Perinatal Mood Disorder California Parenting Institute Santa Rosa, CA Grace Harris, MFT

California Parenting Institute Santa Rosa, CA Grace Harris, MFT.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Perinatal Mood DisorderCalifornia Parenting Institute
Santa Rosa, CA
Grace Harris, MFT

Why?

PMD includes other Mental Health diagnoses:
Depression / Anxiety / OCD / Panic Disorders,Agoraphobia / Bi- Polar Disorder / Psychosis / PTSD
PMD occurs before, during & up to 12 months postpartum.
(Also PMAD – Peri Natal Mood & Anxiety Disorders)
Why “Perinatal Mood Disorder” vs. “Postpartum Depression”?

• Postpartum Depression is highly prevalent• Postpartum Depression is not time-limited• Postpartum Depression is a major risk factor for an
infant’s development• Postpartum Depression IS HIGHLY TREATABLE• Postpartum Depression does not get treated
4
Why is this important?

Prevalence

Data collected from 17 states through the Pregnancy Risk Assessment Monitoring System (PRAMS) revealed that 11-20% of women experienced postpartum depression.
The Agency for Healthcare Research and Quality reports the prevalence for depression during pregnancy as 14-23%.
Prevalence of Depression*
* No data available on Perinatal Mood Disorder

7
Prevalence
Major depression during pregnancy:9 -13 % of U.S. Women
(Gaynes et al. 2005, AHRQ)
Major depression postpartum:7 % of U.S. women in the first 3 months22 % of U.S. women in the first 12 months 10% of fathers develop depression within the first year after the birth of a child
(Gaynes et al. 2005, AHRQ)

Started with small group of pediatricians – voluntary participation (Sonoma County – Santa Rosa facility)
Used PHQ-9 Rate of depression first trial 19% Now screening is routine (pediatrics,
gynecology and other departments) Rate is close to 20%
8
Kaiser Small Test of Change

Major and Minor Depression in Pregnancy ACOG VOL. 113, NO. 6, JUNE 2009

Type Onset Prevalence Symptoms
Prenatal depression
During pregnancy
10 to 20 percent of pregnant mothers
• Crying, weepiness• Sleep problems• Fatigue• Appetite
disturbance• Anhedonia• Anxiety• Poor fetal
attachment• Irritability
Prevalence maternal depression and related symptoms

Type Onset Prevalence Symptoms
Baby Blues Begins during the first few weeks after delivery (usually in first week, peaking at 3-5 days). Symptoms usually resolve by two weeks after pregnancy.
As high as 80 percent of new mothers
• Crying, weepiness• Sadness• Irritability• Exaggerated sense
of empathy• Anxiety• Mood lability (“ups”
and “downs”)• Feeling overwhelmed• Insomnia, trouble
falling or staying asleep; fatigue/exhaustion
• Frustration
Prevalence maternal depression and related symptoms

Type Onset Prevalence
Symptoms
Postpartum depression
Usually within the first two to three months post-partum, though onset can be immediate after delivery (distinguishable from “baby blues” as it lasts beyond two weeks post-partum)
10 to 20 percent of new mothers
• Persistent sadness• Frequent crying, even about little things• Poor concentration• Difficulty remembering things• Feelings of worthlessness, inadequacy or
guilt• Irritability, crankiness• Loss of interest in caring for oneself• Not feeling up to doing everyday tasks• Psychomotor agitation or retardation• Fatigue, loss of energy• Insomnia or hyperinsomnia• Significant decrease or increase in
appetite• Anxiety manifested as bizarre thoughts
and fears, such as obsessive thoughts of harm to the baby
• Feeling overwhelmed• Somatic symptoms (headaches, chest
pains, heart palpitations, numbness and hyperventilation)
• Poor bonding with the baby (no attachments), lack of interest in the baby, family or activities
• Loss of pleasure or interest in doing things one used to enjoy (including sex)
• Recurrent thoughts of death or suicide
Prevalence maternal depression and related symptoms

Gestational Diabetes 4.6%
Hypertension 5%
Prevalence of other high risk conditions routinely screened:

6% with standard care
34% with Edinburgh Postnatal Depression Scale
Detection of ante natal depression without formal screening:

Research at Easton Virginia Medical School 28,000 male and female subjects Women 24 % Men 10.4% (compared to typical rate of
4.8%)
15
Paternal Peri-Natal Depression

