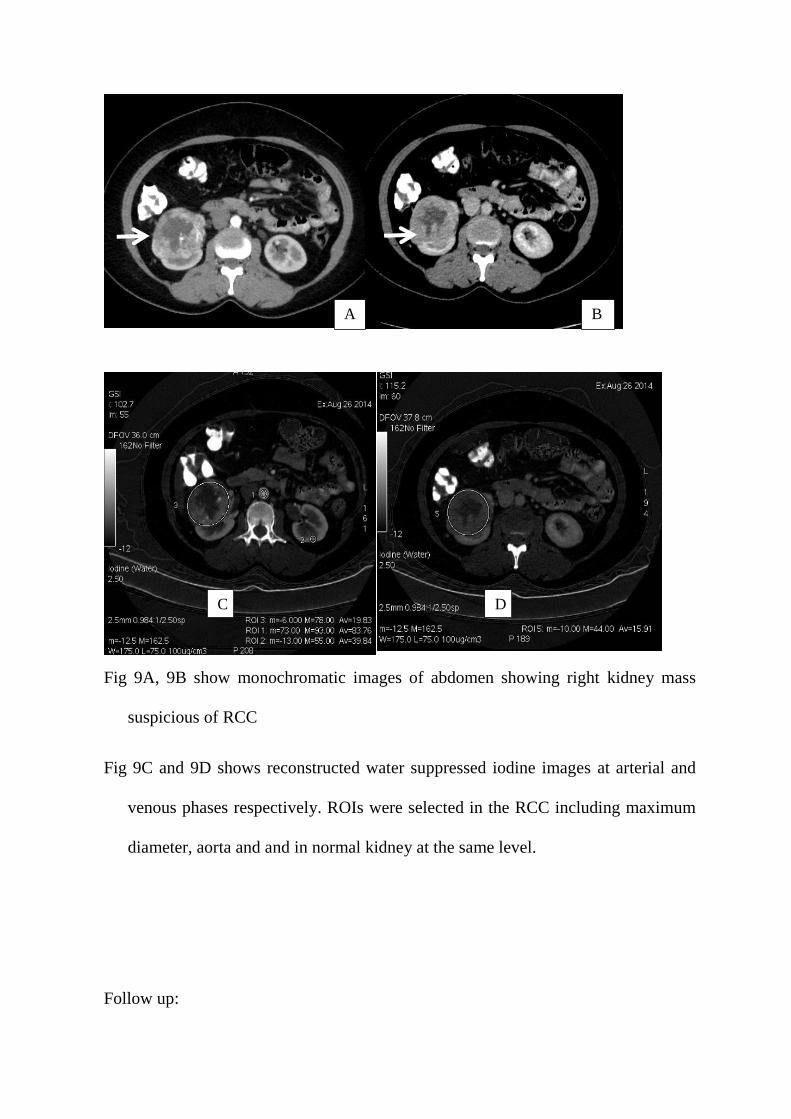
Fig 9A, 9B show monochromatic images of abdomen showing right kidney mass
suspicious of RCC
Fig 9C and 9D shows reconstructed water suppressed iodine images at arterial and
venous phases respectively. ROIs were selected in the RCC including maximum
diameter, aorta and and in normal kidney at the same level.
Follow up:
A B
C D
Patient was followed up till they have surgery or the limit of our time period.
Surgery, partial or radical nephrectomies were done in all the patients included
in final analysis.
Histopathological examination was done and reported in the department of
pathology.
Type of surgery done and histopathological findings as mentioned in coded
proforma were noted down.
VARIABLES:
Routine CT findings, Dual energy post processing data including Iodine
concentrations (Maximum, Minimum and Average) in RCC at three different levels as
well as mean iodine concentration in aorta and normal kidney. HU values at 40 Kev
where the separation of the curves are maximum were noted. Fuhrman nuclear grade
(1 to 4) of RCC were noted (details given in coded proforma)
DATA SOURCES:
Clinical workstation- basic patient details, CT report, pathology report
GE AWHD CT work station- dual energy post processing data
BIAS:
To avoid reporting bias post processing of dual energy images was done
immediately/ preoperatively. However the dual energy data was not be available to the
pathologist.
SAMPLE SIZE:
Sample size was calculated based on the results of the pilot study.
The mean iodine concentration in the RCC and the aorta in the arterial phase was used
for sample size calculation.
Standard Deviation in group I =9.5
Standard Deviation in group II =40
Mean Difference = 16 (Arterial phase mean iodine concentration in RCC compared to
aorta)
Effect size = 0.646464646464647
Alpha error (%) = 5
Power (%) = 80
Sided = Two
Required sample size per group= 104
QUANTITATIVE VARIABLES:
In RCC- maximum iodine concentration (Imax), Minimum iodine concentration
(Imin), mean iodine concentration (Imean) measured in arterial and venous phases
separately
In normal kidney- mean iodine concentration (Imean kid) measured in arterial
and venous phases.
STATISTICAL METHODS:
Mean with SD were evaluated for iodine concentration (arterial and
venous phases)
Mann Whitney U test was used to compare median iodine concentration
across the nuclear grades (1,2 vs 3,4)
ROC curve was plotted to find the best cut off for predicting the nuclear
grade
AUC (area under the curve) for iodine concentration was presented with
95% of confidence interval.
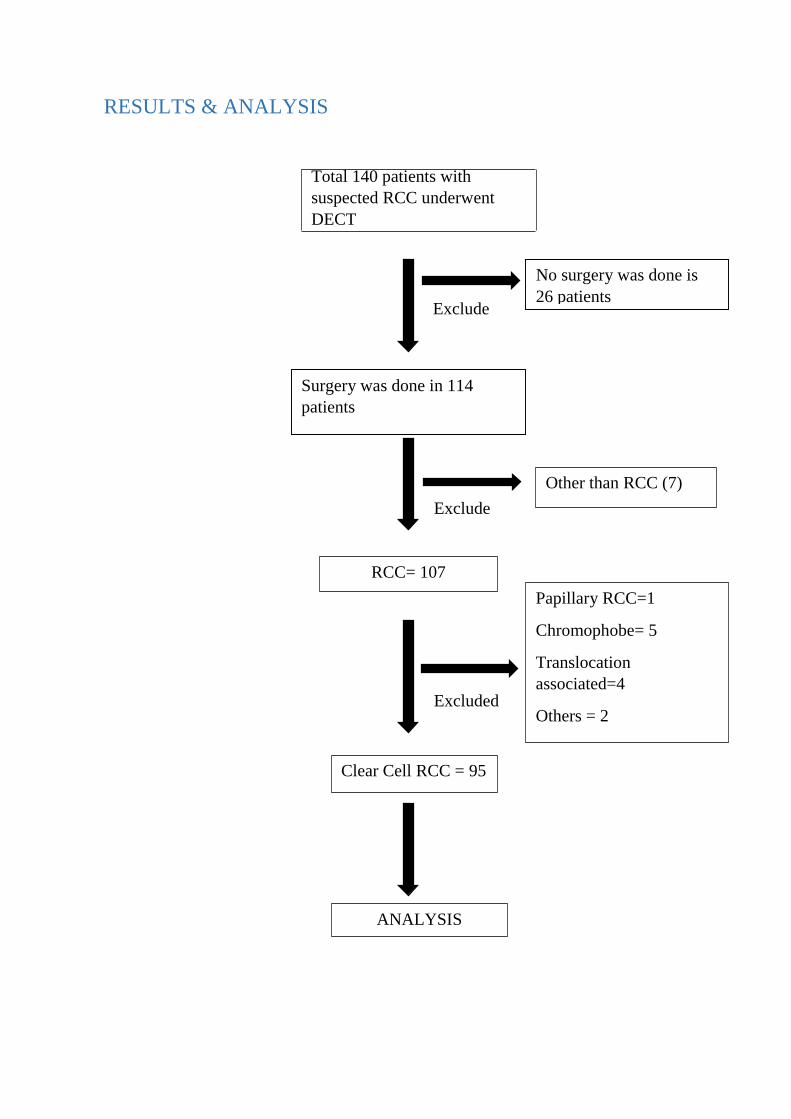
RESULTS & ANALYSIS
Total 140 patients with
suspected RCC underwent
DECT
No surgery was done is
26 patients
Surgery was done in 114
patients
Other than RCC (7)
RCC= 107
Clear Cell RCC = 95
Papillary RCC=1
Chromophobe= 5
Translocation
associated=4
Others = 2
ANALYSIS
Exclude
d
Exclude
d
Excluded
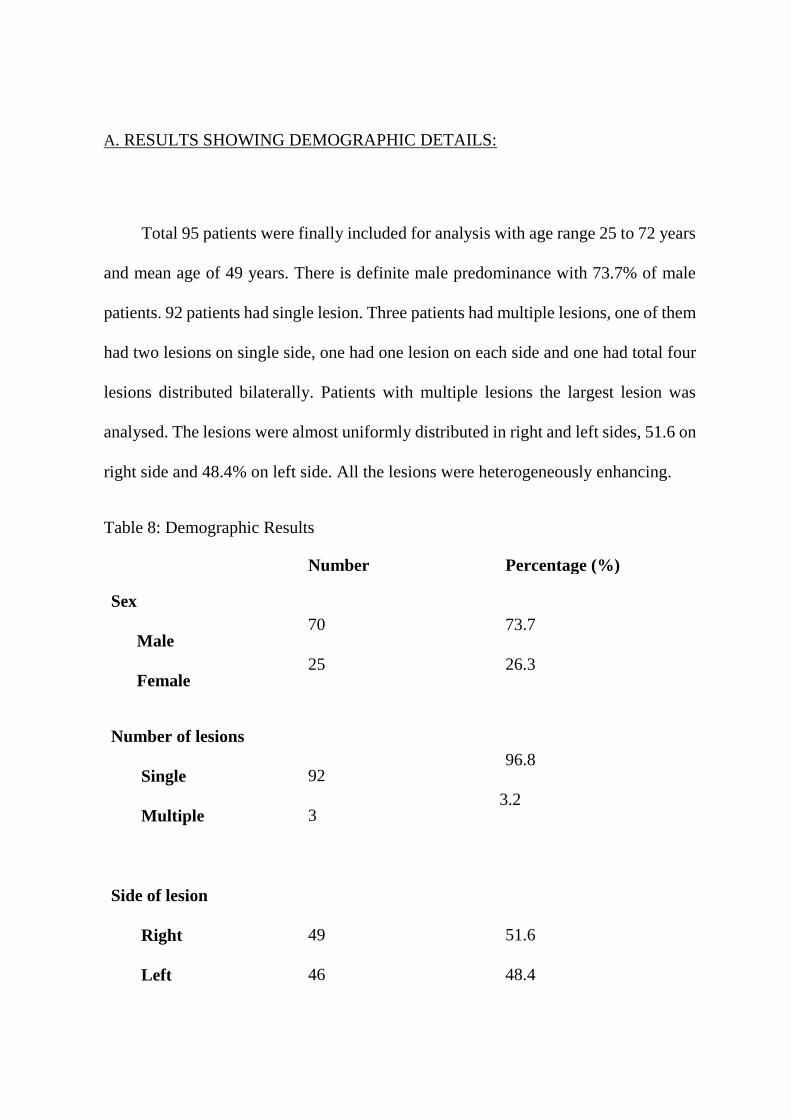
A. RESULTS SHOWING DEMOGRAPHIC DETAILS:
Total 95 patients were finally included for analysis with age range 25 to 72 years
and mean age of 49 years. There is definite male predominance with 73.7% of male
patients. 92 patients had single lesion. Three patients had multiple lesions, one of them
had two lesions on single side, one had one lesion on each side and one had total four
lesions distributed bilaterally. Patients with multiple lesions the largest lesion was
analysed. The lesions were almost uniformly distributed in right and left sides, 51.6 on
right side and 48.4% on left side. All the lesions were heterogeneously enhancing.
Table 8: Demographic Results
Number Percentage (%)
Sex
Male
Female
70
25
73.7
26.3
Number of lesions
Single
Multiple
92
3
96.8
3.2
Side of lesion
Right
Left
49
46
51.6
48.4
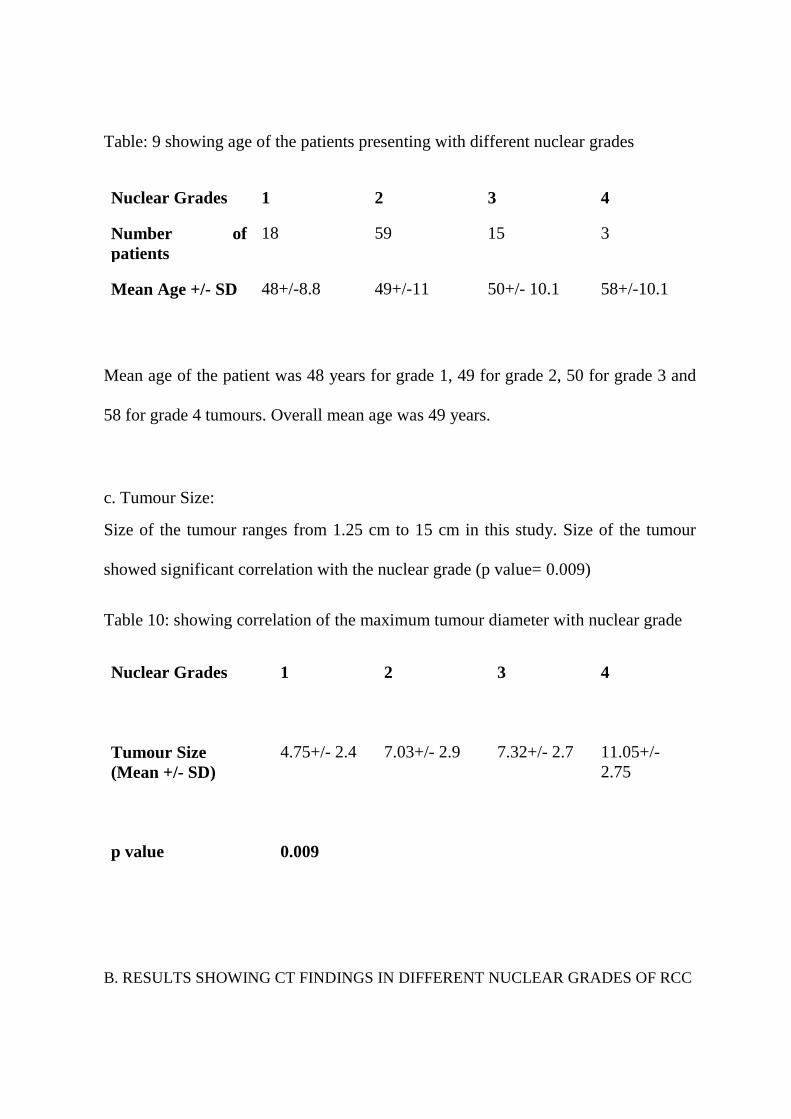
Table: 9 showing age of the patients presenting with different nuclear grades
Nuclear Grades 1 2 3 4
Number of
patients
18 59 15 3
Mean Age +/- SD 48+/-8.8 49+/-11 50+/- 10.1 58+/-10.1
Mean age of the patient was 48 years for grade 1, 49 for grade 2, 50 for grade 3 and
58 for grade 4 tumours. Overall mean age was 49 years.
