Pediatric Urology Can Computerized Tomography Accurately Stage Childhood Renal Tumors? Ahmed Abdelhalim,* Tamer E. Helmy, Ahmed M. Harraz, Mohamed E. Abou-El-Ghar, Mohamed E. Dawaba and Ashraf T. Hafez From the Department of Urology and Department of Radiology (MEA), Mansoura Urology and Nephrology Center, Mansoura University, Mansoura, Egypt Purpose: Staging of childhood renal tumors is crucial for treatment planning and outcome prediction. We sought to identify whether computerized tomography could accurately predict the local stage of childhood renal tumors. Materials and Methods: We retrospectively reviewed our database for patients diagnosed with childhood renal tumors and treated surgically between 1990 and 2013. Inability to retrieve preoperative computerized tomography, intra- operative tumor spillage and nonWilms childhood renal tumors were exclusion criteria. Local computerized tomography stage was assigned by a single experi- enced pediatric radiologist blinded to the pathological stage, using a consensus similar to the Children’s Oncology Group Wilms tumor staging system. Tumors were stratified into up-front surgery and preoperative chemotherapy groups. The radiological stage of each tumor was compared to the pathological stage. Results: A total of 189 tumors in 179 patients met inclusion criteria. Comput- erized tomography staging matched pathological staging in 68% of up-front surgery (70 of 103), 31.8% of pre-chemotherapy (21 of 66) and 48.8% of post- chemotherapy scans (42 of 86). Computerized tomography over staged 21.4%, 65.2% and 46.5% of tumors in the up-front surgery, pre-chemotherapy and post- chemotherapy scans, respectively, and under staged 10.7%, 3% and 4.7%. Computerized tomography staging was more accurate in tumors managed by up-front surgery (p <0.001) and those without extracapsular extension (p <0.001). Conclusions: The validity of computerized tomography staging of childhood renal tumors remains doubtful. This staging is more accurate for tumors treated with up-front surgery and those without extracapsular extension. Preoperative computerized tomography can help to exclude capsular breach. Treatment strategy should be based on surgical and pathological staging to avoid the hazards of inaccurate staging. Key Words: kidney neoplasms; neoplasm staging; tomography, x-ray computed; Wilms tumor CHILDHOOD renal tumors account for 5% to 7% of pediatric cancers, ranking fifth among childhood ma- lignancies, with Wilms tumor being the most common. 1,2 Congenital mesoblastic nephroma, renal cell carcinoma, clear cell sarcoma and rhabdoid tumor of the kidney are some other important pathological entities. Although ultrasound is usu- ally the first ordered investigation for a child presenting with an Abbreviations and Acronyms COG ¼ Children’s Oncology Group CRT ¼ childhood renal tumor CT ¼ computerized tomography NPV ¼ negative predictive value PPV ¼ positive predictive value WT ¼ Wilms tumor Accepted for publication January 24, 2014. Study received internal review board approval. * Correspondence: Urology and Nephrology Center, Mansoura University, Gomhoria St., Man- soura, Egypt 35516 (telephone: 20-10-01349367; FAX: 20-50-2263717; e-mail: a_halim_2010@ yahoo.com ). See Editorial on page 6. 194 j www.jurology.com 0022-5347/14/1921-0194/0 THE JOURNAL OF UROLOGY ® © 2014 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH,INC. http://dx.doi.org/10.1016/j.juro.2014.01.096 Vol. 192, 194-199, July 2014 Printed in U.S.A.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Abbreviations
and Acronyms
COG ¼ Children’s Oncology Group
CRT ¼ childhood renal tumor
CT ¼ computerized tomography
NPV ¼ negative predictive value
PPV ¼ positive predictive value
WT ¼ Wilms tumor
Accepted for publication January 24, 2014.Study received internal review board
approval.* Correspondence: Urology and Nephrology
Center, Mansoura University, Gomhoria St., Man-soura, Egypt 35516 (telephone: 20-10-01349367;FAX: 20-50-2263717; e-mail: [email protected]).
See Editorial on page 6.
194 j www.jurology.com
00
T
©
Pediatric Urology
Can Computerized Tomography Accurately Stage ChildhoodRenal Tumors?
Ahmed Abdelhalim,* Tamer E. Helmy, Ahmed M. Harraz, Mohamed E. Abou-El-Ghar,
Mohamed E. Dawaba and Ashraf T. Hafez
From the Department of Urology and Department of Radiology (MEA), Mansoura Urology and Nephrology Center,
Mansoura University, Mansoura, Egypt
Purpose: Staging of childhood renal tumors is crucial for treatment planning andoutcome prediction. We sought to identify whether computerized tomographycould accurately predict the local stage of childhood renal tumors.