Amanda is 24 years old. She has a history substance abuse. Both she and her partner entered treatment when she learned she was pregnant. She has a 3 month old girl. She has a history of bipolar disorder which was previously controlled well with medication. However, she really wants to breast feed her baby and is worried about the medication’s effects so she is not taking it right now.
She is trying hard to be a good mom but is very worried that she “will do the wrong thing.” She is feeling isolated because she can’t talk to old friends who are still using and her partner spends a lot of time going to NA meetings because he seriously is trying to stay clean.
She is willing to talk to a doctor about resuming medication and accepted a referral to a baby gym class. She also put her name on a list to receive subsidized housing so hopes she and her partner can move in 6 months to a year. 16
RISK FACTORS

Maricela is a 29 year old monolingual Latina living with her partner and her 5 year old son from a previous relationship and her new baby girl. Her father recently died in Mexico. She was unable to attend the funeral due to finances.
She reported being depressed after her last delivery and scored 16 on the EPDS which is in the clinical range. She has difficulty sleeping and worries about the baby. Recently she told her partner she had been sexually abused as a child and her mother told her she just had to live with it. There was IPV in her previous relationship.
17
RISK FACTORS

Biological Vulnerability
Psychological Factors
Life Stressors
Risk Factors

Rule out other medical problems – anemia, thyroid deficiency
Hormone fluctuations including stress hormones
Fatigue Prior history of depression
Biology

20
Psychology / Life Stressors

Women who have never been depressed: 10% develop PPD
Women who have been depressed: 25% develop PPD
Women with previous PPD: 50% develop PPD
Biology / Psychology

22

23
24

Mother – Child – Family
Effects

Suffering Lack of joy in child Lack of confidence in parenting
ability Missed work Social withdrawal Somatic symptoms Guilt Suicidality
Mother

Increased anger/conflict with others Increased use of alcohol/drugs – misuse of Rx Isolated from family Feeling discouraged Impulsive – reckless driving, extra-marital
relationship Physical problems – headaches, indigestion Work constantly or worry about performance at work Conflict between how he thinks he should be as a
man and how he actually is27
Father

Marital discord Withdrawal from other family
members Challenging relationship with
other children
Family

PMD affects pregnancy outcomes
↑ preterm birth ↑ low birth weight ↑ miscarriage ↑ preeclampsia
Research suggests maternal depression leads to an alteration in the mother’s neuroendocrine axis and uterine blood flow which may contribute to premature delivery, LBW etc.
Babies of mothers who suffered from depression during pregnancy have elevated cortisol and catecholamine levels at birth. They cry more often and are more difficult to console.
Marcus, S., & Heringhausen, J. (2009). Depression in Childbearing Women: WhenDepression Complicates Pregnancy. National Institute of Health. Primary Care, March 2009.

Wright State University School of Medicine Study Boonshoft School of Medicine 2009 (Kohake, Paton and Heis)
Maternal age and trimester entry into prenatal care not statistically significant relative to infant birth weight.
EPDS score and maternal race was statistically significant relative to EPDS score.
Future studies should quantify if antenatal depression existed with low birth weight infants.
30
PMD & BIRTHWEIGHT

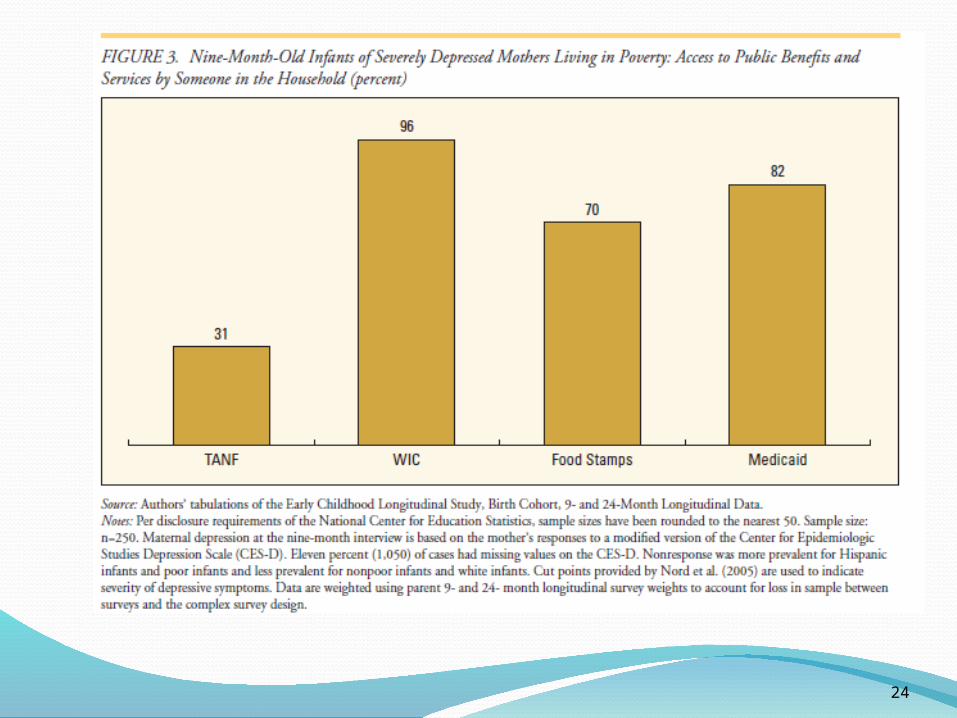
INFANT CARE
Health Care Consequences
- Less frequent HSV- More urgent care/ER- Ineffective Anticipatory
Guidance- Behind on Immunizations

Video

Do babies have mental health?

