Can Chronic Intra-Abdominal Hypertension Cause Oxidative Stress to the Abdominal Wall Muscles? An Experimental Study Efstathios Kotidis, M.Sc., Ph.D.,* ,1 Theodosis Papavramidis,* Konstantinos Ioannidis,* George Koliakos,† Thomai Lazou,* Aggeliki Cheva,‡ Michalopoulos Nikolaos,* and Papavramidis Spiros* Q2 *AHEPA Hospital, C’ Department of Surgery; †Faculty of Biochemistry; and ‡Faculty of Pathology, Aristotle University of Thessaloniki, Thessaloniki, Greece Originally submitted April 7, 2011; accepted for publication July 11, 2011 Background. The aim of this study was to test the hypothesis that intra-abdominal hypertension alone could trigger such changes to the rectus abdominis muscle that would lead to an imbalance between oxi- dant production and antioxidant protection. Materials and Methods. Forty-five New Zealand white rabbits were divided into three groups and a rub- ber bag was implanted into their peritoneal cavity. In group A (n [ 15), the bag was empty. In group B (n [ 15), it was filled with normal saline to achieve an intra-abdominal pressure of over 12 mm Hg. In group C(n [ 15), it was filled with lead equiponderant to the mean weight of the normal saline injected in group B. After 8 weeks, we measured in rectus abdom- inis muscle biopsies the lipid peroxidation products, the protein carbonyl content, the total glutathione and superoxide dismutase (SOD) concentration, the activity of glutathione reductase and glutathione per- oxidase, and the pro-oxidant–antioxidant balance. Results. The lipid peroxidation products were sig- nificantly higher in group B compared with both group A(P [ 0.026) and group C (P < 0.001). The total protein carbonyl content was significantly higher in group B compared with both group A (P [ 0.006) and group C (P < 0.001). No difference was found between the three groups in total glutathione (P [ 0.735) and SOD (P [ 0.410) concentration. Glutathione peroxidase activity was higher in groups B and C compared with group A (P [ 0.05 and P [ 0.003, respectively). Glutathione re- ductase activity was higher in group B compared with group A (P [ 0.005) and group C (P [ 0.001). The pro-oxidant antioxidant balance was higher in group B compared with the group A (P [ 0.012). Conclusions. Maintaining the IP over 12 mm Hg for 8 wk caused increased oxidative damage to both lipids and proteins with an increased pro-oxidant–antioxi- dant balance. In an attempt to compensate for this damage the muscle fibers increased their glutathione reductase and glutathione peroxidase activity. Ó 2011 Elsevier Inc. All rights reserved. Key Words: intra-abdominal hypertension; oxidative stress; rectus abdominis muscle; SOD; superoxide dis- mutase; glutathione; glutathione peroxidase; glutathi- one reductase; lipid peroxidation; protein carbonyls; pro-oxidant–antioxidant balance. INTRODUCTION Intra-abdominal pressure is defined as the pressure concealed within the abdominal cavity, and in critically ill patients, it is approximately 5 to 7 mm Hg. According to the World Society of the Abdominal Compartment Syndrome consensus statements, intra-abdominal hy- pertension (IAH) is defined as a sustained or repeated pathologic elevation of intra-abdominal pressure (IAP) over 12 mm Hg [1]. A wide variety of physiologic as well as pathologic conditions can lead to chronically increased intra-abdominal pressure. Obesity is virtually the most common clinical condition causing chronic intra- abdominal hypertension. Indeed, there is a linear corre- lation between BMI and intra-abdominal pressure (IP) in patients with BMI > 40 Kg/m 2 [2]. Several studies have been published on the effect of acute intra-abdomi- nal hypertension and abdominal compartment syndrome on various organs and systems. Simultaneously, several clinical problems, including hypertension, congestive 1 To whom correspondence and reprint requests should be ad- dressed at C’ Department of General Surgery, AHEPA University Hospital, 51 Amalias Street, 54640 Thessaloniki, Greece. E-mail: [email protected] or [email protected]. 0022-4804/$36.00 Ó 2011 Elsevier Inc. All rights reserved. 1 FLA 5.1.0 DTD ĸ YJSRE10931_proof ĸ 9 August 2011 ĸ 3:37 pm ĸ ce Journal of Surgical Research -, 1–6 (2011) doi:10.1016/j.jss.2011.07.020 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Q2
Journal of Surgical Research -, 1–6 (2011)doi:10.1016/j.jss.2011.07.020
123456789
1011121314151617181920212223242526272829303132333435363738394041424344454647484950
51525354
5556575859606162636465Can Chronic Intra-Abdominal Hypertension Cause Oxidative Stress to the