c. Tumour Size:
Size of the tumour ranges from 1.25 cm to 15 cm in this study. Size of the tumour
showed significant correlation with the nuclear grade (p value= 0.009)
Table 10: showing correlation of the maximum tumour diameter with nuclear grade
Nuclear Grades
1
2
3
4
Tumour Size
(Mean +/- SD)
4.75+/- 2.4
7.03+/- 2.9
7.32+/- 2.7
11.05+/-
2.75
p value
0.009
B. RESULTS SHOWING CT FINDINGS IN DIFFERENT NUCLEAR GRADES OF RCC
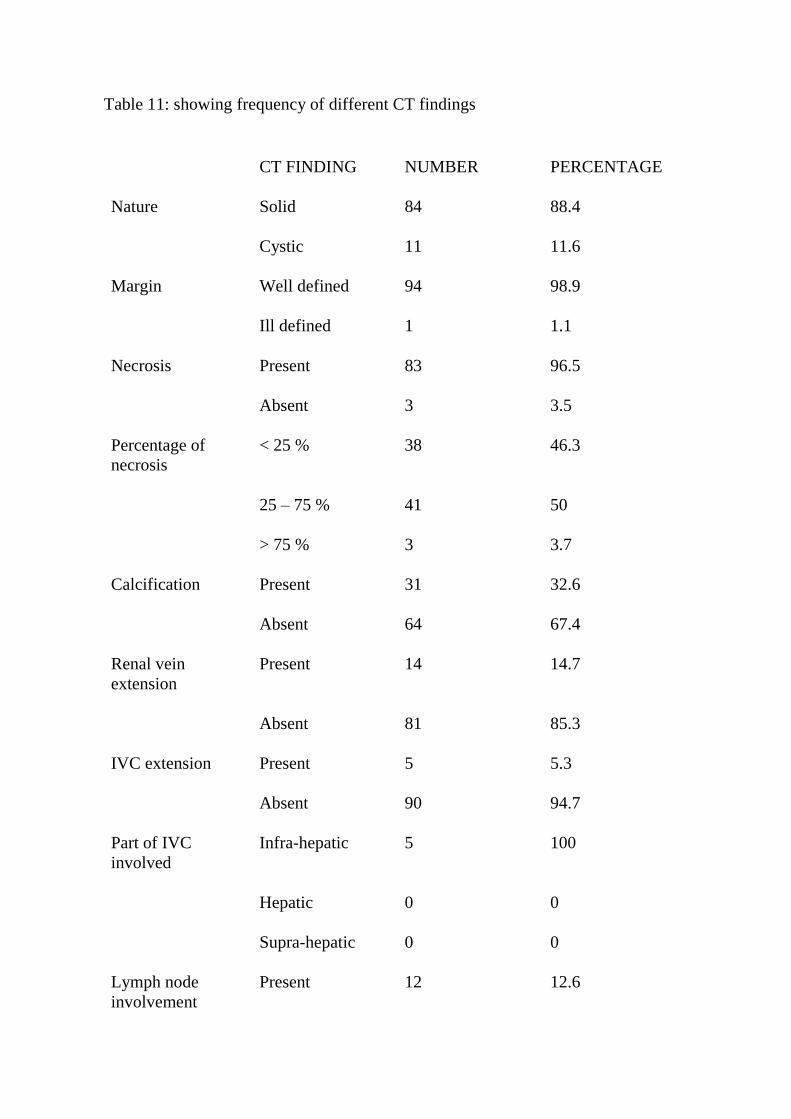
Table 11: showing frequency of different CT findings
CT FINDING NUMBER PERCENTAGE
Nature Solid 84 88.4
Cystic 11 11.6
Margin Well defined 94 98.9
Ill defined 1 1.1
Necrosis Present 83 96.5
Absent 3 3.5
Percentage of
necrosis
< 25 % 38 46.3
25 – 75 % 41 50
> 75 % 3 3.7
Calcification Present 31 32.6
Absent 64 67.4
Renal vein
extension
Present 14 14.7
Absent 81 85.3
IVC extension Present 5 5.3
Absent 90 94.7
Part of IVC
involved
Infra-hepatic 5 100
Hepatic 0 0
Supra-hepatic 0 0
Lymph node
involvement
Present 12 12.6
Absent 83 87.4
Distant metastasis Present 5 5.3
Absent 90 94.7
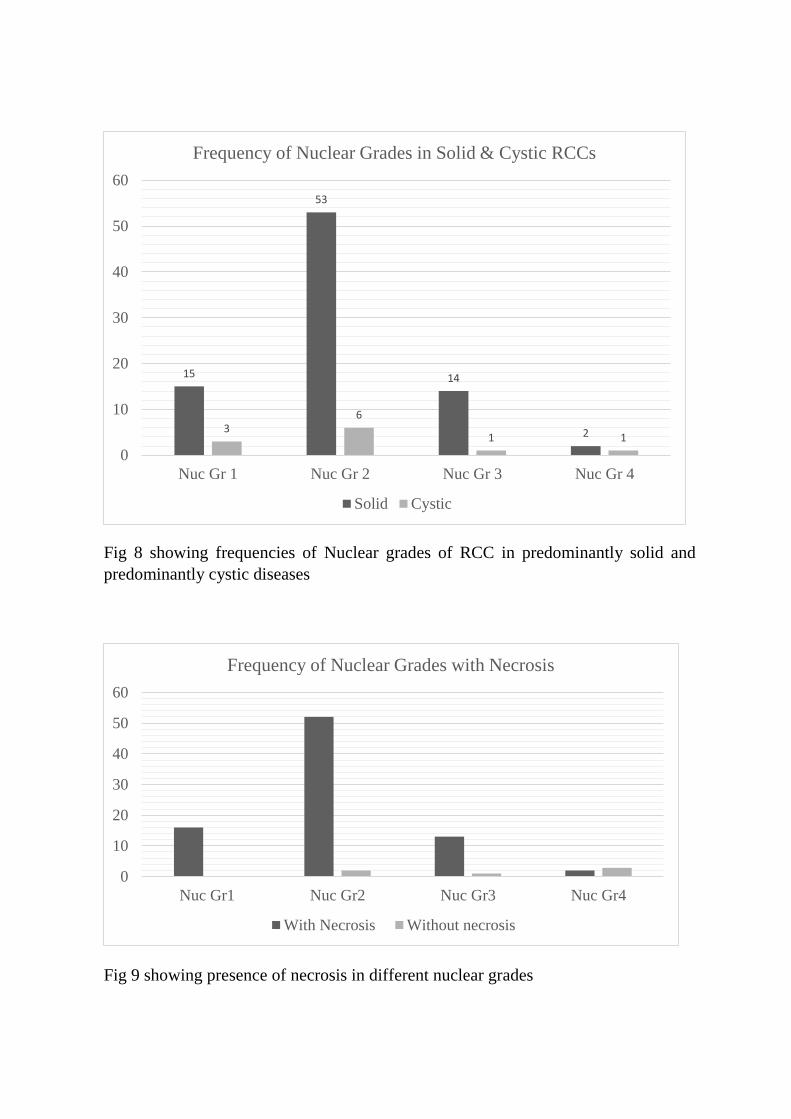
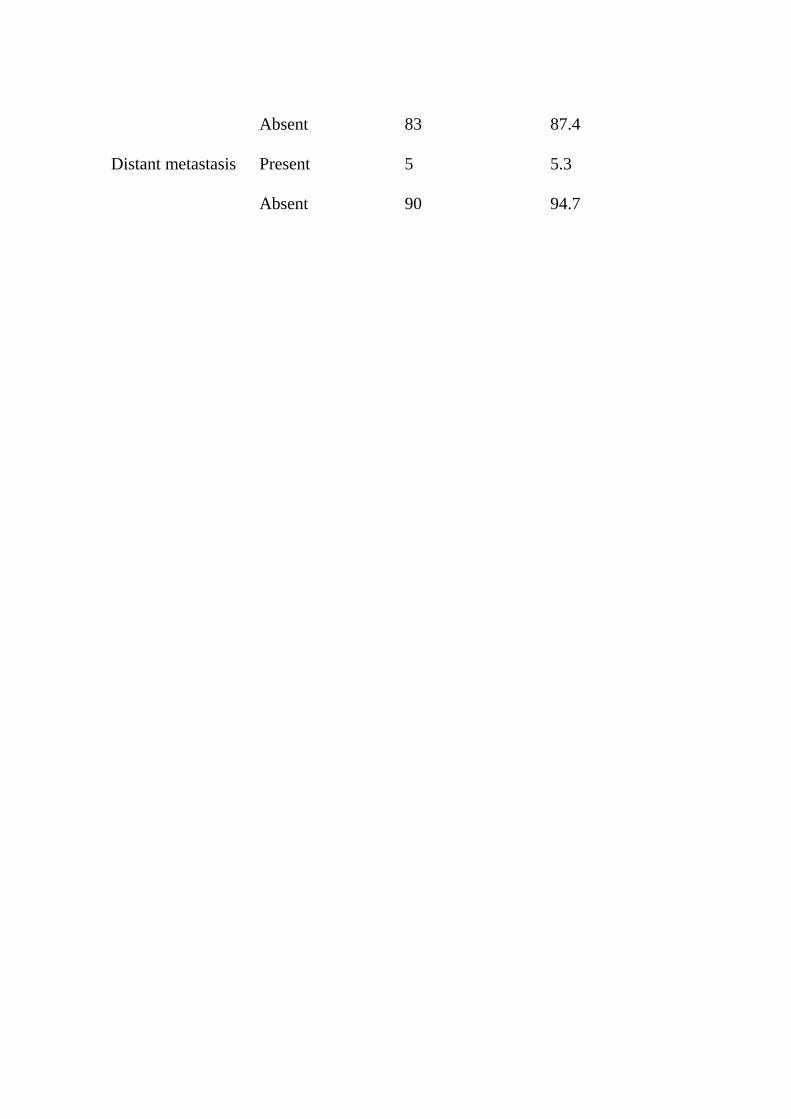
Fig 8 showing frequencies of Nuclear grades of RCC in predominantly solid and
predominantly cystic diseases
Fig 9 showing presence of necrosis in different nuclear grades
15
53
14
236
1 1
0
10
20
30
40
50
60
Nuc Gr 1 Nuc Gr 2 Nuc Gr 3 Nuc Gr 4
Frequency of Nuclear Grades in Solid & Cystic RCCs
Solid Cystic
0
10
20
30
40
50
60
Nuc Gr1 Nuc Gr2 Nuc Gr3 Nuc Gr4
Frequency of Nuclear Grades with Necrosis
With Necrosis Without necrosis
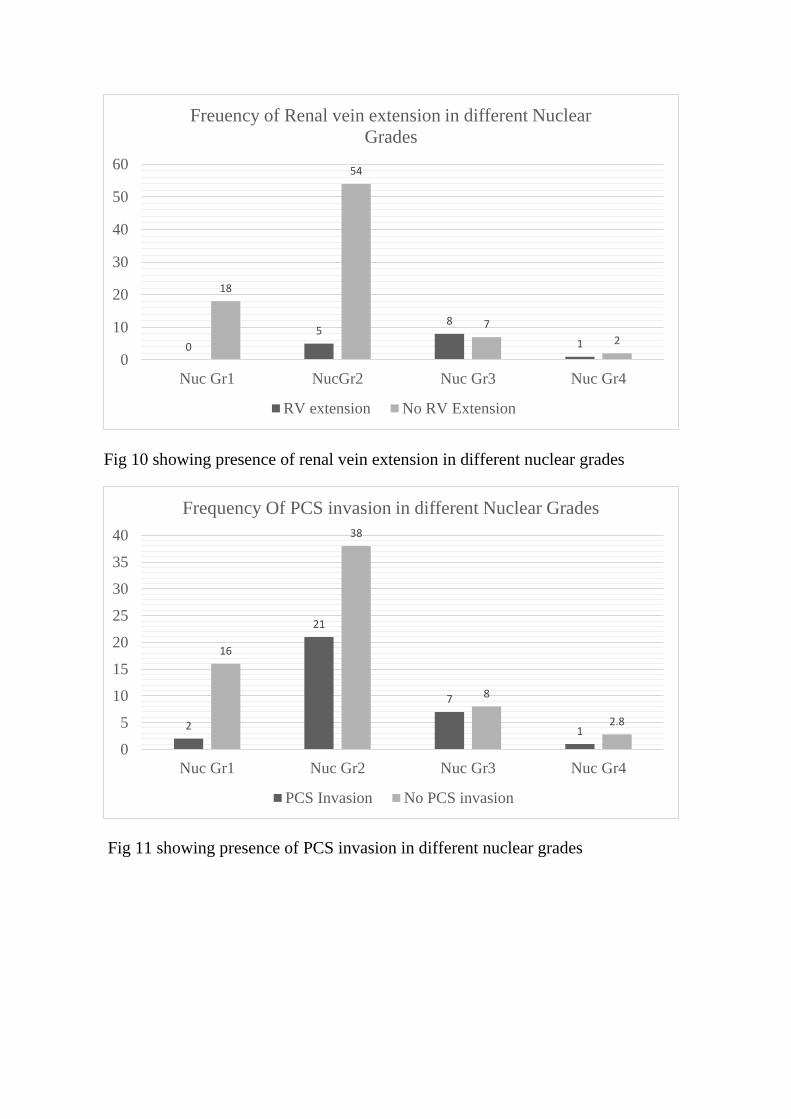
Fig 10 showing presence of renal vein extension in different nuclear grades
Fig 11 showing presence of PCS invasion in different nuclear grades
0
58
1
18
54
7
2
0
10
20
30
40
50
60
Nuc Gr1 NucGr2 Nuc Gr3 Nuc Gr4
Freuency of Renal vein extension in different Nuclear
Grades
RV extension No RV Extension
2
21
7
1
16
38
8
2.8
0
5
10
15
20
25
30
35
40
Nuc Gr1 Nuc Gr2 Nuc Gr3 Nuc Gr4
Frequency Of PCS invasion in different Nuclear Grades
PCS Invasion No PCS invasion
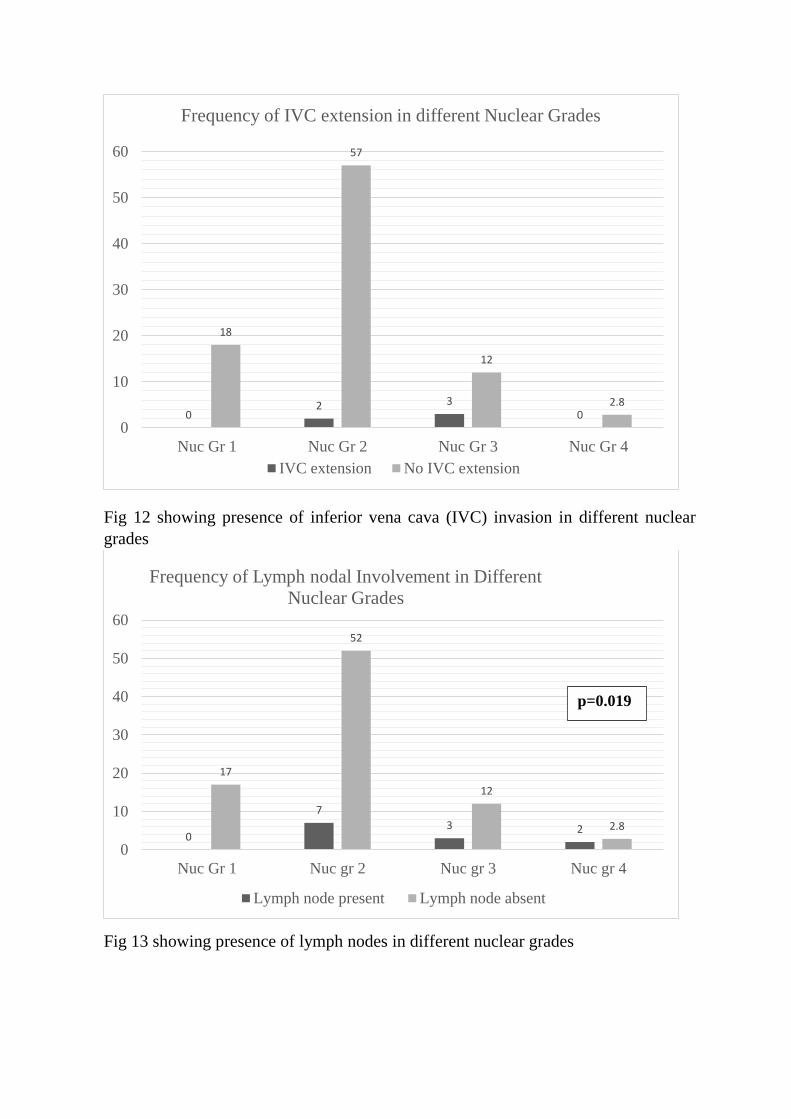
Fig 12 showing presence of inferior vena cava (IVC) invasion in different nuclear
grades
Fig 13 showing presence of lymph nodes in different nuclear grades
02 3
0
18
57
12
2.8
0
10
20
30
40
50
60
Nuc Gr 1 Nuc Gr 2 Nuc Gr 3 Nuc Gr 4
Frequency of IVC extension in different Nuclear Grades
IVC extension No IVC extension
0
7
3 2
17
52
12
2.8
0
10
20
30
40
50
60
Nuc Gr 1 Nuc gr 2 Nuc gr 3 Nuc gr 4
Frequency of Lymph nodal Involvement in Different
Nuclear Grades
Lymph node present Lymph node absent
p=0.019

Fig 14 showing presence of calcification in different nuclear grades
Fig 15 showing frequency of distal metastases in different nuclear grades
3
12
0 0
14
47
15
3
0
5
10
15
20
25
30
35
40
45
50
Nuc Gr 1 Nuc Gr 2 Nuc Gr 3 Nuc Gr 4
Frequency of calcification in Different Nuclear Grades
Calcification No calcification
02 3
0
18
56
12
3
0
10
20
30
40
50
60
Nuc Gr1 Nuc Gr2 Nuc Gr3 Nuc Gr4
Frequency of Distal metastases in different Nuclear Grades
Distal Mets No distal mets
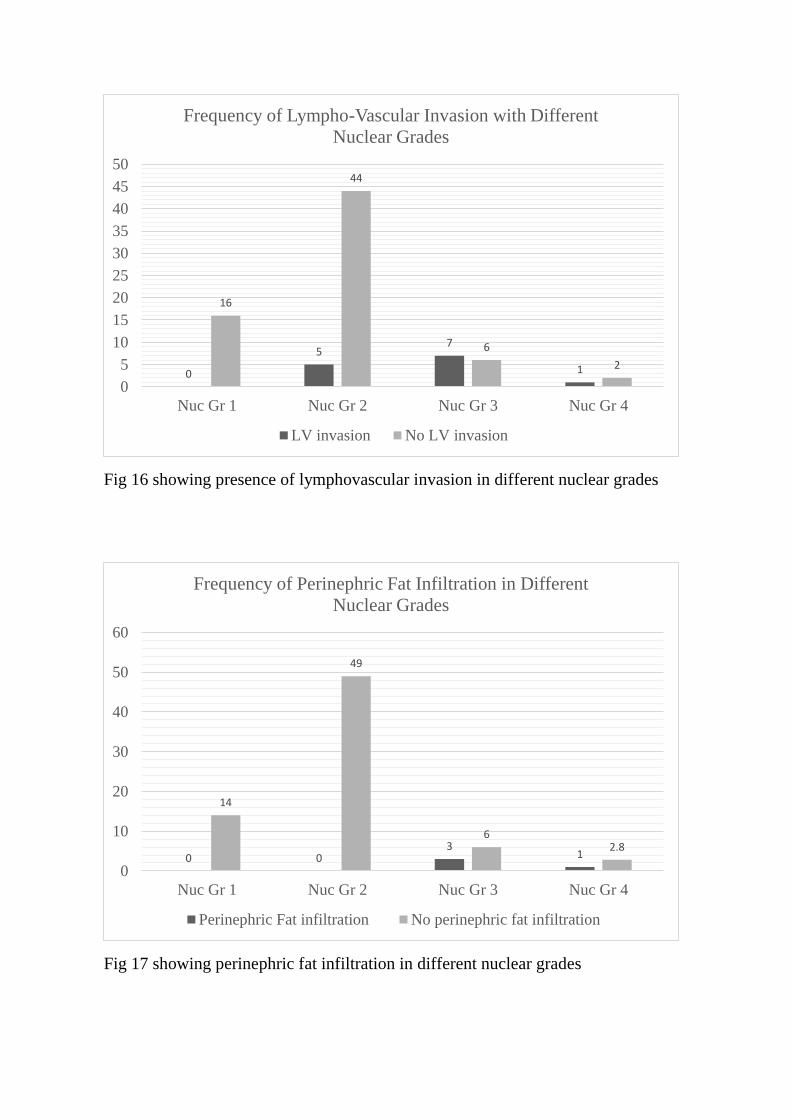
Fig 16 showing presence of lymphovascular invasion in different nuclear grades
Fig 17 showing perinephric fat infiltration in different nuclear grades
0
57
1
16
44
6
2
0
5
10
15
20
25
30
35
40
45
50
Nuc Gr 1 Nuc Gr 2 Nuc Gr 3 Nuc Gr 4
Frequency of Lympho-Vascular Invasion with Different
Nuclear Grades
LV invasion No LV invasion
0 03
1
14
49
62.8
0
10
20
30
40
50
60
Nuc Gr 1 Nuc Gr 2 Nuc Gr 3 Nuc Gr 4
Frequency of Perinephric Fat Infiltration in Different
Nuclear Grades
Perinephric Fat infiltration No perinephric fat infiltration
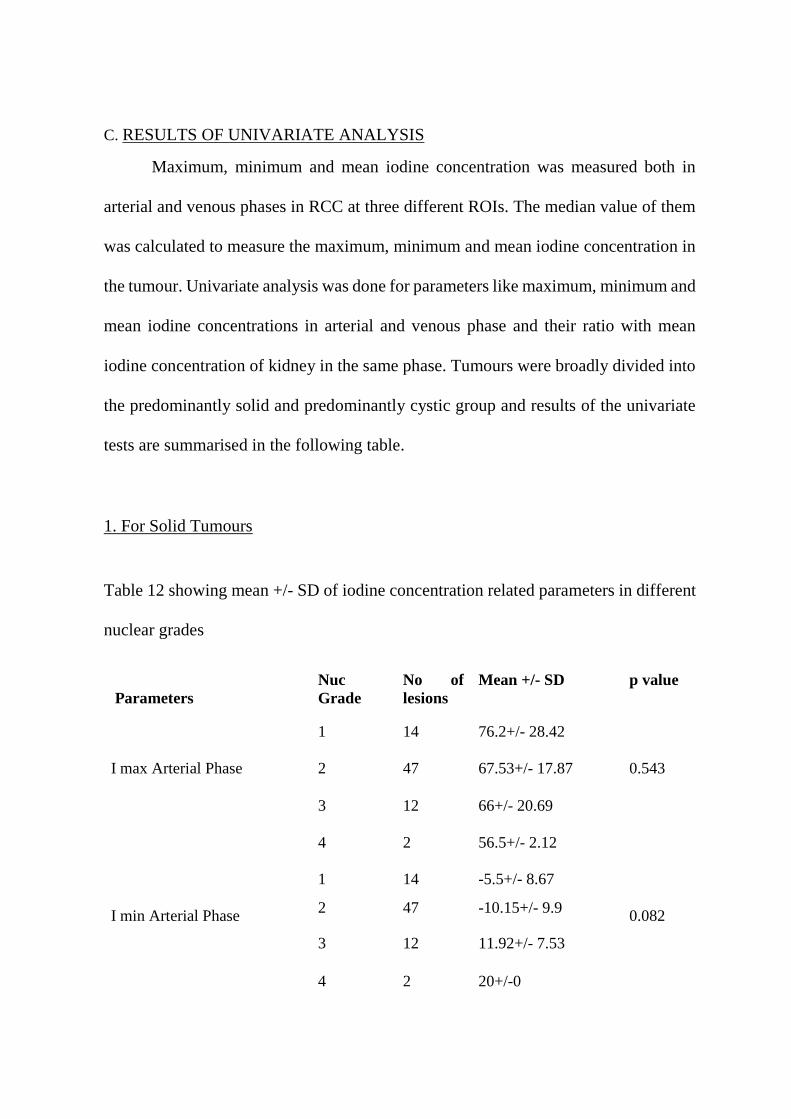
C. RESULTS OF UNIVARIATE ANALYSIS
Maximum, minimum and mean iodine concentration was measured both in
arterial and venous phases in RCC at three different ROIs. The median value of them
was calculated to measure the maximum, minimum and mean iodine concentration in
the tumour. Univariate analysis was done for parameters like maximum, minimum and
mean iodine concentrations in arterial and venous phase and their ratio with mean
iodine concentration of kidney in the same phase. Tumours were broadly divided into
the predominantly solid and predominantly cystic group and results of the univariate
tests are summarised in the following table.
