Laryngeal Malignancies Dr. Krishna Koirala

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Laryngeal Malignancies
Dr. Krishna Koirala

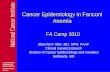
Oncological subsites of Oncological subsites of LarynxLarynx
• Supraglottis
• Epiglottis
• Aryepiglottic folds
• Ventricular bands
• Laryngeal
Ventricle
• Glottis • True vocal cords
• Anterior
commissure
• Posterior
commissure
• Subglottis

• Overview • Most common head and neck malignancy in
adults
• Accounts for 25% of head and neck cancer and 1% of all cancers
• Peak incidence : 55 - 65 years of age
• 10 : 1 male predilection
• High incidence area - Brazil, Afro- Caribbean of USA, India, France, Italy, Poland, Spain, Switzerland
• Low incidence area - Japan, Norway, Sweden

• True vocal cordTrue vocal cord :73%:73%• Aryepiglottic fold Aryepiglottic fold : 7%: 7%• False vocal cordFalse vocal cord : 5%: 5%• SubglottisSubglottis : 5%: 5%

• TypesTypes• Squamous cell carcinoma (85%)Squamous cell carcinoma (85%)• Carcinoma in situCarcinoma in situ• Verrucous carcinomaVerrucous carcinoma• Undifferentiated carcinomaUndifferentiated carcinoma• AdenocarcinomaAdenocarcinoma• Miscellaneous carcinomaMiscellaneous carcinoma• SarcomaSarcoma

• Risk factors • Tobacco
• Alcohol
• Industrial exposure
• Radiation exposure
• Laryngeal keratosis (3.25- 4.3%)
• Laryngeal papilloma - HPV 16 & 18
• GERD
• Genetic

TNM Classification of laryngeal TNM Classification of laryngeal carcinomacarcinoma UICC (1997)UICC (1997)

Supraglottis•T : Primary tumor• T is : Carcinoma in situ• T1 : Tumor limited to one subsite of
supraglottis with normal vocal cord mobility
• T2 : Tumor invades mucosa of more than one subsite of Supraglottis or glottis or region outside the supraglottis ( e.g.. mucosa of base of tongue, vallecula, medial wall of pyriform sinus) without fixation of larynx

• T3T3
• Tumor limited to larynx Tumor limited to larynx with vocal cord with vocal cord fixationfixation &/or &/or invade invade any of the following any of the following : post cricoid area, pre -: post cricoid area, pre - epiglottic epiglottic tissues, deep base of tonguetissues, deep base of tongue
• T4T4
• Tumor Tumor invades through thyroid cartilageinvades through thyroid cartilage &/or &/or extends extends into into soft soft tissues of the tissues of the neck neck , , thyroid and / or esophagusthyroid and / or esophagus

Glottis•T is : Carcinoma in situ
•T 1 : Tumor limited to the vocal cords ( may involve anterior or posterior commissure) with normal mobility
• T1a : Tumor limited to one vocal cord
• T1b : Tumor involves both vocal cords
•T2 : Tumor extends to Supraglottis & /or subglottis, and / or with impaired vocal cord mobility

• T3T3• Tumor limited to larynx Tumor limited to larynx with vocal with vocal
cord fixationcord fixation
• T4T4
• Tumor invades through thyroid Tumor invades through thyroid cartilage & /or invades other cartilage & /or invades other tissues beyond the larynx ( Eg. to tissues beyond the larynx ( Eg. to oropharynx , soft tissues of neck)oropharynx , soft tissues of neck)

SubglottisSubglottis•T isT is : Carcinoma in situ: Carcinoma in situ
•T1T1 : Tumor limited to the subglottis: Tumor limited to the subglottis
•T2T2 : Tumor extends to vocal cord (s) with : Tumor extends to vocal cord (s) with normal or impaired mobilitynormal or impaired mobility
•T3T3 : Tumor limited to larynx with vocal cord : Tumor limited to larynx with vocal cord fixationfixation
•T4T4 : Tumor invades through the cricoid or : Tumor invades through the cricoid or thyroid thyroid cartilage &/or extends to other tissues cartilage &/or extends to other tissues beyond the larynx ( eg. oropharynx, beyond the larynx ( eg. oropharynx, soft soft tissues of neck)tissues of neck)

N0N0 No cervical lymph node involvementNo cervical lymph node involvement
N1N1 Single ipsilateral lymph node ≤ 3cm Single ipsilateral lymph node ≤ 3cm
N2N2 Nodes more than 3 cm and less than 6 cmNodes more than 3 cm and less than 6 cm
N2aN2a Single ipsilateral node > 3cm and ≤6cm Single ipsilateral node > 3cm and ≤6cm
N2bN2b Multiple ipsilateral lymph nodes, each ≤ Multiple ipsilateral lymph nodes, each ≤ 6cm6cm
N2cN2c Bilateral or contralateral lymph nodes, Bilateral or contralateral lymph nodes, each each ≤6cm ≤6cm
N3N3 Single or multiple lymph nodes > 6cm Single or multiple lymph nodes > 6cm

Stage 0 T is N0 M0Stage I T1 N0 M0Stage II T2 N0 M0
Stage III T3 N0 M0
T1,T2,T3 N1 M0
Stage IV A T4 N0/N1 M0Any T N2 M0
Stage IV B Any T N3 M0
Stage IV C Any T Any N M1

Natural history •Supraglottic tumors
• More aggressive , early lymph node metastasis• Direct extension into pre-epiglottic space, glossoepiglottic
fold, and tongue base•Glottic tumors
• Grow slower and , metastasize late (lack of lymphatic drainage)
• Extend superiorly into ventricular walls or inferiorly into subglottic space
•Subglottic tumors• Uncommon• Increased chance of bilateral disease and mediastinal
extension