Abdominal Wall Muscles? An Experimental Study
Efstathios Kotidis, M.Sc., Ph.D.,*,1 Theodosis Papavramidis,* Konstantinos Ioannidis,* George Koliakos,†Thomai Lazou,* Aggeliki Cheva,‡ Michalopoulos Nikolaos,* and Papavramidis Spiros*
*AHEPAHospital, C’ Department of Surgery; †Faculty of Biochemistry; and ‡Faculty of Pathology, Aristotle University of Thessaloniki,Thessaloniki, Greece
Originally submitted April 7, 2011; accepted for publication July 11, 2011
6667686970717273747576777879808182838485868788899091929394
Background. The aim of this study was to test thehypothesis that intra-abdominal hypertension alonecould trigger such changes to the rectus abdominismuscle that would lead to an imbalance between oxi-dant production and antioxidant protection.Materials and Methods. Forty-five New Zealand
white rabbitsweredivided into three groups anda rub-ber bag was implanted into their peritoneal cavity.In group A (n [ 15), the bag was empty. In group B(n [ 15), it was filled with normal saline to achieve anintra-abdominal pressure of over 12 mm Hg. In groupC (n [ 15), it was filled with lead equiponderant tothe mean weight of the normal saline injected ingroup B. After 8 weeks, we measured in rectus abdom-inis muscle biopsies the lipid peroxidation products,the protein carbonyl content, the total glutathioneand superoxide dismutase (SOD) concentration, theactivity of glutathione reductase and glutathione per-oxidase, and the pro-oxidant–antioxidant balance.Results. The lipid peroxidation products were sig-
nificantly higher in groupB comparedwith both groupA (P[ 0.026) and groupC (P< 0.001). The total proteincarbonyl content was significantly higher in group Bcompared with both group A (P [ 0.006) and group C(P< 0.001). No differencewas found between the threegroups in total glutathione (P [ 0.735) and SOD (P [0.410) concentration. Glutathione peroxidase activitywas higher in groups B and C compared with group A(P [ 0.05 and P [ 0.003, respectively). Glutathione re-ductase activity was higher in group B comparedwith group A (P [ 0.005) and group C (P [ 0.001). The
1 To whom correspondence and reprint requests should be ad-dressed at C’ Department of General Surgery, AHEPA UniversityHospital, 51 Amalias Street, 54640 Thessaloniki, Greece. E-mail:[email protected] or [email protected].
1
FLA 5.1.0 DTD � YJSRE10931_proo
pro-oxidant antioxidant balance was higher in groupB compared with the group A (P [ 0.012).Conclusions. Maintaining the IP over 12 mm Hg for
8 wk caused increased oxidative damage to both lipidsand proteins with an increased pro-oxidant–antioxi-dant balance. In an attempt to compensate for thisdamage the muscle fibers increased their glutathionereductase and glutathione peroxidase activity. � 2011
Elsevier Inc. All rights reserved.
Key Words: intra-abdominal hypertension; oxidativestress; rectus abdominis muscle; SOD; superoxide dis-mutase; glutathione; glutathione peroxidase; glutathi-one reductase; lipid peroxidation; protein carbonyls;pro-oxidant–antioxidant balance.
9596979899
100101
INTRODUCTION
Intra-abdominal pressure is defined as the pressureconcealed within the abdominal cavity, and in criticallyill patients, it is approximately 5 to 7 mmHg. Accordingto the World Society of the Abdominal CompartmentSyndrome consensus statements, intra-abdominal hy-pertension (IAH) is defined as a sustained or repeatedpathologic elevation of intra-abdominal pressure (IAP)over 12 mmHg [1]. A wide variety of physiologic as wellas pathologic conditions can lead to chronically increasedintra-abdominal pressure. Obesity is virtually the mostcommon clinical condition causing chronic intra-abdominal hypertension. Indeed, there is a linear corre-lation between BMI and intra-abdominal pressure (IP)in patients with BMI > 40 Kg/m2 [2]. Several studieshave been published on the effect of acute intra-abdomi-nalhypertensionandabdominal compartment syndromeon various organs and systems. Simultaneously, severalclinical problems, including hypertension, congestive
0022-4804/$36.00� 2011 Elsevier Inc. All rights reserved.
f � 9 August 2011 � 3:37 pm � ce
102103104105

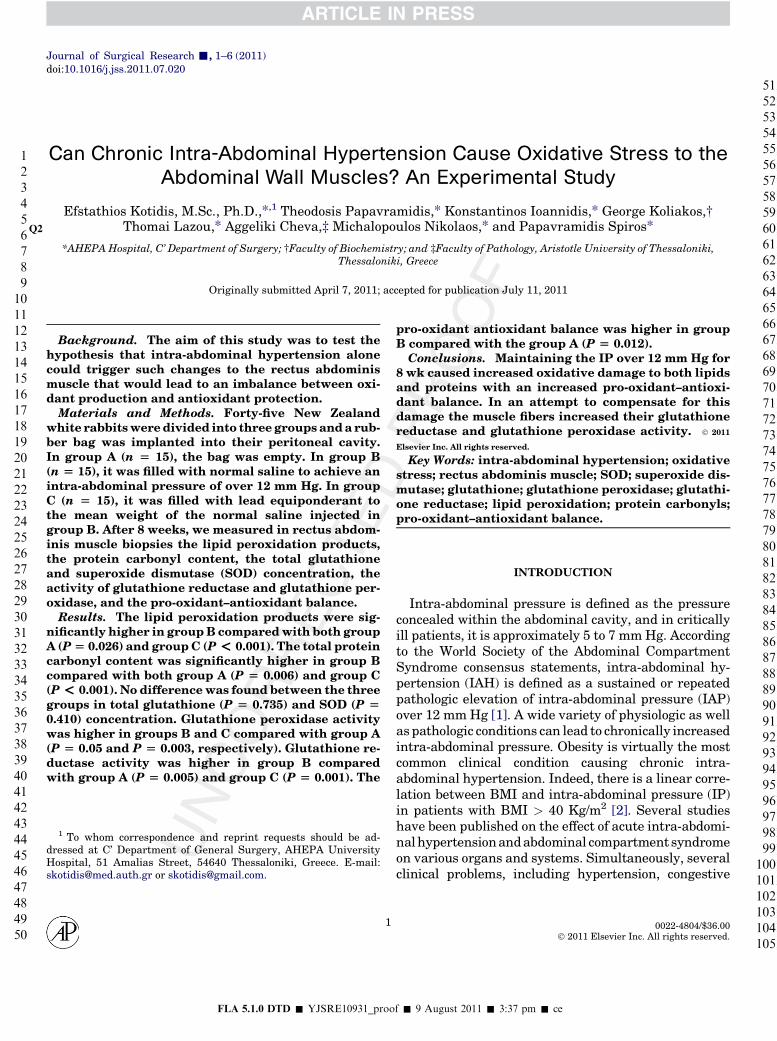
FIG. 1. Schematic representation of the experimental model ofincreased IAP. Q13
JOURNAL OF SURGICAL RESEARCH: VOL. -, NO. -, - 20112
106107108109110111112113114115116117118119120121122123124125126127128129130131132133134135136137138139140141142143144145146147148149150151152153154155156157158159160
161162163164165166167168169170171172173174175176177178179180181