Relationships are central to infant mental health Social-emotional capacities depend on love and
care Trusting and caring by the primary caregiver is the
foundation for later development. Social development includes ability to form
relationships and knowledge of social rules and standards
Emotional development includes experience of feelings about self and others.
34
Infant Mental Health

Impact of maternal depression on developing child
When compared to non-depressed mothers, depressed mothers demonstrate: *Less affectionate behaviors *Less responsive to infant cues *More flat affect or withdrawal
Infants display more sleep problems which further exacerbates mother’s difficulties
As studies continue - effects on child may extend well into early teen years and have continued repercussions
Paternal depression has shown a strong link to future mental health problems in children

PMD directly impacts the infant’s experience and current studies indicate negative consequences on development
• Social• Emotional• Cognitive• Language • Attention• Mother/Father-Infant Relationship/
Interaction 36
Impact of maternal depression on developing child

Maternal Depression and the Developing Child
“Children who experience maternal depression early in life may suffer lasting effects on their brain architecture and persistent disruptions of their stress response systems”.
Maternal Depression Can Undermine the Development of Young Children (2009). Working paper 8, Center on the Developing Child Harvard University. December 2009.
Studies of children of depressed mothers show patterns of brain activity (in EEG) that is similar to what is found in adults with depression. The patterns are more pervasive with the mother is both depressed and withdrawn from her infant

Screening

to increases diagnostic reliability EPDS increased the detection of PPD from 6.3% to 35.4%
(Evins et.al, 2000)
Why screen universally?
to identify women who would otherwise go undiagnosed - including those with suicidal ideation
In a sample of women 6 wks PP, the diagnosis of PPD increased from 3.7% to 10.7% with routine screening. (Georgiopoulous et. al. 2001)
Why use a validated screening tool?

Among women who were screened and identified as depressed, less than half report that they recognized their depression.
Who Knew?

Every health care provider that interacts with women of childbearing age ….
Mental Health Providers Family Practice OB/Gyn Pediatricians Internists Community Health Workers Others including social service providers
41
Who should screen?

Edinburgh (EPDS) 10 questions – available in Spanish and 20 other languages.
Patient Health Questionnaire (PHQ) 9 questions
Postpartum Depression Screening Scale (PDSS) 35 questions
2-question screen: During the past month, have you often been bothered by
feeling down, depressed, or hopeless? During the past month, have you often been bothered by
little Interest or pleasure in doing things?
Validated Screening Tools

DID YOU KNOW? The American Academy of Obstetrics and Gynecology
recommends the screening of pregnant women for depression at least once per trimester, using a simple
two question screening tool
Two question screen: During the past month, have you often been
bothered by feeling down, depressed or hopeless?
During the past month, have you often been bothered by little interest or pleasure in doing things?

Treatment

Blanca is a 27 year old Latina who following the birth of her fourth child became very anxious and wasn’t able to sit still. She was referred by WIC. She scored 22 on the EPDS with many responses indicating anxiety or worry. She also mentioned thoughts to harm herself, but agreed to contract for safety. Her family is supportive and she says she feels comfortable in her mom’s home.
When the symptoms became too much for her she accepted a referral to the county Psychiatric Emergency Services and received a prescription for an antidepressant. She had been offered medication before, but felt that the doctor hadn’t really listened to her and simply gave medication. She felt that the county doctor paid attention to her before he prescribed so she was willing to try medication. She began to feel better and began to sleep.
She then disclosed that she was having problems with her partner who began seeing another woman when Blanca was pregnant. He also had a problem with alcohol which affected his ability to hold a job. Her family supported her decision to leave him and she is grieving the loss of the 10 year relationship. At the same time she is thinking to a future where she might get some training at the local community college and get a job in the medical field. Blanca has 4 sisters and they spend time with her and her children or invite her to their homes during the day. Her mother read the brochure we gave Blanca about peri-natal depression and she has also become more understanding.
Protective Factors

1. Parental Resilience2. Social Connections3. Knowledge of Parenting & Child Development4. Concrete Support in Times of Need5. Social and Emotional Competence of Children
www.strengtheningfamilies.net46
Support – Increased Protective Factors