Materials and Methods: We retrospectively reviewed our database for patientsdiagnosed with childhood renal tumors and treated surgically between 1990and 2013. Inability to retrieve preoperative computerized tomography, intra-operative tumor spillage and nonWilms childhood renal tumors were exclusioncriteria. Local computerized tomography stage was assigned by a single experi-enced pediatric radiologist blinded to the pathological stage, using a consensussimilar to the Children’s Oncology Group Wilms tumor staging system. Tumorswere stratified into up-front surgery and preoperative chemotherapy groups.The radiological stage of each tumor was compared to the pathological stage.
Results: A total of 189 tumors in 179 patients met inclusion criteria. Comput-erized tomography staging matched pathological staging in 68% of up-frontsurgery (70 of 103), 31.8% of pre-chemotherapy (21 of 66) and 48.8% of post-chemotherapy scans (42 of 86). Computerized tomography over staged 21.4%,65.2% and 46.5% of tumors in the up-front surgery, pre-chemotherapy and post-chemotherapy scans, respectively, and under staged 10.7%, 3% and 4.7%.Computerized tomography staging was more accurate in tumors managedby up-front surgery (p <0.001) and those without extracapsular extension(p <0.001).
Conclusions: The validity of computerized tomography staging of childhoodrenal tumors remains doubtful. This staging is more accurate for tumors treatedwith up-front surgery and those without extracapsular extension. Preoperativecomputerized tomography can help to exclude capsular breach. Treatmentstrategy should be based on surgical and pathological staging to avoid thehazards of inaccurate staging.
Key Words: kidney neoplasms; neoplasm staging;
tomography, x-ray computed; Wilms tumor
CHILDHOOD renal tumors accountfor 5% to 7% of pediatric cancers,ranking fifth among childhood ma-lignancies, with Wilms tumor beingthe most common.1,2 Congenitalmesoblastic nephroma, renal cell
22-5347/14/1921-0194/0
HE JOURNAL OF UROLOGY®
2014 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARC
carcinoma, clear cell sarcoma andrhabdoid tumor of the kidney aresome other important pathologicalentities. Although ultrasound is usu-ally the first ordered investigationfor a child presenting with an
H, INC.
http://dx.doi.org/10.1016/j.juro.2014.01.096
Vol. 192, 194-199, July 2014
Printed in U.S.A.
COMPUTERIZED TOMOGRAPHY STAGING IN CHILDHOOD KIDNEY TUMORS 195
abdominal mass, computerized tomography is nowconsidered the standard imaging modality forchildhood renal tumors.3e5 Magnetic resonanceimaging is now mainly used to differentiate betweenWilms tumor and nephrogenic rests, and to monitorthe response to preoperative chemotherapy tominimize radiation exposure.6e8
Staging and histopathology are the most impor-tant outcome predictors in patients with CRTs.9
Staging is based on surgical and pathological find-ings. The role of imaging studies in staging CRTshas been questionable. Previously published datahave demonstrated a poor correlation betweenradiological and pathological staging.5,10e13 How-ever, there is a paucity of literature about theaccuracy of CT in the staging of CRTs. Moreover,these studies were conducted on a limited numberof patients using old generation CT equipment. Ifpreoperative imaging could accurately detect localtumor extension and lymph node involvement,concerns regarding staging in patients treated withpreoperative therapy would be eliminated. Theneed for exploration would be obviated in patientswith unresectable tumors if resectability could bedetermined on preoperative imaging. In addition,patients with locally advanced disease wouldbenefit from preoperative chemotherapy to avoidtumor spillage with up-front surgery. This studywas conducted to identify the accuracy of CT inpredicting pathological stage in a larger cohortof patients diagnosed with CRTs at a singleinstitution.
MATERIALS AND METHODSFollowing internal review board approval, we retrospec-tively reviewed the database of patients diagnosed withCRTs and treated at a single center with radical or partialnephrectomy between August 1990 and October 2013.Inability to retrieve preoperative CT, intraoperativetumor spillage and tumors other than WT at final histo-pathological evaluation were exclusion criteria. We usedour electronic database to retrieve patient age at surgery,gender and tumor side. Preoperative therapy, operativedetails and pathology reports were reviewed. Tumorswere staged according to the COG Wilms tumor stag-ing system.
