CALD Research to assist with development of draft Strategic Plan DiverseWerks This paper was prepared for the Mental Health Commission of NSW to support the development of the Strategic Plan for Mental Health in NSW 2014 – 2024 October 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CALD Research to assist with development of draft Strategic Plan DiverseWerks This paper was prepared for the Mental Health Commission of NSW to support the development of the Strategic Plan for Mental Health in NSW 2014 – 2024
October 2014

Mental Health Commission of NSW
CALD Research to Assist with Development of Draft Strategic Plan
Final report January 2014
Level 1, 93 Norton Street
Leichhardt NSW 2046 Tel: 02 8585 1313
Fax: 02 8585 1325
ABN: 30 065 353 951

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Contents
Introduction .............................................................................................................................................. 3
Stakeholder forums .................................................................................................................................. 6
Case studies ............................................................................................................................................ 18
Data analysis .......................................................................................................................................... 23
Key insights to inform Draft Strategic Plan ............................................................................................. 42
Appendix 1 – Invitation to forums ........................................................................................................... 45
Appendix 2 – Forum discussion questions ............................................................................................... 47
Appendix 3 – References ......................................................................................................................... 50

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
1. Introduction 1.1 Background and objectives of the research
The Mental Health Commission of NSW (‘the Commission’) is currently compiling its Draft Strategic Plan for
mental health in NSW. To ensure that this plan is inclusive, the Commission is keen to include culturally and
linguistically diverse (CALD) input in the development of the plan. This is to augment the Commission’s own
progress in the CALD area, which to date has included conducting a CALD leadership forum in late November
2013 to capture some of the views and experiences that key stakeholders have with regards to CALD mental
health.
DiverseWerks were contracted to provide this CALD input on behalf of the Commission. This involved helping
ensure that there were no gaps in knowledge from a CALD perspective in the development of the Draft
Strategic Plan. Further, DiverseWerks were commissioned to provide insight into what some of the issues
around mental health might be across a range of CALD groups in NSW.
Specifically, DiverseWerks looked at the following areas with a view to understanding any impacts they may
have on the current framework being put forward by the Commission in the development of the Draft
Strategic Plan. It was particularly important to align the consultative approach for CALD communities to the
more general mainstream consultations. As such, the Life Stages Model and the broad set of considerations
applied in the mainstream consultations were used to frame the CALD discussion groups. The areas
considered were as follows:
• The nature of cultural and linguistic diversity within NSW;
• The mental health needs within CALD communities;
• A sense of what the mental health system in NSW looks like within CALD communities;
• What activities, strategies, issues and examples of good practice exist in CALD communities with
regards to mental health and wellbeing;
• The nature of broad mental health service access in NSW from a CALD perspective;
• What key actions are required to help meet the mental health and wellbeing needs of the CALD
population in NSW.
1.2 Methodology
There were three components to this research:
A) Data analysis
This involved scoping a range of data sources to understand where the Commission may expect there to be
demand for mental health and wellbeing services from a CALD perspective, and what the broad nature of this
demand might be. Data used for this analysis included the ABS’ 2011 Census data, recent arrivals data from
© DIVERSEWERKS 3

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
the Department of Immigration and Border Protection as well as independent academic research conducted in
this area.
B) CALD community forums
DiverseWerks also conducted two CALD community forums to understand some of the issues and priorities
within the mental health system for CALD populations in NSW. These ‘grassroots’ forums were comprised of
stakeholders working with CALD communities either specifically in mental health, or in a role where there was
some understanding of CALD mental health needs and issues. CALD consumers and carers were also invited
to these forums.
The first forum was conducted in Campsie on 10 December 2013, while the second was held in Wollongong on
16 December 2013, to provide a less Sydney-centric perspective on these issues. Each forum was
approximately 90 minutes long and facilitated by DiverseWerks. The following table provides a list of all of the
organisations who were represented in each forum. It is worth noting that some organisations were
represented by several staff working in the CALD area. Finally, at least one CALD carer and / or consumer
attended each forum:
Organisations involved in CALD community forums
Forum 1 - Campsie
Forum 2 - Wollongong
Macarthur Diversity Services Initiative South Coast Portuguese Association
Settlement Services international Department of Education and Communities
CoAsIt Partners in Culturally Appropriate Care NSW & ACT)
Transcultural Mental Health Centre of NSW Illawarra Multicultural Services
Multicultural Health Services, Marrickville Illawarra Shoalhaven Local Health District
NSW Refugee Health Service Wollongong City Council
Lebanese Muslim Service Multicultural Communities Council of Illawarra
Metro Migrant Resource Centre (Campsie) Illawarra Multicultural Forum
South Eastern Sydney Local Health District Macedonian Welfare Association
Wesley Mission Serbian Welfare Association
Afford Employment
Polish Australian Welfare Organisation
Ethnic Communities Council of NSW
Australian Foundation for Disability
Total number of participants = 27 Total number of participants = 18
The invitation given to forum participants are attached in Appendix 1, and the questions asked of participants
are attached in Appendix 2 of this report.
© DIVERSEWERKS 4

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
C) Case studies
The third component of this research involved developing two CALD case studies which demonstrate how
mental health and wellbeing issues are managed by CALD consumers. Stakeholders participating in the CALD
forums were able to identify two consumers who agreed to be interviewed for these case studies. As a result,
DiverseWerks have developed two CALD case studies as follows:
• An Italian-speaking woman aged in her 70s, living in Leichhardt;
• A Dari-speaking woman aged in her 40s, living in the Parramatta area.
This report combines the findings of the CALD data analysis, the output from the CALD stakeholder forums
and provides two case studies from CALD communities which the Draft Strategic Plan may draw upon. The
key insights that help inform the Draft Strategic Plan, based on this research, are discussed in more detail in
the final section of this report.
© DIVERSEWERKS 5

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
2. Stakeholder forums 2.1 Response to the NSW Mental Health Strategy
model
Participants in the Campsie and Wollongong forums were presented with a copy of the Commission’s Life
Course Map (see Appendix 2) and asked to comment on the relevance of the Life Stages and Journeys to
CALD communities. Feedback given by forum participants is summarised below.
2.1.1 Response to Life Stages
The most significant response to the Life Stages in the Life Course Map was that they assumed a level of
linearity which may lack relevance for CALD communities:
“For migrant people, it’s not like this. We come in different stages … some people come with
qualifications, some come as a refugee” (Campsie stakeholder);
“It doesn’t acknowledge different migration and settlement issues that may emerge … or the
diversity within communities too” (Campsie stakeholder).
The ‘child 5-12 years’ phase, for example, may lack salience for recently arrived CALD children who are busy
trying to act as ‘small adults’ on behalf of their parents by helping them navigate language barriers for
instance. The child may also have spent time in a refugee camp or in a traumatic environment where the focus
was on surviving or having enough food to eat, rather than ‘being a child’.
Similarly, in terms of the older Life Stages there was some sense in both forums that issues which are of
importance in one’s life as an adolescent (13-25 years) or adult (18-65 years) are different for people from
CALD backgrounds, particularly those recently arrived. Individuals in the adolescent phase in the mainstream
may be focussed on establishing a career and romantic relationships, for instance. However for a recently
arrived refugee, having no English language skills at this stage in their lives ensures that the range of issues
relevant to them are completely different. As one participant in the Campsie forum noted, for some adult
refugees arriving in Australia ‘adulthood’ may be a stage where they experience a complete loss of their
former role, particularly if they were highly educated in their country of origin – “They have to go through a
lengthy process (to have their qualifications recognised), and it could be costly too, to develop highly skilled
English … they go back to being junior (here) compared to being well-qualified back home”.
The older adults (65+ years) life stage was another which was felt to be potentially different for CALD
communities compared to the mainstream. Several stakeholders in the Campsie forum felt that within well-
established migrant communities, this was a period where older people were vulnerable to developing mental
health issues – “…for older people, you’ve got a huge number of older migrants who have a dual diagnosis with
(possibly) dementia and a mental illness”. In some cases, this may be because stressors related to one’s
migration were never entirely dealt with (an issue also mentioned in the Wollongong forum) or they can be
exacerbated due to the isolation that can affect older migrants with poor English, for instance. One
© DIVERSEWERKS 6

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
stakeholder in the Campsie forum commented a focus on positive mental health for migrants upon arrival was
one way of ensuring older adults in CALD communities are more resilient to the challenges of older age -
“…there are stressors that go with migration and we need to acknowledge this to try and avoid mental health
issues in the future. If we don’t look after families and individuals who are migrating, we have to suffer
consequences of that later”.
Participants in both forums felt that across the life stages shown a ‘drop in’ stage for migration was required.
This would help acknowledge the stressors involved in migrating to Australia, and the affect that these could
have on a given life stage and one’s mental health and wellbeing in that life stage.
2.1.2 Response to Journeys
As per the feedback on the life stages presented, there was feeling from some stakeholders that the fluidity of
the journeys, and their seemingly linear progression through life lacked relevance for CALD communities.
Rather, the salience of each journey for CALD communities was contingent on when migration occurred,
under what circumstances and what supports were / are available to migrants after settlement.
Therefore a number of stakeholders commented that across the series of journeys put forward a specific
‘migration journey’ needed to be added to the model in order to be more inclusive of culturally and
linguistically diverse experiences. This would acknowledge the range of issues affecting CALD migrants (e.g.
issues around torture and trauma in country of origin, isolation, learning English, finding appropriate housing,
finding employment etc.) which could challenge their mental health and wellbeing, for instance.
A few participants in the Wollongong forum felt that the journeys assume that migrants come here in
reasonably positive circumstances, which may not be the case for some, particularly asylum seekers. Clearly
arriving in Australia as an asylum seeker has the potential to have a large impact on mental health and
wellbeing, an experience the model currently does not allow for - “…there are thousands of asylum seekers
living in Sydney and Wollongong and this model doesn’t acknowledge them – the mandatory detention and
asylum seeker pathway is its own journey … they’re highly traumatised people, they’re escaping and they’re being
detained here” (Wollongong stakeholder).
Specific examples given by stakeholders for how the journeys may lack relevance for CALD communities, or
how they may be manifested somewhat differently, are given below:
• Building community resilience and wellbeing – Several stakeholders felt the notion of a ‘resilient’
CALD community was of particular importance and was felt to be related to a community’s ability to
settle successfully. There was some suggestion that to increase the relevance of this journey for
CALD communities, a sub-journey around the ‘success of settlement’ should be included due to its
perceived closeness to mental health and wellbeing;
• The best start – The ‘start’ which children of skilled migrants have can be quite different compared to
children in the mainstream. In some cultures (e.g. Chinese) it is not uncommon for young children to
be sent back to their country of origin to be cared for by grandparents while their parents are working
© DIVERSEWERKS 7

