Calgary Headache Assessment & Management Program (CHAMP) EDUCATION SESSION Welcome to the program!

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Calgary Headache Assessment & Management Program (CHAMP)
EDUCATION SESSION
Welcome to the program!
What is the Purpose of this
Session? To provide you with:
• accurate and current headache information
• the option to ask our staff questions
• a roadmap to CHAMP
• a chance to think about what you want your time in CHAMP to look like and to create a plan
2
What is the Purpose of This Session?
To tell you about CHAMP’s unique structure:
•The majority of your time will be spent completing a lifestyle assessment, attending workshops and lectures, and seeing CHAMP’s nurses/ allied health providers.
•If it’s still required, you will see the CHAMP neurologist for 1-3 visits in approximately 12-18 months from now.
3

Who Is This Session For?
All or most of the information in this session can be used by people with:
-migraine headaches
- tension-type headaches
- post-traumatic (e.g., concussion) headaches
Some of this information can be used by people with:
- cluster headaches
- trigeminal neuralgia/facial pain
- other headache types
4
Session Outline
• Introduction to the program
• Headache Diagnosis
• Medical treatment of headaches
• Behavioral Approaches for headache management
• CHAMP program components and roadmap

Calgary Headache Assessment & Management Program (CHAMP)
• Located at 2 sites:
1) South Health Campus
4448 Front Street S.E. (5th Floor)
Phone (403) 956-3543
2) Richmond Road Diagnostic and Treatment Center
1820 Richmond Road S.W.
Phone (403) 956-3543
6
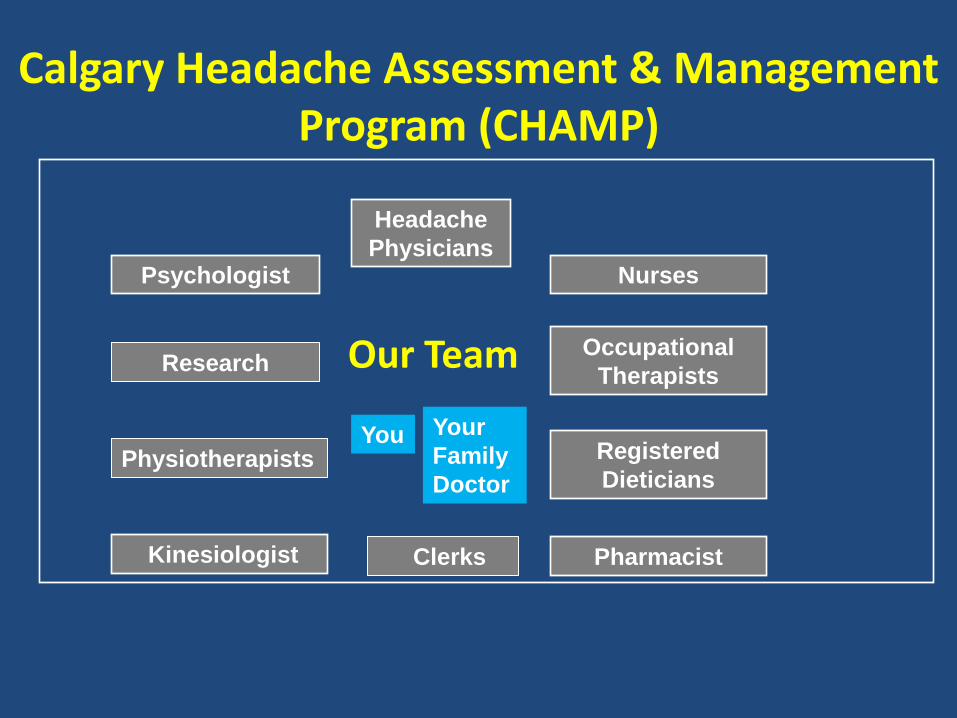
Calgary Headache Assessment & Management Program (CHAMP)
Our Team
Headache
Physicians Nurses Psychologist
Research Occupational
Therapists
Physiotherapists Registered
Dieticians
Kinesiologist Pharmacist
You Your
Family
Doctor
Clerks

