CHAPTER 11 Occlusion and Temporomandibular Disorders Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

C HAPTER 11 Occlusion and Temporomandibular Disorders Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CHAPTER 11
Occlusion and Temporomandibular Disorders Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

INTRODUCTION
The masticatory system is a complex apparatus with an adaptive capacity to function. When that adaptive capacity is exceeded,
dysfunction can range from discomfort to debilitating pain.
Temporomandibular disorders (TMDs) occur as a result of problems with the masticatory system.
2
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
BIOLOGICAL BASIS OF OCCLUSAL FUNCTION
The oral cavity in occlusal function (during talking, chewing, and swallowing) is in a dynamic (ever-changing) state rather than in a static state.
Orthofunction (physiologic occlusion) is a state in which the masticatory forces are within an adaptive physiologic range. In orthofunction, no pathologic changes occur in
the oral tissues.
3
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BIOLOGICAL BASIS OF OCCLUSAL FUNCTION (CONT.)
Dysfunction is a state of morphofunctional disharmony in which the forces during function cause pathologic changes in the tissues. These changes result in abnormal function or
pain. The degree of dysfunction can be slight, with no
great disturbance to the patient; or the degree of dysfunction can be significant, making daily activity difficult or impossible.
4
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
BIOLOGICAL BASIS OF OCCLUSAL FUNCTION (CONT.)
In normal function, axial forces directed along the tooth and periodontium meet functional demands.
Parafunctional activity, such as grinding or clenching, can stress this system.
Antiaxial forces directed along the tooth and periodontium can cause resorption or a hypertrophic response. Some areas will break down, whereas other
areas will not show any injury.
5
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BIOLOGICAL BASIS OF OCCLUSAL FUNCTION (CONT.)
Certain factors affect the response of the teeth and periodontal structures to normal and abnormal function. These factors include the size and shape of the
roots, the quantity and quality of the alveolar bone, and the presence of microbial plaque biofilm.
Oral habits and/or missing or shifting teeth can also increase force on the teeth.
When periodontal disease has weakened the periodontium, these forces may exceed the individual’s adaptive capability, causing injury.
6
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BIOLOGICAL BASIS OF OCCLUSAL FUNCTION (CONT.)
When the condyles rest in a normal closed superoanterior position, the mandible has a well-distributed and even contact with the maxilla.
The masticatory system can tolerate a certain amount of functional change known as hyperfunction.
When functional changes exceed a certain level, alteration to the tissues may begin. This structural breakdown will vary, depending
on the individual and systemic and local factors.7
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TRAUMA FROM OCCLUSION
A traumatic occlusion is an occlusion that has caused injury to the teeth, the muscles, or the temporomandibular joint (TMJ).
A classification of primary traumatic occlusion is made when heavy occlusal forces cause injury to tissues and bone.
A classification of secondary traumatic occlusion is made when normal occlusal forces exceed the capability of a periodontium that is already affected by periodontal disease.
8
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TRAUMA FROM OCCLUSION (CONT.)
Traumatic occlusion does not refer to a malocclusion as described by Angle’s three classifications. Angle’s Class I, II, and III occlusions classify and
describe the skeletal relationship of the maxillary to the mandibular teeth.
The occlusal relationship of the teeth is not a predictor of pain or problems in the TMJ.
9
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TRAUMA FROM OCCLUSION (CONT.)
Trauma associated with orthodontic movement of teeth is self-limiting. Self-limiting means that mobility is greater than
normal but is handled through periodontal adaptation without causing trauma from occlusion.
10
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TRAUMA FROM OCCLUSION (CONT.)
True trauma from occlusion, that is, trauma that exceeds the adaptive capacity of the periodontium, increases bone loss and pocket depth formation. Trauma from occlusion may occur with bruxism
in a patient with periodontal disease.
11
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TRAUMA FROM OCCLUSION (CONT.)
Open or faulty contacts between teeth can cause areas of food impaction. Impaction is the forceful wedging of food into the
periodontium by occlusal forces. It can be a contributing factor in periodontal disease.
In the past, recession, clefting, or thickening of the gingival margin were thought to be caused by trauma from occlusion. Research has not supported these causative
relationships.
12
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TEMPOROMANDIBULAR DISORDERS
TMDs are a grouping of musculoskeletal conditions that produce pain or dysfunction in the masticatory system. When the muscles, not the joint, are involved,
the condition is referred to as extracapsular. A problem occurring within the TMJ is known as
intracapsular.
13
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CAUSES OF TEMPOROMANDIBULAR DISORDERS
The cause of TMDs is multifactorial. Stress is often a factor. Arthritis and psychologic problems can also be
involved. A history of macrotrauma or microtrauma may
exist. Macrotrauma is a single event. Microtrauma is a number of minor
habits or events.
14
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