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
in Australia. This can lead to difficulty in how these children transition to life in Australia - Some are as
young as two … they don’t know who they are when they come here” (Campsie stakeholder);
• Troubled kids – While the journey itself was believed to be experienced quite differently for many
young people of CALD backgrounds, this journey was nevertheless seen as a relatively important one.
A number of stakeholders described the parent-child dynamic in CALD communities as being quite
different as a result of migration. In Wollongong, one stakeholder spoke of the struggle some African
parents experienced in trying to ‘control’ their children by using physical discipline techniques
culturally acceptable in their country of origin, but less so in Australia. Children from African
communities were often keen for greater independence while their parents were reluctant to
encourage this - “It can be hard for (second-generation) kids to know where they fit in”;
• Troubled kids – Another consideration for CALD young people in this journey was the potential for
cultural identity issues. Cultural identity was felt by some stakeholders to be integral to navigating
ones’ childhood, adolescence and even adulthood - “Being a member of the second generation, in the
back of my mind, I’m always thinking ‘how are my parents going to respond? How is my community
going to respond? Culturally, is it appropriate?’ Yes, I am educated and I can do what I want … but you’re
always thinking ‘how is this (behaviour) going to be perceived, is it acceptable?’”
• Towards a better life / Body and soul – Within these journeys, a few stakeholders in the Wollongong
forum felt that there was a sub-journey for some migrants which centred around the ‘pressure to
succeed’. As the ultimate goal for many in migrating to Australia is to ‘build a better life’ for oneself
and one’s family, these stakeholders commented that this could lead to extra pressure on individuals
to ‘do well’, which could impact on one’s mental health and wellbeing;
• Healthy transitions – A stakeholder in Wollongong noted that for some refugees who have
experienced trauma, experiencing panic attacks post arrival could “throw the notion of ‘healthy
transitions’ out the window”,
• Breaking the cycle – It may be difficult for individuals of CALD backgrounds to ‘break the cycle’. For
instance, an Iranian migrant with mental health issues who is hospitalised may have no
accommodation or support to turn to once sent ‘home’ from hospital (an example mentioned in the
Campsie forum);
• Living long and strong - In more established migrant communities (e.g. Italian, Greek) the process of
migration itself and ‘making a life’ can be such a significant undertaking throughout one’s life that
mental health issues that may emerge are not recognised. As a result, these may manifest later in life
around the ‘Living long and strong’ journey. As one stakeholder noted, “For our (Italian) community,
this is when our mental health issues are often commencing. … we’ve found people probably repressed
their mental health issues as they were too busy doing what you have to do to get by” (Campsie
stakeholder).
© DIVERSEWERKS 8

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
A few stakeholders had concerns about the journeys in terms of where carers from CALD backgrounds could
fit. There was some feeling that the role of carers in CALD communities was quite significant, particularly due
to the perception that the public health system was underfunded.
Further to this, there was some criticism in the Wollongong forum about the journeys existing in a context
where it was assumed the mental health system was currently well funded and equipped to deal with the
range of mental health issues affecting the community at large. In Wollongong, a number of stakeholders
criticised local service providers for working in silos instead of collaborating with each other, resulting in
“invisible barriers between multicultural mental health issues and the rest of the sector”.
2.2 Mental health risk factors for CALD communities
A range of factors were mentioned by forum participants which they felt put CALD communities at risk of
developing mental health issues.
2.2.1 Migration
The most significant risk factor mentioned by participants was the act of migration itself. The circumstances
around an individual’s migration to Australia could be particularly traumatic and have considerable impact on
an individual’s capacity to cope in the future. Migrants may have arrived as an asylum seeker, as an
unaccompanied minor, from a refugee camp or a country experiencing conflict, for instance. For example, a
stakeholder in the Campsie forum felt that women on 204 visas (i.e. a visa for ‘women at risk’) were
particularly vulnerable to experiencing poor mental health – “We’re seeing a lot of depression in 204 visa
holders”.
The major adjustment involved in living in a new culture was also seen as potentially traumatic for migrants.
As one stakeholder in Wollongong noted “…adjustment to a new culture is a type of trauma”. As a result,
members of newly arrived CALD communities were felt to be particularly vulnerable to mental distress and
this was certainly reinforced by the types of CALD clients some stakeholders were working with:
“We’re seeing some sort of post-traumatic stress in newly arrived communities … if you’ve
combined the challenges of communities settling in a new country combined with what
they’ve experienced in their country of origin, it does make sense (that mental health issues
would arise)” (Campsie stakeholder);
“I see a lot of psychological distress (in my clients)” (Campsie stakeholder).
This vulnerability to developing mental health issues as a result of migration could be exacerbated by a range
of issues. Those mentioned by stakeholders included:
• Not having one’s qualifications recognised in Australia;
• The stress and pressure individuals / families placed on themselves to be a ‘successful’ migrant;
• A lack of awareness of mental health issues generally, as well as poor awareness of where to get help
– “I see less opportunity for Afghans to go and ask for help in this area” (Campsie stakeholder).
© DIVERSEWERKS 9

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
2.2.2 Arriving as an asylum seeker
It is worth noting that in each forum, several stakeholders felt that asylum seekers were among those at most
risk of developing mental health issues. This was related not only to the traumatic way in which they may have
arrived to Australia, but also due to possibly having spent time in mandatory detention - “…there are
thousands of asylum seekers in Sydney and Wollongong … at risk of self-harm issues, we’ve got kids who’ve been
locked up (in mandatory detention) who’ve developed incontinence issues, depression … they’re highly
traumatised” (Wollongong stakeholder).
One stakeholder felt that the discourse around asylum seekers, in the media and in the wider community, may
also place this category of CALD migrants at risk of mental health and wellbeing issues. There was the belief
that asylum seekers had been demonised in some sections of the media and society, making asylum seekers
feel potentially unsupported or unwelcome - “…it ranges from the headline to the newspaper, to how they’re
spoken about - such as being referred to as ‘illegal’ - right through to the attitudes of the people caring for them”
(Campsie stakeholder).
2.2.3 Stigma and taboo
Stakeholders felt there was considerable stigma and taboo associated with having a mental health issue in a
range of CALD communities. This was not only within recently-arrived communities, but also within more
established CALD communities (e.g. Greek, Italian, Russian):
“…schizophrenia … means you should hide your children … in the five years while my daughter
was being diagnosed (with schizophrenia), in my culture I felt isolated … so many people (in
the Greek community) are uneducated about mental health” (Campsie stakeholder and
carer);
“People (in the Russian community) are afraid to seek support … so they struggle with the
(mental health) issues themselves, afraid there’ll be a stigma on their family” (Wollongong
stakeholder).
Within recently-arrived communities, the stigma around issues such as suicide, for instance, could be so
significant that they are not even acknowledged by these communities in their country of origin and therefore
in these countries are not seen to exist. A Greek stakeholder and carer working around the Campsie area also
spoke of her difficulty in speaking to other members of her community about schizophrenia because of the
general lack of openness to talking about mental health issues, particularly when the level of knowledge
among her community was poor.
The stigma and taboo that exists in many CALD communities was believed to be a major risk factor to talking
about mental health issues in these communities, recognising issues when they arose or in fact seeking help if
it was required. As a result, a number of stakeholders felt there was the potential for people of CALD
backgrounds with mental health issues to ‘fall between the cracks’. Stakeholders related this stigma or lack of
openness to talking about mental health in CALD communities to poor education or general misinformation
within CALD communities about mental health issues.
© DIVERSEWERKS 10

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
2.2.4 General isolation
The isolation that could be experienced by migrants was felt to be another mental health risk factor for CALD
communities. Smaller, more recently-arrived communities were believed to be particularly at risk, as there
was often a lack of existing community infrastructure from which emotional support could be sought. One
stakeholder working with recently-arrived young people in the Wollongong area spoke about how it could be
difficult for Afghan youth to feel a part of the local community, or feel that they had someone to talk to, as
there were few culturally appropriate services available to them - “…lots of Afghan kids in Wollongong don’t
have dads and some youth don’t have culturally appropriate Islamic services available. If you don’t connect to
(existing) church or sporting groups, you’re so isolated”.
Isolation as a risk factor was not only an issue for these types of CALD communities. Stakeholders across both
forums also felt that women across a range of CALD communities were at risk, as they were often more likely
to be at home raising children or running the household and not in any form of paid work. Older people from
CALD backgrounds were also mentioned as potentially at risk of isolation, due to possible mobility issues, the
fact that they were less likely to work as well as the likelihood that they may be widows.
One stakeholder in Wollongong also noted that for CALD communities, exacerbating this issue of isolation
was that it may be difficult to connect with people from one’s own culture as “they may be more traumatised
than you. So you stay away from them”.
2.2.5 Assumption that established CALD communities are more resilient
vs. recent arrivals
Some stakeholders in each forum commented that older, more established CALD communities (e.g. Greek,
Italian, Polish, Russian) were often assumed to be more resilient to developing mental health issues when
compared to those more recently-arrived. This view was dismissed by a number of stakeholders and there was
some feeling that the mental health needs of well-established CALD communities were nevertheless still
important to consider – “…post traumatic stress disorder can come out in your later years” (Wollongong
stakeholder).
As one stakeholder in Wollongong noted, “…there’s a feeling that they (well-established CALD communities)
migrated so long ago, they should speak English by now, and they can access a mainstream service”. Health
services in contact with members of well-established CALD communities may be less likely to focus on the
mental health needs of individuals from these communities as it is assumed that these individuals are well-
connected, have adequate support / a network around them or indeed are aware of where to go if they need
help.
The other issue mentioned by stakeholders that placed well-established CALD communities at risk was the
fact that within many CALD families, parents often spent considerable time and energy helping their children
cope with settlement and life in Australia, that one’s own mental health could be seen as a low priority. One
stakeholder in the Campsie forum spoke of working with a Greek man in his 70s who had spent the majority of
his life as a carer to a son with paranoid schizophrenia. This meant that the mental health issues experienced
by this man himself were not even considered.
© DIVERSEWERKS 11

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
2.2.6 Other risk factors
Other factors which forum participants identified as putting CALD communities at risk of developing mental
health issues included:
• Poor general physical health within some CALD communities, often as a result of poorer levels of
education and literacy – “They have higher rates of smoking or chronic conditions … they can make
people feel older before they actually are” (Wollongong stakeholder);
• A perceived tendency for the physical health of CALD communities to be prioritised instead of mental
health;
• The belief that the mental health system was under-resourced and only had a limited capacity to
work with CALD communities.
2.3 Supporting factors contributing to resilience & recovery
Several factors were thought to be important to CALD communities in terms of their resilience to challenges
to their mental health or indeed their potential to recover when mental health issues arise:
• ‘Successful’ migration - Migrating to Australia ‘successfully’ was seen by some stakeholders as key to
being resilient. The definition of whether migration was viewed to be ‘successful’ was felt to be
contingent on a range of aspects of an individual’s life, such as having a strong identity, feeling loved,
having a secure base and feeling confident in oneself. More broadly, it also relates to an individual’s
ability to feel a part of wider Australian society and the ability to secure appropriate housing,
employment and / or education;
• Having the support of like-minded people – A consumer of a Macedonian background who
participated in the Wollongong forum spoke passionately about her involvement in a local support
group, and how this had made a significant positive impact on her mental health. The group was
comprised of women from Balkan backgrounds (i.e. Macedonia, Bosnian, Croatian and Serbian), all of
whom had experienced mental health issues of their own. The women met on a regular basis at the
local Migrant Resource Centre and used each meeting as an opportunity to talk through their
personal stories and issues. As the consumer commented in the forum – “…there were no support
groups 45 years ago when I migrated. I only found out about them two years ago. I had a very isolated
life before… I didn’t know about local mental health groups … my life is changed now”;
• Flexibility – What was clear from the feedback given in the forums is that there is no ‘one size fits all’
approach to dealing with mental health and wellbeing issues in CALD communities. Rather, CALD
communities are enormously varied in terms of their migration pathways, settlement issues and
capacity to cope with life in Australia. Therefore a few stakeholders commented that a mental health
© DIVERSEWERKS 12