A Multi-Faceted Approach
HEADACHE
SELF-MANAGEMENT
Medications
-symptomatic
-preventative Adequate
Hydration
Sleep
Quality
Food Choices
&
Eating Patterns
Stress
Management
Strategies
Trigger
Management
Exercise
Routine
Good Posture
Habits
Pacing
&
Lifestyle
Balance
Self-
Monitoring
(Diaries)
How We Measure Success
• Reduced frequency, intensity, and/or duration of headache
• Improved day-to-day function despite headaches (coping)
• Quality of life improvement/satisfaction
• Sense of control over headaches

10
Headache Days / Month (N = 85)**
*P< 0.001 **CHAMP self management groups, headache days by patient report at baseline
and 3 months post self management.

CHAMP’s Cancellation Policy
11
• If you can’t make it to a booked appointment, workshop, or lecture, please give us 2 days notice. That way someone else can be booked into the spot and you can be rebooked.
• If an appointment is missed without 2 days notice, you may be discharged.

CHAMP’s Cancellation Policy
• If you have to cancel any type of appointment (including groups), please call (403) 956-3543.
• Sometimes it’s not possible to give 2 days notice (e.g., in times of sickness). Please call anyway, and we will discuss the situation together.

Headache: Diagnosis and Use of Medications
Calgary Headache Assessment and Management Program (CHAMP)
13

Medical Section Outline
• How are headaches diagnosed?
• Where does the pain come from?
• Acute medications to relieve headache attacks.
• Preventative medications to reduce headache frequency.
• Medication overuse headache.
14
Headache Diagnosis
The first decision: Are the headaches:
Secondary Headaches?
or
Primary Headaches?

Secondary Headaches: Headaches from an Identifiable Cause
Examples:
1. Head/neck injury
2. Medication Overuse
3. Caffeine withdrawal
4. Alcohol Induced
5. Meningitis
6. Brain tumor
7. Brain Hemorrhage
8. Neuralgias
9. Others

Primary Headache: Headaches with no other Underlying Cause
Examples:
1. Migraine with or without aura
2. Tension-type headache
3. Cluster headache
4. others
Chronic Migraine and Chronic Tension-Type Headache
• Chronic migraine: migraine with headache on more than 14 days a month
• Chronic tension-type headache: tension-type headache on more than 14 days a month.
• Some people may have migraine on some days and tension-type headache on other days

How do we diagnose primary headaches?
• Migraine without aura • At least 5 attacks, 4-72 hrs • 2 of:
– One-sided – Moderate-severe – Throbbing – Worse with routine activity
• 1 of: – Nausea/vomiting – Light and sound sensitivity
• No other cause
• Tension-Type Headache • At least 10 attacks, 30 min-7 days • 2 of:
- Mild-moderate intensity - Bilateral - Tight, non-throbbing, band-like
headache - No worsening with activity • Both of: - No nausea or vomiting - No more than one of light or
sound sensitivity
• No other cause

What is an aura?
• Nervous system symptoms that come on slowly before a migraine and last less than 1 hour
• Occur in 1/3 of migraine patients
– Vision changes
– Numbness/Pins and needles
– Speech problems
– Less commonly, weakness, dizziness
• Resolve completely

What Causes the Pain in a Migraine Attack?

22

Migraine in the population

Migraine Treatment
• Basics – Lifestyle issues
– Specific triggers
• Treatment for individual headache attacks (acute therapy) – Non-medication
– Medications
• Preventing headache attacks
- Preventative medications
- Behavioural strategies