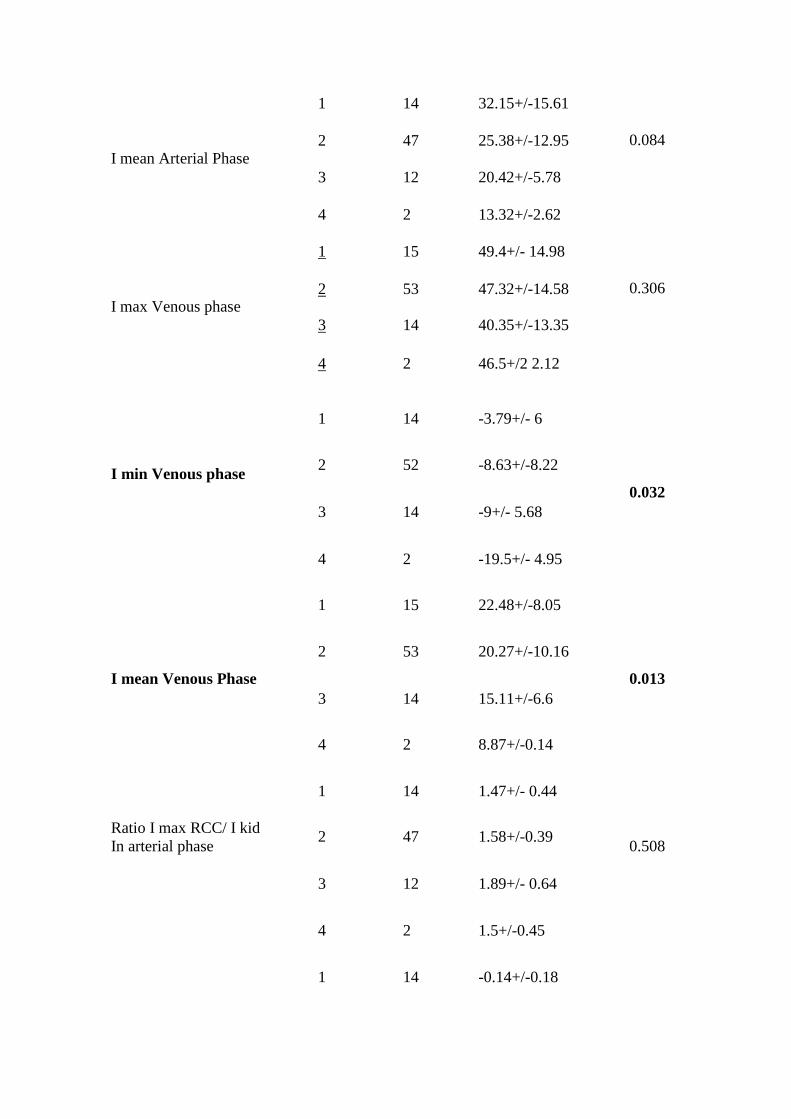
1. For Solid Tumours
Table 12 showing mean +/- SD of iodine concentration related parameters in different
nuclear grades
Parameters
Nuc
Grade
No of
lesions
Mean +/- SD p value
I max Arterial Phase
1 14 76.2+/- 28.42
0.543 2 47 67.53+/- 17.87
3 12 66+/- 20.69
4 2 56.5+/- 2.12
I min Arterial Phase
1 14 -5.5+/- 8.67
0.082 2 47 -10.15+/- 9.9
3 12 11.92+/- 7.53
4 2 20+/-0
I mean Arterial Phase
1 14 32.15+/-15.61
0.084 2 47 25.38+/-12.95
3 12 20.42+/-5.78
4 2 13.32+/-2.62
I max Venous phase
1 15 49.4+/- 14.98
0.306 2 53 47.32+/-14.58
3 14 40.35+/-13.35
4 2 46.5+/2 2.12
I min Venous phase
1 14 -3.79+/- 6
0.032
2 52 -8.63+/-8.22
3 14 -9+/- 5.68
4 2 -19.5+/- 4.95
I mean Venous Phase
1 15 22.48+/-8.05
0.013
2 53 20.27+/-10.16
3 14 15.11+/-6.6
4 2 8.87+/-0.14
Ratio I max RCC/ I kid
In arterial phase
1 14 1.47+/- 0.44
0.508 2 47 1.58+/-0.39
3 12 1.89+/- 0.64
4 2 1.5+/-0.45
1 14 -0.14+/-0.18

Ratio I min RCC/I kid in
arterial phase
2 47 -0.28+/-0.27
0.042 3 12 -0.37+/-0.29
4 2 -0.53+/-0.14
Ratio I mean RCC/ I kid in
arterial phase
1 14 0.6+/-0.21
0.457
2 47 0.57+/-0.24
3 12 0.59+/-0.17
4 2 0.34+/-0.02
Ratio I max RCC/ I kid
Venous phase
1 15 1.09+/-0.32
0.566 2 53 1.11+/-0.27
3 14 1.07+/-0.22
4 2 1.3+/- 0.19
Ratio I min RCC/I kid
Venous phase
1 14 -0.099+/-0.15
0.032
2 52 -0.24+/-0.23
3 14 -0.26+/-0.19
4 2 -0.56+/-0.25
Ratio I mean RCC/I kid
Venous phase
1 15 22.48+/-8.05
0.082
2 53 20.27+/-10.15
3 14 15.10+/-6.6
4 2 8.8+/- 0.14
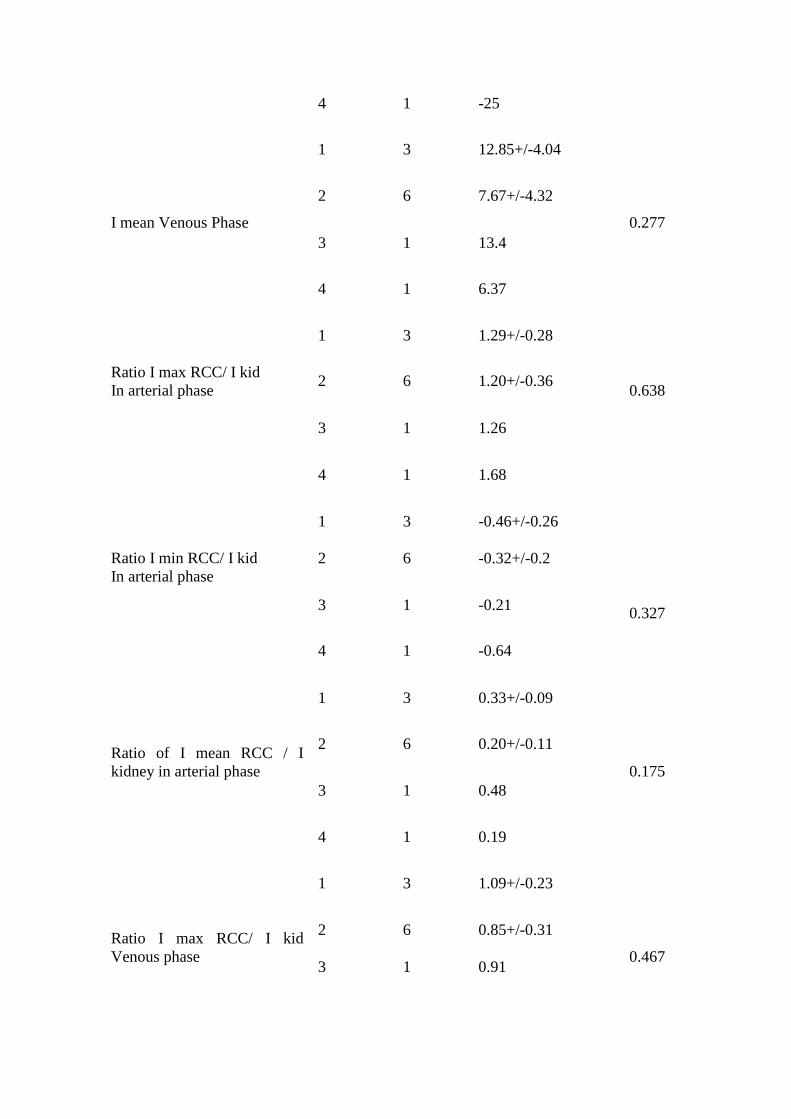
2. For Cystic Tumours
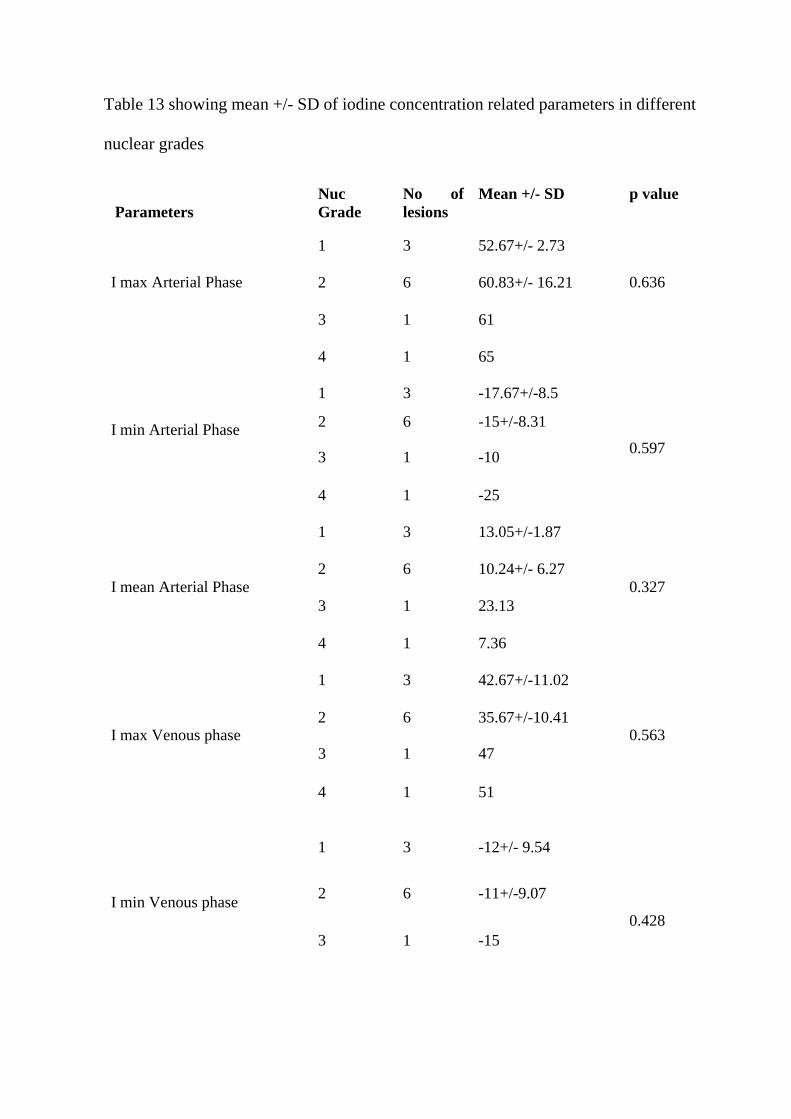
Table 13 showing mean +/- SD of iodine concentration related parameters in different
nuclear grades
Parameters
Nuc
Grade
No of
lesions
Mean +/- SD p value
I max Arterial Phase
1 3 52.67+/- 2.73
0.636 2 6 60.83+/- 16.21
3 1 61
4 1 65
I min Arterial Phase
1 3 -17.67+/-8.5
0.597
2 6 -15+/-8.31
3 1 -10
4 1 -25
I mean Arterial Phase
1 3 13.05+/-1.87
0.327 2 6 10.24+/- 6.27
3 1 23.13
4 1 7.36
I max Venous phase
1 3 42.67+/-11.02
0.563 2 6 35.67+/-10.41
3 1 47
4 1 51
I min Venous phase
1 3 -12+/- 9.54
0.428
2 6 -11+/-9.07
3 1 -15
4 1 -25
I mean Venous Phase
1 3 12.85+/-4.04
0.277
2 6 7.67+/-4.32
3 1 13.4
4 1 6.37
Ratio I max RCC/ I kid
In arterial phase
1 3 1.29+/-0.28
0.638 2 6 1.20+/-0.36
3 1 1.26
4 1 1.68
Ratio I min RCC/ I kid
In arterial phase
1 3 -0.46+/-0.26
0.327
2 6 -0.32+/-0.2
3 1 -0.21
4 1 -0.64
Ratio of I mean RCC / I
kidney in arterial phase
1 3 0.33+/-0.09
0.175
2 6 0.20+/-0.11
3 1 0.48
4 1 0.19
Ratio I max RCC/ I kid
Venous phase
1 3 1.09+/-0.23
0.467
2 6 0.85+/-0.31
3 1 0.91

4 1 1.31
Ratio I min RCC/ I kid
Venous phase
1 3 -0.33+/- 0.24
0.447
2 6 - 0.28+/- 0.23
3 1 -0.29
4 1 -0.64
Ratio I mean RCC/I kid
Venous phase
1 3 0.33+/-0.0.09
0.304
2 6 0.18+/- 0.11
3 1 0.3040.26
4 1 0.16
For solid tumours the minimum venous phase iodine concentration (vImin),
mean venous phase iodine concentration (vImean), ratio of minimum venous phase
iodine concentration to mean kidney iodine concentration (vImin/ vIkid) and ratio of
minimum iodine arterial phase iodine concentration to mean kidney iodine
concentration (aImin/aIkid) showed significant correlation.
For cystic tumours iodine concentration did not show significant correlation
with nuclear grades.
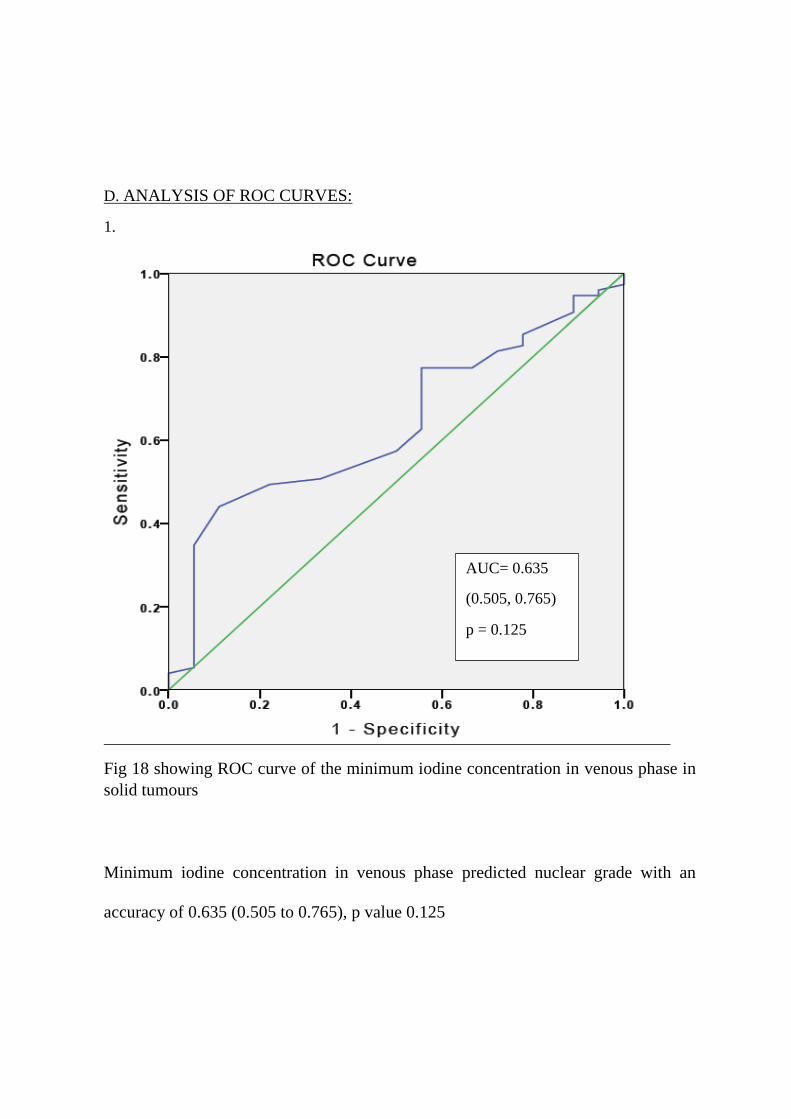
D. ANALYSIS OF ROC CURVES:
1.
Fig 18 showing ROC curve of the minimum iodine concentration in venous phase in
solid tumours
Minimum iodine concentration in venous phase predicted nuclear grade with an
accuracy of 0.635 (0.505 to 0.765), p value 0.125
AUC= 0.635
(0.505, 0.765)
p = 0.125

2.
Fig 19: showing ROC curve for Ratio of venous minimum iodine concentration in
RCC to mean kidney iodine concentration.
The ratio of minimum iodine concentration in venous phase to venous mean iodine
concentration in kidney predicted nuclear grade with an accuracy of 0.648 (00.509,
0.786) and p value 0.068
AUC=0.648
p value= 0.068
CI=0.509, 0.786
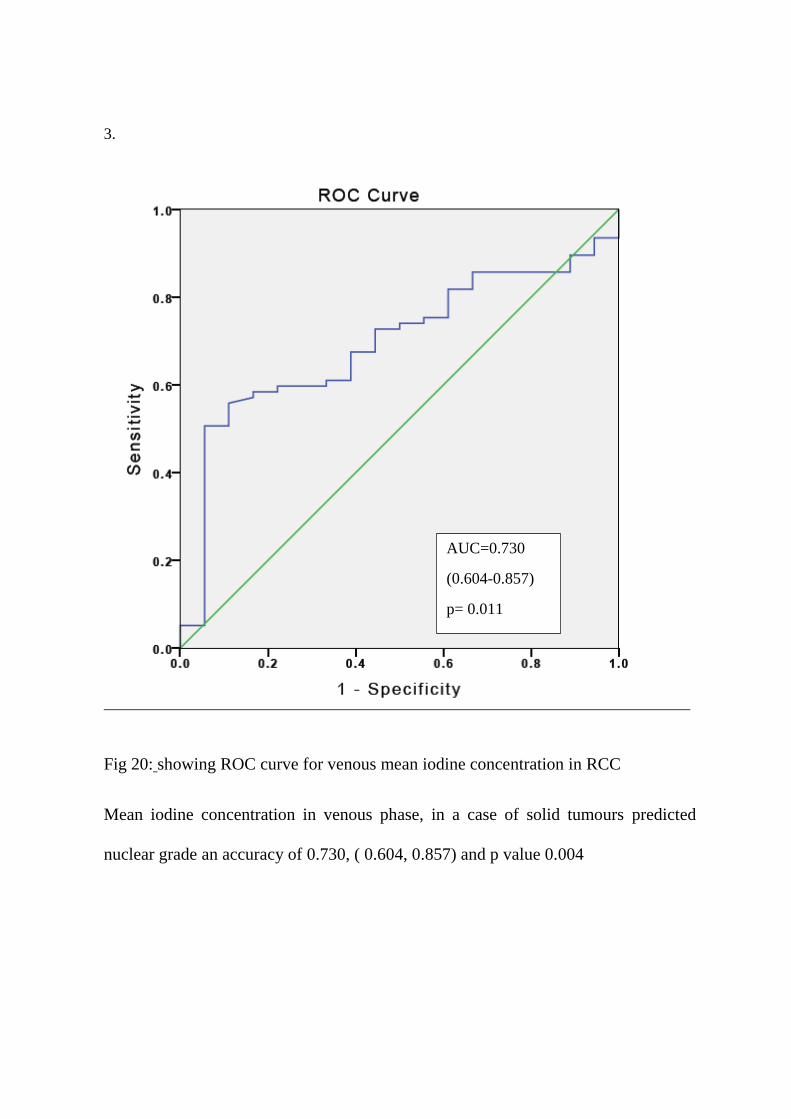
3.