heart failure, sleep apnea syndrome, and gastroesopha-geal reflux disease, have been proved to be directly re-lated to increased intra-abdominal pressure [3–6].Nevertheless, the impact of chronic intra-abdominal hy-pertension on the oxidative balance in the abdominalwall muscles has never been studied before.
Oxidative stress is the state wherein the normallywell balanced control of oxidant production and antiox-idant activity is disturbed. There are numerous sourcesof oxidants in the skeletal muscles.Most of them are de-rived from enzymatic or chemical reactions that pro-duce superoxide anion, hydrogen peroxide (H2O2), ornitric oxide (NO). Once produced, these species convertto secondary, highly reactive oxygen species (ROS) andreactive nitrogen species (RNS) such as hydroxyl radi-cal (OH∙) and peroxinitrate (ONOO�) [7]. The aim ofthe present study is to test the hypothesis that intra-abdominal hypertension alone could trigger suchchanges to the rectus abdominis muscle that wouldlead to an imbalance between oxidant production andantioxidant activity.
182183184185186187188189190191192193194195196197198199
MATERIALS AND METHODS
Animals
The studywas conductedwith the permission of the local veterinaryauthorities and the scientific council of AHEPA University Hospital,complying with all the relative European directives. Anesthesia, in-traoperative monitoring, recovery, and sacrifice were done by a spe-cialized veterinarian. Forty-five male New Zealand white rabbits ofthe same age and weight were used. The animals were divided intothree groups. In all animals, we implanted the same rubber bag intotheir peritoneal cavity. In group A (control group, n ¼ 15) the bagswere kept empty. In group B (n ¼ 15), the IP was constantly keptover 12mmHgpressure, which defines intra-abdominal hypertensionin humans, by filling the rubber bag with normal saline. In group C(n¼ 15), the intra-abdominal bags were filled with lead covered by sil-icon, equiponderant to the average weight of normal saline used ingroup B. Group C was necessary to ensure that potential changes ingroup B would be caused by the increased intra-abdominal pressurerather than the weight of the normal saline.
200201202203204205206207208209210211212213214215
Surgical Procedure
The system used to increase the intra-abdominal pressure con-sisted of three parts [8, 9]. The rubber bag with a capacity of 300mL, the connecting tube, and the valve for external control ofintra-abdominal pressure, similar to the valve used in adjustablegastric bands (Fig. 1). To reduce the volume of the large intestine’scontents, the animals were starved for 3 d before operation. Thesystem was implanted in theater, with the animals deeply anaes-thetized with intramuscular administration of ketamine hydro-chloride 35 mg/kg and xylazine 5 mg/kg, and after they receiveda prophylactic dose of cefuroxime. After the application of local an-tiseptics, we made a small incision in the lateral abdominal wall,and without dividing the muscle, we opened the peritoneum and in-serted the rubber bag into the abdominal cavity, keeping its orificeoutside the muscle layer. We filled the tube with air to ensure theunobstructed air entry and to rule out any leak. Then, we emptiedthe bag and fixed it on the muscle layer with a purse string suture.We performed a second skin incision at the neck and created a
FLA 5.1.0 DTD � YJSRE10931_proo
subcutaneous tunnel connecting the two skin incisions. Throughthis tunnel, we introduced the connecting tube. The control valvewas then connected to the tube and anchored on the fascia with in-terrupted sutures. After completing the connections, we checkedthe IP using amanometer. In group B, we filled the bag with normalsaline to achieve IP of 12 mmHg. The level of IP was checked againafter the animals had fully recovered andwas adjusted accordingly.In group C, we filled the rubber bag with lead covered with silicon.The weight of the lead was 120 g, equal to the average weight of nor-mal saline used in group B. After surgery, the rabbits were kept for8 wk in individual cages with food and water available ad libitum.The decision to maintain the increased IAP for 8 wk was based ona previous study [10] that showed that the rectus abdominis muscleof the rabbit needs at least a 70-d period to display any phenotypicchanges. The animals adapted readily to the intra-abdominal appli-ance and showed no obvious discomfort. The IP was checked every 3d by puncturing the valve at the back of the neck with a 18 g needle.The needle was then connected to the manometer, and the IAP wasmeasured and adjusted accordingly.