Before January 2006 preoperative computerized to-mograms were obtained using 4-slice multidetector CT(LightSpeed Plus, GE Healthcare, Milwaukee, Wiscon-sin). The abdomen was imaged from the diaphragmaticcopulae to the iliac crests at 5 mm slice thickness. Post-contrast images were done by repeating the scan afterinjection of 2 ml/kg nonionic contrast medium using anautomatic pump. Beginning in January 2006 computer-ized tomograms were obtained for all children using64-channel multidetector helical CT (Brilliance, Philips,Andover, Massachusetts) with a slice thickness of 2.5 mm.
The arterial phase images were obtained 50 seconds afterthe start of contrast injection followed by the venousphase 6 to 10 seconds later. In addition, multiplanarreformatted images were obtained in the sagittal andcoronal planes.
Pre-contrast and post-contrast images were reviewedby a single experienced pediatric radiologist (MEA) blin-ded to the pathological stage. Particular attention wasgiven to evidence of capsular breach, adjacent organinfiltration, lymph node involvement and vascular inva-sion. Capsular breach was diagnosed radiographicallybased on the presence of enhancing tissues in the peri-nephric fat, while direct infiltration of neighboring organswas diagnosed when tissue planes were lost or irregularmargins were seen between the tumor and the sur-rounding tissues. CT diagnosis of lymph node metastasesrelied on nodal enlargement greater than 1 cm in shortaxis diameter. Vascular tumor invasion was diagnosedwhen an intraluminal filling defect was seen within therenal vein, inferior vena cava or right atrium during theportal venous phase of the study.
Radiological stage was assigned by a consensus similarto the COG staging system. Tumors that appearedconfined to the kidney were assigned stage I, tumors withlocal extrarenal extension amenable to complete resectionwere assigned radiological stage II and locally advancedtumors not amenable to complete resection or withabdominal lymphadenopathy were assigned radiologicalstage III. Cases of metastatic disease (stage IV) werestaged according to local CT stage. Bilateral and multi-centric tumors were staged according to the local stageof each.
Cases were stratified into 2 groups, ie up-front surgery(group 1) and preoperative chemotherapy (group 2). Theprimary outcome was the relationship between CT stageand pathological stage for each tumor. For tumors treatedwith preoperative chemotherapy the radiological stagesbefore starting and after completion of chemotherapywere compared to the pathological stage. To calculate thesensitivity, specificity, PPV and NPV of extracapsulartumor extension detection by computerized tomography,patients with stage I disease were considered to haveintracapsular disease, while those with stage II or IIIdisease were considered to have extracapsular disease.
Continuous parametric variables were expressed asmean � SD while nonparametric variables wereexpressed as median (range). Categorical variables weredescribed as frequencies in each category. CT stage wascorrelated and tested for association with the pathologicalstage using the Spearman rho correlation coefficientand chi-square test, respectively. Sensitivity, specificity,PPV and NPV for diagnosis of extracapsular diseaseextension by CT were calculated. Statistical analysis wasdone using SPSS�, version 20, and p <0.05 was consid-ered statistically significant.
RESULTSA total of 263 children were diagnosed with CRTsat our institution during the study period, with189 Wilms tumors in 179 patients meeting inclusion

Figure 1. Axial post-contrast CT of abdomen (4-slice multi-
detector scanner) demonstrates heterogeneously enhancing
right renal tumor involving most of kidney without evident
extracapsular extension diagnosed in 2-year-old child. Patient
was treated with radical nephrectomy. Pathological stage
matched radiological stage (stage I).
196 COMPUTERIZED TOMOGRAPHY STAGING IN CHILDHOOD KIDNEY TUMORS
criteria. Up-front surgery was the line of treatmentin 103 tumors (54.5%, group 1), while 86 tumors(45.5%, group 2) were treated with preoperativechemotherapy. Pre-chemotherapy and post-chemotherapy CTs done by the same scannercould be retrieved in 76.7% of group 2 tumors (66of 86). Median interval between CT and surgerywas 8 days (range 1 to 65). Patient and tumorcharacteristics are outlined in table 1.
