www.onlinejacc.org 中文版 /CHINESE EDITION 原创性研究 2018 年 12 月 第3期 ELSEVIER ISSN 0735-1097 1 比伐卢定或肝素在行介入治疗的急性冠脉综合征 患者中的应用 Giuseppe Gargiulo, Greta Carrara, et al ■ 点评 韩雅玲 李洋 13 双联抗血小板治疗评分在瑞典全国人群中的外部 验证 Peter Ueda, Tomas Jernberg, et al ■ 点评 高展 窦克非 徐波 23 急性冠脉综合征患者行完全血运重建与单纯罪犯 血管血运重建的对比研究 Krishnaraj S. Rathod, Sudheer Koganti, et al ■ 点评 于波 代建南 34 伴或不伴心力衰竭患者的 B 型钠尿肽水平和死亡率 Michelle K. York, Deepak K. Gupta, et al ■ 点评 韩雅玲 李洋 43 外科与经皮冠脉血运重建治疗后卒中的发生率 Stuart J.Head, Milan Milojevic, et al ■ 点评 陈纪言 冯颖青 何旭瑜 55 与 2017 年 ACC/AHA 高血压指南定义的 1 期高 血压相关的长期心血管疾病风险 Yue Qi, Xueyu Han, et al ■ 点评 陈绍良

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.onlinejacc.org
中文版 /CHINESE EDITION
原创性研究
2018 年 12 月第 3 期
ELSEVIERISSN 0735-1097
1 比伐卢定或肝素在行介入治疗的急性冠脉综合征
患者中的应用
Giuseppe Gargiulo, Greta Carrara, et al
■ 点评 韩雅玲 李洋
13 双联抗血小板治疗评分在瑞典全国人群中的外部
验证
Peter Ueda, Tomas Jernberg, et al
■ 点评 高展 窦克非 徐波
23 急性冠脉综合征患者行完全血运重建与单纯罪犯
血管血运重建的对比研究
Krishnaraj S. Rathod, Sudheer Koganti, et al
■ 点评 于波 代建南
34 伴或不伴心力衰竭患者的B型钠尿肽水平和死亡率
Michelle K. York, Deepak K. Gupta, et al
■ 点评 韩雅玲 李洋
43 外科与经皮冠脉血运重建治疗后卒中的发生率
Stuart J.Head, Milan Milojevic, et al
■ 点评 陈纪言 冯颖青 何旭瑜
55 与 2017 年 ACC/AHA高血压指南定义的 1期高
血压相关的长期心血管疾病风险
Yue Qi, Xueyu Han, et al
■ 点评 陈绍良

该翻译由中国译者负责并由中国总编辑独自负责修订。Elsevier 或美国心脏病学会基金会不对翻译承担任何责任。尽管翻译过程十
分仔细,但读者必须始终依靠自己的经验和知识来评估和应用本出版物中的所有信息,并始终使用原始来源对其进行检查。对于使
用本出版物中的任何信息和 / 或任何错误、遗漏或不准确信息(无论出于疏忽或其他原因造成的)后产生的后果,译者或中国版主
编不承担任何责任。
从业人员和研究人员必须始终依靠自己的经验和知识来评估和应用本刊所述的任何信息、方法、化合物或试验。由于医学科学的迅
速发展,尤其应对诊断和药物剂量进行独立核查。 在法律覆盖的最大范围内,Elsevier、美国心脏病学会基金会、译者或中国版主
编不对因以下问题导致的人身伤害和 / 或损害承担任何责任:所有产品质量责任、疏忽或其他方面的问题;应用或操作本文材料中
包含的任何方法、产品、说明或想法产生的问题。虽然所刊广告均符合道德(医疗)标准,但本出版物中的内容并不构成对该产品
质量或价值及其制造商声称的内容的保证或认可。
The translation has been undertaken by the Chinese translator and revised by the Chinese Editor-in-Chief at their sole responsibility. No responsibility is assumed by Elsevier or the American College of Cardiology Foundation in relation to the translation. Although much care has been taken in performing the translation, readers must always rely on their own experience and knowledge in evaluating and using any information in this publication, and must always check it with original sources. No responsibility is assumed by the translator or the Editor-in-Chief of the Chinese edition in relation to the use of any information in this publication and/or any error, omission, or inaccuracies, whether arising from negligence or otherwise, or for any consequences arising thereafter.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, the American College of Cardiology Foundation, the translator or the Editor-in-Chief of the Chinese edition for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein. Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of It by its manufacturer.

EDITOR-IN-CHIEF
Valentin Fuster, MD, PhD,New York, NY
EXECUTIVE EDITORJagat Narula, MD, PhD, New York, NY
DEPUTY EDITOR
Jonathan L. Halperin, MD,New York, NY
GUEST EDITORSDeepak L. Bhatt, MD, MPH,Boston, MA
P.K. Shah, MD, Los Angeles, CA
VICE PRESIDENT, PUBLISHINGKimberly Murphy,Washington, DC
EDITORIAL DIRECTOR
Justine Varieur Turco, Washington, DC
INTERNATIONAL ADVISORS
Jane Armitage, FRCP,Oxford, United Kingdom
Edimar A. Bocchi, MD,Sao Paulo, Brazil
Antonio Colombo, MD,Milan, Italy
Gerd Heusch, MD, PhD,Essen, Germany
Chang-Sheng Ma, MD,Beijing, China
Gilles Montalescot, MD, PhD, Paris, France
José C. Nicolau, MD, PhD,Sao Paulo, Brazil
Han Ya-Ling, MD, PhD, Shenyang, China
中文版/CHINESE EDITION
主编 / Editor-in-Chief韩雅玲 / Yaling Han
单位 / Affiliation沈阳军区总医院 / PLA Shenyang General Hospital
副主编(按姓氏拼音排序)
编 委(按姓氏拼音排序) Editorial Board Members(Sequenced by family names)
Social Media Editor Dr. Mingyu Sun社交媒体编辑 孙鸣宇
Jiannan Dai The Second Affiliated Hospital of Harbin Medical University
Kefei Dou Fuwai Hospital,CAMS
Yingqing Feng Guangdong General Hospital
Zhan Gao Fuwai Hospital,CAMS
Jing Li Xuanwu Hospital, Capital Medical University
Yang Li PLA Shenyang General Hospital
Yi Li PLA Shenyang General Hospital
Zhizhong Liu Nanjing First Hospital Affiliated to Nanjing Medicine University
Xiao Wang Beijing Anzhen Hospital, Capital Medical University
Lei Xing The Second Affiliated Hospital of Harbin Medical University
Junqing Yang Guangdong General Hospital
Junjie Zhang Nanjing First Hospital Affiliated to Nanjing Medicine University
Jiyang Chen Guangdong General Hospital
Shaoliang Chen Nanjing First Hospital Affiliated to Nanjing Medicine University
Shaoping Nie Beijing Anzhen Hospital, Capital Medical University
Bo Xu Fuwai Hospital,CAMS
Bo Yu The Second Affiliated Hospital of Harbin Medical University
Associate Editors(Sequenced by the family names)
陈纪言 广东省人民医院陈绍良 南京市第一医院聂绍平 首都医科大学附属北京安贞医院徐 波 中国医学科学院阜外医院于 波 哈尔滨医科大学附属第二医院
代建南 哈尔滨医科大学附属第二医院窦克非 中国医学科学院阜外医院冯颖青 广东省人民医院高 展 中国医学科学院阜外医院李 静 首都医科大学附属宣武医院李 洋 沈阳军区总医院李 毅 沈阳军区总医院刘志忠 南京市第一医院王 晓 首都医科大学附属北京安贞医院邢 磊 哈尔滨医科大学附属第二医院杨峻青 广东省人民医院张俊杰 南京市第一医院
~
~


JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY ©2018 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
VOL. 71, NO. 11, 2018ISSN 0735-1097
PUBLISHED BY ELSEVIER
比伐卢定或肝素在行介入治疗的急性冠脉综合征患者中的应用Bivalirudin or Heparin in Patients Undergoing Invasive Management of Acute Coronary Syndromes
Giuseppe Gargiulo, MD,a,b Greta Carrara, STAT,c Enrico Frigoli, MD,a Pascal Vranckx, MD, PHD,d Sergio Leonardi, MD, MHS,e Nestor Ciociano, PHARMD,f Gianluca Campo, MD, PHD,g,h Ferdinando Varbella, MD,i Paolo Calabrò, MD, PHD,j Stefano Garducci, MD,k Alessandro Iannone, MD,l Carlo Briguori, MD, PHD,m Giuseppe Andò, MD, PHD,n Gabriele Crimi, MD,d,o Ugo Limbruno, MD,p Roberto Garbo, MD,q Paolo Sganzerla, MD,r Filippo Russo, MD,s Alessandro Lupi, MD,t Bernardo Cortese, MD,u,v Arturo Ausiello, MD,w Salvatore Ierna, MD,x Giovanni Esposito, MD, PHD,b Dennis Zavalloni, MD,y Andrea Santarelli, MD,z Gennaro Sardella, MD,aa Simone Tresoldi, MD,bb Nicoletta de Cesare, MD,cc Alessandro Sciahbasi, MD, PHD,dd Antonio Zingarelli, MD,ee Paolo Tosi, MD,ff Arnoud van ’t Hof, MD, PHD,gg Elmir Omerovic, MD,hh Salvatore Brugaletta, MD,ii Stephan Windecker, MD,a Marco Valgimigli, MD, PHDa
翻译:北京大学第一医院心内科 张斌;审校:福建医科大学附属第一医院高血压研究所 韩英
摘 要
背景 关于比伐卢定与普通肝素(unfractionated heparin, UFH)联合计划应用糖蛋白 IIb/IIIa 受体拮抗剂(glycoprotein IIb/IIIa inhibitors, GPIs)的有效性和安全性的对比证据缺乏定论。
目的 此项研究对行介入治疗的急性冠脉综合征(acute coronary syndrome, ACS)患者进行评估,比较比伐卢定与
UFH(无论是否联合 GPIs)的有效性和安全性。
方法 在 MATRIX(经桡动脉入路和全身性应用比伐卢定最小化出血不良事件)计划中,7,213 例患者被随机分配
至比伐卢定组和 UFH 组进行治疗,是否应用 GPIs 则由术者判断。30 天共同主要终点为主要不良心血管事件(major adverse cardiovascular events, MACEs)(包括死亡、心肌梗死、卒中的复合终点)和净不良临床事件(net adverse clinical events, NACEs)(MACEs 和大出血的复合终点)。
结果 3,603 例患者被分配到 UFH 组,其中 781 例(21.7%)在冠脉介入治疗前接受联合 GPIs 的计划治疗。比伐
卢定组和 UFH 组紧急使用 GPIs 的患者比例类似(4.5% 和 5.4%)(P=0.11)。经过校正后,3 组患者在 30 天两项
共同主要终点 MACEs 和 NACEs 的发生率以及包括死亡率、心肌梗死、支架内血栓或卒中在内的独立终点的发
生率无明显差异。与 UFH 和 UFH+GPI 组相比,比伐卢定组可降低出血风险,主要表现在降低严重出血的发生,
包括致死性出血和非介入入路相关事件,同时也降低了输血率以及入路血管外科修复的需要。上述结果不受介入
治疗中应用 UFH 剂量的影响,同时也通过多重敏感分析进行了确认,包括血管介入入路的随机分配。
https://doi.org/10.1016/j.jacc.2018.01.033
From the aDepartment of Cardiology, Bern University Hospital, Bern, Switzerland; bDepartment of Advanced Biomedical Sciences, Federico II University of Naples, Naples, Italy; cAdvice Pharma Group S.r.l., Milan, Italy; dDepartment of Cardiology and Critical Care Medicine, Hartcentrum Hasselt, Jessa Ziekenhuis, and Faculty of Medicine and Life Sciences Hasselt University, Hasselt, Belgium; eSC Terapia Intensiva Cardiologica, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy; fEUSTRATEGY Association, Forli’, Italy; gCardiovascular Institute, Azienda Ospedaliero-Universitaria di Ferrara, Cona (FE), Italy; hMaria Cecilia Hospital, GVM Care and Research, Cotignola (RA), Italy; iCardiology Unit, Ospedali Riuniti di Rivoli, ASL Torino 3, Turin, Italy; jDivision of Cardiology, Department of Cardiothoracic Sciences, University of Campania “Luigi Vanvitelli”, Naples, Italy; kStruttura complessa di Cardiologia ASST di Vimercate, Italy; lDepartment of Cardiology, ASL3 Ospedale Villa Scassi, Genoa, Italy; mInterventional Cardiology Unit, Clinica Mediterranea, Naples, Italy; nAzienda Ospedaliera Universitaria Policlinico “Gaetano Martino”, University of Messina, Messina, Italy; oSC Cardiologia, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy; pUO Cardiologia, Azienda USL Toscana Sudest, Grosseto, Italy; qInterventional Cardiology Unit, Ospedale San Giovanni Bosco, Turin, Italy; rASST Bergamo ovest, Ospedale di Treviglio (BG), Italy; sCardiovascular Interventional Unit, Cardiology Department, S.Anna Hospital, Como, Italy; tUniversity Hospital “Maggiore della Carità”, Novara, Italy; uASST Fatebenefratelli-Sacco, Milan, Italy; vFondazione Monasterio-CNR-Regione Toscana, Toscana, Italy;

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
2
对于接受经皮冠脉介入治
疗(percutaneous coronary in- tervention, PCI)的急性冠脉综 合征(acute coronary syndrome, ACS) 患 者, 如 何 进 行 最 有
效的抗栓治疗仍然存在很大
的争议 [1-3]。普通肝素(unfrac-tionated heparin, UFH)( 无 论
是 否 联 合 计 划 的 糖 蛋 白 IIb/IIIa 受 体 拮 抗 剂 [glycoprotein IIb/IIIa inhibitors, GPIs])和比
伐卢定是两种最普遍的抗栓
策略,从上世纪 90 年代起已
经有一些有关这两种策略对
比的不同临床研究 [4]。从那时
起,这方面的研究结果得到
了许多相互矛盾的数据,因
此,在现有临床实践中,比伐卢定和 UFH 的安全性和有
效性的对比仍没有定论。
虽然一些临床研究,包括 EUORMAX(欧洲院前急
性冠脉综合征造影)研究 [5,6] 和 BRIGHT(急性心肌梗死
中比伐卢定对比肝素及肝素联合 GPIs 试验)研究 [7],已
经显示无论 UFH 组是否联合应用 GPIs,比伐卢定组均可
降低大出血的发生而使患者获益。但是,HEAT-PPCI(急
诊经皮冠脉介入抗栓治疗的有效性研究)研究和近期的
VALIDATE-SWEDEHEART(根据推荐疗法注册试验,在
用于增强和发展心脏病评估循证护理的瑞典网络系统中
比较比伐卢定与肝素在接收现代抗血小板治疗的 ST 段和
非 ST 段抬高心肌梗死患者中的疗效)研究显示,与比伐
卢定相比,单用 UFH 不增加出血事件 [8,9]。由于计划应用
GPIs 的患者在使用 UFH 患者中的比例已经减少,所以这
样的差异是值得注意的。
因此,我们预先设定通过比伐卢定与单用 UFH 或
UFH+GPI 的对比,研究比伐卢定的有效性和安全性,这一
研究是迄今为止在所有 ACS 人群中评价比伐卢定数据规模
最大的研究,也是唯一一项随机分配血管入路的研究。
方法
研究设计 这项 MATRIX(经桡动脉入路和全身性应用比
伐卢定最小化出血不良事件)抗凝血酶研究是一项随机、
多中心试验。它在 7,213 例计划接受 PCI 的 ACS 患者(无
论是否存在 ST 段抬高)中比较比伐卢定(仅限于紧急情
况下应用 GPIs)和 UFH(是否应用 GPIs 由术者研究决定)。
它是 MATRIX 项目(NCT01433627)3 项试验的其中之一,
如前所述 [1,10]。
研究人群 符合纳入标准的非 ST 段抬高型急性冠脉综合
征(non-ST-segment elevation acute coronary syndrome, NSTE-ACS)患者在开始随机分组前的 7 天内,静息或最
小活动量时出现新发或恶化的心肌缺血病史,同时还应满
wCasa di Cura Villa Verde, Taranto, Italy; xSimple Departmental Emodynamic Structure, Ospedale Sirai–Carbonia, Carbonia, Italy; yHumanitas Research Hospital, IRCCS, Rozzano, Italy; zCardiovascular Department, Infermi Hospital, Rimini, Italy; aaDepartment of Cardiovascular, Respiratory, Nephrologic, Anesthesiologic and Geriatric Sciences, Policlinico Umberto I, “Sapienza”, University of Rome, Rome, Italy; bbStruttura complessa di Emodinamica, ASST Monza, Ospedale di Desio, Italy; ccPoliclinico San Marco, Zingonia, Italy; ddInterventional Cardiology, Sandro Pertini Hospital, Rome, Italy; eeClinic of Cardiovascular Disease, IRCCS Policlinico San Martino, Genoa, Italy; ffMater Salutis Hospital-Legnago, Verona, Italy; ggMaastricht University Medical Center, and Zuyderland MC, Maastricht, the Netherlands; hhSahlgrenska University Hospital, Göteborg, Sweden; and the iiClinic Cardiovascular Institute, University Hospital Clinic, IDIBAPS (Institut d' Investigacions Biomèdiques August Pi i Sunyer), Barcelona, Spain. The trial was sponsored by the Società Italiana di Cardiologia Invasiva (GISE, a non-profit organization), which received grant support from The Medicines Company and TERUMO. This substudy did not receive any direct or indirect funding. Dr. Gargiulo has received research grant support from the Cardiopath PhD program. Dr. Vranckx has received speaking or consulting fees from Bayer Health Care and Daiichi-Sankyo. Dr. Leonardi has received grants and personal fees from AstraZeneca; and personal fees from Chiesi, Daiichi-Sankyo, and The Medicines Company. Dr. Varbella has received speaking or consulting fees from Boeringher Ingelheim, Daiichi-Sankyo, Bayer, Pfizer, AstraZeneca, OrbusNeich, Biosensors, AbbottVascular, Amgen, and Bristol-Myers Squibb; and has received grants from Medtronic, Boston Scientific, Abbott, St. Jude, Biosensors, CID Alvimedica, and Abbott Vascular. Dr. Andò has received nonfinancial support from Terumo during the study; personal fees from Daiichi-Sankyo, Pfizer, and AstraZeneca; and personal fees and nonfinancial support from Bayer. Dr. Cortese has received research grants from AB Medica, Abbott, St. Jude Medical, and Stentys; and personal fees from Abbott, AstraZeneca, Daiichi-Sankyo, and Eli Lilly and Stentys. Dr Sciahbasi has served as advisory board member for Bayer HealthCare. Dr van't Hof has received speaker fees from The Medicines Company; has received unrestricted grants from Medtronic and AstraZeneca; and has served as Executive Board member of the EUROMAX trial. Dr. Omervoic has been a member of the advisory board for Boston Scientific; and has received a research grant from AstraZeneca. Dr. Windecker has received research grants from Abbott, Amgen, Bracco, Boston Scientific, Biotronick, St. Jude, and Terumo. Dr. Valgimigli has received grants from The Medicines Company, Terumo, and AstraZeneca; and has received personal fees from Terumo, St. Jude Vascular, and Abbott Vascular. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.Manuscript received November 19, 2017; revised manuscript received January 11, 2018, accepted January 12, 2018.
缩略词表ASC=acute coronary syndrome(s)
急性冠脉综合征
CABG=coronary artery bypass
grafting
冠脉旁路移植术
GPI=glycoprotein IIb/IIIa inhibitor
糖蛋白IIbIIIa受体拮抗剂
MACE=major adverse cardiovascular
event
不良心血管事件
NACE=net adverse clinical event
净不良临床事件
NSTE-ACS=nonL-ST-segment
elevation acute coronary syndrome(s)
非ST段抬高型急性冠脉综合征
PCI=percutaneous coronary
intervention
经皮冠脉介入治疗
ST=stent thrombosis
支架内血栓
TIMI=Thrombolysis In Myocardial
Infarction
心肌梗死溶栓
UFH=unfractionated heparin
普通肝素
结论 在 ACS 患者中,与 UFH-(无论是否联合计划应用 GPI)相比,比伐卢定不能显著降低 MACEs 和 NACEs的发生率。然而,无论 UFH 组是否联合计划应用 GPIs,比伐卢定均能显著降低出血并发症,主要是与血管入路
无关的出血。(经桡动脉入路和全身性应用比伐卢定最小化出血不良事件 [Minimizing Adverse Haemorrhagic Events by Transradial Access Site and Systemic Implementation of AngioX, MATRIX];NCT01433627)
(J Am Coll Cardiol 2018;71:1231–42) © 2018 by the American College of Cardiology Foundation.

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
3
足以下高危标准中的至少 2 条:1)年龄大于等于 60 岁,
心肌损伤标志物升高,心电图符合缺血改变;2)冠脉造
影后拟行PCI者。符合纳入标准的ST段抬高型心肌梗死(ST segment elevation myocardial infarction, STEMI)患者需满足
症状发作 12 小时内或症状发作 12-24 小时之间仍存在持
续缺血证据或之前已接受溶栓治疗。主要纳入和排除标
准如前所述 [1,10]。所有患者需签署书面知情同意书。
研究方案和随机化 通过计算机随机生成序列号的方法将
患者按照 1:1 的比例随机分配到接受比伐卢定组和接受
UFH 组,随机区组大小按照患者 ACS 的类型(即 ST 段抬
高 vs. 非 ST 段抬高),即将应用或已经应用 P2Y12 受体拮
抗剂类型(氯吡格雷 vs. 替格瑞洛或普拉格雷)和研究中
心进行分层。STEMI 患者冠脉造影前进行随机化,NSTE-ACS 患者完成冠脉造影后在 PCI 前进行随机化。
所有干预都以开放的方式进行。比伐卢定按照说明书
给药,根据体重以 0.75mg/kg 推注,随后立即给予每小时
1.75mg/kg 注射维持至 PCI 结束。PCI 术后是否继续维持
比伐卢定注射以随机方式决定(在 MATRIX 计划治疗期
间)。在被分配到延长比伐卢定给药时间组的患者中,有
两种给药方式供选择(足量注射至 PCI 术后 4 小时或每
小时减量至 0.25mg/kg 注射至少 6 小时),如何选择由负
责治疗的医师决定。UFH 的起始给药分别为 70-100U/kg (单药)或 50-70U/kg(联合 GPIs)。追加的 UFH 量根据监
测的活化凝血时间(activated clotting time, ACT)调整,由
负责治疗的医师决定。UFH 组患者在 PCI 前可由负责治疗
的医师判断是否需要联合应用 GPI。但比伐卢定组患者只
有在PCI后出现围术期缺血并发症(即无复流或大块血栓)
时才可应用 GPI。其它药物的使用可根据相关专业指南。
随访和研究终点 术后 30 天进行临床随访。预先设定两个
30 天共同主要复合终点,分别为:主要不良心血管事件
(major adverse cardiovascular events, MACEs),其定义为
全因死亡、心肌梗死(myocardial infarction, MI)、卒中
的复合终点;净不良临床事件(net adverse clinical events, NACEs),定义为 MACEs 或非冠脉旁路移植术(coronary artery bypass graft, CABG)相关大出血(出血学术研究协
会规定的 3 型或 5 型出血)的复合终点。次要终点包括
复合终点的任意一项、心血管死亡和支架内血栓(stent thrombosis, ST)。出血程度由 TIMI(心肌梗死溶栓)和
GUSTO(链激酶和组织型纤溶酶原激活剂的全球性应用)
量表评判。支架内血栓根据学术研究协会分类标准定义
为确定或可能的支架相关血栓事件。所有研究终点均为
预先设定。独立临床事件判定委员会在并不知晓治疗分
组的情况下,对所有存在疑问的事件进行裁定。
统计分析 该研究为检测 30 天两项主要复合终点的优势
提供了支持,期待终点事件发生率的下降比率为 30%,
相当于发生率的比值为 0.70。
所有分析均按照意向性治疗原则进行,包括所有纳入
基于血管入路分配分析的患者。随机后 30 天内的事件均
纳入分析。我们应用 Mantel-Cox 方法在发生第一次事件
时进行主要和次要终点的统计分析,并通过对数秩检验
计算相应的双侧 P 值。我们在多重比较中未进行任何调
整,但将一类错误发生率设定在 2.5% 以校正两个共同主
要终点。我们在次要终点分析中将双侧 α 值设定在 5%,
以便于运用常规方法对结果进行阐释。用 Kaplan-Meier法进行生存曲线的构建。我们根据肝素剂量和血管入路
(桡动脉或股动脉)进行了分层分析,也评估了比较中可
能存在的交互作用。
尽管比伐卢定组或 UFH 组的患者是随机分配的,只
允许在 UFH 组允许联合计划 GPI 的使用,且是否联合
应用由医师判定。由于 UFH 组 GPI 的联合使用具有非随
机特点,我们对临床终点进行了混杂因素的校正。用多变
量 logistic 模型进行校正后分析,相关变量包括年龄、性
别、体重指数、ACS 类型、中心、糖尿病、吸烟、高血压、
MI 病史、CABG 病史、卒中 / 短暂性脑缺血发作(transient ischemic attack, TIA)病史、外周动脉疾病、Killip 分级、
溶栓治疗病史、肌酐、主动脉球囊反搏泵、导管室前肝
素应用、PCI 手术完全成功、手术持续时间、治疗血管、
SYNTAX(紫杉醇药物支架经皮冠脉介入治疗与心脏手
术的协同作用)积分、近段病变、较大的血管直径(定
义为支架直径大于等于 3mm 或后扩张球囊直径大于等于
3.5mm)、至少 1 例复杂病变、治疗病变的血栓、PCI 术前
TIMI 血流 0-1 级及氯吡格雷出院用药。
由于两个治疗组(即单用 UFH 组和 UFH+GPI 组)
之间基线临床特征存在差异,我们运用倾向性评分作为
一种敏感性分析的方法将选择偏倚降至最低。UFH 组的
每例患者均会得到,由非简化多变量 logistic 回归计算而
来的倾向性评分,用来反映其接受联合 GPI 治疗的可能
性。因此,每一例患者会对应一个由 logistic 方程计算得
出的倾向性评分,来反映在被观察的协变量中,预测接
受某种特殊治疗的可能性。这一公式同样适用于比伐卢
定组患者(不允许符合方案计划的 GPI)。分析中包含以
下变量:年龄、性别、体重指数、ACS 类型、中心、糖

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
4
表 1 30 天比伐卢定与单用 UFH 组临床终点的对比
总计 (N=7,213)
比伐卢定 (n=3,610)
单用 UFH (n=2,822)
未校正的比值比(95% CI)
P 值多变量校正后比值比(95% CI)
P 值倾向性积分校正后比值比比(95% CI)
P 值
死亡、MI、卒中 762 (10.6) 371 (10.3) 327 (11.6) 0.89 (0.76−1.03) 0.113 1.02 (0.85−1.22) 0.843 0.96 (0.81−1.13) 0.618
死亡、MI、卒中、BARC 3 或 5
845 (11.7) 401 (11.1) 362 (12.8) 0.87 (0.75−1.00) 0.047 0.96 (0.81−1.14) 0.664 0.92 (0.78−1.07) 0.282
死亡、MI、卒中、BARC 3 或 5、TVR、ST
860 (11.9) 410 (11.4) 367 (13.0) 0.87 (0.76−1.01) 0.059 0.97 (0.82−1.15) 0.739 0.92 (0.79−1.08) 0.309
死亡 142 (2.0) 59 (1.6) 65 (2.3) 0.71 (0.5−1.01) 0.055 0.91 (0.43−1.94) 0.805 0.71 (0.48−1.04) 0.08
心血管死亡 136 (1.9) 56 (1.6) 63 (2.2) 0.69 (0.48−1.00) 0.046 1.01 (0.45−2.28) 0.976 0.69 (0.47−1.03) 0.072
MI 610 (8.5) 307 (8.5) 258 (9.1) 0.93 (0.79−1.1) 0.391 1.03 (0.85−1.24) 0.771 1.03 (0.86−1.23) 0.778
卒中 29 (0.4) 13 (0.4) 15 (0.5) 0.68 (0.32−1.42) 0.301 0.56 (0.24−1.28) 0.17 0.58 (0.27−1.28) 0.178
TIA 14 (0.2) 5 (0.1) 7 (0.2) 0.56 (0.18−1.76) 0.313 0.91 (0.21−4.02) 0.905 0.73 (0.22−2.42) 0.611
TVR 87 (1.2) 52 (1.4) 25 (0.9) 1.63 (1.01−2.62) 0.044 1.50 (0.90−2.51) 0.118 1.40 (0.85−2.29) 0.186
确定的 ST 57 (0.8) 36 (1.0) 15 (0.5) 1.88 (1.03−3.43) 0.037 1.77 (0.91−3.41) 0.091 1.56 (0.84−2.91) 0.163
急性 33 (0.5) 20 (0.6) 9 (0.3) 1.74 (0.79−3.82) 0.164 1.85 (0.76−4.50) 0.178 1.45 (0.64−3.27) 0.369
亚急性 24 (0.3) 16 (0.4) 6 (0.2) 2.08 (0.82−5.33) 0.117 1.56 (0.57−4.25) 0.386 1.72 (0.65−4.54) 0.275
确定或可能的 ST 80 (1.1) 45 (1.2) 26 (0.9) 1.35 (0.83−2.19) 0.218 1.57 (0.88−2.83) 0.129 1.32 (0.79−2.23) 0.291
急性 38 (0.5) 22 (0.6) 12 (0.4) 1.43 (0.71−2.90) 0.313 1.93 (0.80−4.68) 0.144 1.25 (0.59−2.66) 0.562
亚急性 42 (0.6) 23 (0.6) 14 (0.5) 1.28 (0.66−2.50) 0.459 1.18 (0.52−2.64) 0.692 1.39 (0.68−2.85) 0.371
出血 873 (12.1) 391 (10.8) 345 (12.2) 0.89 (0.77−1.02) 0.101 0.84 (0.71−1.00) 0.044 0.85 (0.72−1.00) 0.043
BARC 1 427 (5.9) 190 (5.3) 170 (6.0) 0.87 (0.71−1.07) 0.201 0.83 (0.66−1.04) 0.10 0.84 (0.68−1.05) 0.126
BARC 2 304 (4.2) 151 (4.2) 107 (3.8) 1.10 (0.86−1.41) 0.437 1.03 (0.79−1.34) 0.827 1.09 (0.84−1.42) 0.505
BARC 3 116 (1.6) 44 (1.2) 50 (1.8) 0.69 (0.46−1.03) 0.069 0.69 (0.45−1.07) 0.096 0.65 (0.42−0.99) 0.045
BARC 3a 62 (0.9) 24 (0.7) 24 (0.9) 0.78 (0.44−1.38) 0.392 1.03 (0.55−1.90) 0.935 0.76 (0.42−1.37) 0.361
BARC 3b 49 (0.7) 16 (0.4) 25 (0.9) 0.50 (0.27−0.94) 0.027 0.42 (0.22−0.81) 0.01 0.47 (0.24−0.90) 0.024
BARC 3c 5 (0.1) 4 (0.1) 1 (0) 3.13 (0.35−27.98) 0.282 — — 2.17 (0.23-20.59) 0.499
BARC 4 5 (0.1) 1 (0) 4 (0.1) 0.20 (0.02−1.75) 0.104 — — 0.31 (0.03−2.98) 0.31
BARC 5 21 (0.3) 5 (0.1) 14 (0.5) 0.28 (0.10−0.78) 0.009 — — 0.20 (0.06−0.62) 0.006
BARC 5a 15 (0.2) 4 (0.1) 9 (0.3) 0.35 (0.11−1.13) 0.065 0.26 (0.03−2.08) 0.206 0.24 (0.06−0.96) 0.043
BARC 5b 6 (0.1) 1 (0) 5 (0.2) 0.16 (0.02−1.34) 0.051 — — 0.12 (0.01−1.12) 0.063
BARC 3 或 5 137 (1.9) 49 (1.4) 64 (2.3) 0.60 (0.41−0.87) 0.006 0.65 (0.43−0.99) 0.043 0.55 (0.37−0.81) 0.003
BARC 3 或 5 入路部位
51 (0.7) 19 (0.5) 23 (0.8) 0.65 (0.35−1.19) 0.155 0.65 (0.34−1.24) 0.19 0.66 (0.35−1.26) 0.209
BARC 3 或 5 非入路部位
86 (1.2) 30 (0.8) 41 (1.5) 0.57 (0.36−0.92) 0.018 0.64 (0.37−1.12) 0.117 0.49 (0.30−0.81) 0.005
BARC 2、3 或 5 441 (6.1) 200 (5.5) 171 (6.1) 0.91 (0.75−1.12) 0.389 0.90 (0.72−1.13) 0.361 0.88 (0.71−1.10) 0.257
BARC 2、3 或 5 入路部位
237 (3.3) 105 (2.9) 98 (3.5) 0.84 (0.64−1.10) 0.206 0.81 (0.61−1.09) 0.165 0.86 (0.65−1.14) 0.298
BARC 2、3 或 5 入路部位
204 (2.8) 95 (2.6) 73 (2.6) 1.02 (0.75−1.38) 0.912 1.04 (0.74−1.46) 0.83 0.92 (0.66−1.27) 0.599
TIMI 大出血 49 (0.7) 16 (0.4) 26 (0.9) 0.48 (0.26−0.9) 0.019 0.39 (0.18−0.83) 0.015 0.38 (0.20−0.74) 0.005
TIMI 小出血 50 (0.7) 17 (0.5) 20 (0.7) 0.66 (0.35−1.27) 0.212 0.79 (0.40−1.56) 0.492 0.65 (0.33−1.29) 0.216
TIMI 大或小出血 99 (1.4) 33 (0.9) 46 (1.6) 0.56 (0.36−0.88) 0.010 0.57 (0.34−0.95) 0.03 0.49 (0.30−0.79) 0.004
GUSTO 严重出血 42 (0.6) 16 (0.4) 20 (0.7) 0.63 (0.32−1.21) 0.158 0.67 (0.29−1.54) 0.35 0.47 (0.23−0.95) 0.037

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
5
总计 (N=7,213)
比伐卢定 (n=3,610)
单用 UFH (n=2,822)
未校正的比值比(95% CI)
P 值多变量校正后比值比(95% CI)
P 值倾向性积分校正后比值比比(95% CI)
P 值
GUSTO 中 等 程 度出血
42 (0.6) 16 (0.4) 17 (0.6) 0.74 (0.37−1.46) 0.376 0.92 (0.43−1.96) 0.823 0.79 (0.39−1.62) 0.526
GUSTO 轻微出血 784 (10.9) 358 (9.9) 304 (10.8) 0.92 (0.79−1.07) 0.289 0.86 (0.72−1.02) 0.081 0.89 (0.75−1.05) 0.173
GUSTO 中 等 或 严重出血
84 (1.2) 32 (0.9) 37 (1.3) 0.68 (0.42−1.09) 0.103 0.79 (0.45−1.37) 0.398 0.61 (0.37−1.01) 0.053
外科修复入路血管和需要输血的复合终点
103 (1.4) 36 (1.0) 51 (1.8) 0.55 (0.36−0.85) 0.006 0.52 (0.32−0.84) 0.008 0.58 (0.37−0.91) 0.018
外科修复入路血管 17 (0.2) 5 (0.1) 8 (0.3) 0.49 (0.16−1.49) 0.199 0.52 (0.15−1.74) 0.289 0.58 (0.18−1.84) 0.354
输血 94 (1.3) 31 (0.9) 47 (1.7) 0.52 (0.33−0.81) 0.004 0.47 (0.28−0.79) 0.004 0.54 (0.33−0.87) 0.011
BARC 3 或 5 的分布情况
颅内出血 7 (0.1) 4 (0.1) 3 (0.1) 1.04 (0.23−4.66) 0.957 0.48 (0.06−3.92) 0.496 0.83 (0.18−3.91) 0.815
心包出血 28 (0.4) 11 (0.3) 14 (0.5) 0.61 (0.28−1.35) 0.222 0.76 (0.24−2.40) 0.637 0.49 (0.21−1.13) 0.094
消化道出血 27 (0.4) 6 (0.2) 16 (0.6) 0.29 (0.11−0.75) 0.006 0.31 (0.12−0.85) 0.023 0.26 (0.09−0.71) 0.008
泌尿系出血 12 (0.2) 5 (0.1) 2 (0.1) 1.95 (0.38−10.07) 0.415 2.80 (0.40−19.41) 0.298 2.04 (0.39−10.64) 0.399
入路部位出血 49 (0.7) 19 (0.5) 22 (0.8) 0.68 (0.37−1.25) 0.207 0.70 (0.36−1.33) 0.27 0.69 (0.36−1.33) 0.267
其它出血 10 (0.1) 3 (0.1) 5 (0.2) 0.47 (0.11−1.96) 0.288 1.17 (0.12−11.52) 0.891 0.37 (0.07−1.90) 0.232
如无特殊备注,数值表示为n(%)。BARC=出血学术研究协会;CI=置信区间;GUSTO=链激酶和组织纤溶酶原激活剂的全球应用;MI=心肌梗死;ST=支架内血栓;TIA=短暂性脑缺血发作;TIMI=心肌梗死溶栓;TVR=靶血管血运重建;UFH=普通肝素。
续表 1
尿病、吸烟、冠心病家族史、高血压、高胆固醇血症、
MI 病史、PCI 病史、卒中和 / 或 TIA 病史、外周动脉疾
病、慢性阻塞性肺病、Killip 分级、心脏骤停、左室射血
分数、肌酐、治疗血管、SYNTAX 积分、近段病变、较
大和 / 或较小的血管直径、至少 1 个复杂病变、治疗病
变的血栓、PCI 术前 TIMI 血流 0-1 级、导管室用药(磺
达肝癸钠、依诺肝素、β 受体阻断剂、替格瑞洛、氯吡
格雷)以及每例患者治疗的病变和植入支架的病变。个
体化倾向性评分用于校正模型比较各组的终点。此外,
为了减少治疗的选择偏倚和观察指标中潜在混杂因素的
影响,我们用下列算法进行倾向性评分配对法严格校正
患者基线特征中具有显著差异的项目。这种算法为以
0.1 作为标准差进行 1:1 无替代优化配对。所有统计应用
STATA 版本 14.1(StataCorp, College Station, Texas)和 R(R Foundation, Vienna, Austria)统计分析软件完成。
结果
纳入患者 本项 MATRIX 抗凝血酶研究纳入了 2011 年 10月至 2014 年 11 月期间来自意大利、荷兰、西班牙、瑞典
78 个中心的 7213 例 ACS 患者。其中 3610 例被分配到比
伐卢定组,3603 例被分配到 UFH 组,UFH 组中 2822 例
未接受计划 GPIs 输注(仅 UFH 组),781 例在 PCI 前开始
接受计划的 GPI 输注(UHF+GPI 组)。在比伐卢定和 UFH两组中,治疗过程中接受 GPIs 紧急应用的比例类似(分别
为 4.5% 和 5.4%,P=0.11)。
三组患者的临床及手术相关特征,包括住院期间和
出院时服用药物情况并不平衡(在线表 1-3)。
与单独应用 UFH 组相比,联合计划应用 GPI 组的
患者更年轻、具有更多男性、更多吸烟、更高比例患有
STEMI、发病时更多心跳骤停,但更少合并糖尿病、高
血压、MI、PCI、CABG、卒中 /TIA、慢性阻塞性肺疾病、
外周血管疾病或肾功能不全的病史(在线表 1)。尽管计
划使用 GPI 输注的患者行单支血管介入治疗的比例更高,
但手术时间却更长。他们更可能需要主动脉气囊反搏,
存在血栓再通、近段血管病变、血栓病变,更多直径较
大的支架、支架总长度更长(在线表 2)。
临床终点 表 1-3 中描述了未校正及校正后的各组 30 天临
床终点的对比情况。通过多因素校正或倾向性评分校正后,
两个共同主要终点 MACEs 和 NACEs 在 3 组中无差异(见
图 1、重点插图和表 1-3)。