Biochemical Analysis
The animalswere sacrificed and biopsies of the rectus abdominismus-cle were put into a Petri dish containing normal saline. After extraction,a series of biochemical assays was performed. Pro-oxidant–antioxidantbalance was determined following the protocol proposed by Alamdarietal. [11].Theassay for lipidperoxidationwasdone following theprotocolproposed by Ohkawa et al. [12]. Protein carbonyl content was measuredby using the protocol published by Alamdari et al. [13].The superoxidedismutase activity assay was done according to the procedure describedbyTatzber et al. [14]. Total glutathionewasdeterminedafter theprotocolproposedbyTeare etal. [15].Theglutathionereductaseactivitywasmea-sured following the protocol proposed by Cribb et al. [16]. Glutathioneperoxidase activity wasmeasured following the protocol proposed by Pa-glia and Valentine [17].
Statistical Analysis
The statistical analysis was done using the statistical packageSPSS 15 for windows (SPSS Inc., Chicago, IL). All parameterswere expresses as mean 6 SD. Kruskall-Wallis test was performedto check for differences between the three groups. In case of statis-tically significant difference, this was followed by a paired Mann-Whitney U test. The level of statistical significance was P < 0.05.
f � 9 August 2011 � 3:37 pm � ce

Q1KOTIDIS ET AL.: CHRONIC INTRA-ABDOMINAL HYPERTENSION 3
216217218219220221222223224225226227228229230231232233234235236237238239240241242243244245246247248249250251252253254255256257258259260261262263264265266267268269270
271272273274275276277278279280281282283284285286287288289290291292293294295296297298299300301302303304305306307308309310311312313314
RESULTS
The three groups were comparable in body weightboth at the time of surgery as well as at the time of sac-rifice. The mean volume of normal saline used to main-tain the intra-abdominal pressure at the level of 12 mmHg in group Bwas 120mL. Themean IP in group Awas0.7 mmHg and in group C 2.9 mmHg (Table 1). On sac-rifice, loose adhesions between the tube and the adja-cent organs were noted. However, they did not affectthe integrity of the tube, and no leak of fluid was noted.
The results of the biochemical tests are summa-rized in Table 2. Lipid peroxidation was significantlyhigher in the group with the chronically increased IP(group B) compared with both group A (P ¼ 0.026)and group C (P < 0.001). On the contrary, chargingwith lead in group C caused no change in lipid perox-idation compared to group A (P ¼ 0.775). Similarly,the total protein carbonyl content was significantlyhigher in group B compared with both group A (P ¼0.006) and group C (P < 0.001), whereas no differencewas found between groups A and C (P ¼ 0.233).Therefore, the chronically increased IP caused signif-icantly higher oxidative damage on both lipids andprotein molecules in the rectus abdominis muscle.
Regarding the antioxidant defense of the muscle fi-bers, no difference was found between the three groupsin total glutathione (P ¼ 0.735) and SOD (P ¼ 0.410).On the contrary, glutathione peroxidase activity washigher in groups B and C compared with group A (P ¼0.05 and P ¼ 0.003, respectively). Glutathione peroxi-dase activity was actually even higher in group Cthan in group B (P ¼ 0.037). Significant differencewas also found in glutathione reductase activity, whichwas higher in group B compared with group A (P ¼0.005) and group C (P ¼ 0.001) whereas no differencewas found in glutathione reductase activity betweengroups B and C (P¼ 0.744). This means that themusclefibers tried to compensate for the overproduction of ox-idants, due to the chronic intra-abdominal hyperten-sion, by increasing their antioxidant capacity in theform of increased glutathione reductase and glutathi-one peroxidase activity, although the total glutathioneconcentration remained unchanged.
TABLE 1
Animal Characteristics
Group A Group B Group C
Initial weight (kg) 3.1 6 0.2 3.2 6 0.3 3.1 6 0.3Final weight (kg) 3.7 6 0.5 3.5 6 0.4 3.6 6 0.4Mean IP (cm H2O) 1 16 4Volume of natural saline (mL) – 120 6 24 –
FLA 5.1.0 DTD � YJSRE10931_proo
The pro-oxidant–antioxidant balance was higher ingroup B compared with the control group A (P ¼0.012) but not compared with group C (P ¼ 0.089). Nodifference was also found between groups A and C(0.217). This means that both intra-abdominal hyper-tension and weight charging did cause a degree of oxi-dative damage that was better compensated in thegroup of animals charged with lead rather than in thegroup with the increased intra-abdominal pressure.
3
315316317318319320321322323324325
DISCUSSION
Our knowledge on intra-abdominal hypertension andthe abdominal compartment syndrome has signifi-cantly increased over the past few years. According tothe world society of the abdominal compartment syn-drome, a sustained intra-abdominal pressure over12 mm Hg is defined as intra-abdominal hypertension.Upon this definition was based our decision to inflatethe rubber tube until the IP reached the level of12 mm Hg. Several factors can cause chronically in-creased IP in humans, with obesity being the common-est of them. Especially in BMIs over 40 kg/m2, there isa linear correlation between BMI and IP [2]. The inci-dence of obesity is constantly increasing worldwideand has become an epidemic. The consequences of mor-bid obesity are very well studied and proved [18–23].However, the pattern of pathophysiologic changesthat lead to the clinical consequences of morbid obesityis far from being clarified.