When correlating the local CT stage with thepathological stage, the Spearman rho correlationcoefficient was 0.426 in group 1 tumors (p <0.001),and 0.27 (p ¼ 0.028) and 0.428 (p <0.001) in group2 tumors in the pre-chemotherapy and post-chemotherapy scans, respectively. Local CT stagematched the pathological stage in 68% of group 1tumors (70 of 103), compared to 48.8% of group 2tumors (42 of 86) on post-chemotherapy scans(p <0.001, fig. 1). On reviewing the pre-chemotherapy scans the radiological staging wasaccurate in only 31.8% of tumors (21 of 66). Overstaging was observed in 22 tumors (21.4%) in group1, and in 43 (65.2%) and 40 tumors (46.5%) in pre-chemotherapy and post-chemotherapy scans ingroup 2 (figs. 2 and 3), while under staging wasobserved in 11 tumors (10.7%) in group 1, and in2 (3%) and 4 tumors (4.7%) in pre-chemotherapy andpost-chemotherapy scans in group 2. Matching wasbest in tumors that were radiological stage I (82.2%of group 1, and 92.3% and 93.8% of group 2 tumors inpre-chemotherapy and post-chemotherapy scans,respectively), while it was worst for those that wereradiological stage II (30.8% of group 1, and 5.9%and 5% of group 2 tumors in pre-chemotherapy andpost-chemotherapy scans, respectively, p <0.001).The correlation between radiological and patholog-ical staging in both groups was cross-tabulated
Table 1. Patient and tumor characteristics
Median yrs pt age (range) 3 (0.16e15)No. gender (%):
Male 102 (54)Female 87 (46)
No. laterality (%):Rt 98 (51.9)Lt 91 (48.1)
Mean � SD largest tumor diameter (cm) 10.6 � 3.94No. treatment (%):
Up-front surgery 103 (54.5)Preop chemotherapy 86 (45.5)
