
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


ProlactinProlactin
Enhances breast development during pregnancy, induces lactation & binds to specific receptors in the gonads
Secretion is under tonic inhibitory control of dopamine, which acts via D2 receptors located on lactotrophs
Production can be stimulated by thyrotropin-releasing hormone (TRH) and vasoactive intestinal peptide (VIP)
Normal level in women: less than 500 mIU/L (20 ng/ml or µg/l)
Prolactin is down regulated by dopamine and is up regulated by estrogen

Prolactin LevelProlactin Level
Underlying conditionUnderlying condition PRL levelPRL level
Prolactinoma.Over 150 µg/L (five times higher than normal values)
Psychoactive drugs, estrogen, functional (idiopathic) or microadenomas
Values between normal and 100 µg/L
Macroadenomas Over 250 µg/L In some cases over 1000 µg/L
Normal PRL level
Women: below 25 µg/L - Men: below 20 µg/L

Hyperprolactinaemia ManifestationsHyperprolactinaemia Manifestations
In Women:•Disruptions of normal menstrual period (oligomenorrhea / amenorrhea)
•Hypogonadism, anovulation & Infertility
In Men:•Signs of androgen deficiency and infertility (impotence, loss of libido, and rarely gynecomastia and galactorrhea)
In both Sexes:•Galactorrhea
•Tumor mass may cause visual-field defects or headache

Osteoporosis increased with elevated PRL due to estrogen lackOsteoporosis increased with elevated PRL due to estrogen lack
If normal menses are present, osteoporosis does not occurIf normal menses are present, osteoporosis does not occur
HyperprolactinemiaHyperprolactinemiaHow frequent is it?How frequent is it?
Clinical symptoms Indicates elevated PRL in
Galactorrhea 10% of women 99% of men
Amenorrhea 15%
Galactorrhea plus amenorrhea 75%
Infertility 33%
PCO 19-50 %


Hyperprolactinemia Mechanisms on Hyperprolactinemia Mechanisms on Reproductive Dysfunction Reproductive Dysfunction
A. A. Inhibition of pulsatile GnRH secretion
B. B. Interference with gonadotropin action in ovary
C. C. Interference with estrogen positive feedback
D. D. Inhibition of progesterone synthesis
E. E. Impaired follicle development
F. F. Inhibition of 5-alpha-reductase enzyme in men, thereby
decreasing the conversion of testosterone to DHT

Hyperprolactinemia Inhibits Hyperprolactinemia Inhibits progesterone synthesis and Impairs progesterone synthesis and Impairs
follicle developmentfollicle development
• Prolactin is involved in the induction of LH receptors to maintain progesterone synthesis.
• Prolactin is necessary for complete lutenization.
• Very high prolactin level in the early phase of follicular growth inhibit progesterone secretion.
(J Endocrinol 64:555, 1975)
• If prolactin exceeds 100 ng/mL, 100% of the follicles are atretic.
(Nature 250:653 1974)

CabergamounCabergamouncabergoline 0.5 mg tabcabergoline 0.5 mg tab
More HopeMore HopeWithWith
No MoreNo MoreSufferingSuffering

Composition
Form
Pharmacological action
Preserved in
Pack
PRODUCT PROFILE
: 0.5mg cabergoline
: Scored tablets
: Prolactin Inhibitor
: PVC/PVDC strips
: One strip of 2 tablets
CabergamounCabergamoun

IS AN ERGOLINE DOPAMINE AGONIST WITH
Agonist activity on
D2 receptors
in pituitary lactotrophs
------- Potent -------
----- Selective -----
--- Long-lasting ---
As compared to bromocriptine
Cabergamoun is more potent in agonizing the D2 receptor and it occupied the receptor for longer
CabergamounCabergamoun
Prolactin is down regulated by dopamine ..

• Cabergamoun has a potent and long-lasting PRL-lowering effect by direct stimulation of D2-receptors on lactotrophs
• Cabergamoun at higher doses, has a central dopaminergic effect
• Cabergamoun single oral administration of 0.25 - 1.5 mg, produces a significant decrease in serum PRL levels.
CabergamounCabergamounPharmacodynamicsPharmacodynamics

• Cabergamoun has a prompt effect (within 3 hrs. from administration) and persists for
- Up to 7 - 28 days in hyperprolactinemic patients
- up to 14 - 21 days in puerperal women
• Cabergamoun PRL-lowering effect is dose-related in terms of degree of effect and duration of action
• Cabergamoun has a very selective action with no effect on basal secretion of other pituitary hormones or cortisol
CabergamounCabergamounPharmacodynamicsPharmacodynamics

CabergamounCabergamounPharmacokineticsPharmacokinetics
• Cabergamoun absorption and disposition is not affected by food.
• Cabergamoun is rapidly absorbed from the GIT with a peak in plasma between 0.5 and 4 hours
• Cabergamoun is 41-42% bound to plasma proteins.