In a recent study, Nagamoto et al. [24] showed thatlife style related diseases have unique mRNA expres-sion patterns and fiber profiles depending on the typeof the disease. More specifically, obese diabetic ratshave only low oxidative type I fibers, whereas ratswith hypertension or hyperlipidemia have both high ox-idative type IIA and type IIC and low oxidative type Ifibers in their skeletal muscles. The proportion of mus-cle fibers, as well as the capillary density in skeletalmuscles is positively correlated with the levels of thecirculating adiponectin, a hormone associated with in-sulin resistance and type II diabetes [25]. These studiesshowed that changes in the muscle fiber profile can re-sult from metabolic abnormalities. In a previous study[9], using the same animal model, we proved thatchronic intra-abdominal hypertension can also causeremodeling in the rectus abdominis muscle. In the pres-ent study, we test the hypothesis that chronic intra-abdominal hypertension can cause oxidative stress tothe rectus abdominis muscle and trigger compensatorymechanisms. Oxidative damage is typically related tothe ischemia–reperfusion syndrome. Intra-abdominalhypertension causes decreased visceral blood flow
Q[28]. Could the hypo-perfusion of the rectus muscle
f � 9 August 2011 � 3:37 pm � ce

Q4
5
6
TABLE 2
Results of the Biochemical Tests
Group A Group B Group C P value*
Lipid peroxidation (pmol TBARS/mL) 4.44 6 0.84 5.73 6 1.89 4.33 6 0.42 0.042Protein carbonyl content (nmol of
carbonyls/mg prutεΐnh2)Q12
8.96 6 1.00 9.97 6 0.98 8.61 6 0.67 0.010
Total glutathione (mmol/mL) 24.35 6 11.58 26.05 6 13.65 27.86 6 15.98 0.735Glutathione peroxidase (U/mL) 0.0552 6 0.0300 0.0773 6 0.0053 0.0821 6 0.0901 0.004Glutathione reductase (U/mL) 6.51 6 2.78 10.42 6 3.75 5.65 6 2.39 0.020Superoxide dismutase (SOD) (U/mL) 13.92 6 7.08 14.40 6 8.20 15.61 6 7.20 0.410Pro-oxidative antioxidative balance 65.05 6 18.16 86.65 6 26.20 74.25 6 12.73 0.029
*Kruskal-Wallis test.
JOURNAL OF SURGICAL RESEARCH: VOL. -, NO. -, - 20114
326327328329330331332333334335336337338339340341342343344345346347348349350351352353354355356357358359360361362363364365366367368369370371372373374375376377378379380
381382383384385386387388389390391392393394395396397398399400401402403404405406407408409410411412413414415416417418419420421422423424425426427428429430431432433434435
also cause oxidative stress to the muscle fibers? If thatis the case, oxidative stress could be one of the missinglinks that could explain several pathologic conditionsassociated with morbid obesity.
In the present study, we measured in rectus abdomi-nismuscle biopsies themarkers of lipid and protein per-oxidation, the concentration and activity of severalantioxidative systems (total glutathione, SOD, gluta-thione reductase, and glutathione peroxidase), as wellas the pro-oxidant–antioxidant balance. The resultsshowed that keeping the IP over 12 mm Hg for 8 wkcan cause increased oxidative damage to both lipidsand proteins with an increased pro-oxidant–antioxi-dant balance. In an attempt to compensate for this dam-age, the muscle fibers increased their glutathionereductase and glutathione peroxidase activity. How-ever, the total glutathione concentration and the SODactivity remained unchanged.
A previous study in rats, with occlusion of the bloodsupply to the rear legs, showed that although the ische-mia caused oxidative damage and increased the proteincarbonyl content, there was no significant change to theSOD activity, probably because ischemia deactivatesthe SOD [26]. This could explain why the SOD activityremained unchanged in our study. But how can in-creased intra-abdominal pressure be associated with is-chemia in the rectus abdominis muscle? A recentexperimental study with in vivo pressure measure-ments in rats has shown that the compartment pres-sure of the rectus sheath (CPRS) reflects theintraabdominal pressure (IAP) under various condi-tions of intra-abdominal hypertension (IAH). Aftera stepwise increase and decrease in IAP with continu-ous measurement of the correspondent CPRS, theyproved that CPRS accurately reflects IAP for IAP of12 mm Hg or higher [27]. In another study, using thecolored microsphere technique to measure blood flowdistribution in the rectus abdominis muscle, the au-thors found that increased IAP causes substantial de-crease in the blood flow of the rectus abdominismuscle. Specifically, an increase in IAP from 0 mm Hg
FLA 5.1.0 DTD � YJSRE10931_proo
to 10 mm Hg leads to a decrease in the arterial bloodflow in the RA muscle (P < 0.01 and P < 0.001, respec-tively) [28]. Thismeans that increased IAP significantlyrestricts the blood flow in rectus abdominis muscle.