Choosing Acute Migraine Medications
Mild Attacks:
– ASA, Acetaminophen (Tylenol), Ibuprofen (Advil)
Moderate:
– NSAIDS (Ibuprofen, Naproxen, Diclofenac, Others)
Triptans
Severe Attacks:
DHE, Triptans
Treating Acute Migraine Attacks
• Treat early in the attack if you can
• Avoid too frequent use
• NSAIDS and Triptans can be taken together
• Medications that include codeine, oxycodone, or other opioids are not recommended for routine use (e.g., Percocet or Tylenol #1,2,3,4)
26
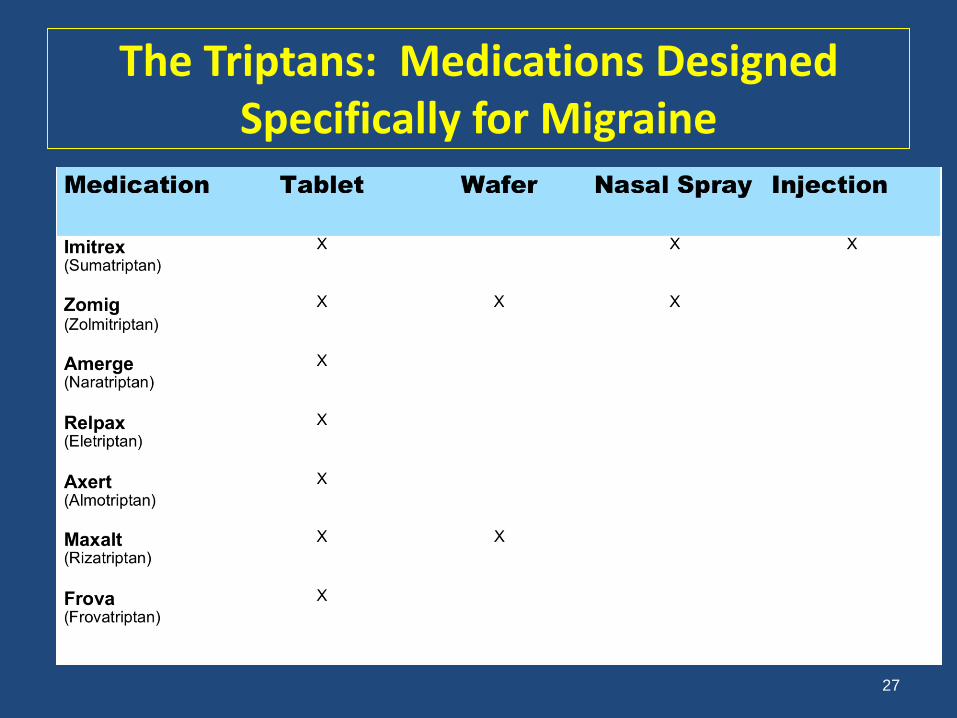
The Triptans: Medications Designed Specifically for Migraine
27

Tension-Type Headaches
• Attacks are often not severe, so not all attacks require medication.
• For individual attacks, NSAIDs (Ibuprofen, Naproxen, etc.) are best.
28

Preventive Medication
• Consider a daily preventive if:
– you have significant disability despite the use of acute treatments.
– you need to use acute medications so frequently that you are at risk for medication-induced headache.
– Preventive medications need to be taken every day

Migraine Preventive Medications
• Certain blood pressure medications (e.g., Propranolol)
• Certain antidepressants (e.g., Amitriptyline)
• Certain anti-seizure medications (e.g., Topiramate)
• Others (e.g., Botulinum toxin A (Botox) for chronic migraines)
• Certain vitamins, minerals, herbs • Riboflavin (400 mg per day)*
• Magnesium citrate (500-1000 mg per day)*
• Coenzyme Q10 (150 mg twice a day)*
*If you’re pregnant or thinking of becoming pregnant, talk to your doctor or ask about our handout.*
30
Preventive Medications for Other Headache Types
Tension-type headache:
• Amitriptyline, Nortriptyline, Venlafaxine
Cluster headache:
• Verapamil, Lithium
Post-traumatic headaches:
• Depends on the headache type 31
Preventive Medication Key Messages
• It may take up to 3 months for a preventive medication to work effectively.
• You may need to be on a high enough dose for the medication to work.
• Taking too much pain medication may limit how well a preventive medication will work.
32

Too much of a good thing: Medication Overuse Headache
Taking too much pain medication can
cause more headaches.

How much is too much?
• Triptans, opioids, DHE, ergotamine (e.g. migranal, imitrex, codeine, demerol, 222s, Tylenol #3)
– 10 or more days/month for more than 3 mo.