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
6
表 2 30 天比伐卢定与 UFH 联合计划应用 GPI 组临床终点的对比
总计 (N=7,213)
比伐卢定 (n=3,610)
UFH+GPI (n=781)
未校正的比值比 (95% CI)
P 值多变量校正后的
比值比 (95% CI)
P 值倾向性评分校正后的比值比比
(95% CI)P 值
死亡、MI、卒中 762 (10.6) 371 (10.3) 64 (8.2) 1.25 (0.96−1.64) 0.094 0.99 (0.70−1.39) 0.947 0.95 (0.70−1.29) 0.731
死亡、MI、卒中、BARC 3 或 5
845 (11.7) 401 (11.1) 82 (10.5) 1.06 (0.83−1.34) 0.642 0.80 (0.59−1.09) 0.153 0.79 (0.60−1.05) 0.108
死亡、MI、卒中、B A R C 3 或 5 、TVR、ST
860 (11.9) 410 (11.4) 83 (10.6) 1.07 (0.84−1.35) 0.581 0.81 (0.60−1.10) 0.170 0.81 (0.62−1.07) 0.146
死亡 142 (2.0) 59 (1.6) 18 (2.3) 0.71 (0.42−1.2) 0.2 0.60 (0.29−1.27) 0.184 0.75 (0.40−1.41) 0.377
心血管死亡 136 (1.9) 56 (1.6) 17 (2.2) 0.71 (0.41−1.23) 0.219 0.60 (0.28−1.29) 0.190 0.76 (0.40−1.45) 0.406
MI 610 (8.5) 307 (8.5) 45 (5.8) 1.48 (1.08−2.02) 0.014 1.05 (0.73−1.50) 0.800 0.97 (0.68−1.38) 0.856
卒中 29 (0.4) 13 (0.4) 1 (0.1) 2.81 (0.37−21.5) 0.298 2.40 (0.27−21.18) 0.43 4.50 (0.56−35.99) 0.156
TIA 14 (0.2) 5 (0.1) 2 (0.3) 0.54 (0.1−2.79) 0.456 0.57 (0.06−5.46) 0.624 0.45 (0.07−2.77) 0.391
TVR 87 (1.2) 52 (1.4) 10 (1.3) 1.12 (0.57−2.21) 0.733 1.16 (0.57−2.39) 0.678 1.20 (0.58−2.49) 0.619
确定的 ST 57 (0.8) 36 (1) 6 (0.8) 1.30 (0.55−3.08) 0.553 1.55 (0.63−3.85) 0.341 1.68 (0.67−4.21) 0.265
急性 33 (0.5) 20 (0.6) 4 (0.5) 1.08 (0.37−3.16) 0.886 1.53 (0.50−4.68) 0.459 1.65 (0.53−5.12) 0.385
亚急性 24 (0.3) 16 (0.4) 2 (0.3) 1.73 (0.4−7.53) 0.459 1.36 (0.28−6.59) 0.699 1.73 (0.36−8.19) 0.492
确定或可能的 ST 80 (1.1) 45 (1.2) 9 (1.2) 1.08 (0.53−2.21) 0.83 1.28 (0.57−2.86) 0.554 1.33 (0.62−2.87) 0.467
急性 38 (0.5) 22 (0.6) 4 (0.5) 1.19 (0.41−3.45) 0.749 1.62 (0.53−4.94) 0.394 1.80 (0.58−5.53) 0.306
亚急性 42 (0.6) 23 (0.6) 5 (0.6) 1.00 (0.38−2.62) 0.992 0.78 (0.23−2.65) 0.686 0.97 (0.34−2.77) 0.953
出血 873 (12.1) 391 (10.8) 137 (17.5) 0.62 (0.51−0.75) <0.001 0.64 (0.5−0.83) 0.001 0.64 (0.50−0.80) <0.001
BARC 1 427 (5.9) 190 (5.3) 67 (8.6) 0.61 (0.46−0.81) 0.001 0.72 (0.52−1.00) 0.052 0.70 (0.51−0.96) 0.029
BARC 2 304 (4.2) 151 (4.2) 46 (5.9) 0.71 (0.51−0.99) 0.041 0.75 (0.51−1.10) 0.139 0.72 (0.49−1.04) 0.080
BARC 3 116 (1.6) 44 (1.2) 22 (2.8) 0.43 (0.26−0.72) 0.001 0.46 (0.25−0.85) 0.013 0.43 (0.24−0.77) 0.005
BARC 3a 62 (0.9) 24 (0.7) 14 (1.8) 0.37 (0.19−0.72) 0.002 0.30 (0.13−0.68) 0.004 0.32 (0.15−0.70) 0.004
BARC 3b 49 (0.7) 16 (0.4) 8 (1.0) 0.43 (0.19−1.01) 0.046 0.60 (0.24−1.50) 0.275 0.43 (0.16−1.10) 0.078
BARC 3c 5 (0.1) 4 (0.1) 0 (0) — — — — — —
BARC 4 5 (0.1) 1 (0) 0 (0) — — — — — —
BARC 5 21 (0.3) 5 (0.1) 2 (0.3) 0.54 (0.10−2.79) 0.456 — — 0.57 (0.09−3.63) 0.553
BARC 5a 15 (0.2) 4 (0.1) 2 (0.3) 0.43 (0.08−2.36) 0.319 — — 0.38 (0.05−2.73) 0.336
BARC 5b 6 (0.1) 1 (0) 0 (0) — — — — — —
BARC 3 或 5 137 (1.9) 49 (1.4) 24 (3.1) 0.44 (0.27−0.72) 0.001 0.47 (0.26−0.85) 0.013 0.44 (0.25−0.77) 0.004
BARC 3 或 5 入路部位
51 (0.7) 19 (0.5) 9 (1.2) 0.46 (0.21−1.01) 0.047 0.57 (0.23−1.37) 0.209 0.44 (0.18−1.07) 0.070
BARC 3 或 5 非入路部位
86 (1.2) 30 (0.8) 15 (1.9) 0.43 (0.23−0.8) 0.006 0.42 (0.19−0.95) 0.036 0.45 (0.22−0.91) 0.027
BARC 2、3 或 5 441 (6.1) 200 (5.5) 70 (9.0) 0.62 (0.47−0.81) <0.001 0.64 (0.46−0.89) 0.009 0.61 (0.45−0.84) 0.002
BARC 2、3 或 5 入路部位
237 (3.3) 105 (2.9) 34 (4.4) 0.67 (0.45−0.98) 0.04 0.66 (0.42−1.03) 0.067 0.60 (0.39−0.93) 0.021
BARC 2、3 或 5 非入路部位
204 (2.8) 95 (2.6) 36 (4.6) 0.57 (0.39−0.84) 0.004 0.65 (0.40−1.03) 0.069 0.65 (0.42−1.00) 0.049
TIMI 大出血 49 (0.7) 16 (0.4) 7 (0.9) 0.49 (0.20−1.20) 0.113 0.47 (0.15−1.43) 0.183 0.68 (0.26−1.79) 0.430
TIMI 小出血 50 (0.7) 17 (0.5) 13 (1.7) 0.28 (0.14−0.58) <0.001 0.29 (0.11−0.76) 0.012 0.30 (0.13−0.70) 0.006
TIMI 大或小出血 99 (1.4) 33 (0.9) 20 (2.6) 0.36 (0.20−0.62) <0.001 0.37 (0.18−0.76) 0.007 0.43 (0.23−0.81) 0.009
GUSTO 严重出血 42 (0.6) 16 (0.4) 6 (0.8) 0.58 (0.23−1.47) 0.245 0.67 (0.20−2.20) 0.505 0.75 (0.27−2.11) 0.590

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
7
总计 (N=7,213)
比伐卢定 (n=3,610)
UFH+GPI (n=781)
未校正的比值比 (95% CI)
P 值多变量校正后的
比值比 (95% CI)
P 值倾向性评分校正后的比值比比
(95% CI)P 值
GUSTO 中等程度出血
42 (0.6) 16 (0.4) 9 (1.2) 0.38 (0.17−0.87) 0.017 0.29 (0.11−0.80) 0.017 0.29 (0.12−0.74) 0.010
GUSTO 轻微出血 784 (10.9) 358 (9.9) 122 (15.6) 0.63 (0.52−0.78) <0.001 0.68 (0.53−0.88) 0.004 0.67 (0.52−0.85) 0.001
GUSTO 中 等 或 严重出血
84 (1.2) 32 (0.9) 15 (1.9) 0.46 (0.25−0.85) 0.011 0.42 (0.20−0.88) 0.022 0.46 (0.23−0.92) 0.027
外科修复入路血管和需要输血的复合终点
103 (1.4) 36 (1) 16 (2.0) 0.49 (0.27−0.88) 0.014 0.42 (0.20−0.88) 0.022 0.39 (0.20−0.76) 0.006
外科修复入路血管 17 (0.2) 5 (0.1) 4 (0.5) 0.27 (0.07−1.01) 0.036 0.25 (0.06−1.15) 0.075 0.18 (0.04−0.79) 0.023
输血 94 (1.3) 31 (0.9) 16 (2.0) 0.42 (0.23−0.77) 0.004 0.33 (0.15−0.72) 0.005 0.34 (0.17−0.67) 0.002
BARC 3 或 5 的分布情况
颅内出血 7 (0.1) 4 (0.1) 0 (0) — — — — — —
心包出血 28 (0.4) 11 (0.3) 3 (0.4) 0.79 (0.22−2.84) 0.722 0.81 (0.16−4.23) 0.807 1.02 (0.26−4.05) 0.976
消化道出血 27 (0.4) 6 (0.2) 5 (0.6) 0.26 (0.08−0.85) 0.016 0.18 (0.03−0.93) 0.041 0.16 (0.04−0.64) 0.009
泌尿系出血 12 (0.2) 5 (0.1) 5 (0.6) 0.22 (0.06−0.75) 0.008 0.07 (0.01−0.67) 0.021 0.22 (0.06−0.88) 0.032
入路部位出血 49 (0.7) 19 (0.5) 8 (1.0) 0.51 (0.22−1.17) 0.108 0.65 (0.26−1.64) 0.36 0.51 (0.20−1.28) 0.150
其它出血 10 (0.1) 3 (0.1) 2 (0.3) 0.32 (0.05−1.94) 0.194 — — 0.11 (0.01−1.51) 0.098
如无特殊备注,数值表示为n(%)。GPI=糖蛋白IIbIIIa受体拮抗剂;其它缩写同表1。
续表 2
相似的,包括死亡、心肌梗死、支架内血栓或卒中
在内的各项独立终点在各组间也没有差异(表 1-3)。然
而,比伐卢定仍表现出与最严重出血事件发生风险降
低的相关性,与单用 UFH 组相比,降低致死性和非介
入入路相关的严重出血(主要为胃肠道出血事件)。与
UFH+GPI 组相比,比伐卢定能降低消化道和泌尿系出血
的风险(表 1 和 2)。
在比伐卢定组,输血率和需要外科入路血管修复的
事件明显减少(表 1 和 2)。相反,与单用 UFH 组相比,
UFH+GPI 组中出血并发症(符合出血学术研究协会分级
3A 级的泌尿系大出血)、TIMI 轻微程度出血或 GUSTO中等程度的出血并发症增加(表 3)。
分层分析和倾向性匹配分析 我们对 3 组主要临床结局进
行分层分析。经校正后观察发现,不同 UFH 剂量亚组间
结果无明显差异(在线表 4)。同时,我们按照不同血管
入路对大出血事件进行了分层分析,结果提示与 UFH 组
相比,无论患者被随机分配至何种动脉入路组,比伐卢
定始终可降低血管入路相关或无关的出血事件。
在对 MATRIX 研究人群进行倾向性评分匹配后,将
2698 对匹配患者进行比伐卢定与单用 UFH 对比;747 对患者
进行比伐卢定与 UFH+GPI 对比,578 对患者进行单用 UFH与 UFH+GPI 对比。这个用于评估 UFH 组非随机应用 GPI 疗
效的模型表现出良好的辨识力和准度(曲线下面积 0.85,
95% 置信区间:0.83-0.87;Hosmer-Lemeshow 拟合优度检验: P=0.352)(在线图 1)。几乎所有匹配后协变量的标准差小
于 10%,这提示各组在很大程度上是平衡的(在线图 2-4,在
线表 6-11)。30 天的临床终点确定比伐卢定对比单用 UFH,
在各项公认的出血分级标准下的致死性出血和大出血方面
均有获益,这与主要校正后分析相一致(在线表 12-14)。
讨论
这项 MATRIX 研究预设分析的主要发现归纳如下:
1. 与单用 UFH 或 UFH 联合计划应用的 GPI 相比,比
伐卢定并不能显著降低 PCI 时 MACEs 和 NACEs 的发生率。
2. 与 UFH 和 UFH+GPI 组相比,比伐卢定可降低大
出血事件的发生,包括致死性和非血管入路相关的出血
事件,以及输血率和需要外科入路血管修复的事件。这
一结果与多变量分析、倾向性评分校正分析及倾向性评
分匹配分析的结果相一致。虽然应用比伐卢定与单用
UFH 及 UFH+GPI 相比,ST 发生率有升高趋势,死亡率
有降低趋势,但主要复合终点中(除了出血以外)任一
终点事件发生率的差异均未达到统计学显著水平。
在一些初步研究之后,与 UFH+GPI 相比,比伐卢定
可降低出血并发症同时并不增加缺血风险,因此在 PCI

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
8
表 3 30 天 UFH 联合计划应用 GPI 组与单用 UFH 组临床终点的对比
总计 (N=7,213)
UFH+GPI (n = 781)
单用 UFH (n=2,822)
未校正的比值比(95% CI)
P 值多变量校正后的比值比(95% CI)
P 值倾向性评分校正后的比值比(95% CI)
P 值
死亡、MI、卒中 762 (10.6) 64 (8.2) 327 (11.6) 0.71 (0.54−0.92) 0.011 0.96 (0.66−1.4) 0.827 1.02 (0.73−1.44) 0.888
死亡、MI、卒中、BARC 3 或 5
845 (11.7) 82 (10.5) 362 (12.8) 0.82 (0.64−1.04) 0.101 1.09 (0.77−1.52) 0.633 1.15 (0.84−1.57) 0.377
死 亡、MI、 卒中、BARC 或 5、TVR、ST
860 (11.9) 83 (10.6) 367 (13.0) 0.82 (0.64−1.04) 0.096 1.05 (0.75−1.47) 0.785 1.10 (0.81−1.50) 0.526
死亡 142 (2.0) 18 (2.3) 65 (2.3) 1.00 (0.59−1.69) 0.998 0.84 (0.22−3.18) 0.799 0.82 (0.41−1.63) 0.565
心血管死亡 136 (1.9) 17 (2.2) 63 (2.2) 0.98 (0.57−1.67) 0.926 0.59 (0.12−2.89) 0.515 0.74 (0.36−1.51) 0.401
MI 610 (8.5) 45 (5.8) 258 (9.1) 0.63 (0.46−0.86) 0.004 0.99 (0.66−1.47) 0.959 1.11 (0.76−1.64) 0.581
卒中 29 (0.4) 1 (0.1) 15 (0.5) 0.24 (0.03−1.82) 0.134 0.11 (0.01−1.50) 0.098 0.15 (0.02−1.37) 0.093
TIA 14 (0.2) 2 (0.3) 7 (0.2) 1.03 (0.21−4.97) 0.968 2.60 (0.32−21.17) 0.372 1.42 (0.20−9.84) 0.725
TVR 87 (1.2) 10 (1.3) 25 (0.9) 1.45 (0.69−3.01) 0.322 1.08 (0.47−2.45) 0.859 0.86 (0.35−2.14) 0.747
确定的 ST 57 (0.8) 6 (0.8) 15 (0.5) 1.45 (0.56−3.73) 0.443 1.09 (0.38−3.17) 0.871 0.78 (0.24−2.52) 0.683
急性 33 (0.5) 4 (0.5) 9 (0.3) 1.61 (0.49−5.21) 0.426 1.22 (0.30−5.00) 0.780 0.81 (0.19−3.47) 0.775
亚急性 24 (0.3) 2 (0.3) 6 (0.2) 1.20 (0.24−5.97) 0.820 1.22 (0.20−7.68) 0.829 0.74 (0.11−5.24) 0.766
确定或可能的 ST 80 (1.1) 9 (1.2) 26 (0.9) 1.25 (0.59−2.67) 0.562 1.13 (0.43−2.93) 0.805 1.02 (0.39−2.65) 0.969
急性 38 (0.5) 4 (0.5) 12 (0.4) 1.20 (0.39−3.73) 0.747 1.22 (0.30−5.00) 0.780 0.80 (0.2−3.27) 0.757
亚急性 42 (0.6) 5 (0.6) 14 (0.5) 1.29 (0.46−3.58) 0.624 1.22 (0.30−4.95) 0.782 1.26 (0.35−4.59) 0.724
出血 873 (12.1) 137 (17.5) 345 (12.2) 1.43 (1.18−1.75) <0.001 1.27 (0.97−1.68) 0.084 1.27 (0.97−1.66) 0.082
BARC 1 427 (5.9) 67 (8.6) 170 (6.0) 1.42 (1.07−1.89) 0.014 1.14 (0.79−1.65) 0.471 1.08 (0.75−1.55) 0.687
BARC 2 304 (4.2) 46 (5.9) 107 (3.8) 1.55 (1.10−2.19) 0.012 1.45 (0.95−2.20) 0.084 1.48 (0.95−2.30) 0.084
BARC 3 116 (1.6) 22 (2.8) 50 (1.8) 1.59 (0.96−2.63) 0.067 1.66 (0.86−3.18) 0.129 1.84 (0.98−3.46) 0.059
BARC 3a 62 (0.9) 14 (1.8) 24 (0.9) 2.11 (1.09−4.07) 0.023 3.07 (1.20−7.86) 0.019 2.82 (1.24−6.44) 0.014
BARC 3b 49 (0.7) 8 (1.0) 25 (0.9) 1.16 (0.52−2.56) 0.721 0.94 (0.35−2.47) 0.892 1.10 (0.41−2.93) 0.851
BARC 3c 5 (0.1) 0 (0) 1 (0) — — — — — —
BARC 4 5 (0.1) 0 (0) 4 (0.1) — — — — — —
BARC 5 21 (0.3) 2 (0.3) 14 (0.5) 0.52 (0.12−2.27) 0.373 — — 0.25 (0.05−1.34) 0.105
BARC 5a 15 (0.2) 2 (0.3) 9 (0.3) 0.80 (0.17−3.72) 0.778 — — 0.37 (0.06−2.28) 0.284
BARC 5b 6 (0.1) 0 (0) 5 (0.2) — — — — — —
BARC 3 或 5 137 (1.9) 24 (3.1) 64 (2.3) 1.35 (0.85−2.17) 0.203 1.41 (0.74−2.68) 0.293 1.33 (0.74−2.41) 0.342
BARC 3 或 5 入路部位
51 (0.7) 9 (1.2) 23 (0.8) 1.41 (0.65−3.06) 0.376 1.49 (0.57−3.91) 0.417 1.86 (0.71−4.84) 0.205
BARC 3 或 5 非入路部位
86 (1.2) 15 (1.9) 41 (1.5) 1.32 (0.73−2.39) 0.353 1.35 (0.58−3.13) 0.482 1.10 (0.52−2.32) 0.805
BARC 2、3 或 5 441 (6.1) 70 (9.0) 171 (6.1) 1.48 (1.12−1.95) 0.005 1.43 (1.00−2.05) 0.051 1.44 (1.01−2.07) 0.047
BARC 2、3 或 5入路部位
237 (3.3) 34 (4.4) 98 (3.5) 1.25 (0.85−1.85) 0.255 1.31 (0.82−2.12) 0.262 1.53 (0.94−2.49) 0.089
BARC 2、3 或 5非入路部位
204 (2.8) 36 (4.6) 73 (2.6) 1.78 (1.20−2.66) 0.004 1.65 (0.98−2.79) 0.062 1.32 (0.79−2.21) 0.285
TIMI 大出血 49 (0.7) 7 (0.9) 26 (0.9) 0.97 (0.42−2.24) 0.948 0.66 (0.23−1.93) 0.447 0.66 (0.24−1.83) 0.424
TIMI 小出血 50 (0.7) 13 (1.7) 20 (0.7) 2.35 (1.17−4.72) 0.014 2.61 (0.92−7.43) 0.072 2.66 (1.09−6.51) 0.032
TIMI 大或小出血 99 (1.4) 20 (2.6) 46 (1.6) 1.57 (0.93−2.66) 0.089 1.37 (0.66−2.84) 0.404 1.38 (0.70−2.70) 0.351
GUSTO 严重出血 42 (0.6) 6 (0.8) 20 (0.7) 1.08 (0.44−2.7) 0.862 0.86 (0.25−2.99) 0.816 0.83 (0.27−2.53) 0.746

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
9
总计 (N=7,213)
UFH+GPI (n = 781)
单用 UFH (n=2,822)
未校正的比值比(95% CI)
P 值多变量校正后的比值比(95% CI)
P 值倾向性评分校正后的比值比(95% CI)
P 值
GUSTO 中 等 程 度出血
42 (0.6) 9 (1.2) 17 (0.6) 1.91 (0.85−4.29) 0.109 3.11 (1.03−9.43) 0.044 3.04 (1.13−8.21) 0.028
GUSTO 轻微出血 784 (10.9) 122 (15.6) 304 (10.8) 1.45 (1.18−1.79) <0.001 1.22 (0.92−1.62) 0.167 1.23 (0.92−1.62) 0.158
GUSTO 中 等 或 严重出血
84 (1.2) 15 (1.9) 37 (1.3) 1.46 (0.80−2.67) 0.21 1.73 (0.76−3.94) 0.192 1.63 (0.77−3.43) 0.199
外科修复入路血管和需要输血的复合终点
103 (1.4) 16 (2.0) 51 (1.8) 1.13 (0.65−1.99) 0.661 1.29 (0.61−2.72) 0.51 1.52 (0.76−3.05) 0.233
外科修复入路血管 17 (0.2) 4 (0.5) 8 (0.3) 1.81 (0.54−6.00) 0.327 2.54 (0.49−13.23) 0.267 2.91 (0.65−12.95) 0.161
输血 94 (1.3) 16 (2.0) 47 (1.7) 1.23 (0.7−2.17) 0.474 1.39 (0.65−2.97) 0.400 1.65 (0.82−3.33) 0.163
BARC 3 或 5 的分布情况
颅内出血 7 (0.1) 0 (0) 3 (0.1) — — — — — —
心包出血 28 (0.4) 3 (0.4) 14 (0.5) 0.77 (0.22−2.69) 0.687 0.92 (0.15−5.78) 0.928 0.52 (0.12−2.27) 0.384
消化道出血 27 (0.4) 5 (0.6) 16 (0.6) 1.13 (0.41−3.08) 0.812 1.30 (0.34−5.05) 0.703 0.99 (0.29−3.36) 0.985
泌尿系出血 12 (0.2) 5 (0.6) 2 (0.1) 9.03 (1.75−46.56) 0.001 — — 11.14 (1.69−73.65) 0.012
入路部位出血 49 (0.7) 8 (1.0) 22 (0.8) 1.31 (0.58−2.95) 0.507 1.41 (0.51−3.90) 0.505 1.62 (0.59−4.44) 0.345
其它出血 10 (0.1) 2 (0.3) 5 (0.2) 1.45 (0.28−7.45) 0.658 0.87 (0.03−27.51) 0.936 1.88 (0.17−21.24) 0.610
如无特殊备注,数值表示为n(%)。其它缩写同表1和表2。
续表 3
过程中已被批准使用。尽管与应用 UFH+GPI 相比,比伐
卢定治疗 STEMI 患者导致急性 ST 发生率有所提高 [11],
但是在 HORIZONS-AMI(急性心肌梗死患者的血运重建
和支架的协调结局)研究中,比伐卢定组患者的早期死
亡率获益来源于对出血的预防,该发现进一步增强了学
界的一种观念,即出血预防至少与缺血性事件一样可以
影响死亡率终点 [12]。然而,常规在 UFH 基础上加用 GPI是没有依据的,且在选用比伐卢定作为对照组的研究中,
它会进一步增加出血风险。
近十年间,强效口服 P2Y12 受体拮抗剂的引入和桡动
脉入路的普及分别降低了 PCI 相关的缺血和出血事件。然
而,在大多数 ACS 患者中,常规还是选择性应用 GPIs 还
需进一步明确。大多数近期的研究(包括 EUREMAX 研
究 [6] 和 BRIGHT[7] 研究)发现, 在 UFH 组,无论是否联
合 GPI,比伐卢定组在降低大出血方面均有获益。相反,
在 HEAT-PPCI 研究中发现,与比伐卢定相比,肝素可降
低 MACEs 和 ST 的发生率,同时不增加出血并发症 [8]。最
近的 VALIDATE-SWEDEHEART 研究旨在于经桡动脉入
路进行 PCI、接受 P2Y12 受体拮抗剂治疗的 ACS 患者中
(STEMI 与 NSTEMI 配对)对比比伐卢定与单用 UFH 的
疗效和安全性,以解决上述未确定的临床问题 [9]。此项研
究纳入了 6006 例患者,比伐卢定与 UFH 相比,在 6 个月
时包括缺血事件和出血事件的复合终点以及独立终点事件
均无明显差异。研究中比伐卢定未能表现出减少出血事件
的净获益与桡动脉入路率高(约 90%)和很少应用 GPIs(只在紧急情况下应用 [ 约 3%])相关。然而,此研究中,
还可能存在除桡动脉入路和未计划应用 GPIs 以外的因素
影响比伐卢定的在减少出血方面的获益。在术后 30 天,
该研究发现比伐卢定具有减少出血事件的趋势,以此推断
术后 30 天这一时间点可能更适合反映围术期抗栓药物的
真实价值。除此之外,在比伐卢定组患者中允许应用 UFH(术前最多 5000U,在导管室术中最多 3000U)可能使结果
产生偏倚,从而导致阴性结果。在 MATRIX 研究中,UFH组允许联合计划应用的 GPIs,但实际仅有少于 1/4 的患者
最终应用了 GPI。此外,按照研究设计,所有患者会被随
机、等量分配到桡动脉或股动脉入路组。
我们发现比伐卢定在各组间均可减少出血风险,主要
减少非血管入路相关的出血并发症。这一结果提示,除血管
入路的选择或计划应用 GPIs 以外,不同的研究设计和 / 或研
究人群也许可以解释比伐卢定在出血终点中不一致的表现。
然 而, 此 研 究 与 VALIDATE-SWEDEHEART 研 究
以及其它较早的研究类似,无论 UHF 组是否联合应用

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
10
图 1 30 天内共同主要复合研究终点
0 5 10 15 20 25 30
比值比: 0.71 (0.54-0.92); P = 0.011校正比值比: 0.94 (0.66-1.40); P = 0.83
随机化后天数
主要
不良
心血
管事
件
0
12
10
8
6
4
2
0 5 10 15 20 25 30
比值比: 0.82 (0.64-1.04); P = 0.10校正比值比: 1.09 (0.77-1.52); P = 0.63
781 735 727 720 718 718 7172822
UFH + GPI单用UFH
风险暴露患者数
2551 2526 2516 2507 2502 2497781 717 708 702 700 700 699
2822UFH + GPI单用UFH
风险暴露患者数
2529 2493 2482 2472 2466 2462
随机化后天数
0
12
10
8
6
4
2
普通肝素+糖蛋白IIb/IIIa抑制剂对比单用普通肝素
0 5 10 15 20 25 30
比值比: 0.89 (0.76-1.03); P = 0.11校正比值比: 1.02 (0.85-1.22); P = 0.84
随机化后天数
主要
不良
心血
管事
件
0
12
10
8
6
4
2
0 5 10 15 20 25 30
比值比: 0.87 (0.75-1.10); P = 0.047校正比值比: 0.96 (0.81-1.11); P = 0.66
3610 3296 3266 3259 3251 3248 32402822
比伐卢定单用UFH
风险暴露患者数
2551 2526 2516 2507 2502 24973610 3272 3238 3230 3222 3220 32112822
比伐卢定单用UFH
风险暴露患者数
2529 2493 2482 2472 2466 2462
随机化后天数
比伐卢定对比单用普通肝素
净不
良临
床事
件净
不良
临床
事件
净不
良临
床事
件
0
12
10
8
6
4
2
比伐卢定对比普通肝素+糖蛋白IIb/IIIa抑制刘
0 5 10 15 20 25 30
比值比: 1.25 (0.96-1.64); P = 0.094校正比值比: 0.99 (0.70-1.39); P = 0.95
随机化后天数
主要
不良
心血
管事
件
0
12
10
8
6
4
2
0 5 10 15 20 25 30
比值比: 1.06 (0.83-1.34); P = 0.64校正比值比: 0.80 (0.59-1.09); P = 0.15
3610 3296 3266 3259 3251 3248 3240781 735 727 720 718 718 717
3610 3272 3238 3230 3222 3220 3211781 717 708 702 700 700 699
随机化后天数
0
12
10
8
6
4
2
比伐卢定 单用UFH
比伐卢定 单用UFH
UFH + GPI 单用UFH
比伐卢定单用UFH
风险暴露患者数比伐卢定单用UFH
风险暴露患者数
在30天内(上)接受比伐卢定与单用普通肝素(UFH)的患者、(中)比伐卢定与UFH联合糖蛋白IIb/IIIa抑制剂(GPI)的患者和(下)UFH联合计划GPI与单用UFH的患者中,(左)共同主要终点主要不良心血管事件和(右)净不良临床事件的累积发生率。
GPIs,比伐卢定组在主要复合终点均无获益。此外,比
伐卢定组与单用 UHF 组相比,在 ST 和死亡率上也无明
显差异。这可能反映出此研究效力有限,不足以评估发
生率较低终点事件的治疗效果。同时,由于需要应用多
变量分析工具解释 GPI 的非随机特性或真实治疗效果不
足,该研究效力会进一步的扩大。
既往相关研究中对照组 UFH 的剂量也值得讨论。在
HEAT-PPCI 研究中,UFH 剂量为 70U/kg,这种剂量可
能与比伐卢定未能表现出减少出血的优势相关 [8]。相反,
EUREMAX 和 BRIGHT 研 究 中 在 UFH 组 应 用 100U/kg 剂量可能导致 UFH 组患者的出血风险增加 [5-7]。然而,
在 MATRIX 研 究 中, 对 照 组 应 用 UFH 的 平 均 剂 量 为

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
11
78U/kg,我们的结果显示,在对 UHF 剂量进行的分层分
析中,无论高剂量组还是低剂量组都呈现出一致的结果。
因此,我们现有的结果并不支持用 UFH 推荐剂量的不同
来简单地解释不同研究中的差异。
这一研究在既往研究的基础上增加了新的证据,即
比伐卢定不能提供包括缺血或缺血和出血事件的复合终点
的获益。然而,我们的结果显示,无论桡动脉或股动脉入
路,比伐卢定均可减少出血风险。因此在肝素诱导的血小
板减少的患者中,除了一些对患者的既定建议,比伐卢定
应被考虑为UFH的替代疗法,尤其在高出血风险的患者中。
最后,在现有临床实践中,针对所有比伐卢定研究的个体
病例数据荟萃分析,可能为进一步评价比伐卢定对比 UFH
联合或不联合 GPI 的优势和局限性的研究带来启示 [3]。
研究局限 虽然本研究基于预先设定的分析,但是否联合
GPI 的计划性应用则交由医生判定,因此,导致 3 组在数
量和临床特征上具有不平衡性。多变量校正和倾向性评分
配对分析的应用很好的消除了一些可测量的混杂因素。然
而,仍然不能除外残余不可测量混杂因素的干扰。由于
PCI 术后比伐卢定的输注存在两种非随机分配的给药方法,
且在既往研究的单变量分析中得出的结论不同 [1],所以本
研究并未对其进行分析,可能需要进一步的多变量研究。
结论
在接受介入治疗的 ACS 患者中,对照组是否联合计划
重点插图 比伐卢定或肝素在 ACS 患者中的应用:主要终点的森林图
0.50 1.0 2.0 3.0 4.0 5.00.10
死亡、MI、卒中
死亡、MI、卒中、BARC 3或5
全因死亡
心肌梗死
卒中
确定的ST
BARC 3或5
1.02 (0.85-1.22)
多变量Adj RR (95%CI)
比伐卢定更好 UFH更好
0.96 (0.81-1.14)
0.91 (0.43-1.94)
1.03 (0.85-1.24)
0.56 (0.24-1.28)
1.77 (0.91-3.41)
0.65 (0.43-0.99)
0.50 1.0 2.0 3.0 4.0 5.00.10
死亡、MI、卒中
死亡、MI、卒中、BARC 3或5
全因死亡
心肌梗死
卒中
确定的ST
BARC 3或5
多变量Adj RR (95%CI)
比伐卢定更好 UFH更好
0.99 (0.7-1.39)
0.8 (0.59-1.09)
0.6 (0.29-1.27)
1.05 (0.73-1.5)
2.4 (0.27-21.18)
1.55 (0.63-3.85)
0.47 (0.26-0.85)
比伐卢定对比单用UFH
比伐卢定对比UFH+GPI
A
B
(A)比伐卢定与单用普通肝素(UFH)或(B)比伐卢定与UFH联合计划的糖蛋白IIb/IIIa抑制剂(GPI)的比较,30天时主要终点的多变量校正比值比(rate ratio, RR)。BARC=出血学术研究协会;CI=置信区间;MI=心肌梗死;ST=支架内血栓。

JACC VOL. 71, NO. 11, 2018MARCH 20, 2018:1231–42
Gargiulo et al. 比伐卢定或肝素在 ACS 中的应用
12
应用 GPIs 对比伐卢定与 UFH 的有效性和安全性的比较并不
产生影响。与主要研究结果一致的是,比伐卢定与单用 UFH
相比并未减少共同主要终点的发生率,但它仍有减少持续出
血并发症方面的获益,这种获益主要来自于与入路部位无
关的重要事件。比伐卢定和单用 UFH 相比,在其他非常
用终点(比如 ST 或致死事件)的疗效,需要进一步研究。
通信地址 Dr. Marco Valgimigli, Department of Cardiology, Bern University
Hospital, Freiburgstrasse 4, CH-3010, Bern, Switzerland. E-mail: marco.
观 点
患者治疗和操作技巧的能力 在行经皮血运重建的
ACSs 患者中,无论何种入路、是否联合 GPIs 治疗,
比伐卢定与 UFH 相比具有相同的有效性,同时减少
出血风险。
转化前景 比伐卢定与 UFH 对比在其它终点(例如支
架内血栓和死亡率)方面还需要进一步研究,还应该
对这些治疗策略的成本收益进行评估。
参考文献
1. Valgimigli M, Frigoli E, Leonardi S, et al. Bivalirudin or unfractionated heparin in acute coronary syndromes. N Engl J Med 2015;373:997–1009.2. Gargiulo G, Moschovitis A, Windecker S, Valgimigli M. Developing drugs for use before, during and soon after percutaneous coronary intervention. Expert Opin Pharmacother 2016;17:803–18.3. Stone GW. Procedural anticoagulation in myocardial infarction. N Engl J Med 2017;377:1198–200.4. Valgimigli M, Gargiulo G. Bivalirudin in current practice: melius abundare quam deficere? J Am Coll Cardiol Intv 2016;9:1321–3.5. Steg PG, van 't Hof A, Hamm CW, et al. Bivalirudin started during emergency transport for primary PCI. N Engl J Med 2013;369:2207–17.6. Zeymer U, van 't Hof A, Adgey J, et al. Bivalirudin is superior to heparins alone
with bailout GP IIb/IIIa inhibitors in patients with ST-segment elevation myocardial infarction transported emergently for primary percutaneous coronary intervention: a pre-specified analysis from the EUROMAX trial. Eur Heart J 2014;35:2460–7.7. Han Y, Guo J, Zheng Y, et al. Bivalirudin vs heparin with or without tirofiban during primary percutaneous coronary intervention i n a c u t e m y o c a r d i a l i n f a r c t i o n : t h e BRIGHT randomized clinical trial. JAMA 2015;313:1336–46.8. Shahzad A, Kemp I , Mars C, et al . Unfractionated heparin versus bivalirudin in primary percutaneous coronary intervention ( H E AT- P P C I ) : a n o p e n - l a b e l , s i n g l e centre, randomised controlled trial. Lancet 2014;384:1849–58.9. Erlinge D, Omerovic E, Frobert O, et al. Bivalirudin versus heparin monotherapy in myocardial infarction. N Engl J Med 2017;377:1132–42.
10. Valgimigli M, Gagnor A, Calabro P, et al. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet 2015;385:2465–76.11. Capodanno D, Gargiulo G, Capranzano P, Mehran R, Tamburino C, Stone GW. Bivalirudin versus heparin with or without glycoprotein IIb/IIIa inhibitors in patients with STEMI undergoing primary PCI: an updated meta-analysis of 10,350 patients from five randomized clinical trials. Eur Heart J Acute Cardiovasc Care 2016;5:253–62.12. Stone GW, Witzenbichler B, Guagliumi G, et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med 2008;358:2218–30.
关键词 急性冠脉综合症、比伐卢定、糖蛋
白 IIb/IIIa 受体拮抗剂、肝素、MATRIX
附录 补充表格及图片,请见本文线上版本。
沈阳军区总医院 韩雅玲 李洋
急性冠脉综合征(ACS)患者经皮冠状动脉介入治疗(PCI)术中实施安全、有效的抗凝是确保手术成功的关键
因素。近年来,关于新型直接凝血酶抑制剂比伐卢定在 PCI 围术期的应用成为国际介入心脏病学界的热点问题。本研
究评价了比伐卢定和普通肝素联合或者不联合 GPI 治疗 ACS 患者的有效性和安全性。30 天结果显示,相比于普通肝
素组和普通肝素联合 GPI 治疗组,比伐卢定组患者的出血事件、输血率和外科治疗率均更低,主要心血管不良事件
和净不良事件无明显差异。该研究结果表明,在 ACS 患者中,无论是否应用 GPI,比伐卢定和普通肝素在预防主要
心血管不良事件发生方面无明显差异,但比伐卢定可显著减少患者出血事件尤其是严重出血的发生风险。值得注意的
是,研究中 3610 例应用比伐卢定的患者中仅有 631 例采用 PCI 术后持续高剂量(每小时 1.75mg/kg)的方案,1106例采用 PCI 术后持续低剂量(每小时 0.25mg/kg)的方案,而 1873 例患者术后停用比伐卢定,且术后延长应用比伐
卢定的患者并未进行随机分组。综上,期待未来的研究进一步明确比伐卢定在 PCI 围术期的最佳治疗方案。
点 评

JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY ©2018 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
VOL. 72, NO. 10, 2018ISSN 0735-1097
双联抗血小板治疗评分在瑞典全国人群中的外部验证External Validation of the DAPT Score in a Nationwide PopulationPeter Ueda, MD, PHD,a Tomas Jernberg, MD, PHD,b Stefan James, MD, PHD,c,d Joakim Alfredsson, MD, PHD,e,f David
Erlinge, MD, PHD,g Elmir Omerovic, MD, PHD,h,i Jonas Persson, MD, PHD,b Annica Ravn-Fischer, MD, PHD,i Per Tornvall,
MD, PHD,j Bodil Svennblad, PHD,d Christoph Varenhorst, MD, PHDc,k
翻译:浙江大学医学院附属邵逸夫医院心内科 毕徐堃;审校:浙江大学医学院附属邵逸夫医院心内科 赵炎波
摘 要
背景 双联抗血小板治疗(dual antiplatelet therapy, DAPT)评分通过同步预测冠状动脉支架术后出血和缺血风险从
而决定 DAPT 持续时间。
目的 本研究旨在评估瑞典国内真实世界人群中 DAPT 评分的使用情况。
方法 本研究共纳入 41,101 例 2006 至 2014 年在瑞典注册的接受支架植入术 12 个月内无并发症的患者,并进一步
随访搜集术后 12-30 月的数据。通过 DAPT 评分比较心肌梗死(myocardial infarction, MI)或支架内血栓风险、主
要心血管和脑血管不良事件(major adverse cardiovascular and cerebrovascular events, MACCE)(包括心肌梗死、卒
中和全因死亡)、致命性或主要出血事件发生率。
结果 DAPT 评分在 MI 或支架内血栓形成事件、MACCE 事件和致命性或大出血事件中的区分能力分别为 0.58(95% 置信区间 [confidence interval, CI]:0.56-0.60)、0.54(95% CI:0.53-0.55)和 0.49(95% CI:0.45-0.53)。DAPT 评分≥ 3分患者 MI 或支架内血栓形成的风险显著升高,评分≥ 4 分时 MACCE 事件风险增加并呈 J 形相关。各评分水平之间致
命性或大出血事件风险的绝对差异很小。本研究中 DAPT 评分高分(≥ 2)和低分(<2)患者缺血和出血事件发生率与
推导出评分的 DAPT 研究存在较大差异,致命性或大出血事件发生率仅约 DAPT 研究中安慰剂对照组的一半。
结论 在本项全国范围人群的研究中,DAPT 评分并不能充分区分缺血和出血风险高低,且评分与缺血风险之间
的关系与延长 DAPT 的建议决策不一致。与 DAPT 研究相比,出血事件发生率显著降低。DAPT 评分及其延长
DAPT 的决策规则也许不能推广至真实世界人群。(J Am Coll Cardiol 2018;72:1069–78)© 2018 by the American College of Cardiology Foundation.
From the aClinical Epidemiology Division, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden; bDivision of Cardiovascular Medicine, Department of Clinical Sciences, Danderyd University Hospital, Karolinska Institutet, Stockholm, Sweden; cDepartment of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden; dUppsala Clinical Research Center, Uppsala University, Uppsala, Sweden; eDepartment of Cardiology, Linköping University, Linköping, Sweden; fDepartment of Medicine and Health Sciences, Faculty of Health Sciences, Linköping University, Linköping, Sweden; gDepartment of Cardiology, Skåne University Hospital, Lund University, Lund, Sweden; hDepartment of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska University Hospital, Gothenburg, Sweden; iDepartment of Cardiology, Sahlgrenska University Hospital, Gothenburg, Sweden; jDepartment of Clinical Science and Education, Södersjukhuset, Karolinska Institutet, Stockholm, Sweden; and kPfizer AB, Sollentuna, Sweden. This work was supported by Stiftelsen för ålderssjukdomar, Karolinska Institutet. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Dr. James has served on the advisory board for AstraZeneca and Bayer; has received institutional research grants from AstraZeneca; has received research grants from Janssen and Bayer; and has received grants and personal fees from The Medicines Company. Dr. Alfredsson has received lecture fees from AstraZeneca, Novartis, Merck, and Sanofi; has served on the advisory board for Bristol-Myers Squibb, Sanofi, and Eli Lilly; and has received grant support from AstraZeneca. Dr. Erlinge has received personal fees from AstraZeneca, during the conduct of the study. Dr. Omerovic has received grants from AstraZeneca and Abbott; and has received personal fees from AstraZeneca. Dr. Svennblad has received institutional grants from AstraZeneca. Dr. Varenhorst has received institutional grants and advisory board fees from AstraZeneca; and is after the conduct of this work but before the submission of this paper an employee of Pfizer. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.Manuscript received April 26, 2018; revised manuscript received May 31, 2018, accepted June 4, 2018.
为减少缺血事件的再发,冠状动脉支架植入术后患
者需要接受包括阿司匹林和一种 P2Y12 拮抗剂在内的双联
抗血小板治疗(dual antiplatelet therapy, DAPT)治疗。支
架植入后 1 年以上 DAPT 的获益大部分来源于减少自发
性心肌梗死(myocardial infarction,MI)(即与支架无关
的事件)[1,2]。但是,DAPT 的缺血保护获益被出血风险
PUBLISHED BY ELSEVIER https://doi.org/10.1016/j.jacc.2018.06.023

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
14
增加部分抵消,因此,DAPT持续时间需根据患者的缺血和
出血风险进行个体化调整 [3,4]。 但是缺血和出血事件的预测
因子会相互重叠 [3,5,6],造成风
险权衡和决策困难。
DAPT 评分是一种可同时
预测缺血和出血风险的临床
预测工具,该评分最近也被
写入美国和欧洲 DAPT 指南
的重点更新 [3,4]。对于接受 12 个月 DAPT 后未发生严重
缺血或出血事件的患者,通过权衡出血与缺血风险,该
评分使他们在后续 18 个月 DAPT 治疗中可以有更大获益
和更小伤害 [7]。DAPT 研究是 DAPT 评分的来源,目前只
有在这项研究中使用 DAPT 评分观察了 12 个月和 30 个
月 DAPT 的治疗效果。其他针对外部人群的研究评估了比
上述 DAPT 研究 [8,9] 更短的治疗时间,同时评估了 DAPT评分根据缺血和出血风险对患者进行分组的能力 [7-10]。然
而这些分析仅限于临床试验人群和一项日本临床登记研
究 [7-10]。另外,DAPT 研究中大部分患者植入的是第一代
药物洗脱支架 [1],而现在更多人选择植入安全性更高的新
一代支架 [11]。因此,这项风险评分对经皮冠状动脉介入
(percutaneous coronary intervention, PCI)治疗术后未经选择
的真实世界人群的效果仍不确定。
我们分析的数据来源于 SWEDEHEART(瑞典心脏
病循证医疗促进与发展网络系统)。我们评价了 DAPT 评
分对接受 12 个月 DAPT 治疗患者的缺血和出血风险进
行评估分组的能力,并且将缺血和出血事件的发生率与
DAPT 研究中的数据进行比较。
方法
DAPT 评分 DAPT 研究是一项临床试验,纳入冠状动脉支
架植入术后 12 个月内未发生重大缺血和出血事件的患者,
这些患者被随机分为继续用阿司匹林 + 氯吡格雷 / 普拉格
雷组或阿司匹林 + 安慰剂组继续治疗 18 个月 [1]。DAPT 评
分的研发基于独立的出血预测模型(链激酶和组织纤溶酶
原激活剂在治疗闭塞动脉的全球应用 [Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Arteries, GUSTO] 重度或中度)和缺血事件模型(MI 或
血栓形成)[7]。这两个模型包括一个用于 DAPT 随机延长
的变量。两个模型可模拟延长 DAPT 后每个患者的风险
差异(缺血风险降低 - 出血风险增加)。在第三个预测模
型中,9 个风险差异预测因子构成简化风险评分即 DAPT评分,评分范围为 -2 到 10,评分高低基于患者的特征
和治疗过程指数分配点计算得出。高分(≥ 2)显示延长
DAPT的患者缺血风险降低程度大于出血风险,而低分(<2)
显示患者的出血风险大于缺血风险。
数据源 患者来源于瑞典冠状动脉造影和血管成形术登记
处(Swedish Coronary Angiography and Angioplasty Registry, SCAAR),该登记处收集来自瑞典所有冠状动脉造影的
患者信息、手术过程和支架特征的信息,也是 SWEDE HEART 注册研究的一部分,其他文章已详细描述 [12,13]。
我们将 SCAAR 注册数据通过个人身份号码与瑞典的全国
健康登记相关联,包括国家患者登记(医院入院时所记载
的诊断和治疗过程)、国家处方药品注册(填写处方)和
死因登记,如在线附录中所述。
研究人群 我们纳入 2006 年 1 月 1 日至 2013 年 12 月 31日期间在瑞典所有经历冠状动脉支架 PCI 术,并在手术
后 7 天仍然存活的患者。我们首先排除了出院时仍接受
抗凝治疗的患者,其次我们排除了 PCI 术后 12 个月内发
生死亡或经历过支架内血栓形成、MI、血运重建、卒中
或大出血事件的患者,如在线附录中所述。我们进一步
排除了未满足至少 12 个月连续 DAPT 处方依从的患者(阿
司匹林和 P2Y12 抑制剂 [ 氯吡格雷,每日一次;替格瑞洛,
每日两次;或普拉格雷,每日一次 ]),包括给予阿司匹林
30 天宽限期,P2Y12 抑制剂 10 天宽限期,两者均导致依从
性较差。在线表 1 中展示了因发生缺血或出血事件或 <12个月 DAPT 而被排除的患者的特征。因用于计算 DAPT评分的变量数据缺失而被排除的患者,缺失数据包括用
于诊断肾功能不全的肾小球滤过率(n = 1,902 [4.0% ])、 吸烟(n = 1,734 [3.6%])、PCI 指征(n = 111 [0.2% ])和
支架直径(n = 5 [<0.01% ])。对于完成了 12 个月的平稳
DAPT 的有多于 1 处支架植入的患者,我们随机选择其
中 1 处 PCI 手术(图 1)。最终研究人群的基线特征(n= 41,101)和 DAPT 研究的临床试验人群显示于在线表 2 中。
终点 国际疾病分类 - 第 10 版(International Classification of Disease-10th reversion, ICD-10)代码和手术操作码被用
于挑选及验证瑞典注册研究的出血事件(在线表 3)[14]。
主要出血终点是致命性出血和非致命性大出血的复合终点,
大致相当于 GUSTO 中度或重度出血定义 [15],并且我们根
据斯德哥尔摩心房颤动的患者医疗记录进行验证研究发现
其敏感性为 84.5%,特异性为 95.9% [14]。次要出血终点是
缩略词表CI=confidence interval
置信区间
DAPT=dual antiplatelet therapy
双联抗血小板治疗
HR=hazard ratio
风险比
MACCE=major adverse
cardiovascular and cerebrovascular
event(s)
主要心血管和脑血管不良事件
MI=myocardial infarction
心肌梗死
PCI=percutaneous coronary intervention
经皮冠状动脉介入治疗

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
15
致命或大出血和需要住院的出血的复合终点(在同一验证
研究中敏感性为 99.5%,特异性为 94.0%)[14]。
对于缺血性事件,我们使用了 2 类事件结果:1)MI
(ICD-10:国家患者登记簿或死因登记中代码 I21-I22)或
支架内血栓形成(通过 SCAAR 中冠状动脉造影及记录识
别);2)主要不良心血管和脑血管事件(major adverse
cardiovascular and cerebrovascular events, MACCE),包括
MI、中风(ICD-10:I60-I64)和全因死亡。
统计方法 我们对患者从索引 PCI 术后 12 个月进行随访
直至死亡,数据收集至 PCI 术后 30 个月,目标结果出现,
或研究时间结束(2014 年 12 月 31 日)。我们对以下三方
面进行评估:1)评估 DAPT 评分来源的缺血和出血风险
预测模型;2)比较分析 SWEDEHEART 注册研究数据与
DAPT 研究数据中缺血和出血事件发生率;3)DAPT 评
分根据患者的缺血和出血风险进行分层的能力。
在评价风险预测模型中,我们假设所有患者在第
12 个月时停止 DAPT,将延长 DAPT 的预测因子设置为
“否”。这是因为在 PCI 术后 12 个月内患者未随机分配到不
同的治疗时间组,且很少患者需要接受长期 DAPT,同时
在研究期间本地指南中没有建议需要延长 DAPT 治疗 [16]。
我们使用 Harrell's C 统计数据评估预测模型为患者分配风
险的能力,即为后续经历该事件的患者分配更高的风险,
亦即其“区分”属性。我们通过将预测风险值与观察事
件发生率相对应程度进行评估校正,运用预测风险的五
分位数来比较预测风险值与实际风险值(运用 Kaplan-Meier 进行校正)。然后我们使用 Cox 比例风险回归分别
计算预测因子与缺血 / 出血模型的相关系数。
根据 DAPT 评分算法为每位患者分配了分数,并评
估了评分对缺血和出血结果的区分度。然后根据所建议
的延长 DAPT 决策准则(高分 [ ≥ 2] 和低分 [<2])将人群
进行分组 [7]。我们将 PCI 术后 12 个月至 30 个月的发生
缺血和原发性出血的 Kaplan-Meier 事件发生率与 DAPT研究中接受安慰剂的患者的发生率进行了比较 [7]。
我们比较了高分患者与低分患者的缺血和出血事件
发生率,并且通过 Cox 回归对每个评分水平计算风险比
(hazard ratios, HRs)。由于分数范围的下限或上限的患者
很少,因此评分为 -2、-1 和≥ 5 的患者被分为一组。
因为 MI 是 PCI 的指征,我们分别对有无发生 MI 的
患者进行了分析,同时对接受新一代药物洗脱支架的患
者也进行分析,如在线表 4 中所示。最后,我们将 DAPT评分常数作为独立变量,同时将缺血和出血结果作为因
图 1 研究人群流程图
2006年1月1日至2013年12月31日期间进行冠状动脉支架植入且术后7天患者仍然存活的117,313例PCI手术。
在12个月平稳DAPT治疗后有47,561例进行PCI手术
最终数据集包括41,101例患者
3,752例由于缺少任何DAPT评分变量的数据被排除 1,734例缺少吸烟状况 5例缺少支架直径 111例缺少PCI指征 1,902缺少GFR2,708例患者被随机排除,因他们曾接受12个月DAPT治疗后无并发事件且接受过多于一次的PCI治疗
69,752例在索引PCI后12个月内被排除 7,644例服用口服抗凝剂治疗 18,036例发生了相关事件 1,426例有致命性出血或大出血 313例有支架内血栓 7,226例有致命性或非致命性心肌梗塞 1,078有致命性或非致命性卒中 6,348进行了血运重建 1,645因其他原因死亡44,072例≥12个月DAPT治疗的患者没有填写处方
纳入研究人群为SWEDEHEART(瑞典心脏病循证医疗促进与发展网络系统)中接受冠状动脉支架经皮冠状动脉介入治疗(PCI)后完成12个月DAPT治疗且无缺血或出血事件的患者。 DAPT=双联抗血小板治疗; GFR =肾小球滤过率。

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
16
变量,通过 Cox 回归模型计算 DAPT 评分变量的 HRs。
我们运用 STATA version 15 软件(StataCorp,College Station,Texas)进行分析。该研究得到了斯德哥尔摩和
瑞典乌普萨拉地区伦理委员会的批准。不需要知情同意。
结果
研究人群和随访 在冠状动脉支架植入术后平稳完成 12 个
月 DAPT 治疗的 41,101 例患者中,22,615 例(55%)患者
DAPT 评分较低(<2 分),18,486 例(45%)评分较高(≥ 2 分)。
除 DAPT 评分变量的预期差异之外,高分患者较低分患者
更可能选择冠状动脉旁路移植术并且具有癌症病史的可
能性更低(表 1 和 2)。每个结果的随访时间的中位数和
表 1 DAPT 评分分组后患者特征低 DAPT 评分 (n=22,615)
高 DAPT 评分 (n=18,486)
索引年份2006 571 (2.5) 767 (4.1)2007 1,264 (5.6) 1,443 (7.8)2008 1,765 (7.8) 1,987 (10.7)2009 2,156 (9.5) 2,082 (11.3)2010 3,006 (13.3) 2,517 (13.6)2011 4,016 (17.8) 2,980 (16.1)2012 4,815 (21.3) 3,434 (18.6)2013 5,022 (22.2) 3,276 (17.7)
患者特征平均年龄,岁 69.5 ± 9.8 61.2 ± 9.6中位年龄,岁 70 (65–77) 61 (55–67)女性 6,328 (28.0) 4,618 (25.0)BMI,kg/m2 27.0 ± 4.0 28.1 ± 4.6糖尿病 2,262 (10.0) 5,513 (29.8)高血压 12,735 (56.6) 10,628 (57.9)从不吸烟者 11,426 (50.5) 5,414 (29.3)戒烟者 9,729 (43.0) 6,146 (33.2)吸烟者 1,460 (6.5) 6,926 (37.5)eGFR,ml/(min·1.73 m2) 81.0 ± 16.7 87.6 ± 19.0
合并症 *
肾功能不全 † 2,642 (11.7) 1,629 (8.8)既往心梗病史 4,310 (19.1) 7,789 (42.1)卒中 906 (4.0) 746 (4.0)心衰或 LVEF <30%‡ 179 (0.8) 2,105 (11.4)外周血管病变 332 (1.5) 493 (2.7)既往 PCI 3,894 (17.2) 6,116 (33.1)既往 CABG 1,246 (5.5) 2,330 (12.6)房颤 704 (3.1) 645 (3.5)肿瘤 2,082 (9.2) 1,074 (5.8)
出院时 P2Y12 拮抗剂种类替格瑞洛 4,874 (21.6) 3,825 (20.7)氯吡格雷 17,218 (76.1) 13,966 (75.5)普拉格雷 523 (2.3) 695 (3.8)
出院时服用的其他药物他汀 15,771 (96.6) 14,392 (97.3)ACEi 10,593 (64.9) 9,951 (67.3)血管紧张素 II 受体阻滞剂 2,461 (15.2) 2,380 (16.3)钙离子拮抗剂 2,507 (15.4) 2,287 (15.5)β- 受体阻滞剂 14,519 (88.9) 13,610 (92.0)
数值以n(%)、平均值± SD、或中位数(四分位数范围)表示。∗定义为国家患者登记簿中或SWEDEHEART(瑞典心脏病循证医疗促进与发展网络系统)登记处记录的任何合并症 (初步或补充诊断) 。†使用来自SWEDEHEART登记处的估计肾小球滤过率(eGFR)进行诊断,肾小球滤过率(eGFR)定义为eGFR <60 ml/min/1.73 m2。‡仅适用于心肌梗死或不稳定型心绞痛患者,作为经皮冠状动脉介入治疗(PCI)指征(290名患者缺失)。对于稳定性冠状动脉疾病作为PCI的指征,数据仅使用在国家患者注册中心中有心力衰竭病史的患者。相关指标数据缺失值如下:体重指数(n=1,237);高血压(n=260);出院时的其他药物:他汀类药物(n = 9,976)、血管紧张素转换酶(ACE)抑制剂(n=9,991)、血管紧张素II受体阻滞剂(n = 10,313)、钙拮抗剂(n=9,974)和β-受体阻滞剂(n=9,973)。CABG=冠状动脉旁路移植术;DAPT=双联抗血小板治疗;LVEF=左心室射血分数。
表 2 DAPT 评分分组后治疗和支架特征低 DAPT 评分(n=22,615)
高 DAPT 评分(n=18,486)
PCI 指征
STEMI 5,047 (22.3) 4,516 (24.4)
NSTEMI 7,974 (35.3) 9,066 (49.0)
不稳定心绞痛 3,533 (15.6) 1,635 (8.8)
稳定性冠脉疾病 6,061 (26.8) 3,269 (17.7)
手术特征
支架内血栓形成 112 (0.5) 231 (1.2)
支架个数 1.6 ± 0.9 1.7 ± 1.0
斑块个数 1.5 ± 0.8 1.6 ± 0.9
支架总长度(mm) 29.8 ± 19.3 32.1 ± 21.3
支架直径 <3 mm 8,873 (39.2) 12,028 (65.1)
静脉桥血管 PCI 97 (0.4) 1,109 (6.0)
支架类型
新一代 DES* 13,904 (61.5) 10,308 (55.8)
任何老一代 DES 2,793 (12.3) 4,236 (22.9)
任何金属裸支架 6,787 (30.0) 4,887 (26.4)
DES类型 †
西罗莫司涂层洗脱支架 1,566 (6.9) 1,264 (6.8)
依维莫司涂层洗脱支架 7,490 (33.1) 5,830 (31.5)
佐他莫司涂层洗脱支架 3,542 (15.7) 2,869 (15.5)
Biolimus 涂层洗脱支架 584 (2.6) 392 (2.1)
紫杉醇涂层洗脱支架 979 (4.3) 2,783 (15.1)
其他 2,986 (13.2) 1,939 (10.5)
统计数值以n (%) 或平均数± SD表示。所有数据来源于SWEDE-HEART注册中心。∗不包括在同一PCI手术期间也接受老一代药物洗脱支架(DES)的患者。†包括任何类型的DES支架(即在PCI期间患者植入不止1种类型支架)。NSTEMI = non–ST-segment elevation myocardial infarction,非ST段抬高型心肌梗死;STEMI = ST-segment elevation myocardial infarction,ST段抬高型心肌梗死;其他缩略词见表1。

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
17
推导 DAPT 评分预测模型的性能 缺血预测模型的 C 统计
量为 0.67(95%置信区间 [confidence interval, CI]:0.65-
0.68)(在线表 6)。MI 或支架内血栓形成的风险被高估了,
预测风险的五分位数从最低风险五分位数的 0.6 个百分点
(观察的风险 1.7%与预测的风险 2.3%),到最高风险五
四分位数范围如在线表 5 所示。在冠状动脉支架植入术
后 24 个月,3,797 名(Kaplan-Meier 调整率 11.7%)患者
仍在接受 DAPT,在 30 个月时这一人数为 2,353(7.9%)。
支架植入术后 30 个月仍接受 DAPT 的患者中高分人数的
比例大于低分人数(10.0% vs. 6.2% ; P<0.001)。
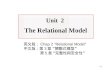
重点插图 在 SWEDEHEART 注册研究和 DAPT 研究中缺血和出血事件发生率
SWEDEHEART 双联抗血小板治疗研究(安慰剂)
心肌梗死或支架内血栓
累计
发病
率(
%)
累计
发病
率(
%)
累计
发病
率(
%)
累计
发病
率(
%)
累计
发病
率(
%)
累计
发病
率(
%)
8
7
6
5
4
3
2
1
0
4.5
3.0
高分(≥2)
低分(<2)
高分(≥2)
低分(<2)
高分(≥2)
低分(<2)
高分(≥2)
低分(<2)
高分(≥2)
低分(<2)
高分(≥2)
低分(<2)
8
7
6
5
4
3
2
1
0
5.7
2.3
主要心血管和脑血管不良事件
8
7
6
5
4
3
2
1
0
7.1
5.8
8
7
6
5
4
3
2
1
0
7.6
3.8
致命性出血或大出血/链激酶和组织纤溶酶
原激活剂在治疗闭塞动脉的全球应用(GUSTO)中的
中度或重度出血
8
7
6
5
4
3
2
1
0
0.7 0.8
8
7
6
5
4
3
2
1
0
1.4 1.4
在SWEDEHEART注册研究(n=41,101)和DAPT研究的安慰剂组(n=5,786)中,冠状动脉支架术后第12个月至第30个月高分和低分患者的事件累积发生率。 出血结果为致死性或大出血,如SWEDEHEART注册研究中的在线表3和DAPT研究中的GUSTO中度或重度出血所定义。 冠状动脉支架术后30个月,7.9%的SWEDEHEART患者仍在接受DAPT治疗(高分组为10.0%,低分组为6.2%)。

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
18
分位数的 4.3 个百分点(观察的风险 7.9%与预测的风险
12.1%)(在线图 1)。出血模型的 C 统计量为 0.67(95% CI:0.63-0.70)(在线表 6),并且风险始终被高估,过高
估计的风险从最低风险五分位数的 0.5 个百分点(观察
的风险 0.3%与预测的风险 0.8%)至最高风险五分位数
的 2.4 个百分点(观察的风险 1.8%与预测的风险 4.2%) (在线图 2)。PCI 指数中有无发生 MI 的患者和接受新一
代支架的患者区分和校准情况大致相似(在线表 6,在
线图 1 和 2)。缺血和出血预测模型的 Cox 回归系数和
SWEDEHEART 注册研究中估计系数如在线表 7 中所示。
SWEDEHEART 注册研究与 DAPT 研究中缺血和出血事件发生率的比较 PCI 术后第 12 个月至第 30 个月,与 DAPT研究中接受安慰剂的患者相比,SWEDEHEART 注册研究
关于MI和支架内血栓形成的累积发生率的绝对差异更小,
同时 DAPT 评分高分与低分患者 MACCE 的绝对差异也
较小(重点插图)。SWEDEHEART 注册研究 DAPT 评分
高的患者 MI 或支架内血栓形成发生率低于 DAPT 研究
中高评分患者(Kaplan-Meier 调整累积发生率,4.5% vs. 5.7%),而 SWEDEHEART 注册研究 DAPT 低评分患者上
述发生率则高于 DAPT 研究中相应患者(3.0% vs.2.3%)。 SWEDEHEART 注 册 研 究 和 DAPT 研 究 中 高 分 患 者 的
MACCE 的发生率分别为 7.1%和 7.6%,低分患者该数值
分别为 5.8%和 3.8%。SWEDEHEART 注册研究发生致
命性出血或大出血的发生率低于 DAPT 研究中安慰剂组
GUSTO 中重度出血风险的发生率(高分 0.7% vs. 1.4%;
低分 0.8% vs. 1.4%)(重点插图)。
DAPT 评分对缺血和出血风险进行分层的能力 研究人群
中 DAPT 评分的分布如图 2 所示。DAPT 评分的 C 统计
量对 MI 或支架内血栓形成事件为 0.58(95% CI:0.56-0.60), 对 MACCE 为 0.54(95 % CI:0.53-0.55), 对 于
致命或重大出血事件为 0.49(95% CI:0.45-0.53),对于
需要住院治疗的致命或大出血或出血事件为 0.48(95%
CI:0.46-0.51)。在索引 PCI 中有无发生 MI 的患者和接受
新一代支架的患者中区分度相似(表 3)。在线表 8 中显示
了 DAPT 评分中每个组分的缺血和出血结果的风险比。
与评分低的患者相比,评分高的患者 MI 或支架内
血栓形成率明显较高(累计发生率 4.5% vs. 3.0% ;HR:
1.52;95% CI:1.36-1.69),同时 MACCE 发生率也较高
(7.1% vs. 5.8% ;HR:1.23;95% CI:1.14-1.34)。高分 患者与低分患者的心肌梗死或支架血栓形成率的差异在很 大程度上取决于评分为 3 分(HR vs. 评分 -2 和 -1:1.94;
95 % CI:1.47-2.57)、4 分(HR:3.38;95 % CI:2.51-4.56)、≥ 5 分(HR:4.99;95% CI:3.60 至 6.91),而评
分为 0 至 2 分的患者的比率相似。MACCE 事件发生率也
没有随着得分水平线性增加。与评分为 -1 和 -2 的患者相
比,评分为 1 和 2 的患者 MACCE 事件发生率较低,并
且仅在评分为 4 和≥ 5 时显著增加(表 4)。
在致命性出血或大出血事件发生率上高分组与低分
组相似(累计发生率 0.7% vs. 0.8% ;HR:0.88;95%
CI:0.69-1.12),在需要住院治疗的致命性出血或大出血
图 2 DAPT 评分分布
患者
,%
30年龄,岁
65–<75
吸烟
糖尿病
出现MI
既往PCI或既往MI
紫杉醇洗脱支架
支架直径<3 mm
充血性心力衰竭或LVEF<30%
静脉移植支架
分数DAPT评分变量
<65
–2
–1
1
1
1
1
1
1
2
2
总评分范围:-2-10
0 20
10
0–2 –1 0 1 2 3 4 5 6 7 8 9 10
DAPT评分
SWEDEHEART注册研究人群(n = 41,101)中DAPT评分分布。 LVEF =左心室射血分数; MI=心肌梗死; 其他缩写如图1所示。

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
19
或出血事件发生率上两组也相似(2.1% vs. 2.4% ;HR:
0.89;95% CI:0.77-1.02)。尽管各评分水平之间风险的
绝对差异很小,但致命性出血或大出血风险与评分之间的
关系并非线性:与评分为 -2 和 -1 时相比,风险在评分为 2时显著降低,并且在评分≥ 5 时趋向于增加(表 5)。尽管在
≥ 5 分的亚组中的患者发生致命性出血或大出血的比率显著
较高,但是在 PCI 中有无发生 MI 的患者和接受新一代支架
治疗的患者中发生率大致相似(在线表 9 至 11)。
讨论
DAPT 评分已被纳入美国和欧洲 DAPT [3,4] 的指南更
新,因此评估其在日常临床实践中的表现显得越来越重
要 [17]。之前对 DAPT 评分的分析仅限于临床试验和几年
前的一项日本患者队列研究 [7-10]。我们的研究扩展了有关
DAPT 评分的现有数据,纳入未经选择的来自瑞典全国
41,101 名真实世界患者。
PCI 术后 12 个月至 30 个月,在出血风险方面 DAPT评分没有显示出区分度,同样在缺血风险方面的区分度
也不尽人意。尽管 DAPT 评分仍然可以识别高缺血风险
的患者,但风险并未随着评分水平线性增加。MI 或支架
内血栓形成的发生率仅在评分为 3 分或更高的患者中显
著升高。评分与 MACCE 事件风险之间关系呈 J 形,即
在评分为 1 和 2 时风险较低,在评分为 4 或更高时风险
增加。致命性出血或大出血事件风险在各评分水平之间
的绝对差异很小。若将分析限制在接受新一代药物洗脱
支架的患者时,这些研究结果仍然相似,这表明 DAPT评分在区分出血和缺血风险时不能发挥作用。尽管该评
分可能有助于识别高缺血风险的患者,但评分与缺血风
险之间的关系是非线性的,且不符合在评分≥ 2 的患者中
建议延长 DAPT 的决策规则。
与延长 DAPT 相关的缺血和出血风险之间的权衡,
受患者群体中缺血和出血事件发生率的影响。我们在新
人群中使用 DAPT 评分及其决策规则有一个重要假设,
即使用评分分层患者的缺血和出血事件发生率与 DAPT研究中的相似(即风险评分得到很好的校准)[17,18]。在
DAPT 评分高或者评分低的患者中,SWEDEHEART 注册
研究和 DAPT 研究之间的事件发生率明显不同。值得注
意的是,SWEDEHEART 注册研究致命或大出血事件的
表 3 DAPT 评分对缺血和出血终点的区分度
总计 新一代 DES 索引PCI 时存在MI 索引 PCI 时无 MI
MI 或支架内血栓 0.58 (0.56–0.60) 0.57 (0.54–0.59) 0.58 (0.56–0.60) 0.58 (0.55–0.61)
MACCE 0.54 (0.53–0.55) 0.54 (0.52–0.56) 0.54 (0.52–0.55) 0.54 (0.52–0.56)
致命或大出血事件 * 0.49 (0.45–0.53) 0.51 (0.46–0.57) 0.48 (0.43–0.52) 0.49 (0.42–0.56)
需住院治疗的致命或主要缺血事件或出血 ∗ 0.48 (0.46–0.51) 0.48 (0.45–0.51) 0.48 (0.46–0.51) 0.48 (0.45–0.52)
数值以Harrell’s C (95%置信区间)表示。∗在DAPT评分区分度分析中低分意味着更高的出血风险。MI=心肌梗塞;MACCE=主要不良心血管和脑血管事件;其他缩略词见表1。
表 4 支架植入后 12 至 30 个月根据 DAPT 评分分层后缺血终点发生率和风险比
评分 n (%)MI 或支架内血栓 MACCE
事件数 (IR)* 累积发生率 (%) 风险比 (95% CI) 事件数 (IR)* 累积发生率 (%) 风险比 (95% CI)
-2 和 -1 3,159 (7.7) 63 (17) 2.4 1.00 (ref) 171 (45) 6.5 1.00 (ref)
0 7,871 (19.2) 202 (21) 3.1 1.28 (0.96–1.70) 416 (44) 6.3 0.97 (0.81–1.16)
1 11,585 (28.2) 294 (21) 3.0 1.24 (0.94–1.63) 515 (36) 5.3 0.80 (0.67–0.95)
2 10,363 (25.2) 274 (21) 3.1 1.27 (0.96–1.67) 482 (37) 5.4 0.82 (0.69–0.97)
3 5,375 (13.1) 218 (32) 4.8 1.94 (1.47–2.57) 347 (52) 7.5 1.14 (0.95–1.36)
4 1,913 (4.7) 136 (56) 8.0 3.38 (2.51–4.56) 193 (80) 11.2 1.76 (1.44–2.17)
≥ 5 835 (2.0) 85 (83) 11.3 4.99 (3.60–6.91) 126 (124) 16.4 2.73 (2.17–3.44)
∗每1,000 人-年。CI=置信区间;HR=风险比;IR=发病率;其他缩略词见表1和3。

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
20
发生率约为 DAPT 研究中安慰剂组 GUSTO 中重度出血
发生率的一半。虽然这可能因为两项研究对出血事件的
定义不同以及健康登记中潜在风险未完全登记 [14],但本
研究中致命性出血或大出血事件发生率与其他真实世界
数据库 [19] 和临床试验 [2,7,20] 中冠心病患者人群相似。重要
的是,根据目前的指南 [3,4],SWEDEHEART 注册研究的
患者在 PCI 术后 DAPT 治疗可以小于 12 个月,而 DAPT研究中的所有患者都接受了至少 12 个月的 DAPT 治疗,
那些被认为具有高出血风险的患者可能被给予较短时间
的 DAPT 治疗,从而被排除在我们的分析之外。此外,
SWEDEHEART 注册研究的大多数患者接受了氯吡格雷
或替格瑞洛的 DAPT 治疗,而在 DAPT 研究中使用了氯
吡格雷或普拉格雷。
DAPT 研究与其他患者群体之间事件发生率的差异
已如前述 [7,9,10]。此外,在日本的 2 项临床试验和 1 项临
床登记研究的数据提示,DAPT 评分高的患者 MI 或支架
内血栓形成的发生率不到 DAPT 研究中的一半,而出血发
生率相似 [10]。因此,相比其他人群,在日本患者中预防出
血更为重要。而 SWEDEHEART 注册研究人群则具有相对
更高的缺血风险和更低的出血风险,这些研究表明 DAPT评分及其决策规则不能在所有人群中推广。其他可能影响
DAPT 评分的普遍性及其决策规则的因素包括:P2Y12 抑制
剂的类型对权衡缺血和出血风险的作用 [2,21,22],及分配给出
血和缺血事件的权重应该根据每种事件相关危害(例如,
死亡率)的类型决定 [23,24]。
研究局限 一项治疗绝对风险的增减不仅取决于在未经治
疗下患者发生事件的风险(正如本研究中所分析),还取
决于治疗效果的大小(相对风险)。我们无法观察 DAPT评分水平对延长 DAPT 效果或潜在效应的影响,因为在
SWEDEHEART 注册研究没有对 DAPT 时间进行随机化,
并且很少有患者在支架植入术后接受达到 30 个月的延长
DAPT[16]。因为 DAPT 研究人群的预测能力没有提高 [7],
所以在缺血和出血事件的预测模型中预测因子和 DAPT延长之间没有相互作用。虽然在 DAPT 研究中未经正式
风险评分验证,然而有迹象表明高分和低分的效果修正
可部分解释这两组不同的治疗效果。例如,DAPT 研究中
高分患者 GUSTO 为中重度出血的比率在第 30 个月为 1.8%,而第 12 个月为 1.4%(相对风险:1.3),而在低分数
患者中上述比率分别为 3.0%和 1.4%(相对风险:2.1)。
在真实世界人群中,延长 DAPT 的效果和得分水平的潜
在影响仍然值得进一步研究。
我们的研究存在许多缺陷。我们把所有患者都当做
是在 PCI 后 12 个月停用了 P2Y12 抑制剂治疗。尽管 PCI术后 30 个月仍接受 DAPT 的患者比例较小(7.9%),但
比起低分患者,在高分患者中该比例明显较高。这可能
导致我们低估了 DAPT 评分根据缺血和出血风险对患者
进行分层的能力。此外,我们用于识别健康登记簿中的
大出血事件的算法虽大致对应于 GUSTO 中重度出血定义,
但两者的定义不尽相同。最后的缺陷是我们仅使用健康注
册表来获取有关 DAPT 治疗状态、预测因子和相关结果信
息。瑞典登记数据在心血管结局方面具有良好的覆盖率 [25], 同时致命性或大出血事件的算法在验证研究中具有良好
的敏感性(84.5%)和特异性(95.9%)[14]。
结论
在一项纳入大量冠状动脉支架植入术后未经选择的
真实世界的瑞典患者研究中,我们发现 DAPT 评分不能
区分出血风险高低,对缺血风险的区分度亦不尽人意。
虽然评分可以识别高缺血风险的患者,但评分与缺血风
表 5 支架植入后 12 至 30 个月根据 DAPT 评分分层后出血终点发生率和风险比
评分 n (%)致命或严重出血 致命或严重出血或需住院治疗的出血
事件数 (IR)* 累积发生率 (%) 风险比 (95% CI) 事件数 (IR)* 累积发生率 (%) 风险比 (95% CI)
−2 和 −1 3,159 (7.7) 27 (7) 1.0 1.00 (ref) 88 (23) 3.3 1.00 (ref)
0 7,871 (19.2) 61 (6) 1.0 0.90 (0.57–1.41) 162 (17) 2.5 0.73 (0.56–0.95)
1 11,585 (28.2) 68 (5) 0.7 0.67 (0.43–1.04) 210 (15) 2.2 0.63 (0.49–0.81)
2 10,363 (25.2) 51 (4) 0.6 0.55 (0.34–0.87) 161 (12) 1.8 0.53 (0.41–0.69)
3 5,375 (13.1) 39 (6) 0.8 0.80 (0.49–1.31) 105 (15) 2.2 0.66 (0.50–0.88)
4 1,913 (4.7) 13 (5) 0.8 0.74 (0.38–1.43) 45 (18) 2.6 0.78 (0.55–1.12)
≥ 5 835 (2.0) 13 (12) 1.7 1.72 (0.89–3.33) 34 (32) 4.6 1.38 (0.93–2.05)
∗每1,000 人-年。缩略词见表1、3和4。