Fig 20: showing ROC curve for venous mean iodine concentration in RCC
Mean iodine concentration in venous phase, in a case of solid tumours predicted
nuclear grade an accuracy of 0.730, ( 0.604, 0.857) and p value 0.004
AUC=0.730
(0.604-0.857)
p= 0.011

Fig 21 showing ROC curve for ratio of minimum arterial Iodine concentration in RCC
to mean arterial concentration of kidney
The ratio of minimum iodine concentration in arterial phase to arterial mean iodine
concentration in kidney predicted nuclear grade with an accuracy of 0.644
(0.477,0.811) and p value 0.094.
AUC= 0.644
().477- 0.811)
p=0.094
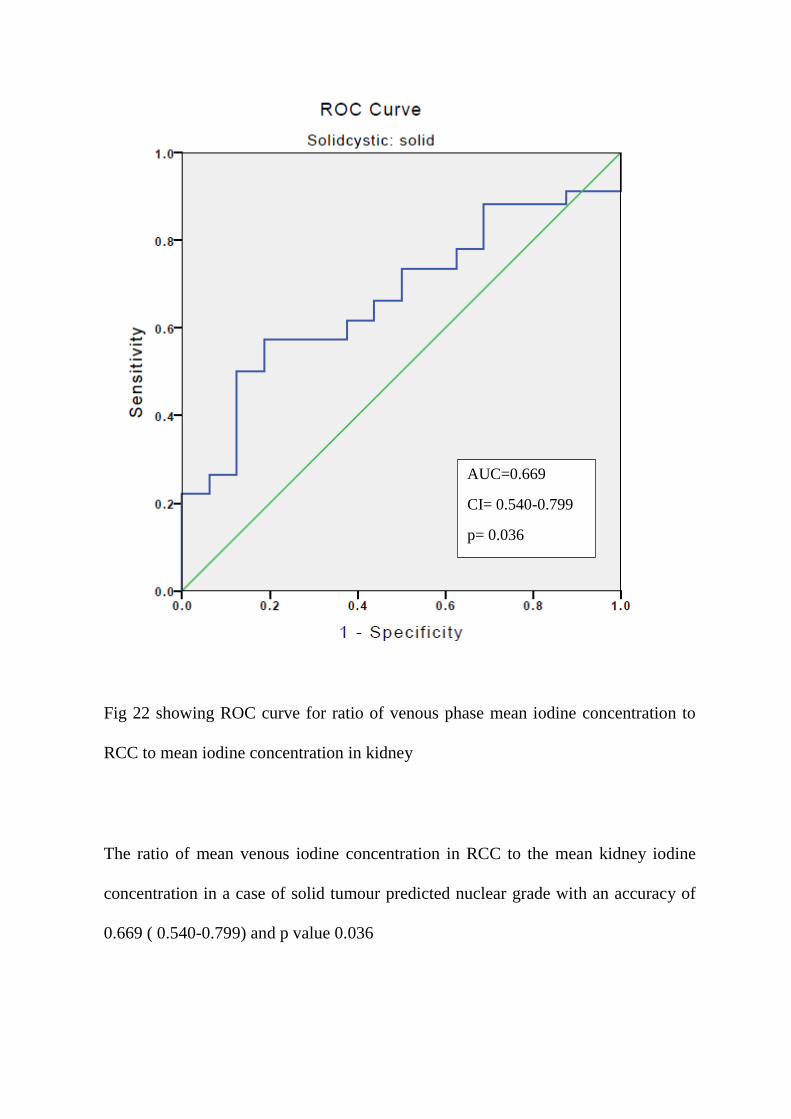
Fig 22 showing ROC curve for ratio of venous phase mean iodine concentration to
RCC to mean iodine concentration in kidney
The ratio of mean venous iodine concentration in RCC to the mean kidney iodine
concentration in a case of solid tumour predicted nuclear grade with an accuracy of
0.669 ( 0.540-0.799) and p value 0.036
AUC=0.669
CI= 0.540-0.799
p= 0.036

6.
Fig 23 showing ROC curve for ratio of venous phase maximum iodine concentration
in RCC to mean iodine concentration in kidney
The ROC curve shows that ratio of maximum venous phase iodine concentration in
RCC to mean iodine concentration in kidney, in a case of solid tumour does not help
in predicting the chance with nuclear grades.
AUC= 0.473
p= 0.741
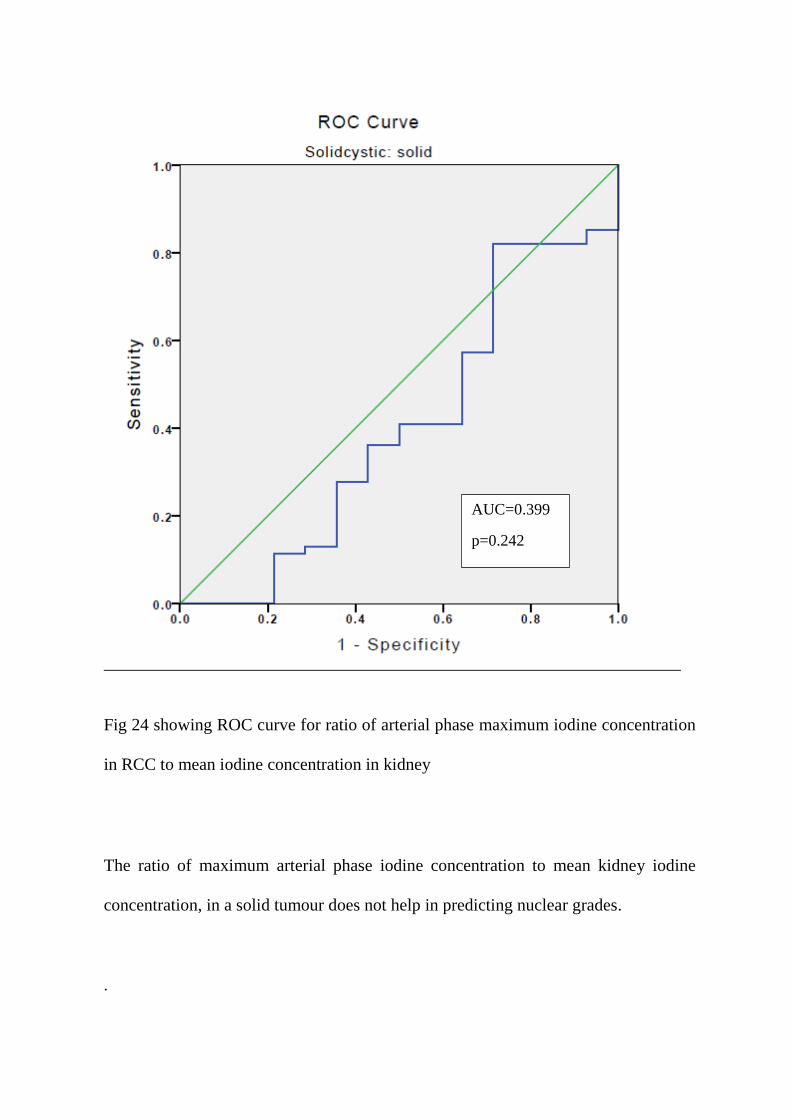
Fig 24 showing ROC curve for ratio of arterial phase maximum iodine concentration
in RCC to mean iodine concentration in kidney
The ratio of maximum arterial phase iodine concentration to mean kidney iodine
concentration, in a solid tumour does not help in predicting nuclear grades.
.
AUC=0.399
p=0.242
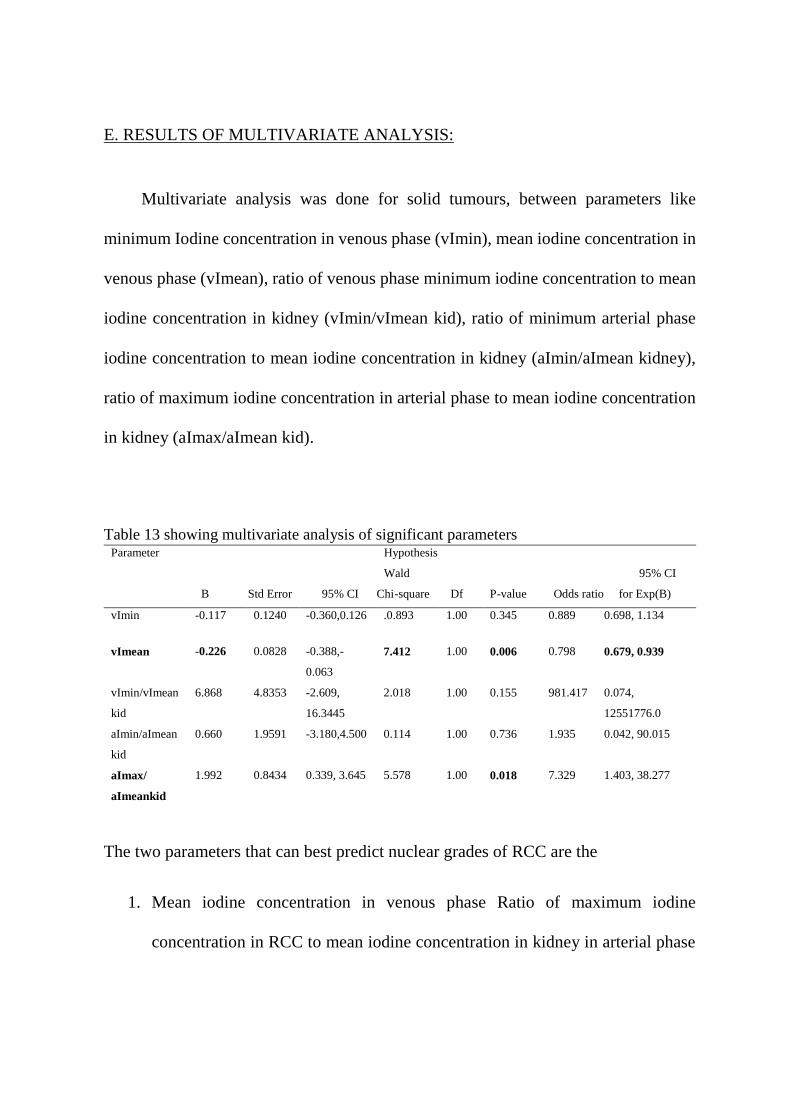
E. RESULTS OF MULTIVARIATE ANALYSIS:
Multivariate analysis was done for solid tumours, between parameters like
minimum Iodine concentration in venous phase (vImin), mean iodine concentration in
venous phase (vImean), ratio of venous phase minimum iodine concentration to mean
iodine concentration in kidney (vImin/vImean kid), ratio of minimum arterial phase
iodine concentration to mean iodine concentration in kidney (aImin/aImean kidney),
ratio of maximum iodine concentration in arterial phase to mean iodine concentration
in kidney (aImax/aImean kid).
Table 13 showing multivariate analysis of significant parameters
Parameter Hypothesis
Wald 95% CI
B Std Error 95% CI Chi-square Df P-value Odds ratio for Exp(B)
vImin -0.117 0.1240 -0.360,0.126 .0.893 1.00 0.345 0.889 0.698, 1.134
vImean -0.226 0.0828 -0.388,-
0.063
7.412 1.00 0.006 0.798 0.679, 0.939
vImin/vImean
kid
6.868 4.8353 -2.609,
16.3445
2.018 1.00 0.155 981.417 0.074,
12551776.0
aImin/aImean
kid
0.660 1.9591 -3.180,4.500 0.114 1.00 0.736 1.935 0.042, 90.015
aImax/
aImeankid
1.992 0.8434 0.339, 3.645 5.578 1.00 0.018 7.329 1.403, 38.277
The two parameters that can best predict nuclear grades of RCC are the
1. Mean iodine concentration in venous phase Ratio of maximum iodine
concentration in RCC to mean iodine concentration in kidney in arterial phase
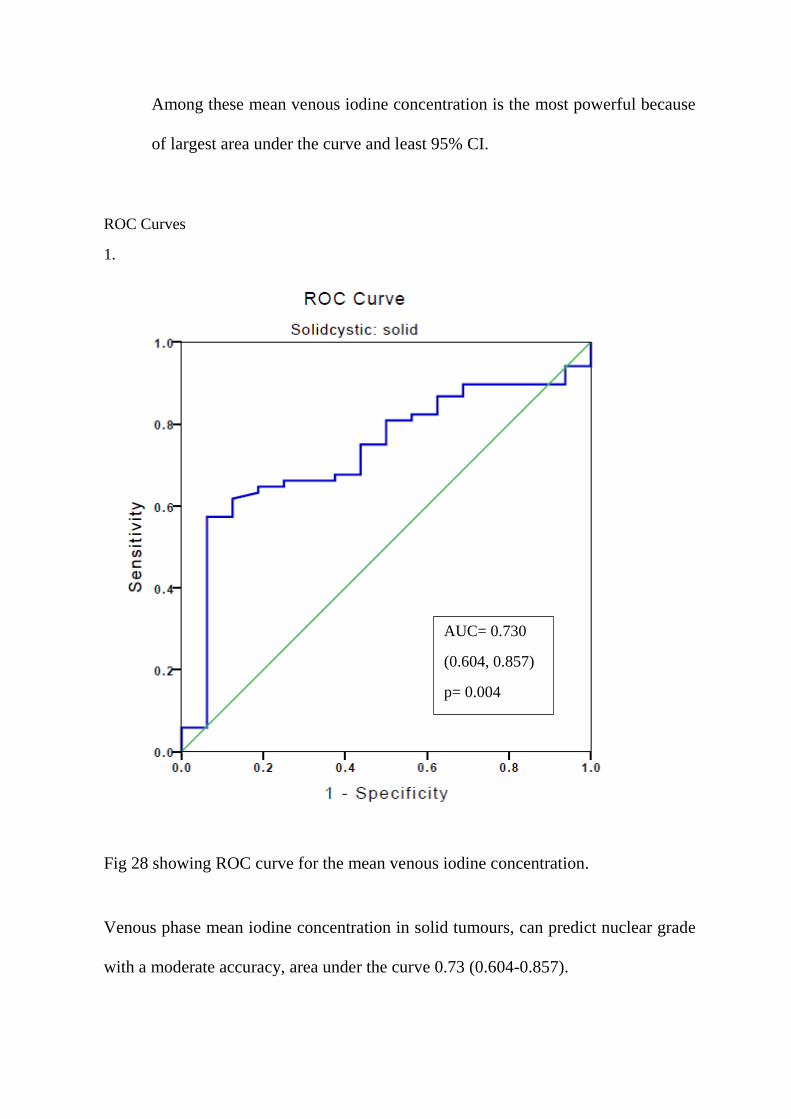
Among these mean venous iodine concentration is the most powerful because
of largest area under the curve and least 95% CI.
ROC Curves
1.
Fig 28 showing ROC curve for the mean venous iodine concentration.
Venous phase mean iodine concentration in solid tumours, can predict nuclear grade
with a moderate accuracy, area under the curve 0.73 (0.604-0.857).
AUC= 0.730
(0.604, 0.857)
p= 0.004

Venous phase mean iodine concentration with a cut off value of 16.74 or less can have
65% sensitivity and 81% specificity is predicting the higher nuclear grades of tumour.
DISCUSSION
With the steady increase in annual incidence of RCC, number of incidentally
detected tumours (>50%)(1) and number of localised (64%)(5) tumours are also
increasing. Surgery is the treatment of choice for all localised disease. However in
elderly patients, patients with significant comorbidity active surveillance of the disease
with periodic imaging is a valid option for treatment. Studies have shown only small
percentage (9.2%) of renal tumours are of high grade.
CT scan is the gold standard for assessing the anatomical stage of the disease.
There has been a continuous attempt to use different CT findings to correlate with the
other prognostic factors of RCC, like histological subtypes and nuclear grades.
In our study, we used post processed water suppressed iodine density images to
measure iodine concentration. Maximum, minimum and mean iodine concentration
was measured in both arterial and venous phases after selecting maximum possible
ROIs at three different levels of RCC (details given in methodology). Mean iodine
concentration in aorta and normal kidney was also measured for comparison.
We studied 95 different lesions in 95 patients. Three patients had more than one
lesions, among which the largest one was taken for analysis. Mean age of the patients
was 49 year with a range of 25-72years, which is less compared to the western
population. This supports Agnihotri et al who found relatively younger age of onset of
RCC in Indian population, contrast to the western population.
There was a clear male predominance with 73% patients being male. Equal
incidence of tumour was seen on both sides. Only 3 out of 95 patients (3.1%) of
patients have multifocal disease. Out of 95 lesions, 84 was predominantly solid, 11
were predominantly cystic.
The size of the solid tumour showed very strong correlation with the tumour
grade (p= 0.009). Higher tumour grades are more likely to have large tumour size.
Among other CT findings presence of lymph nodal involvement show significant
correlation with the tumour grade (p=0.019).
For analysis of the iodine concentration and its correlation with the nuclear grade
we split up the cases in predominantly solid and cystic. Overall these solid tumours
show good correlation with the iodine concentrations but the predominantly cystic
lesions fail to do so.
We found, a decreasing iodine concentration with increasing grade of RCC.
Though considerable overlaps are noted in iodine concentrations in Grade 2 and Grade
3 RCCs, it could reasonably separate high grade (grades 3, 4) from low grade (grades
1, 2) tumours.
The mean iodine concentration, minimum iodine concentration measured in
venous phase, ratio of minimum iodine concentration in RCC to that of kidney in the
venous phase as well as in arterial phase showed significant correlation with nuclear
grades of RCC.
Multivariate analysis was done between parameters which showed venous phase
mean iodine concentration in RCC can be the most powerful predictor of the nuclear
grade as it has the largest area under the curve. A cut of value of mean iodine
concentration in venous phase 16.74 or less has 64.7% sensitivity and 81.2%
specificity of predicting grade 3, 4 RCCs.
In recent study Mileto et al (40) showed iodine concentration in RCC has a strong
correlation with nuclear grades. They found increasing iodine concentration with
increasing nuclear grades. This difference is due to the methodology they applied.
They chose smallest ROI in the most enhancing parts of RCC after carefully avoiding
area of necrosis. Whereas in our study we included maximum area possible in ROI
including necrosis. Because necrosis increases with the increasing grade of tumour we
found the low iodine concentration values for higher grades.