No. pathology status (%):Favorable 169 (89.4)Unfavorable 20 (10.6)
No. local CT stage (%):I 96 (50.8)II 33 (17.5)III 60 (31.7)
No. pathological stage (%):I 135 (71.4)II 19 (10.1)III 35 (18.5)
(table 2). Sensitivity, specificity, PPV and NPV forextracapsular tumor extension by preoperative CTare outlined in table 3.
DISCUSSIONSurvival in patients with CRTs has improveddramatically in the last few decades. An excellent
Figure 2. Post-chemotherapy axial contrast enhanced CT of
abdomen (4-slice multidetector scanner) reveals right renal
tumor in 3-year-old child treated with 4 weeks of vincristine and
actinomycin D. Tumor was assigned radiological stage II based
on capsular breach (arrows). On histopathological examination
tumor was confined to kidney with no extracapsular extension
(stage I).
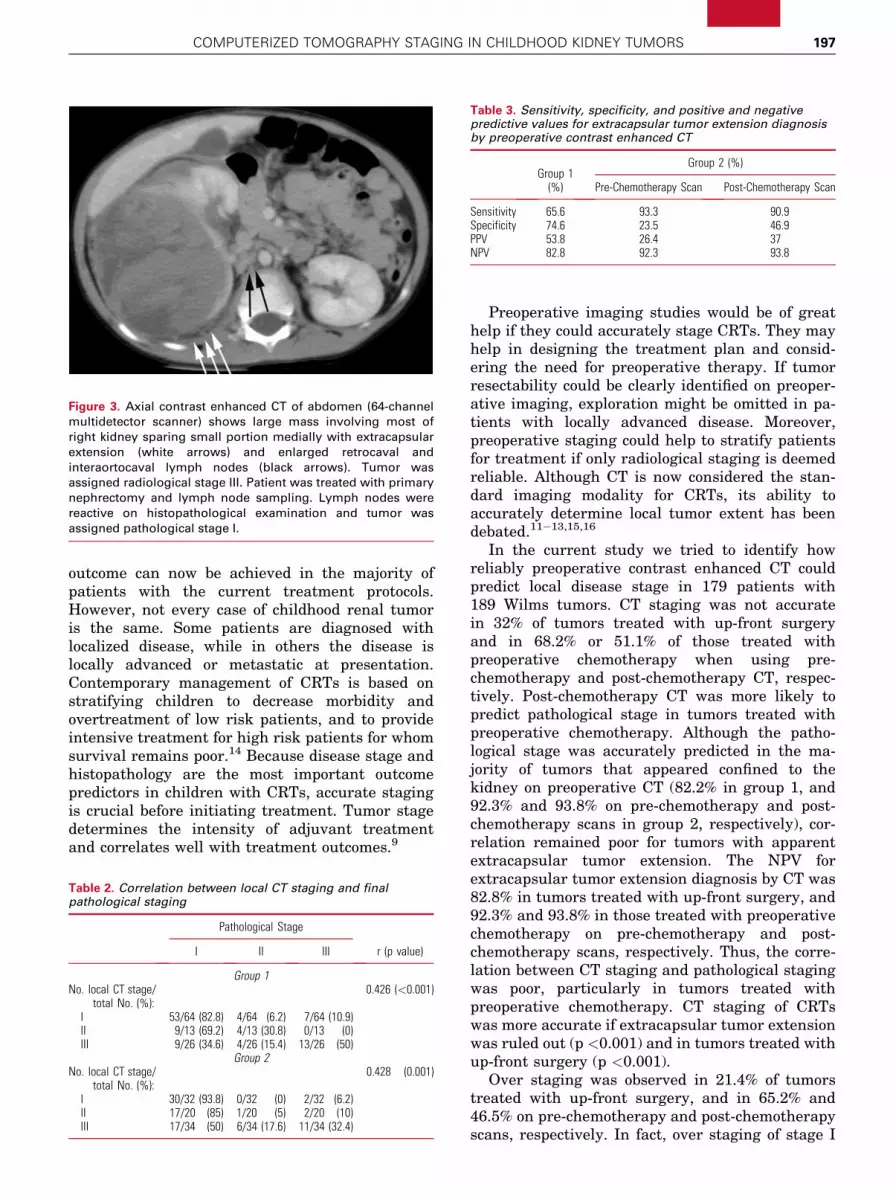
Table 3. Sensitivity, specificity, and positive and negativepredictive values for extracapsular tumor extension diagnosisby preoperative contrast enhanced CT
Group 1(%)
Group 2 (%)
Pre-Chemotherapy Scan Post-Chemotherapy Scan
Sensitivity 65.6 93.3 90.9Specificity 74.6 23.5 46.9PPV 53.8 26.4 37NPV 82.8 92.3 93.8
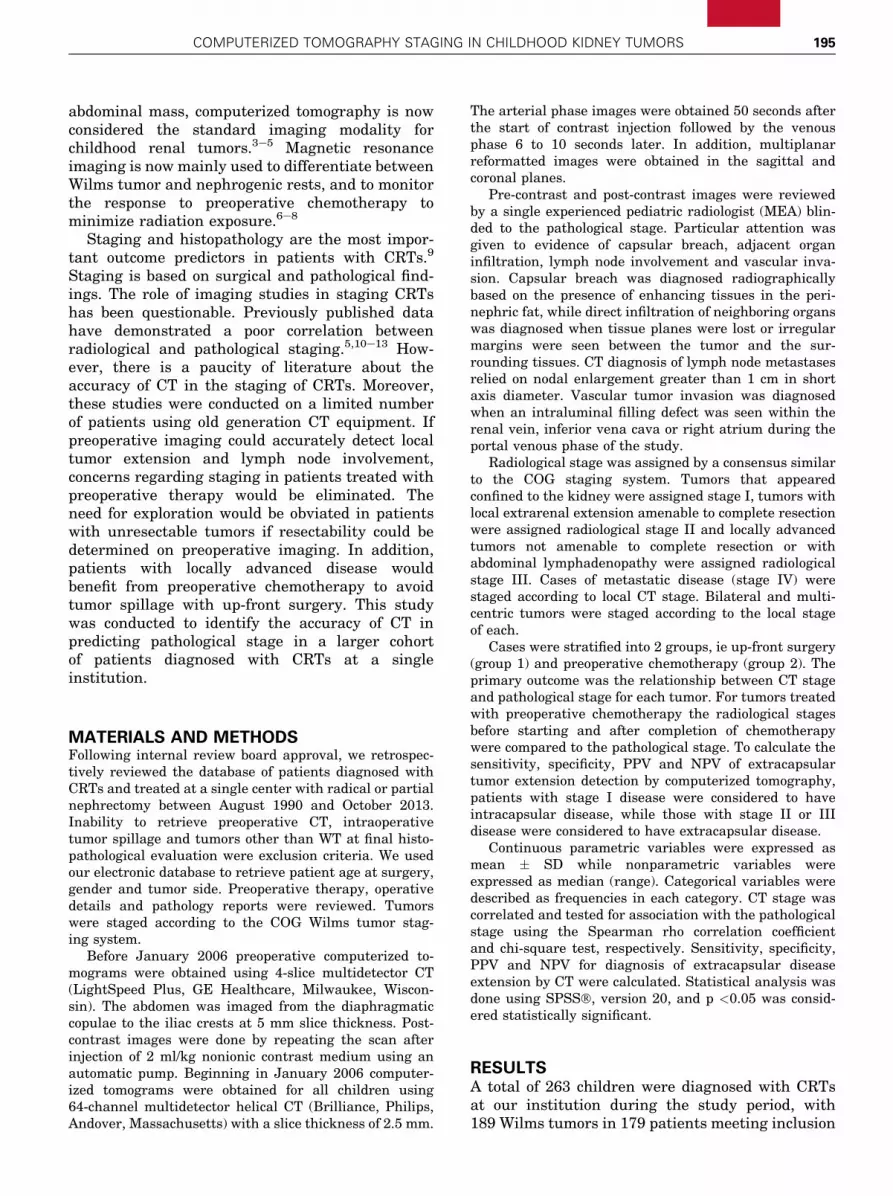
Figure 3. Axial contrast enhanced CT of abdomen (64-channel
multidetector scanner) shows large mass involving most of
right kidney sparing small portion medially with extracapsular
extension (white arrows) and enlarged retrocaval and
interaortocaval lymph nodes (black arrows). Tumor was
assigned radiological stage III. Patient was treated with primary
nephrectomy and lymph node sampling. Lymph nodes were
reactive on histopathological examination and tumor was
assigned pathological stage I.
