Brucellosis with p-ANCA- associated renal failure and leukocytoclastic vasculitis, endocarditis : a case report. *, Orhan Küçükşahin*Ali Şahin* * Ankara University Medical Faculty, Rheumatology Department ABSTRACT: Brucellosis is a systemic infectious disease caused by pathogens of the genus Brucella. We report a case of brucellosis with perinuclear anti-neutrophil cytoplasmic antibody (p-ANCA) associated renal failure, leukocytoclastic 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Brucellosis with p-ANCA- associated renal
failure and leukocytoclastic vasculitis,
endocarditis : a case report.
*, Orhan Küçükşahin*Ali Şahin*
* Ankara University Medical Faculty, Rheumatology Department
ABSTRACT: Brucellosis is a systemic infectious disease
caused by pathogens of the genus Brucella. We report a case of
brucellosis with perinuclear anti-neutrophil cytoplasmic
antibody (p-ANCA) associated renal failure, leukocytoclastic
1
vasculitis, and endocarditis. No similar case has been
reported previously in regard to p-ANCA anti-lactoferrin
antibodies associated glomerulonephritis in brusellosis in the
literature.
Key words. Brucellosis, p-ANCA, glomerulonephritis,
leukocytoclastic vasculitis, endocarditis, anti-lactoferrin
antibodies
Orhan Küçükşahin
Ankara Universitesi Tıp Fakültesi,
İbni sina Hastanesi,
Romatoloji Bilim Dalı.
4.kat c-Blok . Sıhhıye 06140
ANKARA/TÜRKİYE
Tlf:+90-312-3103333 / 2658
Fax:+90-312-3097779
e-mail: [email protected]
2
Brusellosis is a systemic infectious disease and still a
serious health problem in developing countries. The organism
enter the body by ingestion of contaminated milk products or by
direct contact. The disease can affect virtually any organ
(1). For this reason, Brucellosis shows variability in clinical
presentation.The disease can frequently affect the
musculoskeletal system. Cardiac involvement occurs in less
than 2% of the cases (2,3). Endocarditis is a severe and a
lethal complication and is more frequent in men. There is
usually involvement of the aortic valve (1,3-6,7). During the
course of Brusellosis, microorganism can be isolated from urine
(9), but serious renal involvement is uncommon (2,10,11). Skin
manifestations affect less than 5 % of the patients, and there
are no characteristic skin lesions in association with
brucellosis infection ( 2,12 ). Palpable purpura indicates the
3
presence of leucocytoclastic vasculitis related with
accumulation of immune complexes.(14) In this case, a case
with brucellosis who was consulted to our outpatient clinics
for palpable purpura was presented ,endocarditis and ANCA-
related glomerulonephritis was detected. in clinical
evaluation
Case :
A 52 year old male was admitted to the Emergency Department
with a three months history of progressively worsening
fatigue, swelling of the legs, intermittent fever reaching
39°C, night sweating, diffuse arthralgia, myalgia, abdominal
pain, and purpuric rash on his legs. His blood pressure was
140/90 mmHg, body temperature was 38.4°C, pulse was regular,
110 beats /min. Physical examination revealed palpabl purpura
on legs and hips, systolic murmur in the area of the aortic
valve. He had lost 8 kg of weight in three months. He had no
known previous illness and no dyspnea and palpitations on
exertion. Laboratory examination revealed ESR:52 mm/hr,
CRP:20.0 mg/L (N:0-3mg/L), hemoglobine (Hb): 7.8g/dL, white
blood cell count (WBC): 7950 (72% neutrophile, 19% lymphocyte),
4
microscopic hematuria and proteinuria (100mg/dl). Occult stool
blood was negative. Hemoptysis or melena was not detected.
After blood cultures were taken and skin biopsy was performed,
methylprednisolone 40mg/d (0.5mg/kg/d) was started.