However studies based on the enhancement pattern showed decreasing
enhancement with increasing grade. Villalobos-Gollas(18) et al concluded that lower
enhancing areas are negatively related with nuclear grade. In a another study Zhu et al
(19) analysed the enhancement pattern of clear cell RCC and showed increasing
nuclear grades with the decreasing enhancement of the tumour. They also suggested
cortico-medullary phase relative enhancement is the best predictor for nuclear grade.
In our study also ratio of arterial phase (cortico-medullary) maximum iodine
concentration in RCC to iodine concentration in kidney showed significant ability to
predict the higher nuclear grade. However, mean iodine concentration in the venous
phase appears to be most powerful predictor of the nuclear grade as it has larger area
under the curve. A mean venous phase iodine concentration of 16.74 mg/cc or less can
predict the higher nuclear grades (grades 3, 4) with 64.7% sensitivity and 81.2%
specificity.
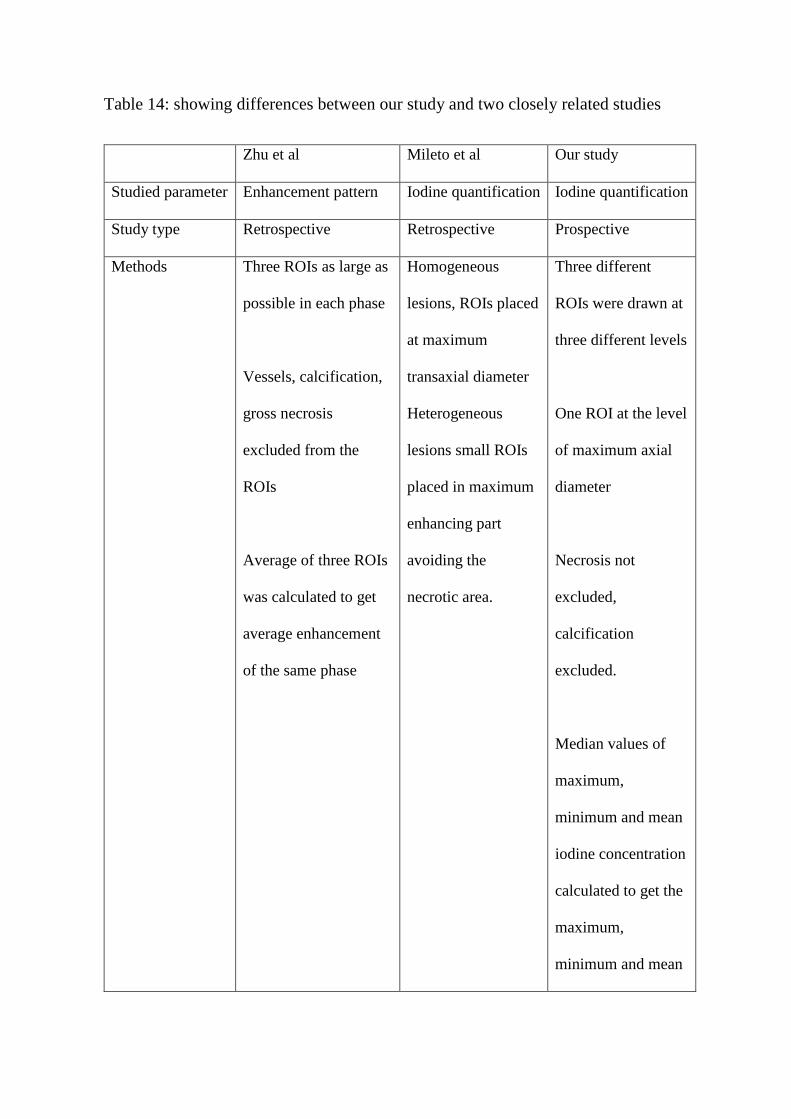
Table 14: showing differences between our study and two closely related studies
Zhu et al Mileto et al Our study
Studied parameter Enhancement pattern Iodine quantification Iodine quantification
Study type Retrospective Retrospective Prospective
Methods Three ROIs as large as
possible in each phase
Vessels, calcification,
gross necrosis
excluded from the
ROIs
Average of three ROIs
was calculated to get
average enhancement
of the same phase
Homogeneous
lesions, ROIs placed
at maximum
transaxial diameter
Heterogeneous
lesions small ROIs
placed in maximum
enhancing part
avoiding the
necrotic area.
Three different
ROIs were drawn at
three different levels
One ROI at the level
of maximum axial
diameter
Necrosis not
excluded,
calcification
excluded.
Median values of
maximum,
minimum and mean
iodine concentration
calculated to get the
maximum,
minimum and mean
iodine concentration
of the tumour.
Results Corticomedullary
phase relative
enhancement- most
significant predictor.
Other important
predictors are cortico-
medullary phase
tumour enhancement,
nephrographic tumour
enhancement and
nephrographic relative
tumour enhancement
Increasing iodine
concentration was
found with increase
in the nuclear grades
Mean iodine
concentration in
venous phase
(nephrographic) is
the most powerful
predictor. A cut off
value of 16.74 or
less can be used
with a very high
specificity of 81.2%
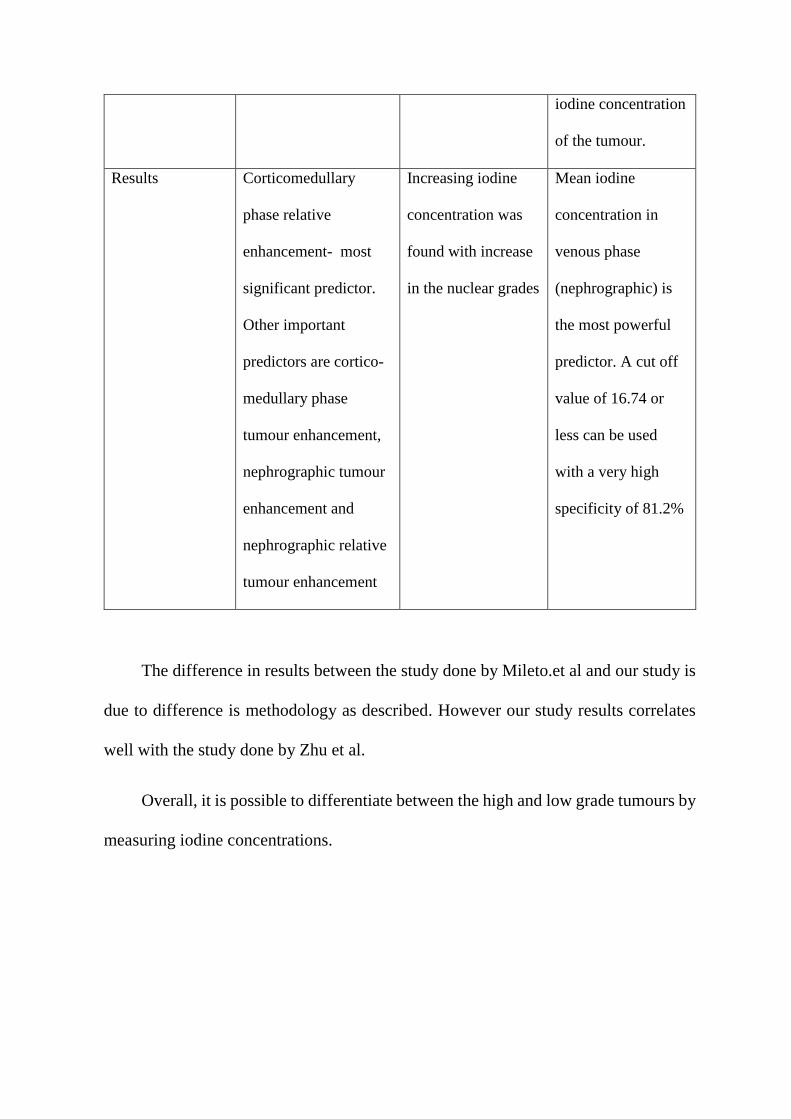
The difference in results between the study done by Mileto.et al and our study is
due to difference is methodology as described. However our study results correlates
well with the study done by Zhu et al.
Overall, it is possible to differentiate between the high and low grade tumours by
measuring iodine concentrations.
Prediction of nuclear grade can help the doctors to determine the prognosis of
patients with multiple other comorbidities and put the patient on active surveillance.
Patients with multiple lesions or patients with syndrome associated RCC, where
nephron sparing surgery is of utmost importance, knowledge of approximate high or
low grade tumour can help surgeons deciding the resection margin.
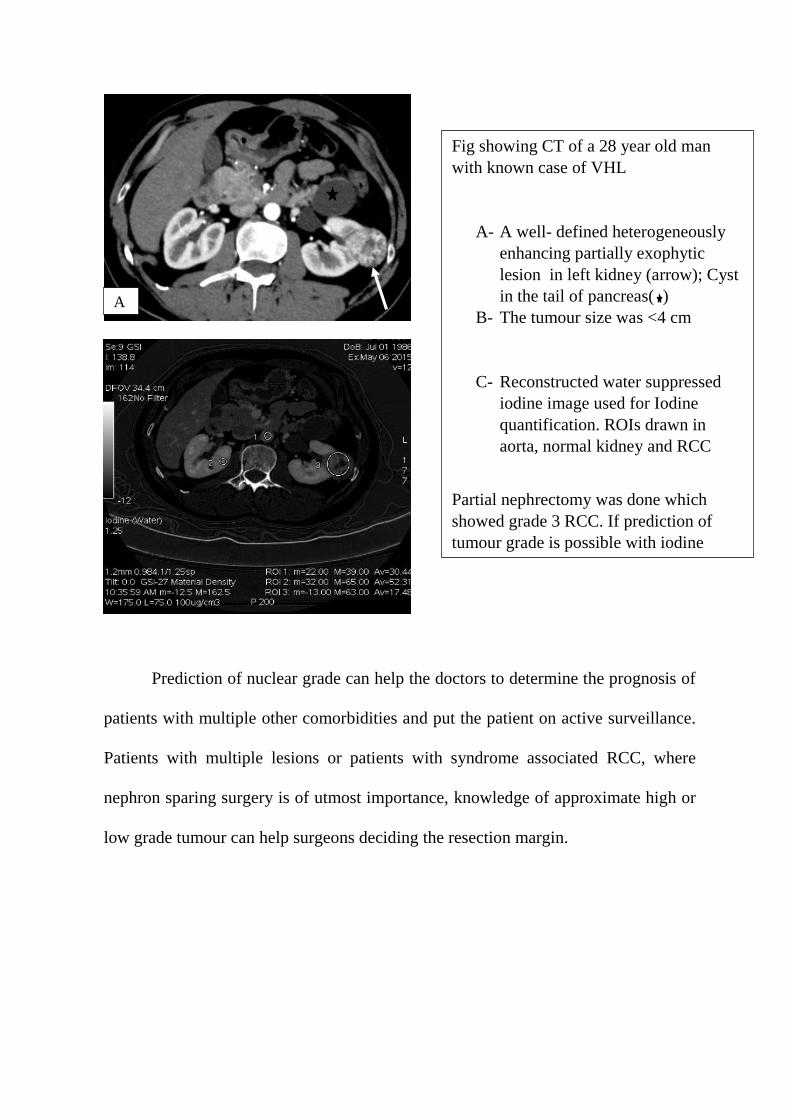
Fig showing CT of a 28 year old man
with known case of VHL
A- A well- defined heterogeneously
enhancing partially exophytic
lesion in left kidney (arrow); Cyst
in the tail of pancreas( )
B- The tumour size was <4 cm
C- Reconstructed water suppressed
iodine image used for Iodine
quantification. ROIs drawn in
aorta, normal kidney and RCC
Partial nephrectomy was done which
showed grade 3 RCC. If prediction of
tumour grade is possible with iodine
concentration, a wider surgical margin
can be obtained.
C
A
B
CONCLUSION
Iodine concentration in clear cell type of renal cell carcinoma can predict high or
low nuclear grades of RCC. There is significant overlaps of values obtained for grade
2 and grade 3 diseases. Mean iodine concentration is the most powerful predictor of
nuclear grade with a cut off value of 16.7 mg/ml or less has 65% sensitivity and 81%
specificity of predicting higher nuclear grade.
LIMITATION
This study has some limitations
- It was conducted on a relatively small sample size.
- Relatively less number of high grade tumours, especially the grade 4 tumours.
- For predominant cystic lesions entire lesion was included in the ROI, leading to
unreliable iodine concentration in the tumour.
FUTURE DIRECTION:
With the use of dual energy technique it is possible to get reconstructed at images
at different keVs (between 40-140keV). Subtle enhancing lesions can become more
prominent lower keVs (compared to the tube potential used in conventional CT).
Contrast dose also can be reduced. Single phase acquisition with split bolus of contrast
can give useful set of images with relatively low radiation dose.
BIBLIOGRAPHY 1. Wein. Campbell-Walsh Urology. Tenth Edition. Vol. two. Elsevier Saunders;
2. Lane BR, Samplaski MK, Herts BR, Zhou M, Novick AC, Campbell SC. Renal Mass
Biopsy—A Renaissance? J Urol. 2008 Jan;179(1):20–7.
3. Wang R, Wolf Jr. JS, Wood Jr. DP, Higgins EJ, Hafez KS. Accuracy of Percutaneous
Core Biopsy in Management of Small Renal Masses. Urology. 2009 Mar;73(3):586–90.
4. Global Burden of Disease Cancer Collaboration. The Global Burden of Cancer 2013.
JAMA Oncol. 2015 Jul 1;1(4):505–27.
5. National Cancer Institute Surveillance, Epidemiology and End Results Proagramme
[Internet]. Available from: http://seer.cancer.gov/
6. Agnihotri S, Kumar J, Jain M, Kapoor R, Mandhani A. Renal cell carcinoma in India
demonstrates early age of onset & a late stage of presentation. Indian J Med Res. 2014
Nov;140(5):624–9.
7. Srigley JR, Delahunt B, Eble JN, Egevad L, Epstein JI, Grignon D, et al. The
International Society of Urological Pathology (ISUP) Vancouver Classification of Renal
Neoplasia. Am J Surg Pathol [Internet]. 2013;37(10). Available from:
http://journals.lww.com/ajsp/Fulltext/2013/10000/The_International_Society_of_Urolog
ical_Pathology.2.aspx
8. Tsili AC, Argyropoulou MI. Advances of multidetector computed tomography in the
characterization and staging of renal cell carcinoma. World J Radiol. 2015 Jun
28;7(6):110–27.
9. Rekha PR, Rajendiran S, Rao S, Shroff S, Joseph LD, Prathiba D. Histological
reclassification, histochemical characterization and c-kit immunoexpression in renal cell
carcinoma. Indian J Urol IJU J Urol Soc India. 2008;24(3):343–7.
10. Johnson PT, Horton KM, Fishman EK. How Not to Miss or Mischaracterize a Renal
Cell Carcinoma: Protocols, Pearls, and Pitfalls. Am J Roentgenol. 2010 Apr
1;194(4):W307–W315.
11. Ng CS, Wood CG, Silverman PM, Tannir NM, Tamboli P, Sandler CM. Renal Cell
Carcinoma: Diagnosis, Staging, and Surveillance. Am J Roentgenol. 2008 Oct
1;191(4):1220–32.
12. Reznek RH. CT/MRI in staging renal cell carcinoma. Cancer Imaging. 2004;4(Spec No
A):S25–S32.
13. Lee-Felker SA, Felker ER, Tan N, Margolis DJA, Young JR, Sayre J, et al. Qualitative
and Quantitative MDCT Features for Differentiating Clear Cell Renal Cell Carcinoma
From Other Solid Renal Cortical Masses. Am J Roentgenol. 2014 Oct 23;203(5):W516–
W524.

14. Israel GM, Bosniak MA. How I Do It: Evaluating Renal Masses. Radiology. 2005 Aug
1;236(2):441–50.
15. Kim JK, Kim TK, Ahn HJ, Kim CS, Kim K-R, Cho K-S. Differentiation of Subtypes of
Renal Cell Carcinoma on Helical CT Scans. Am J Roentgenol. 2002 Jun
1;178(6):1499–506.
16. Fujimoto H, Wakao F, Moriyama N, Tobisu K, Sakamoto M, Kakizoe T. Alveolar
Architecture of Clear Cell Renal Carcinomas (≤5.0 cm) Show High Attenuation on
Dynamic CT Scanning. Jpn J Clin Oncol. 1999 Apr 1;29(4):198–203.
17. Jung SC, Cho JY, Kim SH. Subtype differentiation of small renal cell carcinomas on
three-phase MDCT: usefulness of the measurement of degree and heterogeneity of
enhancement. Acta Radiol. 2012 Feb 1;53(1):112–8.
18. Villalobos-Gollás M, Aguilar-Davidov B, Culebro-García C, Gómez-Alvarado MO,
Rojas-Garcia P, Ibarra-Fombona R, et al. Pathological implications of areas of lower
enhancement on contrast-enhanced computed tomography in renal-cell carcinoma:
additional information for selecting candidates for surveillance protocols. Int Urol
Nephrol. 2012;44(5):1369–74.
19. Zhu Y-H, Wang X, Zhang J, Chen Y-H, Kong W, Huang Y-R. Low Enhancement on
Multiphase Contrast-Enhanced CT Images: An Independent Predictor of the Presence of
High Tumor Grade of Clear Cell Renal Cell Carcinoma. Am J Roentgenol. 2014 Aug
22;203(3):W295–W300.
20. Johnson TRC. Dual-energy CT: general principles. AJR Am J Roentgenol. 2012
Nov;199(5 Suppl):S3–8.
21. Kaza RK, Platt JF, Cohan RH, Caoili EM, Al-Hawary MM, Wasnik A. Dual-energy CT
with single- and dual-source scanners: current applications in evaluating the
genitourinary tract. Radiogr Rev Publ Radiol Soc N Am Inc. 2012 Apr;32(2):353–69.
22. McCollough CH, Leng S, Yu L, Fletcher JG. Dual- and Multi-Energy CT: Principles,
Technical Approaches, and Clinical Applications. Radiology. 2015 Aug 24;276(3):637–
53.
23. Kaza RK, Platt JF, Cohan RH, Caoili EM, Al-Hawary MM, Wasnik A. Dual-energy CT
with single- and dual-source scanners: current applications in evaluating the
genitourinary tract. Radiogr Rev Publ Radiol Soc N Am Inc. 2012 Apr;32(2):353–69.
24. Graser A, Johnson TRC, Hecht EM, Becker CR, Leidecker C, Staehler M, et al. Dual-
energy CT in patients suspected of having renal masses: can virtual nonenhanced
images replace true nonenhanced images? Radiology. 2009 Aug;252(2):433–40.
25. Hartman R, Kawashima A, Takahashi N, Silva A, Vrtiska T, Leng S, et al. Applications
of dual-energy CT in urologic imaging: an update. Radiol Clin North Am. 2012
Mar;50(2):191–205, v.
26. Matsumoto K, Jinzaki M, Tanami Y, Ueno A, Yamada M, Kuribayashi S. Virtual
Monochromatic Spectral Imaging with Fast Kilovoltage Switching: Improved Image
Quality as Compared with That Obtained with Conventional 120-kVp CT. Radiology.
2011 Apr 1;259(1):257–62.
27. Yu L, Leng S, McCollough CH. Dual-energy CT-based monochromatic imaging. AJR
Am J Roentgenol. 2012 Nov;199(5 Suppl):S9–S15.
28. Ho LM, Yoshizumi TT, Hurwitz LM, Nelson RC, Marin D, Toncheva G, et al. Dual
Energy Versus Single Energy MDCT: Measurement of Radiation Dose Using Adult
Abdominal Imaging Protocols. Acad Radiol. 2009 Nov;16(11):1400–7.