CATEGORIES OF TEMPOROMANDIBULAR DISORDERS
Four main diagnostic categories for TMD are listed:
1. Muscle and fascial disorders of the masticatory system
This group includes myalgia, trismus, spasm, dyskinesia, bruxism, and other muscle disorders.
2. Internal derangements that impair mechanical function of the TMJ
Arthritis conditions
15
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
CATEGORIES OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Four main diagnostic categories for TMD: (cont.)
3. Disorders of mandibular mobility This group includes ankylosis, muscular fibrosis,
internal derangement, and adhesions in the joint.
4. Disorders of maxillomandibular growth Neoplastic and nonneoplastic conditions Less common disorders
16
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

ORAL HABITS
Oral habits can contribute to periodontal and dental damage in the oral cavity. The amount of damage is related to the intensity
and duration of the habit. Oral habits are repetitive masticatory
activities outside the normal range of function and can involve tooth-to-tooth contact or contact with foreign objects.
These habits can lead to tooth damage, muscular hypertrophy, muscular pain and tenderness, and periodontal tissue injury.
17
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BRUXISM
Bruxism is the most frequently described oral habit.
This oral habit is described as the clenching or grinding of the teeth when the individual is not chewing or swallowing.
Bruxism can occur as rhythmic side-to-side movements or through a sustained clench.
Clenching is the continuous or intermittent closure of the jaws under vertical pressure.
Grinding and clenching are parafunctional habits that are involuntary and may be destructive.
18
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BRUXISM (CONT.)
Bruxism is classified into one of two categories: Nocturnal (nighttime) Diurnal (daytime)
The results of bruxism may be tooth wear, tooth fracture, restoration fracture, myalgia, hypertrophy of the masticatory muscles, and headache. The presence of wear facets that are not caused
by masticatory function are indicative of tooth wear.
19
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BRUXISM (CONT.)
Bruxism treatments include: Occlusal splints Pharmacologic therapy Physical therapy Behavioral modification therapy
20
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BRUXISM (CONT.)
Bruxism can be a significant problem with patients who have advanced loss of periodontal support as demonstrated in the following figure.
21
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

BRUXISM (CONT.)
22
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
SIGNS AND SYMPTOMS OF TEMPOROMANDIBULAR DISORDERS
Four primary symptoms are commonly reported in patients with TMDs and include the following: 1. Pain and tenderness in the muscles of
mastication2. Pain and tenderness in the TMJ3. Painful clicking of the joint during function4. Limitation of mandibular motion
23
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
SIGNS AND SYMPTOMS OF TEMPOROMANDIBULAR DISORDERS (CONT.)
A number of additional symptoms are found in patients with TMDs: Uncomfortable bite Incoordination of the jaw (dyskinesia) Ringing in the ears Muscle swelling
In the dentition, signs include tooth wear, tooth mobility, and pulpitis.
24
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

SIGNS AND SYMPTOMS OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Pain in the masticatory muscles (myalgia) is the most common symptom reported by patients with a muscle disorder.
Myalgia pain is usually dull, aching, and continuous or recurrent.
A reduction in mandibular function, usually the inability to open the mouth widely, is associated with muscle pain.
25
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

SIGNS AND SYMPTOMS OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Tenderness or pain in the TMJ (arthralgia) is another common finding in TMDs.
The pain arises from the soft tissues surrounding the joint because the articular surfaces of the joint are not innervated.
Arthralgic pain is sharp, sudden, and associated with the jaw in function.
26
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