A week later he was accepted to Rhematology Department
with the diagnosis of leukocytoclastic vasculitis. His physical
examination revealed fever: 37°C, pulse 108 beats /min, blood
pressure 150/100 mmHg, respiratory rate 18/min. An aortic
systolic murmur (grade II/VI), and mitral systolic murmur
( grade I/V ) were audible. Palpabl purpura was most
prominent on the legs and hips , less on the upper arms. His
neurological, respiratuar , gastrointestinal and
musculoskeletal examinations were normal. Laboratory
evaluation revealed: Hb:7.1g/dl, Htc: 22 %, WBC: 5560/mm3
(granulocyte 81%, lymphocyte 12%), platelets 248.000/ mm3,
ESR:34 mm/hr, CRP:11.40mg/dl, blood urea nitrogen :10 mg/dl
(N:6-20 mg/dl), creatinine:1.1g/dL(N:0.7-1.1 mg/dl), total
protein:7.2 g/dL(N:6.6-8.3 g/dl), albumin:2.9g/dl (N:3.5-5.2).
Urine analysis revealed proteinuria (100mg/dL), and 20-25/hpf
erythrocytes. Twenty-four hour urinary protein excretion was
1800 milligram, the urine culture was negative. C3 complement
5
(C3) was 0.764 g/L (N:0.9-2g/L)), There is no evidence of
monoclonal gammopathy in the protein and urine
immunoelectrophoresis. Rheumatoid factor, antinuclear antibody,
anti-dsDNA, and cryoglobulin were negative. p-ANCA was
positive, and ELISA revealed positive anti-lactoferrin
antibody (16,8 U/ml; N:0-15). Chest X-Ray, and renal
ultrasonography were normal. Electrocardiography revealed
sinusal tachycardia. Brucella serum agglutination test was
positive at a titer of 1/1280. Anti-Brusella lgG and lgM
antibodies by ELISA were positive. He was started rifampin
600mg/d and doxycycline 200mg/d for brucellosis. When we
questioned our patient about entrance of the infection we
noticed that he had intake of nonpasteurized dairy products.
Skin biopsy taken from purpuric lesions revealed
leukocytoclastic vasculitis with vascular deposition of IgM,
IgA and C3 (figure I). Blood cultures were positive for
brucella. After transthoracic and transesophageal
echocardiography revealed vegetation on the aortic valve and
second degree aortic regurgitation (figure II), his medical
therapy was rearranged as doxycycline (200mg/d), rifampin
(600mg/d) and ceftriaxone (2g/d).
6
In the clinical follow-up his renal functions detoriated
day by day. He was consulted to the Department of Nephrology.
Renal biopsy was planned due to persistent proteinuria,
hematuria and rapidly detoriating renal functions, but he
refused renal biopsy. BUN and serum creatinine levels were
increased day by day reaching values of 98mg/dl and 4.5
mg/dl respectively. He was accepted as p-ANCA-associated
rapidly progressive glomerulonephritis (RPGN) and given 1gm/d
intravenous pulse methylprednisolone once and then 2mg/kg/d.
Renal function impairment could not be controlled under
medical therapy, so plasmapheresis was applied three times in
the consecutive days. Following plasmapheresis ,his renal
functions started to improve. Fifteen days after the begining
of brucellosis therapy thrombocytopenia (60.000 / mm3 ) was
detected. Brucella associated bone marrow involvement was
excluded by bone marrow biopsy . It was accepted as rifampin –
induced thrombocytopenia. The therapy was switched to
ciprofloxacin (1g/d). After medical therapy for six weeks,he
had aortic valve replacement with no complications , and was
discharged with doxycycline (200mg/d) and ciprofloxacin (1g/d)
therapy for 6 more months.
7
Discussion:
Brucellosis is endemic in Türkiye. The incidence of
Brucella infection was 14/100,000 in our country (1). The most
common symptoms are fever, myalgia, arthralgia, low-back pain
and weight loss. Definitive diagnosis is based on recovery of
the organism from the blood, but it is hard to grow in
cultures, and in this case serologic tests are important
(5). The diagnosis mostly depends on the positive brucella
tube agglutination test when the titer is 1/160 or higher (4).
Our patient had fever, arthralgia, myalgia, fatigue,
weight loss, vasculitic purpuric lesions. Blood cultures, tube
agglutination and ELISA results revealed Brucella infection.
Cutaneous manifestations in brucellosis are rare
(2,12,14). Skin lesions were not characteristic. 7 % of these
lesions were extensive purpuric lesions, 11% were diffuse
maculopapular rash (2,9). There were reports of
leukocytoclastic vasculitis (2, 12,13,14). Cutaneous lesions
could be result of direct inoculation, hypersensitivity
phenomena, deposition of immune complexes or direct invasion
by the organism (2). Cryoglobulinemia has been described very
8
rarely in brucellosis and may be the cause of cutaneous
vasculitis (13,14).