29. Thomas C, Patschan O, Ketelsen D, Tsiflikas I, Reimann A, Brodoefel H, et al. Dual-
energy CT for the characterization of urinary calculi: In vitro and in vivo evaluation of a
low-dose scanning protocol. Eur Radiol. 2009;19(6):1553–9.
30. Graser A, Becker CR, Staehler M, Clevert DA, Macari M, Arndt N, et al. Single-phase
dual-energy CT allows for characterization of renal masses as benign or malignant.
Invest Radiol. 2010 Jul;45(7):399–405.
31. Song KD, Kim CK, Park BK, Kim B. Utility of iodine overlay technique and virtual
unenhanced images for the characterization of renal masses by dual-energy CT. AJR
Am J Roentgenol. 2011 Dec;197(6):W1076–1082.
32. Ascenti G, Mileto A, Krauss B, Gaeta M, Blandino A, Scribano E, et al. Distinguishing
enhancing from nonenhancing renal masses with dual-source dual-energy CT: iodine
quantification versus standard enhancement measurements. Eur Radiol. 2013
Aug;23(8):2288–95.
33. Brown CL, Hartman RP, Dzyubak OP, Takahashi N, Kawashima A, McCollough CH,
et al. Dual-energy CT iodine overlay technique for characterization of renal masses as
cyst or solid: a phantom feasibility study. Eur Radiol. 2009 May;19(5):1289–95.
34. Crispen PL, Viterbo R, Fox EB, Greenberg RE, Chen DYT, Uzzo RG. Delayed
intervention of sporadic renal masses undergoing active surveillance. Cancer. 2008 Mar
1;112(5):1051–7.
35. Wehle MJ, Thiel DD, Petrou SP, Young PR, Frank I, Karsteadt N. Conservative
management of incidental contrast-enhancing renal masses as safe alternative to
invasive therapy. Urology. 2004 Jul;64(1):49–52.
36. European Society for Medical Oncology [Internet]. Available from:
http://www.esmo.org/
37. American Urology Association [Internet]. Available from:
https://www.auanet.org/education/guidelines/renal-mass.cfm
38. Renal Cell Carcinoma: ESMO Clinical Practice Guidelines [Internet]. Available from:
http://www.esmo.org/Guidelines/Genitourinary-Cancers/Renal-Cell-Carcinoma
39. Guidelines on Renal Cll Carcinoma, European Association of Urology, 2014 [Internet].
Available from: http://uroweb.org/wp-content/uploads/10-Renal-Cell-
Carcinoma_LR.pdf
40. Mileto A, Marin D, Alfaro-Cordoba M, Ramirez-Giraldo JC, Eusemann CD, Scribano
E, et al. Iodine Quantification to Distinguish Clear Cell from Papillary Renal Cell
Carcinoma at Dual-Energy Multidetector CT: A Multireader Diagnostic Performance
Study. Radiology. 2014 Aug 25;273(3):813–20.
ANNEXURES
1. IRB approval
2. Information sheet with consent form
3. Proforma
4. Data sheet


Department of Radiodiagnosis, Christian Medical College, Vellore
Study Title: Can Dual Energy CT with iodine mapping predict the Nuclear grades of
Clear cell type of Renal Cell Carcinoma
PATIENT INFORMATION SHEET
The following information is provided to inform you about this study and your participation
in it. Please read the information carefully and you are free to ask questions regarding the
study and the information given. Participation in this study is purely voluntary and you are
free to withdraw from the study anytime.
What is this study about?
This study aims to test the possibility of predicting the grade of renal cancer (RCC) before
surgery using a software in the CT (CT machine is called Dual energy CT).
What is dual energy CT? How it is different from the routine CT?
CT performed in dual energy CT scanner is same as any other CT. We will use a special
software to calculate amount of iodine in the kidney mass.
Is there any risk associated with this study?
As in routine CT, iodinated contrast material will be injected intravenously. Some patients
are prone to develop mild contrast reaction like itching, urticaria, running nose, sneezing,
dizziness, nausea. These symptoms usually resolve spontaneously with little or no treatment.
Severe reactions causing laryngeal edema, pulmonary edema, life threatening arrhythmia are
extremely rare. The risk of contrast reaction is same as that of other contrast enhanced CT
scans
Radiation is a known side effect of any study requiring Xray exposure. However there is no
additional radiation or additional risk to the patient for participating in this study.
If I take part in this study, what will I have to do?
Your CT scan abdomen is prescribed as part of your treatment protocol to know the stage of
your disease which will decide further management. This is the existing standard of care for
renal cancer patients. If you agree to participate in this study CT scan will be done using
dual energy CT scanner as per routine protocol and your medical records can be accessed by
the investigators of the study. No additional investigations will be done as part of this study.
The additional information obtained as part of the study will not be used to decide your
management. Your treatment will be as per routine protocol.
Can I withdraw from this study after it starts?

Your participation in this study is entirely voluntary and you are also free to withdraw
permission to participate in this study at any point. If you do so, this will not affect your
usual treatment at this hospital in any way.
Is there any benefit of the study?
There is no immediate benefit to you. However in future it may help the doctors to decide
management protocol of patients with renal cancer.
Will my personal details be kept confidential?
The results of this study will/may be published in a medical journal but you will not be
identified by name in any publication or presentation of results. However, your medical
record may be reviewed by doctors associated with the study, without your additional
permission.
If you have any further queries Please feel free to contact
Dr. Poulomi Mitra
PG registrar, Department of Radiology, CMC Vellore
Contact number: 0416228-3012/3609/3610 (Office), 09787628892 (mobile)
Email: [email protected]
Informed Consent Form Study Title:
Study Number: ____________
Subject’s Initials: __________________
Subject’s Name: _________________________________________
Date of Birth / Age: ___________________________
(Subject)
(i) I confirm that I have read and understood the information sheet dated ____________ for
the above study and have had the opportunity to ask questions.
(ii) I understand that my participation in the study is voluntary and that I am free to
withdraw at any time, without giving any reason, without my medical care or legal rights
being affected.
(iii) I understand that doctors working on the study, the Ethics Committee and the regulatory
authorities will not need my permission to look at my health records both in respect of the
current study and any further research that may be conducted in relation to it, even if I
withdraw from the trial. I agree to this access. However, I understand that my identity will
not be revealed in any information released to third parties or published.
(iv) I agree not to restrict the use of any data or results that arise from this study provided
such a use is only for scientific purpose(s).
(v) I agree to take part in the above study.
Signature (or Thumb impression) of the Subject/Legally Acceptable
Date: _____/_____/______
Signatory’s Name: _________________________________ Signature:
Or
Representative: _________________
Date: _____/_____/______
Signatory’s Name: _________________________________
Signature of the Investigator: ________________________
Date: _____/_____/______
Study Investigator’s Name: _________________________
Signature of the Witness: ___________________________
Date: _____/_____/_______
Name & Address of the Witness: ______________________________
PROFORMA
DEMOGRAPHY
Name: ________________________________ Hospital number: ________________
Age: ____________years
Sex: Male – 1; female – 0
CT FINDINGS:
Number of lesions: ________________
Laterality
1-Unilateral
2-Bilateral
Focality
1-Unifocal
2- Multifocal
Side
1-Right side
2-Left side
Maximum diameter of the lesion ____________ cm
Predominantly solid OR cystic
1- Predominantly Solid
2- Predominantly cystic
Margin:
1- Well defined
2- Ill defined
Enhancement:
1. Present
2. Absent
Pattern of enhancement
1- Homogeneous
2- Heterogeneous
Areas of necrosis:
1- Present
2- Absent
% necrosis:
1- <25%
2- 25-75%
3- >75%
Fat density areas:
1- Present
2- Absent
Calcification:
1. Present
2. Absent
Invasion of pelvicalyceal system:
1. Present
2. Absent
Extension into renal vein:
1. Present
2. Absent
Extension into IVC:
1- Present
2- Absent
If extension into IVC present
1- Infrahepatic
2- Hepatic
3- Suprahepatic
Lymph node enlargement
1. Present
2. Absent
Lymph node groups involved
1. Paraaortic
2. Parailiac
3. Others:
Distal metastases:
1. Present
2. Absent

Site of metastases:
1. Adrenals
2. Lungs
3. Liver
4. Bone
5. Brain
POST PROCESSING:
ARTERIAL
PHASE
Area Maximum
Iodine
Concentration
Minimum
Iodine
Concentration
Mean
Iodine
Concentration
ROI 1
ROI 2
ROI 3
Arterial phase Iodine concentration in aorta____________
Arterial phase Iodine concentration in kidney____________
VENOUS
PHASE
Area Maximum
Iodine
Concentration
Minimum
Iodine
Concentration
Mean
Iodine
Concentration
ROI 1
ROI 2
ROI 3
Venous phase Iodine concentration in aorta ____________
Venous phase iodine concentration in kidney____________
Spectral curve: Maximum HU at lowest KeV where there is maximum separation of spectral
curves
Aorta ____________
Kidney ____________
RCC
1. ____________
2. ____________
3. ____________
PATHOLOGY
Specimen obtained by
1. Surgery
2. Percutaneous biopsy
3. Fine needle aspiration cytology
Type of surgery
1. Partial nephrectomy
2. Radical nephrectomy
Lympho-vascular invasion
1. Present
2. Absent
Infiltration of perinephric fat
1. Present
2. Absent
Pathologic Type:
1. Clear cell renal cell carcinoma
Multilocular cystic clear cell renal cell neoplasm of low malignant potential*
2. Papillary renal cell carcinoma
Type 1
Type 2
3. Chromophobe renal cell carcinoma
Hybrid oncocytic chromophobe tumor
4. Carcinoma of the collecting ducts of Bellini
5. Renal medullary carcinoma
6. MiT family translocation renal cell carcinoma
Xp11 translocation renal cell carcinoma t(6;11) renal cell carcinoma
7. Carcinoma associated with neuroblastoma
8. Mucinous tubular and spindle cell carcinoma
9. Tubulocystic renal cell carcinoma
10. Acquired cystic disease associated renal cell carcinoma
11. Clear cell(tubular) papillary renal cell carcinoma
12. Hereditary leiomyomatosis renal cell carcinoma syndrome associated renal cell
carcinoma
13. Renal cell carcinoma unclassified
Nuclear Grade:
1- Fuhrman Grade 1
2- Fuhrman Grade 2
3- Fuhrman grade 3
4- Fuhrman grade 4
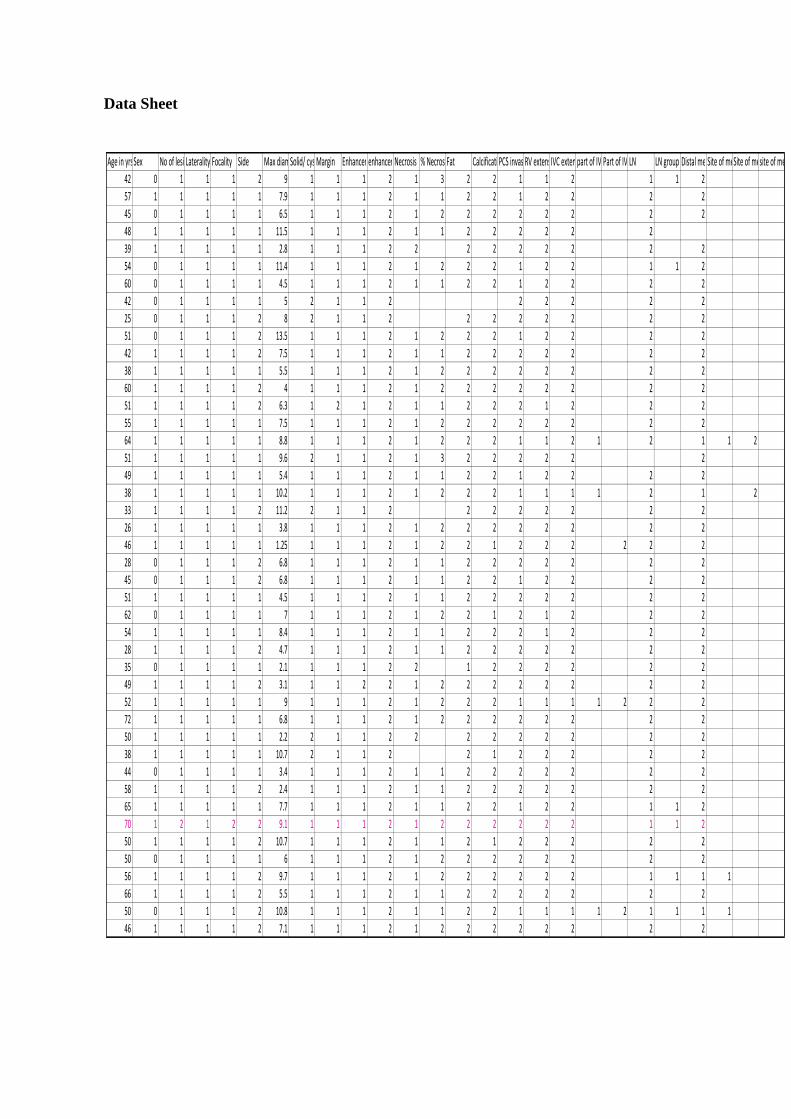
Data Sheet
Age in yrsSex No of lesionsLaterality Focality Side Max diameter cmSolid/ cysticMargin Enhancementenhancement patternNecrosis % NecrosisFat CalcificationPCS invasionRV extensionIVC extensionpart of IVC involvedPart of IVC involvedLN LN group Distal metastasesSite of metastasesSite of metastasessite of metastases
42 0 1 1 1 2 9 1 1 1 2 1 3 2 2 1 1 2 1 1 2
57 1 1 1 1 1 7.9 1 1 1 2 1 1 2 2 1 2 2 2 2
45 0 1 1 1 1 6.5 1 1 1 2 1 2 2 2 2 2 2 2 2
48 1 1 1 1 1 11.5 1 1 1 2 1 1 2 2 2 2 2 2
39 1 1 1 1 1 2.8 1 1 1 2 2 2 2 2 2 2 2 2
54 0 1 1 1 1 11.4 1 1 1 2 1 2 2 2 1 2 2 1 1 2
60 0 1 1 1 1 4.5 1 1 1 2 1 1 2 2 1 2 2 2 2
42 0 1 1 1 1 5 2 1 1 2 2 2 2 2 2
25 0 1 1 1 2 8 2 1 1 2 2 2 2 2 2 2 2
51 0 1 1 1 2 13.5 1 1 1 2 1 2 2 2 1 2 2 2 2
42 1 1 1 1 2 7.5 1 1 1 2 1 1 2 2 2 2 2 2 2