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
system which allowed CALD communities a range of ways to engage with ‘help’ was important,
including less formal options. Using community leaders as trusted support people, for instance, was
seen as one way that there could be more openness to seeking assistance for mental health issues in
some CALD communities. Community leaders were seen by several stakeholders as wonderful,
trusted, non-judgemental supports for people of CALD backgrounds who may be experiencing a
mental health issue;
• Ensuring GPs are well-equipped and resourced – There was a feeling among some stakeholders that
GPs were often poorly equipped and / or resourced to identify potential mental health issues among
CALD patients, particularly if physical health issues were quite pronounced or if there were language
barriers for instance. GPs were seen as an important health resource for CALD communities as they
are usually highly trusted by communities, as well as being service providers who are most likely to
see those at risk in CALD communities;
• Educating CALD communities – Not surprisingly, a number of stakeholders across the forums felt
that educating CALD communities around mental health more broadly, as well as about some of the
specific issues which could arise, was critical to developing resilient communities with a greater
likelihood of recovery. By educating CALD communities about mental health, it was felt that this
could help lessen the stigma associated with poor mental health within CALD communities, and
therefore increase the likelihood that those in need of help feel comfortable seeking assistance.
2.4 Priority areas - mental health and wellbeing in CALD communities
Stakeholders across the Campsie and Wollongong forums were asked to nominate what they felt were priority
areas for mental health in NSW for CALD communities. Tables 1 and 2 below provide a summary of their
responses. The number following each priority area listed indicates the number of ‘votes’ given to that idea by
stakeholders in each forum and therefore its relative importance. Each participant was given the option of
voting for three areas in total.
© DIVERSEWERKS 13

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Table 1: Perceived priority areas for mental health and wellbeing in CALD communities (Campsie)
Improving the overall cultural competence of the mental health system (15)
Removing the stigma and taboo around mental health issues in CALD communities (can lead to better
mental health stabilisation / recovery) (12)
Accessing knowledgeable primary health services (e.g. GPs who are well informed about mental health
issues affecting CALD communities, and the range of pathways available) (11)
Improved community awareness of mental health issues, particularly in CALD communities, and on a
continual basis (e.g. you can stablise the condition but you may not ‘just recover’; these are some of the
symptoms of this mental health issue) (6)
Early intervention to avert mental health and comorbidity issues (6)
Consider cultural needs in care plan development (e.g. consider the cultural, spiritual, religious and ‘whole of
family’ needs of a consumer / their carer) (3)
Provision of easy-to-access emergency response facilities which CALD communities can access. Within this,
ensuring that several access points are available and are simple (2)
A focus on CALD wellbeing and community resilience (2)
Making mental health services more affordable and / or communicating some of the more affordable options
available to CALD communities (1)
The mental health system providing a sense of hope / that there are a range of options available to CALD
communities and their carers. This includes accessible respite care for CALD families where there are mental
health issues (1)
© DIVERSEWERKS 14
Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
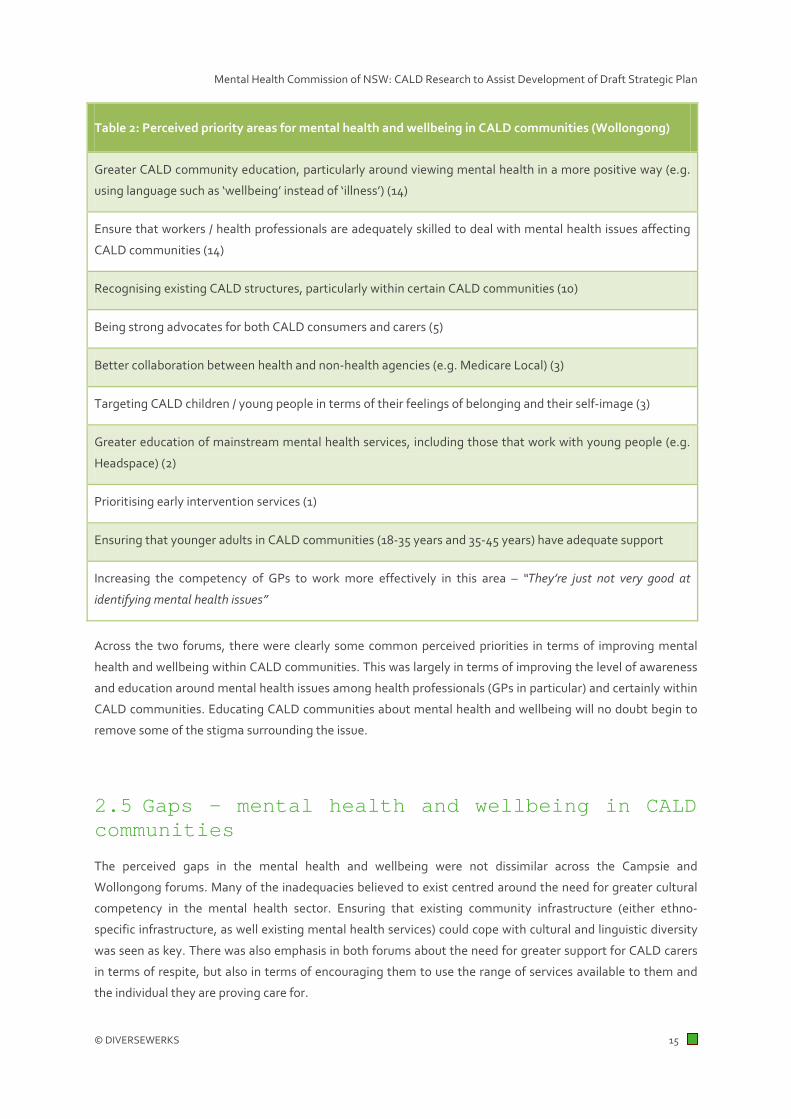
Table 2: Perceived priority areas for mental health and wellbeing in CALD communities (Wollongong)
Greater CALD community education, particularly around viewing mental health in a more positive way (e.g.
using language such as ‘wellbeing’ instead of ‘illness’) (14)
Ensure that workers / health professionals are adequately skilled to deal with mental health issues affecting
CALD communities (14)
Recognising existing CALD structures, particularly within certain CALD communities (10)
Being strong advocates for both CALD consumers and carers (5)
Better collaboration between health and non-health agencies (e.g. Medicare Local) (3)
Targeting CALD children / young people in terms of their feelings of belonging and their self-image (3)
Greater education of mainstream mental health services, including those that work with young people (e.g.
Headspace) (2)
Prioritising early intervention services (1)
Ensuring that younger adults in CALD communities (18-35 years and 35-45 years) have adequate support
Increasing the competency of GPs to work more effectively in this area – “They’re just not very good at
identifying mental health issues”
Across the two forums, there were clearly some common perceived priorities in terms of improving mental
health and wellbeing within CALD communities. This was largely in terms of improving the level of awareness
and education around mental health issues among health professionals (GPs in particular) and certainly within
CALD communities. Educating CALD communities about mental health and wellbeing will no doubt begin to
remove some of the stigma surrounding the issue.
2.5 Gaps - mental health and wellbeing in CALD communities
The perceived gaps in the mental health and wellbeing were not dissimilar across the Campsie and
Wollongong forums. Many of the inadequacies believed to exist centred around the need for greater cultural
competency in the mental health sector. Ensuring that existing community infrastructure (either ethno-
specific infrastructure, as well existing mental health services) could cope with cultural and linguistic diversity
was seen as key. There was also emphasis in both forums about the need for greater support for CALD carers
in terms of respite, but also in terms of encouraging them to use the range of services available to them and
the individual they are proving care for.
© DIVERSEWERKS 15

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Specifically, the gaps mentioned by stakeholders in each forum are summarised below in tables 3 and 4.
Table 3: Perceived gaps in mental health and wellbeing in CALD communities (Campsie)
Research on CALD mental health issues
A multicultural health workforce / counsellors, as well as providing adequate support for them
Flexible funding arrangements for services. There was some feeling among stakeholders that funding
parameters within some services were too narrow compared to the broad range of needs that exist in CALD
communities
Understanding non-traditional areas of consideration from a CALD perspective, such as homelessness,
sexual orientation or substance use, for instance, which have a significant impact on one’s mental health
Telephone helplines or other confidential emergency access points where CALD communities can tap into
mental health services (e.g. internet counselling in-language)
Ethno-specific organisations who have the capacity to provide mental health services (beyond Transcultural
Mental Health Centre)
Respite services for carers. This was seen as a substantial gap among a number of stakeholders
Adequately equipping mainstream mental health services to deal with cultural and linguistic diversity –
“…you can’t just assume that people from certain CALD communities will necessarily use CALD-specific services,
especially if the taboos around mental health are significant in their community”
Learning from and sharing the positive experiences / successes in mental health among well-established
CALD communities
© DIVERSEWERKS 16

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Table 4: Perceived gaps in mental health and wellbeing in CALD communities (Wollongong)
Support services for carers, who were perceived to access existing services poorly either due to the stigma
associated with mental illness or as a result of the lack of awareness about the services available
Early intervention services, particularly for CALD communities in immediate need
Service models that meet the needs of the range of CALD communities living in the area
Ethnic community infrastructure for new and emerging communities
Ensuring there is adequate religious service capacity. This was seen as important as in some communities
religion / religious leaders can act as a proxy for mental health services
Clear definitions of what ‘mental health’ encompasses (e.g. it’s not a ‘bad omen’ or a ‘curse’ – “You need to
know what it isn’t in some communities before you can define what it is”)
Addressing the perceived ‘underperformance’ of migrants (e.g. highly educated migrants not having their
qualifications recognised in Australia)
The mental health sector’s capacity / competency to work with a range of vulnerable people in CALD
communities, such as young refugees or 204 visa holders (‘Women at risk’ visa)
2.6 Successful Innovations – Mental health and wellbeing in CALD communities
In terms of the innovations or successes stakeholders had seen in how CALD mental health needs are
managed, a common theme mentioned in both forums was the utilisation of existing community leaders to
help promote mental health and wellbeing issues more strongly and act as general advocates for the issue
within their community.
Examples of this that were given included a local Imam (a community figure highly respected) educating their
community about mental health issues - “…(religion) can play such a good role in breaking down the taboos
around mental health” (Wollongong stakeholder). Another example given was using existing CALD
‘community assets’ to speak to the community about mental health across a range of formal or informal
settings. These are individuals in CALD communities who are trusted either because they have dealt with
similar issues before, or because they are considered leaders in their community – “Just being around your
culture, and feeling like they understand you can be enough … it doesn’t matter if you’re a clinician or not”
(Campsie stakeholder).
© DIVERSEWERKS 17