COMPUTERIZED TOMOGRAPHY STAGING IN CHILDHOOD KIDNEY TUMORS 197
outcome can now be achieved in the majority ofpatients with the current treatment protocols.However, not every case of childhood renal tumoris the same. Some patients are diagnosed withlocalized disease, while in others the disease islocally advanced or metastatic at presentation.Contemporary management of CRTs is based onstratifying children to decrease morbidity andovertreatment of low risk patients, and to provideintensive treatment for high risk patients for whomsurvival remains poor.14 Because disease stage andhistopathology are the most important outcomepredictors in children with CRTs, accurate stagingis crucial before initiating treatment. Tumor stagedetermines the intensity of adjuvant treatmentand correlates well with treatment outcomes.9
Table 2. Correlation between local CT staging and finalpathological staging
Pathological Stage
r (p value)I II III
Group 1No. local CT stage/
total No. (%):0.426 (<0.001)
I 53/64 (82.8) 4/64 (6.2) 7/64 (10.9)II 9/13 (69.2) 4/13 (30.8) 0/13 (0)III 9/26 (34.6) 4/26 (15.4) 13/26 (50)
Group 2No. local CT stage/
total No. (%):0.428 (0.001)
I 30/32 (93.8) 0/32 (0) 2/32 (6.2)II 17/20 (85) 1/20 (5) 2/20 (10)III 17/34 (50) 6/34 (17.6) 11/34 (32.4)
Preoperative imaging studies would be of greathelp if they could accurately stage CRTs. They mayhelp in designing the treatment plan and consid-ering the need for preoperative therapy. If tumorresectability could be clearly identified on preoper-ative imaging, exploration might be omitted in pa-tients with locally advanced disease. Moreover,preoperative staging could help to stratify patientsfor treatment if only radiological staging is deemedreliable. Although CT is now considered the stan-dard imaging modality for CRTs, its ability toaccurately determine local tumor extent has beendebated.11e13,15,16
In the current study we tried to identify howreliably preoperative contrast enhanced CT couldpredict local disease stage in 179 patients with189 Wilms tumors. CT staging was not accuratein 32% of tumors treated with up-front surgeryand in 68.2% or 51.1% of those treated withpreoperative chemotherapy when using pre-chemotherapy and post-chemotherapy CT, respec-tively. Post-chemotherapy CT was more likely topredict pathological stage in tumors treated withpreoperative chemotherapy. Although the patho-logical stage was accurately predicted in the ma-jority of tumors that appeared confined to thekidney on preoperative CT (82.2% in group 1, and92.3% and 93.8% on pre-chemotherapy and post-chemotherapy scans in group 2, respectively), cor-relation remained poor for tumors with apparentextracapsular tumor extension. The NPV forextracapsular tumor extension diagnosis by CT was82.8% in tumors treated with up-front surgery, and92.3% and 93.8% in those treated with preoperativechemotherapy on pre-chemotherapy and post-chemotherapy scans, respectively. Thus, the corre-lation between CT staging and pathological stagingwas poor, particularly in tumors treated withpreoperative chemotherapy. CT staging of CRTswas more accurate if extracapsular tumor extensionwas ruled out (p <0.001) and in tumors treated withup-front surgery (p <0.001).
Over staging was observed in 21.4% of tumorstreated with up-front surgery, and in 65.2% and46.5% on pre-chemotherapy and post-chemotherapyscans, respectively. In fact, over staging of stage I

198 COMPUTERIZED TOMOGRAPHY STAGING IN CHILDHOOD KIDNEY TUMORS
tumors to stage II might be clinically insignificant(fig. 2), because both groups would be treated simi-larly with 18 weeks of vincristine and actinomycin D.In contrast, up-staging cases of stage I or II diseaseto stage III is significant (fig. 3), since patients withstage III disease are treated with 24 weeks of post-operative chemotherapy, including the cardiotoxicdrug doxorubicin. In addition, radiation therapy isessential for patients with stage III disease (COGprotocol AREN0532). However, radiation therapycarries an added risk of growth retardation, skeletaldeformities, negative fertility impact and secondarymalignant neoplasms.17
Preoperative therapy, with the risk of inaccuratestaging, might be considered if the primary surgeryseems to be too hazardous. However, 10.7% of tu-mors managed by primary surgery, and 4.7% and3% of those managed by preoperative chemotherapywere assigned a lower disease stage on pre-chemotherapy and post-chemotherapy CT staging,respectively. Patients with stage III disease mightbe at greater risk for relapse if a less aggressiveadjuvant treatment is administered secondary tounder staging.