38 1 1 1 1 1 5.5 1 1 1 2 1 2 2 2 2 2 2 2 2
60 1 1 1 1 2 4 1 1 1 2 1 2 2 2 2 2 2 2 2
51 1 1 1 1 2 6.3 1 2 1 2 1 1 2 2 2 1 2 2 2
55 1 1 1 1 1 7.5 1 1 1 2 1 2 2 2 2 2 2 2 2
64 1 1 1 1 1 8.8 1 1 1 2 1 2 2 2 1 1 2 1 2 1 1 2
51 1 1 1 1 1 9.6 2 1 1 2 1 3 2 2 2 2 2 2
49 1 1 1 1 1 5.4 1 1 1 2 1 1 2 2 1 2 2 2 2
38 1 1 1 1 1 10.2 1 1 1 2 1 2 2 2 1 1 1 1 2 1 2
33 1 1 1 1 2 11.2 2 1 1 2 2 2 2 2 2 2 2
26 1 1 1 1 1 3.8 1 1 1 2 1 2 2 2 2 2 2 2 2
46 1 1 1 1 1 1.25 1 1 1 2 1 2 2 1 2 2 2 2 2 2
28 0 1 1 1 2 6.8 1 1 1 2 1 1 2 2 2 2 2 2 2
45 0 1 1 1 2 6.8 1 1 1 2 1 1 2 2 1 2 2 2 2
51 1 1 1 1 1 4.5 1 1 1 2 1 1 2 2 2 2 2 2 2
62 0 1 1 1 1 7 1 1 1 2 1 2 2 1 2 1 2 2 2
54 1 1 1 1 1 8.4 1 1 1 2 1 1 2 2 2 1 2 2 2
28 1 1 1 1 2 4.7 1 1 1 2 1 1 2 2 2 2 2 2 2
35 0 1 1 1 1 2.1 1 1 1 2 2 1 2 2 2 2 2 2
49 1 1 1 1 2 3.1 1 1 2 2 1 2 2 2 2 2 2 2 2
52 1 1 1 1 1 9 1 1 1 2 1 2 2 2 1 1 1 1 2 2 2
72 1 1 1 1 1 6.8 1 1 1 2 1 2 2 2 2 2 2 2 2
50 1 1 1 1 1 2.2 2 1 1 2 2 2 2 2 2 2 2 2
38 1 1 1 1 1 10.7 2 1 1 2 2 1 2 2 2 2 2
44 0 1 1 1 1 3.4 1 1 1 2 1 1 2 2 2 2 2 2 2
58 1 1 1 1 2 2.4 1 1 1 2 1 1 2 2 2 2 2 2 2
65 1 1 1 1 1 7.7 1 1 1 2 1 1 2 2 1 2 2 1 1 2
70 1 2 1 2 2 9.1 1 1 1 2 1 2 2 2 2 2 2 1 1 2
50 1 1 1 1 2 10.7 1 1 1 2 1 1 2 1 2 2 2 2 2
50 0 1 1 1 1 6 1 1 1 2 1 2 2 2 2 2 2 2 2
56 1 1 1 1 2 9.7 1 1 1 2 1 2 2 2 2 2 2 1 1 1 1
66 1 1 1 1 2 5.5 1 1 1 2 1 1 2 2 2 2 2 2 2
50 0 1 1 1 2 10.8 1 1 1 2 1 1 2 2 1 1 1 1 2 1 1 1 1
46 1 1 1 1 2 7.1 1 1 1 2 1 2 2 2 2 2 2 2 2

Site of metastasesA ROI1 areaA ROI1 ImaxA ROI1 IminA ROI1 ImeanA ROI2 areaA ROI2 ImaxA ROI2 IminA ROI2 ImeanA ROI3 areaA ROI3 ImaxA ROI3 IminA ROI3 ImeanA Imean AoA Imean KidV ROI 1 areaV ROI 1 ImaxV ROI 1 IminV ROI 1 I meanV ROI 2 AreaV ROI 2 ImaxV ROI 2 I minV ROI 2 I meanV ROI 3 AreaV ROI 3 ImaxV ROI 3 Imin
4757.9 71 -8 16.71 4180.9 61 -10 17.32 4900.9 67 -19 15.96 89.08 48.65 4908.7 31 -14 6.58 4528.6 31 -25 7.38 4928.5 36 -15
3477.2 114 -15 39.92 2706.5 109 -4 2210.3 98 -9 107.54 48.26 3324 41 -6 2218 37 0 20.71 3715.5 53 -11
2174.8 78 -6 19.83 1896.5 84 -9 23.63 2408.1 70 -8 19.28 83.76 39.84 2150.3 43 -24 14.25 2081 43 -6 16.48 2271.3 44 -10
3567.5 32 -10 10.44 3331.7 34 -12 11.74 3649.5 33 -2
322.6 74 17 49.98 312.4 68 10 39.96 355.5 70 4 42.07 100.6 53.61 335.4 50 -27 28.95 301 50 9 26.36 390.4 55 2
7089 127 -15 13.29 6531.5 76 -13 11.79 6704.4 108 -20 15.24 156.6 64.97 5969.1 48 7 18.05 6196.6 44 -15 12.24 6360.2 44 -6
995.6 82 -20 51.95 681.9 75 3 607.5 82 2 51.11 59.57 710.9 42 -8 27.95 689.2 46 13 27.79 815.7 48 1
1435.7 56 -8 8.92 1124.2 48 -6 10.89 1294.8 51 -14 11.63 154.7 50.86 1365.7 38 -3 8.7 1094.6 42 -2 11.67 1224.8 42 -3
3204.1 69 -12 5.4 3650 71 -9 4.59 3494.8 78 -10 4.47 153 71.12 3419.8 32 -6 5.55 3415.7 33 -5 4.55 3566.3 37 -18
2233.1 74 -6 19.45 1887.6 73 -9 23.07 1897.9 94 -7 36.45 118.5 42.38 2536.2 49 0 23.74 1863.8 46 -1 23.36 2470.9 49 -20
1165.8 61 -13 25.7 925.5 67 -23 24.46 849.8 65 0 34.72 91.21 41.23 1162.3 40 -6 17.82 946.9 39 -6 17.39 826.3 36 0
551.4 45 -3 20.98 551.4 51 -26 23.28 618.4 40 1
884 70 -2 32.55 925.5 71 -21 39.54 822.2 68 -4 34.28 103.8 38.95 1001.1 44 -2 23.37 879.5 41 -3 24.15 819.2 40 -13
2119.9 74 -28 21.14 1351.2 59 -28 19.61 1622.6 66 -23 17.95 106.7 52.67 2064.6 38 -18 13.16 1983 39 -26 14.71 1802 37 -19
3374.5 86 -11 30.96 2290.3 83 -14 20.46 1950.6 87 -9 30.99 96.5 52.22 4026.7 61 20.65 224.1 54 18.9 1575.2 58
2760.1 66 -25 31.41 3359.4 73 -14 30.35 1223.1 61 0 36.76 75.93 38.14 2965.5 43 -5 16.5 2901.1 37 -14 14.53 1623.4 32 -1
3620.8 60 -21 14.15 2439.2 58 -26 17.23 3086.2 51 -15 12.28 47.1 36.99 2854 34 -11 9.97 2213.2 32 -10 10.34 2867.7 26 -15
760 80 6 50.27 624.2 84 8 52.32 548.6 74 0 44.03 82.82 43.89 947 40 1 22.85 874.9 41 -4 24.53 876.1 41 7
3422.6 105 -13 38.48 3148.3 104 -11 43.6 4234.4 106 -13 29.08 95.4 48.95 3684.6 66 -20 30.07 3259 65 -15 32.88 3056.8 74 -12
4767.8 72 -19 14.93 4462.8 81 -19 14.32 4187.9 77 -17 20.93 80.11 45.14 5666.1 54 -16 11.26 3906.1 46 -10 13.36 4361 52 -10
740.5 63 34.52 346.4 55 27.35 695.9 65
27.2 49 4 24.42 13.8 32 1 17.96 26.9 35 4 13.52 77.26 59.84 20.04 49 4 24.42 24 32 1 17.96 34 4
1900.9 40 -12 12.06 2220.3 49 -16 11.15 1434.2 44 -7 16.54 101.2 42.08 2076.4 34 -9 14.78 1774.3 34 -11 10.48 1294.8 34 -5
1217.9 88 -3 35.21 1165.4 87 1 38.26 1034 84 -4 30.57 127.8 53.63 1574.3 65 1 31.32 1212.1 68 0 37.04 1345.1 60 -6
1253.8 90 8 46.76 1157.8 91 8 52.42 1255.2 80 -7 32.88 133.7 56.2 1535.6 69 -5 36.5 1045.6 80 7 42.92 1482.7 75 -18
2426.1 65 -12 21.61 2031.8 74 -9 31.81 2419.3 68 -17 22.18 68.91 30.53 2610 26 -27 6.43 2087.4 21 -8 10.68 2471.6 21 -12
2433.8 37 -20 11.42 1896.8 40 -21 9.37 2572.2 40 -20 11.13 74.19 19.37 2331.6 27 -15 10.41 1641.3 28 -8 9.09 1559.2 24 -1
613.5 63 -11 27.02 406.2 57 -2 25.69 519.7 71 -13 25.81 99.67 56.42 469.7 63 -13 17.48 373.7 68 -7 19.64 471.2 44 -8
114.3 34 -4 18.19 75.9 40 0 24.09 144.4 39 2 21.66 78.5 32.15 180.2 16 0 8.75 128.3 20 3 12.3 199.8 19 4
575 46 -15 11.44 636 42 -14 9.54 545.6 46 -9 14.85 89.14 47.4 575 27 -10 7.01 636 29 -11 6.15 515.8 27 -7
2351.1 66 -15 9.58 2405.2 75 -15 15.16 2174.3 71 -12 15.11 88.53 23.22 2354.8 22 -14 3.23 2231.2 30 -14 4.79 2214.3 31 -13
2598 22 -18 2.44 2429.4 20 -17 2.71 2351.8 24 -15 1.04 48.19 13.63 2591.6 21 -14 0.41 2412.1 23 -18 0.93 2628.1 22 -18
276.3 50 -10 10.51 151.1 36 -9 12.15 188.6 31 -5 9.55 72.9 34.69 128.1 19 -7 5.42 113.7 20 -8 6.7 279.6 31 -10
4515.7 58 -18 5.93 4267 71 -21 6.28 4569.1 87 -20 6.57 96.01 44.54 4854.4 34 -16 3.39 4918.6 34 -24 3.32 5191.5 78 -38
743.9 68 0 36.89 964 75 -13 34.29 671.1 65 -7
152.5 90 22 50.55 122.3 105 32 62.39 228.6 90 16 48.49 179.5 69.99 137.6 80 -22 42.99 122 88 39 61 152.5 81 13
3159.6 75 -10 26.04 2532.2 56 -5 26.35 3145.2 69 -12 27.98 85.02 40.62 2291.5 37 -5 19.87 3256 35 -3 19.15 2822.4 36 -7
3455.7 55 -20 15.17 2181.3 51 -5 18.53 4179.2 63 -27 6.82 79.22 46.57 3906.1 48 -16 7.93 3188.6 53 -15 13.06 4008.5 46 -20
3221.4 81 -20 16.27 3129.5 74 -22 19.63 2005.4 69 -13 16.6 96.74 44.26 2887.4 42 -10 15.56 3299 52 -8 18.77 2934.1 40 -11
1680.2 65 -22 19.27 1283.8 67 -8 24.26 1063.2 72 -10 29.76 95.78 42.94 1377.2 52 -6 20.55 1377.2 50 -3 19.95 1328.9 45 0
6201.1 76 -22 10.86 5259.3 57 -29 8.84 4417.3 74 -22 13.26 71.71 37.71 5992.9 54 -25 11.05 6079.9 66 -29 14.81 3708.4 53 -23
1386.3 57 -6 21.63 1083.2 46 -8 20.81 1490.6 46 -6 19.59 119.2 30.84 1737.3 42 -8 17.29 1525.7 45 -27 16.47 1297.2 39 -8
5088 31 -7 9.84 4148.9 38 -8 10.66 4544.4 28 -4
1865.8 77 -31 17.81 1857.4 75 -14 29.93 2217 78 -27
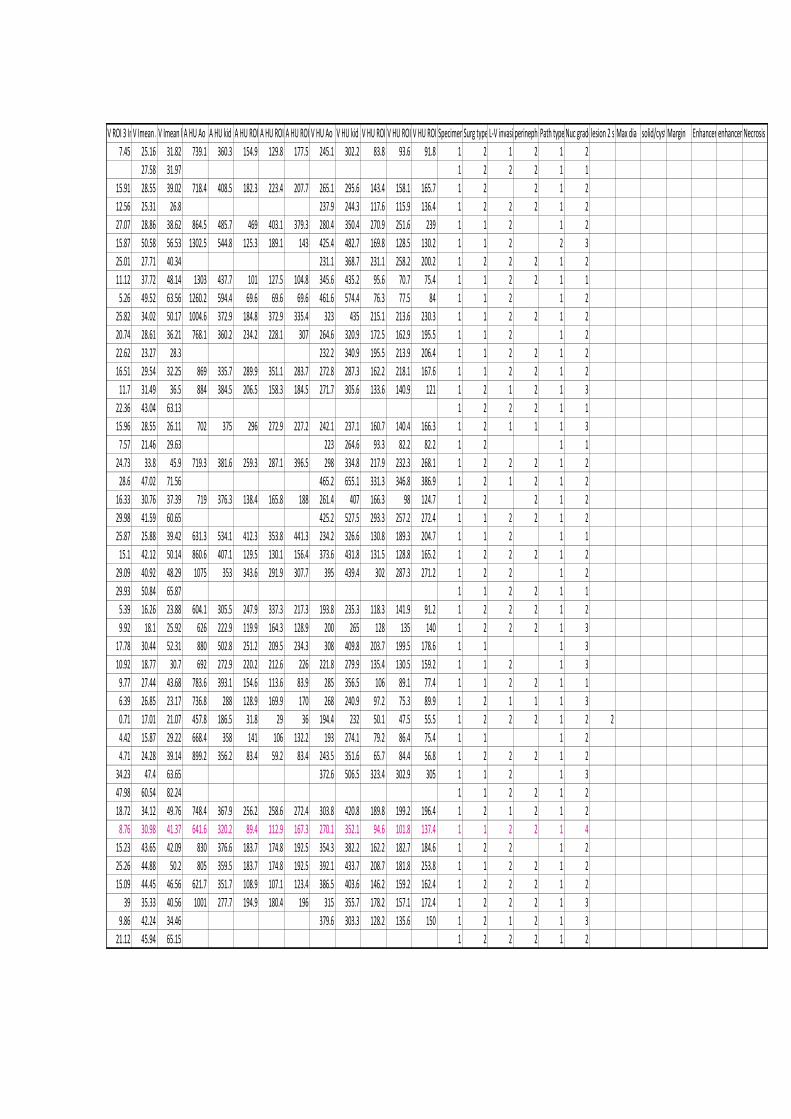
V ROI 3 ImeanV Imean AoV Imean kidA HU Ao A HU kid A HU ROI1A HU ROI 2A HU ROI3V HU Ao V HU kid V HU ROI1V HU ROI2V HU ROI3Specimen Surg type L-V invasionperinephric fat infilPath type Nuc gradelesion 2 sideMax dia solid/cyst Margin Enhancementenhancement typeNecrosis
7.45 25.16 31.82 739.1 360.3 154.9 129.8 177.5 245.1 302.2 83.8 93.6 91.8 1 2 1 2 1 2
27.58 31.97 1 2 2 2 1 1
15.91 28.55 39.02 718.4 408.5 182.3 223.4 207.7 265.1 295.6 143.4 158.1 165.7 1 2 2 1 2
12.56 25.31 26.8 237.9 244.3 117.6 115.9 136.4 1 2 2 2 1 2
27.07 28.86 38.62 864.5 485.7 469 403.1 379.3 280.4 350.4 270.9 251.6 239 1 1 2 1 2
15.87 50.58 56.53 1302.5 544.8 125.3 189.1 143 425.4 482.7 169.8 128.5 130.2 1 1 2 2 3
25.01 27.71 40.34 231.1 368.7 231.1 258.2 200.2 1 2 2 2 1 2
11.12 37.72 48.14 1303 437.7 101 127.5 104.8 345.6 435.2 95.6 70.7 75.4 1 1 2 2 1 1
5.26 49.52 63.56 1260.2 594.4 69.6 69.6 69.6 461.6 574.4 76.3 77.5 84 1 1 2 1 2
25.82 34.02 50.17 1004.6 372.9 184.8 372.9 335.4 323 435 215.1 213.6 230.3 1 1 2 2 1 2
20.74 28.61 36.21 768.1 360.2 234.2 228.1 307 264.6 320.9 172.5 162.9 195.5 1 1 2 1 2
22.62 23.27 28.3 232.2 340.9 195.5 213.9 206.4 1 1 2 2 1 2
16.51 29.54 32.25 869 335.7 289.9 351.1 283.7 272.8 287.3 162.2 218.1 167.6 1 1 2 2 1 2
11.7 31.49 36.5 884 384.5 206.5 158.3 184.5 271.7 305.6 133.6 140.9 121 1 2 1 2 1 3
22.36 43.04 63.13 1 2 2 2 1 1
15.96 28.55 26.11 702 375 296 272.9 227.2 242.1 237.1 160.7 140.4 166.3 1 2 1 1 1 3
7.57 21.46 29.63 223 264.6 93.3 82.2 82.2 1 2 1 1
24.73 33.8 45.9 719.3 381.6 259.3 287.1 396.5 298 334.8 217.9 232.3 268.1 1 2 2 2 1 2
28.6 47.02 71.56 465.2 655.1 331.3 346.8 386.9 1 2 1 2 1 2
16.33 30.76 37.39 719 376.3 138.4 165.8 188 261.4 407 166.3 98 124.7 1 2 2 1 2
29.98 41.59 60.65 425.2 527.5 293.3 257.2 272.4 1 1 2 2 1 2
25.87 25.88 39.42 631.3 534.1 412.3 353.8 441.3 234.2 326.6 130.8 189.3 204.7 1 1 2 1 1
15.1 42.12 50.14 860.6 407.1 129.5 130.1 156.4 373.6 431.8 131.5 128.8 165.2 1 2 2 2 1 2
29.09 40.92 48.29 1075 353 343.6 291.9 307.7 395 439.4 302 287.3 271.2 1 2 2 1 2
29.93 50.84 65.87 1 1 2 2 1 1
5.39 16.26 23.88 604.1 305.5 247.9 337.3 217.3 193.8 235.3 118.3 141.9 91.2 1 2 2 2 1 2
9.92 18.1 25.92 626 222.9 119.9 164.3 128.9 200 265 128 135 140 1 2 2 2 1 3
17.78 30.44 52.31 880 502.8 251.2 209.5 234.3 308 409.8 203.7 199.5 178.6 1 1 1 3
10.92 18.77 30.7 692 272.9 220.2 212.6 226 221.8 279.9 135.4 130.5 159.2 1 1 2 1 3
9.77 27.44 43.68 783.6 393.1 154.6 113.6 83.9 285 356.5 106 89.1 77.4 1 1 2 2 1 1
6.39 26.85 23.17 736.8 288 128.9 169.9 170 268 240.9 97.2 75.3 89.9 1 2 1 1 1 3
0.71 17.01 21.07 457.8 186.5 31.8 29 36 194.4 232 50.1 47.5 55.5 1 2 2 2 1 2 2
4.42 15.87 29.22 668.4 358 141 106 132.2 193 274.1 79.2 86.4 75.4 1 1 1 2
4.71 24.28 39.14 899.2 356.2 83.4 59.2 83.4 243.5 351.6 65.7 84.4 56.8 1 2 2 2 1 2
34.23 47.4 63.65 372.6 506.5 323.4 302.9 305 1 1 2 1 3
47.98 60.54 82.24 1 1 2 2 1 2
18.72 34.12 49.76 748.4 367.9 256.2 258.6 272.4 303.8 420.8 189.8 199.2 196.4 1 2 1 2 1 2
8.76 30.98 41.37 641.6 320.2 89.4 112.9 167.3 270.1 352.1 94.6 101.8 137.4 1 1 2 2 1 4
15.23 43.65 42.09 830 376.6 183.7 174.8 192.5 354.3 382.2 162.2 182.7 184.6 1 2 2 1 2
25.26 44.88 50.2 805 359.5 183.7 174.8 192.5 392.1 433.7 208.7 181.8 253.8 1 1 2 2 1 2
15.09 44.45 46.56 621.7 351.7 108.9 107.1 123.4 386.5 403.6 146.2 159.2 162.4 1 2 2 2 1 2
39 35.33 40.56 1001 277.7 194.9 180.4 196 315 355.7 178.2 157.1 172.4 1 2 2 2 1 3
9.86 42.24 34.46 379.6 303.3 128.2 135.6 150 1 2 1 2 1 3
21.12 45.94 65.15 1 2 2 2 1 2
58 1 1 1 1 2 9.6 1 1 2 2 1 2 2 2 1 1 1 1 2 2
66 1 1 1 1 2 3.4 1 1 1 2 1 2 2 2 2 2 2 2
57 1 1 1 1 1 7.2 1 1 1 2 1 1 2 2 1 1 2 2 2
48 1 1 1 1 2 13.5 1 1 1 2 1 2 2 1 1 2 2 1 1 2
38 0 1 1 1 2 2.8 1 1 1 2 1 1 2 2 2 2 2 2 2
52 1 1 1 1 1 7.1 1 1 1 2 1 1 2 2 1 2 2 2 2
48 1 1 1 1 2 14.2 1 1 1 2 1 2 2 2 1 2 2 2 2
62 1 1 1 1 2 7.3 1 1 1 2 1 1 2 1 2 2 2 2 2
46 0 1 1 1 2 5.7 1 1 1 2 1 2 2 2 2 2 2 2 2
61 1 1 1 1 2 5.8 1 1 1 2 1 2 2 2 2 2 2 2 2
53 0 2 2 2 1 4 1 1 2 2 1 1 2 2 2 2 2 2 2
57 1 1 1 1 1 7.3 1 1 1 2 1 2 1 2 2 2 2 2 2
46 1 1 1 1 1 14 1 1 1 2 1 2 2 1 1 2 2 2 2
60 1 1 1 1 2 4.4 1 1 1 2 1 1 2 2 2 2 2 2 2
67 1 1 1 1 1 5.6 1 1 1 2 1 1 2 2 1 2 2 2 2
52 1 1 1 1 2 15 2 1 1 2 2 2 2 2 2 2 2
36 1 1 1 1 2 4.3 1 1 1 2 1 1 2 2 1 2 2 2 2
36 0 1 1 1 2 9 2 1 1 2 2 1 2 2 2 1 1 2
49 0 1 1 1 1 8.9 1 1 1 2 1 2 2 2 2 2 2 2 2
66 1 1 1 1 2 5.5 1 1 1 2 1 2 2 2 2 2 2 1 1 2
57 1 1 1 1 2 4 1 1 1 2 1 1 2 2 2 2 2 2 2 2
53 1 1 1 1 2 13 1 1 1 2 1 2 2 2 1 1 2 1 1 2 1
48 0 1 1 1 2 7.2 1 1 1 2 1 2 2 1 2 2 2 2 2
38 0 1 1 1 2 2.4 1 1 1 2 1 1 2 2 2 2 2 2 2
40 1 1 1 1 1 4.7 1 1 1 2 1 2 2 2 2 2 2 2 2
50 1 1 1 1 1 7.3 1 1 1 2 1 2 2 2 2 2 2 2 2
53 1 1 1 1 2 3.8 2 1 1 2 2 1 2 2 2 2 2
54 0 1 1 1 2 3.5 1 1 1 2 1 1 2 2 2 2 2 2 2
54 1 1 1 1 1 5.6 1 1 1 2 1 1 2 2 1 2 2 2 2
30 1 1 1 1 1 3.6 1 1 1 2 1 1 2 2 2 2 2 2 2