Our patient had palpabl purpura and skin biopsy revealed
leukocytoclastic vasculitis. He had no medication use before
the lesions developed, and no eosinophilia. Cryoglobulin was
negative in our case. Therefore it was accepted as the
cutaneous manifestation of brucellosis, and lesions were
healed under therapy. The presence of brucella endocarditis
make us think that the reason of leucocytoclastic vasculitis
might be related with immune complex accumulation.
Hematologic alterations are common in brucellosis, mostly
leukopenia, relative lymphocytosis, and thrombocytopenia.
Pancytopenia occurs in 5-20% (2,15). Our patient developed
thrombocytopenia after rifampin use and bone marrow
examination was normal. After ciprofloxacin was started
instead of rifampin , thrombocyte count was normalized.
Therefore thrombocytopenia was accepted as drug- related side
effect.
During the course of brucellosis mild proteinuria is
common, but biopsy-proven glomerulonephritis is very rare
(2,9,10,11). The mechanisms for renal involvement is multiple.
9
Interstitial nephritis caused by directly invasion of bacteria
is most frequently. Therefore, glomerulonephritis due to
accumulation of circulating immune complexes may occur. In our
case, co-existance with endocarditis was present.
Rapidly progressive glomerülonefrit is a clinical syndrome
with an abrupt onset or an insidious onset of hematuria,
proteinuria, anemia, and rapidly progressing renal failure .
Yamagata et al. reported benficial effects of apheresis in
RPGN (11,16). Infections induce glomerulonephritis by
formation of immune complexes and their deposition in the
kidney (11,14,17). Our patient had microscopic hematuria,
proteinuria, p-ANCA positivity , decreased C3 level, and
rapidly detoriating renal functions, therefore RPGN was
diagnosed. Clinical improvement was not observed under
medical therapy, and plasmapheresis was applied. Renal
functions started to return to normal levels following
plasmapheresis. Serum C3 level returned to normal limits, and
proteinüria regressed to 600mg/d. The improvement in renal
functions , hypocomplementemia, and the decrease in the
level of proteinuria together with the resolution of
10
clinical findings after therapy led us to believe that
Brucella infection was the cause of glomerulonephritis.
Lactoferrin is one of the targets for ANCA. Lactoferrin
exerts antimicrobial activity, immune-modulatory and anti-
inflamatory functions, and may contribute to neutrophil
activation by the organisms (18,19) .Anti-lactoferrin
antibodies may hamper these functions , leading to an
increased inflammatory condition. Anti-lactoferrin antibodies
may be detectable in patients with infections (18). Our
patient had p-ANCA , and anti-lactoferrin antibody positivity
with RPGN . After 6 week of therapy, ANCA was negative. This
was another indication for brucella infection as the cause
of RPGN.
Brusella endocarditis is an uncommon but a serious and
lethal complication (3,6,7). The aortic valve is the most
frequently affected cardiac valve (3,5,6,7). In Türkiye, the
rate of endocarditis was 0.7% (1). Blood cultures are usually
negative in uncomplicated chronic brucellosis and positive
blood cultures indicate probability of endocarditis (6). Cure
of brucella endocarditis with medical treatment alone has
been reported occasionally (3,6,8). Antibiotic therapy
11
followed by surgery seems to be the most effective treatment
(1,4,6,7). After six weeks of medical therapy , our patient
had aortic valve replacement .And he was discharged with
doxycycline (200mg/d) and ciprofloxacin (1g/d) therapy for 6
more months.
We present a patient with brucella and p-ANCA associted
renal failure, endocarditis, and leukocytoclastic
vasculitis . Clinical and laboratory evidence of vasculitis
and ANCA-associated renal failure disappeared after
corticosteroid and antibiotic treatment combined with
plasmapheresis. No similar case has been reported previously
in regard to brucellosis with p-ANCA associated
glomerulonephritis in the literature.