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
21
险之间的关系是非线性的,并且与延长 DAPT 的建议决
策不一致。与 DAPT 研究相比,致命或大出血事件发生
率显著偏低。研究结果表明 DAPT 评分及其延长 DAPT的决策规则可能在真实世界人群中不具有普适性。
通信地址 Dr. Peter Ueda, Clinical Epidemiology Division, Department
of Medicine, Solna, Eugeniahemmet, T2,Karolinska Institutet, 171 76
Stockholm, Sweden. E-mail: [email protected]. Twitter: @karolinskainst.
参考文献
1. Mauri L, Kereiakes DJ, Yeh RW, et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. N Engl J Med 2014;371:2155–66.2. Bonaca MP, Bhatt DL, Cohen M, et al. Long-term use of ticagrelor in patients with prior myocardial infarction. N Engl J Med 2015;372: 1791–800.3. Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2016;68:1082–115.4. Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur Heart J 2017;39:213–60.5. Matteau A, Yeh RW, Camenzind E, et al. Balancing long-term risks of ischemic and bleeding complications after percutaneous coronary intervention with drug-eluting stents. Am J Cardiol 2015;116:686–93.6. Joyner CD, Peters RJG, Afzal R, et al. Fondaparinux compared to enoxaparin in patients with acute coronary syndromes without ST-segment elevation: outcomes and treatment effect across different levels of risk. Am. Heart J 2009;157: 502–8.7. Yeh RW, Secemsky EA, Kereiakes DJ, et
al. Development and validation of a prediction rule for benefit and harm of dual antiplatelet therapy beyond 1 year after percutaneous coronary intervention. JAMA 2016;315:1735–49.8. Piccolo R, Gargiulo G, Franzone A, et al. Use of the dual-antiplatelet therapy score to guide treatment duration after percutaneous coronary intervention. Ann Intern Med 2017;167:17–25.9. Harada Y, Michel J, Lohaus R, et al. Validation of the DAPT score in patients randomized to 6 or 12 months clopidogrel after predominantly second-generation drug-eluting stents. Thromb Haemost 2017;117:1989–99.10. Yoshikawa Y, Shiomi H, Watanabe H, et al. Validating utility of dual antiplatelet therapy score in a large pooled cohort from 3 Japanese percutaneous coronary intervention studies. Circulation 2018;137:551–62.11. Stefanini GG, Holmes DR. Drug-eluting coronary-artery stents. N Engl J Med 2013;368: 254–65.12. Lagerqvist B, James SK, Stenestrand U, Lindbäck J, Nilsson T, Wallentin L. Long-term outcomes with drug-eluting stents versus baremetal stents in Sweden. N Engl J Med 2007;356: 1009–19.13. Jernberg T, Attebring MF, Hambraeus K, et al. The Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART). Heart 2010;96: 1617–21.
14. Friberg L, Skeppholm M. Usefulness of Health Registers for detection of bleeding events in outcome studies. Thromb Haemost 2016;116: 1131–9.1 5 . T h e G U S T O I n v e s t i g a t o r s . A n international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N Engl J Med 1993;329:673–82.16. Angerås O, Hasvold P, Thuresson M, Deleskog A, ÖBraun O. Treatment pattern of contemporary dual antiplatelet therapies after acute coronary syndrome: a Swedish nationwide population-based cohort study. Scand Cardiovasc J 2016;50:99–107.17. Royston P, Altman DG. External validation of a Cox prognostic model: principles and methods. BMC Med Res Methodol 2013;13:33.18. Van Calster B, Vickers AJ. Calibration of risk prediction models: impact on decision-analytic performance. Med Decis Mak 2015;35:162–9.19. Pasea L, Chung S, Pujades-Rodriguez M, et al. Personalising the decision for prolonged dual antiplatelet therapy: development, validation and potential impact of prognostic models for cardiovascular events and bleeding in myocardial infarction survivors. Eur Heart J 2017; 38:1048–55.20. Camenzind E, Wijns W, Mauri L, et al. Stent thrombosis and major clinical events at 3 years after zotarolimus-eluting or sirolimus-elut ing coronary stent implantat ion: a randomised, multicentre, open-label, controlled
观 点
患者治疗和操作技巧的能力 DAPT 评分是一种临床
决策工具,用于识别可能在冠状动脉支架植入术后
12 个月需继续双联抗血小板治疗的患者。当这项评
分应用于一个全国人群时,并且该人群不是当初推导
出该评分的人群,该评分不能充分区分缺血和出血风
险,其与缺血风险的关系与延长治疗的决策不一致,
并且出血风险低于 DAPT 研究(DAPT 评分从该研究
推导出)。
转化前景 冠状动脉支架植入术后 12 个月以后,需要
更好的评分工具来识别最有可能从延长 DAPT 中获益
的患者。

JACC VOL. 72, NO. 10, 2018SEPTEMBER 4, 2018:1069–78
Ueda et al .DAPT 评分在瑞典数据中的验证
22
trial. Lancet 2012; 380:1396–405.21. Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2009;361:1045–57.22. Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2007;357: 2001–15.23. Valgimigli M, Costa F, Lokhnygina Y, et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute
coronary syndrome: lessons f rom the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur Heart J 2016;38:ehw525.24. Mehran R, Pocock SJ, Stone GW, et al. Associations of major bleeding and myocardial infarction with the incidence and timing of mortality in patients presenting with non-ST-elevation acute coronary syndromes: a risk model from the ACUITY trial. Eur Heart J 2009;30:1457–66.
25. Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health 2011;11:450.
关键词 出血,双联抗血小板治疗,心肌梗塞,
风险预估,风险评分
附录 有关扩展的方法和参考部分以及补充
表格和图表,请参阅本文的线上版本。
中国医学科学院阜外医院 高展 窦克非 徐波
经皮冠状动脉介入治疗(PCI)术后 12 个月后,是否继续双联抗血小板(DAPT)治疗需要评估患者缺血和出血
的风险。DAPT 研究得出的 DAPT 评分能够定量评估患者的这两种风险。该评分系统包含 9 个临床指标:年龄、吸
烟、糖尿病、心梗、既往 PCI、紫杉醇 DES、支架直径 <3mm、LVEF<30% 及静脉桥血管。根据这 9 个临床指标患者
得出一个 -2 到 10 分的 DAPT 评分。这个评分对缺血和出血同时具有预测价值,更加重要的是如果 DAPT 评分≥ 2 分,
患者缺血的风险大于出血,反之出血的风险大于缺血,这样就能根据 DAPT 评分来指导患者 DAPT 的疗程。据此,
DAPT 评分被欧美的指南推荐作为指导 PCI 患者双抗疗程的工具。但是这个评分系统需要大样本外部数据验证才能证
明其有效性。Ueda 教授等近期在 JACC 发表了针对 DAPT 评分预测缺血和出血的研究。研究纳入了来自瑞典 2006-2014 年 41,101 例接受 PCI 的患者,这些患者接受 12 个月 DAPT 且没有发生缺血及出血事件,继续随访 12-30 个月。
研究发现,DAPT 评分对心梗或支架血栓的预测价值是 0.58(95% CI:0.56-0.60),对 MACCE(死亡 / 心梗 / 卒中)
的预测价值是 0.54(95% CI:0.53-0.55),对主要出血事件的预测价值是 0.49(95% CI:0.45-0.53)。当 DAPT 评分
≥ 3 分时,心梗或支架血栓明显增加;当 DAPT 评分≥ 4 分时,MACCE 明显增加;但这些缺血事件和 DAPT 评分之
间表现为 J 型曲线而非线性关系。研究者认为,DAPT 评分对 PCI 术后患者延长 DAPT 的出血风险没有预测价值,而
对缺血的预测价值也很有限;DAPT 评分并不适用作为真实世界的 PCI 患者出血和缺血的预测工具,也无法指导接受
PCI 患者的 DAPT 疗程。该研究样本量大,反映现代 PCI,得出的结论有很高的价值。本研究使 DAPT 评分的临床价
值受到了挑战,尽管用评分工具指导医生对患者进行个体化治疗的方向是正确的,但寻找出准确的评分任重而道远。
点 评

JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY ©2018 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
VOL. 72, NO. 17, 2018ISSN 0735-1097
急性冠脉综合征患者行完全血运重建与单纯罪犯血管血运重建的对比研究Complete Versus Culprit-Only Lesion Intervention in Patients With Acute Coronary Syndromes
Krishnaraj S. Rathod, MD,a Sudheer Koganti, MD,a Ajay K. Jain, MD,a Zoe Astroulakis, MD, PHD,b Pitt Lim, MD,b Roby Rakhit, MD,c Sundeep Singh Kalra, MD,c Miles C. Dalby, MD,d Constantinos O’Mahony, MD,a Iqbal S. Malik, MD,e Charles J. Knight, MD,a Anthony Mathur, MD, PHD,a Simon Redwood, MD,f Alexander Sirker, MD, PHD,a Philip A. MacCarthy, MD, PHD,g Elliot J. Smith, MD,a Andrew Wragg, MD, PHD,a Daniel A. Jones, MD, PHDa
翻译:湖州市中心医院心内科 胡欢欢;审校:中国医学科学院阜外医院 宋莹
摘 要
背景 大部分急性非 ST 段抬高型心肌梗死(non–ST-segment elevation myocardial infarction, NSTEMI)患者存在多
支血管病变(multivessel disease, MVD)。而对于这组患者行完全冠状动脉血运重建的作用尚不确定。
目的 本研究的目的是在大型同期经皮冠状动脉介入治疗(percutaneous coronary intervention, PCI)的 NSTEMI 患者中进行队列研究,比较完全血运重建和单纯罪犯血管血运重建的预后差别。
方法 本研究是一项观察性的队列研究,纳入 2005 年至 2015 年伦敦 8 个心脏病中心接受治疗的 37,491 例
NSTEMI 患者。临床详细数据见接受介入手术时录入英国心脏介入学会(British Cardiac Intervention Society, BCIS)的 PCI 数据集。总计 21,857 例(58.3%)NSTEMI 合并 MVD 的患者。主要终点是中位随访 4.1 年的全因
死亡率(四分位间距:2.2-5.8 年)。
结果 总计 11,737 例(53.7%)行 PCI 的 NSTEMI 患者接受了同期完全血运重建,该比例在研究期间显著提
高(P=0.006)。与单纯罪犯血管血运重建组相比,完全血运重建组的患者年龄更大,男性更多,更多合并糖尿
病、肾脏疾病和既往心肌梗死 / 血运重建史。虽然两组住院期主要心脏不良事件粗发生率相当(5.2% vs. 4.8%;
P=0.462),但是 Kaplan-Meier 分析显示,两组患者随访期间死亡率有显著差异(完全血运重建组:22.5% vs. 单纯
罪犯血管血运重建组:25.9%;P= 0.0005)。多因素 Cox 分析显示:倾向性匹配前(风险比:0.90;95% 置信区间:
0.85-0.97)及倾向性匹配后(风险比:0.89;95% 置信区间:0.76-0.98),完全血运重建组患者全因死亡风险均降低。
结论 在伴有 MVD 的 NSTEMI 患者中,与接受单纯罪犯血管 PCI 相比,接受同期完全冠状动脉血运重建的患
者虽然住院期死亡率较高,但远期死亡率可能降低。未来还需更多随机研究证实这些发现。(J Am Coll Cardiol 2018;72:1989–99) © 2018 by the American College of Cardiology Foundation.
From the aBarts Health NHS Trust, London, United Kingdom; bSt. George' s Healthcare NHS Foundation Trust, St. George' s Hospital, London, United Kingdom; cRoyal Free London NHS Foundation Trust, London, United Kingdom; dRoyal Brompton & Harefield NHS Foundation Trust, Harefield Hospital, Middlesex, London, United Kingdom; eImperial College Healthcare NHS Foundation Trust, Hammersmith Hospital, London, United Kingdom; fSt. Thomas' NHS Foundation Trust, Guys&St. Thomas Hospital, London, United Kingdom; and the gKings College Hospital, King' s College Hospital NHS Foundation Trust, Denmark Hill, London, United Kingdom. Dr. Dalby has received research grants from Abbott Vascular, Daiichi-Sankyo/Lily, and Sanofi; and has been a consultant for AstraZeneca, Eli Lilly, Medtronic, Edwards Lifesciences, and Boston Scientific. Dr. Smith has received speakers fees/honoraria from Boston Scientific, Abbott Vascular, Vascular Perspectives, and Biosensors International. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.Manuscript received March 20, 2018; revised manuscript received June 29, 2018, accepted July 30, 2018.
PUBLISHED BY ELSEVIER https://doi.org/10.1016/j.jacc.2018.07.089

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
24
在接受冠状动脉造影的
急 性 非 ST 段 抬 高 型 心 肌 梗
死(non-ST-segment elevation myocardial infarction, NSTEMI)患者中,50% 的患者合并多支
血 管 病 变(multivessel disease, MVD)[1,2]。最新的随机试验和
荟萃分析 [3-17] 显示:合并 MVD 的急性 ST 段抬高型心肌梗死
(ST-segment elevation myoca-rdial infarction, STEMI) 患 者,
多支血管血运重建相较于单纯
罪犯血管血运重建降低非计划
性再次血运重建术 [3,7-11,13,14,16]、
全因死亡率 [9]、心源性死亡 率 [3,9,16] 和再发梗死 [9,10,14]。合
并 MVD 的 NSTEMI 患者完全
血运重建的获益尚不清楚。尽管欧洲心脏病学会和美国心
脏病学会指南都建议高危患者行早期介入治疗 [18,19],但血
运重建策略并没有明确推荐。
已有研究证实,NSTEMI 后不完全血运重建患者的
短期和长期预后较差 [20,21]。小规模研究提示,完全血运
重建可改善这组患者的预后 [22-28]。然而尽管替代建议有
利,但近期的荟萃分析并未发现完全血运重建的主要不
良 心 脏 事 件(major adverse cardiac event, MACE) 明 显
减少或死亡率获益 [21],因此,这一话题仍然有一些重要
且未解决的问题,包括血运重建的时机以及完全血运重
建是否真的优于单纯罪犯血管的治疗。本研究旨在当代
大样本连续入组的接受冠状动脉介入治疗(percutaneous coronary intervention, PCI)的 NSTEMI 合并 MVD 的患者
队列中,分析比较完全血运重建与单纯罪犯血管(culprit vessel, CV)血运重建的比例以及长期预后。
方法
本研究是观察性队列研究,使用来自伦敦 8 个心脏
中心登记在 BCIS(英国心脏介入学会)数据集的数据。
研究数据 英国 BCIS 审计收集英国所有行 PCI 的医院数
据,并详细记录每例手术信息 [29]。该数据库是由英国国
家心血管预后研究所赞助收集的数据集的一部分,符合
英国的数据保护法规。数据由每家医院在手术时前瞻性
地收集,经过电子加密,然后在线传输到中央数据库。
每个纳入患者提供详细的住院信息,包括入院的方式和
时间、住院调查、结果、治疗和预后。住院期间同时记
录患者的临床和人口学数据、手术特征、出血并发症、
手术并发症、住院期全因死亡率、非致死性心肌梗死
(myocardial infarction, MI)、再次介入治疗和卒中。患者
的生存数据是通过患者的国民健康服务号码与国家统计
局联系获得的,国家统计局记录了所有死亡患者的生存 /死亡状况和死亡日期。
研究人群及设计 我们检索出 2005 年 1 月至 2015 年 5 月
期间在英国伦敦所有 8 个三级心脏中心接受 PCI 治疗的 37,491 例 NSTEMI 患者。在伦敦没有其他的中心能进行
急性冠脉综合征的 PCI 治疗。将来自国家统计局的关联
死亡数据的匿名数据集合并到 8 个中心进行分析。数据
排除了出现心源性休克的患者、既往冠状动脉搭桥术史
以及心肌梗死溶栓后冠状动脉内血流灌注(Thrombolysis In Myocardial Infarction, TIMI) 血 流 0 级 的 非 CV 慢 性
完全闭塞的患者。研究队列最终纳入 21,857 例(58.3%)
NSTEMI 合并 MVD 的患者。MVD 采用标准定义,指在
两个或多个主要心外膜动脉中存在≥ 75% 的管腔内狭窄[30]。患者分为 CV 组或完全血运重建组(即相同条件下血
运重建组)。结合患者症状、心电图改变以及心肌酶升高(与
NSTEMI 一致),来评估 PCI 指征。冠状动脉造影通过桡
动脉或股动脉进行。罪犯血管确定后使用造影导丝穿过。
是否进行人工血栓抽吸,由术者决定,然后采用常规 PCI方法在 CV 置入支架。是否进行生理学和腔内影像学评估,
由术者决定。
临床终点 主要临床终点是中位时间 4.6 年(四分位间距:
2.2-6.2 年)的全因死亡率。死亡数据来自国家统计局。住
院期 MACE 定义为死亡、MI(定为:治疗相关冠脉区域
新的病理性 Q 波形成,并伴随肌酸激酶 MB 升高至大于
或等于参考值的两倍或肌钙蛋白生物标志物的显著升高)、
卒中以及再次靶血管血运重建。手术并发症包括 MI、急
诊冠状动脉搭桥术、动脉并发症、主动脉 / 冠状动脉夹
层、分支闭塞和心律失常。出院后通过国家统计局获得
长期全因死亡率。手术成功的定义为手术结束时 CV 最
终 TIMI 血流 3 级及罪犯动脉残余狭窄 <20%。
伦理 这些数据是国家强制性心脏审计的一部分,所有可
识别患者身份的字段在分析之前都被删除。地方伦理委
员同意不需要正式的伦理批准。
统计分析 比较行完全血运重建与单纯罪犯血管治疗患者
缩略词表CI=confidence interval
置信区间
CV=culprit vessel
罪犯血管
GP=glycoprotein
糖蛋白
HR=hazard ratio
风险比
MACE=major adverse cardiac events
主要不良心脏事件
MI=myocardial infarction
心肌梗死
MVD=multivessel disease
多支血管病变
NSTEMI=non–ST-segment
elevation myocardial infarction
急性非ST段抬高型心肌梗死
PCI=percutaneous coronary
intervention
经皮冠状动脉介入治疗
STEMI=ST-segment elevation
myocardial infarction
急性ST段抬高型心肌梗死
TIMI=Thrombolysis In Myocardial
Infarction
心肌梗死溶栓后冠状动脉内血流灌注

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
25
的临床特征,分类变量采用皮尔逊卡方检验,连续变量
采用 t 检验。利用Shapiro-Wilks 检验评估数据的正态分布。
计算 Kaplan-Meier 乘积极限比较达到终点事件的累积发
生率,并使用 log-rank 检验证明两组之间存在统计学显
著差异。数据缺失时(左心室射血分数除外),将未知值
归入最常见的分类变量和连续变量的中位数或亚组特异
性中位数。随访时间从患者入院到终点事件(全因死亡率)。
采用前瞻性里程碑分析判断长期预后的差异是受短期效
应影响,还是 6 个月以上事件的累积效应。
采用 Cox 回归进行多因素分析。根据与终点相关的
协变量(P<0.05),估计年龄校正和完全校正模型中完全
血运重建的风险比(hazard ratios, HRs)。模型中协变量
包括年龄、性别、糖尿病、高血压、高胆固醇血症、既
往 PCI、既往 MI、慢性肾衰竭、术前 TIMI 血流分级、
研究时间、手术成功、左主干介入治疗和使用糖蛋白
(glycoprotein, GP)IIb/IIIa受体拮抗剂。通过检验 log(-log)
生存曲线来评估风险比例假设,并且采用 Schoenfeld 残
差进行测试。风险比假设适合所有终点事件评估。此外,
采用灵敏性分析来评估射血分数或既往 PCI 对多变量模
型的影响。
采用非简约的逻辑回归模型进行倾向评分分析比较
CV 介入和完全血运重建的预后。模型中多变量包括年
龄、性别、糖尿病、高血压、高胆固醇血症、既往 PCI、既往 MI、慢性肾功能衰竭、术前 TIMI 血流分级、手术
成功、左主干介入治疗和使用 GP IIb/IIIa 受体拮抗剂。
在对倾向性评分进行升序排序后,采用邻近法进行 1:1匹配,卡钳值设为 0.2 SDs。每例 CV 介入和完全血运
重建患者最多使用 1 对匹配样本,保证组间基线特征分
布的匹配。基于匹配的样本,采用 Cox 比例风险模型确
定完全血运重建与随访死亡率的关系。所有分析都使用
STATA 版本 14(StataCorp, College Station, Texas)。
结果
本研究共纳入 21,857 例患者,平均年龄为 67.3 岁, 其中男性占 74.3%;高血压占 58.0%,血脂异常占 56.0%, 现行或既往吸烟者占 52.2%,糖尿病占 29.8%。大多数
PCI 手术都是通过股动脉途径进行的,占整个研究期间手
术的 70.2%。
其中 11,737(53.7%)例患者行 PCI 时接受了完全血
运重建(完全血运重建组),而 10,120(46.3%)没有接
受(CV 组)。MVD 患者比例从 2005 年的 26.3% 上升到 2015 年 的 35.9%( 图 1A),NSTEMI 合 并 MVD 患 者 接
受 PCI 完全血运重建的比例也随之增加(图 1B)。完全
血运重建比例在不同的心脏中心分布不同(范围 38.1%-79.2%)(图 2)。
患者特征 总体而言,与单纯罪犯血管血运重建组相比,
完全血运重建的患者年龄更大,女性更多,合并糖尿病
更多、存在肾脏疾病、既往 MI 史和既往血运重建(表 1)。
两组患者从症状发作或入院到血运重建的时间无差异。
图 1 研究期间 NSTEMI 合并 MVD 患者的百分比和完全血运重建率
NST
EMI合
并多
支血
管病
变患
者的
百分
比
50A
45
40
35
30
5
10
15
20
25
0
2005
2006
2009
2008
2007
2010
年度20
1120
1220
1320
1420
15N
STEM
I合并
多支
血管
病变
患者
行完
全血
运重
建介
入的
百分
比
80
B
7075
6560555045
51015
2520
3530
40
0
2005
2006
2009
2008
2007
2010
年度20
1120
1220
1320
1420
15
(A)在2005年至 2015年期间接受PCI治疗的NSTEMI合并MVD患者的百分比;(B)2005年至2015年期间NSTEMI合并MVD患者行PCI完全血运重建率。MVD=多支血管病变;NSTEMI=急性非ST段抬高型心肌梗死;PCI=经皮冠状动脉介入治疗。

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
26
图 2 各 PCI 中心的 NSTEMI 患者比率
NST
EMI合
并多
支血
管病
变患
者行
完全
血运
重建
介入
的百
分比 100
9590858075706560
510152025303540455055
01 2 3 4
PPCI中心5 6 7 8
各PCI中心NSTEMI合并MVD 患者的完全血运重建率。PPCI=急诊经皮冠状动脉介入治疗;其他缩写如图1所示。
表 1 完全血运重建组和单纯罪犯血管血运重建组的基线特征
完全血运重建组(n = 11,737)
单纯罪犯血管血运重建组(n= 10,120)
P 值
年龄,岁 68.93 ± 12.59 67.63 ± 12.03 <0.0001
男性 8,521 (72.6) 7,671 (75.8) <0.0001
种族,白人 4,871 (41.5) 3,663 (36.2) <0.0001
既往 MI 6,885 (58.7) 4,412 (43.6) <0.0001
既往 PCI 2,958 (25.2) 1,791 (17.7) <0.0001
高胆固醇血症 6,526 (55.6) 5,687 (56.2) 0.539
糖尿病 4,375 (37.3) 3,168 (31.3) <0.0001
高血压 6,690 (57.0) 5,920 (58.5) 0.091
吸烟史 6,045 (51.5) 5,353 (52.9) 0.122
PVD 563 (4.8) 526 (5.2) 0.41
既往 CVA 534 (4.5) 395 (3.9) 0.173
肾脏疾病 845 (7.2) 527 (5.2) 0.042
左室功能差,EF <35% 669 (5.7) 557 (5.5) 0.755
症状发作到血管造影,天数 5.65 (3.1–9.5) 5.12 (2.2–8.6) 0.859
初次血管造影医院报告,天数 2.83 (2.47–6.9) 2.65 (2.12–5.3) 0.786
数值表示为均值±SD、n(%)或中位数(四分位间距)。肾脏疾病定义为血清肌酐>200 mmol/l或肾脏替代疗法。CVA=脑血管意外;EF=射血分数;MI=心肌梗塞;PCI=经皮冠状动脉介入治疗;PVD=外周血管疾病。
手术特征和预后 手术时,完全血运重建组更有可能通过
股动脉穿刺以及更多使用 GP IIb/IIIa 抑制剂(表 2)。桡
动脉入路途径与死亡率降低相关。完全血运重建组病变
血管数、平均治疗血管数更多且血管长度更高。在两组
间 CV 的平均支架直径和手术成功率无差异。
住院期终点 完全血运重建组住院期死亡率较高,但再
次介入行 PCI 治疗率较低。这可能是两组间未校正的住
院期 MACE 率相当的原因(单纯罪犯血管血运重建组:
3.8% vs. 完全血运重建组:4.1%;P=0.462)(表 3)。此外,
完全血运重建组的动脉并发症发生率较高。
远期预后 患者中位随访时间为 4.6 年(四分位间距:2.2-6.2 年)。Kaplan-Meier 分析显示:两组患者死亡率有显著
统计学差异(单纯罪犯血管组:25.9% vs. 完全血运重建组:
22.5%;P=0.0005)(图 3)
全因死亡率的预测因子 年龄校正后的 Cox 分析(表 4、图 4)
显示:完全血运重建与全因死亡率降低相关(HR:0.86;
95% 置信区间 [confidence intervals, CI]:0.79-0.94)。多因
素校正后(图 4),完全血运重建仍是生存率预测因子(HR:
0.90;95% CI:0.85-0.97)。当校正射血分数(仅适用于
45% 的患者)(HR:0.84;95% CI:0.78-0.95)或 PCI 中心(HR:0.86;95% CI:0.80-0.94)时,结果仍然相同。
倾向性匹配 为了进一步解释混淆变量和偏倚,进行倾向
评分匹配以校正人口学和手术变量的差异。总计 19,980例患者(完全血运重建组 9,900 例,CV 介入组 9,900 例)。
匹配后,基线人口学和手术变量在两组倾向匹配队列中平

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
27
表 2 完全血运重建和罪犯血管介入组的手术特征
完全血运重建介入 (n = 11,737)
单纯罪犯血管血运重建(n= 10,120)
P 值
桡动脉入路行 PCI 3,369 (28.7) 3,137 (31.0) 0.006
病变血管数 2.38 ± 0.66 2.25 ± 0.46 0.259
平均治疗血管数 2.39 ± 0.81 1.00 ± 0.16 <0.0001
靶血管数
右冠状动脉 3,721 (31.7) 3,805 (37.6) <0.0001
左主冠状动脉 904 (7.7) 678 (6.7) 0.002
左前降支 3,850 (32.8) 2,763 (27.3) <0.0001
左回旋冠状动脉 3,263 (27.8) 2,874 (28.4) 0.138
TIMI 血流 3 级预处理 6,303 (53.7) 6,426 (63.5) <0.0001
平均支架直径 3.78 ± 4.86 3.59 ± 6.75 0.541
平均支架长度 46.98 ± 16.92 23.21 ± 12.75 <0.0001
IVUS 运用 381 (3.2) 250 (2.5) 0.258
DES 9,143 (77.9) 7,610 (75.2) 0.164
GP IIb/IIIa 拮抗剂 2,734 (23.3) 2,135 (21.1) 0.004
手术成功 10,822 (92.2) 9,371 (92.6) 0.776
数值表示为n(%)或平均值±SD。DES=药物洗脱支架;GP=糖蛋白;IVUS=血管内超声;PCI=经皮冠状动脉介入治疗;TIMI=心肌梗塞溶栓后冠状动脉内血流灌注。
表 3 完全血运重建组或 CV 介入组的住院期终点及 PCI 术后并发症情况
完全血运重建介入 (n = 11,737)
单纯罪犯血管血运重建(n= 10,120)
P 值
MACE 481 (4.1) 385 (3.8) 0.462
死亡 270 (2.3) 152 (1.5) 0.002
Q 波 MI 59 (0.5) 61 (0.6) 0.343
再次介入行 PCI 治疗 70 (0.6) 101 (1.0) 0.015
CVA 23 (0.2) 10 (0.1) 0.633
急诊 CABG 12 (0.1) 30 (0.3) 0.121
动脉并发症 70 (0.6) 40 (0.4) 0.008
出血并发症 106 (0.9) 81 (0.8) 0.845
数值表示为n(%)。CABG=冠状动脉旁路移植术;CV=罪犯血管;MACE=主要不良心脏事件;其他缩写如表1。
衡。倾向匹配队列的 Cox 回归分析显示:对于 NSTEMI合并 MVD 患者,PCI 时完全血运重建可降低全因死亡风
险(HR:0.89;95%CI:0.76-0.98)。 即 使 LV 功 能 纳 入
倾向匹配评分后,结论仍然一致(HR:0.86;95% CI: 0.65 到 0.96)。
里程碑分析 未匹配队列的 6 个月和 5 年死亡率的 Kaplan Meier 曲线如图 3 所示。在完全血运重建组中,由院内事
件导致的较高死亡率在 6 个月内消失,两组之间不再有显
著 差 异(HR:1.23;95%CI:0.74-3.22;P=0.285)。 应 用
里程碑分析后,在治疗后 6 个月至 5 年期间,接受完全血
运重建的患者与单纯罪犯血管治疗相比,全因死亡率显著
降低(HR:0.65;95%CI:0.35-0.82;P=0.0005)。
讨论
本研究是目前样本量最大的前瞻性、观察性、多中
心注册研究,旨在研究 NSTEMI 合并 MVD 患者行同期
完全血运重建对长期临床预后的影响。本研究基于超过
21,000 例患者预后的分析,有力的证明了与单纯罪犯血管

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
28
图 3 研究期患者的存活率
50
10
20
30
40
01 2 3 4 5
11737 9879 7854 5247 3698 1947
10120 9958 8256 6587 4318 2020
累积
全因
死亡
率发
生率
(%
)累
积全
因死
亡率
发生
率(
%)
累积
全因
死亡
率发
生率
(%
)累
积全
因死
亡率
发生
率(
%)
术后随访时间
术后随访时间 术后随访时间
术后随访时间
A
LR 检验 P = 0.0005
10
2
4
6
8
00 1.0 2.0 3.0 5.04.0 6.0
11737 11258 10472 10021
10120 10098 10056 9995
B
LR 检验 P = 0.285
50
10
20
30
40
01.50.5 1.0 2.0 3.02.5 3.5 4.54.0 5.0
10021
9995
9879
9958
7854
8256
5247
6587
3698
4318
1947
2020
风险暴露患者人数
完全血运重建
罪犯血管介入
风险暴露患者人数
完全血运重建
罪犯血管介入
风险暴露患者人数
完全血运重建
罪犯血管介入
风险暴露患者人数
完全血运重建
罪犯血管介入
C
LR 检验 P = 0.0001
50
10
20
30
40
01 2 3 4 5
9990
9990
9848
9953
7890
8252
5231
6584
3687
4316
1941
2019
D
LR 检验 P = 0.0001
完全血运重建 罪犯血管血运重建
Kaplan-Meier曲线显示了各组PCI术后5年全因死亡率的累积概率(A)、6个月内的全因死亡率的里程碑分析(B)、6个月到 5 年全因死亡率的里程碑分析(C)以及与19,980例患者倾向性匹配后的Kaplan-Meier 曲线(D)。LR =似然比;PCI=经皮冠状动脉介入治疗。
血运重建相比,完全血运重建可降低长期死亡率(重点插
图)。虽然完全血运重建组患者住院死亡率增加,分析考
虑可能与患者高风险和病情复杂相关。这提示对高风险患
者,术者更倾向选择完全血运重建(术者偏倚),而给患
者带来长期获益,并对这些因素进行校正。未来需要随机
研究来探讨这类患者是否能从完全血运重建中真正获益。
此外,里程碑分析结果表明:完全血运重建的死亡
获益在前 6 个月后出现。6 个月前的差异主要是来自于住
院死亡率(完全血运重建组:2.3% vs. 单纯罪犯血管血运
重建组:1.5%)。后续的里程碑分析支持 6 个月至 5 年内
完全血运重建的获益。
近期发表的一项荟萃分析支持了这一事实,其结果
与我们的研究结果非常相似,即在这组患者中,完全血
管重建可能会改善预后 [31]。该研究纳入 4 项 随机对照试
验的 838 例患者,研究发现:与分期多支血管 PCI 相比,
同期完全血管重建可显著降低非计划再次血管重建率,
有降低长期死亡和主要心脑血管不良事件风险的趋势;
然而,由于样本量小而无足够的效力表明这一点。我们
发现与单纯罪犯血管血运重建相比,同期完全血运重建
可改善死亡风险。本研究样本量大,为这一结论提供了
有力的证据。
STEMI 合并 MVD 患者在急诊 PCI 时行完全血运重
建支持证据较多。随机临床试验显示完全血运重建带来
显著获益 [32-34], 促进了指南最新调整 [19]。然而,PRAMI(心
梗死预防性血管成形)[32]、CvLPRIT(急诊 PCI 完全与罪
犯血管血运重建)[33],以及 DANAMI-3-PRIMULTI(ST 段
抬高型心肌梗死合并多支病变患者的急诊 PCI 策略:单纯
罪犯血管血运重建或完全血运重建)[34] 试验的结果是否能
推广到 NSTEMI 患者尚不清楚。与 DANAMI-3-PRIMULTI[34]
一致,部分研究者认为生理评估指导的血运重建策略将有

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
29
表 4 死亡率预测因子 Cox 比例模型的单因素和多因素分析
比较因子 单因素分析 多因素分析 *
年龄 年龄 1.07 (1.06–1.07) 1.07 (1.06–1.07)
男性 女性 1.30 (1.18–1.43) 1.02 (0.93–1.13)
种族(亚洲) 白人 1.32 (1.21–1.44) 1.22 (0.95–1.34)
糖尿病 非糖尿病患者 1.52 (1.39–1.67) 1.38 (1.25–1.62)
既往 MI 无既往 MI 1.62 (1.48–1.76) 1.12 (0.85–1.34)
既往 PCI 无既往 PCI 1.30 (1.17–1.44) 1.02 (0.93–1.15)
高血压 非高血压 1.39 (1.27–1.52) 1.06 (0.97–1.17)
高胆固醇血症 非高胆固醇血症 1.09 (0.997–1.19) NA
吸烟史 无吸烟史 1.16(1.07-1.27) 1.04(0.84-1.15)
eGFR < 60ml/(min·1.73 m2) eGFR>60ml/(min·1.73 m2) 4.16 (3.68–4.71) 2.80 (2.46–3.19)
EF < 35% EF > 35% 2.64 (2.27–3.05) 1.74 (1.52–1.88)
使用 GP IIb/IIIa 拮抗剂 未使用 GP IIb/IIIa 拮抗剂 0.68 (0.61–0.76) 0.89 (0.77–1.15)
手术成功 手术失败 0.94 (0.86–1.03) 0.91 (0.83–0.99)
入路途径,桡动脉 股动脉 0.84 (0.75–0.93) 0.85 (0.76–0.95)
LMS 介入治疗 非 LMS 介入治疗 0.77 (0.54–0.82) 0.72 (0.48–0.96)
手术年限 0.75 (0.74–0.95) 0.81 (0.68–1.12)
完全血运重建 罪犯血管介入 0.86 (0.79–0.94) 0.90 (0.85–0.97)
数值表示为风险比(95%置信区间)。*根据年龄、性别、既往MI、eGFR<60ml/(min·1.73 m2)、EF<35%、手术成功、多支血管病变、LMS 介入治疗和使用GP IIb/IIA拮抗剂进行校正。eGFR=肾小球滤过率;LMS=左主干;NA=不适用;其他缩写见表 1 和表 2。
图 4 总体人群的多因素回归分析
0
1.02 (0.93-1.13)
1.07 (1.06-1.07)
风险比(95%CI)
1.22 (0.95-1.34)
1.38 (1.25-1.62)
1.12 (0.85-1.34)
1.02 (0.93-1.15)
1.06 (0.97-1.17)
1.04 (0.84-1.15)
2.80 (2.46-3.19)
1.74 (1.52-1.88)
0.89 (0.77-1.15)
0.91 (0.83-0.99)
0.85 (0.76-0.95)
0.81 (0.68-1.12)
0.72 (0.48-0.96)
0.90 (0.85-0.97)
变 量
年龄
性别(男性)
种族(亚洲)
糖尿病
既往MI
既往PCI
高血压
吸烟史
CKD
射血分数<35%
GPIIb/IIa
手术成功
入路途径(桡动脉)
手术年份
LMS介入治疗
完全血运重建
多因素分析后风险比
0.5 1 1.5风险比
2 2.5 3.5 53 4.54
冠状动脉介入术后全因死亡的多因素 Cox 回归分析。 CKD=慢性肾病;GP= 糖蛋白;LMS=左主干。

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
30
助于改善接受 PCI 治疗的 MVD 患者的预后。在 FAME(血
流储备分数与血管造影对比评估)研究中,与标准血管造
影指导下的 PCI 相比,血流储备分数指导的 PCI 策略能显
著降低多支 CAD 患者 2 年的死亡或 MI 风险 [35]。
对于使用血管造影结果判断罪犯血管,STEMI 和
NSTEMI 患者存在重要差异;STEMI 患者更易判断,而
NSTEMI 患者并不可行。罪犯血管病变应满足至少以下
2 条标准:管腔内的充盈缺损、斑块溃疡、斑块不规则、
夹层或血流受损 [36-38]。大约 40% 的 NSTEMI 合并 MVD患者有超过一处斑块满足这些血管造影标准 [28,39],同时
25% 患者有一根动脉完全闭塞且多数已形成侧支循环 [38,40]。
在血管造影基础上,有一些方法可用于明确罪犯血管 [19],
包括梗塞区域局部心电图的 ST 段改变、超声心动图或心
室造影的节段性室壁运动减低、激发试验(如乙酰胆碱)
或光学相干断层扫描 [41-43]。本试验中完全血运重建的策略
确保 CV 得到治疗,与同期血管血运重建相比,后者可能
存在第二个不明显的罪犯血管没有得到治疗,以及血运重
建的优势与药物治疗相比是显而易见的。这可能是本研究
中完全血运重建获益的原因 [44-46]。
本研究并未探讨完全血管重建时机这一重要问题。
由于可以避免多支血管介入治疗术中的弊端,无论是住
院期还是出院后的分期完全血运重建均被推荐作为预防
血运重建的手段。遗憾的是,本研究数据集并未记录急
诊 PCI 时进行分期介入的原因。尽管排除了分期 PCI 前
死亡患者可能带来的生存偏倚,这仍然是本研究的一个
局限性。即使在伦敦,术者和医院不同,分期手术的时
机也各有不同;虽然有人认为 2 至 4 周是适当的等待
期,但考虑到报销、费用和再次入院的潜在处罚,这一
期限通常会延长到 30 天以上 [47]。最新的 SMILE(急性
非 ST 段 抬 高 型 心 肌 梗 死 [Non ST Elevation Myocardial
Infarction, NSTEMI] 合并多支血管病变患者不同治疗方
法影响)研究 [48] 将 542 例 NSTEMI 合并 MVD 的患者按
1:1 方式,随机分配至同期完全血运重建和单纯罪犯血管
血运重建后分期完全血运重建两组。同期完全血运重建
组在 1 年随访的主要不良心脑血管事件发生率显著降低。
这种差异完全来自于分期组中靶血管血运重建率升高,而
在临床硬终点(如死亡或 MI)方面两组间并无差异。该
研究支持同期完全血运重建,也印证了我们的研究结果。
优势和局限性 本研究的优势是纳入了来自一个大城市的
8 个不同中心的不同种族和社会构成的患者。研究纳入
大量合并症患者,因此更能代表日常临床实践中的人群。
重点插图 急性冠脉综合征合并多支血管病变患者行完全血运重建与单纯罪犯血管血运重建的生存曲线对比图
全因
死亡
率的
累积
发生
率(
%)
完全血运重建 罪犯血管血运重建
50
20
10
30
40
01 2 3
术后随访时间4 5
完全血运重建风险暴露患者数
9,848 7,890 5,231
似然比检验 P=0.0001
3,687 1,941罪犯血管介入 9,953
9,9909,990 8,252 6,584 4,316 2,019
Kaplan-Meier 曲线显示倾向性匹配后的19,980例多支血管病变合并急性非ST 段抬高型心肌梗死患者,行经皮冠状动脉介入治疗后全因死亡的累积概率。