CabergamounCabergamounPharmacokineticsPharmacokinetics
• Cabergamoun elimination half-life is long
- 63-68 hours in healthy volunteers
- 79-115 hours in hyperprolactinemic patients
• Ten days after administration about 18% and 72% of the dose is recovered in urine and feces, respectively
• Unchanged drug in urine accounted for 2-3% of the dose

CabergamounCabergamounTherapeutic IndicationsTherapeutic Indications
1. Inhibition of physiological lactation
2. Suppression of already established lactation
3. Treatment of dysfunctions associated wit hyperprolactinaemia: “Amenorrhoea, oligomenorrhoea, anovulation, galactorrhea
and infertility”
4. Prolactin-secreting pituitary adenomas (micro- & macroadenoma)
5. Idiopathic hyperprolactinaemia
6. Empty sella syndrome* with associated hyperprolactinaemia
7. Prevention of ovarian hyper-stimulation syndrome

CabergamounCabergamounDosage & AdministrationDosage & Administration

Indication Dose
Inhibition of lactation1mg (two tablets) given as a single dose on the first day after delivery
Suppression of established lactation
0.25 mg (half a tablet) every 12 hours for 2 days (1 mg total dose)
Amenorrhea, infertility & galactorrhea
Initial dose is 0.5 mg per weekTherapeutic dosage is usually 1 mg per week
Prevention of OHSSOne tablet daily for 8 days starting on the day of HCG injection
CabergamounCabergamounDosage & AdministrationDosage & Administration
Cabergamoun doses up to 4.5 mg per week have been used in hyperprolactinemic patients

CabergamounCabergamounNormalizes PRL level in patients with
bromocriptine resistance or intolerance
JCE&M 84(7): 2518-2522; 1999.