• History• Progressive &
continuous hoarseness
• Dyspnea & stridor• Pain and referred
otalgia• Dysphagia• Swelling in the neck• Haemoptysis
• Examination• Laryngeal crepitus• Examination of neck • Indirect
laryngoscopy• Special examination
• Flexible NPL• Videostroboscopy
Diagnosis of Laryngeal tumors

Investigations •Direct laryngoscopy and & biopsy•Panendoscopy•Contact microendoscopy and contact videoendoscopy • Using Methylene blue, toluidine blue, Lugol ‘s
iodine• Helps to delineate the extend of early lesion along
with their margin•Autoimmunofluroscence laryngoscopy• Using lung imaging fluroscence endoscope (LIFE)• Identifies differences in intensity of
autofluroscence between normal & tumor tissue when exposed to blue or violet light

• CT scan & MRI
• Helps to determine size, extent of tumor
• Pre epiglottic & paraglottic extension, anterior subglottic wedge
• Extension to thyroid cartilage, gland & strap muscle
• Positron Emission Tomography (PET)
• Useful in detecting subclinical recurrent subclinical recurrent or persisting cancer or persisting cancer at the stage of high curability


Treatment of Laryngeal cancers
• Goal of treatment
• Remove the tumor and prevent
its recurrence
• Maintain laryngeal function

• Treatment by curative intent
• Surgery ( Partial or Total Laryngectomy)
• Radiotherapy with or without Chemotherapy (5 Fluorouracil and cisplatin)
• Surgery with postoperative radiotherapy or chemotherapy
• Rehabilitation
• Palliative care

• Cordectomy • Supraglottic laryngectomy• Hemilaryngectomy
• Partial laryngectomy • Total laryngectomy and
hemithyroidectomy• Laser surgery
Surgeries performed on the larynx

Chemotherapy
A form of cancer treatment that
uses drugs to stop the growth of
cancer cells, either by killing the
cells or by stopping the cells from
dividing eg. 5 Fluorouracil and
cisplatin

Treatment of Glottic Carcinoma
•T1T2 Glottic Carcinoma
• Radiotherapy : >90% five year survival rates
• Surgical excision using laser or
endolaryngeal scissors : Similar cure rates
• Chemotherapy ( not much role)

•T3 Glottic Carcinoma
•Small tumor - cure rates in RT with
surgery and Surgery alone - similar
•Large tumor - Surgery - TL+/-neck
dissection
•Advanced Glottic Ca (T3T4N+) – Total
Laryngectomy

Treatment of Supraglottic
Laryngeal cancer
• T1/T2N0 : RT or partial Laryngectomy
• T3N0 : RT / TL
• N1 : RT - controversial

Treatment of Subglottic tumors
•Total Laryngectomy and partial thyroidectomy
•T1 and T2 RT + f/u and salvage surgery
•Advanced disease/recurrence/cervical
lymphadenopathy Extended TL, ND + post op
RT

Curative treatment of squamous cell carcinoma Curative treatment of squamous cell carcinoma of larynxof larynx
Glottis N0 N1 N2 N3
T1
T2T3T4
RT,?ELS (cordectomy for recurrence)RT, Hemilaryngectomy or TL + ?RT?RT, ?surgery (STL or TL +?RT)TL + RT
NA or surgery
TL + ?RTTL + ?RTTL + RT
NA or surgery
NA or surgeryTL + RTTL + RT
NA or surgery
NA or surgeryTL + RTTL + RT
Supraglottis N0 N1 N2 N3
T1T2T3T4
RT or endolaryngeal surgeryRT or surgery (SGL or TL) +?RT?RT or surgery (SGL or TL) +?RTSurgery + RT
SGL +?RTSGL or TL + ?RTSGL or TL + ?RTTL + RT
SGL + RTSGL or TL+RTSGL or TL+RTTL + RT
NATL + RTTL + RTTL + RT
Subglottis N0 N1 N2 N3
T1T2T3T4
RadiotherapyRadiotherapy or surgery (TL)Surgery (TL) + ?RTSurgery (TL) + RT
TL + ?RTTL + ?RTTL + ?RTTL + RT
TL + RTTL + RTTL + RTTL + RT
TL + RTTL + RTTL + RTTL + RT

Recent advances in treatment
• Chemoprevention : The use of drugs,
vitamins, or other substances to reduce the
risk of developing cancer or to reduce the
risk cancer will recur ( eg. Isotretinoin )
• Radiosensitizers : Drugs that make tumor
cells more sensitive to radiation

Palliative Care •To ameliorate symptoms
•Used in later stages of diseaseUsed in later stages of disease
•RT/Chemo/analgesicsRT/Chemo/analgesics
•TracheostomyTracheostomy
•Intensive supports to family and Intensive supports to family and friendsfriends

Vocal rehabilitation after Vocal rehabilitation after laryngectomylaryngectomy• Esophageal speech
• Taught to swallow air & hold• Can speak 6-10 words per breath• Voice is rough, loud and understandable
• Artificial larynx• Electrolarynx• Transoral pneumatic device
• Tracheo-esophageal speech• Creation of skin-lined fistula or artificial
prosthesis• Air carried from trachea to oesophagus• Blom-Singer or Panje prosthesis

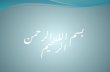
Esophageal speech
• Air is forced into the top of the esophagus and is expelled out through the mouth
• Air movement vibrates the esophageal wall to create the sound

ElectrolarynxElectrolarynx
Related Documents