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
31
虽然纳入这些患者可能会导致两组间存在基线差异,但
本研究采用多因素和倾向性匹配分析减少差异。本研究
死亡数据跟踪由英国国家统计局官方提供,死亡率终点
准确可靠。本研究数据集中,公认的死亡预测因素与不
良预后有关,因此,本研究的多因素分析结果可靠。
然而,我们的研究仍然有局限性。首先,我们的研
究仅适用于接受 PCI 治疗的 NSTEMI 患者,排除了非罪
犯血管慢性全闭塞和心源性休克的患者,这可能限制了
研究结果的普遍性。同时,这项研究和其他注册研究一
样,会受到非随机对照研究的所有潜在的偏倚和不可测
量的混淆因素影响。此外,我们的研究没有探讨是否需
要进行同期或分期完全血运重建的问题(即 4 至 6 周后
进行),因此,完全血运重建时机仍然是本文的一个重要
局限。最后,本研究开始于 2005 年,随着血流储备分数
测定、血管内超声、光学相干断层扫描和药物洗脱支架
使用的增加,目前的临床实践发生了显著的变化。这些
因素都应为未来的研究提供参考。
结论
对 NSTEMI 合并 MVD 的患者,与单纯罪犯血管血
运重建相比,同期完全冠状动脉血运重建可能带来长期
死亡的获益。研究仍需大样本随机对照试验证实,以有
效用于临床硬终点。
通 信 地 址 Dr. Daniel A Jones, Department of Cardiology, Barts Heart
Centre, St. Bartholomew 's Hospital, West Smithfield, London EC1A
7BE, United Kingdom. E-mail: [email protected]. Twitter: @
bhcintervention, @BartsIntervGrp.
观 点
患者治疗和操作技巧的能力 与 STEMI 患者相同,对
于 NSTMEI 合并 MVD 患者,同期完全多支血管经皮
冠状动脉介入治疗比单纯罪犯血管血运重建具有更好
的长期存活率。
转化前景 完全血运重建时机(即同期与分期血运重
建以及手术间隔)对改善接受 PCI 的 NSTEMI 合并多
支血管病变患者的预后十分重要。未来需要更多研究
探讨这一话题。
参考文献
1. Hassanin A, Brener SJ, Lansky AJ, Xu K, Stone GW. Prognostic impact of multivessel versus culprit vessel only percutaneous intervention for patients with multivessel coronary artery disease presenting with acute coronary syndrome. Euro-Intervention 2015;11:293–300.2. Hirsch A, Verouden NJ, Koch KT, et al. Comparison of long-term mortality after percutaneous coronary intervention in patients treated for acute ST-elevation myocardial infarction versus those with unstable and stable angina pectoris. Am J Cardiol 2009;104:333–7.3. Anantha Narayanan M, Reddy YN, Sundaram V, et al. What is the optimal approach to a nonculprit stenosis after ST-elevation myocardial infarction: conservative therapy or upfront revascularization? An updated meta-analysis of randomized trials. Int J Cardiol 2016;216:18–24.4. Bainey KR, Mehta SR, Lai T, Welsh RC. Complete vs culprit-only revascularization for patients with multivessel disease undergoing primary percutaneous coronary intervention for STsegment elevation myocardial infarction: a systematic review and meta-analysis. Am
Heart J 2014;167:1–14.e2.5. Bainey KR, Welsh RC, Toklu B, Bangalore S. Complete vs culprit-only percutaneous coronary in tervent ion in STEMI wi th multivessel disease: a meta-analysis and trial sequential analysis of randomized trials. Can J Cardiol 2016;32:1542–51.6. Bangalore S, Kumar S, Poddar KL, Ramasamy S, Rha SW, Faxon DP. Meta-analysis of multivessel coronary artery r e v a s c u l a r i z a t i o n v e r s u s c u l p r i t o n l y revascularization in patients with STsegment elevation myocardial infarction and multivessel disease. Am J Cardiol 2011;107:1300–10.7. Bangalore S, Toklu B, Wetterslev J. Complete versus culprit-only revascularization for STsegment- elevation myocardial infarction and multivessel disease: a meta-analysis and trial sequential analysis of randomized trials. Circ Cardiovasc Interv 2015;8:e002142.8. E lgendy IY, Wen X, Mahmoud A, Bavry AA. Complete versus culprit-only revascularization for patients with multi-vessel disease undergoing primary percutaneous coronary intervention: an updated meta-analysis of randomized trials. Circ Cardiovasc Interv 2016;88:501–5.
9. El-Hayek GE, Gershlick AH, Hong MK, et al. Meta-analysis of randomized controlled trials comparing multivessel versus culprit-only revascularization for patients with ST-segment elevation myocardial infarction and multivessel disease undergoing primary percutaneous coronary intervention. Am J Cardiol 2015;115:1481–6.10. Kowalewski M, Schulze V, Berti S, et al. Complete revascularisation in ST-elevation myocardial infarction and multivessel disease: meta-analysis of randomised controlled trials. Heart 2015;101:1309–17.11. Moretti C, D' Ascenzo F, Quadri G, et al. Management of multivessel coronary disease in STEMI patients: a systematic review and meta-analysis. Int J Cardiol 2015;179:552–7.12. Navarese EP, De Servi S, Buffon A, Suryapranata H, De Luca G. Clinical impact of simultaneous complete revascularization vs. culprit only primary angioplasty in patients with ST-elevation myocardial infarction and multivessel disease: a meta-analysis. J Thromb Thrombolysis 2011;31:217–25.13. Rasoul S, van Ommen V, Vainer J, et al. Multivessel revascularisation versus infarct-related artery only revascularisation during

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
32
the index primary PCI in STEMI patients with multivessel disease: a meta-analysis. Neth Heart J 2015;23:224–31.14. Sekercioglu N, Spencer FA, Lopes LC, Guyatt GH. Culprit vessel only vs immediate complete revascularization in patients with acute ST-segment elevation myocardial infarction: systematic review and meta-analysis. Clin Cardiol 2014;37:765–72.15. Sethi A, Bahekar A, Bhuriya R, Singh S, Ahmed A, Khosla S. Complete versus culprit only revascularization in acute ST elevation myocardial infarction: a meta-analysis. Circ Cardiovasc Interv 2011;77:163–70.16. Villablanca PA, Briceno DF, Massera D, et al. Culprit-lesion only versus complete multivessel percutaneous intervention in ST-elevation myocardial infarction: A systematic review and meta-analysis of randomized trials. Int J Cardiol 2016;220:251–9.17. Vlaar PJ, Mahmoud KD, Holmes DR Jr., et al. Culprit vessel only versus multivessel and staged percutaneous coronary intervention for multivessel disease in patients presenting with ST-segment elevation myocardial infarction: a pairwise and network meta-analysis. J Am Coll Cardiol 2011;58:692–703.18. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;64:e139–228.19. Roffi M, Patrono C, Collet JP, et al. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016;37:267–315.20. Hambraeus K, Jensevik K, Lagerqvist B, et al. Long-term outcome of incomplete revascularization after percutaneous coronary intervention in SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J Am Coll Cardiol Intv 2016;9:207–15.21. Mariani J, Macchia A, De Abreu M, Gonzalez Villa Monte G, Tajer C. Multivessel versus single vessel angioplasty in non-ST elevation acute coronary syndromes: a systematic review and metaanalysis. PloS One 2016;11:e0148756.
22. Brener SJ, Milford-Beland S, Roe MT, Bhatt DL, Weintraub WS, Brindis RG. Culprit-only or multivessel revascularization in patients with acute coronary syndromes: an American College of Cardiology National Cardiovascular Database Registry report. Am Heart J 2008;155:140–6.23. Ijsselmuiden AJ, Ezechiels J, Westendorp IC, et al. Complete versus culprit vessel percutaneous coronary intervention in multivessel disease: a randomized comparison. Am Heart J 2004;148:467–74.24. Kim MC, Jeong MH, Ahn Y, et al. What is optimal revascularization strategy in patients with multivessel coronary artery disease in non-ST-elevation myocardial infarction? Multivessel or culprit-only revascularization. Int J Cardiol 2011;153:148–53.25. Lee HJ, Song YB, Hahn JY, et al . Multivessel vs single-vessel revascularization in patients with non-ST-segment elevation acute coronary syndrome and multivessel disease in the drug-eluting stent era. Clinical Cardiol 2011;34:160–5.26. Palmer ND, Causer JP, Ramsdale DR, Perry RA. Effect of completeness of revascularization on clinical outcome in patients with multivessel disease presenting w i t h u n s t a b l e a n g i n a w h o u n d e r g o percutaneous coronary intervention. J Invasive Cardiol 2004;16:185–8.27. Rosner GF, Kirtane AJ, Genereux P, et al. Impact of the presence and extent of incomplete angiographic revascularization after percutaneous coronary intervention in acute coronary syndromes: the Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) trial. Circulation 2012;125:2613–20.28. Shishehbor MH, Lauer MS, Singh IM, et al. In unstable angina or non-ST-segment acute coronary syndrome, should patients with multivessel coronary artery disease undergo multivessel or culprit-only stenting? J Am Coll Cardiol 2007;49:849–54.29. Ludman PF. British Cardiovascular Intervention Society Registry for audit and quality assessment of percutaneous coronary interventions in the United Kingdom. Heart 2011;97:1293–7.30. Muller DW, Topol EJ, Ellis SG, Sigmon KN, Lee K, Califf RM, Thrombolysis and Angioplasty in Myocardial Infarction (TAMI) Study Group. Multivessel coronary artery disease: a key predictor of short-term prognosis
after reperfusion therapy for acute myocardial infarction. Am Heart J 1991;121:1042–9.31. Gaffar R, Habib B, Filion KB, Reynier P, Eisenberg MJ. Optimal timing of complete revascularization in acute coronary syndrome: a systematic review and meta-analysis. J Am Heart Assoc 2017;6:e005381.32. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med 2013;369:1115–23.33. Gershlick AH, Khan JN, Kelly DJ, et al. Randomized trial of complete versus lesion-only revascularization in patients undergoing primary percutaneous coronary intervention for STEMI and multivessel disease: the CvLPRIT trial. J Am Coll Cardiol 2015;65:963–72.34. Engstrom T, Kelbaek H, Helqvist S, et al. Complete revascularisation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3-PRIMULTI): an open-label, randomised controlled trial. Lancet 2015;386:665–71.35. Pijls NH, Fearon WF, Tonino PA, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol 2010;56:177–84.36. Libby P. Inflammation in atherosclerosis. Arterioscler Thromb Vasc Biol 2012;32:2045–51.37. Vergallo R, Ren X, Yonetsu T, et al. Pancoronary plaque vulnerability in patients with acute coronary syndrome and ruptured culprit plaque: a 3-vessel optical coherence tomography study. Am Heart J 2014;167:59–67.38. Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol 2006;47 Suppl:C13–8.39. Goldstein JA, Demetriou D, Grines CL, Pica M, Shoukfeh M, O' Neill WW. Multiple complex coronary plaques in patients with acute myocardial infarction. N Engl J Med 2000;343:915–22.40. Kastrati A, Neumann FJ, Schulz S, et al. Abciximab and heparin versus bivalirudin for non-ST-elevation myocardial infarction. N Engl J Med 2011;365:1980–9.41. de Winter RJ, Verouden NJ, Wellens HJ, Wilde AA. A new ECG sign of proximal LAD occlusion. N Engl J Med 2008;359:2071–3.

JACC VOL. 72, NO. 17, 2018OCTOBER 23, 2018:1989–99
Rathod et al .ACS 合并 MVD 患者行完全血运重建与单纯罪犯血管血运重建的对比研究
33
42. Kato M, Dote K, Sasaki S , e t a l . Presentations of acute coronary syndrome related to coronary lesion morphologies as assessed by intravascular ultrasound and optical coherence tomography. Int J Cardiol 2013;165:506–11.43. Tahvanainen M, Nikus KC, Holmvang L, et al. Factors associated with failure to identify the culprit artery by the electrocardiogram in inferior ST-elevation myocardial infarction. J Electrocardiol 2011;44:495–501.44. FRagmin and Fast Revascularisation during InStability in Coronary artery disease Investigators. Invasive compared with non-invasive treatment in unstable coronary-artery
disease: FRISC II prospective randomised multicentre study. Lancet 1999;354:708–15.45. Cannon CP, Weintraub WS, Demopoulos LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med 2001;344:1879–87.46. Fox KA, Poole-Wilson PA, Henderson RA, et al. Interventional versus conservative treatment for patients with unstable angina or non-ST-elevation myocardial infarction: the British Heart Foundation RITA 3 randomised trial. Randomized Intervention Trial of unstable Angina. Lancet 2002;360:743–51.
47. Dangas GD, George JC, Weintraub W, Popma JJ. Timing of staged percutaneous coronary intervention in multivessel coronary artery disease. J Am Coll Cardiol Intv 2010;3:1096–9.48. Sardella G, Lucisano L, Garbo R, et al. Single-Staged Compared With Multi-Staged PCI in Multivessel NSTEMI Patients: the SMILE trial. J Am Coll Cardiol 2016;67:264–72.
关键词 PCI,NSTEMI,多支血管介入治疗,
心肌梗死
哈尔滨医科大学附属第二医院 于波 代建南
包括 PRAMI、CvLPRIT、DANAMI-3-PRIMULTI 在内的多项随机对照研究已经证实伴随多支血管病变的 STEMI患者完全再血管化可显著改善患者预后(主要降低再血管化率)。然而,完全再血管化在 NSTEMI 患者中的作用尚缺
乏相关数据。本研究分析了来自英国伦敦的 8 个急性心肌梗死护理中心 10 年(2005 年至 2015 年)的数据提示,完
全再血管化可降低 NSTEMI 患者长期死亡率(6 个月之后长期死亡率可降低 35%),尽管可能伴随着更高的院内死亡
率。这项纳入 21,857 例患者的注册研究为 NSTEMI 患者完全再血管化的临床获益提供了真实世界的线索,但尚需大
型前瞻研究的证实,以排除注册研究可能掺杂的相关混杂因素。
点 评

JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY ©2018 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
VOL. 71, NO. 19, 2018ISSN 0735-1097
伴或不伴心力衰竭患者的 B 型钠尿肽水平和死亡率B-Type Natriuretic Peptide Levels and Mortality in Patients With and Without Heart Failure
Michelle K. York, BS,a,b,* Deepak K. Gupta, MD, MSCI,a,b,* Cassandra F. Reynolds, BS,a,b Eric Farber-Eger, BS,a,b Quinn S. Wells, MD, PHARMD, MSCI,a,b Katherine N. Bachmann, MD, MSCI,a,c,d Meng Xu, MS,a,e Frank E. Harrell, JR, PHD,a,e
Thomas J. Wang, MDa,b
翻译:浙江医院高血压中心 杨奕;审校:中国医学科学院阜外医院 吴伟春
摘 要
背景 心力衰竭(heart failure, HF)患者循环血液中 B 型钠尿肽(B-type Natriuretic Peptide, BNP)的浓度是死亡率的
强有力预测因子。心源性与非心源性的刺激因子均可影响 BNP 水平,表明 BNP 对非心衰患者也有类似的预测价值。
目的 本研究的目的是比较 BNP 在心力衰竭和非心力衰竭患者中预测价值的差异。
方法 采用范德堡大学医疗中心电子健康数据,研究了 30,487 例患者(平均年龄 63 岁,50% 为男性,17% 为黑人,
38% 为心衰患者),这些患者在 2002-2013 间第一次采集了血浆 BNP 并随访至 2015 年。根据 BNP 水平使用多元
Cox 比例风险回归模型计算死亡风险。
结果 非心衰患者的 BNP 水平(中位数 89 pg/ml;四分位间距:34-238 pg/ml)较心衰患者低(中位数 388 pg/ml; 四分位间距:150-940 pg/ml) (P< 0.0001)。年随访人数超过 90,898 例,其中 5,903 例非心衰患者(31%)和 6,181例心衰患者(53%)死亡。在多元模型中纳入了人口统计学和临床特征资料后,对于患者无论是否有心衰,BNP和年龄是最强的死亡预测因子。急诊、甚至是 BNP 适度升高的门诊病人中,心衰组和非心衰组根据 BNP 计算的
死亡风险相似。例如,BNP 水平在 400 pg/ml 时心衰组的 3 年死亡风险为 21%(95% 置信区间:20%-23%)而非
心衰组则为 19%(95% 置信区间:17%-20%)。
结论 在非心衰患者中,血浆 BNP 相较于传统的风险因子能更好地预测死亡风险。无论是否为心衰患者,其依据
BNP 水平预测的死亡风险相似,此结果在急诊患者中更为明显。(J Am Coll Cardiol 2018;71:2079–88)© 2018 by the American College of Cardiology Foundation.
钠尿肽是由心脏产生具有利尿钠作用的激素,具有
利尿和舒张血管的作用 [1]。当心室壁压力上升时 B 型钠尿
肽(B-type natriuretic peptide, BNP)应激分泌入血,BNP是临床诊断中强大的诊断生物标记物,用于区分心源性和
非心源性呼吸困难 [2-7]。循环血中钠尿肽水平与预后相关
(特别是在心力衰竭 [heart failure, HF] 患者中),较高水平钠
尿肽与复发性 HF 住院和死亡的较高风险相关 [4,8-11]。然而
在临床中,并不是所有监测 BNP 的患者均患有 HF。在临
床指导非 HF 患者中,对 BNP 水平预测意义知之甚少。因
循环中 BNP 的浓度也受到心内和容量负荷以外心内外刺
激因素的影响,故我们假设 BNP 的预测价值压 HF 和非
HF 中是相似的。
PUBLISHED BY ELSEVIER https://doi.org/10.1016/j.jacc.2018.02.071
From the aVanderbilt Translational and Clinical Cardiovascular Research Center, Vanderbilt University School of Medicine, Nashville, Tennessee; bDivision of Cardiovascular Medicine, Vanderbilt University School of Medicine, Nashville, Tennessee; cDivision of Endocrinology, Vanderbilt University School of Medicine, Nashville, Tennessee; dFaculty Research Scholars Program, Vanderbilt University School of Medicine, Nashville, Tennessee; and the eDepartment of Biostatistics, Vanderbilt University School of Medicine, Nashville, Tennessee. This work was supported by National Heart, Lung, and Blood Institute grants K12 HL109019, 1K23HL128928-01A1, and R01 HL131532 and the National Center for Advancing Translational Sciences of the National Institutes of Health (award UL1TR000445) (Vanderbilt University). The authors have reported that they have no relationships relevant to the contents of this paper to disclose. *Ms. York and Dr. Gupta contributed equally to this work and are joint first authors.Manuscript received October 30, 2017; revised manuscript received February 22, 2018, accepted February 25, 2018.

JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
35
本研究使用 13 年间范德堡大学医疗中心电子记录数
据,筛选出进行过血浆 BNP 浓度检测的成年患者。根据
心衰程度,我们量化了临床因素与 BNP 水平之间的关系。
接着对“根据循环血 BNP 水平预测死亡风险在心衰与非
心衰患者中效果近似”这一假设进行验证。
方法
研究人群 范德堡大学医疗中心合成衍生物是未确定的电
子健康数据的识别副本 [12]。 它包含了 20 年间就诊的近
2,500,000 例患者数据,其中包括搜索结构化的 [ 例如,
按 第 9 版 国 际 疾 病 分 类(International Classification of Diseases-9th Revision,ICD-9)编码的诊断,实验值 ] 和
非结构化的(例如,病例叙述部分)数据。从合成衍生物
中导出有 BNP 检查记录的(黑种人或白种人)成年人(≥ 18岁)数据。范德堡大学机构审查委员会批准该研究。
BNP、心衰和其他协变量 范德堡大学自从 2002 年起开始
施行血浆 BNP 临床检测。对于多次检测 BNP 患者,采纳
首次检测数值。生物站点 BNP 试验(生物站点诊断,圣
地亚哥,加利福尼亚)是 2007 年 2 月首次开展的临床试
验。2007 年 3 月至 2013 年 9 月, 使用 Beckman Coulter DXI 平台(Beckman Coulter, Brea, California)进行生物
站点 BNP 检测。上述平台均有 <12% 的系数变异率和 10 pg/ml 的浓度检测下限。
符合以下任一条件则归类为心衰患者:1)检索到 2条或以上 ICD-9 的心衰编码 428.x, 其中至少 1 条编码是
在进行 BNP 检验当天或首次 BNP 检测日录入;和 / 或 2)
正在使用静脉利尿剂在检验 BNP 的同一天或检验后 90天内有 1 条或多条 428.x 编码。设计这些标准是为了分
别找到慢性心衰和新确诊的心衰患者。混合表现型患者
(例如心衰和合并其他可导致呼吸困难的疾病,如哮喘、
慢性阻塞性肺病、肺炎和败血症)归类为心衰。
以检验 BNP 当日记录患者年龄。通过联合 ICD-9、
当前程序的组合术语代码和文本字符串(可在网上附录
中查看)[13] 提取冠状动脉疾病、高血压、肾脏病、糖尿
病状态;生命体征;人体测量数据和实验室数据。使用肾
脏疾病的饮食改变(Modification of Diet in Renal Disease,
MDRD)公式评估肾小球滤过率 [14]。在完成 BNP 检验前
最近的时间点内 90 天内 [15] 或之后,通过经胸超声心动
图报告来获取左心室射血分数(Left Ventricular Ejection Fraction,LVEF)数据。左心室舒张时室间隔厚度、后
壁和管腔直径与 LVEF 一样源于上述报告。依据美国超声
心动图学会推荐公式计算左
心室质量(g):0.8×{1.04× [(LVEDD+IVSd+PWTd)3- LVEDD3]}+ 0.6,LVEDD 代表左 心室舒张末期内径,IVSd 代
表舒张期室间隔厚度,PWTd 为舒张期左室后壁厚度。
全因死亡率 从社会保障管理
死亡文件链接查询到死亡信
息为确认死亡,这个数据可
近似覆盖全国死亡率 [17]。随
访阶段为检验 BNP 当日到死
亡日期,2015 年 12 月 31 日删减了在最后一次进行临床
随诊时还存活的患者。
数据分析 患者根据有无心衰进行分组。应用多元校正次
序回归分析检验与循环 BNP 水平相关的因素,从而避免
自变量与 BNP 之间的线性关系。在现有研究的基础上选
择协变量,其包括年龄、性别、种族、传统心血管风险
因素、身体质量指数(body mass index, BMI)、心率、脉压、
慢性肾脏病、评估肾小球滤过率、血糖、左心室质量和
LVEF。连续变量使用限制性三次样条建模(3 节)。包括
了心衰每个协变量的交互因素。绘制部分效应以描述协
变量与较高 BNP 优势对数之间的关系。
采用 KaplanMeier 法估计死亡率。根据 BNP 水平的
死亡风险,依据协变量调整后采用 Cox 比列风险回归模
型量化。在进入 COX 模型之前,对原始 BNP 值进行自
然对数变换然后使用限制性三次样条扩展从而避免假定
线性效应。为评估 BNP 死亡风险的增量值,从多元校正
Cox 模型中计算有或无 BNP 患者的 C 统计分析,并使用
似然比检验进行比较。丢失数据(在线表 1)使用累计
回归、自举和预测平均匹配进行多重插补。因样本量大,
故进行了 3 次插补。使用 R 语言进行分析(R 统计计算
基金会,维也纳,奥地利)。
结果
检测 30,487 例患者的 BNP 水平,62% 是非 HF。人
口统计学和临床 BNP 参数的关联性因心衰状态的不同而
变化(线上图 1)。表 1 展示了依据据心衰状态的研究样
本的特征。
血浆 BNP 的相关性 表 1 为心衰与非心衰患者中与循环血
液中 BNP 水平相关因子。用卡方值排序,在非心衰组与
缩略词表BMI= body mass index
体重指数
BNP= B-type natriuretic peptide
B型利钠尿肽
CI= confidence interval
置信区间
HF= heart failure
心力衰竭
HR= hazard ratio
危险比
ICD-9= International Classification of
Diseases 9th Revision
第9版国际疾病分类
LV= left ventricular
左心室
LVEF= left ventricular ejection fraction
左室射血分数

36 JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
血浆 BNP 最强的相关因素为年龄、BMI、LVEF 质量。在
心衰患者中,BMI、LVEF 和肾功能与血浆 BNP 呈强相关。
在两组中,女性、冠状动脉疾病、肾功能不全、心率加快、
年龄增长及左心室质量增加与 BNP 水平升高相关,然而
较高的 BMI 和 LVEF 与低水平 BNP 相关。(表 1,在线表 2)。
血浆 BNP 水平与死亡风险 通过对超过 90,898 例患者一
年的随访, 出现 6,181 (53%) 例心衰患者死亡和 5,903 (31%) 例非心衰患者死亡。表 2 为第 1、3、5 年的死亡率。
在多元校正 COX 模型中,较高的 BNP 是非心衰患者死
亡危险增高的强预测因子,而在心衰患者中它是次强预
测因子仅次于年龄(图 2,在线图 3)。非心衰患者中心率
增快是其次强死亡风险预测因子,而心衰患者中肾功能
不全是其第三位死亡预测因子。在两组中,糖尿病和低
LVEF 均与死亡危险增加有关。
随着 BNP 四分位数的增长(四分位间距)非心衰患
者将死亡风险提高 2 倍(风险比 [hazard ratio, HR]:2.08; 95% 置信区间 [confidence interval, CI]1.99-2.20)而与心衰
患者相似(HR:1.91;95% CI:1.75-2.08)。第二次分析限
于既不患有 HF 也不患有冠脉疾病(n=10,438)的患者,得
到了相似的结果(HR:1.89;95% CI:1.76-2.02)。针对所
表 1 范德堡大学医疗中心的成人 HF 患者第一次测量血浆 B 型钠尿肽时的基线特征非心衰患者 (n = 18,850) 心衰患者 (n = 11,637)
年龄,岁 61 (50–72) 66 (55–77)
性别 47 54
黑种人 17 17
冠状动脉疾病 45 76
高血压 77 86
慢性肾脏病 14 23
糖尿病 29 46
药物治疗
抗血小板药 48 60
β 受体阻滞剂 42 66
ACEI 或 ARB 42 61
盐皮质激素受体拮抗剂 4 13
硝酸盐 23 35
利尿剂 46 80
钙通道阻滞剂 29 29
其他降压药物 13 16
他汀类药物 37 51
心率,次 / 分 84 (72–99) 82 (70–96)
收缩压 , mmHg 126 (110–143) 122 (108–140)
舒张压 , mmHg 70 (59–80) 67 (58–79)
脉压 , mmHg 56 (44–70) 54 (41–68)
体重指数 , kg/m2 29 (25–35) 29 (25–35)
血糖 , mg/dl 105 (92–132) 111 (94–146)
eGFR, ml/(min ·1.73m2) 75 (53–94) 58 (39–79)
LVEF, % 55 (55–60) 52 (30–55)
LV 质量 , g 181 (145–225) 223 (172–286)
住院或急诊检测 BNP 69 66
BNP, pg/ml 89 (34–238) 388 (150–940)
自然对数 BNP, pg/ml 4.5 (3.6–5.5) 6.0 (5.0–6.8)
小于最低可检测浓度 BNP (<10 pg/ml) 2.9 0.5
值为中位数 (四分位间距) 或 %。ACE = 血管紧张素转换酶;ARB = 血管紧张素受体; BNP=B-型利尿钠肽; eGFR = 肾小球滤过率; HF=心力衰竭; LV=左心室; LVEF=左心室射血分数。

JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
37
图 1 根据不同心衰状态分组的血浆 BNP 在临床成人患者中的相关性。
0 100 200 300 400卡方
500 600 700 800 900
BMI
非心衰患者
年龄
冠状动脉疾病
心率
性别
eGFR
脉压
血糖
慢性肾病
糖尿病
左心室质量
高血压
左心室射血分数
种族
2
年龄
1
0对数
比
20 40 60 80 100
BMI
10 30 50 70
2
左心室射血分数
0
1
对数
比
20 40 60 80
左心室质量
100 300 500 700
2
eGFR
0
1
对数
比
0 10050 150 200
心率
50 100 150 200
BA
年龄
BMI
0 100 200 300 400卡方
500 600 700
心衰患者
冠状动脉疾病
心率
性别
eGFR
脉压
血糖
慢性肾病
糖尿病
左心室质量
高血压
左心室射血分数
种族
1年龄
0
对数
比
20 40 60 80 100
BMI
10 30 50 70
1
LVEF
0
对数
比
20 40 60 80
LV质量
100 300 500 700
0
1
eGFR
对数
比
0 10050 150 200
心率
50 100 150 200
DC
图A和C阐明了不同水平BNP相关变量(y轴)相对分布情况,按照多元校正模型的卡方值进行排序。卡方值通过模型中协变量的自由度分配进行校正,这样使每个协变量可在统一水平进行比较。例如,在非心衰患者中,年龄、BMI、左心室质量与BNP水平强相关。图B和D为部分效应图展示了特定临床参数与升高或降低的BNP的对数机率的相关性。所列出的所有因素均带入多元校正顺序回归模型中。eGFR=肾小球滤过率;LVEF=左心室射血分数。
有的患者(不考虑心衰状态),用 BNP 加入多元 Cox 模
型后进行分析,C 统计量从 0.68 上升至 0.71(P< 0.001, 似然比检验)。
我们以心衰状态分组(重点插图),并通过血浆 BNP
水平谱检验了相对死亡风险。在 BNP 较低的任何既定水
平,心衰组患者的死亡风险高于非心衰组。但是,适度
提高 BNP 水平甚至更高,根据 BNP 水平所计算的死亡
风险在两组间是相似的。例如,大约 400 pg/ml 的 BNP 水

38 JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
表 2 根据心衰状态及就诊场所对在范德堡大学医疗中心首次检测血浆 B 型钠尿肽的患者采用 Kaplan Meier 方法预测其第 1,3,5 年死亡率。
年合计 门诊 急诊或住院
非 HF HF 无 HF HF 非 HF HF
1 17.0 (16.4–17.6) 21.0 (20.2–21.8) 5.1 (4.5–5.8) 9.1 (8.1–10.0) 22.4 (21.6–23.2) 26.7 (25.6–27.7)
3 28.6 (27.9–29.3) 38.7 (37.7–39.6) 13.6 (12.6–14.6) 24.8 (23.4–26.3) 35.1 (34.1–36.1) 45.2 (43.9–46.4)
5 38.7 (37.8–39.6) 53.9 (52.8–54.9) 22.7 (21.3–24.1) 40.1 (38.2–41.9) 45.3 (44.1–46.4) 60.2 (58.9–61.5)
值为 % (95% 置信区间)。HF = 心力衰竭。
图 2 根据首次 B 型钠尿肽测定的成年患者心力衰竭状况,人口统计学和死亡风险临床因素相关强度排序
心力衰竭患者
0 100 200 300 400卡方
500 600 700 800 9000 100 200 300 400卡方
500 600 700 800 900
BNP
年龄
心律
冠状动脉疾病
性别
BMI
eGFR
慢性肾病
血糖
脉压
糖尿病
左心室质量
高血压
左心室射血分数
种族
年龄
BNP
慢性肾病
冠状动脉疾病
糖尿病
BMI
心律
eGFR
性别
血糖
左心室射血分数
种族
高血压
左心室质量
脉压
非心力衰竭患者
该图说明了临床因素(y轴)的相对贡献和通过多元校正Cox模型计算出卡方值所得的死亡风险。该卡方值通过协变量进行自由度的确定,从而可以在统一水平比较每个协变量的相对分布。例如,在非心衰患者中,BNP是死亡风险的最强决定因素。所有在列因素均纳入多元校正比列风险模型缩略词见图1。
平时,3 年内心衰组死亡风险为 21%(95% CI:20%-23%)
而非心衰组死亡风险为 19%(95% CI:17%-20%)(表 3)。
考虑到首次检测 BNP 时可能被误判为非心衰患者,
在最初检测后的随访中,我们根据患者是否出现过心衰
进行重新分组。总共有 5,468 例患者(29%)在最初分
组时被诊断为非心衰但却拥有至少 1 条 ICD-9 编码(在
线表 2)。与最初确诊为心衰组相比,被重新分类为心衰
组的病人合并症更少、利尿剂的使用少、LVEF 更高和
明显较低的 BNP 水平(中位数 163 pg/ml 和 388 pg/ml,
P< 0.001)。重新划分组与从未发生过心衰组比较,无论
其心衰状态如何,其死亡风险与 BNP 水平的关联是相似
的(在线表 4)。
表 3 根据 BNP 计算的 3 年预测死亡率并依据心衰状态和 BNP 检测的医疗场所分组
BNP (pg/ml)总计 门诊 急诊 / 住院
非 HF HF 非 HF HF 非 HF HF
55 9.9 (9.1–11) 13 (12–14) 5.5 (4.5–6.5) 8.0 (6.6–9.4) 20 (18–21) 21 (19–24)
403 19 (17–20) 21 (20–23) 12 (10–15) 15 (13–17) 33 (31–36) 30 (27–32)
值为 % (95% 置信区间 )。BNP = B 型钠尿肽 ; HF = 心力衰竭。

JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
39
我们更深入地探讨了目前已知 BNP 与死亡的相关性
是否可能归因于其他有关疾病严重程度标志物的混杂因
素。分析包括纳入追加的协变量血清钠浓度、血尿素氮、
血白细胞计数、血红蛋白、红细胞分布宽度,BNP 四分
位数的增长在两组中仍然与死亡强相关,非心衰组(HR: 1.56; 95% CI: 1.48-1.64))与心衰组(HR: 1.55; 95% CI: 1.42-1.69) ( 两组均 P< 0.001)。此外,根据 BNP 水平计算的 3年死亡风险在心衰与非心衰组中仍相似(在线表 5)。
不同临床机构 BNP 水平 我们从不同临床机构获取患者
BNP 水平,据此进行分组后反复分析,定义急救部门(包
括紧急门诊就诊、急诊、住院)或门诊病人。大多数(~
67%)BNP 检测在急救部门完成。急救部门患者 BNP 水
平较非急救部门高,同样在心衰患者 BNP 水平高于非心
衰组。其他可引起呼吸困难或心功能受损的诊断包括肺疾
病、呼吸道感染、败血症,这些都在住院患者中都很常见
(在线表 3 和表 4)。有合并症和心衰(即混合表型)的患者
BNP 水平始终高于非心衰患者。心衰状态与 BNP 水平强
相关性在急救住院和门诊病人间并没有本质上的差异。
尽管在随访阶段急救部门患者死亡率高于非急救部
门(表 2),通过 BNP 水平计算的死亡风险在心衰与非心
衰患者相似,甚至在临床机构 BNP 水平中度升高的门诊
患者中也有同样的结果(表 3)。在两个不同的临床机构
中,BNP 仍然是非心衰患者最强的死亡预测因子,而在
心衰患者中是仅次于年龄的第二位预测因子。
院内死亡病例数据分析可以得到相同的结果。住院
患者 BNP 水平与死亡风险的相关性在心衰组与非心衰组
相似。BNP 是住院非心衰患者最强死亡预测因子(在线
表 5 和表 6)。
讨论
在这项大样本、临床转诊成人研究中,我们的主要
发现如下:1)年龄、BMI、肾功能、左室质量是循环
重点插图 针对心衰或非心衰患者,根据血浆 B 型钠尿肽水平谱估计其 3 年死亡率
40
30
3年死
亡率
(%
)
20
10
2 4
BNP自然对数
6 8(7)BNP (pg/ml) (55) (403) (2981)
HF 非 HF
根据心力衰竭(HF)状态将患者分组,同时依据血浆B型钠尿肽(BNP)水平估计患者三年死亡率(95%置信区间)。 针对以下因素(情节设置)调整Cox模型:年龄(63岁),种族(白人),性别(女性),冠状动脉疾病(是),慢性肾脏疾病(否),高血压(是),糖尿病(否),心率(83次/分),脉压(55 mm Hg),体重指数(29.2 kg / m2),估计肾小球滤过率(每分钟68 ml / 1.73 m2),葡萄糖(107 mg / dl) ),左心室射血分数(55%),左心室质量(199 g)和BNP分析(第一次)。 卡方值=9.07每分钟,自由度=2和心衰状态的相互作用P= 0.01。