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
The utilisation of CALD role models to positively promote mental health and wellbeing within communities
was also felt to be an important preventative strategy. CALD role models could help facilitate successful
migration by helping guide individuals in their community and provide support for how to integrate into the
wider community – “…(they can be) someone to show you the ropes and give you some sense as to what this
society’s about” (Wollongong stakeholder).
There were also suggestions across both forums about shifting the language around mental health in the
marketing or promotion of mental health issues to CALD communities, to be more positive. Although no
stakeholders reported had seen this done successfully, ‘rebranding’ the way mental health is discussed in
CALD communities was seen as an opportunity to demystify mental health issues across these communities,
where (as discussed earlier) taboo and stigma are fairly significant - “…we need to talk about being ‘healthy’ and
‘well’ and ‘fit’ … and talk about resilience, happiness and wellbeing and how to make these pronounced, instead of
what’s ‘wrong’ with a community all the time” (Campsie stakeholder).
In Campsie, several stakeholders felt that there were opportunities for ‘mental health and wellbeing’ to borrow
some of the clever social marketing techniques applied by other potentially sensitive health issues affecting
CALD communities, such as diabetes, HIV and breast cancer screening, for instance. Praise was given for the
way in which social marketing around these issues had tackled stigma, for instance, or even challenged
community perceptions around issues (e.g. ‘diabetes is a condition that needs to be managed’ vs. ‘diabetes
can be cured’) – “… mental health (as an issue) can learn from this”.
Other strategies which were seen, by stakeholders, as being good-practice ways that mental health and
wellbeing issues were managed in CALD communities were:
• Utilising bilingual community education staff to conduct education sessions with CALD communities,
“especially if they’re peers”;
• Open discussion about mental health and wellbeing issues on ethnic radio;
• Creating ethno-specific consumer and carer support groups, so that there were opportunities in
communities for individuals to connect with others who had similar experiences.
© DIVERSEWERKS 18

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
3. Case studies 3.1 Case study 1: Anna Diomedi, Leichhardt NSW
Anna is a 74 year old woman of an Italian background who lives with her husband and two adult twin children,
one of which is married with a child, bringing the household composition to six. She has two other children
who have left home.
Anna migrated to Australia with her immediate family in 1969 from the Marche region of Italy. The family
were joined by her husband’s two sisters to complete the household of eight people. Anna had no other
relatives in Australia at that time. Still today, Anna is devoted to her home, children and grandchildren and
they are the total focus in her life to date.
In terms of her work history, Anna was a cook, working in a number of Italian restaurants, including a stint
when Anna and her husband ran a small pizzeria. This period in food services continued well into the 1980s,
after which she worked in the textiles area supporting her two sisters-in-law who were seamstresses. This
involved long periods of piecework and outwork activities, which continued until the death of one of her
sisters-in-law from cancer. From 1994 to her retirement in 2006, Anna worked in St Vincent’s Hospital in the
food services area. This period is one that Anna looks upon fondly, even though it was the first time she had
worked in an English-speaking work environment. She liked how her experience and skills were valued,
regardless of her poor English.
In 2006 Anna left work following the death of her other sister-in-law from pancreatic cancer, as well as her
husband being diagnosed with colon cancer and Parkinson’s disease. This period of loss and grief was
accompanied by Anna herself having a host of health problems. This included thyroid problems, general pain
as well as a growing sense of anxiety and anger, particularly around her diminished physical capacity to care
© DIVERSEWERKS 19

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
for her husband in the future. Anna found it increasingly difficult to feel better, regularly visiting GPs to help
with her pain management and other physical ailments. This cycle of behaviour continued until 2010 when,
after one GP visit in which Anna expressed increasing feelings of anger, she was referred to Canterbury
Hospital to see an Italian-speaking psychologist. It was the first time Anna had spoken to a psychologist
before. She was diagnosed with depression and referred to CoAsIt in Leichhardt, which provides a range of
mental health services to the Italian community.
Anna has been getting support from an Italian speaking counsellor for the past three years but she does not
see herself getting better: “I don’t think I will get better, I am constantly angry, I act out and things get on my
nerves. Why can’t I do what I want to do?” Despite this, Anna likes the fact that in her counselling sessions, she
feels listened to and has someone who understands the feelings she’s describing.
The view among Italian speaking mental health professionals is that while counselling is important, it is made
difficult by the prevailing attitudes in the Italian community which are typified by a lack of understanding of
what counselling is and what it can achieve: “They aren’t engaging with the notion that they can help
themselves, indeed the opposite if often truer with clients wanting to know what the mental health professional
can do for them and more specially to fix them”.
This is also how Anna feels. She remains angry that her body will not let her do what she wants, due to its
physical limitations brought on by her health complications. Ideally, Anna wants to help support and care for
her family – her children, grandchildren and her husband. Even seemingly simple tasks, such as preparing her
granddaughter’s lunch, can prove to be challenging for Anna and help fuel the anger she feels about her body’s
physical limitations. She has a litany of health conditions and procedures that include ongoing thyroid issues,
an umbilical hernia, a stooped back and increasing back and leg pain requiring ongoing treatment, including
lumbar injections. She jokes that if she were ever to return to Italy, she would have to take a whole pharmacy
with her.
Anna will continue to see her counsellor to help her cope rather than make her better. She retains a very
pessimistic attitude to her own health and that of her husband and seems to endure rather than manage her
days.
Anna also remains pleased with being in Australia: “While it has all been painful, we have been able to achieve
more here. Our kids were able to get educations and there is much less community pressure and judgement here.
That is why I am happy to tell my story”.
© DIVERSEWERKS 20

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
3.2 Case study 2: Husna Ahmadzai, Parramatta NSW
Husna is a 44 year old recently arrived refugee. She came to Australia as part of the offshore refugee program
in late 2013. Her visa category is known as Visa 204 which is a particular visa issued to women at risk. Husna
left her native Afghanistan with her family in 2000, fleeing its civil war to live in Pakistan in the refugee
community. After more than 12 years of not being able to return to Afghanistan, Husna was granted a
protection visa for Australia.
When she first came to Australia, Husna was first settled into the Coffs Harbour area, which has become the
settlement location for many refugee women at risk. Husna talks of the three months she spent in Coffs
Harbour as “awful” as she felt alienated from most of the other Afghan women (who were ethnic Hazaras) and
longed to live in a larger population where there would be an Afghan population she could connect to. Husna
has now been in the Western Suburbs of Sydney for two and a half months. Her English is extremely poor and
she is experiencing a range of problems settling, particularly in terms of finding appropriate accommodation,
employment and learning basic English.
Husna suffers from depression and anxiety attacks. She has periods of strong anger and paranoid behaviour.
She requires a lot of support, which is currently provided on an informal basis by Afghan women she trusts in
the area.
Husna attributed her mental health issues with the long period she spent in Pakistan as a stateless person, not
being able to go back to Afghanistan and experiencing difficulties in moving to a third country. She
experienced a range of stresses, not least of which were many unsuccessful attempts to obtain refugee status
in her three stated preference destinations of the USA, Canada and Australia. While in Pakistan, Husna
suffered extreme bouts of depression brought on in her words “by the stresses of being a young woman in
Pakistan”.
In Pakistan, Husna received support from doctors and psychologists which included both counselling and
medication. She believes the support she received here was useful and gave her the tools to cope and to think
more positively. Part of this positive outlook was her belief that her future life in Australia would be much
better. However, upon arrival her immediate experience did not live up to her expectations. While she received
settlement support (including mental health support) she sought to be relocated to Sydney to have access to
the Dari speaking Afghan community.
Her first few months in Sydney were equally challenging, as she experienced difficulty in getting
accommodation there. She was initially accommodated in short term arrangements and moved from motel to
motel. A settlement case worker did find her accommodation; however it was unacceptable to Husna as it was
a significant distance from the Afghan community (most of whom are concentrated around the Parramatta /
Holroyd area of Sydney) and she found it isolating. Husna then sourced her own accommodation through
informal community networks, and now has a room in a share house where most of the other residents are
Afghan men.
These accommodation issues have been a major stress for Husna and have forced all other issues in her life to
the margins. This has included not yet visiting a GP in Sydney, nor seeing a counsellor. She acknowledges that
© DIVERSEWERKS 21

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
while she has been feeling better, she would like the assurance of seeing a counsellor and having access to
medication as an ‘insurance policy’ to deal with her conditions. Right now she is concerned with acquiring
some level of basic English and starting to seek employment.
Husna currently lives on the Newstart Allowance from Centrelink, and is finding it difficult to make ends meet
financially. Her inability to afford medications is also given as a reason for her not attending mental health
professionals at this time.
She believes that she will get better and she is benefitting from being close to the Afghan community which
she finds supportive, and of help especially in keeping her morale up. In discussing what will make her well
Husna is quite specific: “My aim is to work and to study and getting someone from my family to come to Australia
to stay with me. It will be very difficult to live my life alone in Australia”.
© DIVERSEWERKS 22

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
4. Data analysis 4.1 Size of CALD communities in NSW
A key starting point for understanding the nature of cultural and linguistic diversity in NSW is to examine the
number of people living in the state who speak a language other than English at home (see table 5 below).
According to the 2011 Census, in NSW Chinese languages are most commonly spoken and account for 16.1%
of all languages other than English (LOTE) spoken across the state. This is predominantly made up of
Mandarin and Cantonese speakers, with a similar number of individuals speaking each of these languages.
Arabic is the next most common language spoken at home in NSW, accounting for 10% of all LOTE spoken
across the state. Much further behind in terms of relative number of speakers, however still sizable overall, are
the proportion of the NSW population who speak Vietnamese, Greek and Italian, with over 80,000 people in
each of these language groups speaking these languages at home.
Table 5: Top 20 languages other than English spoken in NSW
Ranking Main language spoken at home Total % of all LOTE
1 Total Chinese 295,080 16.10%
Mandarin 139,619 7.60%
Cantonese 136,180 7.40%
Other Chinese 19,281 1.00%
2 Arabic 184,101 10.00%
3 Vietnamese 87,429 4.80%
4 Greek 86,522 4.70%
5 Italian 83,072 4.50%
6 Spanish 55,514 3.00%
7 Hindi 52,695 2.90%
8 Korean 47,317 2.60%
9 Macedonian 29,440 1.60%
10 Indonesian 24,757 1.30%
11 Croatian 22,852 1.20%
12 Turkish 22,252 1.20%
13 Serbian 22,236 1.20%
14 Russian 16,462 0.90%
15 Portuguese 16,273 0.90%
16 Thai 15,703 0.90%
17 Assyrian Neo-Aramaic 15,573 0.80%
18 Persian (excluding Dari) 14,681 0.80%
19 Japanese 14,333 0.80%
© DIVERSEWERKS 23