References:
1- Mert A, Kocak F, Ozaras R, Tabak F, Bilir M, Kucukoglu S,
Ozturk R, Aktuglu Y. The role of antibiotic treatment alone
for the management of brucella endocarditis in adults: a case
report and literature review. Ann Thorac Cardiovasc Surg
2002;8:381-5.
2- Colmenero JD, Reguera JM, Martos F, Sanchez-de-Mora D,
Causse M, Martin
12
Farfan A, Juarez C. Complications associated with Brucella
melitensis infection:
a study of 530 cases.medicine 1996;75:195-210.
3- Reguera JM, Alarcon A, Miralles F, Pachon J, Juarez C,
Colmenero JD: Brucella endocarditis: clinical, diagnostic and
therapeutic approach. Eur J Clin Microbiol Infect Dis
2003;22(11):647-50.
4- Ozsoyler İ, Yilik L, Bozok S, El S, Emrecan B, Biceroglu S,
Gurbuz A:Brucella endocarditis : The importance of surgical
timing after medical treatment (five cases). Progress In
Cardiovascular Diseases 2005;47(4):226-229.
5- Sharıvker D, Vazan A, Varkel J. Brucella endocarditis
complicated by acute glomerulonephritis-early surgical
intervention. Acta Cardiol 2001;56(6):399-400.
6- Leandro J, Roberto H, Antunes M. Brucella endocarditis of
the aortic valve. Eur J Cardiothorac Surg 1998;13(1):95-97.
7- Ahmet Sasmazel, Ayse Baysal,Ali Fedakar, Onursal Bugra,
Mehmet Özkokeli, Fuat Büyükbayrak, Cüneyt Keles¸, Sinan Göçer,
Hasan Sunar, and Rahmi Zeybek. Treatment of Brucella
Endocarditis: 15 Years ofClinical and Surgical Experience. Ann
Thorac Surg 2010;89:1432–6
13
8- Keleş C, Bozbu N, Şişmanoğlu M, Güler M, Erdoğan HB, Akinci
E, Yakut C. Surgical treatment of brucella endocarditis. The
Annals of Thoracic Surgery 2001;71(4):1160-63.
9- Siegelmann N, Abraham AS, Rudensky B, Shemesh O. Brucellosis
with nephrotic syndrome, nephritis and IgA nephropathy.
Postgrad Med J 1992;68:834-36.
10- Altınparmak MR, Pamuk GE, Pamuk ÖN, Tabak F. Brucella
glomerulonephritis: review of the literature and report on
the first patient with brucellosis and mesangiocapillary
glomerulonephritis. Scand J Infect Dis 2002;34(6):477-80.
11- Kadir Ceylan, Mustafa Kasım Karahocagil, Yasemin Soyoral,
Hayriye Sayarlıoglu,Hasan Karsen, Ekrem Dogan, Hayrettin
Akdeniz, Irfan Bayram, Mustafa Kösem, and Reha Erkoc .Renal
Involvement in Brucella Infection. UROLOGY 73: 1179–1183, 2009
12- Millionis H, Christou L, Elisaf M. Cutaneous menifestations
in Brucellosis:case report and review of the literature.
Infection 2000;28:124-126.
14
13- Hermida LI, Saez ML, Solera SJ. Mixed cryoglobulinemia with
renal failure, cutaneous vasculitis and peritonitis due to
Brucella melitensis. J Infect 2005; 51(5):e 257-9
14- Dizbay M, Hizel K, Kilic S, Mutluay R, Ozkan Y, Karakan T.Brucella peritonitis and leucocytoclastic vasculitis due to brucella melitensis. Braz J Infect Dis. 2007 Aug;11(4):443-4
15- Lee MKP, Fung KSC. A case of human brucellosis in Hong
Kong. Hong Kong Med J 2005;11:403-6.
16- Yamagata K, Hirayama K, Mase K, Yamaguchi N, Kobayashi M,
Takahashi H, Koyama A. Apheresis for MPO-ANCA-associated RPGN-
Indications and efficacy: lessons learned from Japan Nationwide
survey of RPGN. J Clin Apher. 2005; 20(4): 244-51
17- Elzouki AY, Akthar M, Mirza K. Brucella endocarditis
associated with glomerulonephritis and renal vasculitis.
Pediatr Nephrol 1996;10:748-51.