40 JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
BNP 水平的强相关因素;2)无论在心衰或非心衰组中
BNP 与死亡风险的相关性都是相似的,特别是在急诊部
门;3)特别是在非心衰组 BNP 是死亡风险的最强预测因
子。总的来说,这些发现可以帮助临床医生解释 BNP 结果
并能够发现高风险患者,甚至是在非心衰患者中也适用。
循环 BNP 水平是最常用的鉴别心源性与非心源性呼
吸困难的诊断工具 [2-7]。尽管传统临床上中以 100 pg/ml作为截点,仍有相当大一部分的未诊断心衰患者 BNP 水
平高于该值(我们的研究中占 47%)。矛盾的是在医疗单
位首次检测 BNP 的心衰患者中有 1/6 低于 100 pg/ml。因
此,对于临床医生而言在定义和解释 BNP 值时了解与循
环 BNP 水平相关因素非常重要。我们的研究发现,老年
人,肾脏功能减低,左室功能异常都伴随着较高的 BNP值。相反,在两组中较高的 BMI 值与较低的 BNP 水平相
关,同时 BMI 是 HF 患者 BNP 水平最强的总体决定因素。
尽管心衰及社区人群中非心衰临床因素与 BNP 水平的相
关性已有研究报道,我们的研究在现有的研究上进一步
完善,并且提供了临床确定的心衰与非心衰患者的血清
BNP 水平与多项相关的因素相对贡献程度的比较 [18-25]。
例如,在心衰患者中,BMI 和 LVEF 是目前为止与 BNP水平最强相关的两个因素。鉴于其与 BNP 呈强负相关,
我们的研究强调按照 BNP 阈值(例如 100 pg/ml)而将患
者纳入心衰组可能存在潜在局限性和偏倚,特别在射血
分数保留的心衰患者,这类患者中肥胖很常见。非急症
的门诊患者很少能达到心衰试验的 BNP 阈值。
理解 BNP 值的预测价值在临床上非常重要,因为这
种生物标记物在最终未诊断心衰患者中容易获得。实际
上,当临床医生要求患者测量 BNP 水平时,他 / 她可能
不确定患者是否患有心衰。尽管在心衰患者中 BNP 水平
与预后相关性已被广泛认可,但是其相关性在排除了心
衰的患者中知之甚少 [4,8-11]。目前现有的大多数后一组的
数据来自急诊科就诊的急性住院患者和重症监护室的病
人的特定筛选人群中获取 [2, 3, 5, 6, 26-33]。在哥本哈根的一项
研究中,连续检测了 1998-1999 年间任何原因急诊住院
1,337 例患者储存血的前 - 心房钠尿肽和 N 末端前 BNP水平 [33]。与最低四分位数相比,在总体人群和无心血管
病史的亚组中,更高的四分位数的 BNP 水平与更高的死
亡风险相关 [33]。与哥本哈根研究相比,我们评估了更多
数量和种族在急救部门和门诊就诊的基于临床判断后检
测 BNP 的成年患者,并且根据 BNP 的特定值计算了心
衰与非心衰的死亡风险。我们的数据证实了检测 BNP 就
其本身而言可确定高风险患者,如门诊非心衰患者的 1年绝对死亡率为 5%,而住院心衰患者为 27%。我们同样
证实,目前心衰患者在任何给定的 BNP 水平下的死亡风
险是相似的,特别是在急救部门或者甚至在门诊中 BNP中度升高或更高水平患者。这项发现有重要的临床意义,
因为有很大比例(15%)的非心衰患者 BNP ≥ 400 pg/ml。因此,我们的结果提示临床医生不能忽视 BNP 水平的升
高,甚至排除心衰的患者,因为测得的 BNP 水平与心衰
患者都有相同的死亡风险。
很明显,BNP 在与已知的危险标记物例如年龄、肾
功能、糖尿病、生命体征、左心室质量和 LVEF 相比较,
它仍然是非心衰患者的最强死亡预测因子。这与在以社
区为基础的大样本健康人群中的发现相一致 [21]。高 BNP水平成为这样如此强烈的死亡风险标志物的机制并没有
完全清楚。但是,心脏释放心房钠尿肽作为一个调节因
子,能够增加室壁应力、兴奋交感神经,促进血管收缩,
循环高水平的 BNP 会整合非心衰患者多种调节因素造成
心血管压力增高。在非心衰组,心率快是交感活性增高
的标志,并且与循环 BNP 水平显著相关,心率加快是年
龄和 BNP 之后的第三位死亡预测因子,也支持我们研究
中发现患者人群中交感兴奋性增强可能是死亡风险增加
的重要因素这一结论。
研究局限性 我们的研究数据来自于一所三级医疗学术中
心 13 年的电子健康记录,可能不具有普遍性。研究期间
使用两种临床方法测定 BNP 水平。尽管两种检测方法可
能存在差异,但我们通过多元校正模型控制检测方法,
并通过 BNP 测定进行分层分析(数据未显示),得出结果
相似。每个患者的 BNP 检测的临床指征尚不能确定,大
多数是在疾病急性期评估获得的,常应用于提示诊断。
通常不使用常规连续 BNP 测量,除非针对个体 BNP 水平
变化进行评估;单一 BNP 测量的预后价值已被证明 [21]。
心衰和合并症诊断基于 ICD-9 编码,这些编码先前已被
证明具有高度特异性,特别是对于心衰患者 [34]。也就是
说,我们不能排除可能存在的错误分类。为了减少轻度
心衰患者在 BNP 初始测量时被误分类为非心衰组的可能
性,我们使用广义心衰定义进行二次分析,该定义包括
在未来一段时间内发展为心衰的患者,得到类似的结果。
存在数据缺失的情况,但可以通过现代统计方法处理(多
重插补)。
观察性研究因其混杂因素而具有不确定性。尽管
BNP 是心脏的生物标记物,其水平也许与非心源性预后

JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
41
指标具有相关性。其他临床上可检测的标记物如钠、血
尿素氮、白细胞计数、血红蛋白和红细胞分布宽度均与
死亡率相关。尽管如此,在我们的研究中对这些指标进
行进一步的校正后并未否定 BNP 与死亡率的相关性。我
们不能除外其他因素,包括那些临床实践中并非与 BNP同时进行常规测量的因子,如 C- 反应蛋白和肌钙蛋白,
或许他们与死亡风险的相关性比 BNP 更强。我们不能完
全说明 BNP 检测在临床护理中出现的变化,以及在非急
救与急救部门中工作中变化。例如,体重迅速增加(即
急性失代偿)的心衰患者,可使用大剂量的利尿剂从而
减少液体负荷和心室壁压力,结果则 BNP 水平降低。在
急救和非急救的不同状态下,这种变异将会使 BNP 的预
测价值发生更大的改变。在此值得注意的是,临床中我
们实际观察到 BNP 的预测价值是相似的。
之前的研究支持 BNP 检测在非心衰观察对象中的潜
在临床实用价值。Ledwidge 等人 [35] 研究了爱尔兰未既往
诊断或没有心衰症状的门诊患者,发现以 BNP 水平 >50 pg/ml 作为筛选标准,对符合该标准的患者加强护理可减
低左心室功能不全和心衰的风险。本研究显示,高左心室
质量、低 LVEF 与高 BNP 水平强相关。因此,非心衰患者
BNP 水平升高可能预警需进行进一步检查,包括心脏结构
和功能的评估。尽管如此,仍需要更多随机实验的数据来
确认非心衰但伴有 BNP 升高患者的最佳临床路径。最后,
本研究没能评估特定原因(例如心血管)死亡率。
结论
在临床中,无论患者有无心衰,BNP 都是死亡风险
的强预测因子。另外,死亡风险与任何 BNP 水平的相关
性在心衰与非心衰患者中相似。医生不能忽视任何 BNP
水平升高的情况,甚至对已排除心衰诊断的患者也不可
大意。
通 讯 地 址 Dr. Deepak K.Gupta, Vanderbilt Translational and Clinical
Cardiovascular Research Center, Division of Cardiovascular Medicine,
Vanderbilt University School of Medicine, 2525 West End Avenue, Suite
300, Nashville, Tennessee 37203. E-mail: [email protected].
观 点
患者治疗和操作的能力 在心衰和非心衰患者中血浆
BNP 水平是死亡的强预测因子。高 BMI 和 LVEF 与
低 BNP 水平相关,解释 BNP 水平诊断心衰患者的意
义时应考虑到上述因素。
转化前景 在制定临床研究的纳入和排除标准时,应
当认识到使用单一 BNP 阈值会在较高 LVEF 和 BMI患者中产生偏倚,这种情况对于心衰和射血分数保留
的患者比较常见。
参考文献
1.Wang TJ. The natriuretic peptides and fat metabolism.N Engl J Med 2012;367:377–8.2.Levin ER, Gardner DG,Samson WK. N a t r i u r e t i c p e p t i d e s . N E n g l J M e d 1998;339:321–8.3.Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure.N Engl J Med 2002;347:161–7.4.Mukoyama M, Nakao K, Saito Y, et al. Increased human brain natriuretic peptide in congestive heart failure. N Engl J Med 1990;323:757–8.5.Cowie MR, Jourdain P, Maisel A, et al. Clinical applications of B-type natriuretic p e p t i d e ( B N P ) t e s t i n g . E u r H e a r t J 2003;24:1710–8.6.Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide in the diag-nosis of congestive heart failure in
an urgent-care setting. J Am Coll Cardiol 2001;37:379–85.7.Yamamoto K, Burnett JC Jr., Jougasaki M, et al. Superiority of brain natriuretic peptide as a hor-monal marker of ventricular systolic and diastolic dysfunction and ventricular hypertrophy. Hyper-tension 1996;28:988–94.8.Rothenburger M, Wichter T, Schmid C, et al. Aminoterminal pro type B natriuretic peptide as a predictive and prognostic marker in patients with chronic heart failure. J Heart Lung Transplant 2004;23:1189–97.9.Gustafsson F, Steensgaard-Hansen F, Badskjaer J, Poulsen AH, Corell P, Hildebrandt P. Diagnostic and prognostic performance of N-ter-minal ProBNP in primary care patients with sus-pected heart failure. J Card Fail 2005;11:S15–20.10.De Lemos JA, Morrow DA, Bentley JH, et al. The prognostic value of B-type natriuretic peptide in patients with acute coronary
syndromes. N Engl J Med 2001;345:1014–21.11.Berger R, Huelsman M, Strecker K, et al. B-type natriuretic peptide predicts sudden death in pa-tients with chronic heart failure. Circulation 2002; 105:2392–7.12.Roden DM, Pulley JM, Basford MA, et al. Development of a large-scale de-identified DNA biobank to enable personalized medicine. Clin Pharmacol Ther 2008;84:362–9.13.Patel DK, Green KD, Fudim M, Harrell FE, Wang TJ, Robbins MA. Racial differences in the prevalence of severe aortic stenosis.J Am Heart Assoc 2014;3:e000879.14.Levey AS, Adler S, Caggiula AW, et al. Effects of dietary protein restriction on the progression of advanced renal disease in the Modification of Diet in Renal Disease Study. Am J Kidney Dis 1996;27:652–63.15.Wells QS, Farber-Eger E, Crawford DC. Extraction of echocardiographic data from the electronic medical record is a rapid and

42 JACC VOL. 71, NO. 19, 2018MAY 15, 2018:2079–88
York et al .伴或不伴 HF 患者的 BNP 水平和预后
efficient method for study of cardiac structure and func-tion. J Clin Bioinform 2014;4:12.16.Lang RM, Badano LP, Mor-Avi V, et al. Rec-ommendations for cardiac chamber quantificat ion by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015;28:1–39.e14.17.Hanna DB, Pfeiffer MR, Sackoff JE, Selik RM, Begier EM, Torian LV. Comparing the National Death Index and the Social Security Administra-tion’s Death Master File to ascertain death in HIV surveillance. Public Health Rep 2009;124:850–60.18.Krishnaswamy P, Lubien E, Clopton P, et al. Utility of B-natriuretic peptide levels in identifying patients with left ventricular systolic or diastolic dysfunction. Am J Med 2001;111:274–9.19.Maisel AS, Koon J, Krishnaswamy P, et al. Utility of B-natriuretic peptide as a rapid, point-of-care test for screening patients undergoing echo-cardiography to determine left ventricular dysfunction. Am Heart J 2001;141:367–74.20.Das SR, Drazner MH, Dries DL, et al. Impact of body mass and body composition on circulating levels of natriuretic peptides: results from the Dallas Heart Study. Circulation 2005;112:2163–8.21.Wang TJ, Larson MG, Levy D, et al. Plasma natriuretic peptide levels and the risk of cardio-vascular events and death. N Engl J Med 2004; 350:655–63.22.Wang TJ, Larson MG, Keyes MJ, Levy D, Benjamin EJ, Vasan RS. Association of plasma
natriuretic peptide levels with metabolic risk fac-tors in ambulatory individuals. Circulation 2007; 115:1345–53.23.Gupta DK, Claggett B, Wells Q, et al. Racial differences in circulating natriuretic peptide levels: the Atherosclerosis Risk In Communities study. J Am Heart Assoc 2015;4.24.Gupta DK, de Lemos JA, Ayers CR, Berry JD, Wang TJ. Racial differences in natriuretic peptide levels: the Dallas Heart Study. J Am Coll Cardiol HF 2015;3:513–9.25.Gupta DK, Daniels LB, Cheng S, et al. Differ-ences in natriuretic peptide levels by race/ethnicity (from the Multi-Ethnic Study of Athero-sclerosis). Am J Cardiol 2017;6:1008–15.26.Omland T, Aakvaag A, Bonarjee VV, et al. Plasma brain natriuretic peptide as an indicator of left ventricular systolic function and long-term survival after acute myocardial infarction. Com-parison with plasma atrial natriuretic peptide and N-terminal proatrial natriuretic peptide. Circula-tion 1996;93:1963–9.27.Harrison A, Morrison LK, Krishnaswamy P, et al. B-type natriuretic peptide predicts future cardiac events in patients presenting to the emergency department with dyspnea. Ann Emerg Med 2002;39:131–8.28.Nakada Y, Kawakami R, Nakano T, et al. Sex dif-ferences in clinical characteristics and long-term outcome in acute decompensated heart failure pa-tients with preserved and reduced ejection fraction. Am J Physiol Heart Circ Physiol 2016;310:H813–20.29.Januzzi JL Jr., Sakhuja R, O’Donoghue M, et al. Utility of amino-terminal pro-brain natriuretic peptide testing for prediction of
1-year mortality in patients with dyspnea treated in the emergency department. Arch Intern Med 2006;166:315–20.30.Meyer B, Huelsmann M, Wexberg P, et al. N-terminal pro-B-type natriuretic peptide is an in-dependent predictor of outcome in an unselected cohort of critically ill patients. Crit Care Med 2007; 35:2268–73.31.Karmpaliotis D, Kirtane AJ, Ruisi CP, et al. Diagnostic and prognostic utility of brain natri-uretic peptide in subjects admitted to the ICU with hypoxic respiratory failure due to noncardiogenic and cardiogenic pulmonary edema. Chest 2007; 131:964–71.32.Fonarow GC, Peacock WF, Phillips CO, et al. Admission B-type natriuretic peptide levels and in-hospital mortality in acute decompensated heart failure. J Am Coll Cardiol 2007;49: 1943–50.33.Lauridsen BK, Iversen K, Hunter I, et al. ProANP plasma measurement predicts all-cause mortality in acutely hospitalised patients: a cohort study. BMJ Open 2013;3:e003288.34.McCormick N, Lacaille D, Bhole V, Avina-Zubieta JA. Validity of heart failure di-agnoses in administrative databases: a systematic review and meta-analysis. PLoS ONE 2014;9: e104519.35.Ledwidge M, Gallagher J, Conlon C, et al. Natriuretic peptide-based screening and collabo-rative care for heart failure: the STOP-HF ran-domized trial. JAMA 2013;310:66–74.
关键词 死亡,电子健康数据,预后,回顾性。
附录 有关扩展的方法部分以及补充表格和
图表,请参阅本文的线上版本。
沈阳军区总医院 韩雅玲 李洋
B 型钠尿肽(BNP)不仅是诊断心衰的金标准,而且对心衰患者的再住院和死亡风险具有预测作用。本研究通过
对 3 万余例心衰和非心衰患者的 BNP 水平和死亡风险间的回顾分析发现,虽然非心衰患者 BNP 水平较心衰患者低,
但 BNP 对心衰和非心衰患者死亡率均具有预测作用。无论是急性发作期还是慢性稳定期,BNP 升高的心衰和非心衰
患者的 3 年死亡风险相似。期待将来开展的随机对照临床研究提供更多数据阐明 BNP 升高的非心衰患者的死亡原因
及其治疗方案。
点 评

JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY ©2018 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
VOL. 72, NO. 4, 2018ISSN 0735-1097
外科与经皮冠脉血运重建治疗后卒中的发生率Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization
Stuart J.Head, MD, PhD,a Milan Milojevic, MD, MSC,a Joost Daemen, MD, PHD,b Jung-Min Ahn, MD,c Eric Boersma, PHD,b
Evald H.Christiansen, MD, PHD,d Michael J.Domanski, MD,e,f Michael E.Farkouh, MD, MSC,e,f Marcus Flather, MBBS,g Valentin Fuster, MD, PHD,e Mark A.Hlatky, MD,h Niels R. Holm, MD,d Whady A.Hueb, MD, PHD,I Masoor Kamalesh, MD,j
Young-Hak Kim, MD,c Timo Mäkikallio, MD,k Friedrich W. Mohr, MD, PHD,l Grigorios Papageorgiou, MSC,a,m Seung-Jung Park, MD,c Alfredo E. Rodriguez, MD, PHD,n Joseph F. Sabik III, MD,o Rodney H. Stables, MA, DM,p Gregg W. Stone, MD,q Patrick W. Serruys, MD, PHD,r A. Pieter Kappetein, MD, PHDa
翻译:四川大学华西医院急诊科 张海宏;审校:中南大学湘雅医院 段琼
摘 要
背景 对于冠脉多支病变和左主干病变的患者,冠脉血运重建治疗常选择冠脉旁路移植手术(Coronary artery bypass grafting, CABG)和经皮冠状动脉介入治疗(percutaneous coronary intervention, PCI)。卒中是血运重建治疗后最严重
的并发症之一。鉴于其发病率低,因此需要对大样本量患者进行研究来揭示 CABG 和 PCI 间卒中发生率的不同。
目的 本研究旨在比较 CABG 和 PCI 后卒中的发生率,以及由此导致的卒中对长期死亡率的影响。
方法 我们汇总了 11 项比较 CABG 和 PCI 支架植入的随机临床研究,基于个体病人数据进行分析,这 11 项研究
包括:ERACI II 研究(阿根廷随机研究 : 用支架冠脉血管成形术与多支病变患者冠脉旁路术)(n=450)、ARTS 研
究(冠脉血运重建治疗研究)(n=1,205)、MASS II 研究(药物、血管成形术、或外科手术研究)(n=408)、SoS 研
究 (支架或手术)试验(n=988)、SYNTAX 研究(利用 Taxus 支架进行经皮冠脉介入治疗与心脏手术间的协同
效应)(n=1,800)、PRECOMBAT 研究(左主干冠脉病变患者旁路手术与血管成形术使用雷帕霉素洗脱支架对比)
(n=600)、FREEDOM 研究(糖尿病患者伴有冠脉多支病变两项治疗方案的对比)(n = 1,900)、VA CARDS 研究 (糖尿病患者冠脉血运重建术)(n = 198)、BEST 研究(冠脉多支病变患者旁路手术与依维莫司洗脱支架植入术对
比)(n = 880)、NOBLE 研究(经皮冠脉血管成形术与冠状动脉旁路移植术在治疗无保护的左主干狭窄中的对比) (n=1,184), 以及 EXCEL 研究(评价依维莫司洗脱支架与冠状动脉旁路术对左主干血运重建效果)(n = 1,905)。
通过试验分层,运用随机效应 Cox 比例风险模型比较 CABG 和 PCI 之间的 30 天和 5 年卒中率,同时探究卒中对
5 年死亡率的影响。
结果 本次分析共纳入 11,518 例患者,随机分组至 PCI 组(n=5,753)或 CABG 组(n=5,765),平均随访时间
为 3.8±1.4 年,期间共有 293 例卒中发生。在 30 天时,卒中发生率分别为 PCI 后 0.4% 和 CABG 后 1.1%(风
险比 [hazard ratio, HR] 为 0.33;95% 置信区间 [confidence interval, CI] 0.20-0.53;P<0.001)。随访 5 年时,PCI后卒中发生率仍显著低于 CABG 后(2.6% vs.3.2%;HR: 0.77; 95% CI:0.61-0.97; P=0.027)。而 31 天到 5 年
间两组的卒中发生率是接近的,PCI 后为 2.2%,CABG 后为 2.1%(HR:1.05; 95% CI:0.80-1.38; P = 0.72)。
治疗和基线临床或血管造影指标对 5 年卒中发生率无显著相关,但在糖尿病(PCI:2.6% vs. CABG:4.9%)和
aDepartment of Cardiothoracic Surgery, Erasmus Medical Center, Rotterdam, the Netherlands; bDepartment of Cardiology, Erasmus Medical College, Rotterdam, the Netherlands; cDepartment of Cardiology, University of Ulsan College of Medicine,Asan Medical Center, Seoul, South Korea; dDepartment of Cardiology, Aarhus University Hospital, Skejby, Aarhus, Denmark; eCardiovascular Institute, Icahn School of Medicine at Mount Sinai, New York, New York; fDivision of
PUBLISHED BY ELSEVIER https://doi.org/10.1016/j.jacc.2018.04.071

44 JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
已有许多随机临床研究
比较治疗冠心病的冠脉旁路移 植手术(coronary aetery bypass grafting, CABG)和经皮冠状
动 脉 介 入 治 疗(percutaneous coronary intervention, PCI), 最 初是球囊血管成形术,随后是
裸金属支架(bare-metal stents, BMS)的应用 [1, 2],目前是药 物洗脱支架(drug-eluting stents, DES)的应用 [3]。随着科技和
PCI 支架技术不断进步,越来
越多的研究关注更复杂的合
并多支血管疾病(multivessel disease, MVD)、左主干(left main, LM)病变和糖尿病的
患者。
已有一些研究提示,与 PCI 比较,CABG 术后卒中
明显增加 [1],这是一个灾难性的结果,将导致患者患病率
和死亡率增加、生活质量下降。目前为止,对于 CABG或 PCI 术后卒中的准确发生率和结局尚缺乏一个肯定的
证据,原因在于个体随机试验缺少足够的效力来揭示两
者之间微小但有意义的差异 [4]。最近的一项协同分析中,
11 项随机研究纳入 MVD 或 LM 的冠心病患者,随机分
组至 CABG 或 PCI 组,我们发现在 MVD 合并糖尿病的
患者中,与 PCI 比较,CABG 能明显减少 5 年全因死亡率,
但 MVD 未合并糖尿病,以及合并 LM 的患者却没有这种
差异 [5]。除了死亡率,对于包括卒中这类能严重影响生
活质量的终点事件也必须予以重视。
因此,我们基于 11 项随机研究中的个体病人数据进
行分析,比较 CABG 与 PCI 术后和长期卒中发生率及其
对生存的影响。
方法
研究纳入和数据收集 本汇总分析的细节之前已发表 [5]。
简而言之,2017 年 7 月 19 日通过系统性检索,确定比
较治疗 MVD 或 LM 疾病的 CABG 或 PCI 的随机临床研
Cardiology, Peter Munk Cardiac Centre and Department of Medicine, Heart and Stroke Richard Lewar Centre, University of Toronto, Toronto, Ontario,Canada; gDepartment of Medicine and Health Sciences, Norwich Medical School University of East Anglia and Norfolk and Norwich University Hospital, Norwich, United Kingdom; hDepartment of Health Research and Policy, and Department of Medicine(Cardiovascular Medicine), Stanford University School of Medicine, Stanford, California; iHeart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil; jDepartment of Cardiology, Richard L. Roudebush Veterans Affairs Medical Center,Indianapolis, Indiana; kDepartment of Cardiology, Oulu University Hospital, Oulu, Finland; lDepartment of Cardiac Surgery, Herzzentrum Universität Leipzig, Leipzig, Germany; mDepartment of Biostatistics, Erasmus Medical Center, Rotterdam, the Netherlands; nCardiac Unit, Otamendi Hospital, Buenos Aires, Argentina; oDepartment of Surgery, University Hospitals Cleveland Medical Center, Cleveland, Ohio; pInstitute of Cardiovascular Medicine and Science, Liverpool Heart and Chest Hospital, Liverpool, United Kingdom; qDepartment of Cardiology, Columbia University Medical Center and Clinical Trials Center, the Cardiovascular Research Foundation, New York, New York; rDepartment of Cardiology, Imperial College London, London,United Kingdom.This current study was performed without funding. Individual trials did receive funding: SoS (Stent or Surgery) trial received funding from Boston Scientific Corp., Guidant ACS, and Medtronic. MASS II received funding from Zerbini Foundation. ERACI II received funding from Cook Inc. ARTS received funding from Cordis. SYNTAX trial received funding from Boston Scientific Corp. PRECOMBAT trial received funding from the Cardiovascular Research Foundation (Seoul, Korea), Cordis, Johnson and Johnson, and grant 0412-CR02-0704-0001 from Health 21 R&D Project, Ministry of Health and Welfare, South Korea. VACARDS received funding from the VA Cooperative Studies Program. FREEDOM trial was supported by grants U01 01HL071988 and 01HL092989 from the National Heart, Lung, and Blood Institute, Cordis, Johnson and Johnson, Boston Scientific Corp., Eli Lilly, Sanofi, and Bristol-Myers Squibb. BEST received funding from CardioVascular Research Foundation, Abbott Vascular, and grant HI10C2020 from the Korea Healthcare Technology Research and Development Project, Ministry for Health and Welfare Affairs, South Korea. EXCEL trial received funding from Abbott Vascular. NOBLE trial received funding from Biosensors, Aarhus University Hospital, and participating sites. Dr. Daemen has received institutional research grants from Abbott, Acist Medical, Boston Scientific, Pie Medical, St. Jude Medical, ReCor Medical, and Medtronic; and has received consulting fees from Acist, AstraZeneca, Pythagoras Medical, and ReCor. Dr. Farkouh has received research support from Amgen and Novo Nordisk. Dr. Holm has received institutional research grants from Abbott, Biosensors, Biotronik, and Boston Scientific; and has received speaking honoraria from Abbott, Biotronik, and Terumo. Dr. Sabik has served on the Cardiac Surgery Advisory Board of Medtronic; and is the North American surgical principal investigator for the EXCEL trial, sponsored by Abbott. Dr. Stone has received grant support from the Cardiovascular Research Foundation during the conduct of the study; has received personal fees from Velomedix, Toray, Matrizyme, Miracor, TherOx, Reva, V-wave, Vascular Dynamics, Ablative Solutions, Neovasc, and Medical Development Technologies; has received other support from the MedFocus family of funds, Guided Delivery Systems, Micardia, Vascular Nonotransfer Technologies, Cagent, Qool Therapeutics, Caliber, Aria, and the Biostar family of funds outside the submitted work; has served as a consultant on prasugrel patent litigation paid for by Lupin Pharmaceuticals; and his institution, Columbia University, receives royalties from Abbott Vascular for sale of the MitraClip. Dr. Serruys has served as a consultant for Abbott Laboratories, AstraZeneca Pharmaceuticals, Biotronik, Cardialysis B.V., GLG Research, Medtronic, Sino Medical Sciences Technology Inc. Tianjin China, Stentys France, Svelte Medical Systems Inc., Volcano/Philips Europe, Q3Medical Devices Limited, and St. Jude Medical; and has served as a member of the corporate advisory board for Xeltis. Dr. Kappetein is an employee of Medtronic. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Amar Krishnaswarmy, MD, served as Guest Editor for this paper.Manuscript received March 17, 2018; accepted April 23, 2018.
非糖尿病患者(PCI:2.6% vs. CABG: 2.4%)之间有显著差异(相关性 P=0.004)。与未发生卒中患者比较,术后 30天内发生卒中的患者有较高的 5 年死亡率,无论是 PCI 后(45.7% vs. 11.1%,P< 0.001)还是 CABG 后(41.5% vs. 8.9%,P< 0.001)。
结论 这项个体病人数据的汇总性分析表明:与 CABG 相比,PCI 后 5 年卒中发生率明显降低,归因于术后 30 天
中卒中发生率降低,而 31 天到 5 年期间卒中发生率接近。多支病变和糖尿病患者 CABG 后卒中风险比 PCI 后更高,
血运重建治疗后 30 天内发生卒中的患者,5 年死亡率更高。
缩略词表BMS=bare-metal stent(s)
裸金属支架
CABG=coronary artery bypass
grafting
冠脉旁路移植术
CI=confidence interval
置信区间
DAPT=dual antiplatelet therapy
双联抗血小板治疗
DES=drug-eluting stent(s)
药物洗脱支架
HR=hazard ratio
风险比
LM=left main
左主干
MVD=multivessel disease
多血管病变
PCI=percutaneous coronary
intervention
经皮冠脉介入

45JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
究。如符合以下标准,则纳入该研究:1)患者随机分组,
接受 CABG 或 PCI 治疗;2)MVD 或 LM 疾病患者;3)
未表现为急性心肌梗死;4)PCI 治疗使用支架(BMS 或
DES),而不是球囊血管成形术;5)随访 30 天以上,收
集卒中相关数据;以及6)随访大于1年的全因死亡有效性。
本研究的执行遵循 PRISMA(Preferred Reporting Items for Systematic Review and Meta-Analyses, PRISMA)指南 [6]。
11 项研究的研究者为本汇总分析提供了数据:ERACI II 研究(阿根廷随机研究 : 用支架冠脉血管成形术与多支
病变患者冠脉旁路术)[7]、ARTS 研究(冠脉血运重建治
疗研究)[8]、MASS II 研究(药物、血管成形术、或外科
手术研究)[9]、SoS 研究(支架或手术)[10]、SYNTAX 研
究(利用 Taxus 支架进行经皮冠脉介入治疗与心脏手术间
的协同效应)[11]、 PRECOMBAT 研究(左主干冠脉病变
患者旁路手术与血管成形术使用雷帕霉素洗脱支架对比)[12]、FREEDOM 研究(糖尿病患者伴有冠脉多支病变两
项治疗方案的对比)[13]、VA CARDS 研究(糖尿病患者
冠脉血运重建术)[14]、BEST 研究(冠脉多支病变患者旁
路手术与依维莫司洗脱支架植入术对比)[15]、EXCEL 研
究(评价依维莫司洗脱支架与冠状动脉旁路术对左主干
血运重建效果)[16]、以及 NOBLE 研究(经皮冠脉血管成
形术与冠状动脉旁路移植术在治疗无保护的左主干狭窄
中的对比)[17](参见在线图 1)。仅 LE MANS(无保护左
主支架置入术与旁路手术对比研究)研究的数据未能获
取(n=105)[18]。研究的基线和手术特征参见在线表 1。
每项研究在实施时均获得当地医学伦理委员会的批
准。11 项研究中的每位患者都签署了知情同意书。
终点、定义和随访 随访时间是由手术时间到研究中普遍
定义的随访时间计算得来。如果患者在术前发生卒中或
死亡,或患者没有接受血运重建治疗而只是药物治疗,
随访时间从随机分组开始计算。本研究的主要终点是卒
中。由手术导致的卒中定义为术后 30 天内发生的卒中。
除 SoS 研究外,所有研究均在整个随访期内收集卒中信息;
SoS 研究只收集到血运重建术后一年 [10]。卒中的定义采
用统一标准,其中主要包括以下两点:1)有或无神经影
像学检查证实的中枢源性的局灶性神经功能缺失持续 24小时以上;2)神经功能缺失超过 72 小时直接认定为卒中,
而无需神经影像学检查证实。本研究的次要终点是卒中
后全因死亡率以及全因死亡率或卒中的联合终点。所有
研究中,临床事件委员会对事件进行裁定。
MVD 定义为 2 或 3 支血管病变,不合并 LM 疾病。
LM 疾病定义为左主干病变,单独存在或合并单血管或多
支血管病变。
统计学方法 按照意向性治疗原则进行主要分析。终点数
据也是在治疗基础上分析,更准确地确定特定治疗方案
对卒中发生率的影响。连续性变量以均值 ± 标准差表
示,采用 t 检验;离散性数据以频率表示,采用卡方检
验。我们汇总 11 项研究的患者数据,提供了描述性统计
分析和未校正的 Kaplan-Meier 曲线。CABG 与 PCI 卒中
发生的风险比(hazard ratios, HR)采用随机效应 Cox 比
例风险模型进行评估,该模型通过试验分层,使用伽玛
衰弱因子来说明各试验间的异质性。衰弱因子是非观测
性指标,呈 γ 随机变量分布,均值为 1,方差为 ϑ。因
此,衰弱因子的变量表示各研究中基线风险的异质性,
而似然比检验方差参数的统计学差异。30 天和 5 年时
评估脑中发生率,在随访 30 天后进行界标分析来评估
CABG 和 PCI 后卒中的长期风险。基于基线临床和解剖
特征以及 MVD 或 LM 疾病,对 30 天和 5 年卒中率进行
预先指定的亚组分析。相关性 P 值在随机效应 Cox 比例
风险模型中计算得出。由于分析 30 天卒中的几个亚组中
发生事件有限,无法建立衰弱模型;因此在这些特殊分
析中,风险比和相关因子通过标准 Cox 比例危险模型分
析得出。因为 LM 和 MVD 组不是相互排斥的,因此我
们没有根据 LM/MVD 进行相互作用分层分析。除此之
外,我们探讨了实验中非体外循环(off pump)CABG 而
不是体外循环 CABG 的影响,为使用心肺旁路术策略提
供了信息;也分析了 PCI 手术使用 BMS 或 DES 的影响,
以及出院时单联和双联抗血小板治疗(dual anti-platelet therapy, DAPT)的影响。构建包含基线和治疗特征的多
因素 Cox 比例风险模型,用于预测 30 天和 5 年卒中的
发生。如单变量分析中 P<0.05 的变量纳入多因素分析
模型中,而 CABG 和 PCI 这两个变量则必须包含在模型
中。通过 Kaplan-Meier 法比较 30 天发生和未发生卒中的
病人,来探究 30 天内卒中对死亡的影响。基于糖尿病、
SYNTAX 评分和 MVD 或 LM 等信息,对所有患者在 30天和 5 年时总的全因死亡或卒中的发生率进行了分析。
双侧 P<0.05 认为有统计学意义。采用 SPSS 21.0 (IBM Corporation, Armonk, New York)或 R 软件 3.2.4(Institute for Statistics and Mathematics of Wirtschaftsuniversität, Wien, Austria)进行统计分析。
资助来源 虽然一些研究是由企业资助的,但该项汇总分
析没有外部资助,也不涉及任何一家原研究赞助者。

46 JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
结果
研究人群 11 项研究随机入组 11,518 例患者;其中 5,765
例 随 机 分 配 至 CABG 组,5,753 例 至 PCI 组。CABG 组
的 5,765 例患者中,5,421 例接受了 CABG 治疗(94%),
233 例 接 受 了 PCI 治 疗(4%),111 例 两 种 治 疗 都 未 接
受(2%)。PCI 组的 5,753 例患者中,5,610 例接受了 PCI
治 疗(98%),101 例 接 受 了 CABG 治 疗(2%),42 例
两种治疗都未接受(1%)。在接受治疗分析(as-treated
analysis)中,5,522 例患者接受 CABG 治疗,5,843 例患
者接受 PCI 治疗。每项研究的交叉数据详见在线表 2。
患者纳入时间为 1995 年至 2015 年(见在线表 1)。4
项研究的 PCI 治疗完全采用 BMS(MASS II、ERACI II、
SoS 和 ARTS; n=1,518 PCI 病例),3 项研究采用第一代
DES(PRECOMBAT、SYNTAX 和 FREEDOM;n=2,156 PCI 病例),3 项研究采用第二代 DES(BEST、EXCEL、
和 NOBLE;n = 1,978 PCI 病例),1 项研究中两代支架均
有(VA CARDS;n = 101 PCI 病例)。
随机分组至 CABG 或 PCI 两组的患者,其基线特
征无显著临床差异(表 1)。汇总后病人的平均年龄为
63.6±9.8 岁,女性占 24%。38% 的患者有糖尿病,其中
12% 使用胰岛素治疗。39% 患者有 LM 疾病。离院时,
PCI 后的患者中抗血小板治疗的情况多于 CABG 后的患
者(P<0.01)。平均随访时间为 3.8 ± 1.4 年。
卒中的频率和预测因素 随访中共有 293 例卒中病例。5年随访时累积卒中率在 PCI 组为 2.6%(129 例),CABG
表 1 随机队列的基线、手术和离院数据PCI(n=5,753) CABG(n = 5,765)
年龄(岁) 63.6 ± 9.8(5,753) 63.7 ± 9.9 (5,765) 女性 23.9 (1,373/5,753) 23.8 (1,371/5,765)
BMI >30 kg/m2 28.1 (1,548/5,506) 28.3 (1,558/5,511)
吸烟,目前 22.3 (1,274/5,701) 22.3 (1,273/5,703)
糖尿病 38.5 (2,215/5,753) 37.7 (2,171/5,765)
胰岛素治疗 12.9 (545/4,234) 11.9 (504/4,245)
高血压 67.6 (3,880/5,739) 68.1 (3,913/5,748)
高胆固醇血症 69.5 (3,982/5,726) 67.3 (3,862/5,735)
外周血管疾病 8.2 (424/5,158) 8.5 (440/5,164)
主动脉疾病 7.8 (161/2,072) 8.1 (168/2,074)
既往 TIA 或 CVA 5.4 (218/4,052) 6.2 (253/4,054)
既往 MI 28.0 (1,438/5,138) 27.5 (1,417/5,156)
左心室功能障碍,<30% 0.9 (49/5,303) 1.0 (54/5,430)
不稳定疾病 34.6 (1,786/5,158) 34.2 (1,767/5,160)
三支血管病变 * 58.6 (2,460/4,201) 61.8 (2,594/4,197)
左主干病变 38.8 (2,233/5,753) 38.9 (2,245/5,765)
SYNTAX 评分 26.0± 9.3 (4,081) 26.0± 9.8 (4,057)
PCI-DES† 73.4 (4,120/5,610) -
PCI 支架数 3.1± 2.0 (4,935) -
CABG-LIMA - 96.2 (4,574/4,753)
CABG-BIMA - 18.7 (771/4,122)
CABG- 非体外循环 - 27.5 (1,085/3,945)
离院时开阿司匹林 97.3 (4,487/4,612) 95.5 (3,814/3,994)
离院时开噻吩吡啶 96.7 (4,479/4,630) 45.1 (1,815/4,026)离院时 DAPT 治疗 95.1 (4,384/4,612) 44.0 (1,759/3,994)
数据以均数±标准差(N)或%(n/N)表示,*多支血管病变患者所在组。†仅限于随机入组至PCI组并实际接受PCI治疗的患者。VA CARDS研究中有1例患者未交代支架类型。BIMA=双侧乳内动脉;BMI=身体质量指数;CABG=冠脉旁路移植术;CVA=脑血管事件;DAPT=双联抗血小板治疗;DES=药物洗脱支架;LIMA=左侧乳内动脉;LV=左心室病变;MI=心肌梗死;PCI=经皮冠脉介入;SYNTAX=利用Taxus支架进行经皮冠脉介入治疗与心脏手术间的协同效应;TIA=短暂脑缺血发作;VACARDS=糖尿病患者冠脉血运重建。

47JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
重点插图 经皮冠脉介入与冠脉旁路移植后卒中
0 126 18 24随访(月)
30 36
0-1,825 天HR: 0.77 (95% CI: 0.61-0.97)P = 0.027
42 48 54
2.6%
3.2%
60
A
0
3
2
1
4
5
累积
卒中
率(
%)
0 1 6随访(月)
12 18
0-30 天HR: 0.33 (95% CI: 0.20-0.53)P < 0.001
31-1,825 天HR: 1.05 (95% CI: 0.80-1.38)P = 0.72
24 30 36 42 5448
2.2%
2.1%
1.1%
0.4%
60
5,555 5,421 5,282 5,138 4,901 4,550 3,677 3,446 2,9573,213 2,202
5,643
CABG
风险数
PCI
冠脉旁路移植术(CABG)经皮冠脉介入(PCI)
5,765
830,3455,3887,3356,4440,5562,5514,5545,5357,5 3,320 2,360
B
1
0
3
2
4
5
累积
卒中
率(
%)
此图对比冠脉旁路移植术(CABG)与经皮冠脉介入(PCI)随访5年内的卒中率(A)临界分析30天内和30天后卒中率(B)。PCI 和 CABG的风险比(HR)。CI=置信区间。
组 为 3.2%(164 例)[ 风 险 比:0.77;95% 置 信 区 间
(confiderene interval, CI):0.61-0.97;P=0.027](重点插图,
图 A)。30 天时,PCI 组 21 例发生卒中(0.4%),CABG
组 64 例 发 生 卒 中(1.1%)(HR:0.33; 95% CI: 0.20-0.53; P< 0.001)(重点插图,图 B)。而从 31 天到 5 年间卒中率
在 PCI 组(2.2%;108 例) 和 CABG 组(2.1%;100 例)
间无差别(HR:1.05; 95% CI: 0.80-1.38; P= 0.72)(重点插图,
图 B)。在接受治疗分析中得到了类似的结果。异质性分
析的衰弱因子(θ)值为 0.09 (P< 0.001)。在多因素分析中,
30 天卒中的独立预测因素是 CABG(HR:8.33; 95% CI:
1.06- 62.5; P= 0.043),但 CABG 不是 5 年卒中的独立预测
因素(HR:1.43; 95% CI:0.94- 2.13; P= 0.089)。
在 7 项提供了非体外循环 (off-pump)和体外循环 (on-
pump)CABG 数据(n=3,945)的研究中,28% 患者接受了