SIGNS AND SYMPTOMS OF TEMPOROMANDIBULAR DISORDERS (CONT.)
A common dysfunction observed in the TMJ is a joint sound caused by a disruption of the normal movement of the condyle and articular disk in the joint. A single sound is known as a click or a pop. A grating sound is known as crepitus.
27
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

SIGNS AND SYMPTOMS OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Other inflammatory joint disorders include osteoarthritis and polyarthritis. The pain of these disorders in the TMJ is dull,
aching, and constant, and is increased with function.
28
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

SCREENING FOR TEMPOROMANDIBULAR DISORDERS
A TMD screening examination will lead to one of three conclusions:
1. The jaw system is in orthofunction; no contraindications to proceeding with dental hygiene treatment are revealed.
2. Problems exist in the jaw system; dental hygiene and dental treatment should proceed with caution, and the patient should be informed.
3. The patient should be referred for a comprehensive evaluation before any dental hygiene or dental treatment is administered.
29
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

SCREENING FOR TEMPOROMANDIBULAR DISORDERS (CONT.)
The screening examination has subjective and objective components.
The subjective component is a series of questions that the patient is asked while the medical history is taken or during the examination of the oral cavity.
The clinician completes the objective portion; it is divided into the assessment of clinical jaw function and the assessment of occlusion.
30
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MUSCLE PALPATION
The temporalis and masseter muscles are bilaterally examined by palpating the origin, body, and insertion of the muscle.
Gentle finger pressure along the muscle, lasting a few seconds, is applied. This pressure may elicit a response from the
patient. The patient should be instructed to
differentiate pressure from pain.
31
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MUSCLE PALPATION (CONT.)
The muscle palpation examination is illustrated in the following figure.
32
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MUSCLE PALPATION (CONT.)
33
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MANDIBULAR MOVEMENT
The normal opening and closing of the jaw should be smooth and symmetrical. The patient should be able to achieve a
minimum of a 40 mm opening distance. If the clinician can passively increase the
interincisal distance for a patient, that is, use the thumb and finger to open the jaw wider, then a muscular problem may exist.
34
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MANDIBULAR MOVEMENT (CONT.)
The interincisal opening (incisal edge to incisal edge) is measured after the patient is asked to open the mouth as wide as possible as illustrated in the following figure.
35
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MANDIBULAR MOVEMENT (CONT.)
36
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MANDIBULAR MOVEMENT (CONT.)
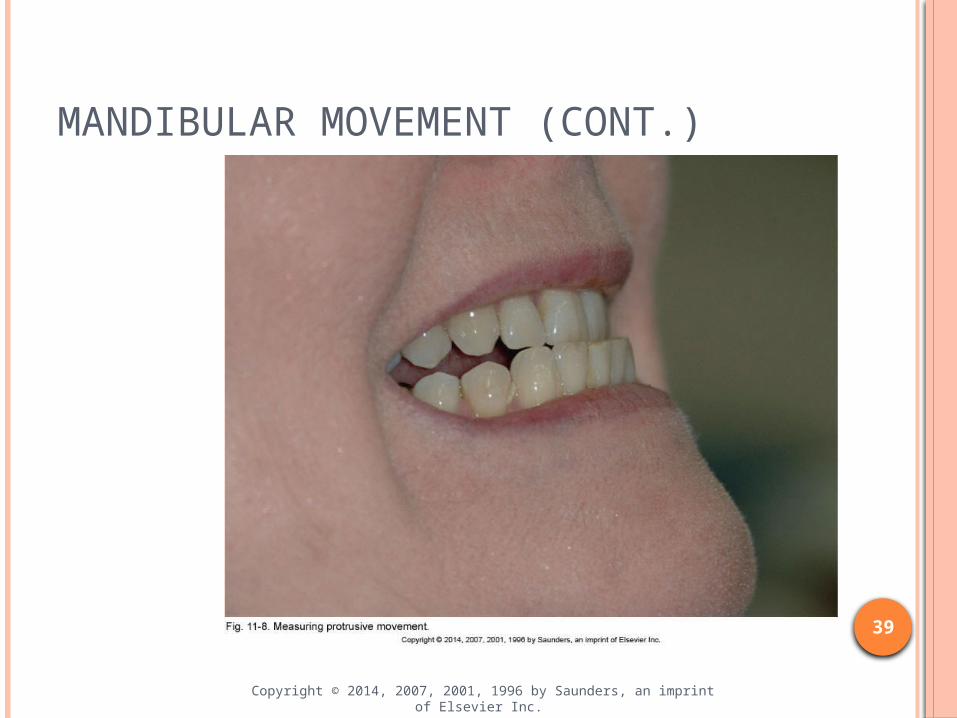
The normal mandibular movement from side to side and forward, with the teeth not in contact, should be approximately 8 mm.
37
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