18- Caccavo D, Rigon A, Picardi A, Galluzzo S, Vadacca M, Ferri
GM, Amoroso A, Afeltra A. Anti-lactoferrin antibodies in
systemic lupus erythematosus: isotypes and clinical correlates.
Clin Rheumatol 2005;24:381-87.
15
19-Deriy LV, Chor J, Thomas LL. Surface expression of
lactoferrin by resting neutrophils. Biochemical and Biophysical
Research Communications 2000; 275:241-46.
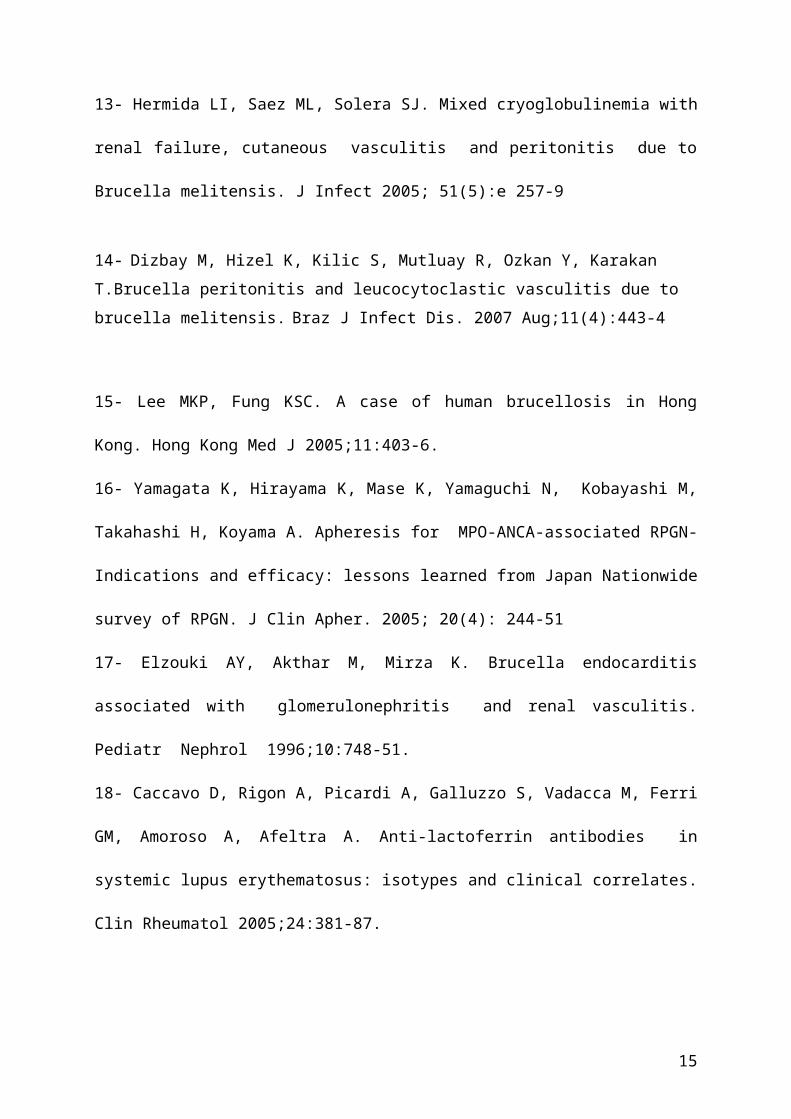
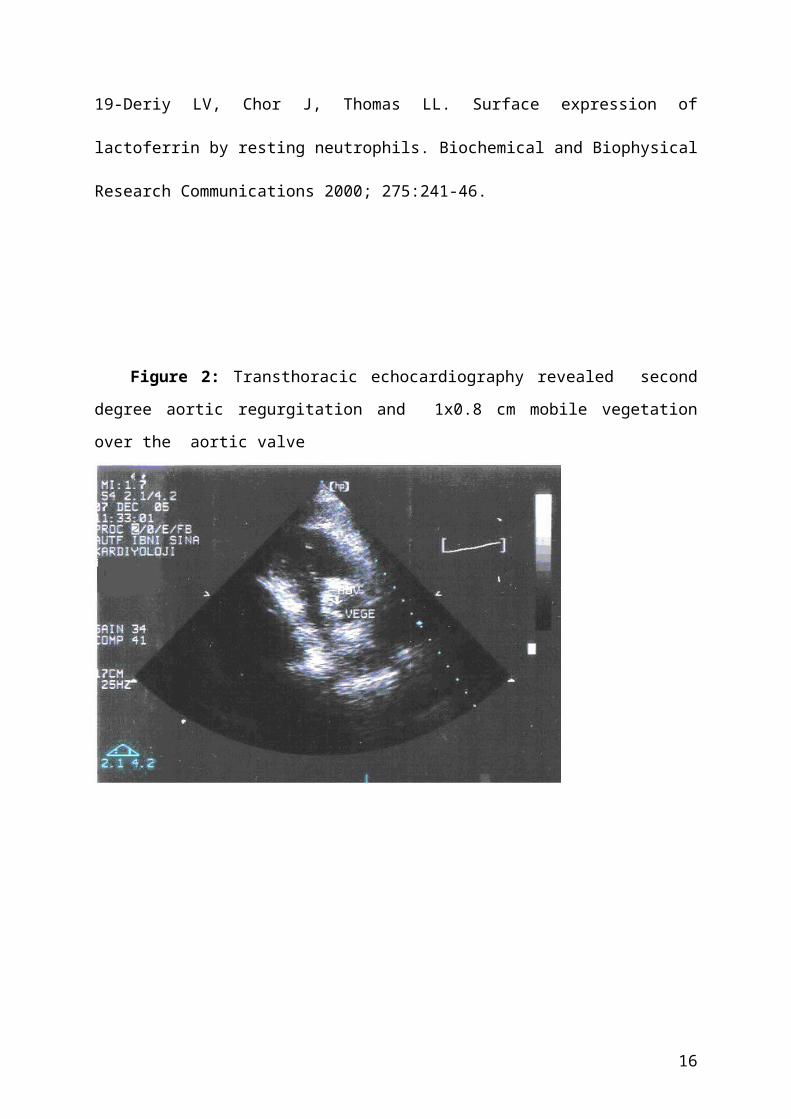
Figure 2: Transthoracic echocardiography revealed second
degree aortic regurgitation and 1x0.8 cm mobile vegetation
over the aortic valve
16
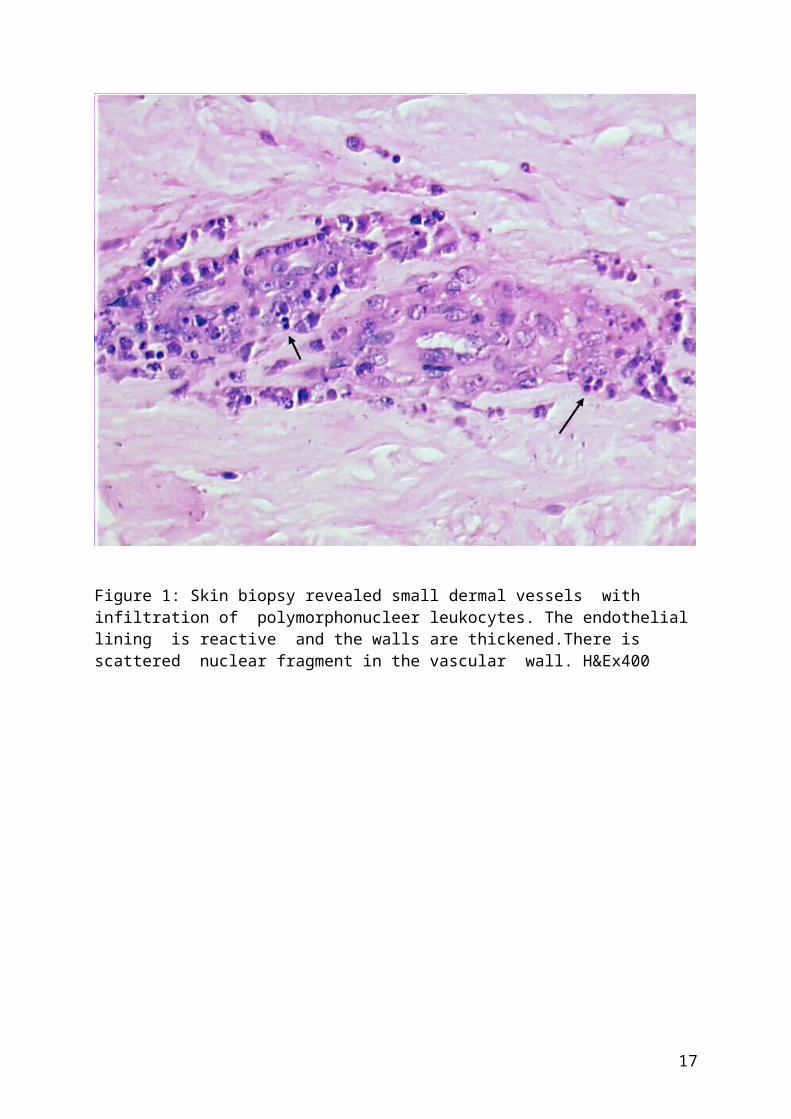
Figure 1: Skin biopsy revealed small dermal vessels with infiltration of polymorphonucleer leukocytes. The endothelial lining is reactive and the