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
20 Khmer 10,243 0.60%
Source: ABS Census, 2011
In terms of where those who speak a LOTE reside, further analysis of 2011 Census data clearly demonstrates
that overwhelmingly, the vast majority of CALD speakers in NSW live in urban areas (Table 6 below). In some
language groups (Arabic, Mandarin, Cantonese, Vietnamese, Korean, Macedonian and Turkish, for instance)
over 98% of people live in urban areas.
Table 6: Top 20 languages other than English spoken in NSW by Urban dwellers
Ranking Top 20 LOTE Urban NSW % of total Total
1 Arabic 180,159 98.8% 182,421
2 Mandarin 136,789 98.3% 139,089
3 Cantonese 132,626 98.1% 135,219
4 Vietnamese 86,062 98.8% 87,109
5 Greek 83,406 97.4% 85,590
6 Italian 72,206 91.9% 78,584
7 Filipino (incl. Tagalog) 54,873 95.2% 57,614
8 Spanish 52,401 95.8% 54,700
9 Hindi 51,294 97.9% 52,410
10 Korean 46,520 98.7% 47,116
11 Macedonian 28,926 98.9% 29,255
12 Indonesian 24,114 97.9% 24,643
13 Turkish 21,724 98.2% 22,127
14 Serbian 21,176 97.1% 21,801
15 Croatian 21,042 95.1% 22,115
16 Tamil 20,961 97.8% 21,440
17 Bengali 20,929 97.6% 21,446
18 Punjabi 18,996 90.2% 21,064
19 German 17,266 81.1% 21,280
20 Urdu 17,133 97.4% 17,592
Total 1,124,965 96.9% 1,160,780
Source: ABS Census, 2011
An examination of languages spoken in NSW by older people (55+ years) does yield a slightly different
demographic profile. As the data in Table 7 demonstrates, the most commonly spoken language for non-
English speakers in NSW aged 55 years and over is Italian (41,252 speakers with the majority, or 32.7%, aged
between 65 and 74 years).
Those 55+ years who speak either Cantonese or Greek at home are also relatively sizable overall in NSW, with
over 30,000 people speaking each of these languages. Interestingly, among Chinese speakers overall, older
© DIVERSEWERKS 24

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
people in NSW aged 55+ years are far more likely to speak Cantonese than Mandarin (34,852 versus 19,473
people), with the majority of Cantonese speakers 55+ years aged in the 55 to 64 year old category (56%).
The majority of Greek speakers 55+ years in NSW are also aged between 65 and 74 years (38.9%), as was also
seen among Italian speakers.
© DIVERSEWERKS 25

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
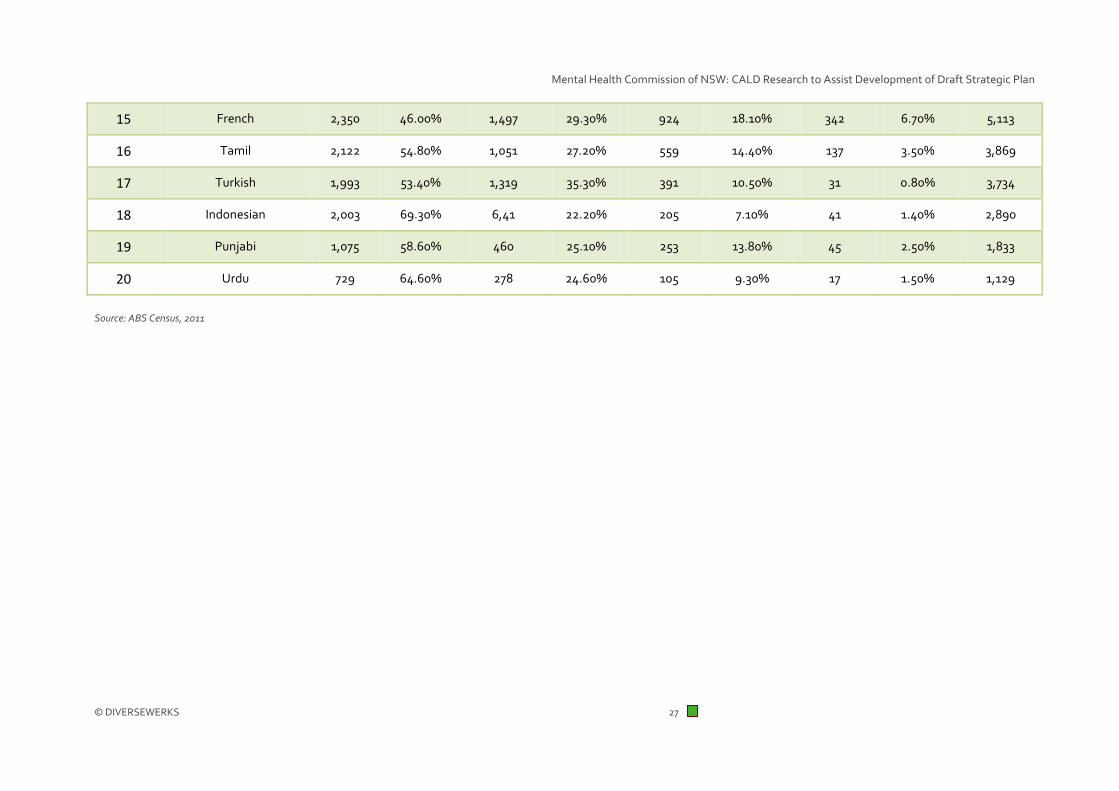
Table 7: Top 20 languages other than English spoken in NSW by older people 55+ years
Ranking Top 20 LOTE in NSW 55-64 years
% of total 55-64 NSW
65-74 years % of total 65-74 NSW
75-84 years % of total 75-84 NSW
85+ years % of total 85+ NSW
Total 55+ NSW
1 Italian 11,691 28.30% 13,498 32.70% 13,023 31.60% 3,040 7.40% 41,252
2 Cantonese 19,509 56.00% 8,376 24.00% 5,469 15.70% 1,498 4.30% 34,852
3 Greek 9,553 29.50% 12,603 38.90% 8,815 27.20% 1,397 4.30% 32,368
4 Arabic 15,622 53.50% 8,893 30.50% 3,916 13.40% 765 2.60% 29,196
5 Mandarin 11,328 58.20% 4,799 24.60% 2,968 15.20% 378 1.90% 19,473
6 Spanish 7,807 48.10% 5,539 34.10% 2,421 14.90% 464 2.90% 16,231
7 Vietnamese 8,064 61.40% 2,792 21.30% 1,824 13.90% 453 3.40% 13,133
8 Filipino (incl. Tagalog) 8,621 70.10% 2,361 19.20% 1,002 8.10% 314 2.60% 12,298
9 German 2,674 27.00% 3,367 34.00% 2,816 28.40% 1047 10.60% 9,904
10 Croatian 3,336 34.40% 4,007 41.30% 2,120 21.80% 245 2.50% 9,708
11 Macedonian 4,836 50.00% 2,995 31.00% 1,591 16.40% 254 2.60% 9,676
12 Serbian 3,336 50.40% 2,144 32.40% 991 15.00% 152 2.30% 6,623
13 Korean 3,453 53.80% 2,001 31.20% 815 12.70% 148 2.30% 6,417
14 Hindi 3,662 60.30% 1,683 27.70% 634 10.40% 99 1.60% 6,078
© DIVERSEWERKS 26
Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
15 French 2,350 46.00% 1,497 29.30% 924 18.10% 342 6.70% 5,113
16 Tamil 2,122 54.80% 1,051 27.20% 559 14.40% 137 3.50% 3,869
17 Turkish 1,993 53.40% 1,319 35.30% 391 10.50% 31 0.80% 3,734
18 Indonesian 2,003 69.30% 6,41 22.20% 205 7.10% 41 1.40% 2,890
19 Punjabi 1,075 58.60% 460 25.10% 253 13.80% 45 2.50% 1,833
20 Urdu 729 64.60% 278 24.60% 105 9.30% 17 1.50% 1,129
Source: ABS Census, 2011
© DIVERSEWERKS 27

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
4.2 Poor English language proficiency
As well as understanding the proportion of people speaking a language other than English in NSW, it is
important to examine the level of English language proficiency (ELP) within language groups. Those in the
community with poor ELP are often considered more vulnerable in terms of gaining access to services.
Services themselves may also lack the capacity to provide culturally appropriate help.
Table 8 below shows the proportion of people within the top 20 languages spoken in NSW who speak English
‘not very well’ or ‘not at all’, as captured in the 2011 Census. Of the more widely spoken languages, those who
speak Vietnamese, and to a lesser extent, Korean are notable in terms of their poor ELP, with one third of
speakers in each of these communities not speaking English well or at all. Mandarin and Cantonese speakers
had similar proportions of poor ELP, with just over one quarter of speakers having poor English in each
language group. Within the more popular CALD language groups, Arabic, Greek and Italian speakers appear to
be less likely to have poor English language comparatively, with poor ELP only an issue for 15.5% of Arabic-
speakers, 15.9% of Greek-speakers and 13.3% of Italian speakers across NSW.
Table 8: Poor English Language Proficiency (ELP) among top 20 languages other than English spoken in NSW
Ranking Top 20 LOTE spoken at home Total Total number with poor ELP
Total % Poor ELP
1 Total Chinese 295,080 77,995 26.4%
Mandarin 139,619 36,578 26.2%
Cantonese 136,180 36,272 26.6%
Other Chinese 19,281 5,145 26.7%
2 Arabic 184,101 28,457 15.5%
3 Vietnamese 87,429 29,078 33.3%
4 Greek 86,522 13,793 15.9%
5 Italian 83,072 11,073 13.3%
6 Spanish 55,514 7,168 12.9%
7 Hindi 52,695 2,802 5.3%
8 Korean 47,317 15,780 33.3%
9 Macedonian 29,440 5,061 17.2%
10 Indonesian 24,757 2,449 9.9%
11 Croatian 22,852 3,032 13.3%
12 Turkish 22,252 4,410 19.8%
© DIVERSEWERKS 28