How much is too much?
• NSAIDs (ibuprofen, naproxen, diclofenac, etc.), ASA, acetaminophen
– 15 or more days/month for more than 3 mos.
35

36
Example of Medication Overuse
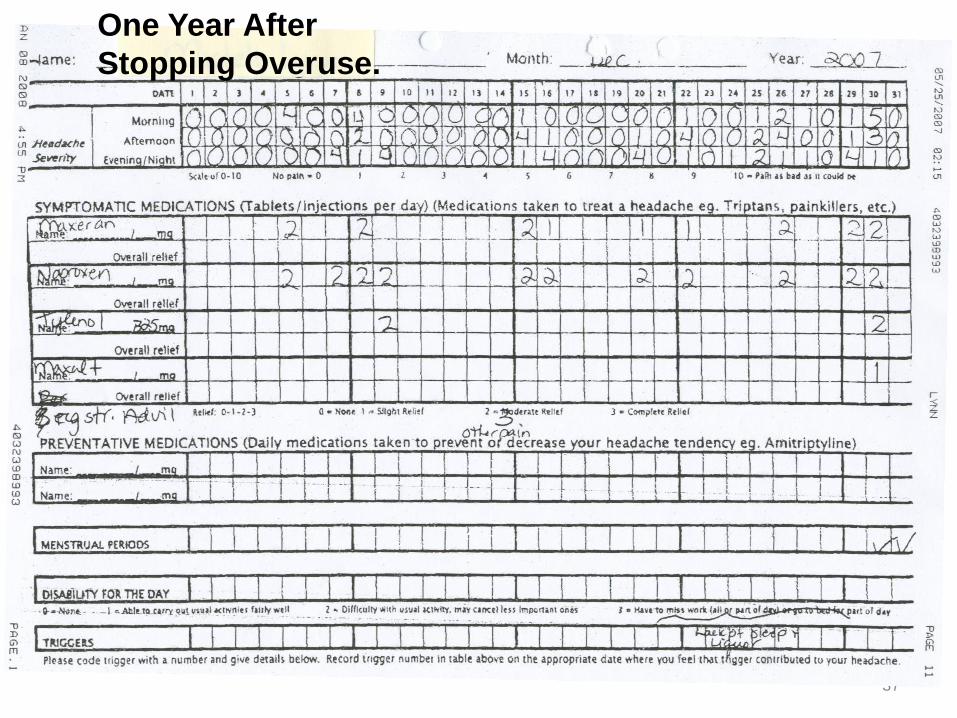
37
One Year After
Stopping Overuse.
Medication Overuse: Case Two – 58 year old male (LGB)
• Migraine since 12 years of age
• Chronic daily headache for at least ten years prior to being seen, associated with daily use of acetaminophen and ibuprofen
• On amitriptyline 25 mg daily
• In October, 2013, he attended the CHAMP education session, and stopped his medication overuse.

• His headaches worsened, but after two weeks they were much improved.
• Headaches reduced to one migraine attack every two months
39

Treating Medication Overuse
• Patient Education
• Stop medication overuse (support available)
• Provide a good acute medication
• Start a preventive medication
40

Key Messages
• Understand your headaches and diagnosis.
• Become skilful in using acute medications.
• Use preventive medications if necessary.
• Avoid medication overuse. Ask about a handout you and your doctor can review.
• Use diaries to monitor headaches and medication use.
• Attend the CHAMP medication lecture.
41
Opportunity To Enter Research Trials
Medication Overuse Study - 3 month study • For chronic migraine sufferers (more than 14 days of
headache per month) • Use pain medications on 15 or more days per month
Migraine and Exercise Study - 6 month study • For migraine sufferers ages 18-58 • Are interested in an exercise program and are not currently
exercising regularly Sleep and Migraine Study – 6 month study • For migraine sufferers age 18+ with sleep problems • Participants will complete an 8-week on-line educational
workshop If interested, please sign up during the break
*30 days of diaries are needed to assess eligibility
*

For more information go to
43

Behavioural Headache Strategies
44
Behavioural Approach in Headache Treatment
“…interventions intended to change the behaviour of a headache sufferer with the goal of reducing symptoms, improving functional status, or improving health related quality of life.”
Penzien et al. 2005

Why Consider Behavioural Strategies?
• The individual prefers a non-drug approach.
• Effective medications cannot be taken or don’t work.
• The patient is pregnant, has plans to become pregnant or is nursing.
• There is excessive use of acute medication.
• High stress levels or limited stress coping skills.