45 1 1 1 1 1 8.3 1 1 1 2 1 2 2 2 1 2 2 2 2
49 1 1 1 1 2 7.3 1 1 1 2 1 2 2 2 1 2 2 2 2
42 1 1 1 1 2 4.8 2 1 1 2 2 2 2 2 2 2 2
34 1 1 1 1 1 4 1 1 1 2 1 2 2 2 2 2 2 2 2
36 1 1 1 1 2 3.4 2 1 1 2 2 2 2 2 2 2 2
41 1 1 1 1 1 6.6 1 1 1 2 1 2 2 2 1 1 1 1 2 2
32 1 1 1 1 1 3.7 1 1 1 2 1 1 2 2 2 2 2 2 2
47 1 1 1 1 1 10 1 1 1 2 1 2 2 1 1 2 2 2 2
55 0 1 1 1 2 7.5 1 1 1 2 1 1 2 2 1 1 2 2 2
57 1 1 1 1 2 6.7 1 1 1 2 1 3 2 2 2 1 2 2 1 1
61 0 4 2 2 2 12.4 1 1 1 2 1 2 2 2 2 2 2 2 2
54 1 1 1 1 2 10 1 1 1 2 1 2 2 1 1 2 2 1 1 2
50 1 1 1 1 1 3.3 1 1 1 2 1 1 2 2 2 2 2 2 2
53 0 1 1 1 1 8.5 1 1 1 2 1 2 1 1 1 2 2 2 2
63 1 1 1 1 2 6.1 1 1 1 2 1 1 2 1 2 2 2 2 2
51 1 1 1 1 1 8.3 1 1 1 2 1 2 2 2 1 2 2 1 1 2
53 1 1 1 1 1 5.7 1 1 1 2 1 1 2 2 1 2 2 2 2
48 1 1 1 1 1 4.6 1 1 1 2 1 1 2 1 2 2 2 2 2
72 1 1 1 1 1 2.9 1 1 1 2 1 2 2 2 2 2 2 2 2
52 1 1 1 1 1 8 1 1 1 2 1 1 2 2 2 2 2 2 2
62 1 1 1 1 2 3.7 1 1 1 2 1 1 2 2 2 2 2 2 2
2531.2 70 1 38.95 4048.6 73 -4 20.35 4131.6 77 -4 26.54 91.3 44.11 3483.7 44 -5 20.23 4219.5 42 -9 16.57 4127.6 34 -11
507.5 57 -7 25.07 565.4 44 -9 14.55 287.8 64 20 39.16 85.39 37.47 480.2 36 -9 12.42 309 40 -3 14.97 565.4 36 -10
1809.9 76 -3 40.79 1342.7 61 -13 25.01 1897.9 86 -10 41.96 98.44 40.79 1390.7 50 -8 23.29 1880.6 48 9 30.31 2141.7 49 -10
7381.6 59 -14 17.99 5336.7 80 -16 15.86 5804 58 -16 17.39 82.32 43.17 6469.5 46 -12 14.63 5750.7 44 -17 13.9 5295.3 40 -18
409.2 42 -8 10.65 232.5 50 -6 18.3 337.4 50 -9 11.4 74.96 35.83 312.3 63 3 24.59 359.2 48 6 23.88 292.7 46 3
1682.4 37 -18 11.13 2183 44 -16 13.61 1387.2 37 -7 15.95 74.61 40.04 1341.8 37 -9 11.27 2155 28 -8 11.25 1748.1 35 -10
7070.6 85 -17 16.13 3960 77 -24 22.45 8821.8 78 -33 11 98.36 43.19 9080.4 43 -21 10.52 7448.5 42 -11 10.2 8434.3 128 -12
2022.5 46 -14 12.4 1979 36 -10 12.96 1208.8 34 -5 14.12 85.25 39.61 2658.8 35 -19 15.22 2014.1 35 -4 14.99 1297.3 32 -2
1241.7 74 -6 21.47 1549.9 64 -16 22.08 1273.4 59 -12 20.47 96.62 34.61 1887.1 44 -6 16.25 1579.1 40 -6 16.92 1625.5 46 -5
1156.2 61 -7 15.87 1595.4 46 -14 16.35 1235.4 58 -12 17.29 77.04 33.42 1746 53 -18 15.07 1465.2 41 -12 12.43 1361.8 49 -18
568.7 97 -1 58.32 370.7 102 -1 54.24 631.7 92 -4 59.37 143.2 62.56 629.8 68 12 49.4 920.1 76 -11 50.03 864.9 78 -7
1481.2 126 -7 50.99 1484.6 122 -12 41.14 1418.9 107 -10 50.31 135.7 65.24 1628 61 -5 28.07 1106.9 59 -3 32.95 2452.4 53 -6
5657.9 75 -22 17.65 5573.6 82 -21 18.05 3614.1 77 -20 19.04 93.68 51 4307.9 49 -21 13.19 5461.3 56 -21 12.73 3875.6 51 -17
686.2 39 -21 11.58 538.5 49 -6 19.89 451.2 58 -14 22.84 78.34 35.02 584.9 43 -5 20.29 562.8 47 2 20.63 566.2 43 -10
2183.3 74 -26 30.16 1972.8 64 -8 23.43 1537.4 73 -8 33.89 100.4 64.22 2085.5 66 -13 26.19 1938 62 -3 26.85 1746.6 71 -5
7954.9 65 -16 7.36 5796.6 87 -25 11.21 11220.6 62 -33 2.89 84.05 38.79 11162.9 57 -25 6.37 6311.4 47 -16 11.11 12660.4 51 -27
604.8 42 -13 7.75 409.2 45 -12 11.59 541.2 36 -10 10.16 79.69 35.97 408.7 35 -2 15.54 677.3 37 -5 15.34 707 36 -22
3260.5 80 -22 4.95 4054.1 46 -27 5.01 4918 41 -29 4.34 73.55 45.15 5246.7 53 -23 5.65 3902.5 40 -13 6.22 6484.9 40 -19
4384.7 110 -13 41.22 3764 109 -15 48.34 4086.6 110 -28 35.38 110.1 49.63 4649 74 -2 42.58 3762.2 77 5 42.78 4109.2 80 -12
1389.2 62 -12 28.99 1295.3 73 -14 26.45 1433.7 64 -22 26 93.01 33.7 1435.2 38 -8 19.16 1337.8 44 -6 17.23 1324.5 41 -8
3839.9 79 -38 2.61 3428.9 35 -36 2.19 3652.8 38 -34 1.37 84.04 45.59 4023.3 32 -35 4.04 3735 30 -28 3.43 2880.6 39 -29
7603 53 -20 10.58 9332.7 64 -30 11.46 5251.4 58 -13 13.96 72.6 31.87 7381.2 46 -23 14.66 10234.8 45 -28 8.96 8517.8 39 -22
1359.6 67 -12 32.11 1949.4 74 -14 28 2358.7 66 -11 21.11 105.15 40.07 1992.9 49 -2 26.28 2292.5 59 -9 23.2 2214.3 52 -8
161.1 95 9 50.81 160.1 90 3 52.99 219.7 102 10 51.7 78.59 72.64 224.8 54 -3 27.59 155.1 58 9 33.47 142.2 64 -3
1548.4 88 -12 35.5 1224.5 85 -17 32.84 1224.5 85 -11 70.46 51.79 54.79 1526.2 56 -16 17.95 1317.7 62 -17 15.78 833 44 -5
2024.9 65 -23 26.05 2644.3 68 -4 31.22 2568.9 67 -22 19.62 58.75 38.27 2092.2 59 -13 24.06 3354.1 47 -25 17.29 2293 48 -17
551 44 -27 12.36 450.2 54 -22 14.1 313.4 49 -24 15.6 74.01 37.25 486.4 54 -27 17.47 602 59 -15 13.76 486.4 51 -22
778.7 65 -5 31.53 515.8 72 0 37.65 643.2 69 -15 29.23 129 30.92 811.8 72 3 30.81 849.8 71 -8 30.05 643.2 53 -10
1796.1 80 -20 26.59 1923 74 -13 28.32 1617.1 69 -35 20.21 74.85 32.18 1796.1 54 -32 21.14 1927.1 66 -10 24.41 1078.7 63 -15
752 84 -8 38.22 724.5 80 -10 34.22 506.9 85 0 44.19 103.4 66.07 613.5 78 -5 36.45 611.6 71 3 33.69 613.8 62 0
1994.8 83 -18 19.9 2293 83 -18 19.9 1577.6 74 -6 27.17 74.82 40.49 2231.2 54 -12 17.46 2223.2 47 -17 16.49 1824.8 45 -13
3083.5 59 -23 41.18 3207.4 54 -8 26.98 2681.9 52 -4 25.22 41.18 39.89 3050.5 23 -21 4.48 2971.5 24 -15 4.69 2684.3 24 -21
1168.7 57 -14 10.96 845.9 64 -10 23.13 815.7 61 -7 29.68 109.2 48.45 1165.3 51 -15 12.86 1128.7 47 -15 17.8 1005.6 46 -16
1159.3 53 -11 14.7 1149 56 -12 17.92 777.7 77 -13 19.27 97.32 51.82 1108.6 36 -9 13.82 733.2 30 -1 14.25 930.6 34 -9
850.3 64 -5 20.17 1004.4 72 -3 17.36 900.3 56 -7 20.22 87.38 75.01 746.5 35 -3 12.95 742.1 38 1 13.72 642.2 27 1
1531 90 -12 25.12 1123.7 92 -8 29.35 1002.6 96 -11 53.96 93.53 40.04 1390.7 44 -3 16.94 1582.7 49 -4 26.44 884.5 47 4
599.4 41 15 26.59 666.2 39 -2 25.48 904.5 35 -9
5258.8 46 -16 54.91 4789.1 51 -14 17.95 3129.9 52 -18 14.55 54.91 38.12 4999.7 33 -7 11 3813.9 32 -5 10.91 2237.2 53 -5
1934.5 95 -15 19.97 1903.4 98 -6 22.57 2050.7 96 -2 23.7 100.4 35.33 1786.7 37 -10 13.91 1994.8 40 -6 14.84 1578.1 33 -2
1898.4 75 -14 19.33 1626.5 70 -4 21.2 3046.4 56 -13 10.74 103.9 25.37 2045.8 35 -2 14.12 1414.4 35 -18 16.85 2768.6 39 -114
7236.6 55 -19 6.31 7120.6 66 -27 8.11 5873.3 59 -22 4.75 50.42 30.15 7623.9 31 -18 1.99 7360.5 31 -19 4.02 5272.4 41 -28
4080.7 53 -18 19.1 3703.4 46 -8 18.16 3869.1 45 -12 13.53 82.53 36 4105.9 29 -12 13.57 4054.9 39 -11 14.18 3950.1 31 -10
778.7 66 -15 32.58 544.1 49 9 29.82 560.9 58 7 30.24 117.6 64.88 715.9 56 -8 27.72 573.5 56 7 29.21 711.4 44 8
3852.7 68 -3 17.3 3774.6 49 -3 15.74 2792.3 57 -4 19.4 119.2 41.51 3267.9 63 -6 18.48 3689.6 33 -4 17.58 2917.4 37 -4
2 1532.7 52 -30 18.41 1237.2 51 0 23.34 1501.8 51 -13
4162 54 -14 17.76 2810.6 48 -11 19.54 3620.7 54 -10 17.24 67.49 26.6 3614.7 52 -10 16.13 3540.5 54 -15 17.87 3442 48 -14
2089 72 -5 16.33 1800 51 -6 14.95 2089 64 -7 21.08 113.4 49.74 1924.2 52 0 20.08 1919.1 44 -12 15.91 1707.5 47 2
674.8 66 11 39.88 455.9 63 9 37.84 649.1 61 -11 37.06 92.92 57 771.7 51 -18 29.8 455.6 48 1 30.98 749.5 52 0
314.9 59 3 25.99 314.2 44 -1 20.98 273.3 59 3 25.99 91.97 46.88 360.8 58 0 25.64 292.7 53 -6 23.06 381.3 57 1
3874 40 -3 16.55 3579.3 36 -2 16.85 4481.1 43 -25
470.4 121 -8 51.83 724.2 119 -6 59.35 533.9 119 0 60.2 108.6 64.2 586.5 97 0 33.18 621.1 77 0 33.2 519.9 76 4
12.99 30.25 36.57 747.3 348.5 317.8 213 258 282.1 327.8 220.4 155.1 187.6 1 2 1 1 3
18.68 31.87 43.48 723.4 408.4 150 289.6 137 288.1 358.9 158 257.7 139.9 1 1 2 1 1
27.1 38.69 23.29 825.3 327.7 369.7 369 338.9 351.4 379.7 270.8 251.7 238.1 1 2 1 2 1 2
14.72 32.86 42.16 698.3 375.5 178.2 165.7 169.3 287.5 345.2 146.9 159.7 160.7 1 2 2 2 1 2
24.67 41.32 55.49 637 295.6 113.1 136.5 136 367.6 476.9 233.3 224.9 250.5 1 1 2 2 1 1
12.08 26.19 26.38 648.4 333.2 168.5 201.7 143.7 251.4 331.7 126.7 127.4 130.8 1 2 2 2 1 2
9.91 35.87 53.59 835.5 426.9 95.6 120.1 154.4 307.3 433.6 102.2 127.1 109.7 1 2 1 2 1 2
14.17 29.74 38.22 700 286.1 134.2 152.2 124.6 282.7 335.6 159.7 157.7 168.3 1 2 2 2 1 2
18.05 35.84 34.5 817.2 311.1 215.8 209.4 224.7 309.1 255.6 176.7 167.6 167.6 1 2 2 2 1 1
17.38 31.45 32.29 691.3 235.7 99.8 165.2 160.9 305 315 144.6 135.2 131.1 1 2 2 1 2
52.11 70.78 51.16 1198.8 601.6 392.3 495.6 462.1 470.8 589.3 449 435.9 429.1 1 1 2 1 2
28.54 47.5 55.18 1149.7 535.2 438.5 400.4 479.4 413.5 515.1 258.3 274.4 284.2 1 2 2 2 1 1
11.82 37.29 43.24 778.2 434.1 183.2 146.4 109.6 328.1 394.1 134.1 139.3 87.9 1 2 2 2 1 2
24.21 37.37 46.18 670.4 265.3 120.4 204 171.2 329.3 397 261.9 277 202.1 1 1 2 2 1 2
32.31 50.09 76.48 883.5 486.1 244.2 219.5 305.1 444.2 587.2 244.3 250.9 292.7 1 2 2 2 1 2
4.88 47.36 39.04 718 330.8 73.5 82.5 50.4 407.7 359.5 83.3 99.7 41.1 1 2 2 1 4
13.28 24.92 33.62 632.7 309.4 96.5 134.2 120.9 229.2 292.1 128.2 155.2 159.3 1 2 2 2 1 2
4.37 36.72 41.34 657 350 53.9 53.4 69.6 315.4 373.4 72.3 53.5 76.9 1 2 2 2 1 2
31.39 47.47 54.33 926.9 435.7 438.7 454.2 304.5 401.4 463.8 364.5 293.3 282.8 1 2 2 2 1 2
17.56 34.16 33.19 796.6 272.3 262.5 281.3 283.7 300.1 310.8 179.6 166.5 178.5 1 2 2 2 1 2
3.33 32.23 42.97 641.3 297.8 91 102 137.4 229.3 397.6 154.1 154.9 127.7 1 1 2 1 2
8.02 27.62 31.25 630.8 263.6 127 148.3 130.3 258.3 289 105.6 148.9 110 1 2 1 1 1 4
23.56 38.09 50.02 883.9 384.1 313.3 384.1 200.9 350 435.7 234.1 221.6 250.4 1 2 2 2 1 2
26.57 46.12 75.97 685 731.7 397.3 434.8 425.8 415 582.2 306.5 282.2 269.1 1 1 2 2 1 1
21.45 31.3 35.95 483.3 453.4 483.3 465.8 356.8 314.8 333 190.5 166.1 210 1 1 2 2 1 1
14.79 24.83 39.12 506.5 367 252.1 297.6 175.4 236.7 326.8 180 220.6 139.6 1 2 2 1 2
18.67 31.42 40.59 650 323 145.8 139.8 108 279.2 212.8 122.5 161 127.4 1 1 2 1 1
24.48 45.6 56.33 1024 367.1 333.8 283.1 273.1 420.9 515.2 288.8 299.8 249.8 1 1 2 1 2
24.62 29.18 34.33 679.6 312.1 275 252.2 194.2 312.7 291.8 210.8 224.4 175.1 1 2 2 2 1 2
33.19 38.02 48.2 933.6 570.4 351.4 310.9 357.2 340 501.1 289.8 327.7 322.2 1 1 2 1 2
17.5 35.06 37.06 648 351.7 226.4 233 216.2 296.5 325.9 162.6 167.4 179.8 1 2 2 2 1 2
3.42 15.2 24.04 1 2 2 2 1 2
13.4 45.82 51.75 914 399.7 266.5 329.8 86.4 352 446.3 201.7 247.9 109.7 1 1 2 2 1 3
11.87 32.89 47.37 873.8 430.9 157.2 152.5 149.5 297.8 387.3 125.2 149.4 121.8 1 2 2 1 2
12.73 37.67 53.14 749 632.7 176.7 134.5 171 343.5 475.3 131.6 121.8 116.6 1 2 2 2 1 2
31.21 36.04 44.35 794.8 341.6 299.5 229.1 225 349.4 400.7 189.9 250.9 167.4 1 2 1 2
23.32 30.73 35.7 282.5 307.8 233.8 225.4 233 1 1 2 2 1 1
9.7 19.7 28.52 479.2 364 152.9 129.8 169.5 187.1 251.6 115.8 112.4 116.4 1 2 2 2 1 1
15.25 38.35 35.1 826.9 320.8 206.7 222.5 222.9 347.7 324.1 159.8 167.7 173.6 1 2 1 1 1 3
9.45 26.46 35.29 860.2 292.7 127 109.7 164.2 259.7 305.7 117.9 83.9 138.9 1 2 1 3
4.84 22.81 29.66 437.7 357.1 80.6 122.7 138.7 250.7 297.5 49.1 74.2 75.1 1 2 2 1 2
26.09 10.51 29.81 707.1 300.5 206.2 216.9 173.8 295.7 335.1 141.1 173.8 184.5 1 2 2 2 1 2
26.32 47.14 54.14 1009.8 597.7 270.8 264 266.8 417 483.3 241.8 234 259.3 1 2 2 2 1 1
17.31 37.07 44.01 993.9 358.1 165.1 181.1 147.3 340 377.8 169 162.3 172.1 1 2 2 2 3 2
17.07 42.05 56.16 398.8 417.7 163.1 223.1 167.8 1 2 2 2 1 2
12.01 32.54 37.96 565.5 301.2 174.2 150.3 203.9 329.9 372.7 124.4 101.8 173.6 1 2 1 2 1 3
22.79 45.82 55.5 956.6 418 180.7 206.5 187.8 394 475.3 177.6 182.7 211 1 2 2 2 1 2
30.11 33.4 41.25 796 515.3 355.9 323 355.9 299.5 426.8 278.9 278.9 284.4 1 1 2 1 2
25.33 33.45 47.7 817.3 449.3 181.6 237 166.1 330.4 437.3 262.1 246.5 255.5 1 1 2 2 1 2
16.33 34.44 44.09 308 388.4 170.1 172.8 171.8 1 2 2 2 1 2
41.51 25.98 40.86 987.8 657.9 496.6 515.7 424.5 243 460.8 294.3 289.5 292.6 1 1 2 1 1

Related Documents
![Review Article Iodine: A Longer-Life Positron Emitter Isotope New … · 2019. 7. 31. · 131 Iodine (131 I), 123 Iodine (123 I), and 125 Iodine (125 I), have limitations[ ]. Due](https://static.cupdf.com/doc/110x72/60fd8c07bb6c4a2e9a0c696e/review-article-iodine-a-longer-life-positron-emitter-isotope-new-2019-7-31.jpg)