walls are thickened.There is scattered nuclear fragment in the vascular wall. H&Ex400
17
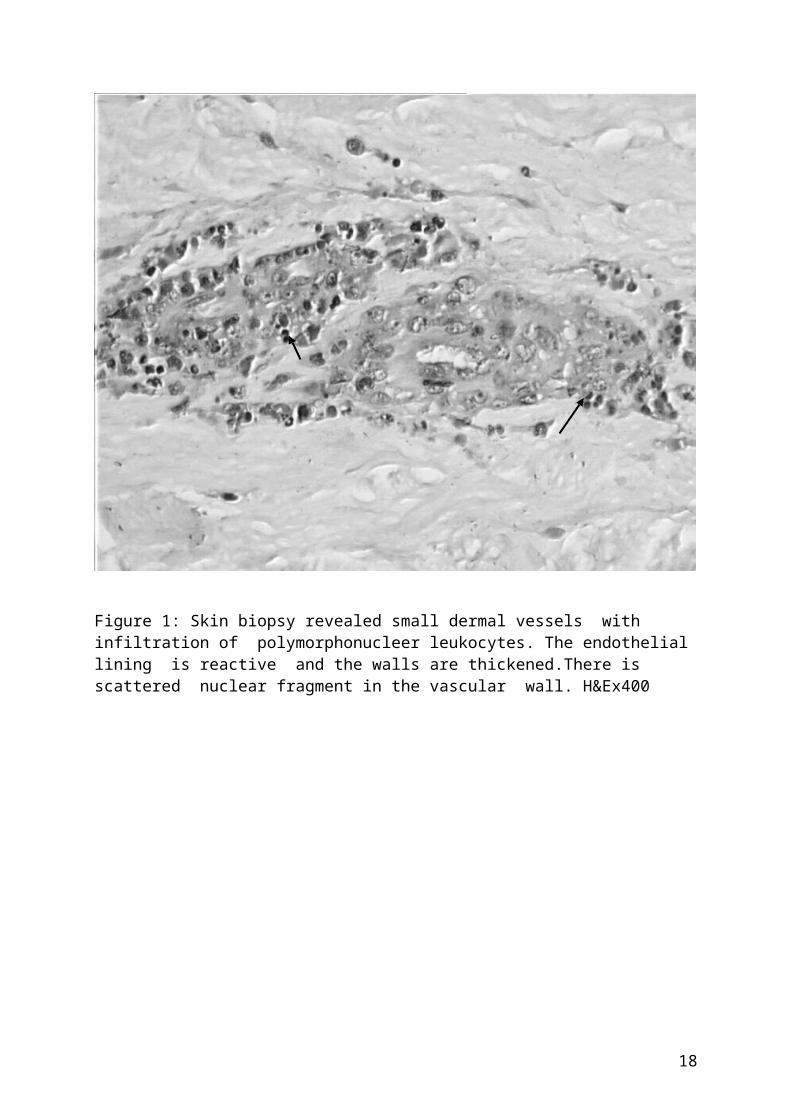
Figure 1: Skin biopsy revealed small dermal vessels with infiltration of polymorphonucleer leukocytes. The endothelial lining is reactive and the walls are thickened.There is scattered nuclear fragment in the vascular wall. H&Ex400
18

19
Related Documents