Main Behavioural Strategies
1) Identify and Manage Triggers
2) Lifestyle Adjustments
3) Relaxation
4) Cognitive Behavioural Therapy (Self Talk)
Behavioral Strategy #1: Identify and Manage Triggers
• Become aware of potential triggers
• Determine your personal headache triggers
(Daily headache diary entries can help.)
• Minimize/avoid the triggers you can control
• Develop a coping plan for times when you cannot control triggers (e.g., weather change)

Some Common Triggers (Identified by Patients in “Belief Surveys”)
• *Stress/Let down
• Anxiety/worry and depression
• Overexertion
• Caffeine, alcohol
• MSG, Aspartame, Nitrates
• Odors/fumes
• Weather (e.g., Chinooks)
• Hormones (e.g., menstrual cycle)
• Changes in eating or sleeping habits

Headache Triggers: CHALLENGES
•not everyone has the
same triggers
• the exact way in which
headaches are triggered is
still not known for sure
•most triggers work in
combination, and it can be
hard to tease out which
ones are involved.
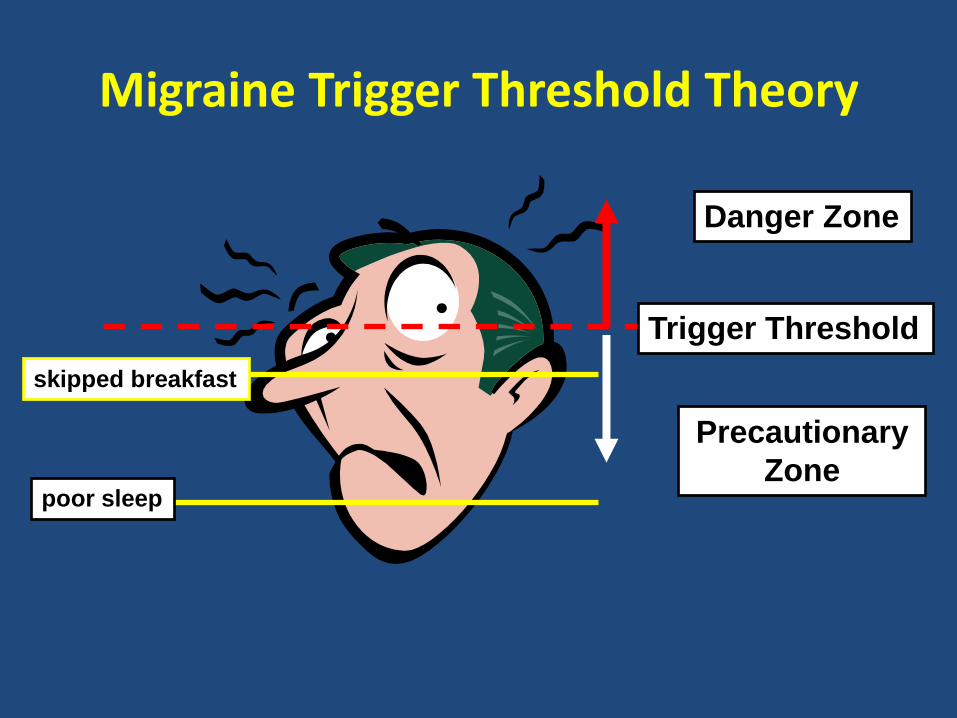
Migraine Trigger Threshold Theory
Trigger Threshold
Danger Zone
Precautionary
Zone poor sleep
skipped breakfast
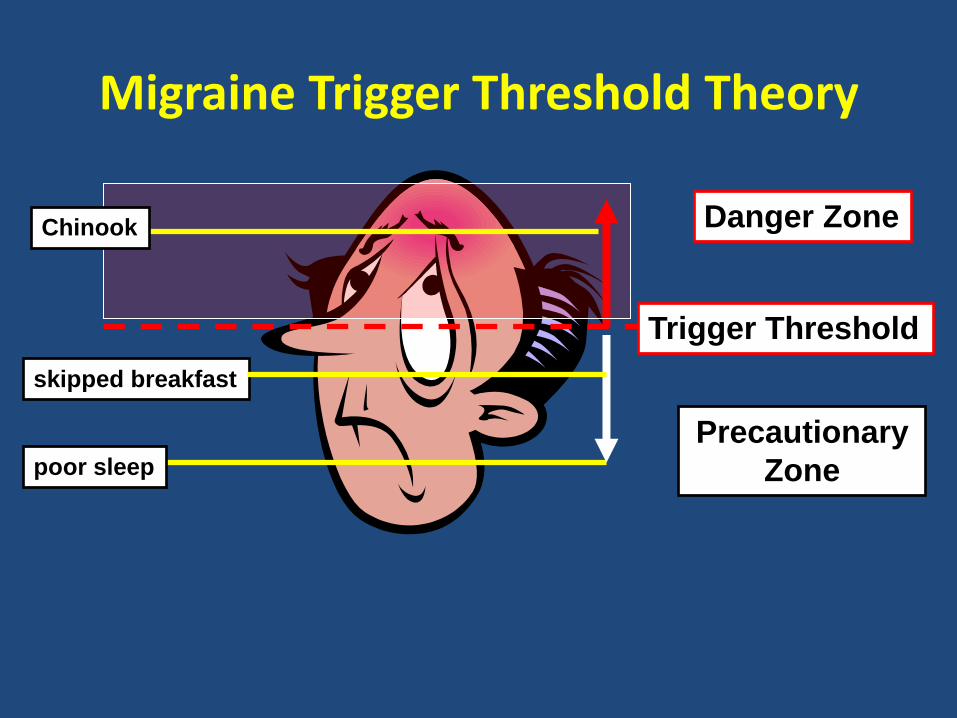
Migraine Trigger Threshold Theory
skipped breakfast
Trigger Threshold
Danger Zone
Precautionary
Zone poor sleep
Chinook
Examples from Research Showing How Triggers Add Up
• Headache was more likely to follow two consecutive days of poor sleep and high stress than either poor sleep or high stress alone.
• Stress on its own didn’t impact migraine, but it did during the premenstrual phase.
53