MANDIBULAR MOVEMENT (CONT.)
The left lateral, right lateral, and protrusive movements are demonstrated in the following figure.
38
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
MANDIBULAR MOVEMENT (CONT.)
39
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
JOINT FUNCTION
Opening and closing should be observed for any alteration from the midline. A deviation is a shift in the midline during
opening that disappears later in the opening movement.
Interference in the disk of the joint may cause this deviation.
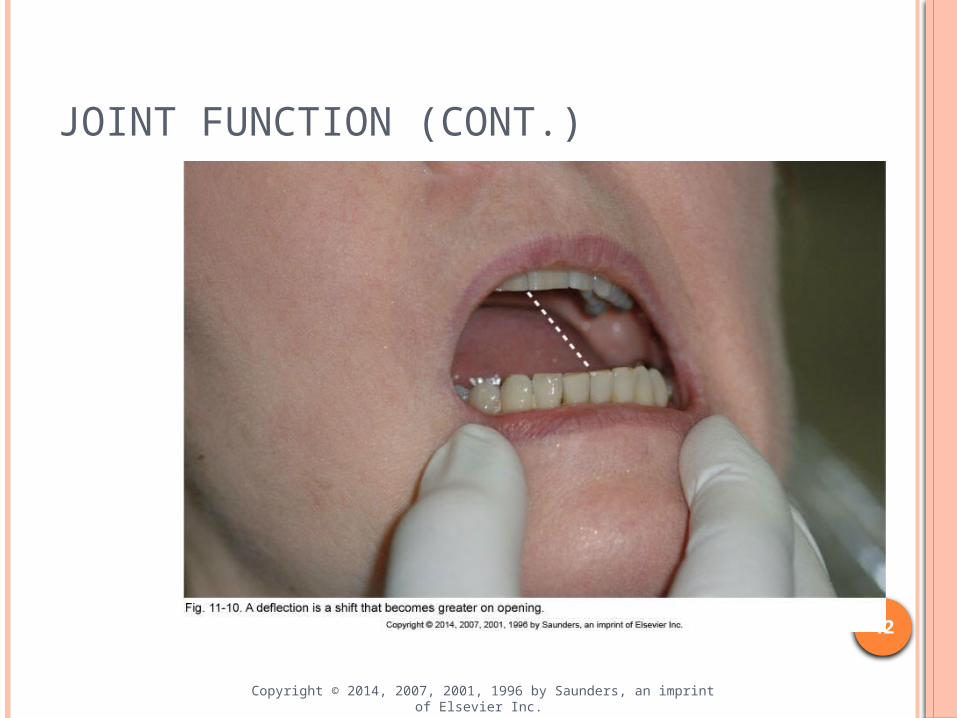
A deflection is a shift in the midline that becomes greater as opening continues.
A restriction in one joint causes a deflection.
40
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

JOINT FUNCTION (CONT.)
The joint function movements are demonstrated in the following figure.
41
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
JOINT FUNCTION (CONT.)
42
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
JOINT SOUNDS
On opening, the condyle and disk of the TMJ move forward (anteriorly) to the articular eminence.
If a sound is elicited, then it is either a click or crepitus. A click is a short sound. Crepitus is a grating sound.
A sound that occurs on opening and closing is called a reciprocal click.
43
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