CabergamounCabergamounRestores gonadal function in women with
hyperprolactinemic amenorrhea
New Engl J Med. 331(14): 904-909; 1994.
More HopeMore HopeWithWith
No MoreNo MoreSufferingSuffering
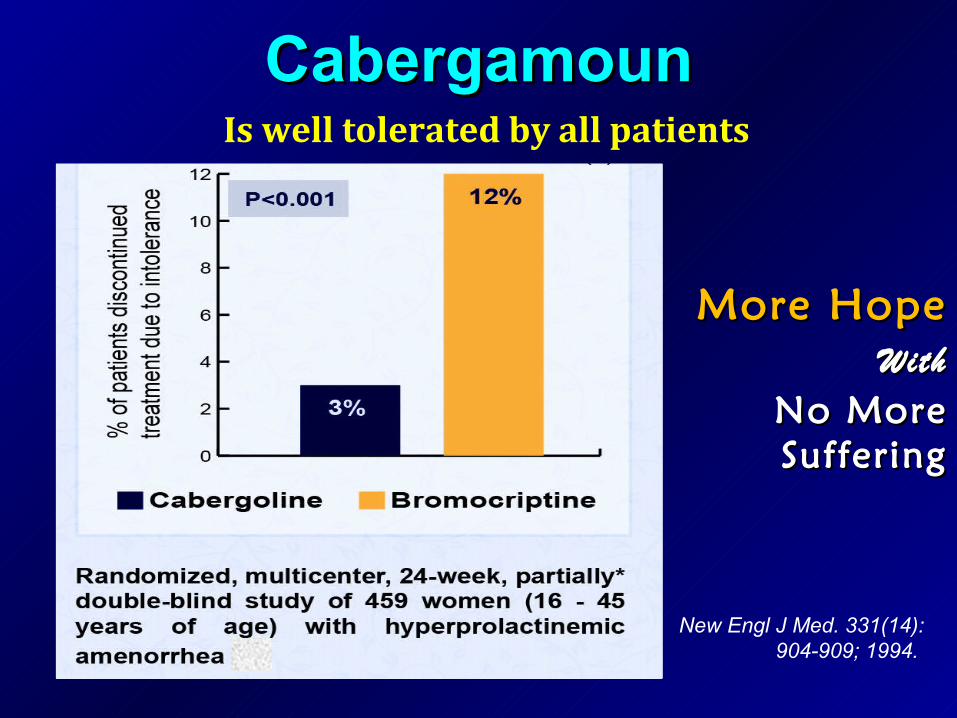
CabergamounCabergamounIs well tolerated by all patients
More HopeMore HopeWithWith
No MoreNo MoreSufferingSuffering
New Engl J Med. 331(14): 904-909; 1994.
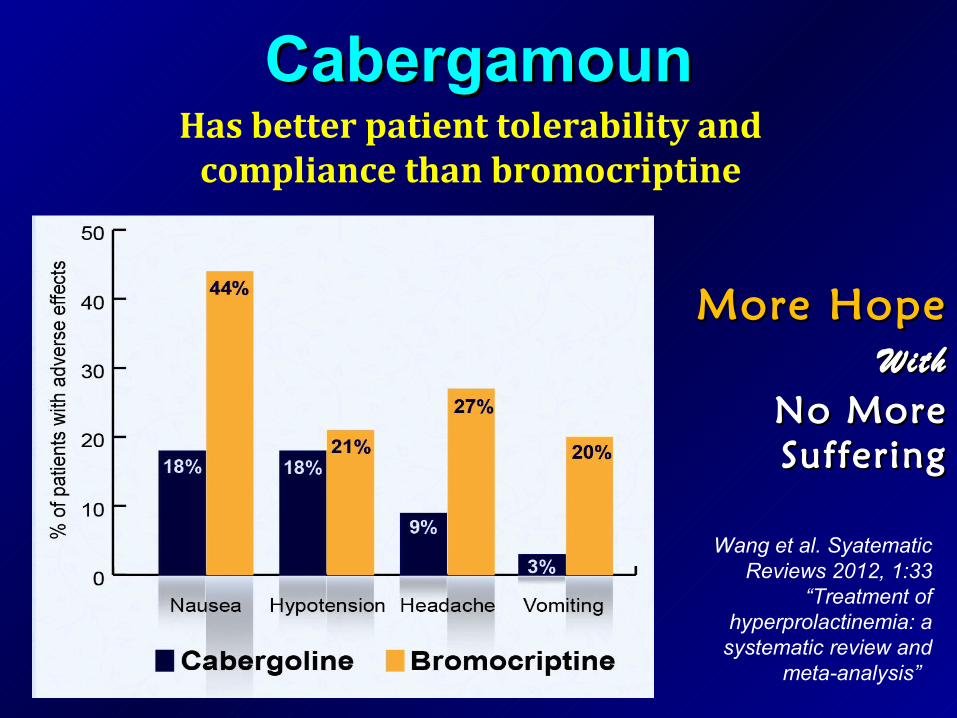
CabergamounCabergamounHas better patient tolerability and
compliance than bromocriptine
Wang et al. Syatematic Reviews 2012, 1:33
“Treatment of hyperprolactinemia: a
systematic review and meta-analysis”
More HopeMore HopeWithWith
No MoreNo MoreSufferingSuffering

PITUITARY PITUITARY ADENOMAADENOMA



Management of Pituitary AdenomaManagement of Pituitary Adenoma
SurgeryIf cabergoline is not successful, trans-
sphenoidal surgery could be considered
Radiation
Observation
Pharmacotherapy“Dopamine agonists are treatment of choice for most prolactinomas”
Cabergoline is more effective than bromocriptine
Liu, C, Tyrrell, JB. Successful treatment of a large macroprolactinoma with cabergoline during pregnancy. Pituitary 2001; 4:179.

Pharmacotherapy of ProlactinomaPharmacotherapy of Prolactinoma
• First evidence of size reduction may occur after 6 weeks
• Size reduction does not correlate with basal PRL or percentage reduction in PRL levels
• In first 2-3 years, most will re-expand
• After a few years, few re-expand

OVARIAN OVARIAN HYPERSTIMULATION HYPERSTIMULATION
SYNDROMESYNDROME
““OHSS”OHSS”


Cabergamoun
•Reduces the risk of OHSS in high-risk women
•Dose: 0.5 mg (one tablet) daily 0.5 mg (one tablet) daily
•Duration: starting on the day of HCG injectionDuration: starting on the day of HCG injection and and continue for 8 days continue for 8 days
Cabergamoun in OHSSCabergamoun in OHSS

POLYCYSTIC POLYCYSTIC OVARIAN SYNDROM OVARIAN SYNDROM
“PCO”“PCO”

Ovulatory dysfunction - PCOOvulatory dysfunction - PCO
• 20% of all women on scan
• Overweight, hirsute, oligomenorrhoea & acne
• LH/FSH raised
• Raised androgens
• Mildly raised prolactin (in 19-50% of women with PCO - may be due to the high estrogen levels present in PCO)

Cabergamoun in PCOCabergamoun in PCO
Cabergamoun
in hyperprolactinemia patients with PCO will:
– Reduces testosterone and LH levels
– Resumes ovulatory cycles.

Thank YouThank You