Migraine Trigger Threshold Theory
The objective of headache trigger management is to keep your trigger level below your threshold.
Reduce your trigger load
(minimize/avoid exposure)
Raise your threshold
(regular aerobic exercise, preventive medication)

Behavioural Strategy #2: Lifestyle Adjustments
This involves adjustments in the areas of:
• hydration and nutrition
• caffeine intake
• sleep routine and habits
• exercise and posture
• stress management

Lifestyle Adjustments
• eat at regular intervals (every 3-4 hours)
• avoid foods high in simple carbohydrates (sugars), especially eaten alone
• drink 2-2.5 litres of fluid per day
• limit caffeine to no more than 100* mg per day; consider reducing it to 2 times/week or stopping it completely.
* (e.g., ~ 8-oz. cup of brewed coffee, 2 cups of black tea, 3 cups of green tea, 1 energy drink).

Lifestyle Adjustments
• Maintain a consistent sleep-wake schedule daily
• make regular physical activity part of your routine
• learn about stretching and strengthening exercises to support good postural habits
• practice a relaxation strategy daily (e.g. diaphragmatic breathing, meditation)

Modifiable Risk Factors Associated with Developing Chronic Daily Headache
• Medication overuse
• Obesity
• Poor sleep
• Caffeine intake > 100 mg/day
• Habitual (daily) snoring
• Stressful life events (e.g., moves, deaths, marital status changes, other highly stressful events)
58
Headache Behavioural Strategy #3: Relaxation
•Relaxation can be used to help prevent headaches or
stop headaches in their early stages.
•Relaxation practice can:
•counteract the stress response
•manage negative emotions,
•enhance sleep
•help manage pain.
Relaxation Research
• Regular use of relaxation techniques is associated with less frequent and less intense headaches for most individuals with migraine and tension headaches.
– Progressive Muscle Relaxation
– Diaphragmatic Breathing
– Visualization/Imagery
– Meditation
The Physical Stress Response
• When someone perceives they are under stress, their body reacts with the stress response (fight or flight):
-Increased heart rate -Release of hormones (Adrenalin) -Shallow breathing -Muscle Tension
• The stress response can be a trigger for headaches.
Relaxation Resources
• Free relaxation tracks
https://myhealth.alberta.ca/alberta/Pages/Relaxation-Audio-Tracks.aspx
www.dawnbuse.com/relaxation.htm
• Relaxation Workshop
• Self-Management Workshop
• Apps (e.g., Stop, Breathe & Think)
62