JOINT SOUNDS (CONT.)
The examination of joint sounds is demonstrated in the following figure.
44
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

JOINT SOUNDS (CONT.)
45
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
INTERCUSPAL POSITION
The normal position of the teeth in maximum intercuspation is called centric occlusion. A normal position should be a well-distributed
pattern of occlusal contact. The posterior teeth should have firm, even
contact. The anterior teeth may have only light or no
contact.
46
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

INTERCUSPAL POSITION (CONT.)
To evaluate anterior contact, polyester film (Mylar) or occlusal indicator (shim stock) paper is placed between the teeth at small intervals.
The patient is asked to close and hold on the Mylar while the operator tugs slightly outward. If the Mylar strip holds, then contact exists. If the Mylar strip slips through the teeth, then no
contact exists.
47
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

INTERCUSPAL POSITION (CONT.)
The presence or absence of intercuspation contact should be noted for the incisors, canines, premolars, and molars on the right and left sides of the mouth as demonstrated in the following figure.
48
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
PROTRUSIVE, LATERAL, AND MEDIAL EXCURSIVE MOVEMENTS
Lateral movement of the jaw is examined starting from the intercuspal position.
The patient protrudes the jaw as far as possible and moves the jaw toward the right shoulder and then toward the left shoulder.
A supracontact (high spot) is an area on a tooth that prevents well-distributed stable contact between the maxillary and the mandibular teeth.
49
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PROTRUSIVE, LATERAL, AND MEDIAL EXCURSIVE MOVEMENTS (CONT.)
Medial movement is also examined starting from the intercuspal position.
Mylar film is placed between the molars on the right side and the patient moves the jaw 2 mm toward the opposite side. If the Mylar does not hold, then no contact
exists. If it holds, then a mediotrusive contact exists.
This test is repeated on the left side.
50
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
PROTRUSIVE, LATERAL, AND MEDIAL EXCURSIVE MOVEMENTS (CONT.)
The test for medial movement is illustrated in the following figure.
51
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