48 JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
非体外循环 CABG。非体外循环组的 30 天卒中率为 0.6% (1,085例中有6例),体外循环组为1.4% (2,860例中有40例)
(P= 0.13),而 5 年卒中率两组分别为 2.9% (1,085 例中有 25例)和 3.5% (2,860 例中有 84 例)(P=0.60)。CABG 后 44%的患者离院时开具了 DAPT。DAPT 和单联药物治疗的 5 年
卒中发生率是相近的,分别为(3.1%[1,759 例中有 48 例 ]和 3.8% [2,109 例中有 67 例 ] P= 0.84)。
PCI 治疗采用 BMS 或 DES 对 30 天(0.5%[1,518 例
中有 7 例 ]vs. 0.3% [4,235 例中有 14 例 ];P= 0.89)和 5年卒中率(2.6% [1,518 例中有 39 例 ]vs. 2.7% [4,235 例中
有 90 例 ];P= 0.83)均无影响。如单独分析 BMS 和 DES时,PCI 和 CABG 后 5 年 卒 中 率, 无 论 BMS( 分 别 为
2.6% 和 3.2%,P=0.39)还是 DES(分别为 2.7% 和 3.3%, P=0.038)均无明显差异(相关性,P=0.78)。PCI 后仅
有 190 例患者离院时开具单联抗血小板药物,DAPT 组 5年卒中率为 2.5% (4,384 例中有 91 例),而单联药物组为
图 1 根据基线和治疗特征,PCI 和 CABG 后 30 天卒中发生率的亚组分析
0.26 (0.14-0.49)
0.53 (0.22-1.24)
0.28 (0.12-0.64)
0.36 (0.19-0.66)
0.37 (0.22-0.61)
0.12 (0.02-1.00)
0.26 (0.14-0.49)
0.52 (0.22-1.24)
0.21 (0.11-0.41)
0.69 (0.32-1.48)
0.23 (0.11-0.49)
0.44 (0.23-0.84)
0.24 (0.05-1.12)*
0.35 (0.19-0.63)
0.26 (0.10-0.69)*
0.39 (0.20-0.73)
0.34 (0.19-0.61)
0.32 (0.12-0.88)
0.28 (0.15-0.50)
0.50 (0.20-1.24)
0.31 (0.11-0.83)
0.25 (0.09-0.68)
0.23 (0.07-0.79)
HR (95% CI)
<0.001
0.14
0.003
0.001
<0.001
0.050
<0.001
0.14
<0.001
0.34
<0.001
0.013
0.069
<0.001
0.007
0.001
<0.001
0.028
<0.001
0.14
0.020
0.007
0.020
P 值
0.19
0.62
0.33
0.28
0.023
0.20
0.54*
0.34*
0.92
0.28*
0.89
相关性 P值
49/4,394 (1.1)
15/1,371 (1.1)
25/2,940 (0.9)
39/2,825 (1.4)
54/3,953 (1.4)
8/1,558 (0.5)
49/3,913 (1.3)
15/1,835 (0.8)
46/3,862 (1.2)
17/1,873 (0.9)
34/2,171 (1.6)
30/3,594 (0.8)
8/440 (1.8)
52/4,724 (1.1)
19/1,417 (1.4)
41/3,739 (1.1)
45/4,597 (1.0)
15/833 (1.8)
50/4,232 (1.2)
14/1,533 (0.9)
17/1,585 (1.1)
18/1,545 (1.2)
14/927 (1.5)
CABG
13/4,380 (0.3)
8/1,373 (0.6)
7/2,971 (0.2)
14/2,782 (0.5)
20/3,958 (0.5)
1/1,548 (0.1)
13/3,880 (0.3)
8/1,859 (0.4)
10/3,982 (0.3)
11/1,744 (0.6)
8/2215 (0.4)
13/3538 (0.4)
2/424 (0.5)
19/4,734 (0.4)
5/1,438 (0.3)
16/3,700 (0.4)
15/4,447 (0.3)
7/1,518 (0.5)
5/856 (0.6)
5/1,533 (0.3)
5/1,677 (0.3)
14/4,235 (0.3)
3/871 (0.3)
PCI
性别
亚组
210.0 10.50.3支持PCI 支持CABGHR
(95% CI)
5
男
女
年龄基线
<65
65或更大
身体质量指数
<30
30或更高
高血压
是
否
高胆固醇血症
是
否
糖尿病
是
否
外周血管病变
是
否
MI病史
是
否
LVEF
正常
异常(<50%)
病变复杂性
SYNTAX分数 0-22
SYNTAX分数 23-32
SYNTAX分数 >33
PCI
DES
BMS
*由于事件发生率低,相关性是由Cox比例风险模型而不是包含衰弱点的Cox比例风险模型随机效应引起的。BMS=裸金属支架;CI=置信区间;DES=药物洗脱支架;HR=风险比;LVEF=左心室排血分数;MI=心肌梗死;SYNTAX=利用Taxus支架进行经皮冠脉介入治疗与心脏手术间的协同效应。

49JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
4.0% (190 例中有 5 例)(P= 0.41)。
亚组分析 除了高胆固醇血症,PCI 和 CABG 的任何治疗
效应在 30 天卒中率上无明显关联(相关性,P=0.023)(图 1)。
除了糖尿病,PCI 和 CABG 之间和基线特征在 5 年卒中
率上无明显关联(图 2 和 3)。如图 3A 所示,随机分配在
PCI 组的糖尿病患者中的 5 年卒中率低于 CABG 组,分别
为(2.6% [n=472,251 例中有 47 例 ] 和 4.9% [n=862,171 例
中有 86 例 ]; HR:0.52;95% CI: 0.37-0.75; P<0.001),但非
糖尿病患者差别不明显,两组分别为(2.6% [n=823,538 例
中有 82 例 ] 和 2.4% [n=783,594 例中有 78 例 ];HR:1.04;
95% CI: 0.77-1.42; P=0.78;相关性 P 值为 0.004)。
4,478 例 LM 疾 病 患 者,PCI 治 疗 后 30 天 卒 中 率
较 CABG 组 降 低( 分 别 为 0.3% [2,233 例 中 有 6 例 ] 和
1.0% [2,245 例中有 23 例 ];HR: 0.26; 95% CI 0.11-0.64; P = 0.003),但这个差异在 5 年时就不再明显了(分别为 2.6% [2,233 例 中 有 43 例 ] 和 2.6% [2,245 例 中 有 51 例 ];HR: 0.83; 95% CI: 0.55-1.24; P =0.36)( 图 3B)。7,040 例 MVD患者中,PCI 治疗后 30 天卒中率较 CABG 组降低(分别
为 0.4% [3,520 例中有 15 例 ] 和 1.2% [3,520 例中有 41 例 ];HR:0.36; 95% CI: 0.20- 0.65; P<0.001),这种差异在 5 年时
图 2 根据基线和治疗特征,PCI 和 CABG 后 5 年随访期卒中发生率的亚组分析
0.83 (0.63-1.09)
0.64 (0.42-0.98)
0.69 (0.48-0.99)
0.84 (0.62-1.13)
0.81 (0.62-1.06)
0.62 (0.38-1.01)
0.68 (0.52-0.89)
1.09 (0.70-1.70)
0.75 (0.56-1.00)
0.85 (0.58-1.24)
0.52 (0.37-0.75)
1.04 (0.77-1.42)
1.05 (0.55-2.00)
0.66 (0.51-0.86)
0.76 (0.48-1.20)
0.69 (0.52-0.92)
0.69 (0.52-0.91)
0.93 (0.57-1.51)
0.75 (0.57-0.98)
0.83 (0.54-1.27)
0.87 (0.48-1.23)
0.65 (0.42-1.03)
0.88 (0.52-1.50)
HR (95% CI)
0.19
0.038
0.042
0.25
0.12
0.054
0.005
0.71
0.053
0.40
<0.001
0.78
0.89
0.002
0.24
0.010
0.008
0.76
0.038
0.39
0.28
0.065
0.64
P 值
0.31
0.40
0.37
0.08
0.65
0.004
0.18
0.71
0.32
0.75
0.73
相关性 P 值
111/4394 (2.8)
53/1371 (4.8)
72/2940 (2.7)
92/2825 (3.8)
118/3953 (3.3)
42/1558 (3.3)
127/3913 (3.8)
37/1835 (2.1)
102/3862 (3.1)
61/1873 (3.6)
86/2171 (4.9)
78/3594 (2.4)
18/440 (4.7)
139/4724 (3.3)
42/1417 (3.3)
115/3739 (3.5)
122/4597 (3.0)
33/833 (4.5)
117/4232 (3.3)
47/1533 (3.2)
40/1585 (3.0)
45/1545 (3.6)
30/927 (3.8)
CABG
94/4380 (2.5)
35/1373 (3.0)
51/2971 (2.0)
78/2782 (3.3)
97/3958 (2.7)
27/1548 (2.3)
88/3880 (2.7)
41/1859 (2.4)
81/3982 (2.4)
48/1744 (3.1)
47/2215 (2.6)
82/3538 (2.7)
19/424 (5.1)
94/4734 (2.2)
33/1438 (2.6)
80/3700 (2.4)
84/4447 (2.2)
39/1518 (2.6)
31/856 (4.4)
31/1533 (2.6)
33/1677 (2.4)
90/4235 (2.7)
25/871 (3.3)
PCI亚组
0.3 210.5支持PCI 支持CABGHR
(95% CI)
5
性别
男
女
年龄基线
<65
65或更大
身体指数
<30
30或更高
高血压
是
否
高胆固醇血症
是
否
糖尿病
是
否
外周血管病变
是
否
MI病史
是
否
LVEF
正常
异常(<50%)
病变复杂性
SYNTAX分数 0-22
SYNTAX分数 23-32
SYNTAX分数 >33
PCI
DES
BMS
缩略词如图1。

50 JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
同样显著(分别为 2.7% [3,520 例中有 86 例 ] 和 3.6% [3,520例中有 113 例 ];HR: 0.74; 95% CI: 0.56-0.99;P=0.039)。
卒中对死亡的影响 随访过程中共发生 976 例死亡。血运
重建后 30 天内发生卒中的患者,与未发生的患者相比,
5 年死亡率较高,无论是 CABG 组(分别为 41.5% [64 例
中 有 23 例 ] 和 8.9% [5,701 例 中 有 414 例 ];P<0.001)
还 是 PCI 组(分 别 为 45.7% [21 例 中 有 9 例 ] 和 11.1%
[5,732 中有 530 例 ];P<0.001)(图 4)。
全因死亡或卒中的联合终点 如表 2 所示,PCI 后全因死
亡或卒中 30 天发生率为 1.6% (5,753 例中有 91 例),而
CABG 后 为 2.4%(5,765 中 有 135 例)(P=0.003)。 而
31 天到 5 年间 PCI 后全因死亡或卒中的联合发生率要
高 于 CABG (分 别 为 11.6% 和 9.3%,HR:1.26;95% CI: 1.11-1.32; P <0.001)。最终,5 年时两组的全因死亡
图 3 伴有或不伴有 DM、LM 或 MVD 的患者,PCI 和 CABG 后 5 年随访期中卒中发生率
0 126 18 24随访(月)
30 36 42 48
2.6%
4.9%
2.4%
2.6%
54 60
PCI-DMCABG-DM
> HR: 0.52 (95% CI: 0.37-0.75, P < 0.001)PCI-非 DMCABG-非 DM
> HR: 1.04 (95% CI: 0.77-1.42, P = 0.78)
PCI-LMCABG-LM
> HR: 0.83 (95% CI: 0.55-1.24, P = 0.36)PCI-MVDCABG-MVD
> HR: 0.74 (95% CI: 0.56-0.99, P = 0.039)
风险数
2,171 1,9211,986 1,862 1,744 1,579 1,287 1,141 1,007 846 6042,215 2,0252,097 1,955 1,842 1,647 1,354 1,209 1,068 890 6713,594 3,3613,435 3,276 3,157 2,971 2,390 2,305 2,206 2,111 1,5993,538
CABGPCICABGPCI
(DM)(DM)(非DM)(非DM) 3,3903,448 3,310 3,202 3,006 2,434 2,345 2,252 2,148 1,690
A
0
3
2
1
4
5
累积
卒中
率(
%)
0 126 18 24随访(月)
30 36 42 48
2.7%
3.6%
2.6%
2.6%
54 60
风险数
2,245 2,0612,132 1,985 1,875 1,659 917 856 788 714 3982,233 2,1112,175 2,033 1,938 1,700 968 903 838 769 4763,520 3,2213,289 3,153 3,026 2,891 2,760 2,590 2,425 2,243 1,8053,520
CABGPCICABGPCI
(LM)(LM)(MVD)(MVD) 3,3043,370 3,232 3,106 2,953 2,820 2,651 2,482 2,269 1,885
B
0
3
2
1
4
5
累积
卒中
率(
%)
在5年随访时间内有或者无糖尿病患者PCI(经皮冠脉介入)与CABG(冠脉旁移植术)后的卒中率。(A)以及患者伴有左主干病变(LM)或多血管变病(MVD)(B)。重要糖尿病治疗相关性(相互作用P=0.004)。没有探究到LM与MVD之间相关性,因为各组并不相互排斥。缩略词如图1。

51JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
或卒中联合发生率并没有统计学差异(分别为 13.0% 和
11.4%;HR: 1.11; 95% CI: 0.99-1.24; P=0.069)。虽然没有
明显的关联,但在糖尿病和较高 SYNTAX 分值的患者中,
CABG 相对 PCI 具有较多获益。
PCI 和 CABG 两组间 30 天全因死亡或卒中的联合终
点率,在 MVD 患者(分别为 1.8% [n=62] 和 2.6% [n=90];HR 0.68; 95% CI: 0.49-0.94; P =0.020) 和 LM 患 者( 分
别为 1.3% [n = 29] 和 2.0% [n=45];HR: 0.64; 95% CI: 0.40-1.02;P=0.062)中都无明显差异。31 天到 5 年之间,两
组间全因死亡或卒中联合终点率在 MVD 患者分别为
11.9%(n= 371) 和 9.1% (n = 274)(HR: 1.31; 95% CI: 1.12-1.53; P<0.001),LM 患 者 中 分 别 为 11.3% (n = 174)
和 10.2%(n= 147)(HR: 1.16; 95%CI: 0.93-1.44; P =0.20)。到
5 年时,两组间全因死亡或卒中联合终点率在 MVD 患者
中有差异(13.5% [n = 433] 和 11.4% [n = 364]; HR:1.16; 95% CI: 1.01-1.33; P=0.041),但在 LM 患者中无差异(12.4% [n= 203] 和 12.0% [n = 192]; HR:1.02; 95% CI: 0.84-1.25;P =0.81)。
讨论
本分析汇总 11 项随机临床研究,比较了多支血管
病变或 LM 病变治疗的 CABG 或 PCI 手术,结果发现
CABG 后 5 年卒中发生率显著升高。术后 30 天较高的卒
中发生率是造成这个差异的原因。两组之间在 31 天到随
访 5 年间的卒中发生率是相似的。与 PCI 相比,CABG
后 5 年卒中发生风险较高的患者仅限于 MVD 和糖尿病患
者。术后 30 天内卒中的发生与长期死亡率增加密切相关,
到 5 年时接近 50%。与 CABG 相比,PCI 后 30 天全因死
亡或卒中的联合终点率较低,但 5 年时较高,尤其是伴
有糖尿病、MVD 以及其 SYNTAX 分值较高的患者。
围手术期卒中在 CABG 后更常见,在目前大型研究
中绝对风险增加约 0.7%。强调卒中外科手术风险增加的
机制是多方面的。首先,大多数 CABG 手术是在体外循
环下进行的,需要置管和夹闭主动脉;即使是在非体外循
环下进行,近段吻合术也涉及主动脉的操作 [19-21]。队列研
究发现,如果不能完全避免,通过非主动脉的非体外循环
CABG 手术来尽量减少主动脉的操作,可以显著减少卒中
的发生率 [22-23]。采用双侧乳内动脉避免近段吻合和侧夹闭
主动脉,可减少卒中发生率 [24]。目前的研究中,双侧乳内
动脉 CABG 手术的使用率相对较低。第二,CABG(不是
PCI)常需要减少术后出血的治疗,如使用氨甲环酸,会
造成高凝状态,增加卒中风险 [25]。第三,CABG 后房颤更
多,增加术后早期卒中的风险 [26,27]。第四,术中低灌注期
和术后早期低心排综合征会损害脑灌注,导致缺血和部分
脑区卒中 [28]。另外一种假设是支架置入后 DAPT 的常规使
用是PCI后卒中发生低的原因 [29]。然而,在目前的研究中,
我们没有发现这与 CABG 后低卒中率有关。
我们的界标分析提示 30 天后卒中发生率在 CABG和 PCI 间是类似的。如一些研究所示 [30],与 CABG 相
图 4 血运重建后 30 天内发生或未发生卒中的患者,接受 PCI 和 CABG 后的死亡率
0 126 18 24随访(月)
30 36 42 48
29.8%
2.1%2.4%
20.3%
45.7%
41.5%
11.1%
8.9%
54 60
PCI-卒中CABG-卒中
> P < 0.001PCI-无卒中CABG-无卒中 > P < 0.001
64 5051 49 48 43 34 32 27 25 1621 1314 13 13 11 10 9 7 7 5
5,701 5,3105,428 5,174 4,946 4,599 3,727 3,502 3,272 3,012 2,2475,732
风险数
CABGPCICABGPCI
(卒中)(卒中)(无卒中)(无卒中) 5,4455,559 5,305 5,088 4,708 3,843 3,607 3,375 3,086 2,400
0
30
20
10
40
50
累积
卒中
率(
%)
实线代表随访30天内发生卒中的患者,以及虚线 代表患者无卒中。随访开始于30天,此处记为0次。缩略词如图1和图3。

52 JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
表 2 全因死亡或卒中的联合终点30 天 31 天 -5 年 5 年
PCI vs.CABG
HR(95% CI)
P 值相互作用P 值
PCI vs.CABG
HR(95% CI)
P 值相互作用P 值
PCI vs.CABG
HR(95% CI)
P 值相互作用P 值
全部1.6 (91) vs.2.4 (135)
0.67(0.51–0.87)
0.003 -11.6 (545) vs.
9.3 (421)1.26
(1.11–1.43)<0.001 -
13.0 (636) vs.11.4 (556)
1.11(0.99–1.24)
0.069 -
糖尿病
有2.2 (48) vs.
3.1 (66)0.70
(0.48–1.02)0.063 0.68
15.4 (263) vs.11.2 (180)
1.39(1.15–1.68)
<0.001 0.1417.2 (311) vs.
13.9 (246)1.20
(1.02–1.42)0.031 0.19
无1.2 (43) vs.
1.9 (69)0.63
(0.43–0.92)0.016
9.5 (282) vs.8.3 (241)
1.15(0.97–1.37)
0.1110.6 (325) vs.
10.0 (310)1.03
(0.88–1.21)0.69
SYNTAX 分值
0–220.9 (14) vs.
2.2 (34)0.42
(0.23–0.79)0.007 0.015
10.3 (116) vs.8.0 (94)
1.19(0.91–1.57)
0.20 0.2211.1 (130) vs.
10.0 (128)0.98
(0.77–1.26)0.89 0.09
22-321.4 (23) vs.
2.1 (32)0.65
(0.38–1.12)0.12
12.8 (162) vs.11.4 (123)
1.18(0.93–1.49)
0.1614.0 (185) vs.
13.3 (155)1.07
(0.86–1.32)0.56
≥ 332.6 (23) vs.
2.7 (25)0.97
(0.55–1.71)0.92
16.3 (111) vs.11.1 (75)
1.61(1.20–2.16)
0.00118.5 (134) vs.
13.6 (100)1.45
(1.12–1.88)0.005
事件发生率是基于Kaplan-Meier方法,以时间-首次事件方式分析,以%(n)表达。CI=置信区间;HR=风险比;其他缩略词参见表1。
比,PCI 后常需要更多的反复血运重建,但这并没有增加
随访期间卒中的发生率。而且,亚组分析中,基线特征
中除了糖尿病,没有发现明显的异质性。糖尿病患者中,
CABG 后卒中的发生率接近 PCI 后的两倍,但在非糖尿
病患者中,两者几乎相等(相关性 P=0.004)。该发现应
该形成一个假说,并在以后的研究中去证实。
对于 MVD 和 LM 疾病的患者,与 CABG 相比,PCI的围手术期卒中发生率较低,但对于 LM 患者,PCI 后长期
卒中的风险高于 CABG 术后。这个发现可能源于 NOBLE研究的纳入,该研究中 PCI 后长期卒中发生率令人费解地
高于 CABG 后 [17],但在其他随机研究中并未得到证实。
当把全因死亡和卒中作为联合终点时,PCI 和 CABG之间的 5 年死亡率或卒中发生率并没有明显差异。然而
MVD、糖尿病和 SYNTAX 较高分值的患者中,CABG 后
的预后较好,但在 LM 患者中则没发现。
CABG 和 PCI 后卒中严重程度是否有差异尚不清楚。
FREEDOM 研究中,CABG 后严重致残性卒中率占所有卒
中患者的 55%,PCI 后仅为 27%[13]。SYNTAX 研究中对卒
中的深入分析发现,CABG 后卒中患者离院时有 68% 存在
局灶功能缺失,而 PCI 后为 47%[31]。显然,卒中患者的生
活质量是下降的,但尚无研究比较 CABG 或 PCI 后卒中
患者的生活质量差异来明确 CABG 后较高的局灶功能缺
失会导致长期较差的生活质量。不过,我们发现术后 30天发生卒中的患者与未发生的患者比较,术后 5 年死亡
率明显增高,无论卒中发生在 CABG 后还是 PCI 后。
本分析有许多优点。重要的是,研究者分享研究数据,
这样才能对如卒中等低发病率的结局进行比较,以及评估
患者亚组中的安全性和有效性 [32]。本汇总分析来自 11 项
随机临床研究,足以分析CABG和PCI后卒中的发生情况。
此外,纳入来自不同地理区域的患者增加了我们结果的外
延性。所有的试验都前瞻性地纳入患者,并且有一个临床
事件委员会来进行裁决,确定卒中的诊断。
研究局限性 首先,从 1995 年到 2015 年病人入组期间,
CABG 和 PCI 技术都已发生变化。虽然我们发现 PCI 后
无论是 BMS 还是 DES,CABG 无论是非体外循环还是
体外循环,卒中发生是一致的,但是否有其他不可测的
因素发挥作用尚不清楚。第二,各研究间基线特征还是
有一些异质性,越近的研究纳入的患者冠脉疾病更复杂,
糖尿病比例更高。第三,许多入组的研究没有收集一些
潜在与 CABG 后卒中有关的变量(如主动脉操作,术后
心房颤动),因此,我们的多因素模型没有将这些可能预
测围手术期卒中的因素纳入其中。第四,由于独立神经
功能评估没有常规进行或用于卒中的诊断,因此,卒中
发生率可能被低估。卒中神经科专家的参与已被证明会
增加主动脉瓣术后卒中的病例数,因此在目前的经导管
和外科主动脉瓣膜置换的相关研究中,这是强制要求的[33]。第五,由于只有 2 项研究收集了卒中严重度和局灶
功能缺失的数据,且定义不尽相同,因此本分析没有对

53JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
这些数据进行评估。最后,抗血小板治疗可降低卒中的
发生,但我们缺少随访中的药物方案。不过,大多数患
者在 CABG 或 PCI 后接受了至少 1 种抗血小板药物,目
前普遍认为这足以预防卒中的发生。
结论
本次大规模、基于随机试验的个体患者数据的汇总分
析,纳入了接受冠状动脉血管重建的多血管或 LM 冠状动
脉疾病患者,结果提示,与 CABG 相比,PCI 显著降低了
30 天和 5 年的卒中发生率,在 31 天到 5 年之间卒中发生
率相似。CABG 增加 5 年卒中的风险仅限于 MVD 和糖尿
病患者。CABG 后和 PCI 后 30 天内卒中患者 5 年死亡率很
高。在综合评估这些供选择的血管重建方案的长期风险 - 效益比时,应考虑 PCI 后和 CABG 后卒中的差异风险。
参考文献
1. Hlatky MA, Boothroyd DB, Bravata DM, et al.Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet 2009;373:1190–7.2. Daemen J, Boersma E, Flather M, et al. Longterm safety and efficacy of percutaneous coronary intervention with stenting and coronary artery bypass surgery for multivessel coronary artery disease: a meta-analysis with 5-year patient-level data from the ARTS, ERACI-II, MASS-II, and SoS trials. Circulation 2008;118:1146–54.3. Stefanini GG, Holmes DR Jr. Drug-eluting coronaryartery stents. N Engl J Med 2013;368:254–65.4. Palmerini T, Biondi-Zoccai G, Reggiani LB, et al.Risk of stroke with coronary artery bypass graft surgery compared with percutaneous coronary intervention. J Am Coll Cardiol 2012;60:798–805.5. Head SJ, Milojevic M, Daemen J, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018;391:939–48.6. Stewart LA, Clarke M, Rovers M, et al., for the PRISMA-IPD Development Group. Preferred Reporting Items for Systematic Review and MetaAnalyses of individual participant data: the PRISMA-IPD Statement. JAMA 2015;313:1657–65.
7. Rodriguez A, Bernardi V, Navia J, et al., for ERACI II Investigators. Argentine Randomized Study: Coronary Angioplasty with Stenting versus Coronary Bypass Surgery in patients with MultipleVessel Disease (ERACI II): 30-day and one-year follow-up results. J Am Coll Cardiol 2001;37:51–8.8. Serruys PW, Unger F, Sousa JE, et al. Arterial Revascularization Therapies Study Group. Comparison of coronary-artery bypass surgery and stenting for the treatment of multivessel disease.N Engl J Med 2001;344:1117–24.9. Hueb W, Soares PR, Gersh BJ, et al. The Medicine, Angioplasty, or Surgery Study (MASS-II): a randomized, controlled clinical trial of three therapeutic strategies for multivessel coronary artery disease: one-year results. J Am Coll Cardiol 2004;43:1743–51.10. SoS Investigators. Coronary artery bypass surgery versus percutaneous coronary intervention with stent implantation in patients with multivessel coronary artery disease (the Stent or Surgery trial): a randomised controlled trial. Lancet 2002;360:965–70.11. Serruys PW, Morice MC, Kappetein AP, et al.,for the SYNTAX Investigators. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med 2009;360:961–72.12. Park SJ, Kim YH, Park DW, et al. Randomized trial of stents versus bypass surgery for left main coronary artery disease. N Engl J Med 2011;364:1718–27.
13. Farkouh ME, Domanski M, Sleeper LA, et al.,for the FREEDOM Trial Investigators. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med 2012;367:2375–84.14. Kamalesh M, Sharp TG, Tang XC, et al.Percutaneous coronary intervention versus coronary bypass surgery in United States veterans with diabetes. J Am Coll Cardiol 2013;61:808–16.15. Park SJ, Ahn JM, Kim YH, et al., for the BEST Trial Investigators. Trial of everolimus-eluting stents or bypass surgery for coronary disease.N Engl J Med 2015;372:1204–12.16. Stone GW, Sabik JF, Serruys PW, et al. , for the EXCEL Trial Investigators. Everolimus-eluting stents or bypass surgery for left main coronary artery disease. N Engl J Med 2016;375:2223–35.17. Makikallio T, Holm NR, Lindsay M, et al., for the NOBLE Study Investigators. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): a prospective, randomised, open-label, non-inferiority trial. Lancet 2016;388:2743–52.18. Buszman PE, Kiesz SR, Bochenek A, et al.Acute and late outcomes of unprotected lef t main s tent ing in comparison with surgical revascularization. J Am Coll Cardiol 2008;51:538–45.19. Head SJ, Borgermann J, Osnabrugge RL, et al.Coronary artery bypass grafting: part 2—
optimizing outcomes and future prospects. Eur Heart J 2013;34:2873–86.
通 信 地 址 ADDRESS FOR CORRESPONDENCE: Dr. Stuart J.Head,
Department of Cardiothoracic Surgery, Erasmus University Medical
Center, PO Box 2040, 3000 CA, Rotterdam, the Netherlands. E-mail:
[email protected]. Twitter: @ErasmusMC.
观 点
展望患者护理能力和手术技能 接受冠脉血运重建治
疗的多支血管或 LM 疾病患者,PCI 后 30 天内卒中发
生率低于 CABG,但接下来 5 年时发生率是接近的。
转化前景 需要更多的研究来制定策略以预防 CABG后患者围手术期卒中。

54 JACC VOL. 72, NO. 4, 2018JULY 24, 2018:386–98
Head et al.CABG 与 PCI 后卒中的发生率
20. Lamy A, Devereaux PJ, Prabhakaran D, et al.,for the CORONARY Investigators. Off -pump or onpump coronary-ar te ry bypass grafting at 30 days.N Engl J Med 2012;366:1489–97.21. Diegeler A, Borgermann J, Kappert U, et al., for the GOPCABE Study Group. Off-pump versus onpump coronary-artery bypass grafting in elderly patients. N Engl J Med 2013;368:1189–98.22. Börgermann J, Hakim K, Renner A, et al.Clampless off-pump versus conventional coronary artery revascularization: a propensity score analysis of 788 patients. Circulation 2012;126 Suppl 1:S176–82.23. Zhao DF, Edelman JJ, Seco M, et al. Coronary artery bypass grafting with and without manipulation of the ascending aorta: a network metaanalysis. J Am Coll Cardiol 2017;69:924–36.24. Tarakji KG, Sabik JF 3rd, Bhudia SK, Batizy LH,Blackstone EH. Temporal onset, risk factors, and outcomes associated with stroke after coronary artery bypass grafting. JAMA 2011;305:381–90.25. Myles PS, Smith JA, Forbes A, et al., for the ATACAS Investigators of the
ANZCA Clinical Trials Network. Stopping vs. continuing aspirin before coronary artery surgery. N Engl J Med 2016;374:728–37.26. Villareal RP, Hariharan R, Liu BC, et al. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol 2004;43:742–8.27. Kosmidou I, Chen S, Kappetein AP, et al. Newonset atrial fibrillation after PCI or CABG for left main disease: the EXCEL trial. J Am Coll Cardiol 2018;71:739–48.28. Hogue CW Jr., Murphy SF, Schechtman KB,Davila-Roman VG. Risk factors for early or delayed stroke after cardiac surgery. Circulation 1999;100:642–7.29. Iqbal J, Zhang YJ, Holmes DR, et a l . Optimal medical therapy improves clinical outcomes in patients undergoing revascularization with percutaneous coronary intervention or coronary artery bypass grafting: insights from the Synergy Between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery (SYNTAX) trial at the 5-year follow-up. Circulation 2015;131:1269–77.30. Parasca CA, Head SJ, Milojevic M, et al. Incidence, characteristics, predictors, and
outcomes of repeat revascularization after percutaneous coronary intervention and coronary artery bypass grafting: the SYNTAX trial at 5 years. J Am Coll Cardiol Intv 2016;9:2493–507.31. Mack MJ, Head SJ, Holmes DR Jr., et al.Analysis of stroke occurring in the SYNTAX trial comparing coronary artery bypass surgery and percutaneous coronary intervention in the treatment of complex coronary artery disease. J Am Coll Cardiol Intv 2013;6:344–54.32. Stefanini GG, Baber U, Windecker S, et al.Safety and efficacy of drug-eluting stents in women: a patient-level pooled analysis of randomised trials. Lancet 2013;382:1879–88.33. Kappetein AP, Head SJ, Genereux P, et al.Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document. J Am Coll Cardiol 2012;60:1438–54.
关键词 冠脉旁路移植术,左主干,死亡率,
多支血管,经皮冠脉介入,支架,卒中
附录 补充图和表,请见本文的线上版本。
广东省心血管病研究所 陈纪言 冯颖青 何旭瑜
冠状动脉旁路移植术(CABG)和经皮冠状动脉介入治疗(PCI)均用于冠脉多支病变和 / 或合并左主干病变患
者的冠脉血运重建。卒中是临床上关注的术后严重并发症之一。但由于卒中在 CABG 或 PCI 术后的发生率并不高,
需要较大的样本量才能进行研究。该文章荟萃了 11 项随机临床试验进行数据分析,分析的研究包括有 ERACI II、ARTS 研究、MASS II 研究、SoS 研究、SYNTAX 研究、PRECOMBAT 研究等等。比较 CABG 和 PCI 术后的 30 天
和 5 年的卒中发生率,并探讨卒中对 5 年死亡率的影响。结果共纳入患者 11,518 例,随机分成 PCI 组(n=5,753)和
CABG 组(n=5,765),平均随访 3.8±1.4 年,共发生卒中 293 例。30 天时,PCI 组卒中发生率比 CABG 组低(0.4% vs. 1.1%,P<0.001)。5 年随访,PCI 组卒中发生率明显低于 CABG 组(2.6% vs. 3.2%,P= 0.027)。31 天至 5 年之间
的卒中发生率相当(PCI:2.2% vs. CABG:2.1%,P=0.72)。但是,糖尿病患者与非糖尿病患者中卒中的发生情况并
不一样,糖尿病患者 PCI 术后 5 年的卒中发生率比 CABG 术后低(2.6% vs. 4.9%);非糖尿病患者 PCI 术后和 CABG术后的卒中发生率无明显差异(PCI:2.6% vs. CABG:2.4%)(相关性 P=0.004)。术后 30 天内发生过卒中的患者无
论在 PCI 组( 45.7% vs. 11.1%,P < 0.001)还是 CABG 组(41.5% vs. 8.9%,P < 0.001),其 5 年的死亡率显著升高。
从以上的荟萃分析结果提示:PCI 与 CABG 相比,术后 30 天及 5 年的卒中风险较低,而 31 天至 5 年内的卒中风险相
近。同时,CABG 术后的糖尿病患者比 PCI 术后的糖尿病患者发生卒中的风险明显升高。然而,荟萃分析的结果有
一定的不足,首先入组研究的时间跨度接近 20 年,期间患者接受的 PCI 术或 CABG 术均有不同程度的进展,不同时
段的技术条件对结果有一定的影响。其次,不同研究的人群基线情况有所不同,例如冠脉病变程度、合并糖尿病比例
等不同。另外,因神经系统症状并非是常规评估,部分研究可能会出现卒中诊断的漏诊,导致低估了发生率。并且,
CABG 术后可能因为出血的原因而使用了止血药物,而 PCI 术后双抗血小板 1 年,均对卒中的发生率有影响。因此,
在综合评估血管重建方案的短期及长期风险收益时,应考虑卒中的不同风险。
点 评

JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY ©2018 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
VOL. 72, NO. 11, 2018ISSN 0735-1097
与 2017 年 ACC/AHA 高血压指南定义的 1 期高血压相关的长期心血管疾病风险Long-Term Cardiovascular Risk Associated With Stage 1 Hypertension Defined by the 2017 ACC/AHA Hypertension Guideline
Yue Qi, MD, PHD*, Xueyu Han, MD*, Dong Zhao, MD, PHD, Wei Wang, MD, Miao Wang, MD, Jiayi Sun, MD, Jun Liu, MD, Yan Li, MD, Shen Gao, MD, Yongchen Hao, PHD, Qiuju Deng, PHD, Jing Liu, MD, PHD
翻译:北京大学第三医院心内科 杨林承;审校:暨南大学附属第一医院心内科 刘福成
摘 要
背景 2017 年美国心脏病学会(American College of Cardiology, ACC)/ 美国心脏协会(American Heart Association, AHA)高血压指南近期将收缩压 130-139mm Hg 和(或)舒张压 80-89mm Hg 定义为 1 期高血压。在衡量此 BP 分
级标准在中国人群的适用性时应量化其对心血管风险的影响程度。
目的 本研究目的为评价与 1 期高血压相关的心血管疾病(cardiovascular disease, CVD)的相对风险和人群归因危
险度以及年龄特异性差异。
方法 中国多省市队列研究共纳入 21,441 例年龄≥ 35 岁且无基线 CVD 病史的受试者,对其进行长达 20 年的随访。
计算与 1 期高血压相关的 CVD 校正风险比(hazard ratio, HR)及人群归因危险度。
结果 队列中,25.8% 的受试者诊断为 1 期高血压。在 35-59 岁的受试者中,与 BP < 120/80mm Hg 相比,1 期高
血压患者 CVD 发病风险为 1.78 (95% 置信区间 [confidence interval, CI] 1.50-2.11),冠心病发病风险为 HR:1.77(95% CI 1.33-2.36),卒中发病风险为 HR:1.79(95% CI 1.45-2.22),CVD 死亡率为 HR:2.50(95% CI 1.66-3.77)。在
35-59 岁的受试者中,26.5% 的心血管死亡及 13.4% 的心血管事件与 1 期高血压相关。而在年龄≥ 60 岁的受试者中,
与 BP <120/<80mm Hg 者相比,1 期高血压并不增加 CVD 风险且未发现与此分级相关的归因危险度。在随访超
过 15 年时,在 35-59 岁的受试者中,65.0% 的 1 期高血压患者 BP 升高至 140/90mm Hg 或更高水平,其心血管疾
病风险较 BP <130/<80mm Hg 的受试者增加 3.01 倍。
结论 2017 年 ACC/AHA 高血压指南定义的 1 期高血压对中国中青年人群的心血管风险影响已获得有力证据,但
缺乏年龄≥ 60 岁的人群心血管风险相关支持数据。
From the Department of Epidemiology, Beijing An Zhen Hospital, Capital Medical University, Beijing, China; Beijing Institute of Heart, Lung and Blood Vessel Diseases, Beijing, China; The Key Laboratory of Remodeling-Related Cardiovascular Diseases, Ministry of Education, Beijing, China; and the Beijing Municipal Key Laboratory of Clinical Epidemiology, Beijing, China. *Drs. Qi and Han contributed equally to this work and are joint first authors. This work was supported by the National Key Research and Development Program of China (grant 2016YFC0900902); the National Science & Technology Pillar Program (grants 2011BAI09B01, 2011BAI11B03, 2006BAI01A01, and 2006BAI01A02); and the capital health research and development of special (grant 2016-1-1051). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.Manuscript received April 16, 2018; revised manuscript received June 7, 2018, accepted June 12, 2018.
美国心脏病学会(American College of Cardiology, ACC)/ 美国心脏协会(American Heart Association, AHA)临床
实践指南小组近期发布了 2017 年高血压指南 [1]。该版指
南的一项更新是将收缩压(systolic blood pressure, DBP)
130-139mm Hg 和(或)舒张压(diastolic blood pressure, DBP)80-89mm Hg 定义为 1 期高血压。
PUBLISHED BY ELSEVIER https://doi.org/10.1016/j.jacc.2018.06.056