Behavioural Strategy #4: Cognitive Behavioural Therapy (Self Talk)
Negative/Unhelpful thoughts and behaviour can generate stress and stress-related headaches
A coping style of self-talk can help reduce stress and negative emotions
The person is less vulnerable to stress-related headache

CHAMP Behavioural Programs
• Lifestyle Assessment – individual appointment
• Workshops/Lectures – small group format
Dates, times, locations on schedule
Call (403) 956-3543 to register.
64
Lifestyle Assessments
• Focuses on key health domains (sleep habits, hydration/nutrition, exercise and posture, and stress)
• Guidance given for lifestyle adjustments in these domains that can improve headache management
• Identify/clarify your goals for headache management
• Identify program workshops that may help you work towards your goals
Self Management Workshop • An opportunity to learn and practice coping skills for
headache management, including: – Relaxation techniques – Stress Management – Pacing – Self-talk strategies
• A supportive group environment
• Increase your confidence in your ability to have control over your headaches
Bodyworks Workshop
Postural Awareness and Adjustments
Stretching and Strengthening Exercises
Relaxation Workshop
• Focus is primarily on relaxation skills; stress management is also addressed
• An 8-week self-study format:
- 3 clinic sessions,
- 2 phone contacts
- self-study at home

Web-Based Sleep Workshop
• Ongoing enrollment
• 8 parts
• Designed for people with headaches and sleep problems
• An alternative to traditional workshops
69

Nutrition and Headache Lecture
• Addresses what a healthy diet means for people with headaches.
• Examines potential dietary triggers for headache and associated management strategies.
70
Medication Lecture
• Learn about medications used to prevent headaches.
• Learn about medications used to treat headaches.
• Learn about medication overuse headache.
71
Ergonomics Lecture
• An introduction to possible ergonomic risk factors in headache and strategies to address them.
• Job modification ideas
• General “work survival” strategies

CHAMP Client “Lori”
• Age 28
• Referral letter: Chronic migraines + ?MOH
• Maxalt, Naproxen, Tylenol #3
• Known triggers: posture, delayed meals, poor sleep, menstruation
73

CHAMP Client “Lori”
• Education Session: May 2014
• Lifestyle Assessment: June 2014 Plan (as identified by Lori):
(1) Posture – Body Works, Ergonomics, 1:1 kinesiology if required
(2) Nutrition – Nutrition Lecture, Increase hydration, more frequent meals/snacks
(3) Stress Management – Self Management Workshop
(4) Meds/Supplements/MOH – Medication Lecture; start
recording painkiller use in diaries to establish frequency
(5) Miscellaneous Self-Management – Attend Sleep Lecture, Relaxation Workshop, and continue recording in diary.
74

CHAMP Client “Lori” - Timeline June 2014 26 headache days/month (intensity 1-10/10)
Medication/Ergonomics lectures, Body Works
July-Aug 2014 Sleep/Nutrition lectures, Self Mgmt. Workshop
Sept.-Nov 2014 Relaxation Workshop
Oct. 2014- Kinesiologist appointments (additional stretches/core exercises/body mechanics)
April 2015- CHAMP MD Appointment ( Elavil, Propranolol)
Dec. 2015 Discharged from program
10 headache days/month; (intensity 1-5/10)
75
What’s Next?
• Participate in a Lifestyle Assessment
• Enroll in CHAMP Workshops and Lectures
• Participate in a CHAMP Clinical Trial (study)
CHAMP Website
www.ahs.ca/3672.asp
• Workshop schedules
• Blank headache diaries
• Useful information
77
Related Documents