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
13 Serbian 22,236 4,053 18.2%
14 Russian 16,462 2,711 16.5%
15 Portuguese 16,273 2,656 16.3%
16 Thai 15,703 3,241 20.6%
17 Assyrian Neo-Aramaic 15,573 3,018 19.4%
18 Persian (excluding Dari) 14,681 2,429 16.5%
19 Japanese 14,333 2,379 16.6%
20 Khmer 10,243 3,606 35.2%
Source: ABS Census, 2011
However English language proficiency does differ considerably by age, with a general increase in poor ELP
among those who are older.
Table 9 shows the adults aged 55+ years in NSW who speak a language other than English and who also speak
English poorly. In some communities, the majority of people aged 55+ years speak little or no English (e.g.
Vietnamese, Korean, Mandarin and, to a lesser extent, Cantonese-speakers). Other CALD groups which are of
significance are Greek and Italian speakers aged 55+ years. Even though the proportion of people in these
communities who have little or no English is far less compared to other languages, the sizable nature of these
communities means that the total number of people with poor ELP overall is still of relative importance
(11,670 and 9,720 people with poor ELP in NSW respectively). This has implications for mental health service
provision in NSW, as there are clearly likely to be considerable language needs for older people from these
communities who require mental health and wellbeing services.
© DIVERSEWERKS 29

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Table 9: Poor English Language Proficiency (ELP) among top 20 languages other than English spoken in NSW (55+ years)
Ranking 55+ years Total number with poor ELP
% of Poor ELP Total Population
1 Italian 9,720 23.1% 42,012
2 Cantonese 18,172 51.7% 35,163
3 Greek 11,670 35.6% 32,766
4 Arabic 10,062 34.2% 29,392
5 Mandarin 12,880 65.8% 19,571
6 Spanish 4,562 27.9% 16,360
7 Vietnamese 9,006 68.1% 13,229
8 Filipino Tagalog 777 6.3% 12,369
9 German 301 3.0% 10,113
10 Croatian 2,490 25.5% 9,778
11 Macedonian 4,074 41.8% 9,746
12 Maltese 933 10.7% 8,708
13 Polish 1,166 17.3% 6,749
14 Serbian 2,581 38.8% 6,657
15 Korean 4,294 66.6% 6,449
16 Hindi 952 15.6% 6,099
17 Russian 1,875 35.4% 5,293
18 French 256 4.9% 5,181
19 Dutch 86 1.8% 4,728
20 Hungarian 533 13.0% 4,100
Source: ABS Census, 2011
Communities with poor ELP can be more vulnerable in terms of service access, therefore identifying where
these individuals reside is valuable as it highlights where existing services may need to adopt different
strategies to attract CALD community members, for instance. Furthermore, such geographical information
may also be useful in highlighting where there may be a need for more culturally competent practice. In NSW,
the Local Government Areas (LGAs) with the highest numbers of people with poor English are shown in Table
10 which follows.
© DIVERSEWERKS 30

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Table 10: Top 10 LGAs in NSW with highest number of poor ELP dwellers
Ranking LGA Poor ELP % of Total Population in LGA
Total Population in
LGA
1 Fairfield 38,244 20.4% 187,929
2 Canterbury 20,168 14.6% 138,046
3 Bankstown 19,970 10.9% 182,963
4 Liverpool 15,737 8.7% 180,688
5 Parramatta 15,016 8.8% 170,239
6 Auburn 13,759 18.4% 74,921
7 Hurstville 7,931 10.0% 79,084
8 Kogarah 5,022 8.8% 56,759
9 Burwood 3,885 11.8% 32,903
10 Strathfield 3,845 10.8% 35,442
Total 143,577 12.6% 1,138,974
Source: ABS Census, 2011
Clearly, the Fairfield LGA is a priority area in terms of providing services in-language, with just over one in five
residents (38,244 or 20.4% of the LGA’s population) speaking English poorly. Canterbury and Bankstown also
have a relatively large number of people with poor ELP compared to other LGAs (about 20,000 people in each
LGA). Also of note when examining ELP data by LGA is the Auburn area, where almost one in five residents
(18.4% or 13,759 people) have poor English, which represents the second highest proportion overall.
When these top 10 LGAs for poor ELP are placed on a map, it is clear that the LGAs with the most significant
language needs are located in close proximity to one another and skewed west and south west of the CBD, as
shown in figure 1 below.
© DIVERSEWERKS 31

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Figure 1: Top 10 LGAs in NSW with highest number of poor ELP dwellers
Source: ABS Census, 2011. Counting: Persons, Location on Census Night
4.3 Country of birth
Data on language spoken can indicate priority groups for mental health services, particularly in terms of their
size and the level of English language proficiency. Understanding country of birth data is also a useful measure
for the Commission to consider as an individual’s experiences in their home country may be critical in shaping
current and / or future mental health needs, particularly if there has been a history of conflict in one’s country
of origin, for instance.
According to the 2011 Census, the top 10 countries of birth among people living in NSW are shown in Table 11.
© DIVERSEWERKS 32

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Table 11: Top 10 countries of birth among people living in NSW
Ranking Country 0-24
years
% of total pop.
25-54
years
% of total pop
55-85+ years
% of total pop
Total
1 China 84,056 26.4% 175,125 55.0% 59,156 18.6% 318,337
2 India 59,289 20.1% 197,355 66.9% 38,348 13.0% 294,992
3 Vietnam 18,350 9.9% 125,230 67.8% 41,192 22.3% 184,772
4 Italy 2,574 1.4% 30,618 16.8% 149,349 81.8% 182,541
5 Philippines 34,425 20.1% 105,537 61.7% 31,130 18.2% 171,092
6 Malaysia 26,081 22.5% 61,639 53.1% 28,365 24.4% 116,085
7 Germany 6,883 6.4% 32,238 30.1% 67,936 63.5% 107,057
8 Greece 1,746 1.8% 17,144 17.3% 80,067 80.9% 98,957
9 Sri Lanka 14,104 16.4% 50,873 59.0% 21,227 24.6% 86,204
10 Lebanon 5,206 6.8% 45,091 59.1% 25,953 34.0% 76,250
Source: ABS Census, 2011
Migrants from China are the largest group of individuals in NSW born overseas (318,337 people), the majority
of who are aged 25-54 years (55% of all Chinese-born migrants). Also significant in size are Indian-born
migrants, who make up the second largest migrant group in NSW (294,992 people, with 66.9% aged between
25 and 54 years).
Within the top 10 countries of birth among people living in NSW, it is important to note the inclusion of
Vietnamese (184,772), Sri Lankan (86,204) and Lebanese-born (76,250) migrants, as these countries have had
a history of conflict in recent years, which could heighten their vulnerability to developing issues around
mental health and wellbeing.
4.4 Recent arrivals data
Recent arrivals data is also important to consider when understanding the nature of CALD communities in
NSW. Recent arrivals have a greater likelihood of having pressing issues with settlement, migration or general
challenges to one’s mental wellbeing, for instance, than other CALD groups living in Australia for a longer
period of time.
Data captured in the 2011 Census, shown in table 12, demonstrates the broad nature of migration to NSW
over the last ten years. Of all the Chinese-born migrants to NSW from 2002 until late 2011, almost half (47.4%,
or 70,638) only arrived in the last ten years. Even more pronounced in terms of recency of arrival is the Indian
community, where almost two thirds of people in NSW born in India (63.7%) have arrived in the last decade.
© DIVERSEWERKS 33

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Other countries of origin where migration has to NSW has largely been a recent activity and predominantly
occurred in the last ten years are:
• Nepal - 88.9% of all people born in Nepal arrived in the last ten years;
• Bangladesh - 65.5% of all people born in Bangladesh arrived in the last ten years;
• Thailand - 54.4% of all people born in Thailand arrived in the last ten years.
One community to be cognisant of when examining country of birth data over the past 10 years is the Iraqi
community. In NSW, the 2011 Census recorded 13,695 people born in Iraq who arrived in NSW the past ten
years. This represents almost half (48.2%) of the total number of people in NSW who have arrived from Iraq,
and the fifth largest country of birth for all people in NSW born overseas who have migrated in the past ten
years. The history of war in Iraq has no doubt had an adverse effect on the mental health and wellbeing of this
community.
Table 12: Top 20 countries of birth among people living in NSW (1 January 2002 – 9 August 2011*)
Ranking Top 20 Countries of birth for arrivals
2002 or later (last 10 years)
% Total of all arrivals
1 China 70,638 47.4%
2 India 58,838 63.7%
3 Philippines 21,085 31.0%
4 South Korea 18,391 46.6%
5 Iraq 13,695 48.2%
6 Nepal 13,230 88.9%
7 Vietnam 11,506 16.9%
8 Bangladesh 10,836 65.5%
9 Indonesia 10,244 39.7%
10 Thailand 8,962 54.1%
11 Sri Lanka 7,752 33.7%
12 Malaysia 7,576 28.8%
13 Fiji 7,396 23.9%
14 Pakistan 6,970 54.3%
15 Lebanon 6,897 13.0%
16 Hong Kong 6,541 17.5%
17 Iran 5,741 38.6%
© DIVERSEWERKS 34

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
18 Japan 5,148 45.2%
19 Germany 4,746 15.9%
20 Brazil 4,249 68.6%
Total 300,441 39.3%
Source: 2011 ABS Census *: 2011 Census conducted on August 9, 2011
An examination of data from the Department of Immigration and Border Protection‘s Settlement Reporting
Facility1 allows a more recent and detailed description of migration to Australia. Table 13 provides a snapshot
of all permanent arrivals to NSW according to their migration stream, from 31 October 2003 to 31 October
2013, by:
• Humanitarian entrants: These are individuals who have arrived in Australia with a visa under the
Department’s humanitarian stream. This is comprised of individuals entering Australia under the
onshore protection / asylum component (i.e. people already in Australia who are found to be refugees
according to the Refugees Convention) and the offshore resettlement component;
• Family entrants: These individuals are selected on the basis of their family relationship with their
sponsor in Australia and includes four main categories - partner, child, parent and other family visa
categories;
• Skilled entrants: Individuals who have been granted a visa based on their possession of a certain set
of skills which are of value to Australia.
Within these three migration streams, it is highly likely that people who migrate via the humanitarian stream
are far more vulnerable in terms of their mental health and wellbeing, due to the events leading up to their
arrival from their country of origin (e.g. civil war, torture and trauma), the method in which they arrived to
Australia (e.g. by boat seeking asylum) or due to the difficulty they may have had in adjusting to life in
Australia (e.g. cultural or language barriers, homesickness, isolation). Clearly, all of these issues are closely
linked to one’s mental health and capacity to cope with life in a new and, often, very different country.
As the data in table 13 demonstrates, permanent arrivals to NSW via the humanitarian stream are enormously
varied in terms of their countries of origin, although many hail from the Middle East and Africa (Sudan, Sierra
Leone, Liberia and the Congo).
The most significant CALD community in terms of humanitarian entrants and therefore the community most
at risk of developing mental health issues within this category of migrants are permanent arrivals from Iraq,
with 14,420 people settling in NSW over the last ten years. This is substantially more than any other group of
humanitarian entrants in NSW over the same period.
1 http://www.immi.gov.au/settlement/srf/
© DIVERSEWERKS 35