In our study, the total glutathione concentration re-mained unchanged. On the contrary, glutathione perox-idase and glutathione reductase activity wassignificantly higher in the group with the increased IP.Glutathione peroxidase activity was also higher in thegroup which was charged with lead, compared withboth the control and the intra-abdominal hypertensiongroup. It is well established that acute muscle exercisecan lead to oxidative stress and increase in the antioxi-dant defense systems [35]. QHowever, in a more chronicbasis, this has never been examined before. It is possiblethat an increase in glutathione peroxidase activity is oneof themain compensativemechanismsagainst the oxida-tive damage. Glutathione is the principal intracellularnon-protein thiol [29] and provides a primary defenseagainstoxidative stressby itsability to scavenge freerad-icals or participate in the reduction ofH2O2. Glutathioneis central to the detoxification of ROS, but in the absenceof an enzyme system to catalyse the many different de-toxification reactions, as well as the ability to catalysethe reduction of oxidized glutathione, this thiol couldnot function as an intracellular antioxidant. Therefore,it seems that the most important element in this antiox-idant system is the ability to quickly regain the reducedglutathione rather than the total glutathione concentra-tion. This is supported by other studies, which haveshown that the total glutathione concentration is not af-fected by several conditions causing oxidative stress tothe muscle fibers [30], whilst cold Qacclimatation caneven cause reduction in the total glutathione concentra-tion [31]. On the contrary, exposure to low temperatures[32], hypoxia [33], high altitude [34], exercise [35], andaging [36] are followed by an increase in glutathione per-oxidase or glutathione reductase activity in skeletalmuscles.
The lipid peroxidation products were significantlyhigher in the group B compared with both the control
f � 9 August 2011 � 3:37 pm � ce

7
8
9
KOTIDIS ET AL.: CHRONIC INTRA-ABDOMINAL HYPERTENSION 5
436437438439440441442443444445446447448449450451452453454455456457458459460461462463464465466467468469470471472473474475476477478479480481482483484485486487488489490
491492493494495496497498499500501502503504505506507508509510511512513514515516517518519520521522523524525526527528529530531532533534535536537538539540541542543544545
group A and group C. This means that intra-abdominalhypertension caused significantly higher oxidativedamage to the fatty acids of the muscle fibers, confirm-ing their increased sensitivity to the oxidative stresscaused by hypoxia [37, 38]. Similarly, protein carbonylcontent, as a biomarker of protein oxidative modifica-tion, was also higher in group B compared with bothgroups A and C. No difference was found betweengroups A and C. Previous studies have shown that ag-ing, alcohol abuse, and congestive heart failure areassociated with increased protein carbonyl content[39–42]. On the other hand, oxidative modification ofenzymes or structural proteins is proved to play a cen-tral role in the etiology or progression of several humandiseases [43]. This underlines the importance of proteincarbonilation as a potential link between intra-abdominal hypertension and obesity related diseases.
Finally, the pro-oxidant–antioxidant balance wassignificantly higher in group B compared with groupA. No difference was found between groups A and Cas well as between groups B and C. The balance valuewas slightly higher in the group of animals that werecharged with lead compared with the control group,but this was not statistically significant. Apparently,both increased intra-abdominal pressure and chargingwith lead triggered an oxidative attack to the musclefibers of the rectus abdominis muscle. This attack waseither at a smaller scale or better compensated in groupC, probably because group B suffered the additional ef-fect of decreased blood flow due to the intra-abdominalhypertension. If we take into account the significantlyhigher glutathione peroxidase activity in group C com-pared with both groups A and B, we may assume thatthe animals charged with lead did compensate betteragainst the oxidative damage.
The generation of reactive oxygen species and thesubsequent oxidative damage is typically related tothe ischemia–reperfusion syndrome. However, recentstudies in both humans [44] and animals [34] haveshown that exposure to hypoxia caused by high altitudecan also lead to the overproduction of ROS and oxida-tive damage. Similarly, the occlusion of the arterialsupply alone caused myopathy with mitochondrial dys-function and oxidative stress to rats [26]. This is proba-bly a result of the readjustment or dysfunction ofvarious metabolic processes, such as the electron trans-port chain of the mitochondria, leading to increasedpremature leakage of electrons to the oxygen molecule[45]. Indeed, our study confirmed that hypoxia alonecan also lead to increased ROS production and cause ox-idative stress to the rectus abdominis muscle. The re-ducing condition caused by the decreased blood flow isprobably the cornerstone of the pathophysiologicchanges leading to oxidative stress. It is well knownthat obesity is associated with increased incidence of
FLA 5.1.0 DTD � YJSRE10931_proo
diabetes as well as gastrointestinal malignancies [46].Could the oxidative stress be one the connection linksbetween IAH and the several pathologic conditions as-sociated with obesity? Further studies are required todefine the exact pathways that link the oxidative dam-age caused by the increased intra-abdominal pressurewith the various obesity related morbidities.
REFERENCES
1. http://www.wsacs.org/consensus_summary.php Q2. Sugerman H, Windsor A, Bessos M, et al. Intra-abdominal pres-
sure, sagittal abdominal diameter and obesity comorbidity. J In-tern Med 1997;241:71.
3. Kron IL, Harman PK, Nolan SP. The measurement of intra-abdominal pressure as a criterion for abdominal re-exploration.Ann Surg 1984;199:28.