Hence, over and under staging might haveserious consequences regarding the treatmentplan and subsequently relapse rates, long-termmorbidity and patient survival. Therefore, treat-ment strategies should rely on surgical and patho-logical staging to avoid the hazards of over andunder staging.
The implication of radiological staging in child-hood malignant abdominal tumors in general andrenal tumors in particular has met with severalconstraints in the previous literature. Damgaard-Pedersen et al questioned the ability of CT todetect local tumor invasiveness and lymph nodeinvolvement in 56 patients with various types ofextracranial solid malignant tumors.15 In a studycarried out by Ng et al liver invasion was incorrectlydiagnosed by CT in 4 of 18 children diagnosedwith WT.18
Several authors have noted difficulty in detectingnodal disease in patients with WT.18e20 Zoelleret al reported down staging in 2 of 11 children withWT based on radiological findings.10 Gow et altried to correlate CT stage and pathological stage in26 children with unilateral nonmetastatic WT.11
CT correctly staged 38.5% and over staged 46.1%of cases. In that study CT images were acquiredat 10 mm slice thickness.
The COG authors reported that CT had a sensi-tivity of 65.6% and a specificity of 84.8% for detectionof tumor thrombus in patients treated with primarynephrectomy, and a sensitivity of 86.7% and speci-ficity of 90.6% for patients treated with preoperativetherapy.12 CT hadmoderate specificity but relatively
low sensitivity in the detection of preoperative WTrupture in patients enrolled in the AREN03B2study by COG.13 Thus, the previously publisheddata revealed a poor correlation between radiolog-ical and pathological staging in CRTs. However,most of these series are limited by small numbers ofpatients and outdated imaging techniques.
To our knowledge, this is the largest contempo-rary series addressing the correlation betweenradiological and pathological staging in patientswith CRTs. In this study the accuracy of CT stagingis better than what has previously been reported.This finding may be explained by the evolution ofimaging techniques with the use of helical scannersand smaller slice thickness. Nevertheless, radio-logical staging was not reliable in a substantial setof patients. Thus, CT staging of CRTs should beinterpreted cautiously, bearing in mind the serioushazards of over and under staging. Moreover, thisstudy is the first to address the impact of treatmentstrategy (up-front surgery vs preoperative chemo-therapy) on the accuracy of radiological staging.
This study is not without limitations, notably itsretrospective nature. The study cohort is also rela-tively small to draw solid conclusions. In addition,the study was conducted during a long intervalusing 2 different CT machines. Although the accu-racy of CT staging is better with the new machine(61.7% vs 57.4%), the difference did not reach sta-tistical significance (p ¼ 0.55). Although the NPVfor diagnosing extracapsular tumor extension washigh, this finding may be explained by the relativelysmall number of tumors with truly extracapsulardisease. Moreover, radiological staging is subjectiveand vulnerable to intraobserver and interobserverdifferences, lacks clearly defined criteria and mightbe limited by the expertise of the radiologist.Finally, intraoperative tumor spillage, which mightup stage CRTs, is unpredictable with preoperativeimaging.
CONCLUSIONSAlthough CT is a valuable tool in diagnosing CRT,the correlation between CT staging and pathologicalstaging remained poor, particularly in tumorsmanaged by preoperative chemotherapy. CT stagingwas more accurate in tumors that appeared intra-capsular and tumors managed by up-front surgery.CT might be helpful to rule out extracapsular tumorextension. Therefore, the treatment algorithmshould be based on surgical and pathological stag-ing. Our results need to be validated in largerstudies. Hopefully advances in imaging techniquesand the use of other imaging modalities, such asmagnetic resonance imaging, will improve the roleof radiological staging in pediatric renal tumors.

COMPUTERIZED TOMOGRAPHY STAGING IN CHILDHOOD KIDNEY TUMORS 199
REFERENCES
1. Breslow NE, Beckwith JB, Perlman EJ et al: Agedistributions, birth weights, nephrogenic rests,and heterogeneity in the pathogenesis of Wilmstumor. Pediatr Blood Cancer 2006; 47: 260.