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Permanent arrivals from Iran, Sudan and Afghanistan comprise the next most significant group of
humanitarian entrants to NSW over the last decade. Again, the conflict experienced in these regions and / or
countries no doubt challenges the mental health and wellbeing of migrants from these areas substantially and
should be taken into account when considering the nature of mental health and wellbeing services available.
Table 13: Country of origin of permanent arrivals to NSW by migration stream (31 October 2003 – 31 October 2013)
Country of birth
Humanitarian
% All Humanitari
an
Family % Total Family
Skilled % Total Skilled
Total Humanitarian, Family & Skilled
1 Iraq 14,420 33.5% 3,078 1.5% 270 0.1% 17,768
2 Iran 3,692 8.6% 1,562 0.8% 3,806 1.3% 9,060
3 Sudan 3,657 8.5% 461 0.2% 47 0.0% 4,165
4 Afghanistan 3,467 8.0% 2,442 1.2% 25 0.0% 5,934
5 People’s Republic of China
2,147 5.0% 41,251 20.1% 5,1173 17.3% 94,571
6 Sri Lanka 1,699 3.9% 2,318 1.1% 5,360 1.8% 9,377
7 Burma 1,482 3.4% 726 0.4% 488 0.2% 2,696
8 Sierra Leone 1,312 3.0% 259 0.1% 7 0.0% 1,578
9 Arab Republic of Egypt
1,160 2.7% 1,473 0.7% 1,728 0.6% 4,361
10 Pakistan 970 2.3% 3,219 1.6% 5,115 1.7% 9,304
11 Australia 692 1.6% 435 0.2% 6,657 2.2% 7,784
12 Liberia 544 1.3% 65 0.0% 4 0.0% 613
13 Bhutan 536 1.2% 4 0.0% 11 0.0% 551
14 Democratic Republic of Congo
429 1.0% 61 0.0% 24 0.0% 514
15 Nepal 406 0.9% 1,668 0.8% 8,220 2.8% 10,294
16 Syria 368 0.9% 1,106 0.5% 139 0.0% 1,613
17 Thailand 357 0.8% 6,337 3.1% 2,390 0.8% 9,084
18 Kenya 310 0.7% 288 0.1% 554 0.2% 1,152
19 Ethiopia 303 0.7% 309 0.2% 32 0.0% 644
© DIVERSEWERKS 36

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
20 Lebanon 299 0.7% 7,410 3.6% 1,083 0.4% 8,792
Total 43,087 88.8% 205,650 36.2% 295,880 29.4% 544,617
A breakdown of languages spoken among permanent arrivals, particularly humanitarian entrants, over the
same ten year period also gives some indication of where the mental health and wellbeing priorities may be
for more recent arrivals in NSW (as shown in table 14).
Arabic is by far the most commonly spoken language among humanitarian entrants to NSW over the past ten
years (14,599 people speaking Arabic), followed by Assyrian (3,322), a language largely spoken in Iraq, and
Dari (2,383), spoken by many Afghans.
Table 14: Language spoken by permanent arrivals to NSW by migration stream (31 October 2003 – 31 October 2013)
Language spoken
Humanitarian
% All Humanitaria
n
Family % Total Family
Skilled % Total Skilled
Total Humanitarian, Family &
Skilled
1 Arabic 14,599 33.9% 7,720 3.8% 430 0.1% 22,749
2 Assyrian 3,322 7.7% 621 0.3% 4 0.0% 3,947
3 Dari 2,383 5.5% 887 0.4% 3 0.0% 3,273
4 Farsi (Persian)
1,991 4.6% 704 0.3% 301 0.1% 2,996
5 Mandarin 1,637 3.8% 16,538 8.0% 5,665 1.9% 23,840
6 Tamil 1,592 3.7% 868 0.4% 282 0.1% 2,742
7 African Languages (NFD*)
1,276 3.0% 31 0.0% 1 0.0% 1,308
8 English 1,238 2.9% 35,357 17.2% 59,050 20.0% 95,645
9 Persian 1,082 2.5% 365 0.2% 99 0.0% 1,546
10 Nepali 904 2.1% 485 0.2% 276 0.1% 1,665
11 Dinka 883 2.0% 51 0.0% 0 0.0% 934
12 Hazaragi 839 1.9% 43 0.0% 0 0.0% 882
13 Not stated 718 1.7% 88,677 43.1% 215,591 72.9% 304,986
14 Burmese / Myanmar
683 1.6% 302 0.1% 28 0.0% 1,013
15 Urdu 541 1.3% 981 0.5% 243 0.1% 1,765
16 Swahili 517 1.2% 36 0.0% 0 0.0% 553
© DIVERSEWERKS 37

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
17 Chaldean Neo-Aramaic
512 1.2% 37 0.0% 0 0.0% 549
18 African Languages (NEC**)
491 1.1% 28 0.0% 2 0.0% 521
19 Farsi (Afghan)
482 1.1% 143 0.1% 20 0.0% 645
20 Krio (Sierra Leone)
395 0.9% 37 0.0% 0 0.0% 432
Total 43,087 83.7% 205,650 74.8% 295,880 95.30% 471,991
*: NFD = Not further defined **: NEC = Not elsewhere classified
4.5 Carers in CALD communities
The 2011 Census also collected data on whether individuals provided ‘unpaid assistance’ to family members, or
other people, in the last two weeks. Unpaid assistance was defined in the 2011 Census as providing unpaid
care, help or assistance because of a disability, a long term illness or problems related to old age. Analysis of
this data can give some indication of the proportion of carers from CALD backgrounds in NSW, and also how
this may differ compared with the proportion of carers in the mainstream. While this Census question may not
specify that mental illness is included in the definition of unpaid assistance, the broadness of the definition
nevertheless encompasses caring for someone with a mental health issue.
Table 15 shows the top 20 languages (other than English) spoken among those in NSW who provided some
form of unpaid assistance to someone in the last fortnight. Among all CALD carers in NSW, Arabic-speakers
are the largest group, with 20,735 people providing some form of unpaid assistance to someone else
(representing 11.3% of the Arabic-speaking population in NSW, compared to 9.2% in NSW overall). The
number of carers in the Arabic-speaking community is almost double the amount seen in other CALD
communities.
Other CALD communities where there appears to be a relatively high level of caring are the Italian and Greek
communities - 14.9% of Italian speakers and 13.6% of Greek speakers in NSW provided some unpaid care to
others in the two weeks leading up to the 2011 Census. This was also somewhat higher than was reported in
the total population in NSW (9.2%).
© DIVERSEWERKS 38

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Table 15: Provided ‘unpaid assistance’ to family / other people in last 2 weeks by language other than English spoken (NSW)
Top 20 LOTE Provided unpaid assistance
No unpaid assistance provided
Total % of Total Population
1 Arabic 20,735 112,020 184,103 11.3%
2 Italian 12,400 61,172 83,068 14.9%
3 Greek 11,755 60,277 86,519 13.6%
4 Cantonese 11,595 103,632 136,184 8.5%
5 Mandarin 10,747 104,562 139,616 7.7%
6 Vietnamese 6,881 59,219 87,430 7.9%
7 Spanish 5,093 41,381 55,516 9.2%
8 Filipino (incl. Tagalog) 4,629 45,519 58,163 8.0%
9 Hindi 4,344 37,341 52,693 8.2%
10 Korean 3,574 33,746 47,316 7.6%
11 Macedonian 3,481 21,048 29,440 11.8%
12 Croatian 2,880 16,673 22,853 12.6%
13 Serbian 2,422 15,572 22,237 10.9%
14 Turkish 2,331 14,835 22,250 10.5%
15 German 2,236 17,024 23,295 9.6%
16 Tamil 2,103 14,776 21,498 9.8%
17 Russian 2,042 11,609 16,463 12.4%
18 Bengali 1,846 14,643 21,481 8.6%
19 Polish 1,834 11,345 14,841 12.4%
20 Assyrian Neo-Aramaic 1,791 10,006 15,575 11.5%
Total CALD 148,376 1,084,818 1,533,720 9.7%
Total NSW Population 636,016 4,442,164 6,889,472 9.2%
According to Carers Australia, it is likely that the carer figures captured in the 2011 Census are conservative
due to a lack of self-identification of taking on a caring role, misinterpretation of the Census question or not
providing a response to the question.
© DIVERSEWERKS 39

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
Carers Australia have identified a range of issues which are particularly salient for carers from CALD
backgrounds. Among some of the key issues identified are:
• The term ‘carer’ having the potential to be interpreted differently in CALD communities;
• A lack of awareness of the term ‘carer’ overall within CALD communities;
• A tendency for professionals to not identify CALD carers as being so, often due to perceptions made
about the carer’s role in their family;
• Lesser uptake of Centrelink carer payments, benefits and concessions, due in part to the factors
identified above;
• A range of issues related to the cultural appropriateness of assessment processes, eligibility criteria
for assistance as well as the nature of services provided;
• A lack of choice between mainstream and culturally specific carer services such as respite, counselling
and support groups;
• Within support services, a lack of availability of bilingual staff, CALD staff more generally as well as
information and resources translated into different languages.
4.6 Other research on mental health in CALD
communities
There is not a large amount of research conducted on the prevalence of mental health issues in CALD
communities in NSW, and some of the research that has been conducted in this area is relatively dated. There
are, however, several papers which can be drawn upon to examine the level or nature of mental health issues
experienced in CALD communities. A few of the studies which are of some relevance to this research are
summarised below:
• Nielssen et al (2012) conducted data analysis of the NSW Health Admitted Patient Data Collection
(APDC) for all people admitted to a mental health unit in a NSW public hospital from 2001 to 2010 for
a psychotic disorder (including schizophrenia and mania). Based on their analysis, they found that
individuals in NSW born in Oceania (including Melanesia, Fiji, Samoa, Tonga and other Polynesian
islands, but excluding Hawaii and New Zealand) were at an increased risk of admission to NSW
psychiatric hospitals for the treatment of psychotic illness. This increased risk may be explained by a
range of factors, such as migrants being more likely to visit a hospital for help, for instance, as
opposed to another service. However it may also be a reflection of the challenges experienced by
migrants from Oceania to life in Australia. While many migrants are admitted to Australia based on
skills or enrolment in education, unskilled workers from Oceania can be permitted to enter Australia
for limited periods. This higher rate of hospitalisation may therefore reflect the more challenging
social and economic circumstances faced by migrants from Oceania compared with skilled CALD
migrants, for instance.
© DIVERSEWERKS 40