4. Sugrue M. Intra-abdominal pressure: Time for clinical practiceguidelines? Intensive Care Med 2002;28:389.
5. Sanchez NC, Tenofsky PL, Dort JM, et al. What is normal intra-abdominal pressure? Am Surg 2001;67:243.
6. Sugrue M. Abdominal compartment syndrome. Curr Opin CritCare 2005;11:333. Review.
7. Moylan JS. ReidMB.Oxidative stress, chronic disease, andmus-cle wasting. Muscle Nerve 2007;35:411. Review.
8. Papavramidis TS, Lazou TP, Cheva A, et al. Chronically in-creased intra-abdominal pressure: Validating a model. ObesSurg 2010;20:900.
9. Kotidis EV, Papavramidis TS, Ioannidis K, et al. The effect ofchronically increased intra-abdominal pressure on rectus ab-dominis muscle histology an experimental study on rabbits.J Surg Res, 2010 Jul 21 Q.
10. Lalatta Costerbosa G, Barazzoni AM, Lucchi ML, et al. Fibersizes and histochemical characteristics of the rectus abdominismuscle of the rabbit under conditions of pregnancy andmechan-ically induced stress. Anat Rec 1988;222:136.
11. Alamdari DH, Paletas K, Pegiou T, et al. A novel assay for theevaluation of the pro-oxidant–antioxidant balance, before andafter antioxidant vitamin administration in type II diabetes pa-tients. Clin Biochem 2007;40:248. Epub 2006 Nov 21 Q.
12. OhkawaH, Ohishi N, Yagi K. Assay for lipid peroxides in animaltissues by thiobarbituric acid reaction. Anal Biochem 1979;95:351.
13. Alamdari DH, Kostidou E, Paletas K, et al. High sensitivityenzyme-linked immunosorbent assay (ELISA) method for mea-suring protein carbonyl in samples with low amounts of protein.Free Radical Biol Med 2005;39:1362.
14. Tatzber F, Griebenow S, Wonisch W, et al. Dual method for thedetermination of peroxidase activity and total peroxides-iodideleads to a significant increase of peroxidase activity in humansera. Anal Biochem 2003;316:147.
15. Teare JP, PunchardNA, Powell JJ, et al. Automated spectropho-tometric method for determining oxidized and reduced glutathi-one in liver. Clin Chem 1993;39:686.
16. Cribb AE, Leeder JS, Spielberg SP. Use of a microplate readerin assay of glutathione reductase using 5,50-dithiobis(2-nitrobenzoic acid). Anal Biochem 1989;183:195.
17. Paglia DE, ValentineWN. Studies on the quantitative and qual-itative characterization of erythrocyte glutathione peroxidase.J Lab Clin Med 1967;70:158.
18. Yokoyama Y, Alterman DM, Sarmadi AH, et al. Hepatic vascu-lar response to elevated intraperitoneal pressure in the rat.J Surg Res 2002;105:86.
19. Wachsberg RH, Sebastiano LLS, Levine CD. Narrowing ofthe upper abdominal inferior vena cava in patients withelevated intra-abdominal pressure. Abdom Imaging 1998;23:99.
f � 9 August 2011 � 3:37 pm � ce

Q10
11
JOURNAL OF SURGICAL RESEARCH: VOL. -, NO. -, - 20116
546547548549550551552553554555556557558559560561562563564565566567568569570571572573574575576577578579580581582583584585586587588589590591592593594595596597598599600
601602603604605606607608609610611612613614615616617618619620621622623624625626627628629630631632633
20. Cardwell CB, Ricotta JJ. Change in visceral blood flow with ele-vated intra-abdominal pressure. J Surg Res 1987;43:14.
21. Bai SW, Kang JY, RhaKH, et al. Relationship of urodynamic pa-rameters and obesity in women with stress urinary inconti-nence. J Reprod Med 2002;47:559.
22. SugermanHJ, FeltonWL 3rd, Sismanis A, et al. Gastric surgeryfor pseudotumor cerebri associated with severe obesity. AnnSurg 1999;229:634.
23. Tsoutsos D, Rodopoulou S, Keramidas E, et al. Early escharot-omy as a measure to reduce intra-abdominal hypertension infull-thickness burns of the thoracic and abdominal area. WorldJ Surg 2003;27:1323.
24. Nagatomo F, Gu N, Fujino H, et al. Skeletal muscle characteris-tics of rats with obesity, diabetes, hypertension, and hyperlipid-emia. J Atheroscler Thromb 2009;16:576. Epub 2009 Sep 18.
25. Ingelsson E, Arnl€ov J, Zethelius B, et al. Associations of serumadiponectin with skeletal muscle morphology and insulin sensi-tivity. J Clin Endocrinol Metab 2009;94:953. Epub 2008 Dec 23.
26. Pipinos II, Swanson SA, Zhu Z, et al. Chronically ischemicmouse skeletalmuscle exhibitsmyopathy in associationwithmi-tochondrial dysfunction and oxidative damage. Am J PhysiolRegul Integr Comp Physiol 2008;295:290.
27. Meier C, Schramm R, Holstein JH, et al. Measurement of com-partment pressure of the rectus sheath during intra-abdominal hypertension in rats. Intensive Care Med 2006;32:1644.