2. Ries LA, Smith MA, Gurney JG et al: CancerIncidence and Survival among Children andAdolescents: United States SEER Program1975-1995. Bethesda, Maryland: National Can-cer Institute, SEER Program 1999. NIH Pub No.99-4649; pp vi, 182.
3. Goske MJ, Mitchell C and Reslan WA: Imagingof patients with Wilms’ tumor. Semin Urol Oncol1999; 17: 11.
4. Riccabona M: Imaging of renal tumours ininfancy and childhood. Eur Radiol, suppl., 2003;13: L116.
5. Kembhavi SA, Qureshi S, Vora T et al: Under-standing the principles in management ofWilms’ tumour: can imaging assist in patientselection? Clin Radiol 2013; 68: 646.
6. Rohrschneider WK, Weirich A, Rieden K et al: US,CT and MR imaging characteristics of nephro-blastomatosis. Pediatr Radiol 1998; 28: 435.
7. Schenk JP, Graf N, G€unther P et al: Role ofMRI in the management of patients with neph-roblastoma. Eur Radiol 2008; 18: 683.
8. Hoffer FA: Magnetic resonance imaging ofabdominal masses in the pediatric patient.Semin Ultrasound CT MR 2005; 26: 212.
9. D’Angio GJ, Breslow N, Beckwith JB et al:Treatment of Wilms’ tumor. Results of theThird National Wilms’ Tumor Study. Cancer1989; 64: 349.
10. Zoeller G, Pekrun A, Lakomek M et al: Stagingproblems in the pre-operative chemotherapyof Wilms’ tumour. Br J Urol 1995; 76: 501.
11. Gow KW, Roberts IF, Jamieson DH et al: Localstaging of Wilms’ tumordcomputerized tomog-raphy correlation with histological findings.J Pediatr Surg 2000; 35: 677.
12. Khanna G, Rosen N, Anderson JR et al: Evalua-tion of diagnostic performance of CT for detectionof tumor thrombus in children with Wilms tumor:a report from the Children’s Oncology Group.Pediatr Blood Cancer 2012; 58: 551.
13. Khanna G, Naranjo A, Hoffer F et al: Detectionof preoperative Wilms tumor rupture with CT:
a report from the Children’s Oncology Group.Radiology 2013; 266: 610.
14. Metzger ML and Dome JS: Current therapy forWilms’ tumor. Oncologist 2005; 10: 815.
15. Damgaard-Pedersen K, Yssing M and MauritzenK: CT in the staging of children with malignanttumours. Pediatr Radiol 1982; 12: 139.
16. Cohen MD: Staging of Wilms’ tumour. ClinRadiol 1993; 47: 77.
17. Wright KD, Green DM and Daw NC: Late effectsof treatment for Wilms tumor. Pediatr HematolOncol 2009; 26: 407.
18. Ng YY, Hall-Craggs MA, Dicks-Mireaux C et al:Wilms’ tumour: pre- and post-chemotherapy CTappearances. Clin Radiol 1991; 43: 255.
19. Othersen HB Jr, DeLorimer A, Hrabovsky E et al:Surgical evaluation of lymph node metastasesin Wilms’ tumor. J Pediatr Surg 1990; 25: 330.
20. Cushing B and Slovis TL: Imaging of Wilms’ tumor:what is important! Urol Radiol 1992; 14: 241.
EDITORIAL COMMENT
Stage is a major determinant for therapy in Wilms chemotherapy, and cannot replace the role of
tumor. In this study the authors evaluated whetherCT could accurately predict local and disease stagein patients with Wilms tumor treated with primaryor delayed nephrectomy. Despite improved imagingcapabilities during the last few decades, the resultsare disappointing. In this study CT over staged up to65% of the cases and under staged almost 11%. Theseerrors are clinically significant, as over staging canresult in excess therapy such as unnecessary expo-sure to doxorubicin and radiation, with the associ-ated short and long-term morbidity. Converselyunder treatment risks relapse. Prior work has alsoshown that CT cannot predict preoperative tumorrupture or nodal status. Therefore, CT alone does notallow for accurate initial or subsequent staging forpatients enrolled in studies that use up-frontup-front surgical staging for selection of optimalrisk based therapy (references 11 to 13 in article).
Peter F. EhrlichDepartment of Surgery
University of Michigan Medical School
Ann Arbor, Michigan
and Surgery Renal Tumors Committee
Children’s Oncology Group
and
Fernando FerrerDivision Pediatric Urology
Connecticut Children’s Medical Center
and Department of Surgery
University of Connecticut School of Medicine
Farmington, Connecticut
Related Documents