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
• Research conducted by McDonald and Steel (1997) on behalf of the Transcultural Mental Health
Centre in NSW indicated that 25% of suicide deaths from 1979 to 1994 were among people born
overseas. Within this, 60% of suicides by those born overseas were by individuals from a non-English
speaking background. More recently, in collaboration with the Transcultural Mental Health Centre
and Diversity Health Institute, the Australian Institute for Suicide Research and Prevention
examined suicide rates among first-generation migrants from 1974 - 2006. This more recent research
showed considerable diversity among migrant suicide rates based on one’s country of birth. The
highest risk of suicide was found among males and females from Eastern European countries
compared with those Australian-born. In addition, those from Northern and Western European
countries and New Zealand also had higher rates comparatively. As this research was focused on
country of birth (and therefore first-generation CALD migrants), it is somewhat limited as it does not
examine suicide rates among second-generation CALD migrants. However it is worth noting that the
Australian Institute for Suicide Research and Prevention have acknowledged that this will be what the
second component of this research will do (i.e. examine second-generation migrant suicide rates).
• In their 2003 paper summarising some of the issues around the health and wellbeing of children and
youth in detention, Raman and Goldfeld highlight the vulnerability of children exposed to violence
through war, and how this can lead to trauma post-migration. Other factors that can contribute to
the development of trauma in children include being separated from one’s family, experiencing the
loss of family and friends, the loss of one’s possessions, being subjected to extreme poverty and
experiencing marginalisation and racism in one’s host country post-migration. While this paper
focuses on the experiences of children and young people, it is highly likely that these factors can also
play a role in the development of trauma in adults from war-torn countries.
© DIVERSEWERKS 41
Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
5. Key insights to inform the Draft Strategic Plan
Key demographic insights
• The significance of the overall size of the CALD population in NSW and its many-layered diversity,
including language, culture, migration process and settlement experience;
• Of particular importance is the size of the Chinese community, representing nearly one in five people
speaking a language other than English at home;
• The over-representation of CALD people in older age cohorts, particularly within the Italian, Greek
and German communities;
• The significant linguistic issues for large populations who do not speak English well, with very high
levels of poor English recorded against a number of Asian language groups such as Vietnamese,
Korean, Cantonese and Mandarin;
• A growing cohort of new arrival groups entering Australia under the humanitarian migration plan
components. Of particular note in this regard is the size of the Iraqi population as a prominent source
country for those in this program. Other significant source countries include Iran, Sudan and
Afghanistan;
• Arabic is by far the most commonly spoken language among humanitarian entrants to NSW over the
past ten years. New minority languages to consider include Assyrian, Dari and Farsi;
• In terms of geographic considerations, the great majority of people from CALD backgrounds in NSW
live in the ten LGAs, covering the area from the inner west to the south west of Sydney. Fairfield is
the largest of these LGAs, in which over 38,000 people do not speak English well.
It is important that the ongoing development of a mental health strategy in NSW take into consideration how
this demographic profile affects both the capacity of CALD communities to understand and respond to their
own mental health issues, as well as the systemic requirements for the mental health and wellbeing sector to
respond appropriately to such diversity.
Risk factors for CALD communities
• The most significant risk factor mentioned by stakeholders in the forums was the act of migration
itself. The circumstances around an individual’s migration to Australia could be particularly traumatic
and have considerable impact on an individual’s capacity to cope in the future;
© DIVERSEWERKS 42

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
• Some stakeholders felt that asylum seekers were among those most at risk of developing mental
health issues. This was related not only to the traumatic way in which they may have arrived to
Australia, but also due to possibly having spent time in mandatory detention, for instance;
• Many stakeholders felt there was considerable stigma and taboo associated with having a mental
health issue in a range of CALD communities. This was not only in recently-arrived communities, but
also within more established CALD communities (e.g. Greek, Italian, Russian);
• The isolation that could be experienced by migrants was felt to be another mental health risk factor
for CALD communities. Smaller, more recently-arrived communities were believed to be particularly
at risk, as there was often a lack of existing community infrastructure from which emotional support
could be sought;
• There was some feeling that the mental health needs of well-established CALD communities were
nevertheless still important to consider.
These risk factors need to form part of the range of considerations and interventions being built into the
Commission’s Draft Strategic Plan. Some of these are so specific and significant, such as migration history, or
asylum seeker status, that they need stand-alone attention and responses in the strategy.
CALD mental health priority areas
• The research sought to not only identify priority areas for CALD communities within the mental
health and wellbeing context, but also to have some understanding of the relative importance of
these areas;
• The highest order issue identified across both forums was the need for the mental health and
wellbeing system, including mental health professionals, to achieve cultural competency in their
interactions with CALD communities;
• The second highest priority was given to the important area of community education and stigma
reduction around mental health issues in CALD communities;
• The third priority issue identified was understanding and enabling the range of intermediary
structures to be able to connect CALD communities with appropriate mental health and wellbeing
services. Specifically, stakeholders in the Campsie forum focused on the primary health sector (e.g.
GPs) while those in Wollongong prioritised community intermediaries and structures (e.g. ethno-
specific community organisations). This difference can be understood with reference to the
geographic reality of both forums.
These priorities should therefore be given adequate coverage and attention in the Draft Strategic Plan, as they
reflect both a high level of consensus in the forums and relevance to how CALD communities can better access
and benefit from mental health and wellbeing services.
© DIVERSEWERKS 43

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
CALD mental health and wellbeing gaps
The perceived gaps in CALD mental health and wellbeing identified in the forums were:
• A lack of ethno-specific infrastructure addressing mental health and wellbeing issues, especially for
new and emerging communities;
• Gaps in the evidence base and knowledge around the extent of mental health issues in specific
communities;
• A lack of data to consider the level of uptake of mental health services, and whether this is
commensurate with the prevalence of mental health issues in communities;
• A lack of service support for family carers, who appear to be picking up the ‘service slack’, resulting in
CALD communities not accessing mainstream services.
The Draft Strategic Plan therefore should consider the need for enhanced systemic capacity to understand
and enumerate CALD service access, as well as strategies and resources to address underutilisation issues.
Relevance of Life Course Map and Journeys to CALD communities
The most significant response to the Life Stages in the Life Course Map was that they assumed a level of
linearity and uniformity which may lack relevance for CALD communities - “For migrant people, it’s not like this.
We come in different stages … some people come with qualifications, some come as a refugee” (Campsie
stakeholder).
In terms of linearity, there was a sense that the model did not allow for one’s complete migration experience,
which stakeholders wanted to see as an identifiable and unique pathway. Therefore a number of stakeholders
commented that across the series of journeys put forward, a specific ‘migration journey’ needed to be added
to the model in order to be more inclusive of culturally and linguistically diverse experiences. This would
acknowledge the range of issues affecting CALD migrants (e.g. issues around torture and trauma in country of
origin, isolation, learning English, finding appropriate housing, finding employment etc.) which could
challenge their mental health and wellbeing, for instance. The implication of this is a strong recommendation
that a migration journey narrative be developed and included.
With regard to the issue of uniformity, the forums provided a wealth of perspectives and experiences as to
how the existing journeys may lack relevance for CALD communities. The reason given for this is that in many
instances, the experiences of CALD communities around these issues may indeed be different. As such, there
was a stated need for the narratives for each journey to be broadened and include a range of diverse
perspectives and experiences in order to give them greater CALD relevance.
© DIVERSEWERKS 44

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
6. Appendix 1: Invitation to forums
© DIVERSEWERKS 45

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
© DIVERSEWERKS 46

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
7. Appendix 2: Forum discussion questions
A. Introduction
• Introductions and purpose of the session
• The Commission, the draft Plan, the story so far
B. Overall response to the NSW Mental Health Strategy model
To what extent is this model the same (or different) from a CALD perspective?
1. Are the pre-natal, early childhood, child, adolescent, adult and older adult life stages similar, or
experienced differently for CALD groups?
2. What about the journeys shown:
3. Which of these are most important, from a CALD point of view and why?
4. What types of experiences may not be reflected in the journeys shown within CALD communities?
© DIVERSEWERKS 47

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
5. Thinking of your own experience with mental illness, do the journeys shown reflect the key issues or
elements of your experience? What is missing?
6. What would need to be changed to alter your experience in these journeys, to make them better?
7. What are some of the mental health risk factors at play for CALD communities during the different life
stages?
8. What are some of the supporting factors which contribute to mental wellbeing in CALD communities?
9. Overall, what factors contribute to the development of resilience in CALD communities?
10. What factors are crucial to helping those from CALD backgrounds make a recovery?
C. What does mental health mean in CALD communities ?
11. What are the priority areas for mental health and wellbeing in CALD communities?
12. Stigma around mental health in CALD communities, and where it’s heightened / less so
13. Experiences causing mental illness / distress in some CALD groups such as migration experience itself,
PTSD, torture / trauma
14. Traditional interpretations of mental illness in CALD communities and the impact of this
15. Lack of access to services and a general underutilisation of social and mental health services in CALD
communities
Access to interpreters and culturally competent care
16. What gaps do you think exist around mental health and wellbeing in CALD communities?
17. A lack of data about CALD mental health
18. Limited understanding of perspectives of mental health and wellbeing, mental ill health and recovery
19. Broad social determinants that impact on mental health and wellbeing in CALD communities
20. Impact of merging and converging cultures on 1st, 2nd and 3rd generations of migrants
21. Limited research on the efficacy of programs that have been developed to address the needs of CALD
communities
22. What strategies or innovations have worked with CALD communities when looking at improving mental
health and wellbeing?
D. What are some of the programs that have successfully addressed these issues in CALD communities?
Explore for ‘success stories’.
© DIVERSEWERKS 48

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
23. What factors have contributed to this success – Why have they worked?
24. How can we continue to build on this success?
E. Informing the development of the NSW Mental Health Strategy
25. Overall what would you say is needed to support CALD communities’ mental health and wellbeing?
26. How can we better support CALD consumers?
27. How do we encourage CALD consumers to participate?
28. What about CALD families and carers – What do we need to do to better support them?
29. What factors need to be addressed when providing services to CALD families and carers?
© DIVERSEWERKS 49

Mental Health Commission of NSW: CALD Research to Assist Development of Draft Strategic Plan
8. Appendix 3: References
Australian Bureau of Statistics (2011). Census of population and housing.
Ide, N. Suicide among immigrants in Australia: Directions for research and prevention. Diversit-e, Issue 3, 2011. Diversity Health Institute. pp. 19-20.
Carers Australia website, ‘Culturally and linguistically diverse carers’ - http://www.carersaustralia.com.au/about-carers/culturally-and-linguistically-diverse-carers/
Department of Immigration and Border Protection ‘Settlement Reporting Facility’ – www.immi.gov.au/settlement/srf
McDonald, R., & Steel, Z. (1997). Immigrants and mental health: An epidemiological analysis. Transcultural Mental Health Centre: Sydney.
Neilssen, O., Sara, G., Lim, Y. & Large, M. (2012). Country of birth and hospital treatment for psychosis in New South Wales. Social Psychiatry and Psychiatric Epidemiology, 48 4: 613-620.
Raman, S. & Goldfeld, S. (2003) ’The health and wellbeing of children and youth in detention: What we know … what we need to know … and what we should do about it’. In Asylum seekers and refugees in Australia: Issues of mental health and wellbeing, No. 9 in Monograph Series. Ed. Barnes. D. Transcultural Mental Health Centre, Sydney, pp. 25-39.
© DIVERSEWERKS 50
Related Documents