56 JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
高血压的定义随时间演
变。从 1977 年时将 SBP/DBP为≥ 160/100mm Hg 诊断为高血
压 [2], 到 1997 年 ≥ 140/90mm Hg 为高血压 [3],而 2017 年将
这一诊断标准进一步降低至
≥ 130/80mm Hg。观察性研究、
临床试验及健康经济学评估
研究的结果均表明了血压控
制对预防心血管疾病的重要
性,而这些研究结果推动了高血压定义的演变。
尽管 2017 年 ACC/AHA 高血压指南已经阐述了新定
义的 1 期高血压对美国人群的影响 [1],但对其是否适用
于其他人群尚不明确,特别是其是否适用于卒中死亡风
险高 [4,5]、高血压患病率高 [6-10] 及老年人群多 [11] 的中国人
群。1 期高血压是否适用主要与该血压(blood pressure, BP) 分级对人群的影响有关,包括高血压进展的风险、心
血 管 疾 病(cardiovascular disease, CVD) 风 险、 治 疗 获
益及经济效益。在我们的既往研究中,在 15 年的随访
期 内,73.2% 的 SBP 130-139mm Hg 的 受 试 者 及 68.9%的 DBP 85-89mm Hg 的受试者最终罹患高血压,即 SBP/DBP ≥ 140/90mm Hg[12]。此外,中国国家高血压调查研究
的随访数据表明,血压升高至高血压前期者(广义 SBP/DBP 为 120-139/80-89mm Hg)心血管风险即增加,但该
血压水平对≥ 65 岁的人群影响不大 [13]。新版 ACC/AHA高血压指南定义的 1 期高血压(SBP/DBP 为 130-139/80-89mm Hg)在中国人群中对 CVD 影响程度的大小及其对
青年人群和老年人群影响程度是否一致尚需进一步研究。
因此,我们在中国受试者中进行随访 20 年的队列研
究,评估与 2017 年 ACC/AHA 高血压指南定义的 1 期高
血压相关的 CVD 的相对风险及人群归因危险度,并检验
风险是否存在年龄特异性。
方法
研究设计与研究人群 本研究为已发表的中国多省队列研
究(Chinese Multi-provincial Cohort Study, CMCS) 的 延
伸 [14]。共纳入原 CMCS 研究 11 个省中 8 个省共计 21,953例受试者,其中 16,811 例 35-64 岁受试者于 1992 年及
1993 年入组。此外,3,129 例 35-64 岁受试者于 1996 年
至 1999 年间入组,2,013 例年龄≥ 35 岁的受试者于 2004年入组。抽样方法详见在线图 1。本研究由首都医科大学
附属北京安贞医院伦理委员会批准。已取得全部受试者
的知情同意。
从基线到 2013 年 12 月 31 日,每 1-2 年对受试者新
发 CVD 事件进行一次随访,随访方式以主动询问为主,
以地方疾病监测系统为辅。20 年随访率为 81.0%。现阶
段研究中,21,441 例受试者(11,047 名男性,10,394 名
女性)数据完整,可用于分析基线血压水平与心血管风
险的关系;5,752 例受试者 1992 年及 1993 年初次体检数
据及 2007 年再次体检数据完整,可用于分析血压变化与
心血管风险的关系。
危险因素评估 在全部研究中,通过标准问卷获得受试者
人口学资料、吸烟史、诊疗史。体格检查时记录血压及
人体测量数据。受试者休息至少 5 分钟后应用水银血压
计测量受试者右臂坐位血压。Korotkoff 第 5 阶段起始读
数为舒张压。最终血压为连续两次血压测量结果的均值。
现症吸烟定义为每日吸烟≥ 1 根。糖尿病定义为空腹血糖
≥ 126mg/dl 或既往诊断糖尿病病史。
空腹≥ 8 小时后采集静脉血标本。血样采集当日即测
定总胆固醇、高密度脂蛋白胆固醇、甘油三酯及空腹血
糖水平 [14, 15]。
事件确定 记录并报告全部致命性及非致命性急性冠脉事
件及卒中事件。急性冠状动脉性心脏病(coronary heart disease, CHD)事件包括:急性心肌梗死、猝死及其他冠
心病死亡。急性卒中事件包括蛛网膜下腔出血、颅内出
血或脑梗死。研究早期诊断标准参照 WHO 发布的《心
血管疾病趋势及决定因素监测草案》,2003 年后诊断标准
因心肌梗死诊断技术的提高而进行修改 [14, 16-18]。内科医
师小组对全部上报事件及 CVD 相关死亡进行判定。在长
达 20 年的随访中(平均随访时间 13.7 年,中位随访时间
14.7 年;294,886 人 - 年),共发生 1,622 例初发 CVD 事
件(550 例 CHD 事件,1,142 例卒中)及 395 例 CVD 相
关死亡;在两次体检数据完整的 5,752 例受试者中共发生
523 例初发 CVD 事件。
统计分析 连续变量采用均值 ± 标准差或中位数(四分位
数范围)表示。分类变量采用数字和 / 或百分数表示。
为评价与血压水平相关的心血管风险,按血压水平对
受试者进行分组(收缩压 / 舒张压:<120/<80、120-129/ <80、130-139/80-89、140-159/90-99、≥160/ ≥100mm Hg)。 在符合应用前提假设的情况下,校正基线年龄、性别、
身体质量指数、目前吸烟状态、糖尿病、总胆固醇水平、
高密度脂蛋白胆固醇水平及降压药物治疗情况后,应
缩略词表BP=blood pressure
血压
CHD=coronary heart disease
冠状动脉性心脏病
CI=confidence interval
置信区间
CVD=cardiovascular disease
心血管疾病
DBP=diastolic blood pressure
舒张压
HR=hazard ratio
风险比
SBP=systolic blood pressure
收缩压

57JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
用 Cox 比例风险回归模型计算不同血压组者 CVD 发病
率、CHD 发病率、卒中发病率及 CVD 死亡率的风险比
(hazard ratio, HR)。以血压<120/<80mmHg 的受试者作
为参照。为检测与 1 期高血压相关的心血管风险在 35-59岁受试者与≥ 60 岁受试者间是否存在异质性,应用 Cox比例风险回归模型计算年龄分组 ×1 期高血压的交互作
用,主要包括比较 1 期高血压与血压< 120/ < 80mm Hg组、年龄分组、1 期高血压 × 年龄分组、年龄分组 × 其
他协变量。应用经分组患病率及校正的 HR 计算得出的
人群归因危险度评估该分组中与 1 期高血压相关的 CVD比例。
为评估 15 年间血压分类变化情况及其与心血管风
险间的关系,依据基线血压及复测血压水平对受试者
进行分组(收缩压 / 舒张压:<130/<80、130-139/80-89、
≥ 140/ ≥ 90mm Hg 或接受降压治疗),最终共分为 9 个亚
组。以基线及复测血压水平<130/< 80mm Hg组为参考,
校正基线传统 CVD 危险因素后,应用 Cox 比例风险回归
模型计算血压变化对 CVD 患病风险影响的 HR。
考虑到竞争性事件,在排除外服用降压药物的受试
者后,应用 Fine 及 Gray 竞争风险回归法,进行敏感性分
析 [20],在不同年龄组间,以血压< 130/ < 80mm Hg 为
基础,进行与 1 期高血压相关的心血管风险的亚组分析。
应用 SAS 9.4(SAS Institute, Cary, North Carolina)统
计学软件进行统计分析。双侧 P 值小于 0.05 认为有显著
统计学意义。
结果
受试者的基线特征 收缩压平均值为 123.7±20.3mm Hg,
舒张压平均值为 80.2±12.0mm Hg。25.8% 的受试者血
压处于 130-139/80-89mm Hg 范围,即达到 2017 年 ACC/AHA 高血压指南定义的 1 期高血压标准。在 3 个年龄组中,
达到这一标准的受试者比例相似,但收缩压 <120mm Hg
表 1 研究受试者的基线特征
合计(N=21,441)
年龄分组 ( 岁 )
35–44 (n=8,551)
45–59 (n=10,734)
≥ 60(n=2,156)
年龄,岁 48.0 ± 8.8 39.3 ± 2.9 51.7 ± 4.2 64.0 ± 4.6
男性 11,047 (51.5) 3,992 (46.7) 5,865 (54.6) 1,190 (55.2)
目前吸烟状态 6,165 (28.8) 2,538 (29.7) 3,111 (29.0) 516 (23.9)
体重指数,kg/m2 24.2 ± 3.3 23.7 ± 3.2 24.4 ± 3.2 24.8 ± 3.6
腰围,cm 80.5 ± 9.7 78.0 ± 9.2 81.6 ± 9.5 85.4 ± 10.4
空腹血糖,mg/dl 93.9 ± 25.4 91.3 ± 21.5 95.0 ± 26.6 98.6 ± 31.9
糖尿病 1,597 (7.4) 406 (4.7) 881 (8.2) 310 (14.4)
总胆固醇,mg/dl 184.5 ± 38.1 176.4 ± 35.0 188.3 ± 37.9 198.0 ± 43.4
HDL 胆固醇,mg/dl 53.9 ± 14.3 54.7 ± 14.3 53.7 ± 14.2 51.5 ± 14.0
甘油三酯,mg/dl 106.0(75.0–145.0) 98.0(69.0–134.0) 110.0(79.0–153.0) 115.0(84.0–155.3)
接受降脂治疗 248 (1.2) 23 (0.3) 189 (1.8) 36 (1.7)
接受降压药物治疗 1,790 (8.3) 230 (2.7) 1,059 (9.9) 501 (23.2)
SBP,mm Hg 123.7 ± 20.3 116.6 ± 16.2 126.5 ± 20.7 137.6 ± 22.3
DBP,mm Hg 80.2 ± 12.0 77.7 ± 11.3 81.7 ± 12.1 82.1 ± 12.0
SBP/DBP 分类,mm Hg
<120/<80 8,158 (38.0) 4,349 (50.9) 3,454 (32.2) 355 (16.5)
120–129/<80 1,659 (7.7) 595 (7.0) 840 (7.8) 224 (10.4)
130–139/80–89 5,529 (25.8) 2,072 (24.2) 2,890 (26.9) 567 (26.3)
140–159/90–99 3,952 (18.4) 1,085 (12.7) 2,266 (21.1) 601 (27.9)
≥ 160/ ≥ 100 2,143 (10.1) 450 (5.2) 1,284 (12.0) 409 (18.9)
数值以均值±标准差(n%)或中位数(四分位间距)表示。DBP=舒张压;HDL=高密度脂蛋白;IQR=四分位间距;SBP=收缩压。

58 JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
且舒张压 <80mm Hg(正常血压)的受试者比例随年龄增
大而下降,而收缩压≥ 140mm Hg 或舒张压≥ 90mm Hg 的
受试者比例随年龄增大而升高(表 1)。
血压分类相关的心血管风险 在 35-44 岁及 45-59 岁的年龄
组中,与 BP 正常者相比,1 期高血压患者 CVD 风险显著
增高;但在≥ 60 岁的年龄组中并未发现此现象(表 2,图 1)。
在年龄 35-59 岁的受试者中,与此 BP 分级相关的 CVD 发
病率为 1.78(95% 置信区间 [confidence interval, CI]:1.50-2.11)、CHD 发病率为 HR:1.77(95% CI:1.33-2.36)、卒 中发病率为 HR:1.79(95% CI:1.45-2.22)、CVD 死亡率为 HR:2.50(95%CI:1.66-3.77)。与血压正常者相比,1 期
高血压患者的 CVD 死亡率 HR 显著高于血压 120-129/ <
80mm Hg 人群,与收缩压在 140-159mm Hg 范围内或舒张
压于 90-99mm Hg 范围内的人群接近。与之相反的,在年
龄≥ 60 岁的人群中,1 期高血压不增加任何 CVD 终点事
件的发生风险,但血压≥ 140/ ≥ 90mm Hg 的人群卒中发病
率及 CVD 死亡率风险显著升高。排除在基线接受降压治
疗的人群后(n=1,790)、考虑互竞风险(在线表 2)及以血
压< 130/ < 80mm Hg 受试者为参考的亚组分析中(在线
图 2),所得结果类似(在线表 1)。
在年龄 35-44 岁受试者及年龄 45-59 岁受试者中 1 期
高血压导致 CVD、CHD 及卒中发病的人群归因危险度为
10.6%-14.7%;而在年龄≥ 60 岁的受试者中为 1.8%-4.0%。
在两个年龄较小的亚组中,1 期高血压导致 CVD 死亡的人
群归因危险度高于其导致 CVD 发病的人群归因危险度(重
点插图)。概括而言,在年龄 35-59 岁的受试者中,26.5%的 CVD 死亡及 13.4% 的 CVD 发病与 1 期高血压相关。
BP 变化相关的心血管风险 本研究对年龄 35-59 岁的受试
表 2 血压分类与其对应 CVD 终点风险比SBP/DBP
分类(mm Hg)
nCVD 发病率 CHD 发病率 卒中发病率 CVD 死亡率
事件数量
校正 HR(95% CI)
事件数量
校正 HR(95% CI)
事件数量
校正 HR(95% CI)
事件数量
校正 HR(95% CI)
合计
< 120/ < 80 8,158 265 参考值 97 参考值 173 参考值 45 参考值
120–129/ < 80 1,659 106 1.51 (1.20–1.89) 43 1.56 (1.09–2.25) 67 1.48 (1.12–1.97) 17 1.32 (0.75–2.31)
130–139/80–89 5,529 387 1.70 (1.45–1.99) 153 1.69 (1.31–2.20) 251 1.73 (1.42–2.11) 84 2.13 (1.48–3.08)
140–159/90–99 3,952 434 2.24 (1.91–2.63) 135 1.65 (1.25–2.17) 318 2.62 (2.16–3.18) 102 3.03 (2.10–4.35)
≥ 160/ ≥ 100 2,143 430 3.79 (3.20–4.49) 122 2.27 (1.69–3.04) 333 4.77 (3.90–5.83) 147 7.18 (5.01–10.29)
35–44 岁
< 120/ < 80 4,349 83 参考值 26 参考值 60 参考值 10 参考值
120–129/ < 80 595 24 1.75 (1.11–2.76) 9 1.99 (0.93–4.29) 15 1.51 (0.86–2.67) 1 0.64 (0.08–5.00)
130–139/80–89 2,072 93 1.87 (1.38–2.54) 34 1.97 (1.16–3.35) 61 1.74 (1.21–2.51) 22 4.07 (1.90–8.73)
140–159/90–99 1,085 82 2.65 (1.92–3.66) 31 2.65 (1.52–4.63) 55 2.56 (1.74–3.77) 15 4.87 (2.11–11.24)
≥ 160/ ≥ 100 450 57 3.81 (2.61–5.55) 16 2.40 (1.20–4.80) 44 4.50 (2.91–6.96) 12 7.98 (3.17–20.08)
45–59 岁
< 120/ < 80 3,454 145 参考值 56 参考值 90 参考值 25 参考值
120–129/ < 80 840 58 1.49 (1.09–2.02) 24 1.52 (0.94–2.46) 38 1.57 (1.07–2.29) 9 1.29 (0.60–2.77)
130–139/80–89 2,890 233 1.72 (1.39–2.12) 92 1.63 (1.16–2.28) 152 1.83 (1.41–2.38) 49 2.08 (1.28–3.38)
140–159/90–99 2,266 262 2.20 (1.78–2.71) 75 1.40 (0.98–2.01) 198 2.77 (2.14–3.58) 54 2.54 (1.56–4.14)
≥ 160/ ≥ 100 1,284 274 3.97 (3.18–4.94) 77 2.21 (1.50–3.24) 213 5.20 (3.99–6.80) 86 6.48 (4.00–10.49)
≥ 60 岁
< 120/ < 80 355 37 参考值 15 参考值 23 参考值 10 参考值
120–129/ < 80 224 24 0.93 (0.55–1.55) 10 0.93 (0.42–2.08) 14 0.87 (0.45–1.70) 7 1.05 (0.40–2.76)
130–139/80–89 567 61 1.04 (0.69–1.57) 27 1.13 (0.60–2.12) 38 1.04 (0.62–1.75) 13 0.89 (0.39–2.05)
140–159/90–99 601 90 1.43 (0.97–2.12) 29 1.13 (0.60–2.13) 65 1.66 (1.02–2.69) 33 2.23 (1.08–4.57)
≥ 160/ ≥ 100 409 99 2.16 (1.45–3.21) 29 1.47 (0.77–2.83) 76 2.64 (1.62–4.31) 49 4.60 (2.27–9.31)
CHD=冠心病;CI=置信区间;CVD=心血管疾病;HR=风险比;其它缩略词见表1。

59JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
图 1 不同年龄组 2017 年 ACC/AHA 高血压指南 1 期高血压患者的 CVD 风险比
0.006
0.191
0.027
0.014
0.25 0.50 1.00 2.00 4.00
326/4,96261/567
事件/1期高血压患者数量
风险比(95%CI)
相互作用P 值
126/4,96227/567
213/4,96238/567
71/4,96213/567
CVD发病率
心血管疾病
CHD发病率
卒中发病率
CVD死亡率
35-59岁 ≥60岁
ACC=美国心脏病学会;AHA=美国心脏学会;CHD=冠心病;CI=置信区间;CVD=心血管疾病。
重点插图 2017 年 ACC/AHA1 期高血压人群归因危险度
总计
11.811.814.014.0 12.712.7
1.81.8
35-44岁 45-59岁 ≥60岁
总计 35-44岁 45-59岁 ≥60岁 总计 35-44岁 45-59岁 ≥60岁
总计 35-44岁 45-59岁 ≥60岁
人群
归因
危险
度,
%
BA B
C DC D
12.412.4 12.712.7 14.114.1
2.32.3
人群
归因
危险
度,
%
0.0
10.0
20.0
30.0
40.0
50.0
0.0
10.0
20.0
30.0
40.0
50.0
19.919.9
43.943.9
19.719.7
–3.5–3.5
人群
归因
危险
度,
%
0.0
10.0
20.0
30.0
40.0
50.0
11.211.214.714.7
10.610.6
4.04.0
0.0
10.0人群
归因
危险
度,
%
20.0
30.0
40.0
50.0
2017年ACC/AHA高血压指南1期高血压人群归因危险度:心血管疾病发病率(A)、冠心病发病率(B)、卒中发病率(C)、心血管死亡 率(D)。ACC=美国心脏病学会;AHA=美国心脏学会。

60 JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
者(n=5,502)15 年随访时间内的 BP 变化及其与 CVD发病风险之间的关系做了进一步研究。1992 年即罹患 1期高血压的受试者,65.0% 在 15 年随访期内血压进一步
升高至≥ 140/90 mm Hg 的水平;与 15 年间血压维持在
< 130/ < 80 mm Hg 的受试者相比,其 CVD 发病率增
加 3.01 倍(95%CI:1.94-4.69)。21.5% 的受试者在随访
1 年后仍为 1 期高血压,其 CVD 发病风险增加 2.28 倍
(95%CI:1.28-4.06), 与 血 压 由 ≥ 140/ ≥ 90mm Hg 下 降
至 1 期高血压者 CVD 发病风险相似(HR:2.37, 95%CI:1.16-4.81)。与之相反的,15 年间血压水平由 1 期高血压
恢复至< 130/ < 80mm Hg 的受试者,其 CVD 发病风险
与血压 15 年间维持在<130/<80mm Hg 的受试者相近(图
2)。在两次检查中,排除接受降压治疗的人群(在线图 3)
及考虑互竞风险后(在线图 4),结果仍是相似。
讨论
本研究为一项随访 20 年的前瞻性队列研究,研究发现
在年龄 35-59 岁的中国人群中,与 BP 正常者相比,2017 年
版 ACC/AHA 高血压指南定义的 1 期高血压患者 CVD 风险
显著升高,该人群中 26.5% 的心血管死亡及 13.4% 的心血
管发病与其相关。但 1 期高血压与正常 BP 人群相比并不额
外增加年龄≥ 60 岁人群的心血管风险,且该人群中没有与 1
期高血压相关的人群归因危险度(重点插图)。
2017 年版 ACC/AHA 高血压指南定义的 1 期高血压
最近引起全球广泛关注。除了为采用这一新标准 [8,21-23] 后
诊断为高血压的患者人数增加而担忧之外,BP 分级在何
种程度上影响了心血管疾病风险也同样是至关重要的议
题。据本研究组所知,本研究为第一个在中国人群中定
量确定与 1 期高血压相关的心血管风险的前瞻性研究。
此外,随访期间多次测量血压使得评估 BP 持续处于 130-139/80-89mm Hg 这一范围对 CVD 发病率及死亡率的影
响具有可行性。
在中国 35-59 岁的人群中,与 BP 正常者相比 1 期高
血压患者 CVD 发病率升高 80%,高于中国国家高血压调
查随访中年龄< 65 岁高血压前期受试者的 CVD 风险(相
对风险:1.40;95%CI:1.30-1.51)[13]。值得注意的是,本
研究中,与 BP 正常者相比,1 期高血压相关的 CVD 死亡
HR 值显著高于血压 120-129/ < 80mm Hg。相似的是,一
项在中国女性人群中进行的研究表明,卒中死亡率在血压
范围较高(SBP/DBP 为 130-139/85-89mm Hg)的受试者中
显著增高,但在血压范围较低的(SBP/DBP 为 120-129/80-84mm Hg)受试者中并未增高 [24]。本研究中 35-59 岁受试
者 BP 随时间的变化进一步证明了 1 期高血压对于 35-59岁人群的危害。在 15 年的随访时间内,65.0% 的 1 期高
图 2 35-59 岁受试者血压变化与 CVD 发病风险比
0.25 0.50 1.00HRs (95% CI)
2.00 4.00 8.00
参考值
1.07 (0.61–1.88)
2.55 (1.64–3.96)
1.07 (0.44–2.60)
2.28 (1.28–4.06)
3.01 (1.94–4.69)
2.09 (0.73–6.03)
2.37 (1.16–4.81)
3.93 (2.57–6.00)
1992年SBP/DBP<130/<80 mm Hg和2007年SBP/DBP<130/<80 mm Hg
1992年SBP/DBP <130/<80 mm Hg和2007年SBP/DBP 130-139/80-89mm Hg
1992年SBP/DBP <130/<80 mm Hg和2007年SBP/DBP ≥140/≥90 mm Hg或经治疗
1992年SBP/DBP 130-139/80-89 mm Hg和2007年SBP/DBP <130/<80 mm Hg
1992年SBP/DBP 130-139/80-89 mm Hg和2007年SBP/DBP 130-139/80-89 mm Hg
1992年SBP/DBP 130-139/80-89 mm Hg和2007年SBP/DBP ≥140/≥90 mm Hg或经治疗
1992年SBP/DBP ≥140/≥90 mm Hg或经治疗和2007年SBP/DBP <130/<80 mm Hg
1992年SBP/DBP ≥140/≥90 mm Hg或经治疗和2007年SBP/DBP 130-139/80-89 mm Hg
1992年SBP/DBP ≥140/≥90 mm Hg或经治疗和2007年SBP/DBP ≥140/≥90 mm Hg或经治疗
心血管疾病发生率的HRs(95%CI)BP分级变化 数量
967
727
1122
172
272
824
50
116
1252
BP=血压;CI=置信区间;DBP=舒张压;HR=风险比;SBP=收缩压。

61JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
血压受试者血压升高至≥ 140/ ≥ 90mm Hg 水平,且 CVD发病风险为血压保持于<130/<80mm Hg 者的 3 倍。美
国 7 个不同的队列研究的汇总结果表明长期 BP 改变影响
心血管疾病风险,BP 曾高于正常水平至高血压前期的中
年人群未来 CVD 发病风险增高 [25]。
本研究发现 1 期高血压可使中青年人群 CVD 风险增
加且具有较高的 CVD 人群归因危险度,这一结果对中
国 CVD 预防具有重要意义。首先,1 期高血压具有较高
的 CVD 人群归因危险度,这表明也许可以通过充分控制
血压使之低于 1 期高血压水平来减少不良事件发生及降
低死亡风险。研究表明卒中及缺血性心脏病是中国排名
前两位导致死亡的疾病 [26]。根据本研究分析估算,若可
预防 1 期高血压,那么中国劳动年龄人群中 CVD 死亡率
可下降超过 25%,CVD 事件可减少 13%。其次,1 期高
血压进展的较大可能性及与长期 1 期高血压相关的 CVD风险表明在中国青年人群中早期将 BP 控制于< 130/ < 80mm Hg 水平的重要性。研究表明中国青年人群高血
压患病率在 1991 年至 2000 年和 2001 年之间的增长速度
已高于老年人群,35-44 岁人群的增速百分比已为 65-74岁人群的 4 倍 [27]。可以预期,1 期高血压的早诊早治可
以延缓血压升高的进展、维持血管健康、避免脏器损害,
最终可降低 CVD 风险。最后,我们的研究结果表明对
于 BP 偏高者需要更严格的生活方式干预。2017 年 ACC/AHA 高血压指南建议对 1 期高血压患者进行非药物治疗,
但对于 10 年 CVD 风险> 10% 的高危者建议药物治疗。
美国成人中高危患者比例为 1.9%[23],中国成人中高危患
者比例为 2.0%[22]。因此,生活方式干预应为 1 期高血压治
疗的基石。但在中国生活方式干预非常不佳。全国数据表
明,仅有 55.5% 的高血压患者在医务人员指导下进行非
药物治疗,且仅有 45.4% 的患者遵照医嘱执行 [27]。这些
结果表明,在中国急需呼吁医务人员及患者将更严格的
生活方式干预作为高血压管理的基础。在药物治疗方面,
中国目前正在进行 2 项多中心随机对照临床研究 [28, 29],将
为 1 期高血压患者接受降压药物治疗后的获益提供证据。
研究发现,1 期高血压对 35-59 岁人群的 CVD 风险存
在显著影响,但在≥ 60 岁的人群中与正常 BP 相比对 CVD风险影响并不显著,即使在校正竞争风险后上述结果仍未
改变。与之相似的,既往对多项队列研究进行的荟萃分
析表明前期高血压并不增加老年人群的 CVD 风险 [30, 31]。 我们的研究和其它观察研究引发了关于 SBP/DBP 为 130-139/80-89mm Hg 的 60 岁以上人群是否应被诊断为高血压
并降低 BP 至 130/80mm Hg 以下的重要讨论。近期发表
的一篇荟萃分析表明,在基线收缩压处于 140-170mm Hg水平的老年人群中,强化降压将 SBP 降低至< 140mm Hg 可降低 CVD 风险 [32]。该分析中,纳入的 4 项研究中
有 3 项强化降压组的 SBP 为 135mm Hg 左右,仅在 1 项
研究中高危患者治疗后 SBP < 130mm Hg,BP 测量通过
患者自测完成。与本观察性研究结果相一致的干预试验
表 明, 在 ≥ 60 岁 且 SBP/DBP 为 130-139/80-89mm Hg 范
围的人群中高血压的诊断及降压治疗应谨慎。
研究的局限性 首先,在长期队列研究中,基于基线 BP水平获得的 1 期高血压相关心血管风险,可能因回归稀
释偏倚而被低估。其次,尽管在研究中我们校正了全部
典型 CVD 危险因素,但未能排除一些尚未明确的混杂因
素的影响。再次,研究样本量虽较大,但在分析 BP 变化
时只反映了原始队列的一部分。需注意的是,只有 250例年龄≥ 60 岁的受试者在 15 年随访期内分别完成了两
次体检,排除 60 岁以上人群中与 BP 变化有关的心血管
风险研究之后,研究中未发现该人群中基线状态下 1 期
高血压与心血管终点事件间存在相关性。除了对 CHD 发
病率分析能力不足之外,与年轻人群比,年龄≥ 60 岁的
受试者样本量对于研究 1 期高血压对所有其他终点事件发
生风险的影响是足够的。因此,本研究结果尚需在纳入更
多老年受试者的研究中进一步验证。最后,为确定失访者
是否对研究造成了潜在偏倚,我们比较了有两次体检信
息及无两次体检信息患者的情况。两组受试者 SBP 水平
(121.4±18.3.mm Hg vs. 121.8±19.9mm Hg)及 DBP 水 平
(79.2±11.6mm Hg vs. 79.7±12.3mm Hg)均相近。
结论
2017 年 ACC/AHA 高血压指南中定义的 1 期高血压
显著增加了中国 35-59 岁人群 CVD 发病率及死亡率,且
人群中大部分的 CVD 事件及死亡与其相关;但在≥ 60岁的人群中未观察到上述现象。本研究对 1 期高血压对
CVD 风险的影响进行了研究,为未来相关领域健康经济
学研究提供了依据,而该领域的研究结果对于决定中国
是否会采用新的高血压诊断标准是必要的。
致谢 The authors are grateful to all of the investigators from
participating centers in the CMCS study for providing data collection.
通信地址 Dr. Jing Liu, Beijing An Zhen Hospital, Capital Medical University, Beijing Institute of Heart, Lung and Blood Vessel Diseases, No. 2 Anzhen Road, Chaoyang District, Beijing 100029, China. E-mail:

62 JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
观 点
患者治疗和操作技巧的能力 新定义的 1 期高血压与
心血管风险相关,中国 35-59 岁之间人群的大部分心
血管事件和死亡率可归因于这一血压分级,但在 60岁或以上的人群中则不然。
转化前景 需要广泛的策略来促进中青年人群中 1 期
高血压的检测,而在将此阈值应用于年龄≥ 60 岁的个
体之前还需要更多证据。
参考文献
1. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71:2199–269.2. Report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. A cooperative study. JAMA 1977; 237:255–61.3. The sixth report of the Joint National Commit tee on Prevent ion , Detec t ion , Evaluation, and Treatment of High Blood Pressure. Arch Intern Med 1997;157:2413–46.4. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;385:117–71.5. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990-2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet 2016;387:251–72.6. Li D, Lv J, Liu F, et al. Hypertension burden and control in mainland China: analysis of nationwide data 2003-2012. Int J Cardiol 2015; 184:637–44.7. Lu J, Lu Y, Wang X, et al. Prevalence, awareness , t r ea tment , and con t ro l o f hypertension in China: data from 1.7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet 2017;390:2549–58.8. Wang Z, Chen Z, Zhang L, et al., for the China Hypertension Survey Investigators. Status of hypertension in China: results from the China Hypertension Survey, 2012-2015.
Circulation 2018;137:2344–56.9. Bundy JD, He J. Hypertension and related cardiovascular disease burden in China. Ann Glob Health 2016;82:227–33.10. NCD Risk Fac to r Col labora t ion . Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet 2017;389:37–55.11. National Bureau of Statistics of the People’s Republic of China. The Sixth National Population Census of the People’s Republic of China. 2010. Available at: http://www.stats.gov.cn/tjsj/pcsj/ rkpc/6rp/indexch.htm. Accessed April 15, 2018.12. Li G, Liu J, Wang W, et al. [Prediction models for the 15 years risk of new-onset hypertension in Chinese people aged from 35 to 64 years old]. Zhonghua Nei Ke Za Zhi 2014;53: 265–8.1 3 . G u D , C h e n J , W u X , e t a l . Prehypertension and risk of cardiovascular disease in Chinese adults. J Hypertens 2009;27:721–9.14. Liu J, Hong Y, D’Agostino RB Sr., et al. Predictive value for the Chinese population of the Framingham CHD risk assessment tool compared with the Chinese Multi-Provincial Cohort Study. JAMA 2004;291:2591–9.15. Li Y, Liu J, Wang W, Zhao D. The association between within-visit blood pressure variability and carotid artery atherosclerosis in general population. PLoS One 2014;9:e97760.16. Wu Z, Yao C, Zhao D, et al. Sino-MONICA project: a collaborative study on trends and determinants in cardiovascular d i s e a s e s i n C h i n a , p a r t I : m o r b i d i t y and mortal i ty monitor ing. Circulat ion 2001;103:462–8.17. Wang Y, Liu J, Wang W, et al. Lifetime risk for cardiovascular disease in a Chinese population: the Chinese Multi-Provincial Cohort Study. Eur J Prev Cardiol 2015;22:380–8.18. Luepker RV, Apple FS, Christenson RH,
et al. Case definitions for acute coronary heart disease in epidemiology and clinical research studies: a statement from the AHA Council on Epidemiology and Prevention; AHA Statistics Committee; World Heart Federation Council on Epidemiology and Prevention; the European Society of Cardiology Working Group on Epidemiology and Prevention; Centers for Disease Control and Prevention; and the National Heart, Lung, and Blood Institute. Circulation 2003;108:2543–9.19. Brunstrom M, Carlberg B. Association of blood pressure lowering with mortality and cardiovascular disease across blood pressure levels: a systematic review and meta-analysis. JAMA Intern Med 2018;178:28–36.20. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Statistical Assoc 1999;94:496–509.21. Wander GS, Ram CVS. Global Impact of 2017 American Hear t Associa t ion/American College of Cardiology Hypertension Guidel ines : a perspect ive f rom India . Circulation 2018;137: 549–50.22. Wang JG, Liu L. Global impact of 2017 American College of Cardiology/American Heart Association Hypertension Guidelines: a perspect ive from China. Circulat ion 2018;137:546–8.23. Muntner P, Carey RM, Gidding S, et al. Potential US population impact of the 2017 ACC/AHA High Blood Pressure Guideline. Circulation 2018; 137:109–18.24. Huang Y, Su L, Cai X, et al. Association of all-cause and cardiovascular mortality with prehypertension: a meta-analysis. Am Heart J 2014; 167:160–8.e1.25. Allen N, Berry JD, Ning H, Van Horn L, Dyer A, Lloyd-Jones DM. Impact of blood pressure and blood pressure change during middle age on the remaining lifetime risk for cardiovascular disease: the cardiovascular lifetime risk pooling project. Circulation 2012;125:37–44.

63JACC VOL. 72, NO. 11, 2018SEPTEMBER 11, 2018:1201–10
Qi et al.1 期高血压的心血管疾病风险
26. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet 2013;381:1987–2015.27. Gu D, Reynolds K, Wu X, e t a l . Prevalence, awareness, treatment, and control of hypertension in china. Hypertension 2002;40:920–7.28. World Health Organization International Clinical Trials Registry Platform. Study of Antihypertensive Treatment in Patients with High-normal Blood Pressure and Risk Factors (CHINOM). Available at: http://apps.who.int/trialsearch/Trial2. aspx?TrialID=ChiCTR-TRC-10000848. Accessed April 15, 2018.
29. ClinicalTrials.gov. Intervention for High-normal or Borderline-elevated Blood Pressure in Adults With Type 2 Diabetes (IPAD). Available at: https://clinicaltrials.gov/ct2/show/NCT03264352? Term=IPAD&cntry1=ES%3ACN&rank=1. Accessed April 15, 2018.30. Wang S, Wu H, Zhang Q, Xu J, Fan Y. Impact of baseline prehypertension on cardiovascular events and all-cause mortality in the general population: a meta-analysis of prospective cohort studies. Int J Cardiol 2013;168: 4857–60.31. Guo X, Zhang X, Guo L, et al. Association between pre-hypertension and cardiovascular outcomes: a systematic review and meta-
analysis of prospective studies. Curr Hypertens Rep 2013; 15:703–16.32. Bavishi C, Bangalore S, Messerli FH. Outcomes of intensive blood pressure lowering in older hypertensive patients. J Am Coll Cardiol 2017;69: 486–93.
关键词 心血管疾病,队列研究,高血压,
发病率,死亡率
附录 参与的研究中心和主要研究人员的列
表以及补充图片和表格,请参阅本文的线
上版本。
南京市第一医院 陈绍良
2017 年美国心脏病学会 / 美国心脏协会(ACC/AHA)高血压指南将高血压的 1 级诊断标准从收缩压 / 舒张压
140/90 mm Hg 降至 130/80 mm Hg,这一新的指南是否也适用于中国人群?中国作为高血压发病率高及中风死亡率高
的一个国家,如果按照 2017ACC/AHA 提出的 1 级高血压诊断标准(SBP/DBP:130-139/80-89 mm Hg)定义我国人
群,该范围内的血压会带来怎样的心血管不良事件风险预测?尤其针对不同年龄段的人群有哪些差异?
本研究是 CMCS(Chinese Multi-provincial Cohort Study)研究的一项延伸性分析,是一项长达 20 年的前瞻性队
列研究,该研究从 1992 年至 2004 年都有人群陆续入组,所有入组人群每 1-2 年均回访记录新发心血管不良事件,近
20 年的随访率达 81%,总共 21,441 例参与者完成全部随访,其中男性 11,047 例,女性 10,394 例。结果显示:按照
2017ACC/AHA 定义的 1 级高血压(130-139/80-89 mm Hg),总共有 25.8% 的人群是 1 级高血压患者,不同的年龄段
发生心血管事件的风险不同。
1. 在 35-59 岁人群中,与血压 <120/80 mm Hg 组人群相比,1 级高血压人群发生心血管疾病的相对危险度(HR)是
1.77(95% CI:1.33-2.36);中风的 HR 是 1.79(95% CI:1.45-2.22);心血管死亡的 HR 是 2.50(95% CI:1.66-3.77)。 而心血管不良事件及死亡的发生率分别是 26.5%、13.4%。
2. 在 35-59 岁人群中,近 15 年有 65% 的人群进展为血压大于等于 140/90 mm Hg,比那些血压维持在 <130/80 mm Hg 的人群心血管事件风险增加 3.01 倍。
3. 在大于等于 60 岁以上的人群中,与血压 <120/80 mm Hg 组人群相比,1 级高血压组未发现以上不良事件的差异。
该研究是我国第一项分析 2017ACC/AHA 提出的新的 1 级高血压定义在中国人群中长期心血管不良事件风险预测
的队列研究,它提示了以下几项结果:第一,新的 1 级高血压定义能较好的预测中国年轻人群(35 岁至 65 岁)的心
血管不良事件(包括心血管疾病、中风及心血管死亡),但对于年龄偏大(超过 60 岁)的患者并无优势;第二,血压的
逐渐进展与心血管事件的风险暴露增加密切相关,这提示了我国应重视 1 级高血压人群的血压管理,将年轻人群的血压
控制在 <130/80 mm Hg 更加安全。第三,对于 1 级高血压人群,应更加强调生活方式的管理,依据 2017ACC/AHA 指南
的推荐,并非所有的 1 级高血压人群都需要立即药物治疗,推荐首选生活方式的控制与管理,药物治疗仅推荐给 10 年
心血管事件风险超过 10% 的人群。据统计,仅 1.9% 的美国和 2.0% 的中国高风险人群需要药物治疗。第四,60 岁以上
的老年人群并不适用于 1 级高血压定义的管理,因为这一范围的血压在风险评估上并未发现临床意义。因此,2017 年
ACC/AHA 定义的 1 级高血压标准更加适用于我国相对较年轻的人群血压管理,而不适用于 60 岁以上的人群。
点 评
Related Documents