28. YavuzY, RønningK, LyngO, et al. Effect of carbon dioxide pneu-moperitoneum on tissue blood flow in the peritoneum, rectus ab-dominis, and diaphragm muscles. Surg Endosc 2003;17:1632.
29. Hayes JD,McLellan LI. Glutathione and glutathione-dependentenzymes represent a coordinately regulated defense against ox-idative stress. Free Radic Res 1999;31:273.
30. Andrade FH, Anzueto A, Napier W, et al. Effects of selenium de-ficiency on diaphragmatic function after resistive loading. ActaPhysiol Scand 1998;162:141.
31. Hong JH, Kim KJ, Suzuki K, et al. Effect of cold acclimation onantioxidant status in cold acclimated skaters. J Physiol Anthro-pol 2008;27:255.
32. Petrovic V, Buzadzic B, Korac A, et al. Antioxidative defence alter-ations in skeletalmuscle during prolonged acclimation to cold: Roleof L-arginine/NO-producing pathway. J Exp Biol 2008;211:114.
FLA 5.1.0 DTD � YJSRE10931_proo
33. Zembron-Lacny A, Ostapiuk J, Slowinska-Lisowska M, et al.Pro-antioxidant ratio in healthy men exposed to muscle-damaging resistance exercise. J Physiol Biochem 2008;64:27.
34. Singh SN, Vats P, Kumria MM, et al. Effect of high altitude(7620 m) exposure on glutathione and related metabolism inrats. Eur J Appl Physiol 2001;84:233.
35. Venditti P, Di Meo S. Effect of training on antioxidant capacity,tissue damage, and endurance of adult male rats. Int J SportsMed 1997;18:497.
36. Rathore R, Zheng YM, Niu CF, et al. Hypoxia activates NADPHoxidase to increase [ROS](i) and [Ca(2þ)](i) through the mito-chondrial ROS-PKCvarepsilon signaling axis in pulmonary ar-tery smooth muscle cells. Free Radic Biol Med 2008;45:1223.
37. Chen ZH, Saito Y, Yoshida Y, et al. Effect of oxygen concentra-tion on free radical-induced cytotoxicity. Biosci Biotechnol Bio-chem 2008;72:1491.
38. Afnasev IB. Free radical mechanisms of aging processes underphysiological conditions. Biogerontology 2005;6:283.
39. Goto S, Nakamura A, Radak Z, et al. Carbonylated proteins inaging and exercise: Immunoblot approaches mechanisms of age-ing and development 1999;107:245. Q
40. Fernandez-Sola J, Garcia G, Elena M, et al. Muscle antioxidantstatus in chronic alcoholism. Alcohol Clin Exp Res 2002;26:1858.
41. Coirault C, Guellich A, Barbry T, et al. Oxidative stress of myo-sin contributes to skeletal muscle dysfunction in rats withchronic heart failure. Am J Physiol Heart Circ Physiol 2007;292:H1009.
42. Van Hees HWH, van der Heijden HFM, Ottenheijm CAC, et al.Diaphragmatic single-fiber weakness and loss of myosin in con-gestive heart failure rats. Am J Physiol Heart Circ Physiol 2007;293:H819.
43. Dalle-Donne I, Giustarini D, Colombo R, et al. Protein carbonyl-ation in human diseases. Trends Mol Med 2003;9:169. Review.
44. BaileyD,Davies B,DavinsonG, et al. Oxidatively stressed out athigh-altitude!. Intern Soc Mountain Med Newsletter 2000;10:3.
45. Magalh~aes J, Ascens~aoA, Soares JM, et al. Acute and chronic ex-position of mice to severe hypoxia: The role of acclimatizationagainst skeletal muscle oxidative stress. Int J Sports Med2005;26:102.
46. Donohoe CL, PidgeonGP, Lysaght J, et al. Obesity and gastroin-testinal cancer. Br J Surg 2010;97:628. Review.
f � 9 August 2011 � 3:37 pm � ce
634635636637638639640641642643644645646647648649650651652653654655

Our reference: YJSRE 10931 P-authorquery-v9
AUTHOR QUERY FORM
Journal: YJSRE
Article Number: 10931
Please e-mail or fax your responses and any corrections to:
E-mail: [email protected]
Fax: 1-845-883-5682
Dear Author,
Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen
annotation in the PDF file) or compile them in a separate list. To ensure fast publication of your paper please return your
corrections within 48 hours.
For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions.
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in
the proof.
Location
in articleQuery / Remark: Click on the Q link to find the query’s location in text
Please insert your reply or correction at the corresponding line in the proof
Q1 Is this running head OK as set?
Q2 Please provide highest academic degrees for all authors.
Q3 Ref 28 is cited out of numerical order. Please revise.
Q4 OK as changed to peroxidase?
Q5 Ref 35 is cited out of numerical order. Please revise.
Q6 Please confirm “acclimation”.
Q7 Ref 1: Please provide date accessed.
Q8 Ref 9: Please provide volume and page numbers, if available.
Q9 Ref 11: Please provide published date, if available.
Q10 Ref 25: Please provide published date, if available.
Q11 Please provide the series title for the reference 39 if applicable.
Q12 Please clarify prusenh2 in Table 2.
Q13 For figure 1, the resolution is good enough, but the image quality is insufficient. Please provide better
quality figure.
Thank you for your assistance.
Related Documents