PROTRUSIVE, LATERAL, AND MEDIAL EXCURSIVE MOVEMENTS (CONT.)
52
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTH MOBILITY AND WEAR
Slight mobility of the teeth, especially the lower incisors, is normal.
This ability to move is called physiologic mobility and occurs because the conical roots of single-rooted teeth are suspended in the periodontal ligament, which allows them to move very slightly.
53
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTH MOBILITY AND WEAR (CONT.)
A classification of primary traumatic occlusion is made when heavy occlusal forces exceed the adaptive range in a normal periodontium.
A classification of secondary traumatic occlusion is made when normal occlusal forces exceed the capability of a periodontium that is affected by periodontal disease.
The visible and palpable movement of a tooth during function or parafunction is called fremitus. 54
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTH MOBILITY AND WEAR (CONT.)
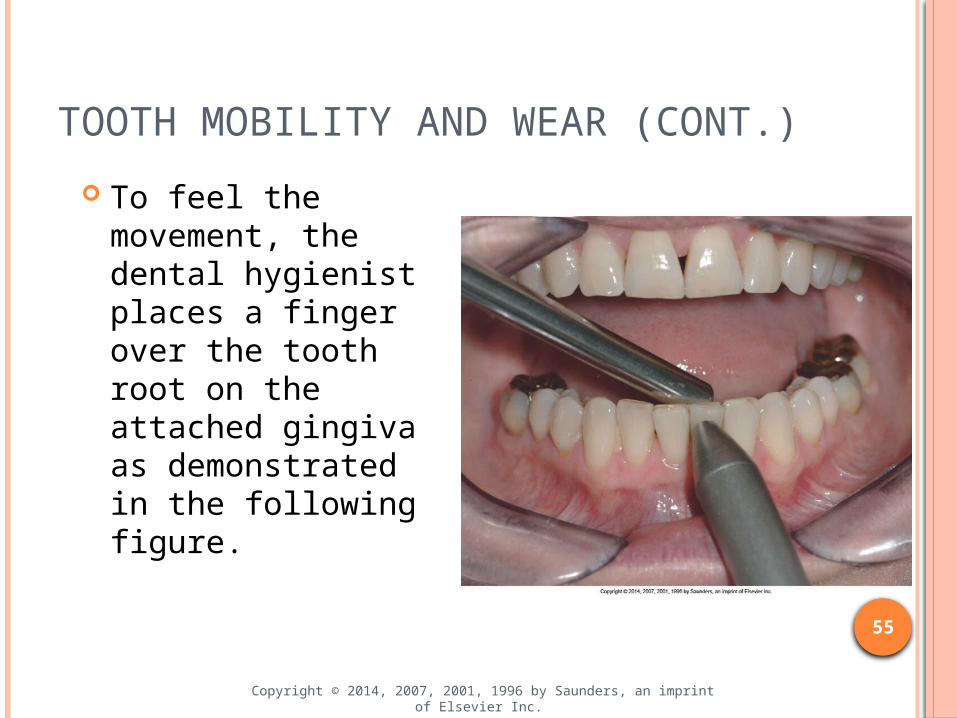
To feel the movement, the dental hygienist places a finger over the tooth root on the attached gingiva as demonstrated in the following figure.
55
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTH MOBILITY AND WEAR (CONT.)
Wear caused by tooth-to-tooth contact is called attrition.
A facet is a type of attrition where the tooth surface is worn by functional or parafunctional causes. A facet is smooth and shiny as a result of the
enamel rods that become fractured and polished. Shiny facets are known as active facets.Nonshiny or velvetlike facets are termed passive facets.
56
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TOOTH MOBILITY AND WEAR (CONT.)
When the facet is angular, the occlusal forces are directed laterally and increase the risk of periodontal injury.
To determine whether the wear is from functional or parafunctional use, the dental hygienist asks the patient to close his or her mouth and then observes the position of the mandible.
If an occlusal pattern for the wear cannot be established, then other factors must be considered.
57
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TOOTH MOBILITY AND WEAR (CONT.)
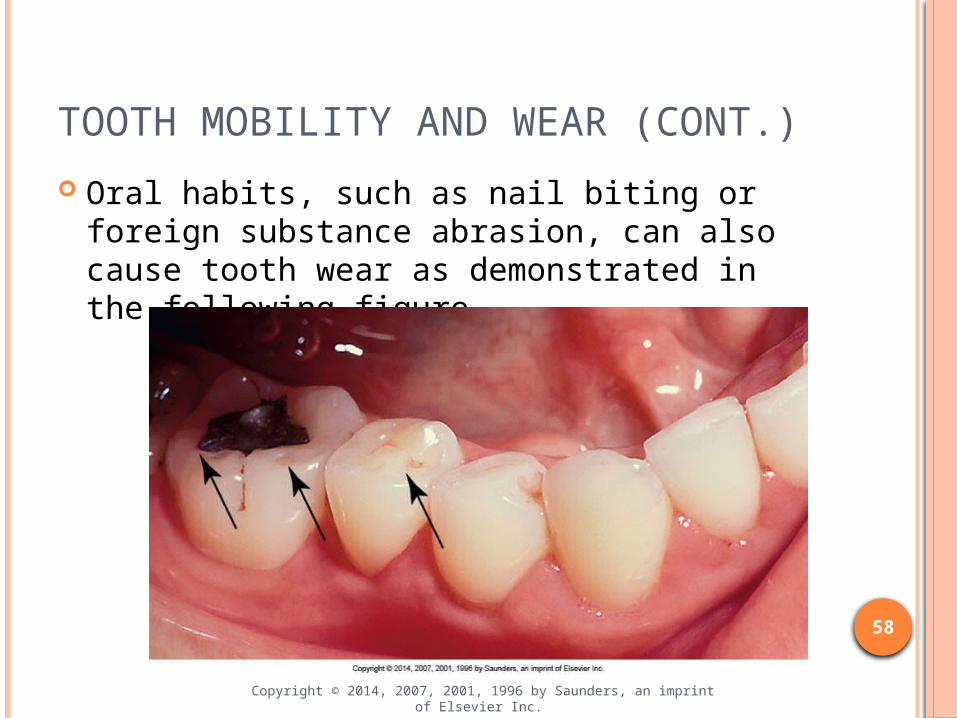
Oral habits, such as nail biting or foreign substance abrasion, can also cause tooth wear as demonstrated in the following figure.
58
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RADIOGRAPHIC EVALUATION
Changes observed in periapical radiographic images include: Widening of the periodontal ligament
This is caused by the resorption of bony support from excessive occlusal forces.
Increased density of the surrounding bone (osteosclerosis)
Increased cementum at the apical areas of the root (hypercementosis) Osteosclerosis and hypercementosis are hypertrophic responses to occlusal forces. 59
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RADIOGRAPHIC EVALUATION (CONT.)
Examples of these changes in conditions are demonstrated in the following figure.
60
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RADIOGRAPHIC EVALUATION (CONT.)
61
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