*Interpersonal Therapy Cognitive Behavioral Therapy *Couples Therapy
*focus on quality of relationships
47
Counseling

Antidepressants
“The research suggests safest choices for breastfeeding mothers include the SSRI sertialine and the tri-cyclic antidepressant nortiptyline”
www.womenshealth.org
48
Medication

1-800-573-6121 The UIC Perinatal Consultation Service assists health
professionals by answering questions they have concerning screening, assessing and treating women with mental health issues during pregnancy and postpartum.
Detailed information about effects of antidepressant medications during pregnancy and breastfeeding
Perinatal anxiety disorders The impact of perinatal mental health issues on the mother-infant
relationship.
The service is sponsored by a grant from the Illinois Department of Healthcare and Family Services.
HANDOUT ON PERINATAL ANTIDEPRESSANTS
University of Illinois at Chicago (UIC)Perinatal Consultation Service

Effective and works faster than drugs
Severe depression Postpartum psychosis
50
Electroconvulsive Therapy

Light box Alternative medicines/practices Infant massage Increased exercise
51
Alternate Therapies

How long before receiving help? How severe are symptoms? How effective is the treatment?
(Medication/Therapist) What is current life situation? How active in self care and
following treatment?
52
Recovery from PMD

Community Engagement

Public Awareness Stigma Professional Education System Barriers Resources System Linkages
Let’s also think about dads here!
54
Barriers to Treatment

Education Culture – Expectations and Experiences Relationships! Other moms, spouse, parents Time of Onset – immediately post-partum vs.
8 months post-partum Messages from Health Care Professionals
55
Stigma & PMD

56
Stigma

STIGMA CONVERSTION
57
1938 law in Great Britain
Infanticide in first year post-partum
Andrea Yates

Reduce stigma – more acceptance of PMD and possible occurrence over pre and long post-natal period.
Capacity building – more providers paying attention to mood disorders during pregnancy and during 1st year of infancy.
Increase 1:1 and group treatment at community health clinics.
Community Education & Advocacy
To increase awareness and understanding of PMD

Group Activity

In 2002 our county convened a group of community providers involved in the care of children aged 0-5 with a focus on mental health concerns, the Children’s Mental Health Partnership.
A sub committee of this group eventually became the Peri Natal Mental Health Partnership.
Partners include Public Health Nursing, Hospitals, physicians, parenting professionals and both agency and private practice therapists.
60
Our CommunitySonoma County, CA

Mental Health Services Act (CA Prop 63) Prevention and Early Intervention
Home Visits for mothers experiencing PMD –Therapist and/or therapist intern.
Parent Support for parents of children 0-5 (Triple P Level 3 or 4)
Peri Natal Mental Health Partnership
61
CPI Model

62
44 mothers identified with a peri natal mood disorder received home visits. Average number of visits per mother = 6. Some mothers received visits for up to 6 months and other mothers were referred for medication and other counseling services so had less visits.
An additional 33 mothers with other mental health concerns that affected parenting received home visits, assessments and referrals.
We have one 32 hour bilingual supervising licensed therapist on staff for this project. We use interns and trainees when possible in order to see more families.
Common sources of referrals: Public Health Nursing, CPI Parent Educators, WIC, clinic doctors and nurse practitioners, hospital social workers.
Services Provided Year One

Community Education
63

64
65

Policy and Politics
66

Federal Mandate Part of Healthcare Reform Initiative Expand research on Postpartum conditions Expand longitudinal studies of mental health
consequences Allows grants for services to individuals with
a postpartum condition and their families
67
Melanie Blocker StokesMOTHERS ACT

68

69
Click icon to add picture

70

HandoutsUIC Perinatal Antidepressants InformationPerinatal Mental Health Partnership of Sonoma County, CA – Action PlanSample Moms Newsletter
Web Sites are easy to find in Searchwww.postpartumprogress.comwww.postpartumdads.orgwww.postpartum.netwww.helpguide.orgwww.jennyslight.org
71
Resources / Handouts

72
GRACE HARRIS, Parent Resources DirectorCalifornia Parenting [email protected]
CHARLENE BOCCA, Perinatal TherapistCalifornia Parenting [email protected]
KAREN CLEMMER, Perinatal Services CoordinatorCounty of [email protected]
Contact
Related Documents




![[MFT] Toriko 161](https://static.cupdf.com/doc/110x72/568c0d191a28ab955a8b71e1/mft-toriko-161-56e4d6247d1d9.jpg)


![[MFT] HxH 320](https://static.cupdf.com/doc/110x72/568bdf901a28ab2034bd8a04/mft-hxh-320.jpg)