RADIOGRAPHIC EVALUATION (CONT.)
A temporomandibular screening form is demonstrated in the following figure.
62
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT OF TEMPOROMANDIBULAR DISORDERS
Three criteria are used as guidelines for selecting a TMD treatment:
1. Corrects the differential diagnosis2. Is selected with reason and purpose3. Is directed toward eliminating or neutralizing the
cause of the symptoms
63
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
A commonly used approach is conservative, using simple, noninvasive methods.
Initial therapy consists of a soft diet, limited movement of the jaw, application of moist heat to the affected area, and a nonnarcotic analgesic. Stronger drugs may be prescribed if symptoms
do not respond to the nonnarcotic analgesic agents.
Patients frequently improve after 2 to 3 weeks of initial therapy. 64
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Home Therapy Home therapy includes a soft diet, heat or ice
packs, nonnarcotic analgesics, rest, and some jaw movement exercises. The jaw movement exercises are demonstrated
to the patient, and a daily program is recommended.
The exercises both relax and stretch the sore muscles to enable them to regain their original function.
65
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Physical Therapy Physical therapy treatments include:
Ultrasound Massage Electrical stimulation of the muscles Soft-tissue manipulation Exercise programs
66
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Occlusal Appliances Occlusal appliances are made of hard acrylic
resin. They fit over the occlusal and incisal surfaces
of the maxillary or mandibular teeth. The appliance may be called a splint, night
guard, or bite guard. An occlusal appliance protects the teeth and
provides a stable position for them.
67
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Occlusal Adjustment Limited occlusal adjustment may be
appropriate in some patients, but it is rarely considered a primary treatment for TMDs.
Behavioral Therapy Behavioral methods include:
Stress or anxiety counseling Depression counseling Psychiatric therapy
68
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Pharmacologic Therapy Groups of medications prescribed include:
Analgesic medications Antianxiety drugs Antiinflammatory agents Muscle relaxants Local anesthetic medications
Administered orally or by injection
69
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Surgical Therapy Arthroscopic and arthrocentesis surgeries
can help patients with acute TMJ derangement–induced hypermobility to gain a full range of jaw motion.
A condylectomy (removal of the condyle), which is more extensive than a condylotomy (partial removal), may be indicated for severe TMJ growth disturbances or tumors.
70
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

TREATMENT OF TEMPOROMANDIBULAR DISORDERS (CONT.)
Irreversible Treatments Irreversible treatments for TMD, such as
surgery to the joint or disk, are permanent alterations. Surgical treatments are indicated only in a small
percentage of patients. Occlusal adjustment is irreversible, and no
evidence suggests that this approach is effective.
71
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.

DENTAL HYGIENE APPOINTMENT
The patient with TMD requires a series of short dental hygiene appointments, rather than one long appointment, to minimize trauma to the masticatory muscles and joint.
The use of a bite-block to maintain the oral opening is one alternative for a patient with a history of jaw pain and fatigue.
The use of a toothbrush with a small head or the use of other interdental cleaning devices can simplify daily oral hygiene care for patients with limited opening.
72
Copyright © 2014, 2007, 2001, 1996 by Saunders, an imprint of Elsevier Inc.
Related Documents











